Palliative Pain Management
70
Palliative Pain Management
-
Upload
meducationdotnet -
Category
Documents
-
view
423 -
download
0
Transcript of Palliative Pain Management

Palliative Pain Management

Content
• Pain – definition, assessment
• Nociceptive and Neuropathic Pain
• Types of pain in cancer
• Opioids – principles and WHO ladder
• Opioids – titration, relative potency, prescribing, formulations, side-effects
• Opioid Induced Neurotoxicity (OIN)
• Adjuvants for types of cancer pain

Principles used in symptom control
• What causes the symptom ?
– Physical
– Psycho-social
– Spiritual
• How do we manage it ?
• Treat the treatable
• Symptom control
• Review your management – things change!

Total Suffering
Pain
Social & Financial
Spiritual
Cultural Psychological
Physical Symptoms
Total Pain/Suffering Woodruff

Pain and advanced cancer
• .. are not synonymous
• ¼ of patients do not have pain
• ¾ of patients experience pain at some stage of their illness – 1/3 of patients have 1 pain
– 1/3 of patients have 2 pains
– 1/3 of patients have >3 pains

Causes of pain in cancer patients Cancer related …
• Visceral
• Bone
• Soft tissue infiltration
• Nerve compression/infiltration
• Muscle spasm
• Raised intracranial pressure
• Metabolic/ Endocrine

Causes of pain in cancer patients Treatment related …
• Surgery – Surgical wound – acute / chronic
– Adhesions
• Radiotherapy – Acute / chronic e.g. mucositis / fibrosis
• Chemotherapy – Acute / chronic e.g. mucositis / neuropathy

Causes of pain in cancer patients Associated factors …
• Constipation
• Pressure sores
• Bladder spasm
• Joint stiffness
• Post herpetic neuralgia

Causes of pain in cancer patients Concurrent illnesses …
• Low back Pain
• Angina
• Arthritis
• IBS
• Trauma
• Other

Specific assessment tools
• Visual analogue scales
• Numeric analogue scales
• Categorical scales
• Body charts
0 10
Severe 3
Moderate 2
Mild 1
None 0
Visual analogue scale
Categorical scale

What is “Total Pain”?
Total
Pain
Physical
Other symptoms
Adverse Rx effects
Insomnia/Chronic fatigue
Psychological
Anger
Disfigurement
Fear of pain/death
Helplessness
Social
Family/Finance worries
Loss of job/income
Loss of role
Abandonment/Isolation
Spiritual
Why me?
Anger at God
What is the point?
Guilt


Other cancer problems
• Social circumstances
• Family communication
• Patient coping - denial
• Family coping
• Treatment side-effects
• Disease symptoms - recurrent disease
• Genetics

SYMPTOMS IN ADVANCED CANCER
0 10 20 30 40 50 60 70 80 90
Asthenia
Anorexia
Pain
Nausea
Constipation
Sedation/Confusion
Dyspnea % Patients (n=275)
Ref: Bruera 1992 “Why Do We Care?” Conference; Memorial Sloan-Kettering

Pain
• Defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage
• Acute pain is generally sudden in onset, temporary, and subsides of its own accord or after successful treatment of the cause
• Chronic pain persists or recurs for prolonged and often indefinite periods of time

Pain Assessment
• Measure pain levels with the patient at regular intervals.
• Cause of pain should be identified and treated promptly.
• Patients can describe:
– location of pain
– aggravating or relieving factors
– intensity or severity
– goals for pain control
– duration, and when it occurs

Pain Scale
Visual Analog Scale (VAS) 100mm long
Simple Descriptive Pain Intensity Scale
Numeric Rating Scale (NRS)
No Pain
No Pain
No Pain
Mild Pain
Moderate Pain
Severe Pain
Worst Possible Pain
0 1 2 3 4 5 6 7 8 9 10
Worst Possible Pain

Assessing pain Investigations may be useful

Assessing pain Investigations may be useful

Classification of Pain
• Nociceptive pain - tissue damage (two types) • Somatic
– e.g. metastatic bone pain
• Visceral – e.g. liver capsule pain – e.g. colic from malignant bowel obstruction
• Neuropathic - arises from nerve damage • Central [brain, spinal cord, autonomic]
• Peripheral nerves
– Dysesthetic (burning) – Lancinating/shooting – Sensory changes – hyperaesthesia, allodynia, numbness

• Somatic Pain
• Arises from bone, muscle, cutaneous and
connective tissue
• Localised
• Typically clinically described as throbbing,
aching or stabbing
• Visceral Pain
• Arises from internal organs
• Generalised / diffuse
• Clinically, typically described as cramping or
gnawing
Nociceptive Pains

• Arises from neural tissue
• Clinical descriptions variable
• Continuous ‘burning’
• Spontaneous ‘lancinating’ or ‘electric’
• Associations
• Allodynia
abnormal sensations
• Hyperalgesia
Neuropathic Pain

Types of pain in cancer
• Visceral pain
• Neuropathic pain
• Bony pain
• Referred pain
• Breakthrough pain

Visceral Pain
• Results from infiltration , compression, distension or stretching of thoracic and abdominal viscera
• Often poorly localised
• Often referred to cutaneous sites
• Can usually be well controlled and responds well to analgesics

Neuropathic pain
• Pain caused by injury to, or disease of, the PNS or CNS
• Puzzling & frustrating: – often seems to have no
cause
– may respond poorly to treatment
– can last indefinitely
– can escalate over time
– often results in severe disability

Neuropathic pain
• Most distinguishing feature: anatomical pattern of distribution,
pain follows nerve distribution
• Two broad classifications: –constant (often described as
burning, throbbing, or stinging) –intermittent (often described as
sharp, jabbing, or shooting) • Often worse at night

‘Bony’ pain • Can be very painful
• Cancer cells multiply inside the bone and put pressure on the nerves
• Also causes bones to crumble – this exposes the nerves, and leads to more pain
• Responds well to analgesics and radiotherapy

Referred pain
• Pain from internal organs felt at a site distant from the tissue damage
e.g. pancreatic cancer pain is felt in the back

Breakthrough pain
• Transient increase in pain over ‘baseline’
• Rapid onset and severe
• Frequent breakthrough pain may indicate inadequate control of ‘baseline’ pain

Dose for breakthrough cancer pain
The breakthrough dose should be equivalent to a 4 hourly dose
• i.e. - 1/6th of total daily opioid dose
• Generally use the same opioid as being used for regular regimen

Around-the-Clock (ATC) Medication
Pain Relief Threshold
Persistent Pain
Treating Persistent Pain P
ain
In
ten
sit
y
Time
Theoretical Model

Breakthrough pain (BTP)
Around-the-clock
Medication
Time
Breakthrough
Pain
Theoretical Model
Pa
in In
ten
sit
y

Increasing ATC Medication – May Increase Side Effects
Around-the-
clock
Medication
Breakthrough
Pain
Theoretical Model
Pa
in In
ten
sit
y
Time


Commonly used medication in palliative care patients
• Analgesics
• Antiemetics
• Laxatives
• Antispasmodics
• Anticholinergics
• Anticonvulsants
• Antidepressants
• Corticosteroids
• Antibiotics
• Sedatives

Drug complications
• Allergy
• Predicted pharmacological effects
• Increased drug levels – Organ failure
– Increasing age
• BNF appendices
– Organ failure • Liver impairment
• Renal impairment
– Drug interactions

Basic Principles of Opioid Analgesia
The right dose of opioid is the one that achieves the best analgesia with the fewest side effects.
• By the cause of the pain(s) • By the clock • By the ladder • By the mouth • For breakthrough pain • For the individual • Adjuvant therapies as needed • Prevent side effects

Opioid Side Effects Advise patients
• Constipation
– Co-prescribe laxatives e.g. Senna/Lactulose
• Nausea & vomiting (30%)
– Prophylactic anti-emetics e.g.. Haloperidol/Cyclizine/ Domperidone/Metoclopramide
• Sedation
– Reassure and monitor
– Advise re driving
• Dry mouth

Polypharmacy
• Concurrent use of several different medications
• Drug interactions
• Increased cost
• Non compliance
• Adverse effects
• Study GP
– Use >5 medications – increased risk

• Polypharmacy & drug interactions • Cytochrome P450 interactions with inhibition
or induction of drug biotransformation (‘bullets’ & ‘blanks’)
• Terfenadine/ ketoconazole- cardiac dysrhythmias by inhibition of terfenadine metabolism
• Rifampicin / phenytoin increases phenytoin clearance- reduced effect

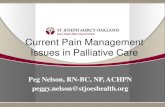
World Health Organization Pain Ladder Cancer Pain Management
Increasing Pain
Step 1
Step 2
Step 3
Non-opioid +/- Adjuvant
Opioid for mild to moderate pain +/- Non-opioid +/- Adjuvant
Opioid for moderate to severe pain +/- Non-opioid +/- Adjuvant
Address psychosocial and spiritual issues; consider adjuvant therapies
Step 4 ?

Analgesics
P
A
I
N
Paracetamol
Codeine
Dihydrocodeine
Tramadol
Morphine
Diamorphine
MILD
SEVERE
Simple analgesics
Opioid agonists
Strong opioid agonists

Paracetamol
Active metabolite of phenacetin
Mode of action: Analgesic
Weak prostaglandin inhibitor
Indications: Mild to moderate pain without
inflammation
Adverse effects: Rare at normal dosage
Liver/renal toxicity in overdosage

Mode of Action
Produce analgesia through actions at regions in the brain that contain endogenous opioid peptides
Receptor Subtype
Mu Delta Kappa
Opioid Peptides + +
AGONIST
Codeine
Morphine
PARTIAL AGONIST
Buprenorphine
(+)
+
±
(+)
(+)
(+)

Prescribing Opioids
• Weak opioids
– Dose often Codeine limited by presence of paracetamol
– Tramadol
• Strong opioids
– Morphine, oxycodone, diamorphine, fentanyl, hydromorphone, methadone, buprenorphine
• Do NOT use:
– Pethidine

Codeine/Morphine relative potency

Initiating Opioids: Starting Doses
• Morphine 2.5-5 mg q4hr PO • Oxycodone 1-2 mg q4hr PO • Diamorphine 2.5mg q4hr SC
• Fentanyl transdermal – ONLY for stable pain
– 12 mcg/hr patch may be excessive in opioid naïve patients
• Add breakthrough dose (4 hrly prn)
• Consider smaller doses in frail, renally impaired and
elderly patients

Pharmacokinetics of Opioids
• Onset of pain relief – Oral opioids 15–30 min
– SC opioids 5–10 min
– IV opioids 1 min
• Duration of pain relief – Short-acting oral opioids 3–5 hours
– Long-acting oral opioids 8–12 hours
– Fentanyl patches 72 hours
– IV or SC opioids 2–4 hours

Short-acting
Formulations
(4 hour duration)
• Opioid-naïve patients
• Pain crises
• Breakthrough cancer pain
Long-acting
Formulations
(12 hour duration)
• Reserve for stable situations
Opioid Formulations

Routes of Opioid Administration
• Preferred route – oral
• When unable to swallow: SC, CSCI, IV, TD
• Seldom used (only in special situations):
– Sub Lingual (breakthrough pain, fentanyl)
– Intraspinal (epidural or intrathecal)
• Do NOT use IM

Titrating the Dose of Opioid
Increase the dose by 25-50% if the patient is not achieving adequate pain control.
Take into account number of breakthrough doses taken.

Opioid Myths
Many patients harbor fears about opioids.
• “It means the end is near”
• “Opioids cause addiction”
• “Opioids will lose their effectiveness over time, leaving nothing to treat severe pain ‘at the end’”
• “Opioids will make me a zombie or take away my mental capacity”
• “They will stop my breathing”
• “They will my shorten life”

Common Opioid Adverse Effects
Common side effects: • Constipation (requires ongoing laxatives) • Nausea
– Usually resolves after a few days – Metoclopramide or cyclizine in the first few days
• Sleepiness (usually resolves after a few days)
Less common side effects: • Opioid neurotoxicity • Sweating, dry mouth, pruritis – very uncommon
(especially with appropriate dosing) • Respiratory depression


Opioid Induced Neurotoxicity (OIN)
• Clinical Presentation – Myoclonus, hallucinations, cognitive impairment,
delirium, severe somnolence, dysaesthesia, allodynia
• Mechanism unclear – Opioid metabolites
– Opioids themselves
• Increased risk – Renal impairment, high doses of opioids, infection
(sepsis)

Management of Opioid Neurotoxicity
(OIN) Seek advice from the Specialist Palliative Care
Team Exclude other causes for symptoms. The main strategies for treatment of OIN are:
– Hydration – Opioid dose reduction – Opioid switching – Change route of administration

Constipation – management
• Pre-empt constipation by putting everyone at risk (e.g. patients on opioids) on regular aperients
• Treat reversible causes e.g. give analgesia if pain on defecation, alter diet, ↑ fluid intake
• Treat with regular stool softener (e.g. lactulose) ± regular bowel stimulant (e.g. senna) or a combination drug (e.g. co-danthrusate). Titrate dose against response

- If that is ineffective consider adding rectal measures.
• if soft stools and lax rectum—try bisacodyl suppositories (0 must come into direct contact with rectum);
• if hard stools—try glycerol suppositories—insert into the faeces and allow to dissolve
• - If still not cleared refer to the district nurse for lubricant ± high phosphate (stimulant) enema (usually act in ~20min.)
• - Once cleared leave on a regular aperient with instructions to ↑ aperients if constipation recurs.
Constipation – management


Types of pain in cancer
• Visceral pain
• Neuropathic pain
• Bony pain
• Referred pain
• Breakthrough pain

Adjuvants for Visceral Pain
• Liver metastases or malignant bowel obstruction
– Corticosteroids (Dexamethasone 2-8 mg OD or BD)
– NSAIDs e.g. Diclofenac SR 75mg bd
• Colic
– Hyoscine Butylbromide SC (20mg)

Dysaesthetic pain (burning)
Neuralgic pain (lancinating)
Opioid and dose titration (moderate to severe pain)
Gabapentin or Pregabalin or TCA
TCA and Gabapentin or Pregabalin +/- lidocaine patch
Corticosteroid (may be used first line in pain crisis)
NMDA antagonists (ketamine)
Drugs for Neuropathic Pain

Adjuvants for Bone Pain [1] • NSAIDs
– Limited use in severe pain – Renal and gastro-intestinal side effects – Limitations of Cox-2 specific NSAIDs recently noted
• Steroids – Useful in pain crises
• Radiotherapy – 75% to 85% response rate (decreased pain) – Few side effects with palliative therapy – Response within 1 to 2 weeks (maximum response up to 4
weeks later) – Duration of analgesia is several months

Adjuvants for Bone Pain [2]
• Bisphosphonates
– Reduction of skeletal events (good evidence)
– Management of more acute pain with parenteral infusion (some controversy)
• Surgery
– impending or pathological fracture

Key points

Pain Management • Nociceptive Pain
– Somatic: arises from bone, muscle, cutaneous tissue and CT. localised, clinically presents as throbbing/aching/stabbing pain.
– Visceral: internal organs, generalised diffuse achy pains like period pains
• Neuropathic Pain – Arises from neural tissue: PNS or CNS
– Can be continuous or spontaneous, descriptions vary from burning to electric
– Associated with allodynia (slightest touch causes pain), hyperalgesia (exaggerated pain response)
– May be disproportionate to injury (chronic) or indicate neural compression (cancer)
– May respond poorly to treatment
– Can last indefinitely and escalate over time – severe disability
– Distinguishing feature: anatomical pattern of distribution
– Constant or intermittent – burning, throbbing OR sharp stabbing, jabbing
– Often worse at night
– Rx: gabapentin, pregabalin, amytriptyline, paroxetine, opioids help a bit, ketamine
• Visceral Pain – Arises from internal organs, is generalised or diffuse and poorly localised
– Crampy/colicky pain
– May respond better to anti-cholinergic/anti-spasmodics e.g. buscopan

Pain Management • Referred Pain
– Pain from internal organs felt at a distant site from tissue damage
– E.g. back pain in pancreatic cancer, shoulder tip pain in diaphragm irritation
• “Bony” Pain – Can be really painful
– Cancer cells multiply inside bones and put pressure on the nerves, they also cause bone to crumble which exposes the nerves pain
– Responds well to analgesics and radiotherapy
– Pathological fractures and prophylactic stinting
• Breakthrough Pain – Transient increase in pain over “baseline”
– Rapid onset of severe pain
– May indicate inadequate control of baseline pain if frequently occurring
– Dose = 1/6 of daily opioid dose ( one 4hourly dose)
– Same opioid as baseline medication, faster acting if possible
– Careful of A/Es
– If too much breakthrough being used: review analgesia and change dose

Pain Management • Prescribing Opioids
– Weak: codeine dose often limited by paracetamol. Tramadol used but nauseating and causes delirium
– Strong: morphine, oxycodone (oxycontin-baseline and oxynorm-breakthrough), diamorphine, hydromorphone, methadone (good for neuropathic pain but last line), buprenorphine
– Do NOT use pethidine: useless, causes epileptic fits
– Codeine is metabolised to morphine – 10g codeine = 1g morphine • E.g. 2 x 8/500 codeine = 16 codeine = 1.6 morphine

Pain Management • Starting Doses
– Morphine: 2.5-5mg q4hr PO
– Oxycodone 1-2mg q4hr PO
– Diamorphine 2.5mg q4hr SC
– Fentanyl transdermal patch for stable pain 12mcg/hr (=45mg oral morphine)
– Add breakthrough dose: 1/6 daily dose
– Smaller doses in renal impairment, old, frail, hepatic failure
– Monitor A/Es for toxicity
– Onset: 15-30min PO, 5-10min SC, 1min IV
– Duration: short acting 3-5 hours (4hrly), long acting 8-12hrs, fentanyl patch 72hrs, IV/SC 2-4hrs
– Long acting: stable pain
– Short acting: breakthrough, pain crises, opioid naïve pts
– CSCI: continuous sub cutaneous infusion
– Do NOT use IM
– Inadequate pain control: increase dose by 25-50%
– A/Es: constipation (laxatives), nausea, (anti-emetics), sleepiness. OD, sweating, dry mouth, pruritis, resp depression

Pain Management • Opioid Induced Neurotoxicity
– Presentation: myoclonus, hallucinations (flashes of light), cognitive impairment, delirium, severe somnolence, dysaethesia, allodynia
– Mechanism: unsure if due to opioid metabolites or opioids themselves
– Increased risk: renal impairment, high dose opioids, infection (natural opioid released by body)
– RR 8+: watch
– RR<8 – give naloxone slowly. Reverses A/Es as well as pain effects
– Management: hydration, opioid dose reduction, opioid switching, changed route
• Adjuvants for visceral Pain – Liver mets or malignant bowel obstruction: steroids, NSAIDs
– Colic: hyoscine butylbromide – buscopan 20mg
• Adjuvants for bone pain – NSAIDs – if not severe, careful with kidneys and liver
– Steroids: good for pain crises. Not long term
– Radiotherapy: 75-85% response rate within 1-2weeks, lasts several months
– Bisphosphonates: reduces skeletal events, helps with pain
– Surgery: stent impending or pathological fracture