
Pamela R, Hanson, DDS, MS To Distract or not Distract in the Surgical/Orthodontic · PDF...
14
Pamela R, Hanson, DDS, MS To Distract or not Distract in the Surgical/Orthodontic I. Definition of Distraction Osteogenesis a. Distraction osteogenesis is a process that results in new bone formation between the surfaces of bone segments gradually separated by incremental traction. b. The volume of soft tissue adjacent to the generating bone is also increased c. Histiogenesis i. occurs in different tissues: ii. bone, skin, fascia, blood vessels, nerves, muscle, ligament, cartilage & periosteum. Melugin MB, Hanson PR, Bergstrom CA, Schuckit WI, Gerald Bradley T. Soft tissue to hard tissue advancement ratios for mandibular elongation using distraction osteogenesis in children. Angle Orthod. 2006 Jan:76(1):72-6 II. Understanding Distraction Osteogenesis a. What it can and can’t do i. Can do: 1. Lengthen bones 2. Increase volume of bones 3- dimensionally 3. Increase the soft tissue envelope 4. Decrease relapse Linear distraction device (above)
Transcript of Pamela R, Hanson, DDS, MS To Distract or not Distract in the Surgical/Orthodontic · PDF...

PamelaR,Hanson,DDS,MSToDistractornotDistractintheSurgical/Orthodontic
I. DefinitionofDistractionOsteogenesisa. Distractionosteogenesisisaprocessthatresultsinnewbone
formationbetweenthesurfacesofbonesegmentsgraduallyseparatedbyincrementaltraction.
b. Thevolumeofsofttissueadjacenttothegeneratingboneisalso
increasedc. Histiogenesis
i. occursindifferenttissues:ii. bone,skin,fascia,bloodvessels,nerves,muscle,ligament,
cartilage&periosteum.Melugin MB, Hanson PR, Bergstrom CA, Schuckit WI, Gerald Bradley T. Soft tissue to hard tissue advancement ratios for mandibular elongation using distraction osteogenesis in children. Angle Orthod. 2006 Jan:76(1):72-6
II. UnderstandingDistractionOsteogenesisa. Whatitcanandcan’tdo
i. Cando:1. Lengthenbones2. Increasevolumeofbones3-dimensionally3. Increasethesofttissueenvelope4. Decreaserelapse
Lineardistractiondevice(above)

(below)3dimensionalvolumeincreaseofrightsideofdogmandiblefollowingdistractionutilizingtheabovelineardistractiondevice
imagesfrom:
KarpNS,etal.Membranousbonelengthening:aserialhistologicalstudy.AnnalsPlastSurg1992:29:2-7.
ii. Cannotdo:1. Makebonesshorter2. Makebonessmaller3. Movebonesbackwards
III. ToDistractornotdistractisthequestiona. ToDistract-Whentoconsiderdistractionasatreatmentmodality
i. Ifmagnitudeistoogreatforanyotherprocedureii. Iffunctiondemandsearlyand/orlargemagnitudecorrectioniii. IfstabilityisbetterwithDOiv. Ifitsetsupthepatientforamorestableandprecisedefinitive
procedureatskeletalmaturityv. Ifskilloftheteamcandeliveranexcellentresult
b. NottoDistract-Whendistractionisnottherecommendedoptioni. Ifmagnitudeisnotgreatandotherproceduresaremoreprecise.
ii. Ifskeletalcorrectionrequiredistoretropositionaboneordecreaseskeletalvolume
iii. Ifnofunctionaldeficitiv. Ifotherproceduresprovidegood/betterstabilityv. Ifskilloftheteamcannotdeliveranexcellentresult
1. Surgicalskill/experienceinadequate2. Skilledorthodontistunavailablefor:
a. Treatmentplanningb. Monitoringtheactivedistractionc. Manipulatingthedistalsegment
vi. IfapatientisincapableofcooperationIV. TeamEffortisrequiredtosuccessfullycompletedistraction

a. Diagnosisi. Identifyingthedeficiency
1. Skeletal2. Softtissue
ii. Identifylocationofthedeficiencyiii. Identifythedifferencesbetween:
1. Volumea. 3dimensionalvalue
2. Locationa. Advancingaskeletalstructure(A-P)b. Placingthedistalsegmentinaprecise
3dimensionallocationc. Verticallymanipulatingtheskeletalstructure
i. Improvesoverallresultii. ie:LeFortIIIadvancement
1. Improvesocclusion-ieclosesanterioropenbite
2. Increasesorbitalvolumeverticallybyloweringtheorbitalfloor
predistraction
postdistraction

predistraction
early distraction prior to orthopedic mgmt
late distraction during orthopedic mgmt
Hanson PR, Melugin MB: Orthopedic and Orthodontic Management of Distal Segment Position During Distraction Osteogenesis, Atlas of Oral and Maxillofacial Surgery Clinics of North America, Sept 2008, 16.2, pp 273-286.
b. Surgicalskilli. Accuracyincorticotomy/osteotomy
c. Deviceplacementi. Accuracyinplacementpositionii. Symmetry-ifbilateraldeviceplacementiii. Idealvectorestablished
d. Protocol-shouldbecarefullyfollowedtomaximizeoutcomei. Ilizarov-1949-1stprotocolwithlowmorbidity
1. Latencyperioda. 5-7dayspriortodeviceactivationb. Fibrovascularmatrixformation

2. Rate/rhythma. 1mm/dayb. 1mm/daycompletedbyseveralincrementsper
day3. Consolidation
a. Length-Roughlytwicetheofnumberofdaysofactivation
b. Whenradiographicevidenceofboneconsolidation
e. Activedistractioni. 1mm/day
f. Controlofdistractioniscruciali. Preparation
1. Treatmentplana. Determinefinalpositionofboneb. Determinemagnitudeofdesireddistractionin
mmc. Determinelengthofdistractiondeviceatleast2X
thatofthedesiredlengthofdistractioninmm2. Orthodonticpreparation
a. Anchoragei. Toprovidetheopportunitytomanipulatethedistalsegment
b. Distractionstabilizationappliancesi. Toprovidemultipleplacesforelastictraction
ii. ToprovidemaxillaryexpansionPRN
HansonPR,MeluginMB.Orthodonticmanagementofthepatientundergoingmandibulardistractionosteogenesis.SeminarsinOrthodontics.March1999:5(1):25-34.

g. Duringdistraction-controliscrucial
i. Activationofthedistractiondevice1. Millimetriclengthening-linear2. Devicemanipulationonlyifdevicesismultidirectional
ii. Forces/manipulationofthedistalsegment1. Elastictraction2. Maxillaryexpansion
h. Afterconsolidationi. Elastictractionii. Maxillaryexpansioniii. Occlusalplanecorrectionviaadjustedbiteblock(figurebelow)
1. Sequentialadjustmentofthebiteblocktopromotesequentialeruptionofthemaxillaryposteriorteeth
2. Closestheposterioropenbitecreatedbydistractionofthemandibletothedesiredverticalbysupereruptingthemaxillaryposteriorteethtocorrectthemaxillaryocclusalplaneandclosethedistractioncreatedopenbite.
IllustrationbyDrBarryGrayson
i. Requirementsi. Cooperationbythepatientcrucialii. Teamtreatment-control/forcescanbeplacedbysomeone
whowillassumethatrole1. Educatepatientandfamily2. Monitorcloselytheadvancing/evolvingdistraction
iii. Knowledge/experienceonhowtodiagnose,deliverforcesandmonitor
V. Parameterswhenconsideringdistractionasatreatmentoptiona. Magnitude
i. Determiningmagnitudehelpsdeterminethefollowing:1. Ifdistractionisthebestmodality
2. Devicetype3. Devicelength
b. Timingi. Timingbasedonfunctionalneedii. Timingbecausemagnitudesogreatasingledefinitive
procedurewouldnotbesuccessfuliii. Timingasthefirststeptoa2stepdefinitive
surgical/orthodonticplanc. Functionaldisordersthatdrivetiming
i. Airway,ii. Masticatoryfunction-Chewing/feedingiii. Speechiv. Facialappearancev. Psychosocialdevelopment
d. Therapeuticbenefite. MaxillaryDOafteralveolarcleftgraftasmaxillaissinglepiecepost
graftVI. UniquetoDistraction
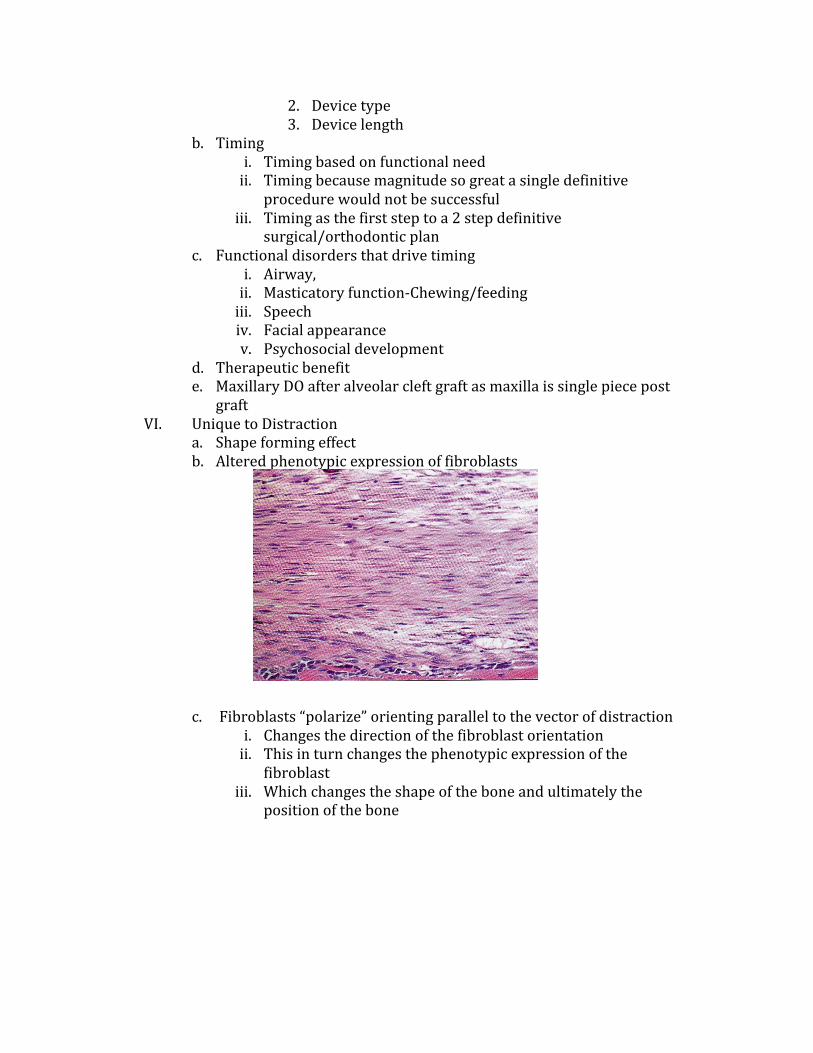
a. Shapeformingeffectb. Alteredphenotypicexpressionoffibroblasts
c. Fibroblasts“polarize”orientingparalleltothevectorofdistraction
i. Changesthedirectionofthefibroblastorientationii. Thisinturnchangesthephenotypicexpressionofthe
fibroblastiii. Whichchangestheshapeoftheboneandultimatelythe
positionofthebone

d. Forcesplacedonthedistalsegmentduringdistractione. TypesofforcesHansonPR,MeluginMB.Orthodonticmanagementofthepatientundergoingmandibulardistractionosteogenesis.SeminarsinOrthodontics.March1999:5(1):25-34.
i. Distractiondeviceactivationoralterationofamultidimensionaldistractiondevice

ii. Elastictraction
iii. Headgeariv. Expansionappliancesv. Distractionstabilizationappliances
VII. Maxillaryhypoplasiaa. LeFortIII/midfacedeficienciesb. LeFortI/maxillarydeficiencies
VIII. UnilateralMandibulardistractionIX. BilateralMandibulardistraction

PamelaR.Hanson,DDS,MSOrthodonticDirectorCleft&CraniofacialTeamsChildren’sHospitalofWisconsinSurgical/OrthodonticDirector,Div.ofOral&MaxillofacialSurgery,MedicalCollegeofWisconsinFaculty,MarquetteUniversitySchoolofDentistry,DepartmentofOrthodontics,DiplomatoftheAmericanBoardofOrthodontics.Citations:AAOToDistractorNotDistract
1. Abbot, L. C. The operative lengthening of the tibia and fibula. J. Bone Joint Surg. 9: 128, 1927.
2. Annino, D. J., Goguen, L. A., and Karmody, C. S. Distraction osteogenesis for reconstruction of mandibular symphyseal defects. Arch. Otolaryngol. Head Neck Surg. 120: 911, 1994.
3. Aronson, J., Good, B., Stewart, C., Harrison, B., and Harp, J. Preliminary studies of mineralization during distraction osteogenesis. Clin. Orthop. 250: 43, 1990
4. Aronson, J., Harrison, B., Boyd, C. M., Cannon, D. J.,Lubansky, H. J., and Stewart, C. Mechanical induction of osteogenesis: Preliminary studies. Ann. Clin. Lab. Sci. 18: 195, 1988.
5. Aronson, J., Harrison, B., Boyd, C. M., Cannon, D. J., and Lubansky, H. J. Mechanical induction of osteogenesis. J. Pediatr. Orthop. 8: 396, 1988.
6. Arnoson, J., and Shen, X. Experimental healing of distraction osteogenesis comparing metaphyseal with diaphyseal sites. Clin. Orthop. 301: 25, 1994.
7. Aro, H. Biomechanics of distraction. In J. G. McCarthy, (Ed.), Distraction of the Craniofacial Skeleton. New York: Springer-Verlag, 1999. Pp. 20-50.
8. Brighton, C. T., and Hunt, R. M. Early histological and ultrastructural changes in medullary fracture callus. J. Bone Joint Surg. (Am.) 73: 832, 1991.
9. Califacno, L., Cortese, A., Zupi, A., and Tajana, G. Mandibular lengthening by external distraction: An experimental study in the rabbit. J. Oral Maxillofac. Surg. 52: 1179, 1994.
10. Carls F, Sailer H. Seven years’ experience with mandibular distraction in children. J Craniomaxillofac Surg 1998;26:197Y208
11. Castero, H. J., and Salyer, K. E. Regenerative potential of bone and periosteum. Surg. Forum 26: 555, 1975.
12. Centrella, M., McCarthy, T. L., and Canalis, E. Current concepts review: Transforming growth factor beta and remodeling of bone. J. Bone Joint Surg. (Am.) 73: 1418, 1991.
13. Civelek B, Karamursel S, Ozdil K, et al. A potential complication with an extraoral distractor for mandible lengthening: facial nerve paralysis. Plast Reconstr Surg 2006;117:698Y699
14. Codvilla, A. On the means of lengthening in the lower limbs, the muscles and

tissue which are shortened through deformity. Am. J. Orthop. Surg. 2: 353, 1905. 15. Constantino, P. D., Shybut, G., Friedman, C. D., et al. Segmental mandibular
regeneration by distraction osteogenesis. Arch. Otolaryngol. Head Neck Surg. 116: 535,
16. Cope JB, Samchukov ML, Cherkashin AM. Mandibular distraction osteogenesis: a historic perspective and future directions. Am J Orthod Dentofacial Orthop 1999;115:448Y460
17. De Bastiani, G., Aldegheri, R., Enzi-Brivio, L., and Trivella, G. Limb lengthening by callus distraction (callotasis). J. Pediatr. Orthop. 7: 129, 1987.
18. Denny AD, Kalantarian B. HansonP. Rotational advancement of the Midface by Distraction Osteogenesis. Plastic & Reconstructive Surgery. 111(6):1800-1803, May 2003.
19. Figueroa AA, Polley JW, Friede H, Ko EW. Long-term skeletal stability after maxillary advancement with distraction osteogenesisusing a rigid external distraction device in cleft maxillary deformities.
20. Plast Reconstr Surg. 2004;114:1382–1392; discussion 1393
21. Fishgrund, J., Paley, D., and Suter, D. Variables affecting time to bone healing during limb lengthening. Clin. Orthop. 301: 31, 1994.
22. Freitas RD, Tolazzi AR, Alonso N, et al. Evaluation of molar teeth and buds in patients submitted to mandible distraction: long-term results. Plast Reconstr Surg 2008;121:1335Y1342
23. Fritz MA, Sidman JD. Distraction osteogenesis of the mandible. Curr Opin Otolaryngol Head Neck Surg 2004;12:513Y518 Master et al The Journal of Craniofacial Surgery & Volume 21, Number 5, September 2010.
24. Frost HM. Mechanical determinants of bone modeling. Metab Bone Dis Relat Res. 1982;4:217–229.
25. Gosain, A. K., Santoro, T. D., Song, L., Capel, C. C., Sudhakar, P. V., and Matloub, H. S. Osteogenesis in calvarial defects: Contribution of the dura, the pericranium, and the surrounding bone in adult versus infant animals. Plast. Reconstr. Surg. 112: 515, 2003.
26. Grayson BH, Santiago PE. Treatment planning and biomechanics of distraction osteogenesis from an orthodontic perspective. Semin Orthod 1999;5:9Y24
27. Grayson BH, McCormick S, Santiago PE, et al. Vector of device placement and trajectory of mandibular distraction. J Craniofac Surg 1997;8:473Y480
28. Guichet, J. M., Braillon, P., Bondenreider, O., and Lascombes, P. Periosteum and bone marrow in bone lengthening: A DEXA quantitative evaluation in rabbits. Acta Orthop. Scand. 69: 527, 1998.
29. Gursoy S, Hukki J, Hurmerinta K. Five year follow-up of mandibular distraction osteogenesis on the dentofacial structures of syndromic children. Orthod Craniofac Res 2008;11:57Y64
30. Hanson PR, Melugin MB. Orthodontic management of the patient undergoing mandibular distraction osteogenesis. Semin Orthod 1999;5:25Y34
31. Hanson PR, Melugin MB: Orthopedic and Orthodontic Management of Distal Segment Position During Distraction Osteogenesis, Atlas of Oral and Maxillofacial Surgery Clinics of North America, Sept 2008, 16.2, pp 273-286.

32. Hettinger P, Hanson P, Denny A, Le Fort III Distraction Using Rotation Advancement of the Midface in Patients with Cleft Lip and Palate. Plast Reconstr Surg 2013: 1532-1541.
33. Hollier LH, Kim JH, Grayson B, et al. Mandibular growth after distraction in patients under 48 months of age. Plast Reconstr Surg 1999;103:1361Y1370
34. Hurmerinta K, Hukki J. The vector control in lower jaw distraction osteogenesis using an extraoral multidirectional device. J Craniomaxillofac Surg 2001;29:263Y270
35. Ilizarov, G. A. The principles of the Ilizarov method. Bull. Hosp. J. Dis. Orthop. Inst. 48: 1, 1988.
36. Ilizarov, G. A. The tension-stress on the genesis and growth of tissue: Part I. The influence of stability of fixation and soft tissue preservation. Clin. Orthop. 238: 249, 1989.
37. Ilizarov, G. A. The tension-stress effect on the genesis and growth of tissue: Part II. The influence of rate and frequency of distraction. Clin. Orthop . 239: 263, 1989.
38. Illizarov, G. A., and Deviatov, A. A. Surgical elongation of the leg. Ortop. Travmatol. Protez. 32: 20, 1971.
39. Illizarov, G. A., Ledyaev, V. I., and Shitin, V. P. Experimental studies of bone lengthening. Exp. Khir. Anesth. 14: 3, 1969.
40. Karaharju-Suvanto T, Peltonen J, Ranta R, et al. The effect of gradual distraction on the mandible on the sheep temporomandibular joint. Br J Oral Maxillofac Surg 1996;25:152Y156
41. Karaharju-Suvanto, T., Peltonen, J., Kahri, A., and Karaharju, E. O. Distraction osteogenesis of the mandible: An experimental study on sheep. Int. J. Oral Maxillofac.
42. Karp, N. S., McCarthy, J. G., Schreiber, J. S., Sissons, H. A., and Thorne, C. H. Membranous bone lengthening:A serial histologic study. Ann. Plast. Surg. 29: 2, 1992.
43. Karp, N. S., Thorne, C. H. M., McCarthy, J. G., and Sissons, H. A. Bone lengthening in the craniofacial skeleton. Ann. Plast. Surg. 24: 231, 1990
44. Knize, D. M. The influence of periosteum and calcitonin on onlay bone graft survival. Plast. Reconstr. Surg. 53: 190, 1974.
45. Kojimoto, H., Yasui, N., Goto, T., Mastuda, S., and Shimomura, Y. Bone lengthening in rabbits by callus distraction. J. Bone Joint Surg. (Br.) 70: 543, 1988.
46. Komori E, Sagara N, Aigase K. A method for evaluating skeletal relapsing force during maxillomandibular fixation after orthognathic surgery: a preliminary report. Am J Orthod Dentofacial Orthop 1991;100:38Y46
47. Massague, J. The transforming growth factor-beta family. Annu. Rev. Cell Biol. 6: 597, 1990
48. McCarthy JG, Schreiber J, Karp N, et al. Lengthening of the human mandible by gradual distraction. Plast Reconstr Surg 1992;89:1Y8
49. McCarthy JG, Katzen T, Hopper R, et al The first decade of mandibular distraction: lessons we have learned. Plast Reconstr Surg 2002;110:1704Y1713
50. McCarthy JG. The role of distraction osteogenesis in the reconstruction of the

mandible in unilateral craniofacial microsomia. Clin Plast Surg 1994;21:625Y631 51. McCarthy JG, Stelnicki EJ, Mehrara BJ, et al. Distraction osteogenesis of the
craniofacial skeleton. Plast Reconstr Surg 2001;107:1812Y1827 52. McCarthy JG, Grayson BH, Williams JK, et al. Distraction of the mandible: the
New York University experience. In: McCarthy J, ed. Distraction of the Craniofacial Skeleton. Berlin, Germany: Springer, 1999:80Y203
53. Melugin MB, Hanson PR, Bergstrom CA, Schuckit WI, Gerald Bradle T. Soft tissue to hard tissue advancement ratios for mandibular elongation using distraction osteogenesis in children. Angle Orthod. 2006 Jan:76(1):72-6.
54. Michieli, S., and Miotti, B. Controlled gradual lengthening of the mandible after osteotomy. Minerva Stomatol. 25: 77, 1976. Mofid MM, Manson PN, Robertson BC, et al. Craniofacial distraction osteogenesis: a review of 3278 cases. Plast Reconstr Surg 2001;108:1103Y1114
55. Mofid, MM, Manson PN, Robertson BC, Tufaro AP, Elias JJ, Vander Kilk CA. Craniofacial distraction osteogenesis: A review of 3278 cases. Plast. Reconstr. Surg. 2001: 108:1103.
56. Munro IR. One-stage reconstruction of the temporomandibular joint in hemifacial microsomia. Plast Reconstr Surg 1980;66:699Y710
57. Owen, M. The origin of bone cells in the postnatal organism. Arthritis Rheum. 23: 1073, 1980.
58. Owen, M. Cell population kinetics of an osteogenic tissue. J. Cell Biol. 19: 19, 1963
59. Paley, D. Problems, obstacles and complications of limb lengthening by Ilizarov technique. Clin. Orthop. 250:81, 1990.
60. Schendel SA, Epker BN. Results after mandibular advancement surgery: an analysis of 87 cases. J Oral Surg 1980;38:265Y282
61. Shetye PR, Warren SM, Brown D, et al. Documentation of the incidents associated with mandibular distraction: introduction of a new stratification system. Plast Reconstr Surg 2009;123:627Y634
62. Skoog, T. The use of periosteal flaps in the repair of clefts of the primary palate. Cleft Palate J. 2: 332, 1965.
63. Snyder, C. C., Levine, G. A., Swanson, H. M., and Browne, E. Z. Mandibular lengthening by gradual distraction. Plast. Reconstr. Surg. 5: 506, 1973.
64. Sproul, J. T., and Price, C. T. Recent advances in limb lengthening: Part II. Biological advances. Orthop. Rev. 21: 425, 1992.
65. Swennen G, Schliephake H, Dempf R, et al. Craniofacial distraction osteogenesis: a review of the literature. Part 1: clinical studies. Int J Oral Maxillofac Surg 2001;30:89Y103
66. Thompson, N., and Casson, J. A. Experimental onlay bone grafts to the jaws. Plast. Reconstr. Surg. 46: 341, 1970. 1498 PLASTIC AND RECONSTRUCTIVE SURGERY, November 2004
67. Tonna, E. A., and Cronkite, E. P. Autoradiographic studies of cell proliferation in the periosteum of intact and fractured femora of mice utilizing DNA labeling with 3H-thymidine. Proc. Soc. Exp. Biol. Med. 107: 719, 1961.
68. Toth BA, Kim JW, Chin M, Cedars M. Distraction osteogenesis and its application to the midface and bony orbit in craniosynostosis syndromes. J

Craniofac Surg. 1998;9:100–113; discussion 119. 69. Uckan S, Veziroglu F, Arman A. Unexpected breakage of mandibular midline
distraction device: case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod 2006: 102:e21-e25.
70. Van Sickels JE, Richardson RA. Stability of orthognathic surgery: a review of rigid fixation. Br J Oral Maxillofac Surg 1996;34: 279Y285
71. Van Strijen PJ, Breuning KH, Becking AG, et al. Stability after distraction osteogenesis to lengthen the mandible: results in 50 patients. J Oral Maxillofac Surg 2004;62:304Y307
72. White, S. H., and Kenwright, J. The timing of distraction of an osteotomy. J. Bone Joint Surg. (Br.) 72: 356,1990.
73. White, S. H., and Kenwright, J. The importance of delay in distraction of osteotomies. Orthop. Clin. North Am. 22: 569, 1991.











![Surgical Orthodontic Treatment of Severe Class Iii and ... · of orthopedic appliances, dentoalveolar compensation (orthodontic camouflage) and orthodontic-surgical treatment [4].](https://static.fdocuments.us/doc/165x107/5d50636588c993dd738b51d7/surgical-orthodontic-treatment-of-severe-class-iii-and-of-orthopedic-appliances.jpg)






