
Paediatric Long Term Ventilation Canada 2010 A Review Ian MacLusky MBBS, FRCP(C) Children’s...
43
Paediatric Long Term Ventilation Canada 2010 A Review Ian MacLusky MBBS, FRCP(C) Children’s Hospital of Eastern Ontario Ottawa Conflicts : Financial Nil Bias Definitely
-
Upload
noel-sanders -
Category
Documents
-
view
217 -
download
3
Transcript of Paediatric Long Term Ventilation Canada 2010 A Review Ian MacLusky MBBS, FRCP(C) Children’s...

Paediatric Long Term VentilationCanada 2010
A Review
Ian MacLusky MBBS, FRCP(C)Children’s Hospital of Eastern OntarioOttawa
Conflicts:
FinancialNil
BiasDefinitely
Paediatric Long Term VentilationOutline
1. Current State
2. Rationale
3. Structure
4. Common Problems
Ventilation i.e. Rx of hypercapnoea by MV Not respiratory support (CPAP /BiPAP for OSA / CHF)
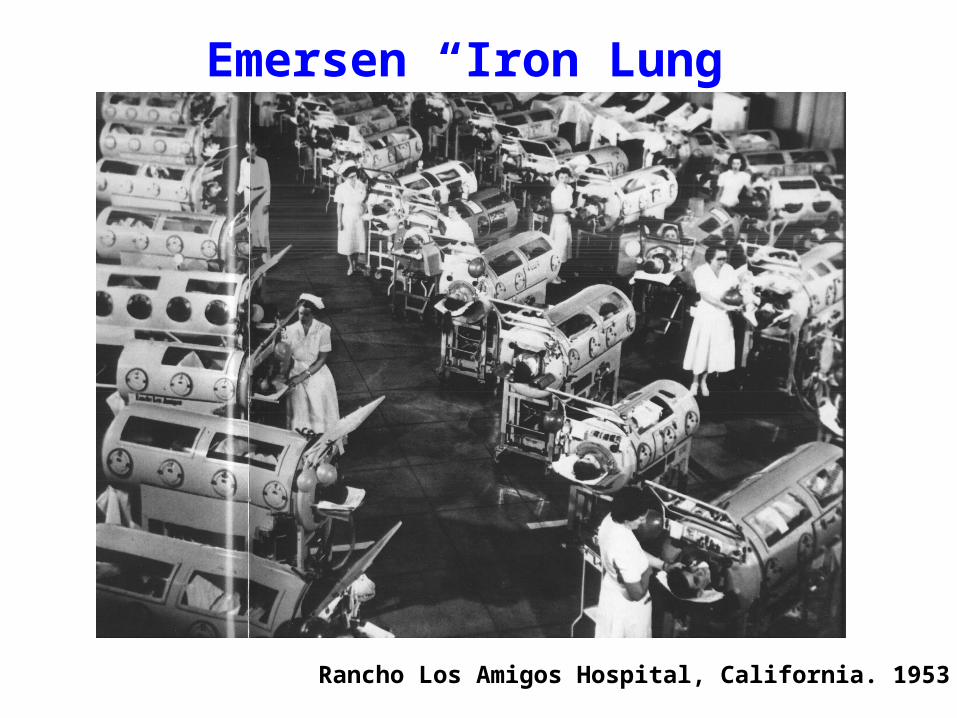
Emersen “Iron Lung”
Rancho Los Amigos Hospital, California. 1953

Long Term Home Ventilation
1. Improved equipmenta. Invasive
b. Non-invasive
2. Changing attitudes / expectationsa. Home better than hospital
b. Care of “invariably fatal” conditions
3. Parental education / information access
4. Home cheaper than hospital (?)
Simonds AK. Eur Resp J. 2003;22(S47):38s-46s
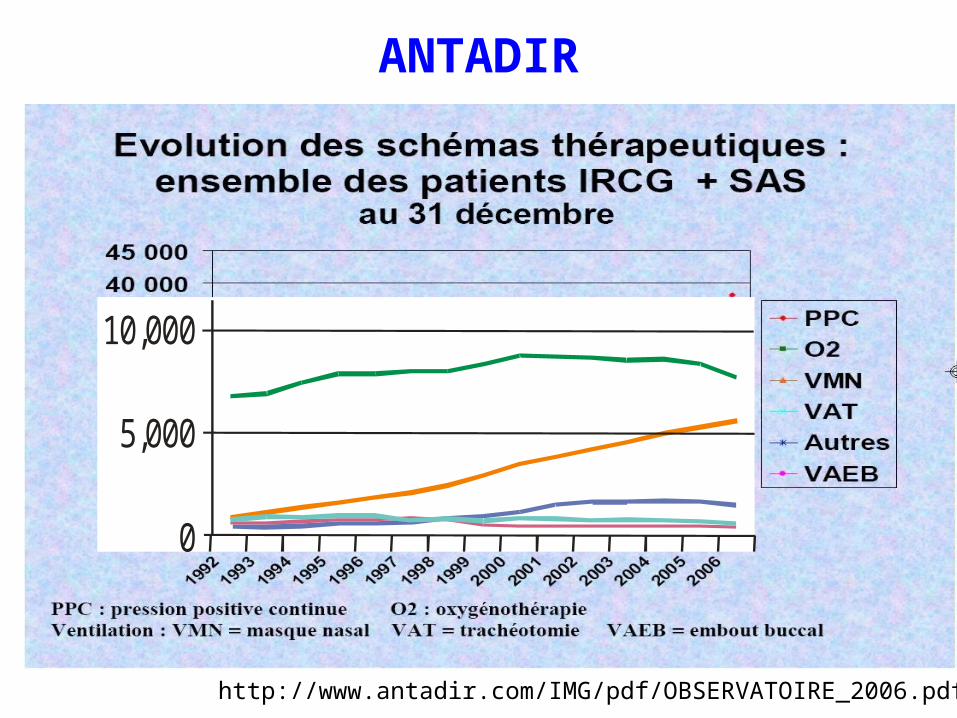
ANTADIR
http://www.antadir.com/IMG/pdf/OBSERVATOIRE_2006.pdf
10,000
5,000
0

Canada?
2006 Canada wide survey*
Non-invasive: c.300 patientsInvasive: c.100 patients
*Jiemin Zhu, RN, MSc (Davis M. MB.ChB.)

Year
1990 1992 1994 1996 1998 2000 2002 2004 2006
Pat
ient
s R
efer
rred
0
10
20
30
40
50
Non-InvasiveInvasive
Hospital for Sick Children: 1990-200640 Invasive. 150 Non-invasive
NewEnrolments

Patient Population
Invasive
NM hypoventilationThoracic hypoventilationCentral hypoventilationObesity hypoventilationCCAHSCardiopulmonary
Non-Invasive40 patients 150 patients

Outcomes (SickKids)
• Total 190 enrolled– Mean age enrolled 8.4 yrs– Mean duration follow up 5.8 years
• 90 still followed, 100 no longer followed– 8 Failed Rx– 8 Referred to local center– 27 Improved (no longer needing support)– 28 Transferred, aged >18 years– 29 Died

Technologies
1. Non-invasivea. Negative pressure (cuirasse)b. Mask: BiPAP
2. Invasivea. Tracheostomyb. Phrenic Nerve Pacing
Simonds AK. Eur Resp J. 2003;22(sup 47):38s-46sToussaint M. Chron Respir Dis. 2007;4(3):167-177Lewarski JS. Chest. 2007;132(2):671-6

NIPPV
Advantages• Ease of initiation and removal: undoable!• Preservation of airway defenses• Patient can eat, drink and communicate• Avoidance of complications of intubation• Less “technology dependency”: caregiver
expertise

NIPPV
Disadvantages
• Mask uncomfortable / claustrophobic – (poor compliance)
• EPAP
• Airway not protected
• Air leaks
• Maximum pressure (30 cm H2O)
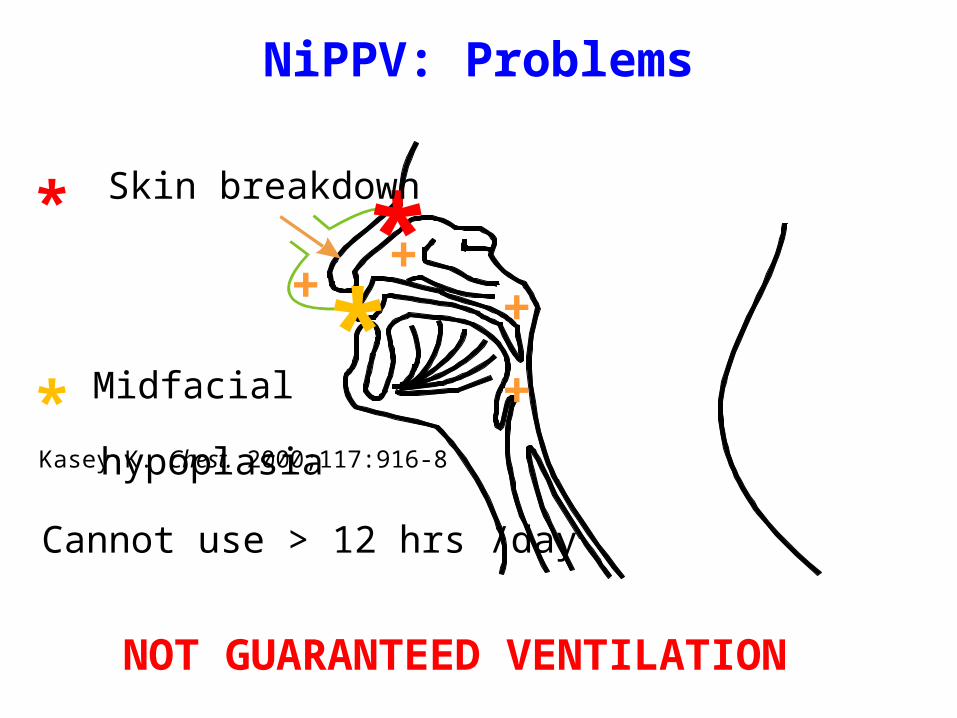
NiPPV: Problems
++
+
+**
* Skin breakdown
* Midfacial
hypoplasia
Cannot use > 12 hrs /day
NOT GUARANTEED VENTILATION
Kasey K. Chest. 2000;117:916-8

Invasive Ventilation: IMV
Pressure vs Volume cycled?

Invasive
Advantages• Guaranteed ventilation
– Return circuit: exhaled volume• Access to airway (but ? need)• Nocturnal?
– Can “cork” during day? • Speak• Cough
– If not able to exhale• Passy-Muir “speaking valve”

Invasive
Disadvantages • Surgical intervention • Trach: Interferes with cough + auto PEEP• Increased caregiver expertise + time• Bypasses nose (filter/ humidify / sterilize)• Not readily “portable”• Not readily “undoable”
– (1/3 do come off / NIPPV)

Alternatives?Phrenic nerve pacing • Portable (24 / 7) @
• Minimal caregiver expertise• (Not interfere cough / speech)BUT
• Expensive ($40-$50K, + surgery)• May still need tracheostomy (?50-90%) • Not guaranteed ventilation (fixed RR/TV)• Still surgery: Complex insertion / setup
– Phrenic nerve damage
• Need intact phrenic nerve (?diaphragmatic*)
Patient selection?
@Guilleminault C. et al Sleep. 1997;14:369-77*DiMarco AF at al. Chest. 2005;127:671-8
.
Long Term Ventilation:Justification?
1. Life expectancy (?)– NIPPV in NM disease
Robert D, Argaud L. Crit Care. 2007;11(2):210-219

Increased Life Expectancy?
Yasuma F at al. Chest 1996;109:590Eagle M Neuromusc Dis 2002;12(10):926-29
99 patients 1980-95 (80 died)1980-87 nil, 87-92 Cuirass, 92 on nIPPV

Long Term Ventilation Program:Justification?
1. Life expectancy
2. Improve quality vs. quantity of life• Sleep fragmentation (NIPPV)• Blood gasses (carry over)
Robert D, Argaud L. Crit Care. 2007;11(2):210-219
Long Term Ventilation Program:Justification?
1. Life expectancy
2. Improve quality vs. quantity of life• Sleep fragmentation (NIPPV)• Blood gasses (carry over)• QOL (?)
Markstrom A et al. Chest 2002;122(5):1695-1700
*
Long Term Ventilation Program:Justification?
1. Life expectancy
2. Improve quality vs. quantity of life• QOL (?)
Whose evaluating? Patients > family > caregivers
“It’s Okay, it helps me breathe”*
Disease vs. ventilation?@
*Earle RJ et al. J Child Health Care 2006;10:270-82 Noyes J. J Advan Nurse 2006;56(4):392-403@ Mah JK Pediatr Neurol 2008;39(2):102-107

Long Term Ventilation Program:Justification?
1. Life expectancy
2. Improve quality as well a quantity of life
3. Costs (?) Hospital

Impact on Hospitalization?
• 15 NM children– Age 11.7 (3.4-17.8)
• NPPV at least 1 yearYear before vs. year after– Days in hospital 85% (48 7.0)– Days in ICU 68% (12 3.9)
Katz S at al. Arch Dis Child 2004;89:121-124
(Leger P at al. Chest 1994;105:100-105)
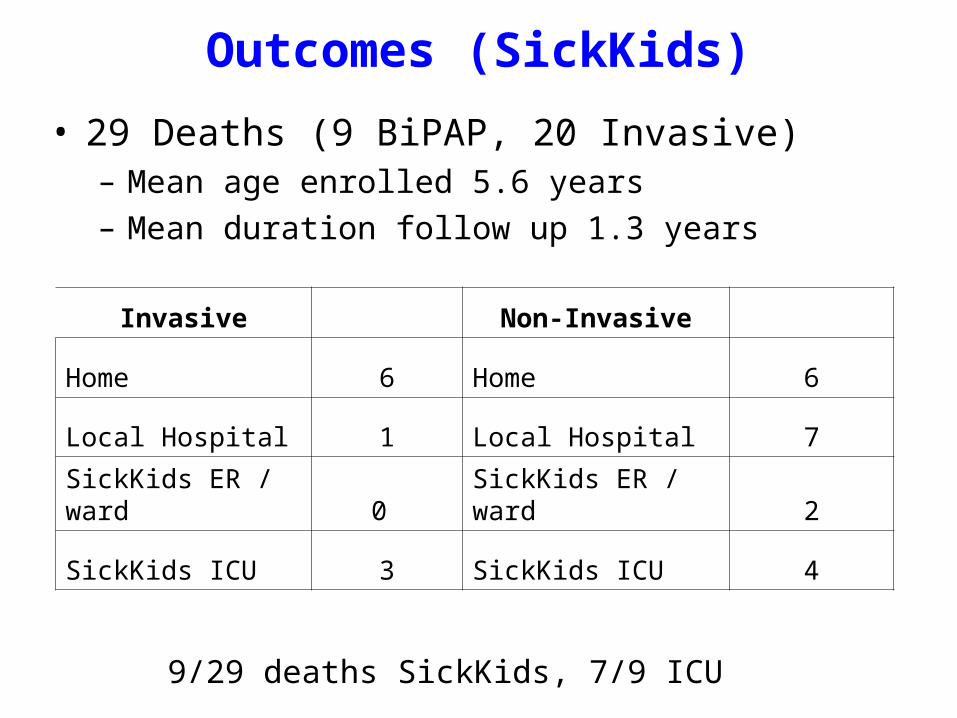
Outcomes (SickKids)
• 29 Deaths (9 BiPAP, 20 Invasive)– Mean age enrolled 5.6 years– Mean duration follow up 1.3 years
Invasive Non-Invasive
Home 6 Home 6
Local Hospital 1 Local Hospital 7
SickKids ER / ward 0 SickKids ER / ward 2
SickKids ICU 3 SickKids ICU 4
9/29 deaths SickKids, 7/9 ICU
Long Term Ventilation Program:Justification?
1. Life expectancy
2. Improve quality as well a quantity of life
3. Costs (?) Hospital
Family (?)

Long Term Ventilation Program:Family Impact?
1. Parents (mother)a. Time + financial demands
b. Physical overburden
c. Emotional turmoilStress / fear
Child “different” from societal norm
Loss family privacy / independence
d. Social Isolation
Carnevale F. Pediatrics 2006;117(1):e48-e60 Heaton J et al. Health Soc Care Comm 2005;13(5):441-450Wang K-W K. J Advan Nurs 2004;4(1):36-46

Long Term Ventilation Program:Family Impact?
1. Parents
2. SiblingsJealousy / resentment / rivalry
Carnevale F. Pediatrics 2006;117(1):e48-e60 Wang K-W K. J Advan Nurs 2004;4(1):36-46

Long Term Ventilation Program:Justification?
1. Prolonged Life
2. Improve quality as well a quantity of life
3. Costs (?) Hospital
Family / community
Net?
Wang K-W K. J Advan Nurs 2004;4(1):36-46
What is Required to Succeed?
A Plan (prepared and agreed on in advance)A Team
Tertiary CenterCommunityLines of communicationContinuity of care
Time!“Informed Consent” when child already trach’ed?Parents (and child) time to digestIdentify caregivers: buy in from communityTeam to review family needs / resources
But: How long is actually required?
Ballangrud R. J Advan Nurs 2008;65(21):425-434
Issues1
• When to start ventilation, and on whom?– 16 European countries– >10 fold variation frequency + who ventilated
Lloyd-Owen SJ at al. Eur Resp J 2005;25(6):1025-1031

Issues2
• When to start ventilation, and on whom*?
• NIPPV: – Recurrent pneumonias (NM patients)– Nocturnal hypoventilation (sleep disturbance)@
– Daytime hypercapnoea– Prophylactic?
• Ineffective• Unlikely to be tolerated
*Fauroux B Resp Med 2009;103:574-581@Ward S at al. Thorax 2005;60(12):1019-1024

Issues3
• When to start ventilation, and on whom?
• Invasive: ? – No alternative (sure?)– Potential for stability or improvement?
• CCAHS• Slowly progressive NM disease
– Rapidly progressive?• SMA1*, tumour
– Don’t know?
*Roper H et al. Arch Dis Child 2010;95:845-849
Yes
No
Yes (?)

Problems1
Availability of Necessary Resources?1. Equipment
a. Ventilator: provision and maintenanceHow long to get?
b. “Expendables”: tubing, etc.?c. Other?
i. Suctionii. Oximeter
2. Trained community caregiversHow much funded?(Great in theory:- In practice availability)?Alternatives? i.e. Health Care Support Workers (HCSW)
3. Availability of Respite?

Problems2
Availability of Necessary Resources?1. Equipment
a. Ventilator: provision and maintenanceb. “Expendables”: tubing, etc.?c. Other?
2. Trained community caregivers3. Respite?4. Transition to Adult Care?
Need National Standards?Optimum vs. bare minimum?

Problems3
Organization: Theoretical
Patient
Family
CommunityMD
CommunityCare
Access
School,etc
CommunityCaregivers
TertiaryCare
Center

Organization: Actual
Patient
Family
NurseCoordinator
Respirology
Paediatrics
Gastro/Nutrition
Physio,RT, etc
NeurologyCommunity
MD
CCAC
School,etc
Who do the parents call at 2:00 am Sat?
?
Tertiary care centerCommunity caregivers
ER

Ethics?Ethics?1. Non-invasive: easy
-“Undoable” therefore patient can determine2. Invasive
- Promising what we can’t deliver?- Prolonging life or prolonging death?
Progressive / Terminal case (SMA1, HIE) Parents “want everything done”?
Whose needs are we meeting?
Who decides?
Brazier M. Med Law Rev 2005;13:671-8
The courts

Ethics (of Finite Resources)?
Conclusions1
• Increasing numbers children home on chronic ventilation- NIPPV and IMV.(success?)
• Heterogeneous population, require complex, coordinated care.
• Significant burden– Family– Community (financial, personnel, knowledge)
Conclusion2
• Improvements required– Improved coordination of healthcare– Increased resources:
• Increased availability of community care & respite• Increased training and availability of local health
care resources*• Alternative to “RN” caregivers?
(Ventilation Support Worker: NHS 2007)
National minimum standards?
National Registry: outcomes?
*Hewitt-Taylor. Inten Crit Care Nurs 2004;20:93-102
http://www.longtermventilation.nhs.uk/
“Suck It Up Princess”
Renee Rodrigues
CMD
TV Ontariowww.superstarrenee.com/index.php


















