Parent Handbook - ACT Health€¦ · · 2015-04-20Parent Handbook. Accessibility ... • Prior to...
56
The Centenary Hospital for Women & Children Neonatal Intensive Care Unit & Special Care Nursery Parent Handbook
Transcript of Parent Handbook - ACT Health€¦ · · 2015-04-20Parent Handbook. Accessibility ... • Prior to...

The Centenary Hospital for Women & Children
Neonatal Intensive Care Unit& Special Care Nursery
Parent Handbook

Accessibility
The ACT Government is committed to making its information, services, events and venues as accessible as possible.
If you have difficulty reading a standard printed document and would like to receive this publication in an alternative format such as large print, please phone 13 22 81 or email [email protected]
If English is not your first language and you require the Translating and Interpreting Service (TIS), please call 13 14 50.
If you are Deaf, or have a speech or hearing impairment and need the teletypewriter service, please phone 13 36 77 and ask for 13 22 81.
For speak and listen users, please phone 1300 555 727 and ask for 13 22 81. For more information on these services visit http://www.relayservice.com.au
© Australian Capital Territory, Canberra, January 2014
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without written permission from the Territory Records Office, Community and Infrastructure Services, Territory and Municipal Services, ACT Government, GPO Box 158, Canberra City ACT 2601.
Enquiries about this publication should be directed to ACT Government Health Directorate, Communications and Marketing Unit, GPO Box 825 Canberra City ACT 2601 or email: [email protected]
www.health.act.gov.au | www.act.gov.au Enquiries: Canberra 13ACT1 or 132281

Congratulations on the birth of your baby
Baby’s Name
Born On
Place of Birth
Weight
Head Circumference
Length
Date Discharged
Weight at Discharge
Weight Conversion ChartOunces
Pounds 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
0 GRAMS 28 57 85 113 142 170 198 207 225 284 312 340 369 387 425
1 454 482 511 539 567 596 624 652 681 709 738 766 794 823 851 879
2 907 935 964 992 1020 1049 1077 1105 1134 1162 1191 1219 1247 1276 1304 1332
3 1361 1389 1418 1446 1474 1503 1531 1559 1588 1616 1645 1673 1701 1730 1758 1786
4 1814 1842 1871 1899 1927 1956 1984 2012 2041 2069 2098 2126 2154 2183 2211 2239
5 2268 2296 2325 2353 2381 2410 2438 2466 2495 2523 2552 2580 2608 2637 2665 2693
6 2772 2750 2779 2807 2835 2864 2892 2920 2949 2977 3006 3034 3062 3091 3119 3147
7 3175 3203 3232 3260 3288 3317 3345 3373 3402 3430 3459 3487 2515 3544 3572 3600
8 3629 3657 3686 3714 3742 3771 3799 3827 3856 3884 3913 3941 3969 3998 4026 4054
9 4082 4110 4139 4167 4195 4224 4252 4280 4309 4337 4366 4394 4422 4451 4479 4507
10 4536 4564 4593 4621 4649 4678 4706 4734 4763 4791 4820 4848 4876 4905 4933 4961

Important Information:For the protection of all the babies:
• Hand washing (up to the elbows with jewellery off) is the most effective precaution in the prevention of infection whilst caring for your baby.
• Please ask visitors to text or ring you on arrival, so you can let them in with your Proximity Card & accompany them into the unit.
• Please limit visitors at the bedside to a parent & two others.
• Children (under 12 years) other than your own are not permitted in the unit.
• If any visitor has an infection it will be necessary to exclude them from visiting.
• 1-3 pm is a `baby rest time’ and parents only are permitted. This is a quiet time for babies to have a deep undisturbed sleep.
• Prior to discharge please return your Proximity Card, in the supplied envelope to the ward clerk or your baby’s nurse.
NICU/ SCN BED NUMBER PHONE NUMBER
Switchboard 02 6244 2222
NICU/SCN Reception 02 6174 7330
NICU Nurse Station 02 6174 7320
SCN Nurse Station 02 6174 7311

Parent Handbook 1
Welcome to the NICU/SCN 2
Mission Statement 3
Family Centred Care 3
The NICU/SCN Team 4
Care of your baby/what to expect 7
Visitor’s guidelines 8
Family centred care 11
Breastfeeding information 12
General Information 17
Spiritual Support 19
NICUCAM 19
Miracle Babies 21
Ronald McDonald House 22
Facilities in the main hospital foyer 23
Transfer of babies 24
Retrieval Service 25
Newborn hearing screen 25
NAPSS – Newborn & Parent Support Service 26
Tube feeding at home 27
NICU Growth & Development Clinic 28
Baby’s early development 28
Kangaroo Care 30
Learning baby’s signals 31
Going home 35
Canberra Hospital Map 36
NICU/SCN Map 37
Calvary ‘Bruce’ Hospital SCN Map 38
Calvary ‘John James’ SCN Map 39
Medical terms & equipment 40
Newborn Intensive Care Foundation 45
Parent Feedback Form 49
Contents

2 Neonatal Intensive Care Unit & Special Care Nursery
Welcome to the NICU/SCN
Congratulations on the birth of your baby! Your baby has been admitted to the Neonatal Intensive Care Unit (NICU) or Special Care Nursery (SCN). These units care for premature babies and infants up to two years of age requiring intensive care. Whether your baby is here for one day or one hundred days, your baby will receive the best possible care from our experienced and dedicated team.
Our team has received advanced training to meet the special health care needs of neonates. The team includes you as parents, doctors, neonatal nurses, midwives, physiotherapists, radiographers, social workers, pharmacists, and many others.
Throughout your baby’s admission we encourage you to be involved in the care of your baby. The Neonatologists (Specialist Paediatrician trained in neonatal intensive care medicine), Registrars, (junior doctors) and Nurses will inform you daily about the ongoing medical care of your baby.
Please write down your questions and worries; this may help to remind you what to ask or what things to share when you meet with us each day.
There are many uncertainties in the
clinical care of ill babies and often changes occur quickly as health care challenges arise. Many babies are admitted to the NICU/SCN unexpectedly. Through providing a nurturing environment, our specialised team will strive to give your baby the best possible start to life and encourage parent/infant bonding.
Research is a vital part of our work. It is only through study and commitment that health care providers can improve the care offered. During your time with us, you may be approached by our nursing, medical and research staff to assist us in our studies. By participating in any of the research studies, you are helping us to achieve our goal.
We understand having a baby in the NICU/SCN is a very worrying and stressful time for parents and their families. Our team aims to support and guide you during your experience as we journey together throughout the recovery and development of your baby. Please do not hesitate to contact any of the team members if you have any questions or comments.
Dr Zsuzsoka Kecskes
Clinical Director, Department of Neonatology Associate Professor of Neonatology Australian National University

Parent Handbook 3
Family Centred CareThe NICU/SCN community (families and staff) believe patient and family centred care is fundamental to the mission of the unit. Family Centred Care incorporates open, effective communication and collaboration.
We will strive to nurture caregivers, while supporting and empowering them to ensure babies’ best outcomes. All members of our community are asked to demonstrate kindness, compassion and respect for each other and all cultures.
Mission StatementThe NICU/SCN provides for babies, families, and staff an environment that is:
• Developmentally appropriate
• Family centred
• Functional, safe and comfortable
• Technologically up to date and able to meet future needs.
4 Neonatal Intensive Care Unit & Special Care Nursery
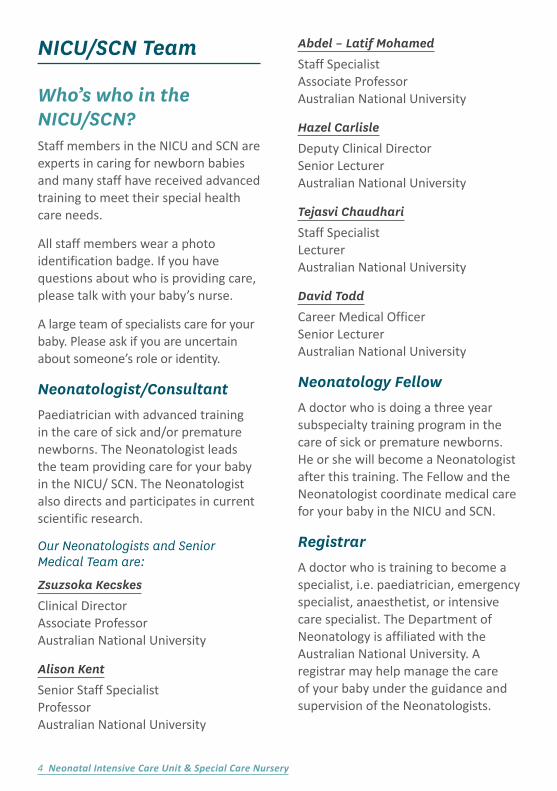
NICU/SCN Team
Who’s who in the NICU/SCN?Staff members in the NICU and SCN are experts in caring for newborn babies and many staff have received advanced training to meet their special health care needs.
All staff members wear a photo identification badge. If you have questions about who is providing care, please talk with your baby’s nurse.
A large team of specialists care for your baby. Please ask if you are uncertain about someone’s role or identity.
Neonatologist/ConsultantPaediatrician with advanced training in the care of sick and/or premature newborns. The Neonatologist leads the team providing care for your baby in the NICU/ SCN. The Neonatologist also directs and participates in current scientific research.
Our Neonatologists and Senior Medical Team are:
Zsuzsoka Kecskes
Clinical Director Associate Professor Australian National University
Alison Kent
Senior Staff Specialist Professor Australian National University
Abdel – Latif Mohamed
Staff Specialist Associate Professor Australian National University
Hazel Carlisle
Deputy Clinical Director Senior Lecturer Australian National University
Tejasvi Chaudhari
Staff Specialist Lecturer Australian National University
David Todd
Career Medical Officer Senior Lecturer Australian National University
Neonatology Fellow A doctor who is doing a three year subspecialty training program in the care of sick or premature newborns. He or she will become a Neonatologist after this training. The Fellow and the Neonatologist coordinate medical care for your baby in the NICU and SCN.
Registrar A doctor who is training to become a specialist, i.e. paediatrician, emergency specialist, anaesthetist, or intensive care specialist. The Department of Neonatology is affiliated with the Australian National University. A registrar may help manage the care of your baby under the guidance and supervision of the Neonatologists.

Parent Handbook 5
Clinical Nurse ConsultantSenior Registered Nurse with advanced training in the care of sick and/ or premature newborns who oversee and direct the overall nursing care and operations of the NICU and SCN.
Our Clinical Nurse Consultants (CNC) are:
Alison Moore
Clinical Nurse Consultant Neonatal Intensive Care Unit/Retrieval
Vicki Gore
Clinical Nurse Consultant Special Care Nursery/NAPSS/NICU Growth & Development Clinic
Health Service Assistant Responsible for co-ordinating the house keeping in both SCN and NICU.
Hospital Assistants/CleanersResponsible for maintaining the cleanliness of the ward and some equipment.
Neonatal NurseOur team includes registered nurses, midwives, and enrolled nurses who have received special education and training in the care of sick and/or premature newborns.
Nurse ManagerManages the nursing team and is responsible for all human, financial and material resources within the clinical area, in conjunction with the management team.
Clinical Audit Officer— Data CollectionInformation gathered is designed to provide us as complete a picture as possible of the pregnancy, and the treatment and progress of your baby in the NICU/ SCN.
Only authorised people have access to this information. Under no circumstances will you or your baby be identifiable in any reports or presentations we deliver on the data.
In an effort to improve patient care nationally, de-identified NICUS data is contributed to the Australian and New Zealand Neonatal Network (ANZNN) data collection.
If you do not want your baby’s de-identified data to be used for audit purposes, please inform the attending Neonatologist.

6 Neonatal Intensive Care Unit & Special Care Nursery
Ophthalmologist Neonatal eye examinations are performed by an Ophthalmologist to monitor the presence and progression of retinopathy of prematurity (ROP), (see page 44).
PhysiotherapistHealth care professional who will assess and provide treatment to your baby if required. The Physiotherapist may assist with activities to increase strength, balance, co-ordination and function.
PharmacistResponsible for reviewing and ordering medications used to treat babies in the NICU/ SCN. The pharmacist also participates in daily rounds with the team and provides drug information to doctors, nurses and parents.
RadiographerTrained in taking x-rays and /or ultrasounds to aid with diagnosis and treatment.
ResearcherThe NICU/SCN has a strong commitment to neonatal research. The units participate in international and national research projects. Should your baby meet study criteria, you may be approached by our Research Team to take part in one of our many projects. At this time the study will then be explained in detail. All participation is voluntary and parental consent is required before recruitment will be considered.
Social WorkerHealth care professional who works closely with the NICU/SCN team to support parents during their stay, helping with emotional stress, post-partum depression, financial hardship or other issues affecting their well-being.
Speech Pathologist Health care professional who will assist your baby with feeding issues and speech development if required.
Technical OfficerMaintains equipment and trains staff in its use.
Ward ClerkCoordinates daily operations in the NICU/SCN, including processing medical orders, answering the phone and intercom, greeting and helping families with visitation procedures and facilitating communication.

Parent Handbook 7
Some babies need help breathing. There are several kinds of respiratory support. Your baby’s nurse will explain these to you.
Some babies need IV fluids. This may be provided by placing a cannula in your baby’s hand or foot. Some babies may also need to have catheters placed in the umbilical cord. This may be used for more concentrated nutrition or to draw blood for laboratory tests.
Care of your babyYour baby has been admitted to the unit because they were born earlier than expected, has become unwell or because closer observation is required.
What to ExpectYour baby will be placed in a cot, isolette, or on a warmer. Their temperature is monitored closely to ensure they are warm and comfortable.
Monitoring leads may be placed on your baby’s chest and abdomen to monitor heart and respiratory rates. A pulse oximeter sensor will be placed on your baby’s foot or hand to monitor the amount of oxygen in their body.

8 Neonatal Intensive Care Unit & Special Care Nursery
EquipmentThe complex equipment that is required to provide a high standard of care for babies can be overwhelming at first glance.
We are happy to explain the function of the equipment to help you to understand your baby’s condition. Please feel free to ask questions.
Please remember the monitors are there to assist the staff in monitoring your baby and allow for us to reduce unnecessary handling so your baby can rest and grow.
Visitor’s guidelines
Speaking Up For Your BabyYou may be concerned about all the different systems and services available.
Parents are equal members of their baby’s health care team so it is important to understand everything your baby’s team is telling you. We encourage you to speak up and ask questions when you don’t understand something.
We regard every question you ask as important. During your baby’s stay in the NICU/SCN, we also encourage you to share information you have learned or observed about your baby’s care.
Over time you will develop working relationships with your baby’s doctors, nurses and other members of the team that are based on trust and mutual respect.
Take an Active RoleAlthough your baby is requiring our specialised skills and equipment they equally need your parenting. They need to know you are there for them, to know your touch, smell & voices. To know that you are their advocate in this early time of their lives.
To be involved with their care whenever possible will be invaluable when you go home with your baby. This will allow you to feel confident in knowing your baby, their needs and being their parent.
To learn more about what you can do refer to:Baby’s early development page 26
Kangaroo Care page 28
Learning your baby’s signals page 29
Please discuss how you would like to be involved with your baby’s care, with your baby’s nurse.
Access to NICU & SCNIn the interest of the babies and effective operation of the NICU/SCN, we ask you to consider the following requirements when visiting;
• General visitors may visit between 3-8 pm.
• All visitors must be accompanied by one or both parents while in the unit unless prior permission has been given by the parents and staff notified.

Parent Handbook 9
To maintain a quiet, restful environment that optimises developmental care your baby, please limit the visitors to three people at the cot side at any one time.
In exceptional circumstances you may wish to bring in more visitors, please discuss this with your baby’s nurse.
Staff will only give information to the parents of the baby. Please make visitors aware of this and ask them to get information from you, the parents.
Depending on the baby’s and/or staff needs, visitors may be asked to limit the length of their visit. Families are encouraged to use the family lounge and other family spaces for long visits and for visiting with larger groups.
Children other than the siblings of your baby are not permitted in NICU/SCN. Adult supervision is required for all children under the age of 12.
Proximity CardParents are considered part of their baby’s health care team, not visitors.
One Proximity card will be allocated to each family so that you have 24 hour access to your baby.
Only the parents are to use the card.
The card must be returned, in the supplied envelope, when your baby is discharged. Please hand the envelope, with card inside, to the Ward Clerk, the Nurse caring for your baby or just leave it in the cot.
The card is deactivated when your baby is discharged and only reactivated when given to the next parents requiring access to the unit.
Please ask your visitors to text you on your mobile when they arrive so that you can escort them into the unit.
Hand WashingHand washing is one of the most important precautions in the prevention of infection whilst caring for your baby. Ensure that you always wash your hands before entering the unit. When first entering the baby’s room, parents and visitors are asked to perform a one-minute, fingertip-to-elbow scrub in the sink. Roll up your sleeves, remove watches, bracelets, and rings, ensure you clean your forearms up to the elbows, and dry thoroughly. Alcohol rub should be used after touching any surfaces and before touching your baby.
Infection ControlWe ask that anyone who has a cold or infectious disease not visit. If visitors or children are unwell, have a cold, a fever, diarrhoea or vomiting do not allow them to visit your baby.
If your other children, friends or relatives have Chicken Pox, German measles or any other infectious disease please discuss this with the medical staff caring for your baby before visiting the unit. It will be necessary to exclude an unwell child from visiting, for the duration of the illness. This is a very important way to protect all the babies in our care.

10 Neonatal Intensive Care Unit & Special Care Nursery
Cold SoresIf you have a cold sore please inform the medical or nursing staff caring for your baby. It may be necessary to take extra precautions to prevent cross infection.
Patient PrivacyWe ask that you and your baby’s visitors respect the privacy of other families. Please do not discuss patient information in public and do not ask our staff questions about other babies or enter other babies’ rooms.
You may have an opportunity to meet other parents during your stay in the NICU/SCN. If you connect with another parent whose baby is in the unit and that parent wishes to invite you in to see their baby, you may enter that room with the parent. You must consider yourself a “visitor” in that baby’s room. The same would apply to inviting another parent in to see your baby.
For patient privacy, please do not take pictures or record video of other babies.
Weighing your babyYour baby will be weighed twice a week whilst in the unit. Sometimes it may be necessary to weigh your baby daily or at different intervals depending on the nature of his/her condition.
Your baby’s own clothingYou are welcome to dress your baby in their own clothing and blankets or swaddling wraps. Please be aware that whilst all care will be taken with these items we cannot be held responsible in the unlikely event of loss of clothing.
Parents are also responsible for taking clothing home for washing.
PhotosPlease enjoy taking as many photos of your baby as you wish. Professional photographers are available if you wish to use their services.
Many parents often return to donate photographs of their baby’s journey through the early stages of their life and our staff love to see how your babies are developing.
We do ask that your donated photos are in digital form as they may be used in art work and media events, if you give permission.
If you would like the hard copies of your photographs returned please contact staff in NICU/ SCN and we can arrange a time for you to come and collect them.

Parent Handbook 11
Family Centred CareFamily Centered Rounds are an important part of the care patients and families receive in the NICU/ SCN. Family centered medical rounds recognize the baby and their family as the focus of care and, as appropriate, involves the family in the decision making process. These rounds provide an opportunity for your baby’s health care team to receive input from the family. The Centenary Hospital for Women and Children is a teaching hospital so discussions may include talk about possible outcomes and different courses of action. If you have questions about your baby’s care or about anything said during rounds, please speak with the staff caring for your baby after rounds.
Many caregivers are involved in each baby’s care and include the baby’s family, medical providers, nurses, and other allied health personnel.
It is important that all caregivers share information so they can work effectively as a team. This sharing takes place during medical rounds. The medical staff participate in rounds every morning to discuss each baby’s status and progress. You are encouraged to be at your baby’s bedside during medical rounds.
Brief questions should be addressed at this time. Complex questions about your baby’s condition will be addressed individually with the doctor or in a family meeting.

12 Neonatal Intensive Care Unit & Special Care Nursery
Family MeetingsPeriodic family meetings with the multidisciplinary team are an opportunity to discuss in more detail your baby’s overall condition, progress, and plan of care. If a family meeting is needed or requested, your nurse will make the arrangements. Understand that you don’t have to wait for a family meeting to ask questions about your baby’s care. Talk with your baby’s nurse or doctor at any time.
Being With Your BabyWe recognise the essential role of parents as part of the team. Parents are not considered visitors, therefore you have 24 hour access to the NICU/SCN, via your Proximity Card, a locked cupboard next to your baby’s cot exclusively for your use and a recliner chair next to your baby’s cot. We also welcome and encourage grandparents and siblings to visit.
Breastfeeding InformationThe Canberra Hospital is a baby friendly accredited hospital and we encourage breastfeeding your baby.
Feeding and Providing Breast Milk for Your BabyMany infants in the NICU/ SCN may be unable to breast feed at first. These babies must be fed through a gavage tube. After your baby gets stronger and continues to grow, he or she will be fed by mouth.
If your baby is able to take a milk feed, he or she generally can be given breast milk. If your baby cannot breastfeed you can express your milk and we can freeze it so that it can be stored and used later.
We encourage all mothers to provide breast milk for their baby. Even if your

Parent Handbook 13
baby is too sick or small to breastfeed, you should hand express your breasts as soon as possible after delivery to assure a good milk supply.
The first milk, colostrum, even the smallest drops, are collected in labelled syringes & fed to your baby.
After 24hrs of hand expressing, your bedside Nurse or Lactation Consultant will provide you with a pump kit and help you begin expressing via a breast pump. We are always available to help you with any questions you may have.
Containers and labels are available in the NICU/ SCN. Ask your baby’s nurse for a supply to take with you. Mark each container with the date and time the breast milk was expressed. Your baby’s nurse can explain this more.
If you chose not to breastfeed your baby, we will discuss artificial feeds with you.
Your baby may require artificial feeds when there is not enough breast milk available. We will discuss this with you first.

14 Neonatal Intensive Care Unit & Special Care Nursery
• Correctly label EBM with your baby’s name, date and time of collection using the baby labels that your nurse gives you.
Your EBM is collected from the NICU/ SCN refrigerators in the morning by the Nutrition Room technician. The milk is then poured into individual amounts for your baby’s feeds over the next 24 hours. The remaining EBM will be frozen for use later.
If your baby is in NICU and only taking very small amounts of EBM e.g. 1 or 2mls — please express and then divide into smaller volumes. Syringes may be used to store these smaller volumes, therefore avoiding larger amounts being defrosted and wasted.
Please number these syringes.
Parents are asked not to place or remove milk from the fridges in their baby’s room. This will be done by the nurse caring for your baby, who will double check that it is labelled correctly and given to the right baby.
For more information on breastfeeding see the Australian Breast Feeding Association www.breastfeeding.asn.au
Looking after yourselfWhilst you are breastfeeding or expressing breast milk, we encourage you to have a well balanced diet and get plenty of rest and fluid.
Expressing RoomThe Expressing Room is located in the SCN. The room provides an area where mothers of babies in the NICU/ SCN can express breast milk in privacy and comfort away from clinical and public areas.
This room is available 24 hours for the use of the mothers who are expressing breast milk for their babies. Due to privacy, males are not permitted in the expressing room.
There are also mobile electric breast pumps available to use in your baby’s room. Please ask your nurse if you would prefer to use one of these so you can express next to your baby. Just remember to bring your kit to attach to the electric pump.
Storage and Use of Expressed Breast Milk (EBM)It is essential that EBM is stored correctly.
• EBM can be stored in the body compartment of the refrigerator. Never store EBM in the refrigerator door
• EBM in NICU/SCN is stored in the Nutrition Room freezer
• EBM should never be refrozen once it has been thawed

Parent Handbook 15
Lactation Consultant (LC)Is a specialist trained to focus on the needs and concerns of the breastfeeding mother-baby pair and to prevent, recognise, and solve breastfeeding difficulties. They have educational and clinical backgrounds in the health professions. The NICU/SCN have Lactation Consultants who are also practicing midwives and nurses. If you would like to speak to a Lactation Consultant please ask your nurse and she will organize a time for the LC to come and speak to you.
Lactation SupportDuring your admission; Nursing staff and lactation consultants are available to:
• Provide you with current, accurate information about feeding infants
• Provide help and information about breast pump rental, breast milk expressing, handling and storage
• Provide one-on-one assistance when you begin breast feeding and ongoing support as needed
• Offer help if you have any concerns with expressing or breastfeeding
• Connect you with breast-feeding support and specialists in your area when you go home.

16 Neonatal Intensive Care Unit & Special Care Nursery
Australian Breastfeeding Association Guidelines for Storage of Breast Milk Storage of Breast milk for home use
Breast milk Room Temperature Refrigerator Freezer
Freshly expressed into a closed container
6–8 hrs (26ºC or lower). If refrigeration is available store milk there
3–5 days (4ºC or lower) Store in back of refrigerator where it is coldest
2 weeks in freezer compartment inside refrigerator.
3 months in freezer section of refrigerator with separate door.
6–12 months in deep freeze
(-18ºC or lower).
Previously frozen— thawed in refrigerator but not warmed
4 hours or less
(i.e. the next feeding)
Store in refrigerator
24 hours
Do not refreeze
Thawed outside refrigerator in warm water
For completion of feeding
Hold for 4 hours or until next feeding
Do not refreeze
Infant has begun feeding
Only for completion of feeding, then discard
Discard Discard
Parent Handbook 17
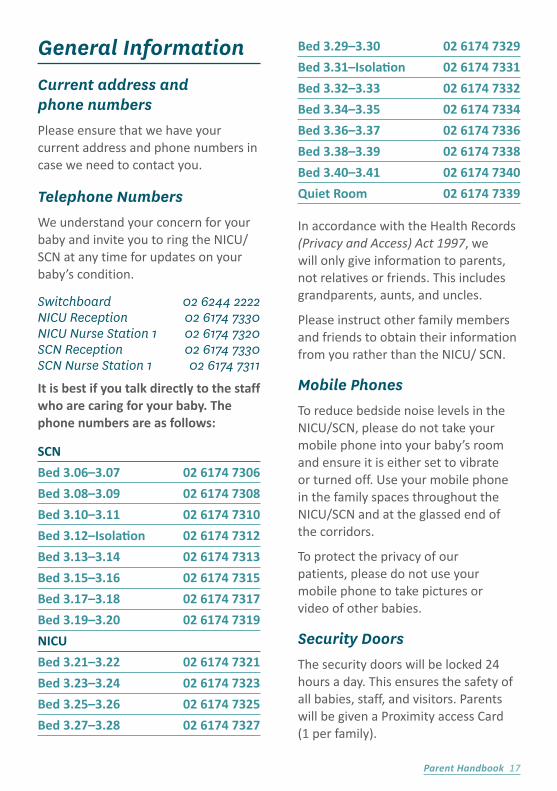
General InformationCurrent address and phone numbersPlease ensure that we have your current address and phone numbers in case we need to contact you.
Telephone NumbersWe understand your concern for your baby and invite you to ring the NICU/ SCN at any time for updates on your baby’s condition.
Switchboard 02 6244 2222 NICU Reception 02 6174 7330 NICU Nurse Station 1 02 6174 7320 SCN Reception 02 6174 7330 SCN Nurse Station 1 02 6174 7311
It is best if you talk directly to the staff who are caring for your baby. The phone numbers are as follows:
SCN
Bed 3.06–3.07 02 6174 7306
Bed 3.08–3.09 02 6174 7308
Bed 3.10–3.11 02 6174 7310
Bed 3.12–Isolation 02 6174 7312
Bed 3.13–3.14 02 6174 7313
Bed 3.15–3.16 02 6174 7315
Bed 3.17–3.18 02 6174 7317
Bed 3.19–3.20 02 6174 7319
NICU
Bed 3.21–3.22 02 6174 7321
Bed 3.23–3.24 02 6174 7323
Bed 3.25–3.26 02 6174 7325
Bed 3.27–3.28 02 6174 7327
Bed 3.29–3.30 02 6174 7329
Bed 3.31–Isolation 02 6174 7331
Bed 3.32–3.33 02 6174 7332
Bed 3.34–3.35 02 6174 7334
Bed 3.36–3.37 02 6174 7336
Bed 3.38–3.39 02 6174 7338
Bed 3.40–3.41 02 6174 7340
Quiet Room 02 6174 7339
In accordance with the Health Records (Privacy and Access) Act 1997, we will only give information to parents, not relatives or friends. This includes grandparents, aunts, and uncles.
Please instruct other family members and friends to obtain their information from you rather than the NICU/ SCN.
Mobile PhonesTo reduce bedside noise levels in the NICU/SCN, please do not take your mobile phone into your baby’s room and ensure it is either set to vibrate or turned off. Use your mobile phone in the family spaces throughout the NICU/SCN and at the glassed end of the corridors.
To protect the privacy of our patients, please do not use your mobile phone to take pictures or video of other babies.
Security DoorsThe security doors will be locked 24 hours a day. This ensures the safety of all babies, staff, and visitors. Parents will be given a Proximity access Card (1 per family).

18 Neonatal Intensive Care Unit & Special Care Nursery
During visiting hours, 3-8pm, please ask your visitors to text or ring you on your mobile when they arrive so you can let them in with your pass.
This avoids visitors ringing the doorbell, allowing the ward to remain a quiet place for the babies.
Levels of CareThe Unit provides three levels of care. The NICU is for seriously ill or premature babies requiring intensive care. It also provides high dependency beds for babies requiring extra observation and care.
The SCN provides care for stable babies prior to discharge. The focus of this unit is parent education and discharge planning.
Waiting RoomA waiting room is located in the Special Care Nursery adjacent to the reception. This area is available 24 hours for the use of parents/families and visitors to wait in comfort.
Family RoomsTwo family rooms are located in the SCN and are available for the use of all parents and carers with babies in NICU/ SCN. These rooms are available 24 hours a day and contain lounges, a television and a beverage bar for the use of the parents/carers.
One room is child friendly and the other room is predominately for the use of adults.
Quiet Room A room located in the NICU available to provide a quiet and private space for parents/cares and the families of babies receriving palliative care. This room is fully equipped with an ensuite and is available 24 hours.
Rooming-in RoomsTwo rooming–in rooms in the SCN are available for use by parents and carers of babies. These rooms are managed by the staff in NICU and SCN and are available to parents just before their baby’s discharge. These rooms are fully serviced and are available 24 hours, seven days a week. Parents are responsible for the house keeping of these rooms and the kitchen area.
Public ToiletThe public toilet and shower is opposite the family rooms in the SCN. It also has a baby changing facility.
Public TelephoneLocated in the main building of the hospital.
SmokingACT Health supports a policy of Non-Smoking. Smoking is NOT permitted outside of the designated smoking area by patients or visitors in any area of the Hospital or on the Hospital ground.

Parent Handbook 19
Spiritual SupportTrained multi-faith chaplains offer spiritual support, a compassionate listening presence, prayer, and other resources. Baby blessings and baptisms can be performed by the chaplains. They can also access priests and clergy from various faiths if needed.
Chaplain’s officeThe chaplains’ office is across the hall from the chapel and Chaplains are available on call via the switchboard 24 hours a day, 7 days a week. The chapel is a multi-faith space that offers quiet and peace to all who enter. The chapel is open 24 hours a day. Regular worship services are offered several times during the week and sessions are advertised in the chapel.

20 Neonatal Intensive Care Unit & Special Care Nursery
NICUCAM is an International award wining video streaming service, providing parents with access to real time images of their baby via the internet. The service operates from the Special Care Nursery. To access this service, you will need a computer or a device that can connect to the internet.
The SCN does not charge families to access the NICUCAM service; however, please take into consideration the costs of data usage that may be incurred from your chosen Internet Service Provider as a result of accessing this service. If you are interested in the use of the NICUCAM please discuss availability with the nursing staff or the NICUCAM project officer.
To find out more about NICUCAM or to view your baby go to: www.nicucam.com.au
NICUCAM

Parent Handbook 21
To find out more:
P: 1300 773 664
www.miraclebabies.org.au
24 hr Family Support Line
1300 MBABIES (1300 622 243)
Miracle Babies Foundation (MBF) is a non-profit organisation that supports premature & sick newborns, their family & the hospitals that care for them. MBF develops vital programs & resources to support & enhance a family’s experience from a threatened pregnancy, hospital journey with a premature or sick newborn, transition to home & beyond.
Nurture Program: a parent to parent support programIf you have experienced the birth of a premature or sick newborn, you may know first hand how overwhelming and traumatic an experience it can be. Watching your baby struggle for life brings inconceivable highs and lows and can be an extremely difficult time for parents, siblings and the extended family.
This successful program is essential for all families and offers:
NurtureTime: In hospital parent to parent support & information sessions. Facilitated by qualified Miracle Babies Foundation Volunteers, these in hospital parent support sessions operate within Australian NICUs. This vital, comforting, emotional support provides parents with the opportunity to share their journey with someone who has been there. Meet other parents who have also experienced a premature or sick newborn. Please ask your nurse for details.
NurtureLine: 1300 622 243 National 24 hour family helpline Support is provided by trained parent support volunteers who themselves have experienced the birth of a premature or sick newborn. Where appropriate, Miracle Babies Foundation endeavour to offer support from a parent support volunteer with a similar experience such as gestational age, medical condition or other shared circumstances. This service is offered to all parents, extended family and friends including those families who have suffered a loss.
NurtureGroup: Out of hospital play & support groups. MBF offer a safe and secure environment for children 0 to 6 years who have been challenged by prematurity or sickness in which they can learn and develop through play, whilst offering families ongoing parent support after leaving the safety of a NICU/SCN. Call 1300 773 664 or 02 9724 8999 to register for the first time.
Like Miracle Babies Foundation Facebook page for social networking with other parents with sick & premature babies.
www.miraclebabies.org.au – offering access to current, relevant & Australian information.

22 Neonatal Intensive Care Unit & Special Care Nursery
RONALD MCDONALD HOUSE provides a ‘home away from home’ for families of babies requiring care in the NICU or SCN, who live greater than 50km from the hospital. Accommodation cost is kept as low as possible and Ronald McDonald House Canberra makes every effort to accommodate families regardless of their financial situations.
Families who live over 100kms from The Canberra Hospital are eligible to have room payments covered by Patient Travel and Accommodation Assistance Scheme (IPTAAS). Families with the greatest need for accommodation are given priority.
The House is located within the Women & Children’s Hospital, on Level 2. Ronald McDonald House provides quality accommodation & a family friendly area to relax in, with ready access to the NICU & SCN.
RONALD MCDONALD FAMILY ROOM provides a relaxing haven within hospitals giving families a break from the stress of many hours spent by their baby’s cotside.
RONALD MCDONALD FAMILY RETREAT–BATEMANS BAY provides families with seriously ill babies a week’s free accommodation, enabling them to reconnect and enjoy a holiday when they most need it and can least afford it.
For more information:
Phone: (02) 6281 5894
Fax: (02) 6281 7093
www.rmhc.org.au/canberra-act
Parent Handbook 23
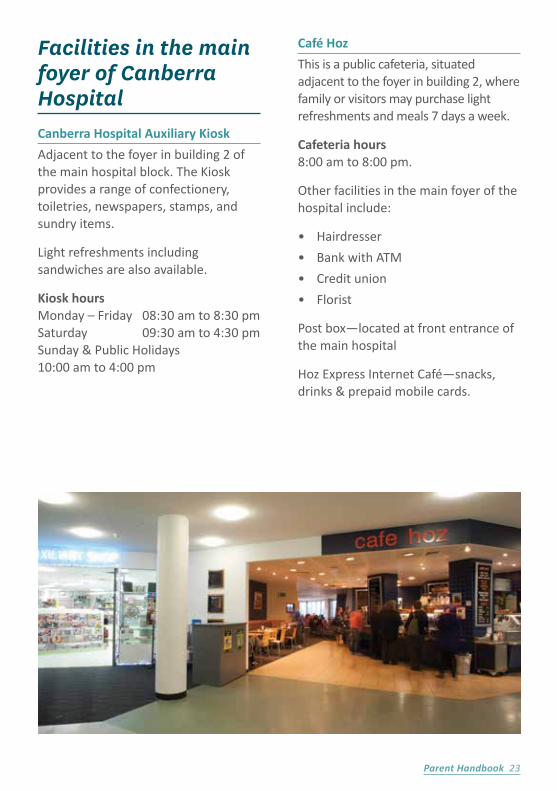
Facilities in the main foyer of Canberra HospitalCanberra Hospital Auxiliary Kiosk
Adjacent to the foyer in building 2 of the main hospital block. The Kiosk provides a range of confectionery, toiletries, newspapers, stamps, and sundry items.
Light refreshments including sandwiches are also available.
Kiosk hours Monday – Friday 08:30 am to 8:30 pm Saturday 09:30 am to 4:30 pm Sunday & Public Holidays 10:00 am to 4:00 pm
Café Hoz
This is a public cafeteria, situated adjacent to the foyer in building 2, where family or visitors may purchase light refreshments and meals 7 days a week.
Cafeteria hours 8:00 am to 8:00 pm.
Other facilities in the main foyer of the hospital include:
• Hairdresser
• Bank with ATM
• Credit union
• Florist
Post box—located at front entrance of the main hospital
Hoz Express Internet Café—snacks, drinks & prepaid mobile cards.

24 Neonatal Intensive Care Unit & Special Care Nursery
Transfer of BabiesThe NICU is a specific advanced life support facility and we treat any baby who requires acute care within the neonatal period.
We are part of a state wide New South Wales and ACT Perinatal Network, which includes all other intensive care units in NSW and smaller hospitals that may be closer to your home. The cooperation of these hospitals helps to provide beds for ongoing treatment.
As your baby’s condition improves and the need for intensive care diminishes, we will consider the transfer of your baby to one of our affiliated special care units closer to your home.
For those families within the ACT, we will consider transfer to Calvary Bruce Hospital or Calvary John James Hospital and will discuss this possibility with you. We hope you will understand that in order to provide intensive care services for other babies in need, such transfers are sometimes required.

Parent Handbook 25
Newborn Hearing ScreeningThe goal of the ACT Newborn Hearing Screening program is to identify babies with possible hearing impairments and link them with services if required by six months of age. Every baby in the ACT will have a hearing screen. Premature babies will be screened close to their due date. We aim to have all babies screened before discharge.
Retrieval ServiceThe Department of Neonatology provides a Neonatal Emergency Transport Service (NETS) in conjunction with NSW NETS, which is supported by ACT Health. The service ensures safe and expedient neonatal retrievals within the ACT for compromised neonates born outside The Canberra Hospital.
This service also provides back transfer of babies to their hospital of origin when their condition permits. The retrieval service is staffed 24 hours a day by experienced Medical and Neonatal Nursing staff.

26 Neonatal Intensive Care Unit & Special Care Nursery
Newborn and Parent Support Services (NAPSS)NAPSS provides a discharge program for NICU/SCN. It is run by experienced midwives and neonatal nurses, who provide a support service for families of babies who still require some nursing care, support and advice at home.
They coordinate care with nurse managers, neonatalogists, paediatricians, physiotherapist, social workers and other health professionals.
NAPSS provides a six day per week (Monday to Saturday) service. Staff assist parents with the management of their baby who may be preterm, of small birth weight, requiring home oxygen, some tube feeds or palliative care.
Before an infant leaves the NICU or SCN, NAPSS arrange an in-patient visit to assess the baby’s needs and assist the parent with preparation for their baby’s discharge home.
Follow-up visits are tailored to the baby’s and parent’s needs. The nurses assess the baby’s growth, assist with any feeding or medical issues and offer general parenting advice.
NAPSS is offered to residents of the ACT and Queanbeyan after discharge from The Centenary Hospital for Women and Children, Calvary Bruce or Calvary John James Hospitals.
Parent Handbook 27
This service is offered to families residing in the ACT or Queanbeyan and certain criteria must be fulfilled. It involves educating parents to perform tube feeds at home once their baby takes about half of its feeds as suck feeds in the SCN.
Parents will be taught how to tube feed their baby at home and the transition to full suck feeds (either by bottle or breast) can occur with the support of the NAPSS team at home.
Be assured that babies will only be discharged if they are otherwise well. If you are interested in this program, please ask the nursing staff for more information.
Tube Feeding at Home PlanThe aim of this feeding plan is to allow parents to administer tube feeds at home with provision of in-home support from the Neonatal and Parent Support Service (NAPSS).
It enhances the approach to neonatal health care by promoting earlier discharge, facilitating positive patient and family centered outcomes without jeopardising patient care.

28 Neonatal Intensive Care Unit & Special Care Nursery
NICU Growth and Development ClinicNICU Growth and Development Clinic Centenary Hospital for Women and Children Building 11, Level 1 Paediatric Outpatients Department Tel: 6174 7573
The NICU Growth and Development Clinic periodically monitors the progress of babies who required intensive care at birth. Formal developmental assessments are undertaken during the first formative years of life by a multidisciplinary team.
As part of our patients’ overall care, we want to ensure all NICU/SCN graduates who may be at risk of developmental and behavioural problems are identified early and referred to the appropriate services to help them to reach their full potential.
Families from the NICU/SCN are invited to participate in the follow-up program. Information regarding the program is provided prior to the baby’s discharge/transfer.
After each clinic visit families are given feedback and a formal report is sent to the child’s parents, Paediatrician, GP, and any other health professionals involved in the child’s care.
Your Baby’s Early Development in the NICU/SCNBabies in the NICU/SCN are born at different gestational ages. As the weeks go by, we add those weeks to your baby’s age. This is called ‘correcting’ your baby’s age. Depending on the severity of your baby’s illness and his or her gestational age, your baby will have different ways of responding to the world.
Remember, your presence at the bedside is important to your baby’s development at any age. At first, your baby will focus on the basics: breathing and sleeping. You can help him or her to stay calm and comfortable by keeping activity at the bedside appropriate to your baby’s needs.
Here are some characteristics of babies at different ages and stages of development, to help you to understand your baby’s behavior:
Less than 26 weeksEarly sensory responsiveness
Light – The eyes are often closed, but eyelids are thin, so your baby is sensitive to changes in lighting.
Sound – Your baby may startle at loud voices or sounds.
Touch – The skin is very fragile. For a soothing touch, gently place your hand on your baby rather than stroking the skin.
Movement – Your baby may startle or have jerky movements. Keep baby’s arms and legs tucked close to the body and provide soothing boundaries.

Parent Handbook 29
26 to 28 weeks• Your baby is still sensitive to light,
sound, touch and movement. He or she may recognize your voice, touch, and smell.
• Continue to keep your baby’s bedside quiet and avoid bright lighting when possible. Avoid wearing strong perfumes.
• Sucking is often soothing for your baby. Offer a dummy when he or she seems stressed.
• Hold your baby’s hand or foot gently, or cradle his or her head and feet with your hand. Provide Kangaroo Care if your baby’s health care team advises it is okay.
• Change your baby’s position slowly to prevent startles.
29 to 31 weeks• Continue to provide a restful
environment for sleep. Deep sleep increases at this age, and your baby grows while sleeping.
• Your baby may become restless with loud voices or sounds. He or she may become still in response to your soft voice and may look at you.
• Movements increase at this age. Your baby may do more stretching, may bring hands to face for self-soothing and may tuck arms and legs close to his or her body. Your baby will probably need to be positioned with nesting to contain some of these movements.
• Continue to change your baby’s position slowly and avoid rocking when you are doing Kangaroo Care.
32 to 36 weeks• Your baby will be more alert,
visually. Continue to use your face and voice rather than introducing toys. It is easy for your baby to become over stimulated at this age so soft talking, singing and reading to him or her are best. Your baby also may enjoy soft music when it’s time to go to sleep.
• Help your baby to bring his or her own hands to face and body for self-soothing. This tucked position goes with sucking and may help to prepare baby for feeding.
• Continue to avoid abrupt movements that may startle your baby.
• Your baby may enjoy different kinds of touch at this age. Continue Kangaroo Care and gentle holding of hands and feet. If your baby seems to enjoy this, introduce gentle massage.
37 to 40 weeks• Your baby will show more interest
in his or her surroundings. Your face and voice are still the best toys, but you also might want to provide a mobile, crib mirror, and toys with soft music, for times when your baby is lying on his or her back, or sitting in an infant seat.
• Babies often prefer to have their head turned to one side at this age. Encourage your baby to look to both sides to see your face and use head supports to keep his or her head at midline when in a baby seat or car seat.
• Slow rocking while you are holding him or her may be enjoyable for your baby at this age.

30 Neonatal Intensive Care Unit & Special Care Nursery
Kangaroo CareKangaroo care is a way of holding your newborn baby that has been shown to have short- and long-term benefits for you and your baby. Being close to the mother’s body helps regulate how awake and attentive the baby is and reduces stress. In addition, babies who receive kangaroo care seem calmer and easier to care for, which sets a path for learning throughout their lives.
Benefits of kangaroo care for breastfeeding:
• Increases your milk hormones
• Increases the success rate of nursing among mothers of premature infants
• Increases milk supply on the next day of expressing
• Increases success with long-term breastfeeding.
Benefits for your baby:• Reduces crying and fussiness
• Helps stabilize your baby’s heart and breathing rates
• Provides a healthy temperature
• Decreases the need for oxygen
• Improves weight gain
• Provides more restful sleep and better awake times
• Boosts mental development and motor skills as he/she grows.
Kangaroo care is safe for most babies. Even a tiny premature baby on a ventilator can receive kangaroo care. If you wonder whether your baby is ready for kangaroo care, ask your baby’s doctor or nurse.
Only your baby’s medical team – you, the doctor and the nurse – can decide whether your baby should receive kangaroo care and when it should begin.
How to provide Kangaroo CareKangaroo care sessions can be planned for day or night.
You can provide kangaroo care by placing the baby upright between your breasts. Place preterm babies “heart-to-heart” and term babies “tummy to tummy.”
The baby should be wearing a nappy and your chest must be bare to provide ‘skin to skin’ contact. So, feel free to remove your bra to facilitate this. Use a blanket to cover the baby and a hat. It is important that your baby stay warm.
Your baby’s nurse can provide you with a gown to protect your modesty.

Parent Handbook 31
Table 1.
Baby coping Baby not coping
alert yawning, crying hiccups, sneezing
steady gaze turning away, back arching
sucking grimacing, frowning
hand to mouth movements finger splaying
stable heart and breathing rate
change in heart or breathing rate
tolerating feeds vomiting
smooth body movements jitteriness
stable colour change in skin colour
Learning Your Baby’s SignalsBabies communicate through behaviours called signals or cues. As your baby matures, these signals will become more robust and easier to interpret. Preterm and sick babies signal to their caregivers with more subtle cues.
Parents can help their babies by learning when their baby is ready to interact and is coping with the level of stimulation, and when their baby is asking for less stimulation. Babies respond in different ways to touch and handling. Sometimes, premature babies become stressed when handled and give signals to let us know how they are coping (see Table 1).
Most babies display a range of these signs at one time or another without necessarily being stressed; however, a baby who consistently displays ‘not coping’ signs while being handled may need the activity modified and frequent breaks introduced.

32 Neonatal Intensive Care Unit & Special Care Nursery
Engagement Cues I’m happy with the level of stimulation.
Figure 1 – Relaxed face and body, eyes open and turned towards caregiver’s face.
Self Soothing Behaviours Babies will help themselves to maintain a calm state with the following behaviours.
Figure 2 – Non-nutritive sucking, hand clasping, foot clasping & bracing.
Figure 3 – Finger holding, holding on to ears or wraps, or hands to face.
Disengagement CuesFor beginner brains there is so much to learn and assimilate. Babies receive information from touch, hearing, seeing, tasting, smelling and moving.
When this becomes overwhelming for babies, they will ask to have the stimulation reduced by displaying a cluster of these behaviours.
Figure 4 – Gaze aversion.

Parent Handbook 33
Figure 5 – Yawning.
Figure 6 – Turning away and clenching hands.
Figure 7
Figure 8
Figure 7-8 – In the first photo the baby is gaze averting, frowning, and her hands are in high guard position to the side. Her mother has helped her by quiet, calm, and supportive holding. The second photo shows a more relaxed face and she is able to meet her mother’s gaze.

34 Neonatal Intensive Care Unit & Special Care Nursery
The process of bonding with your baby is strengthened by the exchange of nonverbal cues. Even in the first days of life, your baby picks up on your cues—your tone of voice, the feel of your touch—and sends you back the subtle signals according to their maturity and health.
Eventually these will become robust crying, cooing, mimicking facial expressions, smiling, laughing, pointing, and even yelling.
You will grow more confident in interpreting your baby’s cues and in tending to their needs for food, warmth and affection. Secure attachment grows out of this nonverbal communication process between you and your baby.
Time For Sleep SignalsUndisturbed sleep is important for growth and development. Recognising when baby needs sleep is an essential part of parenting. Without proper rest, a baby cannot be calm and alert and ready to engage with you. This baby’s posture suggests his muscle tone is very relaxed – another sign he is not ready for more stimulation.
Figure 9 – Sleeping
Parent Handbook 35
Going Home —The Discharge ProcessGoing home with your baby is an exciting time. We want to make sure that both you and your baby are prepared for this happy event.
In general terms, your baby should be ready for discharge by their due date, can maintain a normal temperature in an open cot, has appropriate weight gain, takes all or most feedings by breast or bottle, and is off all IV medications.
Some babies will go home needing extra care and so will require additional support.
We have developed a guide to help us work with you to make sure your baby’s transition home is smooth.
Your baby’s care team wants to make sure you feel as prepared as possible to go home with your baby when the time comes.
Below is a list of activities you should be confident doing before you go home with your baby:
• Taking your baby’s temperature
• Changing your baby’s nappy
• Bathing your baby
• Dressing your baby
• Feeding your baby by breast or bottle
• Preparing breast milk or formula for your baby
• Giving your baby medications
• Placing your baby safely in a car seat
• Putting your baby ‘back to sleep and on ‘tummy to play’
• Ensured that your capsule/carseat is fitted in your car by an approved fitter
• Completed a Cardiopulmonary Resuscitation (CPR) class.

36 Neonatal Intensive Care Unit & Special Care Nursery
Map of Canberra Hospital
Yamba Drive, Garran, ACT, 2606 | Ph: 02 6244 2222
Proceed to Main Foyer (2) of Canberra Hospital. Further directions are available from Main Reception staff
Special Care Nursery
Level 3
Building 11
Centenary Hospital for Women and Children
NICU
Level 3
Building 11
Centenary Hospital for
Women and Children
NICU/SCN
Centenary Hospital for Women and Children
Canberra Region Cancer Centre

Parent Handbook 37
Map of NICU/SCN
N
LIFTS
EXPRESSING ROOM
FAMILY ROOMS
QUIET ROOM BEDS 21-30
BEDS 6-11
BEDS 13-20
BEDS 32-40
WAITING ROOM
ROOMING IN
RECEPTION
Neonatal Intensive Care Nursery
Special Care Nursery
Birthing Centre
TOILET
INTERCOMON PILLAR
Building 11, Level 3, The Centenary Hospital for Women and Children

38 Neonatal Intensive Care Unit & Special Care Nursery
123456789
101112
131415161718192021
18
1514
13
11
17
21
1
20
Belco
nnen
Way
Mary Potter Circuit
Mary Potter Circuit
Haydo
n Driv
eGinn
inder
a Driv
e
7
198
6
9
5
3
10
4
223
All day parking
Disabled parking
2 hour parking
Sylvi
a Cur
ley Ro
ad
12
22
2
P2
P2 P2
P2
Main Entrance and ReceptionDay Service EntranceMaternity EntranceXavier Building Marian BuildingCalvary Clinic: Specialist Medical CentreHyson Green: Private Mental HealthResidence C: Specialists’ RoomsRotary Cottage: Relatives’ AccommodationUC O’Shannassy Centre:Executive AdministrationEngineering ServicesResidences A: Administration
Mark Maher Building: ResidenceNational Office of the Little Company of MaryLewisham Building: Function/seminar RoomsBruce Ridge Early Childhood CentreClinical Decision UnitANU Medical SchoolNorthside Dialysis ClinicKeaney Building Delivery DockICU/CCUEmergency
Map of Calvary – Bruce HospitalCorner of Belconnen Way & Hayden Drive, Bruce, ACT, 2617 | Ph: 02 6201 6111
SPECIAL CARE NURSERY
Special Care Nursery – Level 3, Marion Building Enter ( Maternity Entrance) near Emergency Department
Turn right at Day Services 2 and walk past cafe to Building Go up the stairs or lift to Level 3
Special Care Nursery is opposite the ward clerk/receptionist desk, at the top of the stairs
23
5

Parent Handbook 39
Map of Calvary – John James Memorial Hospital
Special Care Nursery – Level 1, Maternity Centre
Through Maternity Centre entrance
175 Strickland Crescent, Deakin, ACT, 2600 | Ph: 02 6281 8100

40 Neonatal Intensive Care Unit & Special Care Nursery
Medical Terms and EquipmentThe NICU/SCN can be a strange and difficult place because of all the machinery, alarms, and medical terminology used.
Here is a short list of words and definitions that may help you understand the most frequently used jargon in the centre.
Apnoea (Greek: ‘Without Breath’)
This is a period in which the baby does not breathe. Most babies have breathing patterns in which there are short pauses, where it seems they are not breathing at all.
Usually these are harmless and normal. Longer pauses which result in a decrease in heart rate and possibly colour change are detected by the monitor.
An alarm sounds if the baby does not start to breathe again on his/her own. Apnoeas are more common when the baby is very immature and become less common as the baby develops.
AnaemiaA condition of a low level of red blood cells. A blood transfusion may be necessary for treatment.
Blood GasA sample of blood is drawn from an artery, vein, or heel prick and analyzed by a machine. It determines the exact levels of oxygen and carbon dioxide in the blood, showing how well the lungs are working.
Blood Glucose Analysis This test is performed on a small amount of blood in order to measure blood sugar levels.
Blood TransfusionPremature babies often do not produce a sufficient amount of red blood cells, as compared with full term babies. In addition, blood taken for various tests may need to be replaced. Routine testing is done on all donor blood for Hepatitis, HIV, and other viral infections.
Bradycardia(Latin: Slow Heart Rate)
Bradycardic episodes are short periods when the baby’s heart rate slows. A bradycardia usually happens together with an apnoea. The heart usually speeds up again on its own, as the baby takes a breath. Occasionally the baby may need stimulation. As a baby matures and grows, the number of bradycardias decreases and the monitor can be removed.

Parent Handbook 41
BrainZ monitorThis is a simplified brain wave monitor (EEG) used for babies with confirmed or suspected seizures. Four electrodes are placed on the baby’s scalp and one on the shoulder. The monitor does not alarm, but seizures or other abnormalities can be diagnosed straight away at the bedside.
Cardiac MonitorThe cardiac monitor counts the baby’s heartbeat and displays the rate per minute on the screen. Some monitors give a visual display of the heart rate in a wave form. The alarm will sound if the heart rate deviates from the limits set for each baby.
Central/Long LineSome babies require long term intravenous therapy or nutrition. In such cases it may be necessary to use an intravenous catheter, which is longer than a regular cannula, enabling it to lie in a larger vein. The position of the line is checked via an X-Ray. Central lines are inserted under sterile conditions and may remain in-situ for many days.
Continuous Positive Airway Pressure (CPAP) CPAP is sometimes used as a treatment for babies with breathing difficulties. It helps to maintain adequate expansion of the lungs, by providing continuous airway pressure via short prongs in the baby’s nose. This aids in the prevention of lung collapse and apnoeas.
Crib/Isolette/Open Care Centre Newborn babies require a warm environment in order to grow. Small babies are unable to generate enough heat on their own to maintain normal temperature, so they are nursed in an isolette, where the temperature is kept between 26° C and 35° C.
Another effective way of keeping very small or sick infants warm is by using a warmed open care centre. The baby is nursed dressed only in a nappy to facilitate easy access for procedures, and observation.
A sensor is placed on the baby’s skin, which monitors the infant’s skin temperature. This allows your baby’s nurse to make adjustments to keep them warm.
Echocardiogram An Echocardiogram is an ultrasound of the heart. This is a non invasive diagnostic procedure which is done in the unit. It is used to evaluate the structure and function of the heart.
Heel Prick We have to do blood tests on babies in the NICU and SCN. Using special laboratory techniques makes it possible to do a wide range of tests on very small amounts of blood. A small needle prick in your baby’s heel is often the most effective way to obtain a blood specimen.

42 Neonatal Intensive Care Unit & Special Care Nursery
Intravenous Line/CannulaSmall or sick babies are often unable to tolerate milk/fluid in their stomach. Nutrition and fluids may be given into the vein via a cannula for a few days if needed. Drugs, such as antibiotics, are also given through the drip thus avoiding the need for the baby to have many injections.
Jaundice (Hyperbilirubinaemia) A yellow discoloration of the skin is a common condition of the newborn. This may require phototherapy treatment. Approximately 10–15% of all babies are visibly jaundiced at about three days after birth. This is the most likely time of occurrence.
Hyperbilirubinaemia, the medical term for jaundice, is caused by an abnormally high level of bilirubin which is a by-product of the normal breakdown of red blood cells.
Occasionally the immature liver cannot successfully process the excess bilirubin for it to be excreted from the body. The bilirubin may then reach a level which requires treatment with phototherapy.
Magnetic Resonance Imaging (MRI) MRI uses magnetism, radio waves, and a computer to produce three dimensional images of specific anatomical structures. It is a diagnostic technique used to visualise the structure of soft tissue.
Prior to having an MRI babies routinely have oral sedation. There may be several monitors attached to your baby. These will alert the staff to any changes in your baby’s condition.
Neonate Term applied to a baby in the first 28 days of life.
Neonatal Pain Relief Oral Sucrose may be given after informed consent is obtained to reduce pain or discomfort during painful procedures.
Newborn Screening Test This is a routine test done on all babies on day 3–4 to detect rare medical disorders. A few drops of blood are taken from the heel. Amongst many others, the following conditions are screened for:
• Phenylketonuria (PKU)
• Hypothyroidism
• Cystic Fibrosis
• Galactosaemia
• A large number of other rare metabolic diseases.
The test will be done in Sydney and you will not be informed unless the result is abnormal, in which case a Neonatologist will discuss the results with you.
Oxygen Oxygen is a colourless, odourless gas essential for life. Room air contains 21% oxygen but the baby’s supply can be increased to 100% if necessary.

Parent Handbook 43
Patent Ductus Arteriosus (PDA) The ductus arteriosus is a blood vessel which is present before birth but closes soon after birth (when it is no longer needed). Sometimes it remains open in very small babies. It is detected by an echocardiogram and may require treatment with medication or surgery.
Phototherapy Phototherapy is used for the treatment of jaundice when the level of serum bilirubin is high. The need for phototherapy is decided on an individual basis.
Treatment consists of placing the baby, with eyes protected, under the phototherapy lights or wrapped in a bili blanket until the serum bilirubin level falls.
Pulse Oximetry (Oxygen Saturation Monitoring)Pulse oximetry is used to monitor the levels of oxygen in the arterial blood. Light sensor probes are secured opposite each other and placed on the baby’s extremities. The sensors emit beams of red and infra-red light through the tissues. Measurements are then replayed to a computer which displays results on a digital screen. The alarm will sound if the oxygen saturation is different to the set levels. Movement will also cause the alarm to sound.
Reflux (Gastro Oesophageal Reflux) A condition in which there is some regurgitation of the feed. This is not unlike heartburn. Many premature babies suffer from this. Treatment may be conservative or medication may be used.
Respiratory MonitorThis is usually combined with a cardiac monitor. It counts the number of breaths the baby takes per minute. The alarm will sound if it does not detect a breath for a short period. Sometimes the alarm will sound if the baby is restless or the baby’s breathing is shallow.
Respiratory Distress Syndrome (RDS) or Hyaline Membrane Disease (HMD).
RDS or HMD is a disease of premature babies due to immaturity of their lungs. Many women giving birth prematurely will have had a steroid injection to reduce the severity of this disease. Babies may be treated with surfactant (a medication given directly into the baby’s lungs) for this condition.

44 Neonatal Intensive Care Unit & Special Care Nursery
Retinopathy of Prematurity (ROP) ROP is an eye condition seen in some premature babies. ROP is a condition in which the blood vessels in the retina have not developed as they should after birth. In babies that do develop ROP it is usually mild without causing any problems with vision.
ROP is monitored regularly to ensure that treatment occurs when the ROP has advanced. The treatment is generally done with laser surgery by an ophthalmologist in order to minimise the risk of visual impairment.
Tube Feeds/Nasogastric Feeds/Gavage Feeds Some babies, both premature and term may be unable to take their feeds from the breast or bottle. In order to supply those babies with nutrition, a clear plastic tube is inserted through the mouth /nose, into the stomach. Milk is given via the tube.
Ultrasound Sound waves of a very high frequency are often used to produce pictures of structures such as the brain /heart. The examination is safe, painless, and non¬invasive.
Babies born at less than 32 weeks gestation will have an ultrasound of the brain in the first week of life and at 6 weeks of age.
Ventilator/Respirator Ventilators assist with and sometimes take over the work of breathing for your baby as well as provide oxygen to babies with breathing difficulties. The oxygen mixture is given to the baby though an endotracheal tube. The endotracheal tube passes through the nose or mouth and into the wind¬pipe or trachea. It gives direct access to the baby’s lungs.
Other Terms If there are any other words or abbreviations which you do not understand please ask any of the staff, who will be happy to explain.

Parent Handbook 45
The establishment of the Newborn Intensive Care Foundation (NICF) was an initiative of Peter & Susan Cursley as a result of having their newborn baby cared for at the NICU at Canberra Hospital.
The Cursleys established the NICF as a way of saying thank you to the dedicated medical and nursing staff for the support they were given.
Our mission The Foundation’s mission is to raise funds to purchase equipment that enhances the care delivered in the Centre.
Purchases have ranged from additional breast pumps and recliner chairs for nursing mums up to state of the art medical equipment costing hundreds of thousands of dollars. Some of the purchases have meant that babies with particular conditions can now be treated in Canberra rather than being transferred to Sydney for treatment.
The Foundation also contributes to a nurse education fund that enables nursing staff to attend conferences throughout the world to ensure the centre stays at the forefront of neonatal care.
The Need for Funds Whilst the ACT Government provides funding for most staff and necessary equipment, further funding is always required. Ongoing community support is important.
The Foundation needs help from people like you to spread the word on the excellent care provided by the NICU and to encourage people and businesses to donate or hold their own fundraiser for the Foundation.
The Foundation is 100% voluntary so 100% of money donated goes directly to helping sick babies from the Canberra region. All donations over $2 are tax deductible.

46 Neonatal Intensive Care Unit & Special Care Nursery
How to DonateDonations are gratefully accepted by cheque to:
Newborn Intensive Care Foundation Canberra Hospital PO Box 11 Woden ACT 2606
Via direct deposit to either of the following Newborn Intensive Care Foundation bank accounts:
Community CPS Account number: 03425411 BSB: 805-022 Account Name: Newborn Intensive Care Foundation
Service One BSB: 801-009 Account number: 1131937 Account Name: Newborn Intensive Care Foundation

Parent Handbook 47
Would you like to participate in fundraising?You may like to help raise money for a particular piece of equipment – we have a wish list,
or you may like to participate in someone else’s fundraiser.
You can find out more information about this by going to
www.newborn.org.au
Personal Assistant to the Clinical Director on 02 6174 7565.
q YES, I can help with a monetary donation of $
My cheque is enclosed.
An official receipt will be sent by return mail.
q YES, I can help with fundraising activities.
q Please send me further information on the Foundation.
q Please send me an annual reminder for my donation.
Title
First Name
Surname
Organisation
Address
Postcode
Tel
Fax
Post to:
Newborn Intensive Care Foundation Canberra Hospital PO Box 11 Woden ACT 2606

48 Neonatal Intensive Care Unit & Special Care Nursery Patient Handbook 46
Parent Handbook 49
Dear Parent,
We hope that this handbook has helped you understanding a bit more about your baby, the NICU and SCN, and the surrounding area.
This book was written for you, so we would like your feedback regarding what can be improved and what is written well.
Please take a few minutes to fill out this short questionnaire.
When you are finished, please return to your baby’s nurse, or send to:
Project Officer – Neonatology Level 2 Building 11 The Centenary Hospital for Women & Children PO Box 11 Woden ACT
Please do not hesitate to contact us directly to discuss your suggestions.
The Project Officer’s phone number is: 02 6174 7579
Thank you for your time & effort.
1. Do you live in Canberra?
Yes No, I am from
2. Was/ were your baby/ babies admitted to:
NICU SCN NICU & SCN
3. Your baby’s length of stay was:
0-7 days 8-14 days 15-30 days > 30 days
4. What was your overall satisfaction with thr Parent Handbook:
very dissatisfied dissatisfied undecided Satisfied very satisfied
5. The Parent Handbook was easy to navigate
strongly disagree disagree undecided agree strongly agree
Suggestions for improvement:
50 Neonatal Intensive Care Unit & Special Care Nursery
6. The Parent Handbook had all the information I needed:
strongly disagree disagree undecided agree strongly agree
Suggestions for improvement:
7. The Parent Handbook helped decrease the stress of having a baby/ babies admitted
to the NICU/SCN:
strongly disagree disagree undecided agree strongly agree
8. I referred to the Parent Handbook
never rarely occasionally often all the time
9. What was the most helpful information?
a)
b)
c)
d)
10. What was the least helpful information?
a)
b)
c)
d)
11. What else should the handbook include or what should it exclude?
12. Did you find any discrepencies in the Parent Handbook? These were:
13. Any further comments?

Parent Handbook 51

Any feedback & suggestions for this Parent’s Handbook, would be gratefully received, via
the included survey form or can be left with the Neonatology Project Officer on 6174 7579.