Paediatric Gastro-Allergy Symposium - Neocate...Paediatric Gastro-Allergy Symposium The speaker had...
34
Transcript of Paediatric Gastro-Allergy Symposium - Neocate...Paediatric Gastro-Allergy Symposium The speaker had...

Paediatric Gastro-Allergy Symposium
The speaker had sole editorial control over the content in
this slide deck.
Any views, opinions or recommendations expressed in
the slides are solely those of the speaker and do not
necessarily represent those of Nutricia.
Ruth Stanley
Lead Paediatric Gastroenterology Dietitian
GNCH
Aims
• Understand Eosinophilic Oesophagitis (EoE) in a nutshell
• Aware of different dietary treatments for EoE
• Appreciate the nutritional complexity of a top 6 free diet
• Realise its not all doom and gloom
Eosinophilic Oesophagitis
What is it?
• “A chronic immune condition characterised clinically by
symptoms of oesophageal dysfunction and histologically by the
presence of eosinophils in the oesophagus” (1)
• First presentation 1960, later described as a syndrome 1990 (1)
• The prevalence of EoE is increasing
• Unknown numbers in UK
• Estimated rates of prevalence between 13-49 cases per
100,000 in population based studies in Europe and USA (1)
• Past 5 years seen an increase in guidelines and case reports
Clinical Presentation
• Vary with ages, main symptoms (1,2) :
• Infants and toddlers
• Feeding difficulties which can result in poor growth
• Children
• Vomiting, abdominal or retrosternal pain
• Adolescences
• Reflux symptoms, dysphagia and food impaction
Treatment Options EoE
• Combination of medication and dietary manipulation (1,2)
• Medication
• PPI
• Corticosteroids
• Dietary
• Exclusive Amino Acid (AA) Feed
• Targeted Elimination Diet (T.E.D)
• Top 6 Free
Exclusive AA Feed
• Placed on Exclusive AA feed
• 6-8 weeks
• Re-scoped after this period to assess response
• 95-98% success rate at inducing remission (1)
• Comes with down sides:
• Taste
• Compliance
• Psychological
• Cost
Targeted Elimination Diet
• Food avoided based on allergy testing
• Varying length of time
• 45-53% success rate at inducing remission (1)
• High negative predictive value (1, 2)
Top 6 free diet
• Eliminate 6 foods most commonly associated with allergy (IgE and non IgE) • Wheat
• Egg
• Milk
• Soya
• Fish
• Nuts
• 72-74% success rate at inducing remission
• High risk of nutritional deficiency
• Compliance can be an issue
Which dietary treatment
• Joint decision with consultant
• Difficult decision with multiple factors to consider
• Age patient
• Social support
• Severity of symptoms
• Presenting nutritional status
Case Study
• 14 year old boy
• Clinical presentation of food sticking at each meal and
struggling to eat.
• Histology confirmed EoE.
• Already on PPI therapy.
• Weight over 99.6th Centile, Height 91st Centile.
Interactive Voting
• Which dietary manipulation option would you choose to
place this patient on
• A – Exclusive AA
• B - T.E.D
• C – Top 6 free diet
Case Study
continued
• Asked by consultant to place on exclusive AA to ensure EoE under control by time commence GCSE year at school. Symptoms also severe.
During dietetic consultation:
• Doesn’t like Milk or Milkshakes
• Patient very withdrawn
• Recently lost grandmother and due to attend bereavement counselling in next few weeks.
• Mum is extremely anxious
• Social information:
• Mum single parent.
• Patient has older sister on steroids who is currently being treated for depression. Also has 3 younger siblings (triplets)
Interactive Voting
• Which dietary manipulation option would you choose to
place this patient on
• A – Exclusive AA
• B - T.E.D
• C – Top 6 free diet
Case Study
Treatment in Practice
Actual Decision
• Top 6 free
• I felt patient would struggle with AA psychologically
• Very chaotic house hold
• Nutritional status ok
Outcome
• Unfortunately endoscopy after 8 weeks still showed EoE
therefore placed on AA.
Principles of a Dietetic Consultation
• Which foods need to be avoided
• Suitable alternatives to these foods
• Practical advice for living on a restricted diet
Initial tips for Parents
• Ask them to look at the tins and packets of food
already in their home
• Make time to go food shopping
• Provide a list of foods available in major
supermarkets and recipes to help plan meals
• Re-assure them it does get easier
Nutritional Deficiency
-Macronutrients
• When food is removed from the diet there is a risk that
nutritional requirements will not be met.
• 12 cases of Kwashiorkor in American children, half due to
deliberate food avoidance for suspected allergies without
adequate substitution. (3)
• Children with 2 or more food allergies are shorter based
on the population without food allergies (4).
• Weight and height can be useful and important to monitor
overall nutrition
Nutritional Deficiency
-Macronutrients
In practice
• Unfortunately common for patients to loose weight
• Food fortification advice
• Violife cream cheese (48kcal/20g)
• Oat cream ( 150kcal/100ml)
• Swap cartons coconut milk (20kcal/100ml) to tinned
(170kcal/100ml)
• Supplements
• AA based
• Calogen (add to food)
• Monitor regularly
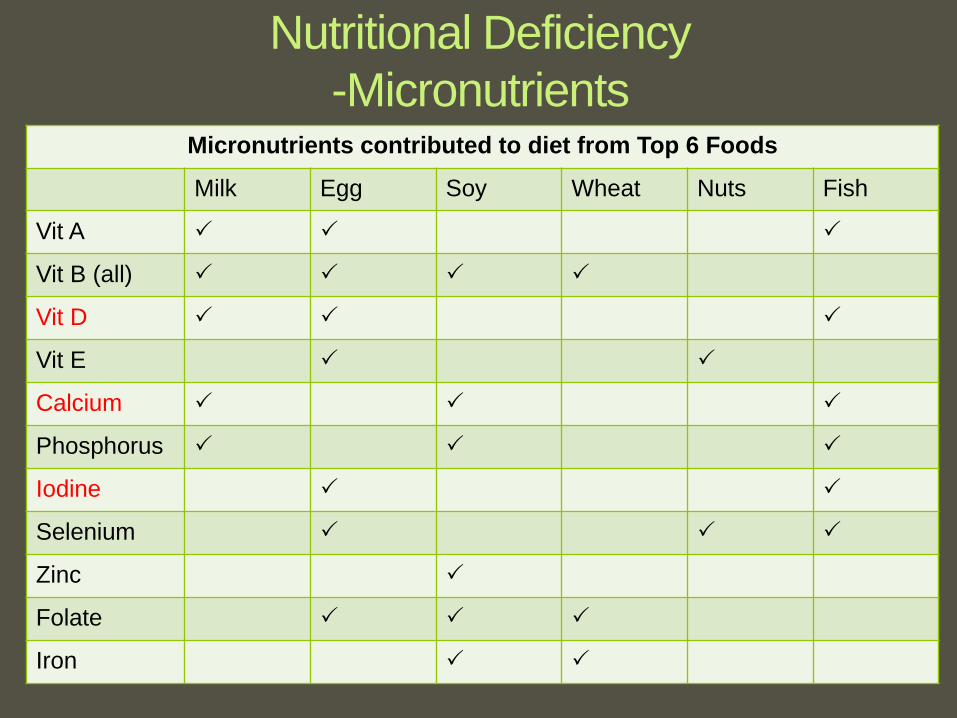
Micronutrients contributed to diet from Top 6 Foods
Milk Egg Soy Wheat Nuts Fish
Vit A
Vit B (all)
Vit D
Vit E
Calcium
Phosphorus
Iodine
Selenium
Zinc
Folate
Iron
Nutritional Deficiency
-Micronutrients
Nutritional Deficiency
-Micronutrients
• Calcium and vitamin D deficiency can result in osteomalacia and rickets
• Increasing reports of restricted diets resulting in iodine deficiency and thyroid dysfunction (5)
• Monitoring
• Food diary analysis
• Blood test if possible
• Try to minimise risk by providing vitamin and mineral supplements.
• There is limited choice on prescription
• Increased variety to buy over the counter
Labelling
• EU food labelling laws require labels to clearly state if
common allergens are in the food product.
• Applies to all packaged and manufactured drinks as well
as foods sold loose and packed for direct sale
• “May contain” / “Made in a kitchen containing…” is often
suitable
• Gluten is ok majority of time - Just avoid wheat
• Soya lethicin - technically ok but advise to avoid all
sources to make more practical
Alternative Foods
• Good range of foods in supermarkets.
• Free from aisles (still double check labels)
• “normal aisles” have plenty of options
• Aware of hidden sources of foods – check labels
• Fussy eaters
• top 6 free diet is still achievable (just a little harder)
Main Foods Missed
• Milk
• Prescribed age appropriate
• Rice, coconut and oat milk, look for “added nutrition”
• Bread
• B-free, ENRG, Schar
• Wraps and bread rolls often better tolerated.
• Cake/biscuits
• Make own cornflake/rice-krispie bars with moo free chocolate/marshmallows
• Biscuits better choice
• Flap jacks/Oat bars (toddler food range)
Main Foods Missed
• Chocolate
• Moo Free (good website)
• Crisps
• Mainly younger children wanting “bite and dissolve” textures
• Skips suitable
• Corn based
• Gravy
• Can make own using meat juices and corn flour
• Tesco free from gravy

Economical
• Can be expensive
• Online shop for 3 days following top 6 free diet = £22.
Buying same products for a non restricted diet = £13.50
Top 6 Free suitable
food
Non restricted diet
food
Bread £3 (400g loaf) £1 (800g branded
loaf)
Milk £1.40 (1L) £0.75 (1.1L cows
milk)
Pasta £1.20 (500g) £0.59 (500g)
Economical
• Advice:
• Bulk buy suitable foods when reduced and freeze
• Try to buy most of the food from “normal aisles”
• Base meals around foods that are naturally suitable
(meat, potatoes, rice etc.)
• Ask GP to prescribe a small amount of suitable products
each month
• This is GP discretion and therefore not guaranteed
Cooking
• Good cooking skills are helpful (remember that not
everyone has these or the confidence to try making new
food)
• Supply basic recipes to help.
• After a few weeks parents tend to find that their cooking
skills and confidence with “new foods” improve.
• Currently looking at setting up top 6 free group cooking
sessions
Eating away from home
- Schools
• Send with packed lunch if possible.
• provide parents with a range of ideas for example: • Sandwich, crisps, fruit, coconut based yoghurt
• Pasta in a tomato sauce (cold), jelly, cereal bar
• Parents to speak to school catering about dietary restrictions.
• If any problems, dietitian can phone and speak to catering staff
• Send child to school with plenty of suitable snacks
• If receive school milk, consider sending own little carton of
suitable milk
Eating away from home
- Parties and Restaurants
• If going to a party take own food
• If child regularly goes to a friends house for meals,
consider proving friends parents with suitable foods to
keep in their house
• If eating out, phone restaurant or look online at menu
beforehand to see if can cater for a top 6 free diet
• Most of the main chain restaurants should be able to
cater.
• Check social media for independent restaurants.
Eating out examples
• Pizza Express • Gluten free dough balls
• Gluten free pizza (no cheese) meat and veg topping
• Sorbet
• Nandos • Any marinated chicken
• Sweetcorn +/- chips or sweet potato wedges
• Mexican style ice-cream
• McDonalds • Burger no bun
• Chips/fruit sides
Conclusion
• Top 6 free diet can induce remission in the majority or
patients with EoE
• Following a top 6 free diet can be difficult and limiting
however providing patients with education and tips can
help children to feel less isolated and excluded
• Important to check nutritional status of patients and
monitor regularly
References
1. Guidelines on eosinophilic esophagitis: evidence-based statements and
recommendations for diagnosis and management in children and adults. Lucendo,
Alfredo J, et al. 0, 2017, United European Gastroenterology Journal, Vol. 0, pp. 1-
24.
2. Management guidelines of eosinophilic esophagitis in children. Papadopoulou, A, et
al. 1, s.l. :ESPGHAN EoE Working Group/GI Committee, 2014, JPGN, Vol 58, pp.
107-118.
3. Kwashiorkor in the United States: fad diets, percieved and true milk allergy, and
nutritional ignorance. Liu T, Howard RM, Mancini AJ, Weston WL, Paller AS,
Drolet BA, et al. Archives of dermatology. 2001; 137(5):630-6. Epub 04/04/2017
4. Growth and Nutritional Concerns in Children with Food Allergy. Mehta H, Groetch M,
Wang J. Curr opin Allergy Clin Immunol. 2013; 13(3):275-279.
5. Dietary restriction causing iodine-deficient goitre. Cheetham T, Plumb E, Callaghan
J, et al. Arch Dis Child Published online First: 15.06.2015