Page1. Chest Sonography in Children: Current Indications, Techniques, and Imaging Findings.
71
page1
-
Upload
georgiana-morrison -
Category
Documents
-
view
221 -
download
1
Transcript of Page1. Chest Sonography in Children: Current Indications, Techniques, and Imaging Findings.

page1

Chest Sonographyin Children: Current
Indications,
Techniques, andImaging Findings

•After plain radiography, CT and MR imaging are the usually preferred modalities for imaging the
pediatric chest. With acoustic limitations imposed by bone and air,
the thorax at first seems unforgiving place to perform ultrasound (US
Various diseases and pathologic conditions, however, can allow an acoustic window into the
chest, and the unique anatomy of the pediatric chest provides other imaging windows for
creative sonologists.

Advances in thoracic US relying on interpretation of artifacts produced by the interface of air in the
lung and pleural space allow important information about the lung itself to be
determined by US. US will never replace CT and MR imaging, but it
can provide important and at times superior information safely and efficiently, particularly in
pediatric patients..

TECHNIQUE•Although US of the chest may be the first
imaging modality used in some acute and critical care settings, in general, pediatric
patients undergoing sonographic examination of the chest have a preceding plain
radiographic examination.

•This helps focus the US study and the combination of information obtained can improve diagnostic accuracy.
• As with sonography elsewhere in the body, the appropriate transducers and frequencies vary with the size
of the patient and the structure examined.• Neonates and small infants are easily examined with high-
frequency linear transducers, whereas older children and adolescents require lower-frequency transducers.
• Smaller footprint sector, vector, or tightly curved array transducers are needed to insonate between ribs, below
the diaphragm, or from the suprasternal notch.• Linear transducers are valuable for examining chest wall
lesions and for examining the lung pleura interface.

•Basic B-mode real-time US is generally all that is required for chest US.
• The use of M-mode imaging has proved helpful, however, in the evaluation of pneumothorax and
quantification of diaphragmatic motion.
• Color Doppler can be useful when evaluating peripheral parenchymal opacities to differentiate
vascularized lesions from infarcts.
•Useful acoustic windows are shown in Fig. 1


•Fig. 1. Acoustic windows for thoracic sonography:•1 ,supraclavicular; 2, suprasternal; 3, parasternal;•4 ,transsternal; 5, intercostal; 6, subxyphoid; 7,
subdiaphragmatic;•and 8, posterior paraspinal. (Adapted•from Kim OH, Kim WS, Min JK, et al. US in the
diagnosis•of pediatric chest disease. Radiographics 2000;20:•653–71 ;with permission).

•The relatively unossified thorax of the neonate and infant, along with the presence of a relatively large
thymus allow imaging of the anterior chest and mediastinum through sternal and costochondral
cartilages.• Suprasternal or supraclavicular approaches may also
be useful in examining the anterior mediastinum and thoracic vessels.
• Intercostal scanning allows imaging of the lung and pleura throughout the thorax and of the posterior
•mediastinum.

•The inferior thoracic cavity can be examined using the liver, spleen, or fluidfilled stomach as
acoustic windows.•For evaluation of the lung and pleural space in
critically ill patients, a systematic organized approach is required.
• One suggested approach divides each hemithorax into 4 quadrants: upper anterior,
lower anterior, upper lateral, and basal lateral2; the anterior axillary line divides the anterior from
lateral regions (Fig. 2)


•Fig. 2. Locations of lung survey imaging. The chest is•divided into anterior and lateral portions by the
anterior•axillary line: 1, anterior superior; 2, anterior basal;•3 ,lateral superior; and 4, lateral basal. (Adapted from•Volpicelli G, Silva F, Radeos M. Real-time lung
ultrasound•for the diagnosis of alveolar consolidation and•interstitial syndrome in the emergency department.•Eur J Emerg Med 2011;17:63–72; with permission).

•If a patient’s condition permits,
•upright posterior imaging should be performed to better evaluate the posterior
chest and to improve detection of small pleural effusions.

INDICATIONS•The most common indication for chest
sonography is to evaluate an opacity detected on a chest radiograph. In the case of a
completely opacified hemithorax,
• US can differentiate whether parenchymal or pleural disease (or both) is the cause (Fig. 3).


•Fig. 3. (A) Newborn with respiratory distress and opaque left hemithorax of unclear etiology. (B)
Longitudinal•parasternal sonogram shows a large anechoic
effusion (E) and consolidated left lung (L). The diaphragm is
•partially everted, displacing the spleen (S). Aspiration revealed a chylothorax. (Adapted from
Coley BD. Pediatric•chest ultrasound. Radiol Clin North Am
2005;43:405–18; with permission).

•Such information is often helpful for guiding the appropriate direction of therapy and possible thoracic intervention.
• Focal masses can be imaged to determine location and whether they are solid or cystic
• .Abnormal mediastinal contours in infants are usually due to an unusually sized or shaped thymus, which can be easily shown by
US,obviating CT.• Palpable chest wall lesions are best initially imaged with US,
because nonpainful pediatric chest wall masses are typically benign and require no further investigation.
• Although CT and MR angiographic techniques can produce exquisite vascular images, US is often the first and only necessary
study for examination of suspected thromboses and other abnormalities of thoracic vasculature.

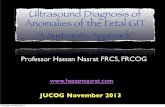
NORMAL ANATOMY•Unossified costochondral and sternal cartilage•appears hypoechoic on US (Fig. 4).


•Fig. 4. Normal costosternal junction. Sonogram along
•the long axis of an anterior rib in a teenager shows
•the bony portion of the rib (R) with posterior acoustic
•shadowing and the hypoechoic cartilaginous rib
•end (C).

•The shape of costochondral cartilage is often varied and may produce irregular chest wall “masses”.
•With aging, these cartilages gradually ossify, diminishing acoustic access to the thorax.
•The thymus is larger compared with the rest of the thorax during the first year of life.
• The thymus is physically largest, however, during adolescence.• Usually confined to the anterior mediastinum, the thymus may
extend into the neck or middle and posterior mediastinum, which may produce concern for pathology.
• Fortunately, the thymus has a characteristic echotexture, with regular linear and punctate echogenicities that allows its confident recognition and differentiation from mediastinal pathology (Fig. 5).


•Fig. 5. Normal thymus. Right parasternal longitudinal•view shows a normal triangular-shaped right thymic•lobe (arrowheads) with characteristic linear and
punctate•echogenicities conforming to the contours of the•brachiocephalic vein (V) and main pulmonary artery•(PA .)Note the hypoechoic costosternal cartilages
)C(.

•The normal pleural space contains a tiny amount•of fluid,27,39 but fluid is seen with US in only
35% of•normal healthy children.39 The acoustic interface•of the chest wall with normal aerated lung
provides•a strong reflective surface and produces a
characteristic•reverberation within the US image, often•referred to as A lines (Fig. 6).


•Fig. 6. Normal chest wall/lung interface; A lines.
•Transverse intercostal sonogram using a linear transducer
•shows the strong echogenic interface of the•aerated lung and pleura (arrows) as well as the
reverberation•artifacts projected within the deeper lung•parenchyma (A lines) (arrowheads).

•The thinner chest wall of infants and small children, however, may not demonstrate this
artifact• .Aerated lung is also seen to move along the
parietal pleural surface with respiration, termed the gliding sign.

Using M mode, the normal motion of the lungproduces a characteristic pattern, termed the
seashore sign (Fig. 7).16

Fig. 7. Normal chest wall/lung interface; seashore sign.
Transverse intercostal gray-scale and M-mode image
shows a normal lung interface (arrows) and a normal
A line (arrowhead). In the M-mode image, the normal
motion of the lung ([ ]) gives a pattern some liken to
sand on a beach, thus the term seashore sign.

•The recent literature is replete with many other terms, which often are more confusing
than clarifying. Recognizing these normal findings, however, is important, because
deviations from their appearances provide clues to pleural and parenchymal disease.

THE PLEURAL SPACEEffusions
•Being superficial to normally echogenic aerated lungs, the pleural space is well visualized by US.
•Although pleural fluid collections are often suspected from chest radiographs, US is more sensitive in detecting pleural fluid than
chest radiographs, particularly in critically ill patients in whom upright or decubitus radiographs are not possible.
• The sonographic appearance of pleural fluid depends on its composition and may range from completely anechoic, in the case
of simple transudative collections, to collections with mobile echogenic debris in cases of infection and hemorrhage, to septated
and more solid appearing collections with empyemas and organizing infection
•(Fig. 8.)


•Fig. 8. Sonographic appearances of pleural collections. (A) Subdiaphragmatic longitudinal sonogram shows
•a mostly anechoic left pleural effusion (E) along with consolidated lung (L). The spleen (S) and kidney (K)
help•to provide acoustic windows into the inferior chest. (B)
Empyema with the formation of fibrinous septations.•(C )Well-organized, solid-appearing empyema (E)
adjacent to aerated lung (L). (Adapted from Coley BD. Pediatric
•chest ultrasound. Radiol Clin North Am 2005;43:405–18; with permission).

•Simple nonloculated collections can be seen to change shape with patient breathing or
change in position. The distinction of echogenic but still fluid collections from more
solid collections can be aided by the fluid color sign, in which mobile debris produces signal with color Doppler whereas nonmobile solid
material does not.

•As infected pleural collections progress and organize, fibrinous strands begin to form.
• Initially thin and mobile, these fibrin strands thicken and increase, creating multiple loculations in which
fluid no longer changes with patient position or respiration.
• The parietal and visceral pleura may be thickened as well, as often seen with CT .
•Infected pleural collections may progress to solidify into a homogenous echogenic gelatinous mass
encasing the underlying lung, eventually producing a fibrothorax.

•US is superior to CT in characterizing the nature of pleural fluid collections and can help
guide percutaneous drainage Simple fluid collections are amenable to percutaneous
aspiration and are most safely performed with US guidance
•(Fig. 9.)


•Fig. 9. Pleural effusion aspiration. Transverse intercostal
•sonogram of the left chest shows a pleural effusion
•(E )with some echogenic material. The aspirating
•needle (arrow) is seen just entering the pleural space.
•S, spleen.

•Because up to 50% of pediatric parapneumonic effusions recur after aspiration, however, it is
often more prudent to leave a drainage catheter in place, even if only for a short time.
• The US detection of fibrinous strands and even honeycombing of the pleural space is not a
contraindication to percutaneous drainage, but it does mean that fibrinolytic therapy is required to
clear the collections and should be started promptly to achieve proper drainage
•(Fig. 10.)


•Fig. 10. Septated parapneumonic effusion. Longitudinal
•sonogram of the left chest shows consolidated•lung (L) and complex partially septated fluid
(asterisks).•This collection responded well to
interventional•drainage and lytic therapy. K, kidney; S,
spleen.

•In the setting of continued fevers and poor clinical response after pleural drainage, plain radiographs
may not adequately assess whether undrained pleural collections or underlying parenchymal
infection is the cause, US can adequately assess the pleural space and portions of the underlying lung,
although there may be limitation from existing chest tubes, dressings, and patient discomfort.
• In these complicated and refractory cases, CT may be a better option, especially if surgical intervention
is planned.

Masses•Malignant disease involving the pleural space is
much less common in children than in adults54 but ca occur with Wilms tumor, neuroblastoma,
leukemia, and sarcoma• Primary chest wall neoplasms and pleural
metastases are often accompanied by hemorrhagic pleural effusions, which appear as echogenic
debris-filled fluid at sonography.•The presence of pleural fluid aids in detection of
solid masses adherent to the parietal or visceral pleura (Fig. 11).


•Fig. 11. Longitudinal sonogram of the right chest in•a child with Wilms tumor shows a pleural effusion•(E )outlining a metastatic deposit on the
diaphragmatic•parietal pleura (arrow). (Adapted from Coley•BD. Pediatric chest ultrasound. Radiol Clin North
Am•2005;43:405–18 ;with permission).

•If visible sonographically, pleural masses are readily biopsied with US guidance (Fig. 12), allowing confirmatory histologic diagnoses


•Fig. 12. Pleural biopsy. Intercostal sonogram in a child
•with Wilms tumor shows a pleural-based solid mass
•(arrowheads .)The aspirating needle (arrow) is seen
•within the lesion, and yielded metastatic Wilms•tumor

Pneumothorax•As discussed previously, the normal stron acoustic
interface between pleura and aerated lung produces repeating posterior echogenicities (A lines), and the
normal sliding motion of the lung can be seen during respiration (see Fig. 6)
•.•When air is introduced into the pleural space, the normal
tension between the pleural layers is lost, and a gap is created between the parietal and visceral pleura
disrupting the normal acoustic interface• .The sliding of the underlying lung can no longer be seen,
and the normal reverberation is replaced by a static homogeneous posterior acoustic shadowing (Fig. 13)


•Fig. 13. Pneumothroax. Transverse intercostal sonogram
•shows a normal pattern of moving lung•(seashore sign )deep to the lung pleural interface•(arrow .)On the right hand side of the image, there•is loss of this normal pattern with a static series of•horizontal echogenicities. Note how this looks•different from normal A lines. An absence of normal•lung sliding adjacent to normal lung is called the•lung point sign (P).

•Some reports indicate that US is superior to plain radiographs in pneumothorax detection and may be useful in monitoring procedural complications
and assessing critically ill and trauma patients.
•Similarly, the curtain sign has been described in hydropneumothorax where the normal pleural
gliding is lost and mobile air fluid levels are visualized.

LUNG PARENCHYMAInterstitial Disease
•Plain radiography usually suffices for the evaluation of parenchymal lung disease in pediatric patients, but unclear cases
may benefit from US or CT examination.• The traditional view is that aerated lung must becom atelectatic
or consolidated before it becomes possible to examine with US.
• More recent studies have shown that there is significant important clinical information that can be obtained by evaluating
the artifacts produced from the surface of aerated lung.• The interaction of the sound beam with interlobular septa
produces so-called B lines, also referred to as lung rockets or comet tails.

•A few scattered B lines can be normally seen and may be caused
•by focal subpleural thickening or distortion by parenchymal disease.
• Multiple B lines can indicate an abnormality with the underlying lung .
•Anything that thickens the interlobular septa can produce a B line, but the distinction between fibrotic change and
interstitial edema can often be made given the clinical context.
• In adults, this finding has been shown with a variety of disorders, such as pulmonary fibrosis, viral pneumonias,
sarcoidosis, lymphangitic carcinomatosis,and bronchiectasis.

•Investigators have subdivided B lines into B7 lines (7 mm apart), indicating thickened
interlobular septa, and B3 lines (3 mmapart), indicating the equivalent of the ground glass
appearance at CT .•The presence of B lines is shown to correlate
accurately with other imaging, pulmonary artery pressures, and fluid status and seem accurate in
diagnosing interstitial and alveolar disease.

•Experience in children is more limited, particularly
regarding interstitial edema,68 but my anecdotal experience indicates that similar
findings occur in children as well (Fig. 14).


•Fig. 14. Interstitial edema. (A) Chest radiograph of a teenage girl with dyspnea and new-onset renal failure
•shows interstitial edema. (B) Longitudinal image of the right upper quadrant shows an abnormally echogenic
•kidney consistent with the subsequent diagnosis of glomerulonephritis. Note the regularly spaced B lines
within•the right lower lobe (arrowheads). These correspond to
the thickened interlobular septa seen on the chest radiograph.
•K, kidney; L, liver.

•Surfactant deficiency disease produces variable appearances ranging from multiple B
lines to a diffusely echogenic lung, which eliminates visualization of the normal chest
wall–pleural interface•(Fig. 15.)


•Fig. 15. Surfactant deficiency disease. (A) Chest radiograph of a preterm infant shows diffuse
granular airspace•disease typical of surfactant deficiency, worst in the
right lower lobe. (B) Transverse sonogram of the right lower
•chest through the liver (L) shows abnormal increased pulmonary echogenicity of the right lower
lobe without•visualization of focal B lines.

•The sonographic appearance correlates well with the clinical and radiographic findings.71
Chronic lung disease in the infant produces similar acoustic interfaces as seen in adult
parenchymal disease, creating multiple ring-down artifacts (Fig. 16).


•Fig. 16. Chronic lung disease. (A) Portable chest radiograph in a former preterm infant with
continued oxygen•requirements shows increased interstitial markings
of chronic lung disease. (B) Longitudinal sonogram through
•the left upper quadrant shows multiple B lines indicating interstitial lung disease. (Adapted from
Coley BD. Pediatric•chest ultrasound. Radiol Clin North Am
2005;43:405–18; with permission).

•The progression of US findings from surfactant deficiency to bronchopulmonary dysplasia may be useful as a
predictor of the development of chronic lung disease and may appear earlier than chest radiographic findings.
•The administration of exogenous surfactant, however, does not seem to improve the sonographic appearance in
surfactant deficiency.• Interstitial prominence causing B lines persists, indicating
that interstitial extravascular fluid clearance remains impaired despite radiographic improvement in aeration
and clinical improvement in ventilation.

Consolidation•Airless lung can appear sonographically similar
to liver, thus has been termed, hepatization (Fig. 17).


•Fig. 17. Lung consolidation. Longitudinal sonogram•over the lower right chest shows consolidated lung•superior to the liver. Although their echogenicities•differ, their internal sonographic appearance is•similar. (Adapted from Coley BD. Pediatric chest
ultrasound.•Radiol Clin North Am 2005;43:405–18; with•permission).

•The underlying internal architecture of the lung is preserved, however, allowing differentiation from masses or other
processes. Branching linear echogenicities representing air bronchograms are often seen
(Fig. 18)