PANCREATIC ENLARGEMENT AND WILSON'S DISEASE
2
337 Serum bilirubin and liver enzyme levels in patient with cholestatic jaundice after exposure to cefazolin (K) and cefadroxil (D) therapy. prompt deterioration followed discontinuation of therapy (figure). The patient was seen as an outpatient on Jan. 26, 8 weeks after onset of jaundice. No further investigations seemed indicated, and the patient was started for 4 weeks on cholestyramine 15 g daily and phenobarbitone. The itching promptly disappeared; the jaundice and liver function test abnormalities disappeared gradually. The patient has been free of symptoms since mid-February. Immunological tests were done in April. Skin tests with penicillin G, ampicillin, cefazolin, and cefadroxil were negative but a lymphocyte transformation stimulation test5 yielded a stimulation index with cefazolin of 2-45 (positive) whereas the index was negative with the two penicillins and with cefadroxil (1-11—1’ 67). Our patient thus had typical intrahepatic cholestasis for which virtually all known causes had been excluded. Mefenamic acid is not known to induce liver disease.6-8 Nor have cephalosporins been implicated in severe liver damage. There is, however, good reason to look at adverse reactions to cephalosporins in the context of reactions to penicillins since cross-reactivity to cephalosporins is demonstrable in about 10% of penicillin-hypersensitive patients,8,9 this being related to the beta-lactam structure shared by both groups of antibiotics. Semisynthetic penicillins may cause cholestasis and/or hepatitis.I,IO-14 Hypersensitivity has been postulated in these cases rather than toxic mechanisms affecting the liver tissue. 1,8,10,11,13 The sequence of events in our patient strongly suggests a direct relation between therapy with cephalosporins and reversible cholestatic jaundice. Although a stimulation index of 2 - 45 with cefazolin in the lymphocyte transformation test indicates sensitisation, it provides no proof for an immune-mediated reaction, and the accompanying rise ofeosinophils within the normal range is non-specific. Nevertheless, in view of similar reactions induced by the structurally related penicillins, hypersensitivity to cephalosporins seems a reasonable explanation for this case. 5. Schellekens PTA, Eijsvogel VP. Lymphocyte transformation in vitro. Clin Exp Immunol 1968; 3: 571-84. 6. Balali-Mood M, Cntchely JAJH, Proudfoot AT, Prescott LF. Mefenamic acid overdosage. Lancet 1981; i: 1354. 7. Robertson CE, Ford MJ, van Someren V, et al. Mefenamic acid nephropathy. Lancet 1980; ii: 232. 8. Goodman LS, Gilman A. The pharmacological basis of therapeutics. New York. Macmillan, 1980. 9. Delafuente JC, Panush RS, Caldwell JR. Penicillin and cephalosporin immunogenicity in man. Ann Allergy 1979; 43: 337. 10. Dismukes WE. Oxacillin-induced hepatic dysfunction. JAMA 1973; 226: 861-63. 11. Bruckstein AH, Attia AA. Oxacillin hepatitis. Am J Med 1978; 64: 519-22. 12. Enat R, Pollack A, Ben-Arieh Y, Livni E, Barzilai D. Cholestatic jaundice caused by cloxacillin. Br Med J 1980; 280: 982-83. 13. Onorato IM, Axelrod AL. Hepatitis from intravenous high-dose oxacillin therapy. Ann Intern Med 1978; 89: 497-500. 14. Williams CN, Malatjalian DA. Severe penicillin-induced cholestasis in a 91-year-old woman. Dig Dis Sci 1981; 26: 470-73. Rechallenge would be unethical. Nevertheless our data indicate that cephalosporins are potentially hepatotoxic. Department of Internal Medicine, University Hospital, CH-8091 Zurich, Switzerland Institute of Pathology, Münsterlingen Institute of Clinical Immunology, Inselspital, Bern R. AMMANN K. NEFTEL TH. HARDMEIER M. REINHARDT NITRATE-REDUCING BACTERIA IN THE STOMACH SIR,-Dr Reed and his colleagues (July 3, p. 39) raised a number of questions about the findings of our study (May 15, p. 1091). Their statement that "absence of nitrate-reducing bacteria for long periods suggests rapid gastric emptying" is only one of several possibilities and it is incorrect to state that "many patients with peptic ulcers have much delayed gastric emptying". Delayed gastric emptying is not a feature of uncomplicated duodenal ulcer’ but may occur with gastric ulcer. 2 Reed answers his own question of why volunteers were not allowed to eat freely by his observation that "the availability of nitrite is very dependent on diet". Standardisation of diet is essential if nitrite derived substances are to be measured. Individual results, which comprise over 5000 measurements, were omitted out of consideration of space and results were expressed as medians to render the data more accessible to the reader without disguising the wide individual variations. Individual results are available on request. Reed and colleagues’ comments on the analytical method are incorrect. This is fully explained in the reference they cited,3 a copy of which can be supplied. Department of Gastroenterology, Royal Naval Hospital, Hasla, Gosport, Hants G. J. MILTON-THOMPSON PANCREATIC ENLARGEMENT AND WILSON’S DISEASE ;)iK,—we nave seen ultrasound evidence tor pancreatic enlarge- ment before and at the beginning of treatment in two unrelated children with Wilson’s disease. This enlargement may represent a congestive pancreatitis and reflect a potential for a child’s pancreas to distend with interstitial oedema in response to early portal and splenic hypertension. These previously normal children came from similar back- grounds and neither had any family history of Wilson’s disease. They presented differently, one with a neurological and the other with hepatic disease. The first patient was a girl of 14 years who, after 4 months of increasing symptoms, presented with the dystonic form of the disease; apart from mild palmar erythema, there was no clinical or biochemical evidence of liver involvement. Copper deposition is generalised, even in the predominantly lenticular presentation. A typical cupriuresis to penicillamine provocation was obtained, and, 1 week after the start of therapy, an abdominal ultrasound showed diffuse enlargement of the pancreas with greater echogenicity than normal. The normal pancreas has an echogenicity slightly greater than that of the liver, and, on this occasion, liver echogenicity was normal, though the liver was difficult to display since it was small and under the rib cage. The portal and splenic veins were, however, slightly dilated (figure). A further ultrasound 2 months later, when the patient was on a reduced dose of penicillamine and oral steroids (because of thrombocytopenia and leucopenia), showed the pancreas now to be of normal size and echogenicity. The portal vein was of normal 1. Fordtran JS, Walsh JH. Gastric acid secretion rate and buffer content of the stomach after eating: Results in normal subjects and in patients with duodenal ulcer. J Clin Invest 1973; 52: 645-57. 2. Miller LJ, Malegelada JR, Longstreth GF, Go VLW. Dysfunction ofthe stomach with gastric ulceration. Dig Dis Sci 1980; 25: 857-64. 3. Bavin PMG, Darkin DW, Viney NJ. Total nitroso compounds in gastric juice. In: Proceedings of 7th International Meeting on Nitroso Compounds (Tokyo, September, 1981). Lyons: IARC (in press).
Transcript of PANCREATIC ENLARGEMENT AND WILSON'S DISEASE

337
Serum bilirubin and liver enzyme levels in patient with cholestaticjaundice after exposure to cefazolin (K) and cefadroxil (D) therapy.
prompt deterioration followed discontinuation of therapy (figure).The patient was seen as an outpatient on Jan. 26, 8 weeks afteronset of jaundice. No further investigations seemed indicated, andthe patient was started for 4 weeks on cholestyramine 15 g daily andphenobarbitone. The itching promptly disappeared; the jaundiceand liver function test abnormalities disappeared gradually. Thepatient has been free of symptoms since mid-February.
Immunological tests were done in April. Skin tests with penicillinG, ampicillin, cefazolin, and cefadroxil were negative but a
lymphocyte transformation stimulation test5 yielded a stimulationindex with cefazolin of 2-45 (positive) whereas the index wasnegative with the two penicillins and with cefadroxil (1-11—1’ 67).Our patient thus had typical intrahepatic cholestasis for which
virtually all known causes had been excluded. Mefenamic acid is notknown to induce liver disease.6-8 Nor have cephalosporins beenimplicated in severe liver damage. There is, however, good reason tolook at adverse reactions to cephalosporins in the context ofreactions to penicillins since cross-reactivity to cephalosporins isdemonstrable in about 10% of penicillin-hypersensitive patients,8,9this being related to the beta-lactam structure shared by both groupsof antibiotics. Semisynthetic penicillins may cause cholestasisand/or hepatitis.I,IO-14 Hypersensitivity has been postulated inthese cases rather than toxic mechanisms affecting the livertissue. 1,8,10,11,13 The sequence of events in our patient stronglysuggests a direct relation between therapy with cephalosporins andreversible cholestatic jaundice. Although a stimulation index of2 - 45 with cefazolin in the lymphocyte transformation test indicatessensitisation, it provides no proof for an immune-mediated reaction,and the accompanying rise ofeosinophils within the normal range isnon-specific. Nevertheless, in view of similar reactions induced bythe structurally related penicillins, hypersensitivity to
cephalosporins seems a reasonable explanation for this case.
5. Schellekens PTA, Eijsvogel VP. Lymphocyte transformation in vitro. Clin ExpImmunol 1968; 3: 571-84.
6. Balali-Mood M, Cntchely JAJH, Proudfoot AT, Prescott LF. Mefenamic acidoverdosage. Lancet 1981; i: 1354.
7. Robertson CE, Ford MJ, van Someren V, et al. Mefenamic acid nephropathy. Lancet1980; ii: 232.
8. Goodman LS, Gilman A. The pharmacological basis of therapeutics. New York.Macmillan, 1980.
9. Delafuente JC, Panush RS, Caldwell JR. Penicillin and cephalosporin immunogenicityin man. Ann Allergy 1979; 43: 337.
10. Dismukes WE. Oxacillin-induced hepatic dysfunction. JAMA 1973; 226: 861-63.11. Bruckstein AH, Attia AA. Oxacillin hepatitis. Am J Med 1978; 64: 519-22.12. Enat R, Pollack A, Ben-Arieh Y, Livni E, Barzilai D. Cholestatic jaundice caused by
cloxacillin. Br Med J 1980; 280: 982-83.13. Onorato IM, Axelrod AL. Hepatitis from intravenous high-dose oxacillin therapy. Ann
Intern Med 1978; 89: 497-500.14. Williams CN, Malatjalian DA. Severe penicillin-induced cholestasis in a 91-year-old
woman. Dig Dis Sci 1981; 26: 470-73.
Rechallenge would be unethical. Nevertheless our data indicate thatcephalosporins are potentially hepatotoxic.Department of Internal Medicine,University Hospital,CH-8091 Zurich, SwitzerlandInstitute of Pathology,Münsterlingen
Institute of Clinical Immunology,Inselspital, Bern
R. AMMANNK. NEFTEL
TH. HARDMEIER
M. REINHARDT
NITRATE-REDUCING BACTERIA IN THE STOMACH
SIR,-Dr Reed and his colleagues (July 3, p. 39) raised a number ofquestions about the findings of our study (May 15, p. 1091).Their statement that "absence of nitrate-reducing bacteria for
long periods suggests rapid gastric emptying" is only one of severalpossibilities and it is incorrect to state that "many patients withpeptic ulcers have much delayed gastric emptying". Delayed gastricemptying is not a feature of uncomplicated duodenal ulcer’ but mayoccur with gastric ulcer. 2Reed answers his own question of why volunteers were not
allowed to eat freely by his observation that "the availability ofnitrite is very dependent on diet". Standardisation of diet is essentialif nitrite derived substances are to be measured.Individual results, which comprise over 5000 measurements,
were omitted out of consideration of space and results were
expressed as medians to render the data more accessible to the readerwithout disguising the wide individual variations. Individual resultsare available on request.Reed and colleagues’ comments on the analytical method are
incorrect. This is fully explained in the reference they cited,3 a copyof which can be supplied.
Department of Gastroenterology,Royal Naval Hospital,Hasla, Gosport, Hants G. J. MILTON-THOMPSON
PANCREATIC ENLARGEMENT AND WILSON’SDISEASE
;)iK,—we nave seen ultrasound evidence tor pancreatic enlarge-ment before and at the beginning of treatment in two unrelatedchildren with Wilson’s disease. This enlargement may represent acongestive pancreatitis and reflect a potential for a child’s pancreasto distend with interstitial oedema in response to early portal andsplenic hypertension.These previously normal children came from similar back-
grounds and neither had any family history of Wilson’s disease.They presented differently, one with a neurological and the otherwith hepatic disease.The first patient was a girl of 14 years who, after 4 months of
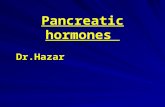
increasing symptoms, presented with the dystonic form of thedisease; apart from mild palmar erythema, there was no clinical orbiochemical evidence of liver involvement. Copper deposition isgeneralised, even in the predominantly lenticular presentation. Atypical cupriuresis to penicillamine provocation was obtained, and,1 week after the start of therapy, an abdominal ultrasound showeddiffuse enlargement of the pancreas with greater echogenicity thannormal. The normal pancreas has an echogenicity slightly greaterthan that of the liver, and, on this occasion, liver echogenicity wasnormal, though the liver was difficult to display since it was smalland under the rib cage. The portal and splenic veins were, however,slightly dilated (figure).A further ultrasound 2 months later, when the patient was on a
reduced dose of penicillamine and oral steroids (because of
thrombocytopenia and leucopenia), showed the pancreas now to beof normal size and echogenicity. The portal vein was of normal
1. Fordtran JS, Walsh JH. Gastric acid secretion rate and buffer content of the stomachafter eating: Results in normal subjects and in patients with duodenal ulcer. J ClinInvest 1973; 52: 645-57.
2. Miller LJ, Malegelada JR, Longstreth GF, Go VLW. Dysfunction ofthe stomach withgastric ulceration. Dig Dis Sci 1980; 25: 857-64.
3. Bavin PMG, Darkin DW, Viney NJ. Total nitroso compounds in gastric juice. In:Proceedings of 7th International Meeting on Nitroso Compounds (Tokyo,September, 1981). Lyons: IARC (in press).

338
Abdominal ultrasound of a 14-year-old girl with Wilson’s disease,showing the enlarged pancreas (P) and slightly dilated splenic vein(SV).
diameter but the spleen was slightly enlarged and the splenic veinjust above normal. A similar ultrasound was seen at 4 months duringan interruption in chelation therapy, brought about by a recurrenceof depressed platelet and white cell counts following trientinetherapy. IThe second case was a boy of 9 years with the slightly more
common hepatic presentation. He was jaundiced and hadabdominal pain on admission and was found to have a severemalabsorptive state with very high amylase values, abdominaldistension, and ascites. There was associated hypoalbuminaemiaand severe normochromic anaemia. The liver edge was palpable, ofnormal consistency, and not tender, but no splenic enlargement orother organomegaly was found.Before a definitive diagnosis of Wilson’s disease was reached, an
abdominal ultrasound scan showed a large transonic structurecrossing the midline and centered 13 cm above the umbilicus andcontaining multiple fine echoes. It was larger in its anteroposteriordiameter on the right side than on the left, and was consistent withan enlarged oedematous pancreas. Subsequent penicillaminetherapy resulted in abolition of the patient’s symptoms.In both of these children, enlargement of the pancreas was
observed on ultrasound either before or within the first week of
copper chelation. In the first case the echogenicity of the gland wasincreased and in the second case it was decreased. Since
echogenicity is a function of the acoustic impedance mismatchesbetween structures,‘ either finding is theoretically compatible withoedema of the pancreas.The pancreas has never been shown to be involved with copper
deposition in Wilson’s disease, and there was no evidence in eitherpatient of other causes for pancreatic hypertrophy, such as
obstructive pancreatopathy from calculi, cystic changes, calcifica-tion, or congenital abnormalities.3 3Since the venous drainage of the pancreas is from the splenic and
superior mesenteric veins (and their tributaries) and ultimately attheir junction, into the portal vein, one could expect the pancreas tosuffer congestive changes from liver disease with portal hyper-tension in a similar manner to the well recognised ascites, gastro-intestinal haemorrhage and oedema, and portocaval shunts.
1. Walshe JM. Treatment of Wilson’s disease with trientine (triethylene tetramine)dihydrochloride. Lancet 1982; i: 643-47
2. Kurtz AB, Rubbins PA, Rubin CS, Kurtz RJ, Cooper HS, Cole-Beuglet Catherine,Goldberg BB. Echogenicity: Analysis, significance, and masking. AJR 1981 (Sept):471-76.
3 White TT Chronic pancreatitis In: Keynes WM, Keith RG, eds The pancreas.London: Heinemann, 1981: 320-29.
We know of no other published observations of pancreaticenlargement in Wilson’s disease and wonder if such enlargement is apotential of the young pancreas only, or if the increasing use ofultrasonography will yield more instances of this phenomenon.Department of Child Life and Health,University of Edinburgh,Edinburgh EH9 1UWand Royal Hospital for Sick Children,
Edinburgh
R. A. MINNSO. B. EDENG. M. A. HENDRY
SOMATOSTATIN IN PERSISTENTGASTROINTESTINAL FISTULA TREATED BY TOTAL
PARENTERAL NUTRITION
SIR,-Total parenteral nutrition (TPN) is helpful in the treatmentof gastrointestinal fistula. Long-term TPN is usually required,leading to spontaneous closure in 70-80 % of cases; on averageTPN lasting 22-45 days has been required for closure in publishedseries. In these circumstances the mortality rate ranges from 10 to53 %, depending upon the age of the patients and whether they havesepsis or cancer. I,TIn a consecutive series of six patients with persistent gastro-
intestinal fistulae, somatostatin3,4 was given together with TPN(figure). In the first two cases somatostatin was given after onemonth of ineffective nutritional therapy. The origins of the fistulaewere colon involvement in a case of severe necrotising pancreatitisand remnant small intestine after subtotal resection. In cases 3 and 4somatostatin was used early-after 2 weeks of TPN. These patientshad fistulae originating from the pancreas after partial resection andfrom the small intestine after extended resection. In the fifth casesomatostatin was added to TPN even earlier-after a week oftreatment for a pancreatic fistula developing after a cephalicresection. In the last case, a duodenal fistula after gastrectomyassociated with acute gastrointestinal bleeding, somatostatin wasgiven in an emergency after the second week of TPN.
Before somatostatin use, daily outputs varied from 300 to 1500 ml(figure). Doses of somatostatin were 250 g/h for 48 h and 125 laglhover the next 48 h.
1. Deitel M. Nutritional management of external gastro-intestinal fistulas In:
Proceedings of the 1st European Congress of Parenteral and Enteral Nutrition,1979: 91.
2. Thomas RJS. The response of patients with fistulas of the gastro-intestinal tract toparenteral nutrition. Surg Gynecol Obstet 1981; 153: 77-80.
3. Konturek SJ. Somatostatin and gastro-intestinal secretion and motility. Adv Exp MedBiol 1978; 106: 235-40.
4. René E, Reyl F, Bonfils S. Intérêt thérapeutique de la somatostatine en gastro-entérologie: Bases théoriques: Orientations pratiques. Gastroenterol Clin Biol 1980;4: 700-08.
Fistula output during TPN and TPN/somatostatin treatment.