Paperless or Paperlight? That is the question… Presented by Hélène Somerville.
29
Paperless or Paperlight? That is the question… Presented by Hélène Somerville
-
Upload
amber-hoover -
Category
Documents
-
view
218 -
download
0
Transcript of Paperless or Paperlight? That is the question… Presented by Hélène Somerville.

Paperless or Paperlight?That is the question…
Presented by Hélène Somerville

Background
• September 2013 – initial discussions - Mobile Working
- Paperless Service.• GPs had been using SystmOne (S1) for several years.• Obvious choice… BUT it was not designed for SLT use!• Initially used for recording SLT face to face contacts and
admin contacts.• 3 different geographical areas operating 3 different S1
units. East & North Herts, West Herts and West Essex.

Process
• Numerous Meetings to map requirements onto S1.- Business change team- Senior Manager
- 2 x Clinicians • Processes need to be exact and comprehensive• Capture each step from referral to discharge.• Then replicated onto the system - S1.

Examples
•How will referrals come in?•How to send appointments out?•How to run a clinic?•What letters do we need?

A Light Bulb Moment
Paperless vs Paperlight is about way more than writing
up the case notes.

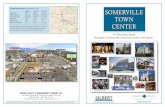
Referral process To Be Process: Register / Referral / Triage (Including Dysphagia)
Service: Children’s Speech & Language Therapy ServiceCreated By: Informatics – Sarah Brannen, Business Change Team
Date / Version / Page 17th Oct 2014 Version 2 Page 1 of 1
START OF PROCESS
Is child already registered on S1 with
the same referral reason?
Record Ethnicity & Smoking Status (Patient Profile) if relevant
Scan Paper Referral into child’s record if available
Contact Referrer to advise that child already referred for this
referral reasonScan referral into record and Task
Therapist to advise further information available
Is child Statemented?
END OF PROCESS
Speech, Language & Communication ReferralReason – Speech, Language & Communication(Routine)Referral Outcome - “Accepted”Referral Status - “Waiting for Care”Caseload – Triage SLCOR Dysphagia ReferralReferral Reason – Feeding & Swallowing(Routine)Referral Outcome - “Accepted”Referral Status - “Waiting for Care”Caseload – Triage Dysphagia
Referral received
Paper referral – Will require scanning into the S1 recordElectronic referral - Tasks must be accepted to report on inappropriate referrals)
Yes
Triage Team checks Triage SLC/Triage Dysphagia Caseload
Review New Referrals
Is Referral Accepted?
Add to appropriateWaiting for Assessment / PSN Dysphagia
CaseloadWaiting for Assessment Waiting List /
Dysphagia (Location) Waiting ListUpdate Waiting List Notes accordingly
Send Admin Discharge at New Referral Task to
End Referral using appropriate discharge Reason
& Print & send Discharge at Referral Letter
Task receivedCreate, print & send
Discharge at Referral Letter using appropriate Discharge Code
End Referral – using Discharge Reason
End Care if no further active referrals
Register (Re-register)Create New Referral In
Service Offered - “Statemented child – SLT in part 3”
Register/Re-registerCreate New Referral In
Service Offered – ‘Children’s SLT”
No
Yes
Complete “Child with Special Needs”
template, include date of Statement “Additional/Previous Record
Held” template with details of where Statement or any other paper records
are held
YesNo
Clinician Admin
Key
Ensure Date of Referral Column included on Caseload screen (as not sending Task) to be able to identify the new referrals
No
Task/Phone Dysphagia therapist to confirm New Referrals
Amend Status for Dysphagia referrals to Urgent if necessary
If further investigation required add patient to ‘Waiting for Action at Triage’ Waiting List, until further information received then move to Waiting for Assessment Waiting Lists as normal

Booking
Appointments
To Be Process: Book Appointment / Initial Assessment (CLINIC)
Service: Children’s Speech & Language Therapy ServiceCreated By: Informatics – Sarah Brannen - Business Change Team
Date / Version / Page 17th Oct 2014 Version 1 Page 1 of 1 LOGO???
START OF PROCESS
Send completed Service Questionnaire to AdminComplete Paediatric SLT Assessment & Diagnosis
Template Generate Screening Report.
Apply relevant Tier Care Plan(s) if appropriate & Perform
If any other paper documents/assessments completed – record location using Additional/Previous Record Held template OR send to admin to Scan into record
‘Report to be Sent’ Task to Admin team for distribution of Screening report
Remove from Waiting for Assessment Waiting List
Add to appropriate Intervention (Waiting) List Update Waiting List Notes accordingly
Assign to Caseload
Is furtherAssessment/Intervention required?
End Tier Care Plan (s) if applied End Referral using Discharge
Reason &End Care if no further active
referralsIf Appropriate (DNA)
Create Discharge Summary/Letter & Task Admin to distribute
END OF PROCESS
‘Initial Appointment Letter to be sent’ Task received
Create, print & send Initial Appointment in Clinic Letter from Waiting List Actions
Update Waiting List Notes as appropriate
Patient contacts within 3 weeks?
Book Appointment into appropriate slot in Therapist’s Staff Diary.
Update Waiting List Notes accordingly
Patient attends
Clinician Admin
Key
Therapist Reviews Waiting for Assessment Waiting List
Books required number of Textual Appointments using Appointment Templates & Presets in Staff
Diary. Sends ‘Initial Appointment Letter to be sent’ Task to admin detailing Waiting List, Number of patients to
be invited and details of Textual appointments
Yes
Questionnaire receivedScan into record - shredRecord/Check Ethnicity
(Patient Profile)Record Consent
‘Report to be Sent’ Task received- Print &
Distribute ReportSend ‘SLT Report to
be Read’ Task to appropriate HV Group in
CUS unit
No
Create Discharge Letter/Summary – using appropriate Discharge Code End Referral –
using Discharge reason
End Care if no further active
referralsTask Admin to print & send Discharge Letter/Summary
Yes
Patient cancels appointment
Attempt to Rebook appointment for child cancelling
AND/OR Update Waiting List notes
accordingly.Review Waiting
List to allocate free appointment to
alternative child (Use Priority & Therapist’s
Initials to identify)
Following review of record, Discharge
patient?
Initial Appointment to be Sent Task to Admin to rebook
Appointment
Yes
No
No
Yes
Yes
Create & send No
Response LetterUpdate
Waiting List Notes
Following review of record,
Discharge patient ?
No
Task Admin to send another Appointment
No
Task ReceivedPrint & send
Discharge Summary/Letter
Task receivedPrint & send Discharge Summary/
Letter
Therapist may book appointments with Dysphagia patients direct to ensure seen within required timescales
Record DNAUpdate
Waiting List Notes
Yes
No
Task Therapist to advise
No Contact Made

Top Tips
• Protected project time: - one staff member seconded as full time role.
• Experience of the system. • Visit locations to see in action.• Co-ordinate training and going live.
- staff can put learning straight into practice.• Check software requirements and compatibility
with any new computers.• Get used to the new vocabulary – semantics.

Clinical vs Non Clinical Contacts
• Record and capture data for Audit: Staff activity, waiting times,
Specialist versus Universal working
Research: Reporting co-existing diagnosis
Outcomes: Adapted the East Kent Outcome System. Called a Questionnaire just to confuse us...all part of
adapting our needs into an existing system.

Letters and Reports Come From The Process
• Letters circulated from central hubs - three hubs with the relevant admin address and telephone number.
• Move to mobile working means many clinics not manned during the day - To avoid messages being left on answerphones,
letters only have the admin telephone numbers • Patients can therefore always speak to a person. • Task from S1 (like an email) then sent to therapist with the
message.• Less personal approach for letters versus less unanswered calls.

Text Messages
• Text Reminder two days before a clinic/home visit when in electronic ledger/diary.
• No text reminder for school visits.• Text can be sent at appointment booking via
electronic ledgers/diary.• Possibility of confusion.• Reduces DNAs.

Setting Objectives To Be Process: School Visits (Setting Objectives / Recording Outcomes)
Service: Children’s Speech & Language Therapy ServiceCreated By: Informatics – Business Change Team
Date / Version / Page 31st Oct 2014 Version 1 Page 1 of 1
Clinician Admin
Key
END OF PROCESS
START OF PROCESS
Start of Term/Treatment (when appropriate)Review Tier Care Plan (s) as appropriate & add
alternative(s) & if required & PerformComplete Therapy Plan Objectives
Questionnaire - Save as Final VersionCreate SLT Objectives Therapy Plan in
Communications & Letters - Save as Final Version
Complete Paed SLT SOAP Progress/Paediatric SLT Assessment & Diagnosis templates as
appropriateIf any other Paper documents completed – record location using Additional/Previous Record Held Template OR send to admin to Scan into recordTask sent to Admin to Print & send copy of SLT
Objectives Therapy Plan to Parents/Carers
Child on School Intervention Waiting List has Appointment(s) booked
Approaching End of Term/TreatmentComplete SLT Therapy Plan Outcomes Questionnaire – Save as Final VersionCreate SLT Outcomes Therapy Plan in
Communications & Letters – Save as Final Version
Task Admin to Print & Send copy of SLT Outcomes Therapy Plan to Parents/Carers
Task received Print and send SLT Objectives/
Outcomes Therapy Plan to Parents/Carers
Therapist attends meeting with SENCo
Further intervention
required
Add to appropriate Schools Intervention Waiting List OR
Update Waiting List Notes accordinglyCheck on appropriate Caseload
Yes
No
End Tier Care Plan(s) Create Discharge Summary/
Letter if appropriate End Referral using appropriate
Discharge Reason End Care if no further active
referralsTask Admin to Print & send Discharge Letter/Summary
Task receivedPrint & Send Discharge
Summary/Letter
‘On-going’ Face to Face TherapyUse Paed SLT Progress (SOAP) Notes
Template to record contactsReview Tier Care Plan(s) as appropriate and add
alternative(s) & if required & Perform
Care Plans will need to be Performed when applied.

Therapy Blocks To Be Process: Therapy Blocks
Service: Children’s Speech & Language Therapy ServiceCreated By: Informatics – Business Change Team
Date / Version / Page 18th Nov 2014 Version 1 Page 1 of 1
Clinician
Admin
Key
START OF PROCESS
Therapist reviews appropriate Intervention (Waiting) List and amends required number of slots to Therapy Blocks
Send Appointment Letter to be Sent Task to Admin detailing Patients to be booked and appointment details
Task received Therapy Appointment Letters created & sent
Update Therapy Intervention Waiting List Notes accordingly
Patient contacts within
3 weeks?
Book (Assign Patient) block of Appointments – Therapy Blocks
Review/add Tier Care Plan(s) & PerformComplete Paed SLT Progress (SOAP) Notes Template OR Paediatric SLT Assessment &
Diagnosis Template as necessaryReview/set SLT Objectives/Outcomes
Questionnaire if appropriate – create appropriate SLT Therapy Plans
Generate SLT Progress Report if requiredReport to be Sent Task sent to Admin Team for
distribution
Task receivedSend ‘SLT Report to be Read’ Task
to appropriate Health Visitor
Group in CUS unitDistribute Report
accordingly
Add to appropriate Intervention Waiting List or update Waiting List Notes accordingly.
Check Caseload
END OF PROCESS
Complete SLT Outcomes Questionnaire & Therapy Plan
(save Final Versions)End Tier Care Plan(s)
End Referral using appropriate Discharge Reason &
End Care if no further active referrals
Create Discharge Letter/ Summary if appropriate
Task Admin to print & send Discharge Letter/summary
Yes
Patient cancels Appointment?
Task Therapist to advise Patient
cancelled and slot now available for
rebooking
Patient attends?Following review
of Record Discharge Patient?
No
Send No Response
Letter Update
Waiting List Notes
Task Admin to rebook
appointment
Yes
Letter includes only Dates not specific times of appointments
Task Admin to rebook
appointment with alternative
patients names
No
Record DNA & Update Waiting
List Notes
At the End of Block is further
Intervention required?
Admin picks from Waiting List or does Therapist confirm names??
Task received Print & send Discharge
Letter/Summary
No
Yes
Yes
Yes
Patient responds?
No
Yes
No
No
Task Therapist to advise No Contact
made
Patient attends next
appointment?
Yes
No


Checklist for Appointments and/or Admin Time• Check child’s address and telephone number.• Add ethnicity if not recorded.• Update consent template.• Initial assessment- complete paediatric SLT assess and
diagnosis notes.• Therapy/review/Drop in- complete SOAP notes.• Care plan- create or check.• After initial assessment – remove from waiting list,
amend caseload and add to intervention list.• Intervention list – amend notes/waiting since and due
date.

Checklist for Appointments and/or Admin Time• Set new objectives (programme).• Complete outcomes for previous objectives.• Write report.• Task admin group to circulate report, programme and
outcomes• Add information to Children’s ongoing diagnosis
template if appropriate e.g. type of cleft• Add details to groups and relationships (e.g. family
members, professionals)• Add reminder if required e.g. safety issues in home,
dog at property.

Benefits• Shared Access to information from involved
services(subject to parental agreement).• Access to alerts: Safeguarding issues, domestic abuse
etc.• Joined up working with local SLTs - one shared set of
notes.• Use of admin staff to deal with all initial queries.• Use of admin for circulation of reports.• Reports and letters templates save time. • Child’s information automatically populates – safer
record.

Benefits
• Drop-in - admin can check if child previously known. - quick access to alerts, HV information. - Can email advice to parents.
• Able to stay in one place to do reports/programmes.• Can complete everything on the day.• Don’t have to go back to clinic to print – task admin.

Benefits
• Reduces SLT admin time – quicker to send task• Standardised formats/templates across the
service• Don’t’ have to carry big files around• Safer transfer of care to colleagues – no case
notes in internal post!

Benefits
• Everything attached to patient record - Tasks from the patient record can check. - Assessments scanned on.- Objectives.- Outcomes.
• Increased Flexibility - Able to access patient information from any location.- Flexibility to work from home, school, other base.

Benefits
• User messaging – - Can message SLT who is logged onto S1 - Can see if staff on annual leave
• Intervention lists for each team- Better information sharing and transparency
• No need to keep end of the month records as all the information there.
• Can see who has breached time constraints as names go red.
• Can collect information on conditions e.g. SLI caseload, Down’s Syndrome.

Challenges
• Reliant on internet access –“dead” spots in the Hertfordshire countryside.
• Time taken to “fireup” the laptop and enter the many passwords and security cards to get onto S1.
• Speed of typing! • Trying to type and simultaneously keep the child from
joining in on the laptop.• Transcription - still allowed to do with pen and paper
but difficult to do with lap top open as well for reasons given above. I need another pair of hands!

Challenges
• Unable to merge the 3 S1 units - I have 3 ledgers!• Took time initially to move all my patients into units.• Only current patients on S1. • Review & cleft clinic only patients discharged & re-
registered each time they are seen.- Extra admin for me.- Potential for loosing them to follow up.
• Can take time for letters, assessments to be scanned on.• Keeping all the information in your head once you are
typing in the SOAP notes as can’t get out of this box and in again.

Challenges
• Maintaining eye contact during consultations whilst typing.
• Reading long reports on screen.• These last two do seem to be a bit age specific
but not exclusively so…..

The Clinical Tree

Paperless or Paperlight?
• Our service is paperlight - much to our relief!• Large documents such as Statements or EHC Plans,
Large booklet assessments such as the ACE are NOT scanned in but kept in manila folders
• We can also keep a paper copy of the questionnaire (i.e. our current targets) so that we can refer to it during therapy sessions and e.g. for my role copies of the GOS.SP.ASS.

How are we doing?
• Just over 6 months in we are slowly getting used to doing everything via our laptops.
• Finding out new things you can do on S1 all the time.
• Not sure the typing is getting quicker.• But probably most importantly we wouldn’t
go back to paper records.

What about the future?
• Looking at the possibility of using Skype as has been trialled by an adult service within our Trust
• Using the intervention lists to find children with similar needs and seeing in groups
• Closer links with GPs.

Any Questions?
Thank you for listening.