Pain management in chronic pancreatitis: A treatment algorithm
13
9 Pain management in chronic pancreatitis: A treatment algorithm Shailendra Chauhan, Assistant Professor of Medicine, Chris E. Forsmark, Professor of Medicine, Chief * Division of Gastroenterology, Hepatology, and Nutrition, University of Florida, United States Keywords: Chronic pancreatitis Abdominal pain Therapy Endoscopy Surgery Neurolysis Abdominal pain is common and frequently debilitating in patients with chronic pancreatitis. Medical therapy includes abstinence from tobacco and alcohol and the use of analgesics and adjunctive agents. In many patients, a trial of non-enteric-coated pancreatic enzymes and/or antioxidants may be tried. Endoscopic or surgical therapy requires careful patient selection based on a detailed analysis of pancreatic ductal anatomy. Those with a non-dilated main pancre- atic duct have limited endoscopic and surgical alternatives. The presence of a dilated main pancreatic duct makes endoscopic or surgical therapy possible, which may include ductal decompression or pancreatic resection, or both. Randomised trials suggest surgical therapy is more durable and effective than endoscopic therapy. Less commonly employed options include EUS-guided coeliac plexus block, thoracoscopic splanchnicectomy, or total pancreatec- tomy with auto islet cell transplantation. These are used rarely when all other options have failed and only in very carefully selected patients. Ó 2010 Elsevier Ltd. All rights reserved. Introduction Abdominal pain is present in the vast majority of patients with chronic pancreatitis. The pancreas is richly innervated with dendrites of nociceptive neurons, whose cell bodies are in the dorsal root ganglia at spinal cord levels T5eT9. The mechanisms which lead to chronic pancreatitis, and in particular chronic inflammation in the gland, also lead to nociceptive nerve injury and activation, and * Corresponding author. Division of Gastroenterology, Hepatology, and Nutrition, University of Florida, Box 100214, Room HD 602,1600 SW Archer Rd, Gainesville, FL 32610-0214, United States. Tel.: þ1 352 273 9400; fax: þ1 352 392 3618. E-mail address: [email protected]fl.edu (C.E. Forsmark). Contents lists available at ScienceDirect Best Practice & Research Clinical Gastroenterology 1521-6918/$ e see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.bpg.2010.03.007 Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335
-
Upload
shailendra-chauhan -
Category
Documents
-
view
213 -
download
0
Transcript of Pain management in chronic pancreatitis: A treatment algorithm

Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335
Contents lists available at ScienceDirect
Best Practice & Research ClinicalGastroenterology
9
Pain management in chronic pancreatitis: Atreatment algorithm
Shailendra Chauhan, Assistant Professor of Medicine, Chris E. Forsmark,Professor of Medicine, Chief *
Division of Gastroenterology, Hepatology, and Nutrition, University of Florida, United States
Keywords:Chronic pancreatitisAbdominal painTherapyEndoscopySurgeryNeurolysis
* Corresponding author. Division of Gastroentero602, 1600 SW Archer Rd, Gainesville, FL 32610-021
E-mail address: [email protected] (C.E
1521-6918/$ e see front matter � 2010 Elsevier Ltdoi:10.1016/j.bpg.2010.03.007
Abdominal pain is common and frequently debilitating in patientswith chronic pancreatitis. Medical therapy includes abstinence fromtobacco and alcohol and the use of analgesics and adjunctive agents.In many patients, a trial of non-enteric-coated pancreatic enzymesand/or antioxidants may be tried. Endoscopic or surgical therapyrequires careful patient selection based on a detailed analysis ofpancreatic ductal anatomy. Those with a non-dilated main pancre-atic duct have limited endoscopic and surgical alternatives. Thepresence of a dilated main pancreatic duct makes endoscopic orsurgical therapy possible, which may include ductal decompressionor pancreatic resection, or both. Randomised trials suggest surgicaltherapy is more durable and effective than endoscopic therapy.Less commonly employed options include EUS-guided coeliacplexus block, thoracoscopic splanchnicectomy, or total pancreatec-tomywith auto islet cell transplantation. These are used rarelywhenall other options have failed and only in very carefully selectedpatients.
� 2010 Elsevier Ltd. All rights reserved.
Introduction
Abdominal pain is present in the vast majority of patients with chronic pancreatitis. The pancreas isrichly innervated with dendrites of nociceptive neurons, whose cell bodies are in the dorsal rootganglia at spinal cord levels T5eT9. The mechanisms which lead to chronic pancreatitis, and inparticular chronic inflammation in the gland, also lead to nociceptive nerve injury and activation, and
logy, Hepatology, and Nutrition, University of Florida, Box 100214, Room HD4, United States. Tel.: þ1 352 273 9400; fax: þ1 352 392 3618.. Forsmark).
d. All rights reserved.

S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335324
to abdominal pain. There is no single or even pathognomonic characteristic pattern of pain. Many, butnot all, patients may initially present with episodes of pain, interspersed with periods of feelingrelatively well. These episodes may be severe enough to require hospitalisation, and during this periodthe patient may be labelled as having acute pancreatitis. In these earlier stages, evidence of acutepancreatic inflammation (visible on computed tomography or associated with elevations in serumamylase or lipase) may be present. Pain can continue to occur in discrete episodes, but often becomesmore chronic or even continuous, although superimposed exacerbations may still occur. These exac-erbations, as the disease progresses, may no longer be associated with features of acute pancreaticinflammation. Pain is often felt in the epigastric region, with radiation to the back inmany patients, andis often made worse by eating. Nausea and vomiting are commonwhen pain is severe. Although thesefeatures describe a common pain pattern, the pain can be quite variable in its location, duration,pattern, and severity. The natural history of pain is also quite variable. Some studies have noted thatpainmay decrease over time inmany patients as the disease reaches its later stages, although this is notuniversal and is difficult to predict. This variable pattern and natural history make it very difficult tojudge efficacy of therapy.
Abdominal pain is the symptom of chronic pancreatitis which most affects quality of life. Numerousquality of life analyses in these patients note that pain dominates the quality of life indices in all majorspheres [1,2]. Interestingly, the maximum severity of pain may not be the most bothersome feature, asthose with episodic severe pain experience somewhat less deterioration in quality of life than thosewith a continuous and constant pain of lesser severity.
Chronic pancreatitis appears to evolve as a consequence of episodes of acute pancreatitis [3],although these episodes may not be clinically apparent. During this process, the acute inflammation,necrosis, and apoptosis of acute pancreatitis are gradually replaced by chronic inflammation. Thischronic inflammation drives the response towards the activation of pancreatic stellate cells, fibrosis,and the eventual destruction of ductal, acinar, and islet cells. As the disease evolves, thesemore chronicand irreversible changes become manifest. In the later stages of the disease, visible evidence of thisprocess is easily seen on imaging studies; which might document pancreatic duct dilation and irreg-ularity, gland atrophy, or pancreatic calcifications. These features take years, and sometimes decades, todevelop. During the time that they are developing, however, pain may be severe. Patients in earlierstages of chronic pancreatitis may have pain, but not have obviously identifiable abnormalities onimaging studies. As such, these patients may be difficult to diagnose using readily available diagnostictools like computed tomography (CT) or magnetic resonance imaging and cholangiopancreatography(MRI and MRCP).
There are numerous potential causes of pain. Endoscopic or surgical therapy for pain often has as itsgoal relieving an obstruction in the pancreatic duct or decompressing the pancreatic duct. One popularhypothesis has been that pain is caused by ductal obstruction. The expected result of ductal obstructionwould be increased pressure within the duct and the gland, particularly during periods of stimulationof pancreatic secretion (e.g. after meals). This increased pressure could produce pain by increasingbasolateral secretion of enzymes (rather than apical against the high pressure), or by causing ischaemiawithin the pancreas by raising pressure to levels which interfere with the blood supply. There isevidence from both animal models and human studies that patients with chronic pancreatitis can haveelevated pressures in the duct or in the parenchyma of the pancreas, and that surgical therapy isassociated with a decrease in this pressure and with pain relief [4,5]. Animal models of chronicpancreatitis also demonstrate that with stimulation of pancreatic secretion, blood flow goes down andischaemia develops, mimicking a compartment syndrome. While this mechanism for pain seemsplausible, other studies have found no clear relationship with pressure and pain or with pressurereduction and pain relief [5].
Evidence continues to accumulate that pain may also be caused via nerve injury and a neuro-immune interaction between neuronal processes and the chronic inflammation [5,6]. Histologicalevidence of injury to neuronal processes is commonly seen in chronic pancreatitis, but evidence is alsomounting that inflammatory mediators may also serve as nociceptive triggers. In addition, as in manychronic pain states, a central neuropathic component can develop. Nociceptive nerves within thepancreas are injured and become abnormal early in the course of chronic pancreatitis. The innervationof the pancreas is complex, and involves both somatic-visceral and autonomic nerves. Neural processes

S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335 325
in the pancreas and pancreatic bed can be activated by heat, pressure, acid, inflammatory cells andmediators, and products of cellular necrosis. The nerve signal travels through the coeliac nerve plexusand then along both left and right greater splanchnic nerves to the cell bodies located in the dorsal rootganglia at spinal cord levels T5eT9. Animal models of chronic pancreatitis and evidence from humanstudies in patients with chronic pain syndromes, including chronic pancreatitis, demonstrate thedevelopment of hypersensitivity or sensitisation of the pain perception [5e8]. These patientsdemonstrate hyperalgesia (increased pain from stimuli which are normally noxious) and allodynia(pain from stimuli that are not normally noxious). This sensitisation occurs not only in the peripheralnociceptive nerve processes in the pancreas, but also in the spinal cord and brain. The central nervoussystem plasticity and neural remodelling is likely just as important as the local (pancreatic) neuralremodelling that occurs in chronic pancreatitis [8]. This process involving both peripheral and centralneurons is demonstrated quite clearly by the patient who does not note pain relief after therapieswhich interrupt neural transmission (coeliac plexus neurolysis or splanchnicectomy) or by theunfortunate but not uncommonpatient who continues to have pain even after the pancreas is removed(total pancreatectomy). A final potential cause of pain is due to hormonal changes, particularlyelevation in cholecystokinin (CCK). CCK is elevated in some patients with chronic pancreatitis, and CCKstimulates the pancreas to secrete a protein rich fluid. In the setting of pancreatic ductal obstruction inlarge or small-ducts, high levels of CCK could drive basolateral secretion of enzymes or could raisepressurewithin the duct or gland, augmenting ischaemia and potentially causing pain. This mechanismis similar to the proposed mechanism of pain due to ductal obstruction underpinning endoscopic andsurgical therapy. Decreasing CCK and reducing pancreatic secretion is the proposed mechanism for theaction of pancreatic enzymes or octreotide in reducing pain. These complex mechanisms of pain arenot mutually exclusive. No one therapy is effective in all patients, which would be expected when oneconsiders the different potential causes of pain.
Pain management
The first step in managing patients with pain presumed to be due to chronic pancreatitis is to makesure that the diagnosis of chronic pancreatitis is correct. In patients with longstanding disease, this isnot difficult as widely available diagnostic tests such as CT, MRI/MRCP, or endoscopic ultrasonography(EUS) will document the presence of structural damage to the pancreas including such features aspancreatic duct dilation, strictures, or irregularity; pancreatic gland atrophy; or calcifications withinthe duct or the parenchyma (Figs. 1 and 2). These features usually take years to develop. Diagnosis isnot so straightforward in those with early chronic pancreatitis. These patients may not have thisevidence of structural damage and yet still have pain, driven by the chronic inflammation and neuralinjury. As the pain of chronic pancreatitis is not uniform in its character, it may be difficult todetermine if a patient is suffering from early chronic pancreatitis or some other condition. Patientswith chronic pancreatitis may be classified as to whether they have these advanced structuralabnormalities (often called ‘big-duct’ disease) or do not (often called ‘early’ or ‘small-duct’ or ‘minimalchange’ chronic pancreatitis). Making a correct diagnosis in these patients with small-duct disease iscritical, although difficult. The best approach involves the use of endoscopic ultrasonography andhormonal stimulation pancreatic function testing [9e11]. Although it is not the subject of this review,this is an important concept and one that poses often substantial diagnostic confusion. We see manypatients who are labelled as having ‘chronic pancreatitis’ based on a compatible pain syndrome(perhaps complemented by periodic low-level elevations in amylase or lipase) in the absence ofabnormalities on imaging studies, and in whom subsequent investigation demonstrates a normalpancreas. It is obviously inappropriate to label these patients with an incorrect diagnosis, given theobvious implications on insurability and state of mind. It is even more obvious that treating thesepatients with expensive or risky therapy directed at chronic pancreatitis, in the absence of a securediagnosis, is equally inappropriate. The interested reader is referred to the above noted referenceswhich review this important topic.
The second step in managing pain is to search for a disease state or complication related to chronicpancreatitis that might be causing pain. These conditions include diseases which occur at increasedfrequency in those with chronic pancreatitis, including pancreatic carcinoma [12] and gastroparesis.

Fig. 1. An EUS image demonstrating a large stone (arrow) within a dilated pancreatic duct.
S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335326
They also include complications of the pancreatitis itself, including pseudocyst, duodenal obstruction,and possibly biliary obstruction. The latter two conditions may develop due to either progressivepancreatic fibrosis or a pseudocyst obstructing a surrounding organ. Pain associated with pancreaticcarcinoma, pseudocyst, or duodenal or biliary obstruction will often respond to therapy directed atthese specific conditions. An up-to-date and high-quality CT scan or MRI is usually appropriate to makesure these conditions are not present. In addition, the imaging study will provide evidence ofpancreatic duct diameter and allow classification of patients as having big-duct or small-duct chronicpancreatitis. Finally, as pain patterns and character are so variable, it is worth spending some timewiththe patient (or having them fill out a pain diary) to develop a clear understanding of the pattern of painin that individual patient.
The distinction between big-duct and small-duct chronic pancreatitis has very important impli-cations for guiding therapeutic choices. While medical therapy may be applied to all patients, mostendoscopic and surgical therapy is only appropriate for those with big-duct disease. The definition ofbig-duct disease is not standardised, but usually means dilation of themain pancreatic duct in the bodyof the pancreas to at least 5 mm. This amount of duct dilation is felt to be the minimal to allow rela-tively easy identification of the duct at the time of surgery. It is not possible to estimate the relativeprevalence of big-duct compared to small-duct disease, as many patients with small-duct disease goundiagnosed. Even in those with big-duct disease, the endoscopic and even surgical options may belimited by features of the ductal anatomy which make particular approaches more or less feasible. Asan example, those with a dilated duct and a single dominant stricture or stone in the head of the glandare most amenable to endoscopic therapy. Thosewithmultiple strictures or stones, particularly if theseare in the body or tail of the gland, are generally not amenable to endoscopic therapy even though theyhave big-duct disease. Choosing therapy requires not just a general knowledge of the differencebetween big and small-duct disease but detailed information on ductal anatomy.
Medical therapy
Medical therapy is appropriate in all patients with chronic pancreatitis. In those who drink alcohol,strong efforts to encourage abstinence are essential. In those with alcohol-induced chronic pancrea-titis, cessation of alcohol appears to slow the continued progression of disease. In addition, abstinencemay have beneficial effects on pain [5,13]. Finally, stopping alcohol prolongs survival in these patientsand has important benefits to quality of life. Studies have demonstrated that adopting an activeapproach to encouraging abstinence, including referral to appropriate counselling and support, ismuchmore effective than simple office-based advice [14]. There is accumulating evidence that tobaccouse is also an important risk factor for chronic pancreatitis and may have equal potency as alcohol

Fig. 2. (a) It demonstrates a massively dilated pancreatic duct with severe gland atrophy and a few visible calcifications. (b) Itdemonstrates ductal dilation with larger pancreatic duct stones.
S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335 327
[15,16]. Smoking is certainly associated with multiple other diseases and dramatically shortens life.Equally strong efforts to encourage patients with chronic pancreatitis to stop smoking are recom-mended, although the evidence supporting smoking cessation and pain relief are scanty.
Most patients will require some form of analgesic agent. There is unfortunately some risk of narcoticdependence or diversion, but this risk should not take precedence over efforts to relieve pain. Lower-potency narcotic analgesics are most appropriate as initial therapy. Studies have shown that the agenttramadol can be equivalent to more potent narcotics, with less potential for addition or diversion andless impact on gastrointestinal motility [17]. An alternative agent of low potency is propoxyphene(often coupled with acetaminophen). It is important to establish a solid doctor-patient relationshipprior to initiating even these lower-potency agents, and to alert the patient that the overall goal is
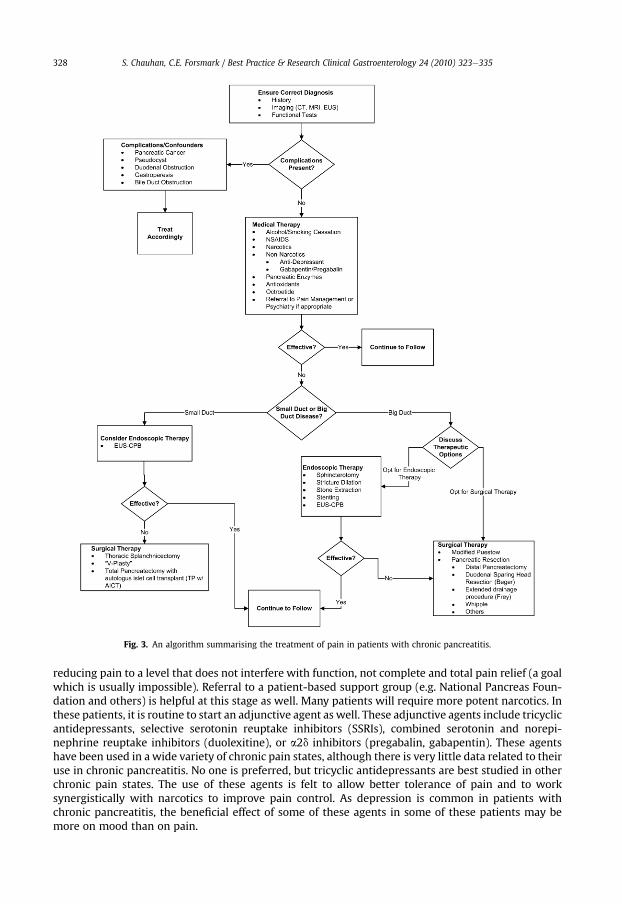
Fig. 3. An algorithm summarising the treatment of pain in patients with chronic pancreatitis.
S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335328
reducing pain to a level that does not interfere with function, not complete and total pain relief (a goalwhich is usually impossible). Referral to a patient-based support group (e.g. National Pancreas Foun-dation and others) is helpful at this stage as well. Many patients will require more potent narcotics. Inthese patients, it is routine to start an adjunctive agent as well. These adjunctive agents include tricyclicantidepressants, selective serotonin reuptake inhibitors (SSRIs), combined serotonin and norepi-nephrine reuptake inhibitors (duolexitine), or a2d inhibitors (pregabalin, gabapentin). These agentshave been used in awide variety of chronic pain states, although there is very little data related to theiruse in chronic pancreatitis. No one is preferred, but tricyclic antidepressants are best studied in otherchronic pain states. The use of these agents is felt to allow better tolerance of pain and to worksynergistically with narcotics to improve pain control. As depression is common in patients withchronic pancreatitis, the beneficial effect of some of these agents in some of these patients may bemore on mood than on pain.

S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335 329
Pancreatic enzymes are not infrequently used in an attempt to reduce pain. The use of enzymes ispredicated on the observation that serine proteases delivered in an active form to the duodenum willdecrease the release of cholecystokinin (CCK) from the duodenum. This reduction in CCK will produceless stimulation to pancreatic secretion of enzymes. In situations where the CCK level is high (as it is insome patient with chronic pancreatitis), it could produce hyperstimulation of the pancreas and thiscould cause pain by raising pressure in the setting of pancreatic ductal obstruction (producingischaemia), or by causing basolateral secretion rather than apical secretion of enzymes, or both. Thishypothetical mechanism of pain relief is similar to the proposed mechanism of pain relief fromendoscopic or surgical duct decompression. Providing active proteases in the feedback-sensitiveportion of the small intestine (duodenum) can reduce CCK and reduce pancreatic secretion, and inthis way potentially reduce pain. The delivery of activated serine proteases to the duodenum is onlypossible with non-enteric-coated enzymes (tablet form). Enteric-coated preparations do not releaseactivated proteases until they reach the jejunum or even ileum. There have been several small rand-omised placebo-controlled trials assessing the ability of pancreatic enzymes to reduce pain. Two smallstudies using non-enteric-coated enzymes demonstrated a reduction in pain. Three other studies usingenteric-coated preparations showed no improvement in pain. Ameta-analysis was performed on thesetrials and reached the conclusion that enzymes are ineffective for pain [18]. This type of analysis maynot provide clear guidance, however, if the hypothesis of the mechanism of pain relief from enzymes iscorrect and only one type of enzyme product is effective. Practice guidelines do include a trial ofenzyme therapy as a reasonable choice in managing pain in these patients [19] and many patientsundergo a trial of enzyme therapy for pain. Nonetheless, the use of enzymes for this purpose iscontroversial and the overall efficacy not well defined. If a therapeutic trial is undertaken, it should usea non-enteric-coated preparation (e.g. Viokase-8� or Viokase-16�) in sufficient dose (8 or 4, respec-tively, with meals and at night) and co-treatment with an agent to reduce gastric acid to prevent theproteases being denatured by gastric acid (H2-blocker or proton pump inhibitor). A trial of 6e8 weeksis usually sufficient to determine response of pain to enzyme therapy.
Antioxidants have been used to treat the pain of chronic pancreatitis. This therapy was consideredas potentially effective sincemarkers of oxidant stress can be seen in patients with chronic pancreatitis,and oxidative stress has been proposed to play a role in the pathogenesis of pancreatic injury. Severalsmall observational studies suggested benefit. A recent randomised placebo-controlled trial of anti-oxidants demonstrated modest benefit [20]. A mixture of selenium, methionine, vitamins E and C, andb-carotene is used.
Octreotide, an analogue of the native hormone somatostatin, will reduce CCK levels and suppresspancreatic secretion. This action is similar to the proposed mechanism of action of non-enteric-coatedpancreatic enzymes. Several small studies have reached differing conclusions. The largest study,available only in abstract form, noted only a trend towards benefit. The drug is used rarely in thiscondition, and usually only after all other therapies have failed. The short acting form of the drug isusually tried first, administered in a dosage of 100 mcg SQ tid and escalating up to 200 mcg tiddepending on response. If the short acting form is effective, a long acting depot form can be substituted.Complications include biliary stasis and gallstone formation. The drug is not approved by the FDA forthis indication.
Nerve block and neurolysis
In patients who do not achieve sufficient pain relief from medical therapy, non medical therapiescan be considered. One such option is nerve block or neurolysis. Pancreatic nociceptive afferents passthrough the coeliac ganglion and the greater splanchnic nerves to the spinal cord and brain. Coeliacplexus block can be achieved by injecting an anaesthetic (often coupled with a steroid) into the area ofthe coeliac plexus under radiographic (CT) guidance or endoscopic guidance (utilising EUS). Coeliacneurolysis is performed by injecting absolute alcohol using similar approaches, with intent topermanently destroy these neuronal processes. EUS-guided and CT-guided approaches have beencompared in randomised trials [21,22]. EUS-guided techniques are safer, more effective, and moredurable than CT-guided techniques. These techniques are utilised more commonly in those withpancreatic carcinoma than in chronic pancreatitis. Coeliac nerve block has a transient effect, with pain
S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335330
returning after several weeks or months. While this may be sufficient for those with malignant diseaseand a short anticipated life span, patients with chronic pancreatitis usually outlive the effect of thenerve block. Nonetheless, it can be considered in thosewith chronic severe pain to provide a temporaryrespite from pain, during which time narcotic dosage or potency may be able to be reduced. Neurolysisis used occasionally in thosewith carcinoma but only rarely in thosewith chronic pancreatitis, and onlyin those who have had a significant benefit from a previous coeliac plexus nerve block. The use ofneurolysis in patients with chronic pancreatitis has not been sufficiently studied to be able to deter-mine its durability and efficacy [21e23].
Neurolysis can also be achieved by transection of the splanchnic nerves. The right and left greatersplanchnic nerve roots contain the same neuronal processes that traverse the coeliac plexus. They enterthe spinal cord over spinal cord levels T5eT9, which is the location of the cell bodies of these neuronalprocesses. Thoracoscopy allows access to these nerve roots, although not always over the entire T5eT9segments. The splanchnic nerves can be sectioned, using either a unilateral or a bilateral approach.Thoracosocopic splanchnicectomy provides pain relief in up to 80% of patients immediately, but morelong-term pain relief falls to less than 50% [24,25]. The reason for failure may be related to the fact thatbilateral splanchnicectomy may not always be performed, and by the fact that access to all nerve rootsmay not be feasible in all patients. The technique is used relatively rarely and generally as a last resort.
Endoscopic therapy and lithotripsy
In addition to EUS-guided coeliac plexus nerve block, therapy can be delivered by ERCP. Endoscopictherapy is directed at relieving obstructions within the pancreatic duct. It is important to note thatendotherapy for chronic pancreatitis can be quite challenging and technically demanding and that theresults are highly operator dependent. Results from specialist or expert centers cannot be generalisedto centers with less volume or experience. Some patients with chronic pancreatitis will develop ductalobstruction from a stricture of the duct or a stone obstructing pancreatic flow or both. Ductal stricturesand obstructing stones are not present in many patients with chronic pancreatitis and usually onlyoccur in the later stages of disease. They are particularly common in those with alcoholic or hereditarypancreatitis. It is an interesting feature of chronic pancreatitis that the presence of ductal strictures andstones does not correlate highly with the presence or absence of pain. One important feature thatmight imply that a stricture or stone is causing a functional obstruction to the duct would be that thereis dilation of the pancreatic duct upstream of the obstruction (Figs. 1 and 2). It is important tore-emphasise that there is not a direct relationship between the presence of duct dilation, pancreaticduct stones, pancreatic duct strictures, and abdominal pain. Many patients with these anatomicfeatures may not have pain. The proposed mechanism of pain in this setting which might respond toendoscopic therapy is elevated pressurewithin the pancreatic duct or the gland, although again there isno direct relationship between pressure and pain [5] and even those in whom pancreatic ductalpressure is elevatedmay have other contributors to pain. Endoscopic therapy would not be expected tohave any effect on pain due to nerve injury or hypersensitivity.
There are two main components of endoscopic therapy for pain. The first is dilation and stenting ofpancreatic duct strictures and the second is removal of main pancreatic duct stones. Both generallyrequire a pancreatic sphincterotomy and both usually require leaving a temporary pancreatic ductstent in place at the completion of therapy. Endoscopic therapy is most appropriate in those witha single obstructing lesion (stricture or stone) in a position that is most amenable to endoscopicmanipulation (close to the working tip of the endoscope). Ductal dilation upstream from thisobstruction is also an appropriate criterionwith which to select patients for endoscopic therapy. Stonesmay be removed if they are not too large (<1 cm in general), not too numerous, located in the mainduct, close to the working tip of the endoscope (in the head of the pancreas), are not tightly impacted,and if no stricture is present between the papilla and the stone. Many stones do not fit these criteriaand hence are not amenable to endoscopic therapy.
There are other endoscopic therapies whichmight be applied in these patients, including treatmentof associated pseudocysts, treatment of a benign stricture of the distal bile duct due to compressionfrom the fibrotic process in the head of the pancreas, or treatment of a pancreatic duct disruption.These techniques may in fact help pain in many patients as well but are not discussed further here.

S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335 331
The largest experience in endoscopic management of chronic pancreatitis is a large case series ofmore than 1000 patients from eight expert centers in Europe, with up to 12 years of follow-up [26].Endoscopic techniques include pancreatic sphincterotomy, stricture dilation, pancreatic ductal stent-ing, and stone extraction including lithotripsy. Although this retrospective study did not use stand-ardised definitions and measurement of success, 2/3 of patients had significant pain relief afterendoscopic therapy. Surgery was eventually required in ¼. These are a very select group of patientswith ductal anatomy that was amenable to endoscopic therapy, and a highly skilled group of endo-scopists. These patients underwent a median of 3 ERCPS but some had as many as 25. Systematicreviews of reports of endoscopic therapy have been performed and note that overall success in thesenon-randomised series is similar [27].
Endoscopic therapy is challenging and requires the highest level of experience and expertise. Unlikebile duct stones, pancreatic duct stones can be exceedingly difficult to extract with endoscopic tech-niques such as pancreatic duct sphincterotomy, intraductal lithotripsy, and balloon or basket extrac-tion. Extracorporeal shock wave lithotripsy (ESWL) can be quite helpful in reducing stones to a moremanageable size and in simplifying endoscopic extraction. An interesting randomised trial comparedESWL alone to ESWL followed by endoscopic removal of stones and found equal efficacy of pain reliefafter two years of follow-up [28]. This enigmatic result is difficult to reconcile with the generalaggressive approach to endoscopic therapy that has become common in recent times. It raises thepossibility that ESWL may have some ‘stunning’ effect on nociceptive neurons or some other mech-anisms of pain, separate from the obvious effect on stones.
Surgical therapy
Like endoscopic therapy, surgical therapy can be directed at decompressing an obstructed pancreaticduct and is usually considered in those whommedical therapy has been ineffective. Unlike endoscopictherapy, surgical therapy can also include resection of all or part of the pancreas. The most commonlyperformed surgical procedure is the modified Puestow operation or lateral pancreaticojejunostomy.This operation involves longitudinally incising the pancreatic duct from the anterior surface of thepancreas, usually beginning in the body of the pancreas and extending to as close to the duodenum as isreasonably accessible. Ductal strictures are incised as well, and any ductal stones can be removed.A Roux-en-Y anastomosis is created and the defunctionalized small bowel limb is used to cover thepancreatic incision. The conceptual underpinning of this operation is to remove any duct obstructionand reduce pressure within the duct and pancreas, which this operation certainly accomplishes. Short-term pain relief is seen in about 80% of patients. Long-term pain relief (over five years) drops to about50% [5]. This operation is usually only considered when the duct has dilated sufficiently to make it easyfor the surgeon to identify and incise, or >5 mm in diameter in the body of the pancreas.
Resection of all or part of the pancreas can also be performed. A variety of respective operations havebeen devised [29e32]. These often involve resection of the head of the pancreas. These more complexoperations are usually considered in those with a large inflammatory mass in the head of the pancreas,not infrequently causing biliary or duodenal obstruction. The classic pancreaticoduodenectomy (stan-dard Whipple operation or pylorus sparing) is one such operation but this surgery sacrifices extensivepancreatic parenchyma. A more limited pancreatic head resectionwith drainage of the upstream gland(duodenum sparing pancreatic head resection or Beger operation) and a more extended drainageprocedure combining a longitudinal incision of the pancreatic duct and excavation of much of thepancreatic head (Frey operation) were both developed for the management of chronic pancreatitis.Variations exist of thesewell-known operations [32]. In general, they are associatedwith similar rates ofimmediate pain relief, compared to the Puestow operation. Long-term pain relief appears to be better,although at the expense of more peri- and post-operative complications. In-hospital mortality for theseoperations is slightly less than 2% [32]. These operations are performed much more commonly inEurope than the US. These operations have been compared in randomised trials and appear to beequally effective and safe, when performed by experienced pancreatic surgeons [32].
Surgical and endoscopic treatments have similar underlying proposed mechanisms of pain relief.Two randomised trials have compared the results of endoscopic and surgical therapy for chronicpancreatitis [33,34]. Both are small and both can be criticised for several major methodological

S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335332
weaknesses. The first trial randomised 72 patients with painful chronic pancreatitis to endoscopictherapy or surgical therapy [33]. This represented about ½ of the eligible study population. Theendoscopic therapy was not overly aggressive as only ½ received a pancreatic duct stent and about ¼underwent stone extraction. ESWLwas not used. The surgical therapy in this trial was more aggressive,with 80% undergoing pancreatic resection and 20% undergoing amodified Puestowoperation. This trialdemonstrated that at five years of follow-up, twice as many patients randomised to surgery hadcomplete relief of pain (34% vs. 15%, p< 0.002). Body weight was also increased at the five year follow-up period in the surgical group, while the rate of diabetes mellitus was similar. Data is also presentedfrom this trial for the 1 year and 3 year time point, but this data is difficult to interpret as it includesboth randomised and non-randomised patients. The second randomised trial only included 39 patientsand the follow-up was only 24 months [34]. The endoscopic therapy was more complex, includinglithotripsy of stones as needed, and the surgical therapy was a standard lateral pan-creaticojejunostomy. This trial was ended early after an interim analysis demonstrated the superiorityof surgery. At 24months, those randomised to surgery had less pain and better quality of life. Completepain relief was seen in 40% of the surgical group and 16% of the endoscopic group, with partial in reliefin 35% and 16%, respectively. The short follow-up is important, as the efficacy of a lateral pan-creaticojejunostomy wanes over time [35,36].
These randomised trials, although imperfect and limited, suggest that surgical therapy is moreeffective andmore durable than endoscopic therapy for selected patients with chronic pancreatitis andappropriate ductal anatomy (i.e. a dilated pancreatic duct). There may, of course, be differences in thespeed with which pain is relieved or the later return of pain. It is important to discuss both thestrengths and weaknesses of the data with patients so that they can reach a decision most suited totheir situation and temperament. In our experience, when patients are presented with this informa-tion, they still often choose endoscopic therapy first due to a desire to avoid surgery.
There are other, less commonly performed surgical procedures for painful chronic pancreatitis. Thelateral pancreaticojejunostomy, which incises a dilated pancreatic duct, can be modified in thosewithout ductal dilation by performing a longitudinal V-shaped incision along the anterior surface ofthe gland down to or beyond the duct, and overlying this with a Roux limb. This ‘V-plasty’ has beenused in small numbers of patients [37] with acceptable results, but most surgeons are unfamiliar withthis technique. A final surgical option is total pancreatectomy, usually coupled with an attempt atharvesting of islet cells and reinfusion of these islets through the portal vein into the liver [38,39]. Theresults of this operation are variable. Up to 50% of patients still require narcotics after total pancrea-tectomy, reinforcing the very complex nature of pain in these patients. In addition, post-operativediabetes, which may be brittle, is relatively common. The likelihood of post-operative diabetes isdependent on the yield of islets from the gland. Prior pancreatic surgery, especially a lateral pan-creaticojejunostomy, seems to limit islet yield. Despite this, pancreatic surgery to treat pain shouldnever be avoided solely in anticipation of improving islet yield at total pancreatectomy if necessary inthe future.
Choosing therapy/algorithm (Fig. 3)
There is no single approach which is effective for all patients. Therapeutic options are unfortunatelylimited. Establishing a stable doctor-patient relationship is an important underpinning in managingany chronic illness and certainly any illness that causes chronic pain. Depending on the patient and theenvironment, it may be prudent to involve other care-givers including social workers, counsellors,psychologists, psychiatrists, support groups, or painmanagement clinics. Painmanagement clinics thatfocus on maximising the role of non-narcotic approaches are particularly helpful in this group ofpatients.
If a specifically treatable condition is found, including a pseudocyst, duodenal obstruction, orsuperimposed carcinoma, therapy directed at this condition is appropriate and may be successful inreducing pain. If not, medical therapy should be initiated. Initial medical therapy should include strongefforts to help the patient stop smoking and drinking, if applicable. This should include referral toappropriate specialists if one does not have expertise in this area. The initiation of narcotics shouldoccur only after a conversation with the patient outlining the chronic nature of the pain, the potential
S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335 333
risk of dependence and addiction, and the concept that the goal of narcotics is usually not completeabsence of pain but rather acceptable control of pain. Narcotic therapy should begin with lower-potency agents, either tramadol or propoxyphene. Initiation of a tricyclic antidepressant or, alterna-tively, a selective serotonin reuptake inhibitor (SSRI) should be considered early in the process asa method to stabilise mood and to improve the efficacy of narcotic analgesics. The initiation of anti-oxidants could certainly be considered at this early stage as a therapeutic trial. In those that remainsymptomatic, wewould recommend a trial of non-enteric-coated pancreatic enzymes together with anagent to reduce gastric acid. A trial of 6e8 weeks is appropriate in most patients to gauge response. Inthose with continued severe pain, increased potency and or dose of narcotic analgesics may berequired. If more potent agents are needed, co-treatment with a TCA or SSRI is very strongly recom-mended if it has not already been initiated.
In those with continued severe pain and small-duct disease, options are limited and include coeliacplexus block or neurolysis, octreotide, surgical V-plasty, or total pancreatectomy with attempts at isletcell autotransplantation. None of these is highly effective and in many patients continued attempts atmedical therapy is most appropriate. In those with large duct disease, a careful analysis of pancreaticductal anatomy with MRCP or ERCP is important in assessing the potential for endoscopic or surgicaltherapy. Decisions on therapy should take into account not only patient preferences but also availableexpertise and as part of a multidisciplinary clinical approach. In most cases, if surgical therapy ischosen, a lateral pancreaticojejunostomy is appropriate as it preserves the maximum amount ofpancreas. Surgical procedures which include pancreatic resection can be considered under certaincircumstances, such as those with a large inflammatory mass of the pancreatic head or with associatedduodenal or biliary obstruction.
Practice points
� Make sure the diagnosis is correct prior to initiating therapy� Look for complications of chronic pancreatitis which can also cause pain� Effective management of pain requires a team approach. Medical therapy should focusstrongly on alcohol and tobacco cessation.
� Treatment options vary depending on the pancreatic ductal anatomy and dilation. Thosewitha dilated pancreatic duct are most amenable to endoscopic or surgical therapy
� Surgical options for pain may be more effective and durable than endoscopic approaches
Research agenda
� The role of the central nervous system in perpetuating pain appears to be important but themechanisms and pathophysiology are unknown.
� The interactions between inflammatory cells and neurons needs to be understood to developnew targeted therapies
� We need better understanding of the various genetic and environmental factors whichpredispose to chronic pancreatitis or effect its clinical expression using a systems biologyapproach.
� Characterisation of pain patterns and better tools to assess response to therapy would allowus a better understanding of the effectiveness of therapy.
� Trials comparing the different forms of therapy are still needed.
Summary
Chronic pancreatitis commonly causes abdominal pain. Abdominal pain is the most frequentsymptom in these patients and the one that leads to themost deleterious effect on quality of life. Pain is

S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335334
also the most common reason for medical, endoscopic, or surgical intervention in these patients. Themechanisms by which pain is produced are speculative but include increased pressure within thepancreatic duct and gland, pancreatic ductal obstruction, ischaemia, nerve injury, and neuro-immuneinteractions between nociceptive neurons and the chronic inflammation in the gland. In addition, likemany chronic pain states, spinal cord and brain neural remodelling and plasticity can produce a cen-trally sensitised pain state which is self-perpetuating and does not respond to therapy directed at thepancreas. Finally, pain may develop from complications of chronic pancreatitis including pseudocyst,duodenal or biliary obstruction, gastroparesis, or superimposed pancreatic carcinoma. The manage-ment of pain is challenging. First, it is important to make sure the diagnosis of chronic pancreatitis iscorrect. Second, a search for specifically treatable complications such as pseudocyst or carcinoma isessential. In the absence of a specifically treatable complication, medical therapy is used first. Medicaltherapy includes abstinence from tobacco and alcohol and the use of analgesics and adjunctive agents.In many patients, a trial of non-enteric-coated pancreatic enzymes, and possibly antioxidants isreasonable. If medical therapy fails, attempts at endoscopic or surgical therapy require appropriatepatient selection based on pancreatic ductal anatomy and available expertise. Those with a non-dilatedmain pancreatic duct have limited endoscopic and surgical alternatives. The presence of a dilated mainpancreatic duct makes endoscopic or surgical therapy possible, which may include ductal decom-pression or pancreatic resection, or both. Small randomised trials perhaps suggest surgical therapy ismore effective and more durable compared to endoscopic therapy. Less commonly employed optionsinclude EUS-guided coeliac plexus block, thoracoscopic splanchnicectomy, or total pancreatectomywith auto islet cell transplantation. These are used when all other options have failed and only in verycarefully selected patients.
Conflict of interest
No conflict of interest has been declared by the authors.
References
[1] Pezilli R, Morselli-labate AM, Fantini L, et al. Assessment of the quality of life in chronic pancreatitis using SF-12 and EORTCQ1q-C30 questionnaires. Dig Liv Dis 2007;39:1077e86.
[2] Wehler M, Nichterlein R, Fischer B, et al. Factors associated with health-related quality of life in chronic pancreatitis. Am JGastroenterol 2004;99:138e46.
[3] Witt H, Apte MV, Keim V, Wilson JS. Chronic pancreatitis: challenges and advances in pathogenesis, genetics, diagnosis,and therapy. Gastroenterology 2007;132:1557e73.
[4] Fasanella KE, Davis B, Lyons J, et al. Pain in chronic pancreatitis and pancreatic cancer. Gastroenterol Clin North Am 2007;36:335e64.
[5] Lieb II JG, Forsmark CE. Review article: pain and chronic pancreatitis. Aliment Pharmacol Ther 2009;29:706e19.[6] AnapurthyR, Pasricha PJ. Pain and chronic pancreatitis. Is it the plumbingor thewiring?CurrGastroenterol Rep2008;10:101e16.[7] Dimcevski G, Sami SA, Funch-Jensen P, et al. Pain in chronic pancreatitis: the role of reorganization in the central nervous
system. Gastroenterology 2007;132:1546e56.[8] Drewes AM, Krarup AL, Detlefsen S, et al. Pain in chronic pancreatitis: the role of neuropathic mechanisms. Gut 2008;57:
1616e27.[9] Gleeson FC, Topazian M. Endoscopic retrograde cholangiopancreatography and endoscopic ultrasound for the diagnosis of
chronic pancreatitis. Curr Gastroenterol Rep 2007;9:123e9.[10] Forsmark CE. The early diagnosis of chronic pancreatitis. Clin Gastroenterol Hepatol 2008;6:1291e3.[11] Chowdhury RC, Forsmark CE. Pancreatic function testing. Aliment Pharmacol Ther 2003;15:733e50.[12] Raimondi S, Maisonneuve P, Lowenfels AB. Epidemiology of pancreatic cancer: an overview. Nat Rev Gastroenterol Hepatol
2009;6:699e708.[13] Strum WB. Abstinence in alcoholic chronic pancreatitis. Effect on pain and outcome. J Clin Gastroenterol 1995;20:4e5.[14] Nordback I, Pelli H, Lappalainen-Lehto R, et al. The recurrence of alcohol-associated pancreatitis can be reduced:
a randomized controlled trial. Gastroenterology 2008;136:848e55.[15] Yadav D, Hawes RH, Brand RE, , et alfor the North American Pancreatic Study Group. Alcohol consumption, cigarette
smoking, and the risk of recurrent acute and chronic pancreatitis. Arch Intern Med 2009;169:1035e45.[16] Tolstrup JS, Kristiansen L, Becker U, Gronbaek M. Smoking and the risk of acute and chronic pancreatitis among women
and men: a population-based cohort study. Arch Intern Med 2009;169:603e9.[17] Wilder-Smith CH, Hill L, Osler W, O’Keefe S. Effect of tramadol and morphine on pain and gastrointestinal function in
patients with chronic pancreatitis. Dig Dis Sci 1999;44:1107e16.[18] Winstead NS, Wilcox CM. Clinical trials of pancreatic enzyme replacement for painful chronic pancreatitis e a review.
Pancreatology 2009;9:344e50.
S. Chauhan, C.E. Forsmark / Best Practice & Research Clinical Gastroenterology 24 (2010) 323e335 335
[19] Warshaw AL, Banks PA, Fernandez-Del Castillo C. AGA technical review: treatment of pain in chronic pancreatitis.Gastroenterology 1998;115:765e76.
[20] Bhardwaj P, Garg PK, Maulik SK, et al. A randomized controlled trial of antioxidant supplementation for pain relief inpatients with chronic pancreatitis. Gastroenterology 2009;136:149e59.
[21] Puli SR, Reddy JB, Bechtold ML, et al. EUS-guided celiac plexus neurolysis for pain due to chronic pancreatitis or pancreaticcancer pain: a meta-analysis and systematic review. Dig Dis Sci 2009;54:2330e7.
[22] Kaufman M, Singh G, Das S, et al. Efficacy of endoscopic ultrasound-guided celiac plexus block and celiac plexus neurolysisfor managing abdominal pain associated with chronic pancreatitis and pancreatic cancer. J Clin Gastroenterol 2010;44:127e34.
[23] Michaels AJ, Draganov PV. Endoscopic ultrasonography guided celiac plexus neurolysis and celiac plexus block in themanagement of pain due to pancreatic cancer and chronic pancreatitis. World J Gastroenterol 2007;13:3575e80.
[24] Buscher HC, Schipper EE, Wilder-Smith OH, et al. Limited effect of thoracoscopic splanchnicectomy in the treatment ofsevere chronic pancreatitis pain: a prospective long-term analysis of 75 cases. Surgery 2008;143:715e22.
[25] Baghdadi S, Abbas MH, Albouz F, Ammori BJ. Systematic review of the role of thoracoscopic splanchnicectomy in palliatingthe pain of patients with chronic pancreatitis. Surg Endosc 2008;22:580e8.
[26] Rosch T, Daniel S, Scholz, , et alfor the European Society of Gastrointestinal Endoscopy Research. Endoscopic treatment ofchronic pancreatitis: a multicenter study of 1000 patients with long-term follow-up. Endoscopy 2002;34:765e71.
[27] Wilcox CM, Varadarajulu S. Endoscopic therapy for chronic pancreatitis: an evidence-based review. Curr Gastroenterol Rep2006;8:104e10.
[28] Dumoneau JM, Costamagna G, Tringali A, et al. Treatment for painful calcified chronic pancreatitis: extracorporeal shockwave lithotripsy versus endoscopic treatment: a randomised controlled trial. Gut 2007;56:545e52.
[29] Strobel O, Buchler MW, Werner J. Surgical therapy for chronic pancreatitis: indications, techniques, and results. Int J Surg2009;7:305e12.
[30] Bachmann ST, Busch P, Mann O, et al. Resection vs. drainage in treatment of chronic pancreatitis: long-term results ofa randomized trial. Gastroenterology 2008;134:1605e7.
[31] Buchler MW, Warshaw AL. Resection versus drainage in treatment of chronic pancreatitis. Gastroenterology 2008;134:1605e7.
[32] Hill JS, McPhee JT, Whalen GF, et al. In-hospital mortality after pancreatic resection for chronic pancreatitis: population-based estimates from the nationwide inpatient sample. J Am Coll Surg 2009;209:468e76.
[33] Dite P, Ruzicka M, Zboril V, Novotny I. A prospective, randomized trial comparing endoscopic and surgical therapy forchronic pancreatitis. Endoscopy 2003;35:553e8.
[34] Cahen DL, Gouma DJ, Nio Y, et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N EnglJ Med 2007;356:676e84.
[35] Saforkas GH, Farnell MB, Farley DR, et al. Long-term results after surgery for chronic pancreatitis. Int J Pancreatol 2000;27:131e42.
[36] Anderson DK, Frey CF. The evolution of surgical treatment of chronic pancreatitis. Ann Surg 2010;251:18e32.[37] Yekebas EF, Bogoevski D, Honarpisheh H, et al. Long-term follow-up in small duct chronic pancreatitis: a plea for extended
drainage by ‘V-shaped excision’ of the anterior aspect of the pancreas. Ann Surg 2006;244:940e6.[38] Garcea G, Weaver J, Phillips J, et al. Total pancreatectomy with and without islet cell transplantation for chronic
pancreatitis: a series of 85 consecutive patients. Pancreas 2009;38:1e7.[39] Ahmad SA, Lowry AM, Wray CJ, et al. Factors associated with insulin and narcotic independence after islet auto-
transplantation in patient with severe chronic pancreatitis. J Am Coll Surg 2005;201:680e7.









![Chronic Pancreatitis: Current Concepts - JSM Central · Chronic Pancreatitis (CP) is an important cause of disabling pain that affects the quality of life of the patients [1]. Globally](https://static.fdocuments.us/doc/165x107/5f0831687e708231d420ccc6/chronic-pancreatitis-current-concepts-jsm-central-chronic-pancreatitis-cp-is.jpg)