Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed ... - Prof A A Narula.pdf · • Otitis...
51
Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed Consultant St Mary’s & Ealing Hospitals Hon. Professor, Middlesex University 17 th July 2004
Transcript of Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed ... - Prof A A Narula.pdf · • Otitis...

Paediatric Otolaryngology
Antony A Narula MA FRCS FRCS Ed
Consultant St Mary’s & Ealing HospitalsHon. Professor, Middlesex University
17th July 2004

Otology
• Acute Otitis Media• Otitis Media with Effusion (glue ear)• Chronic Suppurative Otitis Media• Trauma, Foreign Bodies• Otitis Externa
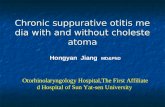
Acute Otitis Media
• Pre-school children; 85% settle spontaneously within 24 hrs
• After 24hrs antibiotics do influence natural history
• Repeated episodes of acute otitis media in 12 months: Adenoidectomy + Grommets
Complications• Perforation
• Facial palsy
• Mastoiditis
• Lateral Sinus Thrombosis
• Intracranial – meningitis, abscess


Mastoiditis
• “masked variety”• Swelling of the postero-superior meatal wall• Systemic upset, swinging pyrexia• CT scanning• Aggressive treatment; IV ABiotics +cortical
mastoidectomy


Otitis Media with Effusion -”Glue Ear”
• Eustachian tube dysfunction • Symptoms - speech and language delay,
behavioural, imbalance• No otalgia : “silent otitis”• Natural history: peak incidence 2-6 years


Treatment• Oral steroids - only medication shown to
clear fluid• Antibiotics, antihistamines, decongestants
do not alter the natural history• Bilateral 30dB loss for 3 months with
symptoms • Grommets• Adenoidectomy • Treat coexisting chronic rhinitis
The Problem
• OME affects 20% of children• Often short-lived• Possible effects on speech / education• Thousands of operations each year• Very poor evidence base

Follow Up Details
• All children followed up for min 2 years• Analysed on intention to treat basis• 550 children entered in 7 centres
• Numerous measures inc. social functioning• Case notes monitored thereafter

Main Outcomes
• Moderate OM history is relevant• Hearing level alone is an inadequate
surrogate measure of disability• Speech and language development• Anti-social behaviour• Social immaturity

Spontaneous Improvers
• season • initial hearing level • referral route • passive smoking• +ve sibling history
Hearing Levels
• >20 dB on two occasions = entry criterion• These are severely affected children• Up to 50% still consulting in year 4

Adenoidectomy
• Respiratory health• Sleep patterns• Hearing levels
• Lasts beyond 2 years with reduced repeat consultations

Other Outcomes
• Grommets reduce acute otitis media• Surgical treatment is cost-effective in
QALYs

TARGET Results
• Grommets do work• Adenoidectomy offers added value• Applicable to children over 3.5 years
Chronic Suppurative Otitis Media “CSOM”
• Otorrhoea and deafness• +/- pain• Classify as SAFE or UNSAFE
• SAFE :Reconstructive - Myringoplasty, Tympanoplasty, Ossiculoplasty
• UNSAFE : Establish a safe ear -Modified/radical mastoidectomyCombined approach tympanoplasty




Complications of unsafe disease
• Facial palsy• Semicircular canal fistula • Dead ear• Meningitis• Brain abscess


Rhinitis• Increasing incidence• Treat both the upper and lower airways• ?Environmental pollution , dust mite faeces• Treatment is environmental and medical• Nasal steroids are the mainstay of treatment• Antihistamines also helpful• Mast cell stabilizers, leukotriene receptor
antagonists disappointing
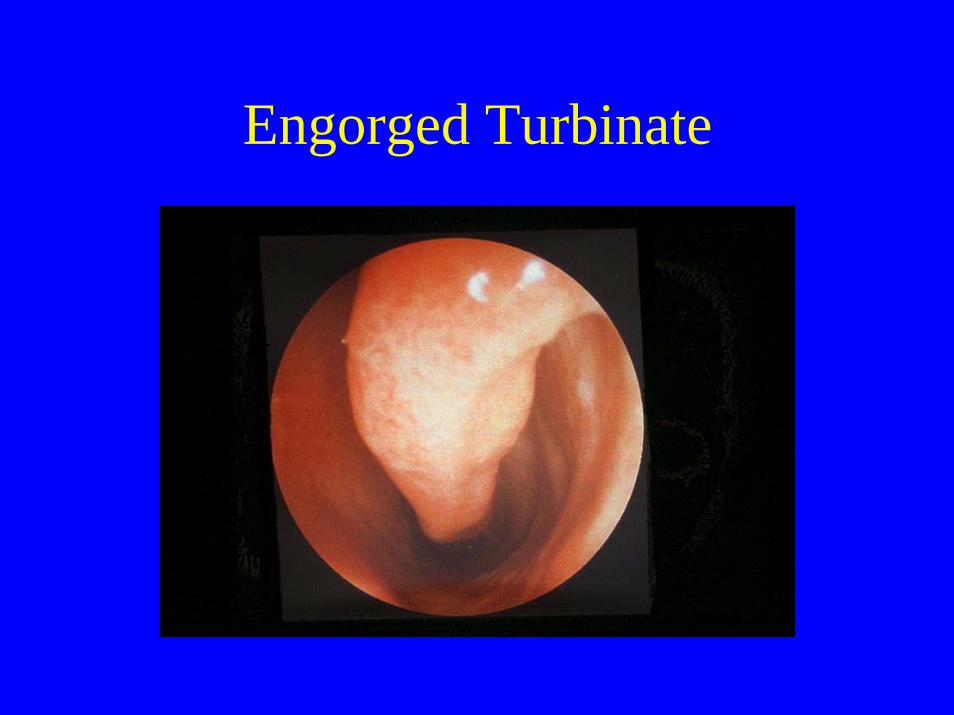
Engorged Turbinate

Polyps

Infective Rhino-sinusitis
• Children- Ethmoiditis• Periorbital cellulitis• Complications - orbital and intracranial• Emergency referral

Peri-orbital Cellulitis

Fractured Nose
• Rare in childhood• Exclude a septal haematoma• No Xrays• If too swollen to assess see in 7 days• Refer if cosmetic displacement


Tonsillitis
• Penicillin is still the antibiotic of choice• Quinsy uncommon in children
Tonsillectomy • for recurrent acute tonsillitis - 5 episodes
each year for two years• in association with adenoidectomy in
adenotonsillar hypertrophy

Indicators for inpatient stay following Ts&As(1)
• Age <36 months• Significant pre-operative apnoea• Medical co-morbidities – asthma, cardiac
disease• Narrow pharyngeal airway:• mandibular hypoplasia eg. Treacher-Collins / Down
syndromes; mucopolysaccharidoses
Indicators for inpatient stay following Ts&As(2)
• Respiratory distress in the immediate postoperative period
• Social factors- distance from hospital
• lack of telephone or car• poor carer reliability
•


Tonsillar hypertrophy can compromise the oropharyngeal airway significantly (especially during URTI)



Paediatric Airway• Neonate – obligate nasal breather• Highly placed larynx• Feeding Difficulties/Reflux• Dysphonia / abnormal cry • Stertor & Stridor
INFECTION
• Epiglottitis, Laryngotracheobronchitis(croup)
• Airway oedema and narrowing• May need intubation• Extubation after MLB

Epiglottitis
• H.influenzae (cf HiB vaccine)• 2-6 years, boys > girls• Rapid onset - 24hr history• Systemic upset with severe pain on
swallowing, sitting up,drooling• Do not place instruments in the mouth

Croup• Parainfluenza virus• Insidious onset• Barking cough• No pain on swallowing• Biphasic stridor
• ?Measles

Tracheostomy• Morbidity and Mortality• Huge social consequences for parents• However, almost all will be ultimately
decannulated



Foreign Bodies
• History of coughing, choking +/- cyanosis• Unilateral wheeze• Signs of paradoxical respiration• Early diagnosis important• Treatment - MLB

Importance of E.N.T.
• Commonly performed procedures• Large % of procedures in children• Day case scenario• High level of morbidity thus requiring
vigilance