
PALS, Complaints, Claims and Incidents Annual Report 2016-17 · concerns investigated through PALS...
30
Kingston Hospital NHS Foundation Trust – Trust Board – July 2017 1 PALS, Complaints, Claims and Incidents Annual Report 2016-17 Trust Board Item: 19 Date: 26 th July 2017 Enclosure: M Purpose of the Report: Provide the annual review of the Patient, Advice and Liaison Service (PALS) contacts, complaints, compliments, claims, inquests and incidents (including serious incidents (SIs)) that occurred during 2016/17. Identify any themes and trends across these areas and over time. For: Information Assurance Discussion and input Decision/approval Sponsor (Executive Lead): Duncan Burton Director of Nursing and Quality Authors: Alison Vizulis, Head of Quality Governance and Risk Clare Parker, Head of Litigation, Complaints and PALs Alannah Hayes, Quality Improvement Lead for Patient Safety Author Contact Details: Ext 3846 [email protected] Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to Relevant Corporate Objective: Strategic Objective 1: to deliver quality, patient centred healthcare services with and an excellent reputation. Document Previously Considered By: Recommendations: The Trust Board is asked to note the annual report.
Transcript of PALS, Complaints, Claims and Incidents Annual Report 2016-17 · concerns investigated through PALS...

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
1
PALS, Complaints, Claims and Incidents Annual Report 2016-17
Trust Board Item: 19
Date: 26th July 2017 Enclosure: M
Purpose of the Report:
Provide the annual review of the Patient, Advice and Liaison Service (PALS) contacts, complaints, compliments, claims, inquests and incidents (including serious incidents (SIs)) that occurred during 2016/17.
Identify any themes and trends across these areas and over time.
For: Information Assurance Discussion and input Decision/approval
Sponsor (Executive Lead):
Duncan Burton Director of Nursing and Quality
Authors:
Alison Vizulis, Head of Quality Governance and Risk Clare Parker, Head of Litigation, Complaints and PALs Alannah Hayes, Quality Improvement Lead for Patient Safety
Author Contact Details:
Ext 3846 [email protected]
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led
Link to Relevant Corporate Objective:
Strategic Objective 1: to deliver quality, patient centred healthcare services with and an excellent reputation.
Document Previously Considered By:
Recommendations: The Trust Board is asked to note the annual report.
Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
2
PALS, Complaints, Claims and Incidents Annual Report 2016-17

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
3
No. Content Page No.
Executive Summary 4
1 Introduction 4
2 Govenance and Assurance 4
3 Patient Advice and Liaison Services (PALS) 5
3.1 – Types of PALS concerns 6
3.2 – Actions in response to PALS concerns 7
4 Complaints 8
4.1 - Types of Complaints 8
4.2 - Actions in Response to Complaints 10
4.3 - Next stage of Complaints 11
5 Claims 11
5.1 - Claims Process 11
5.2 - NHSR and Benchmarking 11
5.3 - Claims Data 11
5.4 - NHSR predictions for 2016/17 12
5.5 - Themes 12
5.6 - Specialities 13
5.7 - Outcomes 13
5.8 - NHSR Contributions 14
5.9 - Actions following Claims 14
6 Inquests 14
7 Compliments 15
7.1 - How are compliments received and managed 15
7.2 - Key Themes 15
8 Incidents 17
8.1 - Incident reporting 17
8.2 - National Reporting and Learning System (NRLS) Benchmarking 17
8.3 - Incident Types 18
8.4 - Patient Safety Incidents: Indentified trends and key points to note. 19
8.4.1 - Falls 19
8.4.2 - Medication 20
8.4.3 - Pressure Ulcers 20
8.5 - Post incident actions 20
8.6 Staff Incidents 21
8.6.1 - Staff incident categories 21
8.6.2 - Post incident actions 22
9. Serious Incidents 22
9.1 - Serious Incident (SI) management process 23
9.2 - Tracking of action plans 23
9.3 - Investigation Training 23
9.4 - Number and category of Serious Incidents (compared to incidents occurring in 2015/16
24
9.5 - Serious Incident (SI) themes and trends analysis 25
9.6 - Never Events 27
9.6.1 - Actions taken as a result of Serious Incident and Never Event investigations
27
9 Duty of Candour 28
10 Triangulation 28
Conclusion 29

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
4
Executive Summary This Annual report provides an overview of the, Patient Advice and Liaison Service (PALS) contacts, complaints, compliments, claims, inquests and incidents (including serious incidents (SIs) that occurred during 2016-17. Headlines from 2016-17
1470 PALS contacts logged, compared to 1579 during 2015/16.
390 formal complaints were received, which is a 16% reduction compared to 2015/16, when 465 were reported.
The response to complaints within 25 working days timeframe was met in 80% of complaints, compared to 82% in 2015/16, which is a very slight decrease.
80 new claims, (69 clinical and 11 non-clinical), occurred compared to 85 in 2015/16.
No Prevention of Future Death’ reports (PFD) were issued from the coroner during 2016/17.
Compliments are being collated and reported to the Patient Experience Committee.
In total 6824 incidents were reported, compared to 6029 in 2015/16 – A 13% increase, building on the 6% increase of 2015/16.
There were 44 serious incidents reported during 2016/17. In 2015-16, 40 had been reported, with 57 in 2014-15.
Only 2.7% of patient safety incidents involved more than minor harm – This is similar to the national average of 2.6% (for the period of April – September 2016).
There has been a significant decline in hospital acquired pressure ulcers.
There was a decrease in the number of reported falls in 2016/17, as 697 were reported, as opposed to 774 for 2015-16.
Common themes from issues staff and patients are reporting are: Communication, appointments, care/treatment and medication.
1. Introduction The Trust has well established systems and processes in place for (PALS) contacts, complaints, compliments, claims, inquests and incidents. The purpose of this report is to summarise activity for the period 2016-17 and identify any themes and trends across these areas and over time. By looking at activity and trends in these areas the Trust can take an informed approach to further developing and improving patient safety and patient experience. Going forward, one of the aims of the 2017/18 report will be to triangulate the findings arising from the incidents, claims, PALS and complaints themes against the Service Line Risk Registers, and the Corporate Risk Register.
2. Governance and Assurance The Quality Assurance Committee (QAC) receives information on all areas of concern, and assurance on the actions that are being taken to address quality of care which falls below expected standards. To strengthen this triangulation, complaints reporting is also feeding into QAC rather than have a separate complaints committee. In addition, information on incidents is also discussed at the Clinical Quality Improvement Committee and Mediation Safety Committee. Complaints and Compliments are also shared with the Patient Experience Committee. The Trust has a weekly Serious Incident Group. The Quality Assurance Committee receives annual claims reports. During this period the following improvements and progress have been achieved:
Improvement work as part of our Sign up to Safety pledges has continued, including the development and implementation of mechanisms to support the prevention and reduction of pressure ulcers, implementation of Year 2 of the Trusts Sign up to Safety Sepsis response,

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
5
and continued work on introducing intrapartum fetal wellbeing assessment and management in high risk pregnancy.
A new Multifactorial Falls Risk assessment incorporating the 7 key recommendations from NICE Clinical Guideline 161 has been piloted and is now being embedded across the Trust. The Trust has also completed the key recommendations from the National Inpatient Falls Audit.
Further work to embed the WHO checklist including regular audit.
Development of a new Pressure Area Support Team (PAST) to assist in areas where numbers of pressure ulcers have developed with the aim of early identification and implementation of actions.
The Trust has continued to achieve all cancer targets in 2016/17, and in quarter 3, we were reported as the best performing trust for the 62 day target in the country as well as the highest performing trust in London for the 62 day standard in January 2017. The trust has consistently achieved 10% higher than the reported national and local cancer performance against the 62 day standard.
Continued embedding of the Trusts Risk Management software and governance processes.
The Serious Incident Group has continued to monitor actions arising from Root Cause Analysis Reports, and identify key learning from SI’s with learning being cascaded to service lines.
Learning identified from our reported incidents and investigations is also utilised by our Clinical Quality Improvement Committee to help to inform our quality improvement projects.
Staff are also given email feedback after reporting incidents and an investigation has been closed.
There has been a sustained focus from the complaints team to support services to reduce complaint response times.
Appointment of additional staff to ensure a seven day face to face palliative care service on site.
3. Patient Advice and Liaison Services (PALS) PALS provide information and help to resolve concerns that a patient or their family/carer may have. The team aims to resolve problems and concerns quickly in order to prevent them escalating into a complaint. The team works hard to ensure that investigations are thorough, and that the outcomes reflect the seriousness of the issues that patients and their relatives or carers have raised. Concerns received from, or on behalf of, patients in no way prejudice how they are treated, and are seen as valuable information to help improve services for patients and carers. The overwhelming majority of concerns investigated through PALS are resolved without escalation to the formal complaints process. The PALS service remained busy throughout 2016/17, with 1470 contacts being logged which provided useful information on themes and trends. The areas that feature most prominently are car parking, Radiology administration, the Royal Eye Unit office, followed by Accident & Emergency and the General Surgery office.
Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
6
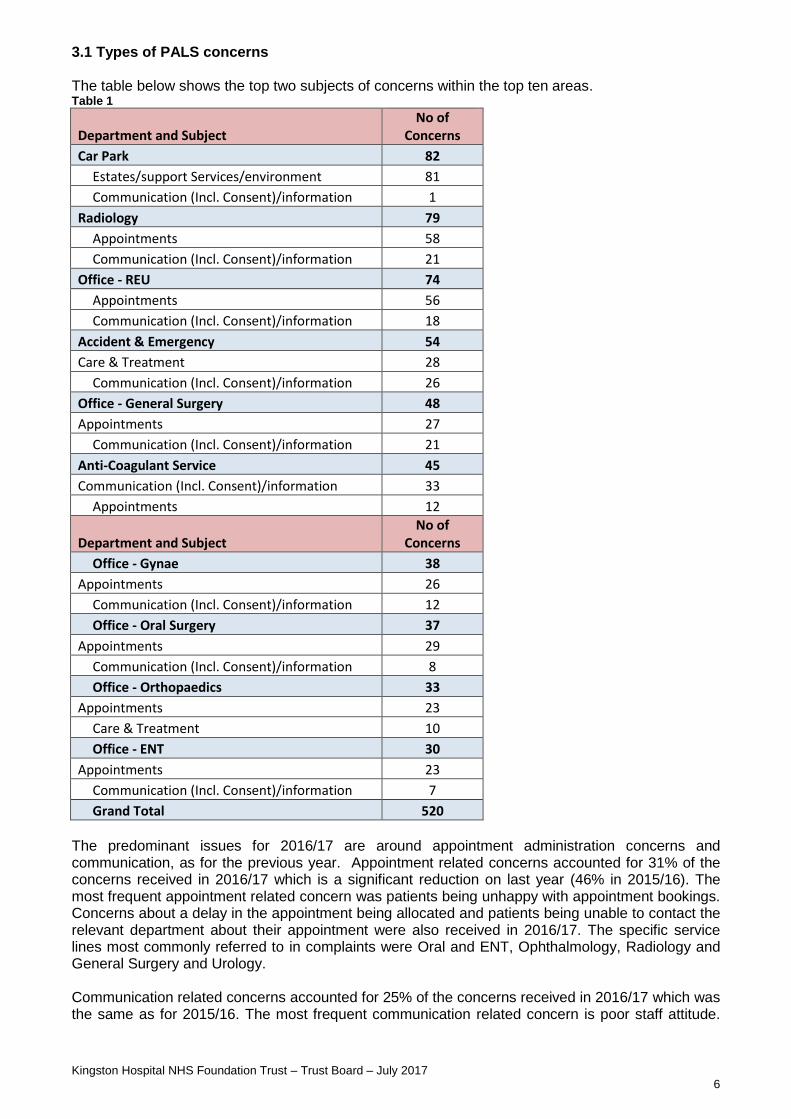
3.1 Types of PALS concerns The table below shows the top two subjects of concerns within the top ten areas. Table 1
Department and Subject No of
Concerns
Car Park 82
Estates/support Services/environment 81
Communication (Incl. Consent)/information 1
Radiology 79
Appointments 58
Communication (Incl. Consent)/information 21
Office - REU 74
Appointments 56
Communication (Incl. Consent)/information 18
Accident & Emergency 54
Care & Treatment 28
Communication (Incl. Consent)/information 26
Office - General Surgery 48
Appointments 27
Communication (Incl. Consent)/information 21
Anti-Coagulant Service 45
Communication (Incl. Consent)/information 33
Appointments 12
Department and Subject No of
Concerns
Office - Gynae 38
Appointments 26
Communication (Incl. Consent)/information 12
Office - Oral Surgery 37
Appointments 29
Communication (Incl. Consent)/information 8
Office - Orthopaedics 33
Appointments 23
Care & Treatment 10
Office - ENT 30
Appointments 23
Communication (Incl. Consent)/information 7
Grand Total 520
The predominant issues for 2016/17 are around appointment administration concerns and communication, as for the previous year. Appointment related concerns accounted for 31% of the concerns received in 2016/17 which is a significant reduction on last year (46% in 2015/16). The most frequent appointment related concern was patients being unhappy with appointment bookings. Concerns about a delay in the appointment being allocated and patients being unable to contact the relevant department about their appointment were also received in 2016/17. The specific service lines most commonly referred to in complaints were Oral and ENT, Ophthalmology, Radiology and General Surgery and Urology. Communication related concerns accounted for 25% of the concerns received in 2016/17 which was the same as for 2015/16. The most frequent communication related concern is poor staff attitude.

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
7
Subject and Department 2016/17 Total for Top 10 Departments Performance Grand Total
Appointments 305 463
Radiology 58
Office - REU 56
Office - Oral Surgery 29
Office - General Surgery 27
Office - Gynae 26
Office - ENT 23
Office - Orthopaedics 23
Office - Neurology 23
Office - Dermatology & Plastics 22
Office - Urology 18
Communication (Incl. Consent)/information 187 370
Anti-Coagulant Service 33
Accident & Emergency 26
Radiology 21
Office - General Surgery 21
Office - REU 18
Acute Assessment Unit 12
Office - Gynae 12
Office - Cardiology 8
Office - Oral Surgery 8
Office - Dermatology & Plastics 7
Office - Urology 7
Office - ENT 7
Office - Neurology 7
Concerns about a patient being unable to contact a particular service, general poor communication with the patient, relative or carer were also received. Trust administration staff were the most frequently cited staff group followed by, and to a lesser degree, nursing then medical staff. The departments with the most communication issues were the Anti-Coagulant Clinic, A&E, Radiology, General Surgery and the Royal Eye Unit offices. 3.2 Actions in response to PALS concerns Examples of actions taken as a result of concerns raised by patients through PALS were:
improvements throughout the service lines in terms of better access to appointment administration staff who can help with appointment queries;
changes made to appointment letters that are sent to patients, to provide greater clarity and contact details;
there has been an increase in administrative staff within the Royal Eye Unit and more training has taken place on how to escalate patient concerns appropriately within the REU;
there is ongoing recruitment to vacant appointment booking posts in Radiology which improves patients’ ability to contact the area.
Table 2, overleaf, demonstrates the top two areas experiencing the most concerns raised through PALs. The table highlights that there has been a significant drop in the number of concerns raised that were associated with appointments when compared to 2015/16. There was a reduction for the communication related PALs concerns in the Anticoagulation Service, and increases in seven other Departments, including A&E and Radiology when compared to the previous year. Table 2

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
8
represents a decrease in number of concerns when compared to 2015/16
represents an increase in number of concerns when compared to 2015/16
represents no change in numbers
4. Complaints The Trust is committed to learning from any complaint received, and considerable focus is placed upon this aspect of the complaints process. The Complaints team ensure that all complaints are robustly investigated and that, where action is needed to improve the care or service a patient receives, this is reflected in the complaint response. The service lines have systems in place to ensure they make such changes in a timely way, to improve the experience of future patients, and complaints are discussed at Service Line business and governance meetings.
Every reasonable effort is made to resolve complaints at a local level (i.e. within the Trust) and this involves correspondence and meetings with complainants. In 2016/2017, the Trust received 390 formal complaints compared to 465 received in 2015/2016 – this is reduction of 16%, against a back drop of increased activity during 2016/2017.
In 2016/2017, 36 complaints related to car parking, compared to 19 in 2015/16. This was the only area where there was a significant increase in complaints.
The Trust recognises that swift action in responding to complaints is key to resolving them. As such, we endeavour to respond within 25 working days to all complaints, or by the timeframe agreed with the complainant. During 2016/17, this deadline was met in 313 complaints. The 25 day compliance rate was 80%, compared to 82% in 2015/16. Work is ongoing to improve this response rate. Nationally, it is recognised that complaints have become more complex as services have expanded and there is more cross over with other local healthcare providers. Complaints may highlight a need to change a practice or improve a service in an individual area. When identified, a change in practice will be implemented to avoid recurrence. Individual complaints (in an anonymised format) are used in training at all levels and for all staff. Complaints, and the actions that arise from them, are discussed and scrutinised at a number of committees including the Quality Assurance Committee, the Clinical Quality Review Group, the Learning Disability Group, and the Patient Experience Committee. Complainants’ stories are shared with the Trust Board at every meeting.
4.1 Types of Complaints The most commonly complained about issues are communication, care and treatment, appointments, car parking and diagnosis. The areas that attracted the highest level of complaints in 2016/17 are reflected in the table below (Table 3).

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
9
** Due to a change in structure of Service Lines in 2015/16, it is not possible to present the data by Service Line. When comparing 2015/16 to 2016/17, complaints received by the Orthopaedics Department have decreased by 70%, Dermatology and Plastics by 42% and Acute Assessment Unit by 28%. Areas that have seen an increase in complaints in 2016-17 are car parking, ENT, and General Surgery. Half the complaints received by the ENT Department related to communication issues. Other complaints included issues such as appointments, care and treatment, and procedure. General Surgery received a number of procedure, communication and appointments related complaints. A small number of complaints related to issues such as care and treatment, diagnosis and documentation. The following table (Table 4) shows the top ten areas by top subjects of complaints. Table 4
Department and Top Subject No of Complaints
2016/17
Car Park 36
Estates/support Services/environment 36
Accident & Emergency 17
Care & Treatment 17
Office - Dermatology & Plastics 8
Appointments 8
Office - REU 7
Appointments 7
Office - ENT 6
Communication (Incl. Consent)/information 3
Appointments 3
OPD - Orthopaedics 5
Care & Treatment 5
Royal Eye Unit - OPD 5
Appointments 5
OPD - General Surgery 4
Procedure (Incl. Surgery/endoscopy/anaesthesia Etc) 4
Office - Neurology 4
Appointments 4
Acute Assessment Unit 4
Admission/discharge 4 From a ward perspective, the wards that attracted the most complaints in 2016/17 were the Acute Assessment Unit (The largest ward with the highest throughput) (n=13, largely admission/discharge), Astor Ward (n=9, care and treatment and admission/discharge) and Kennet
Top 10 Departments 2015-16 2016-17 Performance
Accident & Emergency 67 69
Car Park 19 36
Royal Eye Unit 27 22
Dermatology & Plastics 26 15
General Surgery 10 14
Acute Assessment Unit 18 13
Neurology 10 11
ENT 6 10
Orthopaedics 20 6
Antenatal Clinic 6 6
Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
10
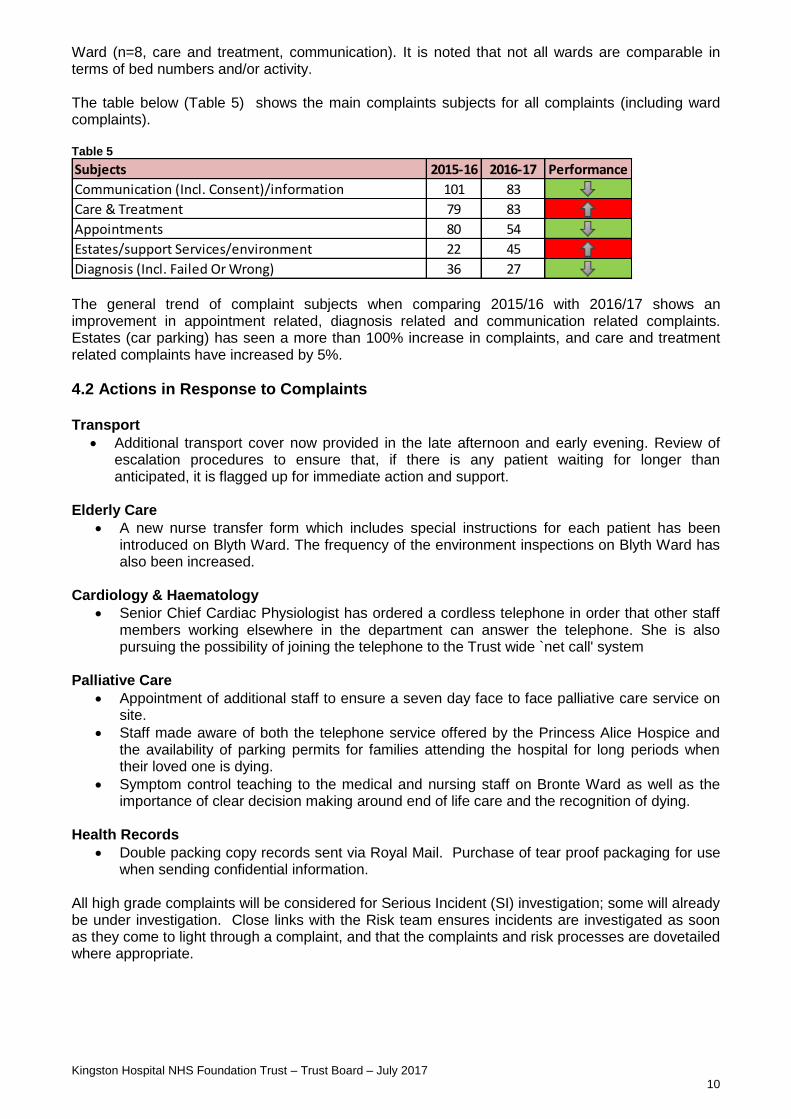
Ward (n=8, care and treatment, communication). It is noted that not all wards are comparable in terms of bed numbers and/or activity. The table below (Table 5) shows the main complaints subjects for all complaints (including ward complaints). Table 5
The general trend of complaint subjects when comparing 2015/16 with 2016/17 shows an improvement in appointment related, diagnosis related and communication related complaints. Estates (car parking) has seen a more than 100% increase in complaints, and care and treatment related complaints have increased by 5%.
4.2 Actions in Response to Complaints Transport
Additional transport cover now provided in the late afternoon and early evening. Review of escalation procedures to ensure that, if there is any patient waiting for longer than anticipated, it is flagged up for immediate action and support.
Elderly Care
A new nurse transfer form which includes special instructions for each patient has been introduced on Blyth Ward. The frequency of the environment inspections on Blyth Ward has also been increased.
Cardiology & Haematology
Senior Chief Cardiac Physiologist has ordered a cordless telephone in order that other staff members working elsewhere in the department can answer the telephone. She is also pursuing the possibility of joining the telephone to the Trust wide `net call' system
Palliative Care
Appointment of additional staff to ensure a seven day face to face palliative care service on site.
Staff made aware of both the telephone service offered by the Princess Alice Hospice and the availability of parking permits for families attending the hospital for long periods when their loved one is dying.
Symptom control teaching to the medical and nursing staff on Bronte Ward as well as the importance of clear decision making around end of life care and the recognition of dying.
Health Records
Double packing copy records sent via Royal Mail. Purchase of tear proof packaging for use when sending confidential information.
All high grade complaints will be considered for Serious Incident (SI) investigation; some will already be under investigation. Close links with the Risk team ensures incidents are investigated as soon as they come to light through a complaint, and that the complaints and risk processes are dovetailed where appropriate.
Subjects 2015-16 2016-17 Performance
Communication (Incl. Consent)/information 101 83
Care & Treatment 79 83
Appointments 80 54
Estates/support Services/environment 22 45
Diagnosis (Incl. Failed Or Wrong) 36 27

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
11
4.3 Next Stage of Complaints Once local resolution has been exhausted, complainants can refer any outstanding concerns to the Parliamentary Health Service Ombudsman, where an assessor will review the subject of the complaint and the complaint investigation. Nationally, there has been a significant increase in the number of cases that the Ombudsman is investigating, with a significantly lower threshold to investigate now in place. In 2016/17, five complaints were taken to the Ombudsman by complainants. Two were partially upheld (one is currently being challenged by the Trust), one was not upheld and the remaining are pending response from the Ombudsman. This low rate is a positive endorsement of our complaints process.
5. Claims Claims Overview This section of the report provides information on clinical negligence, public and employer liability cases which the Trust has received during the financial year. Certain benchmarking information is not available from the NHSR (NHS Resolution – formerly the NHSLA which changed its name in April 2017) and forecasting is calculated from historical figures with reference to quantified trends. 5.1 Claims Process Claims are managed via specific Ministry of Justice protocols concerning the disclosure and timeframes relating to the administration of each particular type of case. The Claims Department follows a strict programme of identifying disclosable data utilising Health Records, CRS, Winpath, Ulysses, Radiology, Complaints, clinicians’ comments, SI/RCA reports and archived information pertinent to each case. Claims are then managed in collaboration with the NHSR and if required, panel solicitors. 5.2 NHSR and Benchmarking In relation to benchmarking the claims received, the NHSR analyses and compares data from all similar Trusts throughout England (size, specialities, demographics, etc). This data is averaged out to reveal a specific category called ‘Member Type’. The Trust is then compared to this Member Type so that our position can be reviewed in relation to cases, claims performance and specialities. Currently, the benchmarking data supplied by the NHSR is limited. For example, information such as the subject of the claim is not available, but will possibly be included in their data set for late 2018. 5.3 Claims Data
In relation to the management of claims, the Trust is performing with better than average timeframes concerning a notification to resolution period of 3.5 years (average timeframe is 4.3 years) and a level of cases closed without damages of 50%. The time from notification to resolution is affected by the specific type of claim; for example Obstetric claims take considerably longer to complete than claims relating to other specialties. Over the financial year period, the Trust has received 80 new cases (69 clinical and 11 non-clinical) and has closed 35 cases received over previous years. There are currently 340 open claims within the database. This is a marked increase over last year due to a general cumulative effect of Obstetrics cases (in line with NHSR data) and a 50% reduction

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
12
in claim closures over this period. In general, the new case load is slightly lower than the previous financial year (2015/2016 was 85 cases). 5.4 NHSR predictions for 2016/17 The NHSR had predicted a general 17% national increase in active claims for this financial period. Our current figures accurately reflect the statistics with a 17.6% growth in total active cases from 289 to 340.
Period
Claims Period Claims
2010/11 42 cases 2014/15 82 cases
2011/12 62 cases 2015/16 85 cases
2012/13 66 cases 2016/17 80 cases
2013/14 76 cases
5.5 Themes
The top subjects for cases within this period are:
1. Treatment/procedure inappropriate in 19 cases 2. Delay in diagnosis in 11 cases 3. Delay in treatment in 9 cases 4. Failure in referral process in 9 cases 5. Diagnosis missed on first presentation in 4 cases
NB – There can be more than one subject theme in a case. At present, there is no NHSR benchmarking relating to themes.
Top 5 subjects
Treatment procedure
inappropriate
Delay in diagnosis
Delay in treatment
Failure in referral process
Diagnosis missed on first presentation
3
0
6
9
12
15
18

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
13
5.6 Specialities
The specialities receiving the most new clinical claims in 2016/17 are as follows:
1. Obstetrics with 17 cases 2. Accident and Emergency with 12 cases 3. Orthopaedics with 12 cases 4. General Medicine with 10 cases 5. Urology with 4 cases
This list generally reflects claims that occurred during 2015/16. Within Obstetrics and Orthopaedics, the most common theme was inappropriate treatment/procedure. Within A&E, a delay in treatment and delay in diagnosis are jointly common subject themes. Surgical complications and diagnostic issues are the basis of the majority of the Orthopaedic claims received, also leading to a general theme of inappropriate treatment/procedure. Obstetrics cases comprise of allegations mainly concerning CTG monitoring, use of Syntocinon, delay in senior Obstetric input and infection. 5.7 Outcomes During 2016/17, 35 cases were closed. They comprised of 15 settled, 8 challenged and withdrawn, 5 defended, 5 simply withdrawn without challenge and 2 closed via lack of response. A robust stance is maintained in relation to closing cases where possible. Closing cases as quickly as possible (where there is lack of merit or weak allegations) significantly reduces claimant solicitors’ costs which are second only to damages, in relation to NHSR expenditure. This process helps in the fight against NHSR contributions.
5.8 NHSR Contributions Every year, the Trust makes a calculated payment to the NHSR in order to maintain clinical negligence scheme cover. This cover protects the Trust in relation to all damages and the majority of costs pertaining to clinical cases. The general basis for calculating this contribution takes into account the number of clinical staff employed, number of patient episodes, historical claims data and claims risk by speciality.
Specialities with most cases 21 18 15 12 9 6 3
Obstetrics Orthopaedics A&E Gen. Medicine Urology

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
14
From information provided by the NHSR, the Trust’s contributions for CNST will increase from £6.4 million (2016/2017) to £8.9 million for the new 2017/18 period. This is a sizable increase which is reflected nationwide and is based on a general trend towards higher case numbers, damages and costs, especially within Obstetrics cases. 5.9 Actions following Claims A crucial part of the claims process is the action taken in relation to the learning from claims. This helps to mitigate risk and reduce future harm to patients. Historically, recommendations of actions were provided independently from panel solicitors or the NHSR on cases which presented a high risk. This no longer happens, and Trusts are now expected to monitor their own recommendations and evidence the actions taken. Commonly, action has been taken at around the time of the incident leading to the claim; particularly, when the incident has been the subject of a risk investigation. The claims process provides a further opportunity to consider whether additional action needs to be taken when the incident is reviewed during the claims process.
6. Inquests
The volume of inquest related work continues to grow in line with the national trend – an increase of 26% was seen in 2016-17. The inquest work is divided into cases that require a full hearing, those that require investigation, and those that require statements from clinical staff. Requests for statements from staff who treated a patient before their death are significantly rising. This overall increase in activity is explained by a better awareness of which cases doctors need to report to the Coroner, and an increased public awareness of the coronial process which has led to more inquests. Hospital staff are commonly called to inquests where they are either asked to provide collateral information about a patient’s condition following an accident or a fall, or where there are concerns that the care of a patient may have more than minimally contributed to a patient’s death. Inquests are now increasingly complex, focusing in great detail on the care given to patients, the risk investigation process and the learning from an incident. The Coroner takes his/her duty to make risk management recommendations very seriously, and the actions taken following a Serious Incident investigation are discussed with the Coroner at the hearing and assurance is sought from the Coroner that these have been undertaken. Where the Coroner feels that an organisation has not addressed deficiencies that might adversely affect another patient, s/he will issue a ‘Prevention of Future Death’ report (PFD). This instructs the Trust to take action, where action has been found wanting. It is sent to the CQC, and the Chief Coroner who publishes such reports on the Courts and Tribunals Judiciary website. The Trust has not received any PFD reports in 2016-17 and continue to work to ensure robust actions are taken at the time of a Serious Incident investigation and can be evidenced at Inquest hearings

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
15
7. Compliments Trust staff receive many compliments via a number of different routes, a selection of which are reported through the Patient Experience Committee on a quarterly basis and some are shared on the Trust-wide email. 7.1 How are compliments received and managed?
The Trust Compliments are received via:
Thank you letters
Compliments gathered via the Friends and Family Test
Compliments via NHS Choices
Compliments received via Twitter
Compliments via other websites such as I Want Great Care and Patient Opinion
Compliments received via other routes such as emails to the PALS Department
Verbal compliments
7.2 Key Themes The Trust receives several thank you letters and emails via the Chief Executive’s Office. More are received directly to the relevant services. Some themes have been consistent and include:
Approach and manner of staff – Dignity and Respect
Individual acts of kindness shown
Efficiency of service
Successful result of treatment
Support Compliments gathered via the Friends and Family Test The Trust asks its patients to complete the Friends and Family Test (FFT) across all of the services that it provides. This is a mechanism used to ask people whether or not they would recommend a particular service to friends and family and also asks for reasons for their rating. The FFT score is calculated by determining the number of people who are "extremely likely" or "likely" to recommend the Trust, as a proportion of the number of people who responded to the question. When combined with supplementary follow up questions, the FFT provides a way of highlighting both good and poor patient experience. This kind of feedback is vital in transforming services and supporting patient choice as it gives all patients the opportunity to leave feedback on their care and treatment. 96% of inpatients and outpatients recommend the hospital. Most of the comments related to the staff, focussed largely on how caring, friendly and helpful they were. Here are some of the adjectives used to describe the staff:
Caring
Happy
Organised
Calm
Helpful
Attentive
Courteous
Reassuring

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
16
FFT Wordcloud – Pictorial representation of feedback for Kingston Hospital services given via the FFT.
Online Ratings: Compliments received via NHS Choices The website enables people to leave reviews and raise issues and concerns. The Trust overall rating is 4 stars based on 190 ratings. Compliments received via I Want Great Care Patients can post comments on the “I Want Great Care” website and these are available for public view. Over 195 reviews have been left for the Trust giving it an overall 5 star rating. Compliments received via Care Opinion The Care Opinion website is the UK’s leading independent feedback platform and allows honest and meaningful conversations between patients and the hospital. There are now over 513 stories related to the hospital with positive areas of feedback relating to fantastic staff, professional attitude and high quality of service received. Compliments received via Twitter The Trust also has a Twitter account and receives a range of feedback via this route. Tweets include: Amazing, friendly, kind and brilliant treatment.

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
17
8. Incidents An incident is an event or circumstance arising in the course of providing or supporting the provision of health care services that could have or, did, lead to unintended or unexpected harm, loss or damage to a patient, member of staff, visitor, the Trust and its property or environment. Staff report incidents on the Trust intranet using a system called Ulysses, which is accessed via the Trust intranet homepage. The Trust has a risk management system and incident reporting mechanism in place for several reasons:
to ensure it complies with its statutory obligations such as meeting the requirements of the Care Quality Commission (CQC), the NRLS (National Reporting & Learning System), the Management of Health & Safety at Work Regulations and Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR).
to ensure that incidents are investigated to identify learning points and influence change to practice, where necessary,
to reduce and prevent reoccurrence(s). Incident reporting is key to staff and patient safety and improving patient experience. High levels of incident reporting, with low harm, are a sign of a Trust that has an open, and
proactive patient safety culture – One that is also keen to learn from incidents and near-misses.
8.1 Incident reporting There were 6824 incidents during the time period 1st April 2016 to 31st March 2017. This is an increase from the previous 2 years incident activity; 5669 incidents in 14/15 and 6029 incidents in 15/16. KHFT aspires to be a high reporter of low/zero harm incidents and near misses. The incident data within this report demonstrates that the Trust is improving its level of progress with meeting this ambition.
There was an increase in incidents occurring between April 2016 and September 2016
Nursing staff have been the highest reporters of incidents. However, it should be noted they are the largest workforce which makes pharmacists, administrators, laboratory staff and radiographers good reporters relative to the total numbers that work in the hospital.
There was a slight dip in incident reporting in December 2016, which was followed by an increase in January 2017. This may be due to retrospective incident reporting on the Ulysses system as a result of conflicting pressures at that time of year.
8.2 National Reporting and Learning System (NRLS) Benchmarking
467 508 523
602 601 628 590 613
510
622 566
594
0
100
200
300
400
500
600
700
Incidents reported by month
Total
Average

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
18
The Trust makes regular uploads to the National Learning and Reporting System (NRLS) which is a requirement of NHS Improvement. These figures are collated and benchmarked with other Acute Trusts across the country. The latest report which provides Trust level data covers the period of April 2016 to September 2016. Kingston Hospital NHS Foundation Trust are with the ‘Acute (non specialist)’ cluster group:
The Trust reported 2,974 incidents to NRLS during this period. The Trust’s number of incidents per 1,000 bed days was reported as 44.57 which is better than the cluster rate of 40.03 per 1,000 bed days.
This demonstrates an improvement from the figures reported for the same period in 2015, in which the Trust’s rate of 32.55 was significantly lower than the cluster rate of 38.25 (per 1,000 bed days).
For the previous 2 years the Trust has shown a decline in the incident reporting rate when compared to national reporting rates which have risen over time. However, for the 2016 time period, both the Trust and National reporting rates have increased.
The Trust continues to promote incident reporting across all services.
April to September
Cluster rate per 1,000 bed days
KHFT rate per 1,000 bed days
2014 35.10 33.80
2015 38.25 32.55
2016 40.02 44.57
8.3 Incident Types
There were 4904 incidents affecting patients, which is 71.9% of all reported incidents.
The numbers of reported community incidents include 461 community acquired pressure ulcers.
The community incident reporting rate has increased since the previous year to 10.6%
The was a slight decrease in patient safety incident reporting and a slight increase in non-patient safety incidents
Only 2.1% of all incidents (patients and staff) involved more than minor harm.
Only 2.7% of patient safety incidents involved more than minor harm which is similar to the national average of 2.6% (for April-September 2016 time period)
The levels of harm during 2016-17 have remained relatively static when compared with the previous year.
High levels of incident reporting, with low harm, are a sign of a Trust with an open culture that is keen to learn from incidents and near-misses.
Incident Reporting by Affected Party 2016-17
Number of incidents
% of Total 2016-17
% of Total 2015-16
Patient 4904 71.9% 79.0%
Staff 729 10.7% 9.6%
Community 720 10.6% 7.7%
Buildings & Infrastructure 727 4.0% 3.3%
Visitor/Relative/Contractor 40 0.6% 0.5%

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
19
Harm levels for all incidents 2016-17 % 2016-17
2015-16 % 2015-16
% Change
1 - No Harm 4461 65.4% 3866 64% 1.4%
2 - Minor, Non Permanent Harm (Upto 1 M)
1971 28.9% 1828 30% -1.1%
3 - Moderate, Semi Permanant Harm (Upto 1 M)
110 1.6% 101 2% -0.4%
4 - Major, Major Permanent Harm
20 0.3% 18 0.3% 0.0%
5 - Catastrophic, Death 10 0.1% 6 0.1% 0.0%
6 - Near Miss 133 1.9% 182 3% -1.1%
7- Not recorded 119 1.7% 28 0.5% 1.2%
8.4 Patient Safety Incidents: Identified trends and key points to note Patient incidents made up 71.9% of all incidents reported during the 2016-17 period. The majority of patient incidents were reported in the Emergency Services (ES) division, which is a reflection of their proactive culture of incident reporting and due to patient complexity and volume, followed closely by Specialist Services (SS) division. The service line reporting the most patient safety incidents were Maternity (SS) followed by A&E (ES) and Elderly Care (ES). Only 2.7% of patient incidents involved more than minor harm The table below outlines the top 10 reporting categories for patient incidents. The top reporting category for patient incidents was ‘Accidents’ (17%) which includes falls, followed by Maternity (15%). Medication incidents made up 12% of patient incidents, of which 84% involved prescribing or administration. Care and Treatment. Care and Treatment made up 11% of patient incidents with a third of these incidents (34%) being categorised as delay in treatment.
Reporting category Number %
1 Accidents (Incl. Falls/sharps/manual Handling) 818 17%
2 Maternity 720 15%
3 Medication (Incl. Blood Products) 583 12%
4 Care & Treatment 534 11%
5 Tests / Investigations 334 7%
6 Appointments 273 6%
7 Documentation (Incl. Patient Records) 246 5%
8 Failure To Monitor / Escalate (Including Pressure 207 4%
9 Admission/discharge 163 3%
10 Transfer (Incl. Transport) 145 3%
Grand total 4904 100%
8.4.1 Falls Falls are reported in the monthly clinical quality report and the Trust scorecard. There was a decrease in the number of reported falls in 16/17 (n=697), compared to 15/16 (n=774), and the rate by bed days also decreased to 5.11 per 1,000 bed days, from 5.50 for 2015/16. Preventing patient falls and reducing harm associated with this remains a priority for the Trust – See Section 7.5 for actions undertaken.
Falls 2016-17 2015-16
Number of Patient Safety Incident (PSI) Falls 697 774
Number of Patient Safety Incident Falls where moderate or severe harm occurred
23 18
Number of Patient Safety Incident Falls per 1000 G&A bed days
5.11 5.50

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
20
8.4.2 Medication The number of reported medication incidents decreased slightly since last year. Medication incidents remain a focus and continue to be monitored at the bi-monthly Medications Safety Group.
Medication 2016-17 2015-16
Medication incidents
654 718
% of medication incidents where moderate harm occurred
0.2% 0.12%
8.4.3 Pressure Ulcers The number of hospital acquired grade 2 pressure ulcers has decreased from 36 in 15/16 to 27 in 16/17, and this is most likely due to the introduction of Daily Multi Disciplinary Team (MDT) discussions regarding pressure ulcers and the inclusion within the RAG and ‘Big 4’. There has also been a new Pressure Area Support Team (PAST) established, with support being provided in areas where numbers of pressure ulcers have developed with the aim of early identification and implementation of actions. A pressure ulcer action tracker is also in place to provide assurance of the monitoring and completion of actions following pressure ulcer investigations. The Trust reported 25 incidents of patients with Trust acquired grade 3 or 4 pressure ulcers in 16/17 Information on these is included within the Serious Incident section of this report.
Pressure Ulcers 2016-17 2015-16
Number of patients with hospital acquired pressure ulcers (Grade 2)
27 36
Number of patients with hospital acquired pressure ulcers (Grade 2) per 1000 bed days
0.2 0.26
Number of patients with hospital acquired pressure ulcers (Grade 3&4)
25 20
Number of patients with hospital acquired pressure ulcers (Grade 3&4) per 1000 bed days
0.18 0.14
8.5 Post incident actions Once an incident is reported to Ulysses, Managers are responsible for reviewing and investigating each incident and ensuring that suitable actions are put in place to prevent a recurrences. The following provides examples of such actions. Falls
A quality improvement project team are now leading on improving the care provided to patients identified as at risk of falling while in hospital. Improvements that have been implemented include the piloting of a new Multifactorial Falls Risk assessment that incorporates the 7 key recommendations from NICE Clinical Guideline 161, which is now being embedded across the Trust.
Falls care plan documentation now included within CRS, the electronic care records system.
The Trust has also completed the key recommendations from the National Inpatient Falls Audit.
Medication All Trusts are now obliged to have a dedicated Medications Safety Officer to oversee reporting of medication incidents to the NRLS, and all medication incidents are reported to the Medication Safety Officer and the CRS Pharmacy team. This has enabled the team to make changes to the

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
21
electronic prescribing system to improve the safe prescribing and administration of drugs. Key changes in 2016-17 include:
Development of a calculator available on all ward laptops to calculate gentamicin doses Powerplan to aid the safe prescribing of direct oral anticoagulants e.g. rivaroxaban IV aciclovir and IV aminophylline powerplans IV phenytoin powerplan with loading and maintenance doses An alert to prevent the co-prescribing of co-dydramol and paracetamol There has been an improvement in the scanning of patient wristbands and medication
following the introduction of regular reports to the Senior nurses. A Medicines Safety Newsletter is published bi-monthly. The Trust’s first Medicine Awareness Week was held in December 2016. The aim of the
week was to raise awareness of the importance of safe storage of medicines and to raise awareness on medication issues with a Medicines Awareness Trolley visiting ward and departments during the week
Pressure Ulcers All grade 2 pressure ulcer incidents across all wards are reviewed in the Pressure Ulcer Management Panel (PUMP) on a monthly basis, and more frequently if required. The Tissue Viability Nurse and respective matrons maintain close surveillance of the patients involved to prevent further deterioration. There was a new Pressure Ulcer Strategy launched during 2015.
8.6 Staff Incidents Staff incidents are reported on the Ulysses system (as per patient safety ones), with the investigation processes including the identification of any RIDDOR related injuries or applicable incidents. All “accident” category incident reports on the Ulysses system are reviewed by the Health and Safety Advisor, and a number of weekly reports are also communicated, including incident information on visitors, volunteers, contractor and others who are attending the site. The Trust has a number of specialist subject subcommittees which are led by subject leads. These subcommittees include aspect such as Fire, Security, Water, Medical Gases, Waste Management, Decontamination, Laser and Nuclear medicine. The subcommittees monitor incident data and KPIs as standing items on the agenda, and this allows for the identification and monitoring of incident trends. Further details are provided on the circumstances for individual incidents, if required, by the subcommittee members. High risk incidents are escalated to the Health and Safety Committee for further consideration and appropriate action. The Health and Safety Advisor is a member of these subcommittees. 8.6.1. Staff incident categories Staff incidents made up 10.7% of all incidents during the 2016-17 period. The top 5 reporting categories for staff incidents is shown below.
Reporting category Number %
1 Security 176 24%
2 Accidents (Incl. Falls/sharps/manual Handling) 162 22%
3 Tests / Investigations 77 11%
4 Infrastructure & Resources 61 8%
5 Medication (Incl. Blood Products) 47 6%
…. … …
Grand total 4904 100%

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
22
The most common incidents within the security category were related to verbal abuse (49%) and physical abuse (35%). Within accidents category, the most reported incident was injury from dirty sharps (27%). Under the test/investigations category, the vast majority of these incidents (97%) were due to the inappropriate use of chutes to deliver specimens, and notices have been added to areas where this occurred to reduce recurrences.
Incident category Current 2016/2017
Previous 2015/2016
Sharps 47 57
Slips Trips and Falls 45 35
Manual Handling 23 19
Body Fluid exposure 11 9
Struck by Object
10 10
Total (of top five)
130
130
8.6.2 Post incident actions Investigation of staff health and safety incidents has shown no significant change in the actualised incident profile for the Trust over the last two years. Sharps injury’s remain the most reported incident cause category. Analysis of the sharps data has not provided any clear common cause. The Health and Safety Advisor is planning an awareness programme to remind all staff of the correct protocol for using needles and bladed instruments with the aim of reducing the numbers of incidents reported.
9. Serious Incidents
Serious incidents are described as incidents that occur during NHS funded healthcare (including in the community), which result in one or more of the following;
unexpected or avoidable death or severe harm of one or more patients, staff or members of the public;
a never event - all never events are defined as Serious Incidents although not all never events necessarily result in severe harm or death;
a scenario that prevents, or threatens to prevent, an organisation’s ability to continue to deliver healthcare services, including data loss, property damage or incidents in population programmes like screening and immunisation where harm potentially may extend to a large population;
allegations, or incidents, of physical abuse and sexual assault or abuse; and/or
loss of confidence in the service, adverse media coverage or public concern about healthcare or an organisation.
The Trust reports these incidents and the investigation outcomes to the appropriate Clinical Commissioning Group and information is also uploaded on to a national database, called STEIS. The impact of serious incidents on patients, relatives and staff, can be significant and often are a result of failures in care or of service delivery. It is essential that all serious incidents are robustly investigated to identify any system or practice weaknesses, and to ensure that lessons are learnt and shared, with mitigations being put in place.

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
23
There were 44 serious incidents declared by Kingston Hospital NHS Foundation Trust from 1st April 2016 to 31st March 2017. This section will provide an overview of those incidents and the lessons learnt and actions taken in order to prevent the recurrence. 9.1 Serious Incident (SI) management process The overarching Trust document associated with the management of Serious Incidents is the ‘Procedure for the Identification and Management of Serious Incidents’. This document is based on the National (NHS England) Serious Incident Framework (March 2015). The Serious Incident Framework explains the responsibilities and actions for dealing with serious incidents and the tools available. It outlines the process and procedures to ensure that serious incidents are identified correctly, investigated thoroughly and, most importantly, learned from to prevent the likelihood of similar incidents happening again. All Serious Incident investigation reports are, once completed, agreed by the relevant Service Line. This process enables the Service Line to review and agree that the action plan that has been developed will address the report’s recommendations, as well as learn from the incident. The Service Line is responsible for ensuring that all Serious Incident action plans are effectively delivered and this is centrally monitored monthly by the Serious Incident Group. The Trust’s Serious Incident (SIG) Group meets weekly. The SIG is responsible for ensuring that comprehensive serious incident investigations take place, and that appropriate recommendations and robust actions are identified and delivered, thus ensuring learning from incidents and improving both the quality and safety of patient care. The SIG is chaired by the Medical Director, and membership includes the Director of Nursing, Divisional representatives, the Head of Quality Governance and the Quality Manager from Kingston Clinical Commissioning Group. Serious Incident reports are presented to SIG by either the Lead Investigator and/or the relevant Clinical Director. Once reports have been approved by the SIG they are submitted to Kingston Clinical Commissioning Group (CCG). All Never Event reports are subject to further scrutiny by a Scrutiny Panel chaired by Non-Executive Director and subsequently the full Trust Board. 9.2 Tracking of Action Plans All actions arising from Serious Incidents and Never Events Incidents are tracked using the SI action plan tracker. This tracker enables both Service Lines and the Serious Incident Group (SIG) to monitor the delivery of actions and to identify any issues that may be preventing the delivery of the action plan. The Serious Incident Group reviews the full SI action trackers of each Division every month. The Trust Board has responsibility for monitoring the Never Events Incidents action plans. These are also presented to the CCG for assurance on progress with delivering the actions. 9.3 Investigation Training In order to deliver a robust SI investigation staff need support and training. In May and July 2016 a ‘Root Cause Analysis Workshop’ was offered to all service lines for which a total of 25 staff attended over the 2 sessions. A further root cause analysis workshop has been scheduled for June 2017 which has been targeted at Services with the most incident activity, and a new patient safety and risk management training schedule is under development for 2017/18. The Quality Improvement Leads for Patient Safety support all SI investigation panels. They provide both group and or one to one investigation training. The training aims to deliver improvements in the Trust SI RCA investigation process and to share learning from previous investigations 9.4 Number and category of Serious Incidents (compared to incidents occurring in 2015/16) For the period 1st April 2016 to 31st March 2017 (the period covered by this report) the Trust declared 41 Serious Incidents (SI) and 3 Never Events, totalling 44 incidents which were reported on to the STEIS system across 11 categories:

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
24
Breakdown of SIs by division:
Emergency Services: 21
Specialist Services: 16
Clinical Support Services: 4
Corporate Services: 3 The service lines which had the most SIs were Maternity (8) and Elderly Care (8). In Maternity, the type of Serious Incidents reported by the this area during 2016-17 period included four Unexpected admissions to neonatal unit, 2 Unexpected admission to neonatal unit and subsequent Neonatal death, one Uterine rupture and intrauterine death and one Theatre related never event. The majority of the Maternity SI’s occurred in the Delivery Suite (5). In Elderly Care, the majority of incidents were patient falls resulting in permanent harm (7) and one failure in the discharge process whereby a district nurse referral was not sent, resulted in a medication incident. Three of the serious incidents occurred on Derwent ward (a ward predominantly for patients with Dementia), followed by two on Kennet ward, and one on each of Keats ward, Blyth ward and Claremont ward (the latter being an escalation ward which is opened during periods of increased activity).
0
2
4
6
8
10
12
14
Slip
s/tr
ips/
falls
Trea
tmen
t d
ela
y
Mat
ern
ity/
Ob
stet
ric
inci
de
nt:
mo
ther
an
db
aby
Dia
gno
stic
inci
de
nt
incl
ud
ing
del
ay
Me
dic
atio
n in
cid
ent
Surg
ical
/in
vasi
vep
roce
du
re in
cid
ent
Pre
ssu
re u
lcer
Co
nfi
den
tial
info
rmat
ion
leak
/in
form
atio
ngo
vern
ance
bre
ach
Sub
-op
tim
al c
are
of
the
det
eri
ora
tin
g p
atie
nt
Envi
ron
men
tal i
nci
den
t
2016-17 Serious Incidents using STEIS reporting criteria

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
25
9.5 Serious Incident (SI) themes and trends analysis
There were less SIs during quarter 1 of 16/17 that there were in quarter 1 of 15/16. Whereas the SI activity in 15/16 dropped during the winter period, there was a noticeable peak in SIs in December 2016 and quarter 4 of 16/17 compared to the previous year.
STEIS Reporting Criteria 16/17 15/16
Slips/trips/falls 13 13
Treatment delay 6 1
Maternity/Obstetric incident: mother and baby 8 4
Diagnostic incident including delay 4 0
Medication incident 4 0
Surgical/invasive procedure incident 2 1
Pressure ulcer 2 11
Confidential information leak/information governance breach 2 5
Sub-optimal care of the deteriorating patient 2 3
Environmental incident 1 0
Apparent/actual/suspected self-inflicted harm 0 1
0123456789
SS: M
ater
nit
y
ES: E
lder
ly C
are
(A
cute
Car
e)
ES: A
&E
/ A
AU
SS: P
aed
s &
NN
U
Co
rpo
rate
Ser
vice
s
ES: C
ard
iolo
gy &
Hae
mat
olo
gy
ES: R
esp
irat
ory
SS: G
en
eral
Su
rge
ry &
Uro
logy C
SS: I
CU
CSS
: Th
eatr
es
SS: O
ral &
EN
T
SS: T
rau
ma
&O
rth
op
aed
ics
CSS
: Rad
iolo
gy
SS: O
ph
thal
mo
logy
2016-17 incidents by Service Line
0
2
4
6
8
10
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Incidents declared by month
16/17 15/16

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
26
Disruptive/aggressive/violent behaviour 0 1
Grand Total: 44 40
Pressure Ulcers The number of pressure ulcer’s meeting the SI criteria has dropped since the previous year, from eleven to two. This can be explained by the agreement of a local protocol in response to the updated Serious Incident Framework, whereby any trust acquired pressure sores are subject to a concise review which is presented to the Pressure Ulcer Management Panel (PUMP); if the pressure sore is deemed avoidable and resulted in significant harm, an SI is declared and a comprehensive investigation conducted. Other improvements in relation to the prevention of pressure ulcers are mentioned at Section 7.4.3. Slips/trips/falls Of the 13 slips/trips/falls meeting the serious incident criteria, the themes included:
Six incidents identified a lack of care plan documentation; in two of these incidents, the care plan had not been updated to reflect new signs of confusion and memory loss in the patient.
Four incidents revealed a delay in diagnosing and treating the injury sustained post fall (in two incidents there was a delay in recognising the injury; in one incident there was a delay in the X-ray being performed; in another incident there was a delay in medical review after a fall).
In three incidents, transfer of the patient between areas was felt to have contributed to confusion and lack of familiarity with the ward environment; in one case the patient had been transferred three times in a twelve hour period.
Two incidents identified falls alarms in use that were faulty, therefore not alerting staff when the patients were attempting to mobilise.
Three incidents were felt to be unavoidable in the circumstance, with the root cause analysis investigations identifying that all appropriate care was in place prior to the fall. Cross cutting themes
Documentation; lack of formalised or updated care plan.
Communication between all members of the multidisciplinary team.
Assessment; consideration of all elements of the multifactorial falls assessment in order that the appropriate intervention is put in place.
Human factors; task focus and distraction.
Patient factors; Cognitive impairment and new confusion was present in the majority of cases
Actions
Implementing the multifactorial falls assessment and ensuring that the CRS (care records system) is updated to support this – Which has been completed.
Recognition of repeat fallers (ward areas currently receive a weekly email highlighting incidents of patients who have fallen in order to support awareness of repeat fallers)
Ensuring dementia and delirium assessment is completed on admission
Consideration of one to one close supervision in patients at high risk of falls. Maternity Of the eight Maternity incidents (six unexpected admissions to neonatal unit and two subsequent neonatal deaths), themes included:
Five incidents identified issues with the interpretation of CTG, including delay in recognition,
escalation and inappropriate management plan with abnormal CTG
Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
27
Three incidents identified a failure to expedite delivery
Three incidents identified a failure of the handover process
Two incidents identified failure to escalate to the on call consultant
One incident identified the mismanagement of sybtocinon
Cross cutting themes:
Communication in teams
Documentation either lacking or absent
Not recognising clinical risk
Escalation to senior colleagues
Increased activity in all areas
Lack of clarity in local guidance
Human error – distraction and lowered vigilance when staff are busy Actions:
Review / implantation of guidelines
Include key messages in obstetric emergency training and fetal surveillance training
Messages shared via anonymous case reflections, risk newsletter, email
Messages shared via anonymous case presentations at consultant meeting ,Risk meeting, clinical governance, perinatal meeting
One to one feedback
Embed robust handover process. 9.6 Never Events Never events are a sub-set of Serious Incidents and are defined as ‘serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented by healthcare providers’. In 2016/17 the Trust declared three Never Events; two Theatre related incidents and one medication incident. The Trust also assisted in the investigation of an additional Never Event with a private provider which involved KHFT staff. All Never Events that occur in the Trust are investigated in line with the Trust’s Serious Incident Policy and are reviewed by a Trust Board sub committee (chaired by a Non-Executive Director), and the Trust Board. Actions arising from Never Events are monitored through the Serious Incident Group monthly and the Trust Board bi-monthly. 9.6.1 Actions taken as a result of Serious Incident and Never Event investigations: A range of actions were identified from the three Never Events including:
Improved escalation and handover processes.
Additional training and emphasis upon compliance with the WHO surgical Safety Checklist.
Recognition of how environmental factors, such as a busy unit, can impact upon decision making, and the identification of a need for human factors training.
Implementation of assertiveness training for staff. All of the actions from the three Never Events have been completed.

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
28
10. Duty of Candour Duty of Candour means frankness, openness and honesty (being open). This regulation was added to the CQC Fundamental Standards of Quality and Safety in 2015 to ensure that healthcare providers, like hospitals, are open and honest with patients if there have been mistakes in their care that have led to significant harm. The trust is continually developing our culture of open and honest conversations with patients and families when things do go wrong and when care has fallen below expected standards, and we support staff to do this. We also seek out patient and carer involvement in our serious incident processes, discussing the findings of our investigations and actions. Progress made with achieving compliance with the Duty of Candour during 2016/17 includes:
Providing multidisciplinary staff training,
Raising awareness via discussions at staff forums,
Updating the Trusts electronic incident reporting system to highlight where Duty of
Candour could apply; and
Introducing audits on patient safety incidents to monitor compliance with the Duty of
Candour requirements. Plans for 2017/18 include developing a patient information leaflet and a web page for staff, and continuing with Duty of Candour training.
11. Triangulation The tables below show the top 10 categories during 2016-17 for all patient safety incidents, complaints and PALS queries.
As would be expected, there is more alignment between the complaints and PALS areas with 8/10 categories matching.
The top 3 categories for both PALS and complaints are also featured within the top 10 incident reporting categories (‘Communication’, ‘Care & Treatment’ and ‘Appointments’) indicating that these are the areas of concern for both staff and patients/visitors.
Additionally, categories of ‘Medication (incl blood products)’ and ‘Tests & Investigations’ feature across all 3 areas indicating a shared awareness of risk areas.
‘Accidents (incl falls/sharps/manual handling)’ and ‘Maternity’ are the top 2 categories for reported incidents, however do not feature in either the complaints or PALS top 10.
‘Infrastructure& Resources’ features both within the top 10 incident reporting categories and the top 10 PALS concerns.
Categories of ‘Estates/Support services/environment’, ‘Procedure incl surgery/ endoscopy/anaesthesia etc’, and ‘Admission/discharge’ feature in both PALS and complaints list but not incidents.
PALS
Category Type - Top 10 No of Concerns
1 Appointments 463
2 Communication (Incl. Consent)/information 370
3 Care & Treatment 203
4 Estates/support Services/environment 122
5 Tests / Investigations 93
6 Admission/discharge 51
7 Procedure (Incl. Surgery/endoscopy/anaesthesia Etc) 35
8 Information Governance 35
9 Diagnosis (Incl. Failed Or Wrong) 22
10 Documentation (Incl. Patient Records) 19

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
29
Complaints
Category Type - Top 10 No of Complaints
1 Communication (Incl. Consent)/information 83
2 Care & Treatment 83
3 Appointments 54
4 Estates/support Services/environment 45
5 Procedure (Incl. Surgery/endoscopy/anaesthesia Etc) 27
6 Diagnosis (Incl. Failed Or Wrong) 27
7 Admission/discharge 25
8 Medication (Incl. Blood Products) 8
9 Tests / Investigations 8
10 Security (Violence/aggression/property/financial Loss) 7
Incidents
Reporting category
Number of incidents
1 Accidents (Incl. Falls/sharps/manual Handling) 818
2 Maternity 720
3 Medication (Incl. Blood Products) 583
4 Care & Treatment 534
5 Tests / Investigations 334
6 Appointments 273
7 Documentation (Incl. Patient Records) 246
8 Failure To Monitor / Escalate (Including Pressure 207
9 Admission/discharge 163
10 Transfer (Incl. Transport) 145
Conclusion In 2016-17, continued progress has been achieved with the implementation and use of the Trusts Risk Management System (Ulysses) and the Serious Incident Group (SIG), which is attended by a range of senior staff and specialist advisors. The number of complaints has dropped significantly and there has been a decrease in PALS contacts. Issues regarding communication and information remain the highest category, and appointment related issues have decreased for the second year. The number of new Claims has also decreased, and the Trust is performing better than average in terms of timeframes for notification to resolution. The number of incidents reported has continued to rise and the level of harm is similar to the national average. A good safety culture is indicated by high levels of reporting with low levels of harm. The NRLS report shows that the Trusts patient safety incident reporting level of 44.57 (per 1,000 bed days) is slightly higher than the cluster rate of 40.03, which is an improvement compared to the same period in 2015 when the rate was lower than the cluster rate by 5.7.

Kingston Hospital NHS Foundation Trust – Trust Board – July 2017
30
Feedback from incidents has improved and work on this will continue throughout 2017-18, along with the development of a patient safety and risk management training schedule to further support staff with the management of incidents and risk. There has been a slight increase in the number of Serious Incidents that were reported, and as would be expected the Emergency Services division and A&E, AAU and Maternity services reported the most incidents. There has been a substantial reduction in hospital acquired pressure ulcers, and there have been fewer grade 3 & 4 pressure ulcers meeting SI criteria. Car parking features heavily within complaints and PALs. Appointments related concerns accounted for 31%, which is a significant reduction compared to the previous year. Communication, appointments, medication and care/treatment are common themes featuring across PALS, incidents and complaints. Active improvements to address themes from incidents include the continued work on Trust wide initiatives such as Sign up to Safety, and improved processes implemented for the management and prevention of pressure ulcers and falls. As the vast majority of care interactions at the Trust are positive experiences for patients, carers and staff, it is important to note the compliments received from visitors, carers and patients throughout 2016/17. The compliments during this period showed staff to be caring, respectful, helpful and kind. By looking at what we do best and what we could do better the Trust is taking an informed approach to further developing and improving patient safety and patient experience.
AUTHORS: Alison Vizulis, Head of Quality Governance and Risk Clare Parker, Head of Litigation, Complaints and PALs Alannah Hayes, Quality Improvement Lead for Patient Safety


















