Papilloedema and hydrocephalus ependymoma · secondary optic atrophy and non-obstructive...
3
BritishJournal of Ophthalmology 1994; 78: 313-315 CASE REPORTS Papilloedema and hydrocephalus in spinal cord ependymoma Anat Kesler, Riri S Manor Department of Neurology, Meir General Hospital, Kfar Saba, Israel A Kesler Neuro-Ophthalmology Unit, Beilinson Medical Center, Petah Tikva, and the Sackler Faculty of Medicine, Tel-Aviv University, Israel R S Manor Correspondence to: Anat Kesler, MD, Department of Neurology, Meir General Hospital, 44281 Kfar Saba, Israel. Accepted for publication 8 October 1993 Figure I Goldmann perimetry performed with III14 and V14 isoptre before the shunt procedure. Note the absolute loss of nasalfields and the strong depression of temporalfields, especially in the right eye. The association of spinal cord tumours with papilloedema is well known but occurs uncom- monly. In most such cases the spinal lesion is intradural and in more than half of the cases it is an ependymoma. 1-3 We present a case of spinal cord ependymoma in which the initial manifesta- tion was a lowering of vision, with the finding of secondary optic atrophy and non-obstructive hydrocephalus, and in which the spinal cord tumour was detected only 1 month after ventriculo-peritoneal shunt. Case report A 29-year-old man was admitted to the neuro- surgical department of our hospital because of progressive visual loss and blackouts. Five years earlier he had complained of low back pain, especially on effort, but computed tomography (CT) of the spine was normal and in recent years there had been no pain or any other com- plaints until the appearance of the ophthalmic symptomatology. On examination visual acuity was 6/30 in the right eye and 6/9 in the left eye and there was a Marcus-Gunn pupil. The visual fields, tested on a Goldmann perimeter with III/4 and V4 isoptres, showed on the right eye an almost absolute nasal field loss, a very strong contraction of the temporal field, and enlarge- ment of the blind spot. In the visual field of the left eye there was also an almost total loss of the nasal field and a peripherally depressed temporal Figure 2 Computed tomography of brain, showing hydrocephalus. field with inferior arcuate scotoma (Fig 1). The fundus examination disclosed the beginnings of optic atrophy in both eyes, secondary to severe prolonged papilloedema. CT of the brain showed a non-obstructive hydrocephalus (Fig 2). The neurological examination was within normal limits. On lumbar puncture the opening pres- sure was 70 mm H20, the cerebrospinal fluid was xanthochromic, its protein level was 465 mg/ 100 ml, and glucose was normal. Figure 3 Computed tomography of lumbar spine, showing ependymoma. 313 on April 11, 2020 by guest. Protected by copyright. http://bjo.bmj.com/ Br J Ophthalmol: first published as 10.1136/bjo.78.4.313 on 1 April 1994. Downloaded from
Transcript of Papilloedema and hydrocephalus ependymoma · secondary optic atrophy and non-obstructive...

BritishJournal ofOphthalmology 1994; 78: 313-315
CASE REPORTS
Papilloedema and hydrocephalus in spinal cordependymoma
Anat Kesler, Riri S Manor
Department ofNeurology, Meir GeneralHospital, Kfar Saba,IsraelA Kesler
Neuro-OphthalmologyUnit, Beilinson MedicalCenter, Petah Tikva, andthe Sackler Faculty ofMedicine, Tel-AvivUniversity, IsraelR S ManorCorrespondence to:Anat Kesler, MD,Department ofNeurology,Meir General Hospital, 44281Kfar Saba, Israel.Accepted for publication8 October 1993
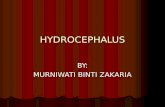
Figure I Goldmannperimetry performed withIII14 and V14 isoptre beforethe shuntprocedure. Note theabsolute loss ofnasalfieldsand the strong depression oftemporalfields, especially inthe right eye.
The association of spinal cord tumours withpapilloedema is well known but occurs uncom-monly. In most such cases the spinal lesion isintradural and in more than half of the cases it isan ependymoma. 1-3 We present a case of spinalcord ependymoma in which the initial manifesta-tion was a lowering of vision, with the finding ofsecondary optic atrophy and non-obstructivehydrocephalus, and in which the spinal cordtumour was detected only 1 month afterventriculo-peritoneal shunt.
Case reportA 29-year-old man was admitted to the neuro-surgical department of our hospital because ofprogressive visual loss and blackouts. Five yearsearlier he had complained of low back pain,especially on effort, but computed tomography(CT) of the spine was normal and in recent yearsthere had been no pain or any other com-plaints until the appearance of the ophthalmicsymptomatology. On examination visual acuitywas 6/30 in the right eye and 6/9 in the left eyeand there was a Marcus-Gunn pupil. The visualfields, tested on a Goldmann perimeter with III/4and V4 isoptres, showed on the right eye analmost absolute nasal field loss, a very strongcontraction of the temporal field, and enlarge-ment of the blind spot. In the visual field of theleft eye there was also an almost total loss of thenasal field and a peripherally depressed temporal
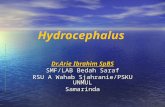
Figure 2 Computed tomography ofbrain, showinghydrocephalus.
field with inferior arcuate scotoma (Fig 1). Thefundus examination disclosed the beginnings ofoptic atrophy in both eyes, secondary to severeprolonged papilloedema. CT ofthe brain showeda non-obstructive hydrocephalus (Fig 2). Theneurological examination was within normallimits. On lumbar puncture the opening pres-sure was 70mm H20, the cerebrospinal fluid wasxanthochromic, its protein level was 465 mg/100 ml, and glucose was normal.
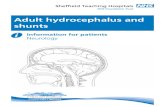
Figure 3 Computed tomography oflumbar spine, showingependymoma.
313
on April 11, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.4.313 on 1 A
pril 1994. Dow
nloaded from

Kesler, Manor
The Millipore examination for cytology wasnegative. The diagnosis was non-obstructivehydrocephalus; it may present with variationsfrom high to normal cerebrospinal pressure andthis normal cerebrospinal pressure was con-sidered to be a momentary variation. A supple-mentary examination of cerebrospinal fluidpuncture was not done and the grossly elevatedprotein result was overlooked.A ventriculo-peritoneal shunt was immedi-
ately instituted. One month later the patientcomplained of lower back pain and urinaryincontinence and examination revealed a sensorylevel at Dlo and bilateral clonus. CT and myelo-graphy demonstrated an intradural blockbetween L2 to DI2 (Fig 3). At operation anintradural and intramedullar mass was found atthe conus covering the filum terminalis. Thehistological examination showed myxopapillaryependymoma.The postoperative course was uneventful and
he received local irradiation. Subsequently, thevisual acuity improved to 6/7 in both eyes andthere was some enlargement of visual fields (Fig4). Ophthalmoscopy showed bilateral secondaryoptic atrophy and a massive depletion of thenerve fibre layer.
CommentAccording to the literature"A more than 50% ofthe spinal cord tumours producing increasedintracranial pressure are ependymomas, mainlylocated in the thoracic and lumbar region. Thecommon denominator in all the reported cases ofpapilloedema with spinal cord tumours was theresolution of the papilloedema following surgicalremoval of the lesion.
In our patient the lack of symptomatologypointing to the presence of a spinal cord tumourled to a delay in its diagnosis, the spinal cordinvestigation having been made only 1 monthafter the diagnosis ofhydrocephalus and second-ary optic atrophy. Retrospectively we can statethat the high level of protein in the cerebrospinalfluid should have served as a warning sign tocontinue the investigation. In fact, the present-
mg sign of the spinal tumour in our case was theisolated visual loss due to secondary opticatrophy. We were able to find only six similarcases in the literature.5
Several authors69 have offered differenttheories in the attempt to explain the develop-ment of increased intracranial pressure andpapilloedema in certain cases of spinal cordtumours. Gardner et al6 postulated that largeprotein molecules may mechanically block thearachnoidal pores and prevent the absorption ofcerebrospinal fluid, thus producing a rise inintracranial pressure. Davson et al7 demon-strated experimentally that infusion of plasmaserum into cerebrospinal fluid slowed its absorp-tion. It is ofnote, however, that in Guillain-Barresyndrome there have been cases with a very highlevel ofprotein in the cerebrospinal fluid withoutdevelopment of increased intracranial pressureand papilloedema, and on the other handthere have been cases in which papilloedemadeveloped although the protein level was onlymoderately elevated or even normal. '0 'The hyperproteinorrhachia may also play an
irritative role, producing an aseptic arachnoiditis,and the extension of the arachnoiditis to thechasmatic cisterns probably explains the exist-ence of severe papilloedema with haemorrhagesand exudates in otherwise asymptomaticpatients. 2 On the other hand, the hyper-proteinorrhachia and the alteration in thecerebrospinal fluid pathway secondary to it, isthe main factor responsible for the developmentof hydrocephalus associated with spinaltumours. Arseni et al8 suggested that undercertain conditions low spinal cord tumours mayrelease products of protein disintegration,increasing the viscosity of the cerebrospinalfluid, and that this hyperviscosity below andabove the tumour upsets the balance betweensecretion and absorption of cerebrospinal fluid,with a slowing down of its circulation from thecranial region to the spinal spaces.
Describing a case very similar to ours Matzkinand Slamovits' implicated repeated episodes ofclinical and subclinical subarachnoid haemor-rhage from the tumour as a possible mechanismof the increased intracranial pressure in spinalcord tumours, particularly ependymoma.Martin et at9 pointed out that the spinal cord actsas an elastic reservoir for cerebrospinal fluid, theflow of the cerebrospinal fluid into and out of thespinal canal being considered of importance inthe maintenance of a constant intracranialvolume. Spinal cord tumours may in fact reducethe capacity of this 'reservoir' by mechanicalblockage and thereby cause papilloedema.5The many explanations offered for the
aetiology ofthe increased intracranial pressure inthese cases indicates that the search for anunequivocal answer has yet to be continued. It isstressed that the possibility of a spinal cordtumour should be kept in mind in cases ofunexplained newly developed papilloedema.
1 Walsh TJ. Neuro-ophthalmology - clinical signs and symptoms.Philadelphia: Lea & Febiger, 1992.
2 Glaser JS. Neuro-ophthalmology. Philadelphia: JB Lippincott,1989.
3 Michowiz SD, Rappaport HZ, Shaked I, Yellin A, Sahar A.Thoracic disc herniation associated with papilledema.JNeurosurg 1984; 61: 1132-4.
Figure 4 Goldmannperimetry performedwith I14and V14 isoptre after theshunt and after the spinalcord ependymoma enision.Note that this time thepatient saw the I14 isoptreand that visualfieldsenlarged.
314
on April 11, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.4.313 on 1 A
pril 1994. Dow
nloaded from

Papilloedema and hydrocephalus in spinal cordependymoma
4 Raynor RB. Papilledema associated with tumors of the spinalcord. Neurology 1969; 19: 700-4.
5 Matzkin D, Slamovits T, Genis I, Bello J. Disc swelling: a talltail? Swv Ophthalmol 1992; 37: 130-6.
6 Gardner WJ, Spitter DK, Whitten C. Increased intracranialpressure caused by increased protein content in cerebro-spinal fluid. An explanation of papilledema in certain casesof small intracranial and intraspinal tumors and in GuillainBarre syndrome. N EnglJ Med 1954; 250: 932-6.
7 Davson H, Hollingsworth G, Segal MB. The mechanism ofthecerebrospinal fluid. Brain 1970; 93: 665-78.
8 Arseni C, Maretesis M. Tumors of the lower spinal cord
associated with increased intracranial pressure andpapilledema.J Neurosurg 1967; 27: 105-10.
9 Martins AN, Wiley JK, Meyers PW. Dynamics of cerebro-spinal fluid and the spinal dura mater. J Neurol NeurosurgPsychiatry 1972; 35: 468-73.
10 Farrell K, Hill A, Chung S. Papilledema in Guillain Barresyndrome. Arch Neurol 1981; 38: 55-7.
11 Sullivan RL, Reeves AG. Normal cerebrospinal fluid protein,increased intracranial pressure and the Guillain Barresyndrome. Ann Neurol 1977; 1: 108-9.
12 Schijman E, Zuccaro G, Monges J. Spinal tumors andhydrocephalus. Child'sBrain 1981; 8: 401-5.
BritishJoumal ofOphthalmology 1994; 78: 315-316
Metastatic prostatic adenocarcinoma presenting ascomplete ophthalmoplegia from pituitary apoplexy
David Frederick Anderson, Farhad Afshar, Namir Toma
Pituitary apoplexy is a rare presentation ofpituitary disease. A case resulting in suddenbilateral complete ophthalmoplegia due to aprostatic metastasis is described for the firsttime. The pathogenesis of this condition andrelevant literature are discussed.
Case reportAn 81-year-old West Indian man presented witha 4 day history of severe headache and suddenvisual loss on the left. He reported polydipsia butno nausea or vomiting. His ophthalmic historyincluded advanced open angle glaucoma blind-ing his right eye, previous left cataract extractioncomplicated by removal ofthe implant, and rightbranch retinal vein occlusion. Thirty two yearsearlier he had undergone a bilateral orchidec-tomy for prostatic carcinoma.
Department ofNeurosurgery, 4th Floor,Queen Elizabeth H Block,St Bartholomew'sHospital, LondonD F AndersonF AfsharN TomaCorrespondence to:Mr F Afshar, Department ofNeurosurgery, QueenElizabeth II Block,St Bartholomew's Hospital,West Smithfield, LondonEC1A 7BE.Accepted for publication23 Sepember 1993
On examination he was afebrile, oriented butinattentive and had complete bilateral ophthal-moplegia and complete ptosis. Best visualacuities were light perception right eye and 3/24left eye. Corneal sensation was absent but therewere no other cranial nerve or long tract signs.He was normotensive with a pulse of54 and therewere no other signs of endocrine disease.Endocrine function tests confirmed panhypo-pituitarism and cranial diabetes insipidus (cD1).A bone scan revealed widespread metastases
and high resolution contrast computed tomo-graphy scan of the head demonstrated destruc-tion of the pituitary fossa by a solitary enhancingmass eroding inferiorly into the sphenoid sinusand posteriorly through the dorsum sella to reachthe pons. There was both supra and parasellarextension (Fig IA and B).A provisional diagnosis of pituitary apoplexy
.~~~~~~~~~~~~~~~~-.1
I~~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~I ----------*-.-_Fig IA Fig IB
Figure I Metastatic deposit demonstrated by contrast enhanced high resolution computed tomography. Horizontal (A), andsagittal sections with vertical reconstruction (B), demonstrating a solitary enhancing deposit filling the fossa and expandingsuperiorly, laterally, and posteriorly.
315
on April 11, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.4.313 on 1 A
pril 1994. Dow
nloaded from