Pain Management in Primary Care - PAIN-OUTLET...
31
Pain Management in Primary Care Michael Mangione, MD Chief of Anesthesia and Director of Pain Service VA Pittsburgh Health Care System Nancy Wiedemer,CRNP VISN 4 Pain Management POC Pain Management Coordinator Philadelphia VA Medical Center 1
Transcript of Pain Management in Primary Care - PAIN-OUTLET...

Pain Management in Primary Care
Michael Mangione, MD
Chief of Anesthesia and Director of Pain Service
VA Pittsburgh Health Care System
Nancy Wiedemer,CRNP VISN 4 Pain Management POC
Pain Management Coordinator
Philadelphia VA Medical Center 1

AGENDA
1. Review VHA Pain Management Initiatives
• Opioid Safety Initiative
• Stepped Care Model
2. Case presentation/ group dialogue • Managing chronic pain in PACT
• Tapering opioids
2
Update on VHA initiatives
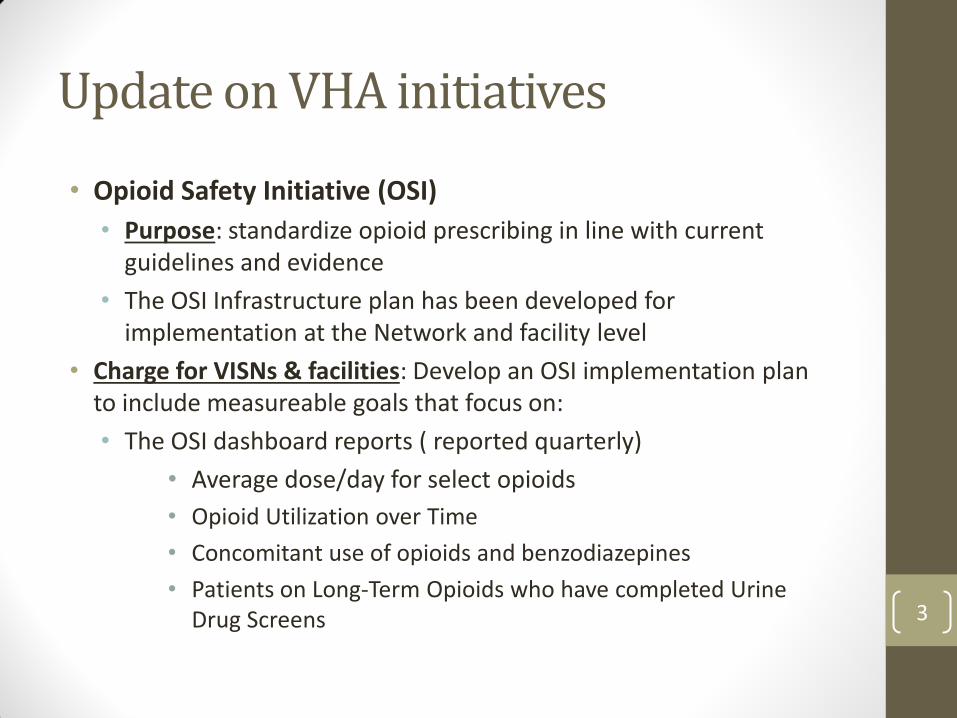
• Opioid Safety Initiative (OSI)
• Purpose: standardize opioid prescribing in line with current guidelines and evidence
• The OSI Infrastructure plan has been developed for implementation at the Network and facility level
• Charge for VISNs & facilities: Develop an OSI implementation plan to include measureable goals that focus on:
• The OSI dashboard reports ( reported quarterly)
• Average dose/day for select opioids
• Opioid Utilization over Time
• Concomitant use of opioids and benzodiazepines
• Patients on Long-Term Opioids who have completed Urine Drug Screens
3

VISN 4 Plan
• VISN 4 OSI group
• Building a dashboard to track metrics in real time
• Metrics:
• Tracking patients > 200 morphine equivalents
• Opioid Treatment Agreements
• Urine Drug Screening
• 2 face to face visit per year *
• EKGs with methadone
• Future metric: concomitant opioid/benzodiazepines
• Education(4th PACT Collaborative) / Tools for practice(methadone reminders)/ Expansion of Pain Services at Pittsburgh and Philadelphia/Development of CARF programs/telehealth-scan echo initiatives/E-Consults 4

VHA'S Pain Management Directive (2009-053)
VHA's single standard of care, the Stepped Pain Care model, including safe opioid prescribing
Transforming VA Pain Care: 6 Goals of the Stepped Care Model 1. Educate Veterans / families to promote and build self efficacy and for
shared decision-making
2. Educate/train all team members to their discipline-specific competencies, including team-based care
3. Develop and integrate non-pharmacological modalities into care plans
4. Institute rationale medication prescribing, use of pain procedures, and safe opioid use (universal precautions)
5. Develop approaches to bringing the Veteran’s whole team together (scan-echo, e-consults, tele-health, clinical video tele-consultation, community support)
6. Establish practical metrics to monitor pain care and outcomes
Plans for supporting OSI Infrastructure
5

Routine screening for presence & severity of pain; Assessment and
management of common pain conditions; Support from MH-PC
Integration; OEF/OIF, &
Post-Deployment Teams; Expanded care management ;
Pharmacy Pain Care Clinics; Pain Schools; CAM integration
Multidisciplinary Pain Medicine Specialty Teams;
Rehabilitation Medicine;
Behavioral Pain Management; Mental Health/SUD
Programs
Advanced pain medicine diagnostics
& interventions;
CARF accredited pain rehabilitation
STEP 2
STEP 3
STEP 4
VA-DoD Stepped Pain
Care
Complexity
Treatment Refractory
Comorbidities
RISK
Understand BPS model; Nutrition/weight mgmt, exercise/conditioning, &
sufficient sleep; mindfulness meditation/relaxation techniques;
engagement in meaningful activities; family & social support; safe
environment/surroundings
STEP 1
6
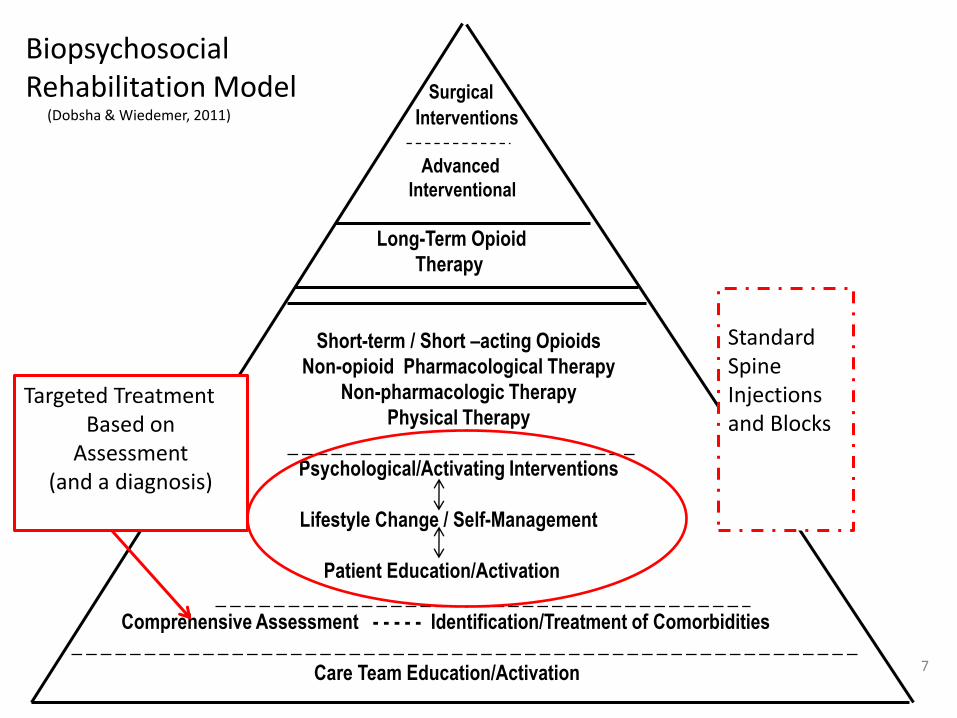
Surgical
Interventions
Advanced
Interventional
Long-Term Opioid
Therapy
Short-term / Short –acting Opioids
Non-opioid Pharmacological Therapy
Non-pharmacologic Therapy
Physical Therapy
Psychological/Activating Interventions
Lifestyle Change / Self-Management
Patient Education/Activation
Comprehensive Assessment - - - - - Identification/Treatment of Comorbidities
Care Team Education/Activation
Biopsychosocial Rehabilitation Model (Dobsha & Wiedemer, 2011)
Targeted Treatment Based on
Assessment (and a diagnosis)
Standard Spine Injections and Blocks
7

Culture of “Cure” Reliance on the biomedical model
Urgent and absolute pain relief: appropriate in acute and cancer pain
Acute/Cancer strategies are inappropriate for chronic pain management
Strategies for Chronic Pain Management → Biopsychosocial Model of care
Rehabilitation
Restoring and preserving function
pain 8

Practice Strategies that are standardized and applicable to ALL patients
“Universal Precautions” • Comprehensive Assessment
• Identification of Pain Diagnosis and co-morbidities
• Careful patient selection using Risk – Benefit framework • Be aware of relative and absolute contraindications listed
in VA/DOD guidelines • Do the benefits of opioid therapy outweigh the untoward
effects and risks for this patient at this time ( “Opioid Risk Evaluation” Note)
• TRIAL of opioid therapy with adjuvant therapy • Plan an exit strategy before starting therapy • Discuss reasonable dose limitations
• Informed Consent/Treatment Agreement
Gourlay & Heit, 2005; VA/DOD Chronic Opioid Therapy CPG,2010
9

Practice Strategies that are standardized and applicable to ALL patients
“Universal Precautions”
• Regular MONITORING: • Regularly assess “4 A’s” : Analgesia, Activity(FUNCTION), Adverse
Reactions, Aberrant Behaviors
• Urine Drug Testing
• Minimum of every six months
• *Need for reliable follow up by PACT team members (No alert for abnormal test)
• Proper interpretation
• DOCUMENTATION • Degree of Analgesia (0-10 scale or other scale acceptable to patient)
• Opioid related side effects
• Functional Status (e.g. physical activities, social functioning, etc.)
• Existence or absence of aberrant behaviors
Gourlay & Heit, 2005; VA/DOD Chronic Opioid Therapy CPG,2010
10

Interpreting the Drug Abuse Urine (DAU) Results
Opioid Prescribed Expected results on DAU
Confirmatory Test GC/MS
Metabolites reported
How long will drug be detected after last
dose?
Codeine
Opiate: positive codeine norcodeine
1-2 days
Hydrocodone (Vicodin)
Opiate: positive * hydrocodone hydromorphone
1-2 days
Hydromorphone (Dilaudid)
Opiate: positive* hydromorphone 1-2 days
Fentanyl
Opiate: negative Can only be detected by GC/MS test. Result reported: Fentanyl confirmed by GC/MS
2-3 days after patch taken off
Methadone
Opiate: negative Methadone: positive
methadone 2-3 days
Morphine
Opiate: positive morphine 1-2 days
Oxycodone
Opiate: usually ** negative
oxycodone oxymorphone
2 days
11
12
* Screening technology is very sensitive in detecting codeine and morphine, not so with hydrocodone or hydromorphone i.e. if low concentration, opiate screen may be reported as non-detected, necessitating follow-up with confirmation(GC/MS). ** Oxycodone: in most screens, opiate will be negative. It may be positive with oxycodone screen used in Philadelphia and Pittsburgh. Take Home: Understand the technology (strengths and limitations) before making clinical judgment. If screening test is ambiguous, follow-up with confirmation (GC/MS) How to detect tampering with urine: Direct observation with select patients, quality of urine specimen based on appearance, temperature, pH, urinary creatinine, and specific gravity. (Chain of custody not required in clinical settings) Some urine drug tests report creatinine and pH Creatinine normal > 30 ( less than 30 is diluted) pH normal 4.5-8

Detection Periods for drugs in urine
13
Amphetamine-High degree of false positives on DAU 1-2 days
Methamphetamine Up to a week
Barbiturates Short acting (i.e. secobarbital) Long-acting (i.e. Phenobarbital)
1 day 2-6 weeks
Cocaine Parent Metabolite
5 hours 2-4 days
Heroin 6-acetyl-morphine Breaks down to morphine
6-8 hours 1-2 days
THC 1 joint 3 x a week Daily
2 days 2 weeks 3-6 weeks or longer
PCP (Phencyclidine) 2-14 days
Benzodiazepines If long-acting and chronic use
3-5 days up to 3-6 weeks
Methadone 2-3 days
Morphine 1-2 days
Codeine 1-2 days
Oxycodone Metabolite: oxymorphone
1-2 days 1-2 days after oxycodone
Fentanyl
2-3 days
Hydromorphone 1-2 days
Hydrocodone 1-2 days
Propoxyphene Metabolite
24 hours up to 4 days

Case presentation: points for discussion • Models of care have emerged from PACTs across the VHA who
have tackled the challenge of chronic pain management
• Utilizing PACT team members to fullest extent
• Realigning resources
• Chronic Disease Model
• As we go through this case, think about what role various members of the PACT could take on to improve outcomes and lighten the load
14

Case • 57 yo with arthritis-> knees, neck and low back and muscle
pain on high dose opioids ( > 14 years)combined with valium and zolpidem
1) Migraine headaches- not currently an issue
2) PTSD/Depression
3) Obesity- BMI 31
4) Memory issues
5) Tobacco use
6) Hypogonadism
7) Osteoarthritis
8) Insomnia
9) Anxiety ? has been on valium
15

Patient was couch bound. Function had deteriorated over the last 5 years. The VA was paying for Home Health Aide to come 3 days/week to help him with bathing
• He was unable to perform the simplest tasks at home.
• Lives alone
• No history of any substance abuse or addiction issues
• No history of any aberrant drug related behaviors
• Patient was very frustrated by his disability
16

History
• “I have a number of issues…it’s always the same, the knees, the neck, the back are the three main areas of pain”
• Assessment of pain:
• Axial spine pain with occasional LE radiation; B/L throbbing knee pain, standing and walking make it worse, nothing much helps to alleviate the pain, no red flags
• Assessment of level of function:
“I don’t function well at all”, attributes it to his pain levels.
Has a home health aide for help bathing
17

Pain Management Regimen: 1) Fentanyl patch 100mcg q 3 days
2) Morphine IR 45 mg qid
3) Valium 10 mg QID
4) Zolpidem 10 mg at HS
5) Cymbalta 60 mg BID
Approximately 400 mg morphine equivalents / day
Note in remote data states that patient takes 10-20 mg of valium with zolpidem and his opioids at night to help him sleep
18
19
Poll Question

Primary Care Provider Assessment and initial approach:
• We discussed: • the side effects of the meds he is on which almost certainly are
exacerbating a number of his problems
• use of opioids on a chronic basis increases in some patients- tolerance, lower pain threshold, opioid induced hyperalgesia, constipation, depressed mood, decreased testosterone, respiratory depression, decreased immunocompetance
• Long-term studies of those prescribed opioids on a chronic basis show they suffer from a lower quality of life and higher rates of depression
• “vicious cycle” of chronic pain-> depression -> opioids-> continued pain -> more depression -> decrease in function
• there is emerging evidence that patients with chronic long-term pain do better with evidence-based nonpharmacologic treatments with lower dose opioids or no opioids
20

Recommendations:
• Safety Issues
1) Dose related overdose on 400 mg morphine eq/day with concomitant benzodiazepine use
2) Opioid related side effect
-He describes memory issues
-Hypogonadism likely related to opioids -> low energy, risk of osteoporosis
-Hyperalgesia is also possible
• Arthritis/axial back pain/myofascial pain are weak indications for opioids
• He acknowledges that he has not had any functional benefit, which is the primary reason to continue opioid therapy 21

Opioid dose in relation to OD rate
22
Recommendations: • We choose not continue this dangerous regimen, with no functional
benefit
Options:
Inpatient detox ( if available)
Outpatient opioid taper – there are a number of options
1) Convert to Morphine SA 60 mg TID for 1 month
60 mg BID for 1 month, 30 mg TID for 1 month, 15mg BID x 1 month then reassess
Continue morphine IR 15 mg qid for a few months
2) Taper with Fentanyl if you have 12 mcg patches available
3) Could also taper with methadone
4) Detox with suboxone 23

Outcome: • Patient came in for inpatient detox
• Placed on Gabapentin with quick titration to 600mg TID, valium was tapered
• Fentanyl was stopped
• Discharged on morphine sa 15 mg tid and morphine IR 15 mg BID prn
• Primary Care Visit 2 weeks after discharge • Pain was 2/10, at times increases to 5-6/10 with activity
• Exam: normal neurological exam, some lumbar facet tenderness
• Treatment Plan • Etodolac 300mg TID prn. NSAID risk of GI, renal, CV issues discussed
• Chair exercises given for home, will consult PT for reconditioning
• Weight loss discussed- MOVE program
• CBT for chronic pain referral
• Update MRI consider referral for facet injections
24

Outcome: • Long-term: improving mobilization, self-care with weight loss,
exercise CBT
• Discussed goal of keeping opioids at low dose
Patient expressed gratitude for my trying to help
“no one ever talked to me like this or offered other options. At the other VA they just kept uping my dose when I said I was still in pain”
25

Tapering opioids (VA/DOD CPG )
1.Rate of taper should be based on degree of risk • Decisions regarding tapering schedule should be made on an individual basis; faster
or slower taper may be warranted • In general, the longer the patient has been on opioids, the slower the taper should be • If there are clearly unsafe or illegal behaviors, opioid prescribing should be stopped
immediately and withdrawal addressed
2. For patients who are at high risk for aberrant behaviors ( threatening suicide, severe impulse control disorders, high dose illicit or unprescribed drugs) refer to Mental Health/ Addiction specialist 3. There is no single protocol that has been proven more efficacious than another Taper by 20-50% per week* of original dose initially then steady 10-25% decrease * could be q 2 -4 weeks for slower taper 4. Patient Education is essential to successfully taper:
• Clear written and verbal instructions given to patient and families about taper protocol
• Reassurance that the team will continue to work with them to manage their pain
26
Tapering opioids
• Medications to ease withdrawal • Autonomic symptoms: Clonidine 0.1 mg 2-3 times daily
• Anti-diarrheal agents: Loperamide (Imodium)
• Anti-emetic: hydroxizne and promethazine
• Abdominal cramps: dicyclomine (Bentyl)
• Muscle cramping: methocarbomol, baclofen
• Physical signs of withdrawal typically resolve after 7-10 days
• It is important for patients to understand that psychological & psychosomatic sequelae can last up to a year
→ insomnia, weakness, nervousness, muscle weakness and aches
27

How to “screw-up” a patient encounter
Provider to patient: “The government is cracking down on high dose opioids, we are going to have to lower your dose”
COMMUNICATION !! Review: Talking points for PCPs from San Francisco VA 28

Some examples from the SFVA “Talking to patients about Chronic Pain and Opioid Risk”
• Living with chronic pain is difficult, but I believe you can have a better quality of life
• I’m committed to working with you to manage your pain. I need you to know if you are not able to keep to the regimen we discussed, I will not be willing to continue prescribing this medication
• I hear what you are saying. Unfortunately we may have to agree to disagree
• Unfortunately, the way you have been using this medication has actually become a barrier to safe and effective pain management
29

In summary
• Opioids …..
• Can be effective in improving pain and function in some patients
• Can be harmful for some
• Can be prescribed safely
• PACTs…
• Collaboration of PCP, Pharm D, RN, Mental Health-Primary Care Integration, PT/Rehab
• All promoting self-management , goal setting
• Care management of pain and depression
• Standardized Opioid Prescribing and Renewals
• Should we think of “Care Management” for patients on chronic opioids ??? Nurse Clinics, PACT Pharmacists
30

Talking to Patients about Chronic Pain and Opioid Risk
31
Having "The Conversation"
Tip: Choose your tools based on your patient's level of resistance/readiness ___________________
Helpful Statements:
What would you like to have happen today?
I am committed to helping you with your pain mgmt plan.
I know you have real pain.
Our goal is to help you function better and live a better quality of life.
Good mood mgmt is good pain mgmt.
Opioid withdrawal is self-limiting and not life-threatening. The symptoms can feel pretty awful sometimes, but they're not physically dangerous and we can help you manage them.
LESS RESISTANT: use realistic, supportive and Motivational Interviewing talk. At best, medications can only address 30-50% of chronic pain. You will need a comprehensive pain mgmt plan. Living with pain is difficult, but I believe you can have a better quality of life. A person with chronic pain is like a care with four flat tires. Medications can fill one of those tires. But to really get moving, to have better functioning and QoL for the long run, you will need to take a wrap-around approach. I'd like to help you with that. So part of you does not like the effects of this medication and would like to take less of it. What is the biggest barrier to trying a change? What part of making a change worries you the most? On a scale of 0 to 10, how important do you think it is to find other ways to manage this pain? From 0 to 10, how ready are you to try a different approach? What would help you get that closer to a [8,9]? What can I do to help? I want to support you to become the expert manager of your pain program. I'd like to hear your ideas about where you think we need to go from here... With your permission I'd like to share my recommendations with you. When to consider adding psychological support: 1) Some anxiety or irritability is normal when patients with pain are being considered for an opioid taper. However, if a patient conveys severe anxiety or anger about taper, consider adding psychological support to the process. 2) Patient has a history of suicidal ideation or attempts. 3) Patient has a history of addiction or is currently abusing substances. 4) Patient's only tool for pain mgmt has been opioids. 5) Patient expresses interest in integrative pain mgmt
VERY RESISTANT: be direct and clear about limits. I'm committed to working with you to manage your pain. I need you to know that if you are not able to keep to the regimen we discussed, I will not be willing to continue prescribing this medication. I cannot responsibly continue to prescribe opioids because I feel that they are causing you more harm than good. I can see that you are really struggling with the pain. But sometimes the things we do to control pain are actually more dangerous than the pain itself. The choices you're making now are actually putting you in danger, and I cannot support that. Unfortunately, the way you have been using this medication has actually become a barrier to safe and effective pain management. I hear what you're saying. Unfortunately we may have to agree to disagree about this. Many people have real pain AND addiction [or, AND real problems regulating their medication use]. A good pain management plan has to balance safety and effectiveness. If the risks outweigh the benefits, it's not good medicine. I would like to work with you to find better ways to manage your pain and need for pain medications. Discussing behavioral health referrals: Coping skills are a first-line treatment for any chronic illness. I would like to bring in a colleague who can help with that. I think you could use a higher level of support for your pain. I'd like to take a team approach. Chronic pain is very stressful, and stress can in turn increase pain. To take a comprehensive approach to your care, I'd like to connect you with a colleague who specializes in managing stress and anxiety.