Pain, Inflammation, NSAIDs and Analgesics BY DR KAUKAB AZIM.
38
Pain, Inflammation, NSAIDs and Analgesics BY DR KAUKAB AZIM
-
Upload
louisa-willis -
Category
Documents
-
view
219 -
download
0
Transcript of Pain, Inflammation, NSAIDs and Analgesics BY DR KAUKAB AZIM.

Pain, Inflammation, NSAIDs and Analgesics
BY DR KAUKAB AZIM

Learning OutcomesBy the end of the lecture the student should be able to
• Define and discuss the pathobiology of pain pathways• Explain the molecular mechanism of action common to all
nonsteroidal antiinflammatory drugs (NSAIDs)• Describe the pharmacological effects of each drug in each class.• Describe the pharmacokinetics of salicylates.• Describe the main adverse effects of the drugs of each class.• Describe the clinically important drug interactions of the drugs of
each class.• Describe the principal contraindications of the drugs of each class.• Describe the main therapeutic uses of NSAIDs and acetaminophen.

What is inflammation?
• Inflammation: is a reaction to tissue injury caused by the release of chemical mediators that cause both vascular response and the migration of fluids and cells to the injured site.
• It is a protective mechanism in which the body attempts to neutralize and destroy harmful agents at the site of tissue injury and establish condition for tissue repair.

What is Pain• Pain: An unpleasant sensory and emotional
experience associated with actual or potential tissue damage, or described in terms of such damage
• Hyperaesthesia (hypersensitivity): Increased sensitivity to stimulation, excluding the special senses.
• Hyperalgesia: Increased pain in response to a noxious stimulus
• Allodynia: Pain due to a stimulus that does not normally produce pain
• From the International Association for the Study of Pain (IASP) definitions (Merskey, and Bogduk 1994)

Physicians Have a Moral Obligation to Provide Comfort and Pain Management
Especially for those near the end of life!
• Pain is the most feared complication of illness• Pain is the second leading complaint in
physicians’ offices• Often under-diagnosed and under-treated• Effects on mood, functional status, and quality
of life• Associated with increased health service use

Common Causes of Pain In Elderly Persons
• Osteoarthritis of back, knee, hip• Night-time leg cramps• Claudication• Neuropathies can be idiopathic, traumatic,
diabetic or herpetic• Cancer

Pain Receptors

Pain Pathway

Mechanisms associated with peripheral sensitization to pain

Nonsteroidal antiinflammatory drugs (NSAIDs)
Salicylic acid derivatives
Propionic acid derivatives
Acetic acid derivatives
Oxicams Indole derivatives
Selective COX-2 inhibitors
-Acetylsalicylic acid
-Sodiumsalicylate-Diflunisal-Mesalamine
IbuprofenKetoprofenNaproxen
DiclofenacKetorolac
PiroxicamMeloxicam
Indomethacin Celecoxib
Analgesic-antipyretic drug:Acetaminophen

11
Prostaglandins as mediators
√

–Non-selective (t NSAIDS) inhibit both isozymes.
–Side effects occur due to inhibition of COX-1(house keeping” enzyme)
•With selective COX-2 inhibitors (Coxibs), chances of GIT toxicity are less.
•CVS side effects can occur
►
▼

NSAIDS: Mechanism of action
• Main mechanism: Inhibition of COX – Reversible (competitive) inhibitors– Irreversible inactivation (by Aspirin)
• OR – Nonselective COX inhibitors (traditional NSAIDS)– Selective COX-2 inhibitors (Celecoxib)

• Anti-inflammatory effect– Reverses vasodilation, edema, tenderness
• Analgesic effect– By preventing PG mediated sensitization of nerve
endings• Antipyretic effect
– Resets the hypothalamic thermostat by decreasing PG synthesis
– Vasodilation and heat loss– DO NOT cause hypothermia
NSAIDS: Effects

• Antiplatelet aggregation effect– Platelets have COX-1.– Aspirin acetylates COX-1 to inhibit its activity in
an “irreversible manner”.– All other tNSAIDS- reversible inhibitors.– Selective COX-2 inhibitors DO NOT disturb
platelet aggregation at therapeutic doses.– Acetaminophen DO NOT inhibit platelet
aggregation.

Common side effects of NSAIDS
1. Gastrointestinal: Nonselective NSAIDS COX-1 inhibition ↓ gastroprotective PGs
• Effects – Gastric irritation, erosions, ulcers, gastric bleeding– Misoprostol (PGE1) can be used to prevent gastric
ulcers caused by tNSAIDS. – Selective COX-2 inhibitors are safer.

2. Renal: – Sodium water retention, Papillary necrosis
3. CVS: – ↑ Na and water retention
4. Platelet inhibition : bleeding– Selective COX-2 inhibitors and acetaminophen do
not disturb platelet function.5. CNS:
– Headache, confusion, seizures6. Hypersensitivity:
– “Pseudoallergic reaction” (due to increased leukotrienes)

Salicylates• Acetylated salicylate: Aspirin (Acetylsalicylic acid)• Non-acetylated salicylates: sodium salicylate,
diflunisal, mesalamine (5-ASA)
• Mechanism of action:– Aspirin: non-selective COX inhibitor; Irreversible
inhibition” by acetylation. – Other salicylates: weak COX inhibitors; other
mechanisms are involved.

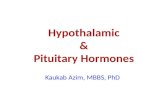
Dose dependent effects of Aspirin
Toxic levels
High Levels

Effects of aspirin
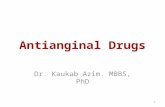
1. Antiplatelet effect:– Irreversible inactivation of COX-1 in platelets causes
decreased production of TXA2 (aggregation promoter). Platelets (enucleated) cannot regenerate COX; effect lasts for 7-8 days.
– Irreversible inactivation of COX in endothelial cells causes decreased production of PGI2 (aggregation inhibitor). Endothelial cells can regenerate cyclooxygenase in a matter of hrs.
– Net effect is decreased platelet aggregation and increase in bleeding time.
– Low doses (80-160mg) are enough to inhibit aggregation without anti-inflammatory effects.

21
COX-1
COX PG I2
Aggregation inhibitor
Aggregation promotor
Irreversible inhibition by Aspirin.
Enucleated platelets cannot regenerate COX.
Irreversible inhibition by Aspirin.
Nucleated endothelial cells can regenerate COX.
ANTIPLATELET EFFECT OF ASPIRIN

2. Other effects of aspirin • ↑ Plasma uric acid levels (at low dose)• ↓ Plasma uric acid levels (at high dose)• Hyperventilation and compensated alkalosis (At high
levels) – Stimulates respiratory center, ↓ pCO2, Increased
bicarbonate in urine• Metabolic acidosis: (At toxic levels)
– Accumulation of salicylic acid due to zero order kinetics at high levels.
– Respiratory center depression; ↑ pCO2

Salicylates: Adverse effects1. Hypersensitivity reactions
– Pts with asthma, nasal polyps, chronic urticaria are more susceptible.
– Pseudoallergic reaction.– Cross reactivity with other NSAIDS.
2. Reye’s syndrome: Encephalopathy, hepatotoxicity.– Do not use aspirin in children with viral fever.
3. Salicylism: – Tinnitus, dimness of vision, mental confusion,
sweating, hyperventilation, nausea and vomiting, diarrhea

Salicylate intoxication
• Tinnitus, Nausea and vomiting, abdominal cramps, gastric bleeding.
• Respiratory depression, Acidosis, generalized convulsions.
• Marked hyperthermia, dehydration.• Skin eruptions, petechial hemorrhages• Coma and death (due to respiratory failure)Treatment: Symptomatic and supportive. • External cooling and I.V. fluids with Na, K, and glucose.• Gastric lavage to remove unabsorbed drug• Forced alkaline diuresis to remove absorbed drug

Salicylates: Therapeutic uses
• Keratolytic: salicylic acid• Counterirritant: Methylsalicylate• Antiinflammatory, analgesic, antipyretic
– Diflunisal: does not enter CNS; no antipyretic effect
Mesalamine (5-ASA):– inflammatory bowel diseases
Aspirin (Low doses):– MI, Angina– Atrial flutter/fibrillation– Transient ischemic attacks

Other tNSAIDSIbuprofen, Naproxen:
– Widely used NSAID for pain and inflammation– GIT and CNS side effects are less
Diclofenec:– Inhibits COX and lipooxygenase (to minor extent) – Decreases free radical production– Accumulates in synovial fluid
Ketorolac:– Can be administered IV, IM– Used in postoperative pain

Indomethacin• One of the most potent COX inhibitor
– Inhibits COX– Inhibits Phospholipase A2 – Reduces neutrophil migration– Reduces T and B cell proliferation
• Severe side effects (in 1/3rd pts)– Abdominal pain, diarrhea, GI bleeding– Frontal headache– Dizziness, confusion, depression, hallucinations
• Therapeutic Uses:– Arthritis (osteoarthritis, rheumatoid arthritis,
Ankylosing spondylitis, Gout)– Closure of ductus arteriosus

Selective Cox-2 inhibitors“Coxibs”
• Celecoxib: first selective COX-2 inhibitor• Potent antiinflammatory, analgesic and antipyretic
activity• Incidence of GI bleeding and peptic ulcers is lower
than tNSAIDS• Does not inhibit platelet aggregation• Increased risk of cardiovascular side effects:
Hypertension, Thrombotic events

Acetaminophen
• Analgesic and antipyretic agent– Inhibits COX-3 in CNS… ?
• Lacks significant anti-inflammatory and antiplatelet activity: very weak COX 1& 2 inhibitor
• Metabolized in the liver• Toxic doses deplete glutathione
– A metabolite, N-acetyl-p-benzoquinoneimine accumulates and causes hepatic necrosis.
– Acetylcysteine administered as antidote.

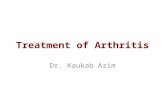
Acetaminophen: MetabolismMINOR
PATHWAYP450 Enzyme
CYP2E1 and CYP1A2
MAJORPATHWAY
(Sulphate Conjugation)
MAJORPATHWAY
(Glucuronide conjugation)
RENAL EXCRETIONTOXIC METABOLITE
NAPQIN-acetyl-p-benzo-
quinone imine)
Toxic Doses (4gm+)Therapeutic Doses
GlutathioneAvailable
GlutathioneDepleted
RENAL EXCRETION Hepatic Necrosis

Antiinflammatory agents:
Steroids

Glucocorticoids: Mechanism of action

33
Steroids: Antiinflammatory effect

Therapeutic uses1. Adrenal Uses2. Non-adrenal uses:
– Inflammatory disorders• Asthma• Allergies: Allergic rhinitis, Acute allergic reactions• Autoimmune disorders: RA, SLE,
glomerulonephritis – Carcinomas– For immunosuppression– This part will be given in details in the Endocrine
pharmacology…..

OPIOID ANALGESICS

History of Opioids
• Opium is extracted from poppy seeds
• Used for thousands of years to produce:– Euphoria– Analgesia– Sedation– Relief from diarrhea– Cough suppression– This part will be given in details in the CNS
pharmacology…..

Opioid Agonists
• Morphine• Heroin• Hydromorphone• Fentanyl• Codeine
Opioid antagonist
• Naloxone• Naltrexone

Good luck