
OVID SP: o MEDLINE (1946-present)iom.nationalacademies.org/~/media/Files/Report...
36
Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 1 Literature Search Strategy for Gulf War and Health: Treatment for Chronic Multisymptom Illness The literature search was conducted in January 2012. Details below include the databases and the Medline search string that was used (other databases were searched similarly to Medline). The electronic databases consulted for this literature review included: • OVID SP: o MEDLINE (1946-present) o EMBASE (1947-present) o Evidence Based Medicine (EBM) Reviews: ACP Journal Club (1991-present) Cochrane Central Register of Controlled Trials (1991-present) Cochrane Database of Systematic Reviews (2005–present) Cochrane Health Technology Assessment (2001-present) Database of Abstracts of Reviews of Effectiveness (DARE) (1991-present) o PsycINFO (1987-present) • Web of Science: o Science Citation Index (1899-present) o Social Science Citation Index (1956-present) • CINAHL (1937-present, searched in April 2012) All searches were limited to years of publication, 2000-present, human studies and adults. The search strategy for MEDLINE is included below. This comprised the “template” for searches run against all other databases: Notes on OVID syntax: Terms immediately followed by a forward slash (/) are Medical Subject Headings (MeSH headings from MEDLINE). The asterisk after some terms (*) is the OVID unlimited truncation symbol (for example, rat*, will retrieve rat, rats, ratify, rational, etc.). The question mark after some terms is used to substitute for one or no characters. The post-qualification .ti,ab. means that a term was searched only in the title and abstract fields. The post-qualification, .pt. means that a term was searched only in the publication type field, and the post-qualification sh means that a term was searched only in the subject heading field. Adj is an adjacency or proximity operator used to capture words that occur within n words of one another in any order, minus stop-words (articles, prepositions, etc.) Exp means that a term was “exploded” in the MeSH vocabulary to also capture all narrower terms
-
Upload
nguyenhanh -
Category
Documents
-
view
215 -
download
2
Transcript of OVID SP: o MEDLINE (1946-present)iom.nationalacademies.org/~/media/Files/Report...

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 1
Literature Search Strategy for Gulf War and Health: Treatment for Chronic Multisymptom Illness
The literature search was conducted in January 2012. Details below include the databases and the Medline search string that was used (other databases were searched similarly to Medline). The electronic databases consulted for this literature review included:
• OVID SP: o MEDLINE (1946-present) o EMBASE (1947-present) o Evidence Based Medicine (EBM) Reviews:
� ACP Journal Club (1991-present) � Cochrane Central Register of Controlled Trials (1991-present) � Cochrane Database of Systematic Reviews (2005–present) � Cochrane Health Technology Assessment (2001-present) � Database of Abstracts of Reviews of Effectiveness (DARE) (1991-present)
o PsycINFO (1987-present)
• Web of Science: o Science Citation Index (1899-present) o Social Science Citation Index (1956-present)
• CINAHL (1937-present, searched in April 2012)
All searches were limited to years of publication, 2000-present, human studies and adults. The search strategy for MEDLINE is included below. This comprised the “template” for searches run against all other databases: Notes on OVID syntax: Terms immediately followed by a forward slash (/) are Medical Subject Headings (MeSH headings from
MEDLINE). The asterisk after some terms (*) is the OVID unlimited truncation symbol (for example, rat*, will retrieve rat, rats,
ratify, rational, etc.). The question mark after some terms is used to substitute for one or no characters. The post-qualification .ti,ab. means that a term was searched only in the title and abstract fields. The post-qualification, .pt. means that a term was searched only
in the publication type field, and the post-qualification sh means that a term was searched only in the subject heading field. Adj is an
adjacency or proximity operator used to capture words that occur within n words of one another in any order, minus stop-words
(articles, prepositions, etc.) Exp means that a term was “exploded” in the MeSH vocabulary to also capture all narrower terms

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 2
associated with the broader concept.
1. persian gulf syndrome/ 2. ((syndrome adj3 persian gulf) or (syndrome adj3 gulf war)).ti,ab. 3. (gulf illness* or "gulf war illness*" or "gulf war related").ti,ab. 4. (chronic multisymptom illness* or chronic multi-symptom illness* or unexplained multisymptom illness* or unexplained multi-symptom illness*).ti,ab. 5. ((unexplained or undiagnosed) adj3 (illness* or symptom* or condition or syndrome* or disease*)).ti,ab. 6. "medically unexplained".ti,ab. 7. or/1-6 8. Somatoform Disorders/ or (somatoform or somatic).ti,ab. 9. Chronic Pain/ 10. chronic pain?.ti,ab. 11. exp headache disorders/ or headache/ 12. (headache or migraine*).ti,ab. 13. exp Memory Disorders/ 14. Cognition Disorders/ 15. ((memory or concentration or cognitive or cognition) adj (problem? or disorder? or symptom? or abnormalit* or disease? or condition? or syndrome?)).ti,ab. 16. exp Gastrointestinal Diseases/ 17. irritable bowel.ti,ab. 18. ((gastrointestinal or intestinal or stomach) adj (problem? or disorder? or symptom? or abnormalit* or disease? or condition? or syndrome?)).ti,ab. 19. Fatigue Syndrome, Chronic/ 20. chronic fatigue.ti,ab. 21. Fibromyalgia/ 22. fibromyalgia?.ti,ab. 23. exp Sleep Disorders/ 24. insomnia*.ti,ab. 25. (sleep* adj (disturbance? or problem? or disorder? or symptom? or abnormalit* or disease? or condition? or syndrome?)).ti,ab. 26. exp Respiration Disorders/ 27. ((respiration or respiratory) adj (problem? or disorder? or symptom* or abnormalit* or disease? or condition? or syndrome?)).ti,ab. 28. exp Skin Diseases/ 29. ((skin or dermatalogic) adj (problem? or disorder? or symptom* or abnormalit* or disease? or condition? or syndrome?)).ti,ab. 30. or/8-29 31. (undiagnosed or unexplained).ti,ab.

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 3
32. 30 and 31 33. trauma response spectrum disorder.ti,ab. 34. ((sub-syndromal or subsyndromal) adj (anxiety or depression)).ti,ab. 35. functional somatic syndrome?.ti,ab. 36. conversion disorder?.ti,ab. 37. mixed anxiety depression.ti,ab. 38. "mixed anxiety and depression".ti,ab. 39. or/33-38 40. 7 or 32 or 39 41. limit 40 to yr="2000 -Current" 42. exp animals/ not humans.sh. 43. 41 not 42 44. exp therapeutics/ or exp combined modality therapy/ or exp complementary therapies/ or exp drug therapy/ or exp patient care/ or exp physical therapy modalities/ or exp rehabilitation/ or exp respiratory therapy/ 45. exp psychotherapy/ 46. (treatment? or intervention? or therap*).ti,ab. 47. integrative medicine.ti,ab. 48. Patient-Centered Care/ 49. exp disease management/ 50. prognosis/ or disease-free survival/ or medical futility/ or treatment outcome/ or treatment failure/ 51. (rehabilitation or self-care or disease management or patient care or patient centered care or exercise).ti,ab. 52. (mind body or stepped intensity).ti,ab. 53. exp clinical trial/ or multicenter study/ 54. exp clinical trials as topic/ 55. clinical trial.pt. 56. randomized controlled trial.pt. 57. controlled clinical trial.pt. 58. multicenter study.pt. 59. clinical trial phase $.pt. 60. (trial or multicenter stud* or multi-center stud*).ti,ab. 61. (randomized or randomly or placebo).ti,ab. 62. or/44-61 63. 43 and 62 64. (adolescent/ or exp child/ or exp infant/) not exp adult/ 65. 63 not 64

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 4
Gulf War and Health: Treatment for Chronic Multisymptom Illness
Excluded Literature at the Full-Text Level Screening
In the literature search for the Gulf War and Health: Treatment of Chronic Multisymptom Illness report, the committee excluded 119 manuscripts for various reasons outlined in the report. The following alphabetical list includes these manuscripts excluded at the full-text level screening with the reason for exclusion in bold italics after each reference.
Review: Antidepressants are effective for clinical improvement in unexplained physical symptoms and syndromes [therapeutics]. 2000. ACP
Journal Club September/October 133(2)(53). (No original data)
Dm approach to unexplained chronic symptoms produces consistent outcomes, solid roi. 2001. Disease Management Advisor 7(6):85-88. (No
original data)
Acker, S. 2010. Occupational therapy should be part of conversion disorder treatment. Journal of Psychosocial Nursing & Mental Health Services 48(3):12, 45. (No original data)
Aiarzaguena, J. M., G. Grandes, I. Gaminde, A. Salazar, A. Sanchez, and J. Arino. 2007. A randomized controlled clinical trial of a psychosocial and communication intervention carried out by gps for patients with medically unexplained symptoms. Psychological Medicine 37(2):283-294. (Does not describe an intervention to treat or manage illness/symptoms)
Amin, M. M., J. E. Broderick, M. S. Gold, and A. R. Gold. 2008. The effect of nasal continuous positive airway pressure (cpap) on the symptoms of gulf war syndrome (gws) [abstract]. Sleep 31(Suppl):a159 [0476]. (Meeting abstract only)
Amin, M. M., M. S. Gold, J. E. Broderick, and A. R. Gold. 2011. The effect of nasal continuous positive airway pressure on the symptoms of gulf war illness. Sleep & Breathing 15(3):579-587. (Does not address CMI)
Ataoglu, A., A. Ozcetin, C. Icmeli, and O. Ozbulut. 2003. Paradoxical therapy in conversion reaction. Journal of Korean Medical Science 18(4):581-584. (Does not address CMI)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 5
Barsky, A. J., and D. K. Ahern. 2004. Cognitive behavior therapy for hypochondriasis: A randomized controlled trial. JAMA: Journal of the
American Medical Association 291(12):1464-1470. (Does not address CMI)
Bleichhardt, G., B. Timmer, and W. Rief. 2005. Predictors for short- and long-term outcome in patients with somatoform disorders after cognitive-behavioral therapy. Zeitschrift Fur Klinische Psychologie Psychiatrie Und Psychotherapie 53(1):40-58. (Does not describe an intervention used
to treat or manage illness/symptoms; Link to Rief 2002; Bleichhardt 2004; and Timmer 2006)
Bradley, L. A., N. E. McKendree-Smith, and L. R. Cianfrini. 2003. Cognitive-behavioral therapy interventions for pain associated with chronic illnesses. Seminars in Pain Medicine 1 (2):44-54. (No original data)
Buil, T., J. A. Spaans, and M. E. F. Buhring. 2009. Bodymentalization, its clinical assessment and therapeutic application in the treatment of severe unexplained physical symptoms. Journal of Psychosomatic Research 66(6):553-553. (Meeting abstract only)
Castao, J., C. Garnier, D. Crcoles, L. Rodriguez, B. Diaz, L. M. Martin, and A. Bulbena. 2008. Efficacy of duloxetine in painful symptoms with major depressive disorder. European Neuropsychopharmacology Conference: 21st ECNP Congress Barcelona Spain. Conference Start: 20080830 Conference End: 20080903. Conference Publication: (var.pagings). 18 (S4):S298-S299. (Meeting abstract only)
Centre for Reviews and Dissemination. 2011. Antidepressant therapy for unexplained symptoms and symptom syndromes (structured abstract). Database of Abstracts of Reviews of Effects(4). (Published prior to 2000)
———. 2011. Cognitive-behavior therapy for medically unexplained symptoms: A critical review of the treatment literature (structured abstract). Database of Abstracts of Reviews of Effects(4). (No original data- Commentary on Nezu et al. 2001)
———. 2011. Efficacy of short-term psychotherapy for multiple medically unexplained physical symptoms: A meta-analysis (provisional abstract). Database of Abstracts of Reviews of Effects(4). (No original data- Commentary on Kleinstauber et al. 2011)
———. 2011. Efficacy of treatment for somatoform disorders: A review of randomized controlled trials (structured abstract). Database of
Abstracts of Reviews of Effects(4). (No original data- Commentary on Kroenke et al. 2007)
———. 2011. Psychosocial treatments for multiple unexplained physical symptoms: A review of the literature (structured abstract). Database of
Abstracts of Reviews of Effects(4). (No original data- Commentary on Allen et al. 2002)
Clauw, D. J., C. C. Engel, S. Donta, A. Barkhuizen, J. S. Skinner, P. Peduzzi, P. Guarino, D. A. Williams, T. Taylor, L. Kazis, J. R. Feussner, and C. S. P. S. G. the. 2002. Effectiveness of aerobic exercise and cognitive behavioral therapy in 1092 veterans with chronic multisymptom illnesses: Results from csp #470. Arthritis and Rheumatism 46(9):S106-S107. (Meeting abstract only)
Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 6
Collins, J. F., S. T. Donta, C. C. Engel, J. B. Baseman, L. L. Dever, T. Taylor, K. D. Boardman, S. E. Martin, A. L. Wiseman, and J. R. Feussner. 2002. The antibiotic treatment trial of gulf war veterans' illnesses: Issues, design, screening, and baseline characteristics. Controlled Clinical Trials 23(3):333-353. (Other- No results presented)
Conboy, L., M. St. John, and R. Schnyer. 2012. The effectiveness of acupuncture in the treatment of gulf war illness. Contemporary Clinical
Trails?(?):? (Other- no results presented)
Cook, D. B., A. J. Stegner, and L. D. Ellingson. 2010. Exercise alters pain sensitivity in gulf war veterans with chronic musculoskeletal pain. Journal of Pain 11(8):764-772. (Does not address CMI)
Crompton, N. 2003. To investigate the effectiveness of (manualised) reattribution therapy in the treatment of medically unexplained symptoms (mus) within the general hospital. National Research Register. (Other- No results presented)
Davidson, J. R. T., C. Crawford, J. A. Ives, and W. B. Jonas. 2011. Homeopathic treatments in psychiatry: A systematic review of randomized placebo-controlled studies. Journal of Clinical Psychiatry 72(6):795-805. (Only describes existing syndromes (CF, FM, IBS, Depression,
Anxiety, etc.))
Dickinson, W., L. Dickinson, F. V. deGruy, D. S. Main, L. M. Candib, and K. Rost. 2003. A randomized clinical trial of a care recommendation letter intervention for somatization in primary care. Annals of Family Medicine 1(4):228-235. (Does not describe an intervention to treat or
manage illness/symptoms)
Edwards, T. M., A. Stern, D. D. Clarke, G. Ivbijaro, and L. M. Kasney. 2011. The treatment of patients with medically unexplained symptoms in primary care: A review of the literature. Mental Health in Family Medicine 7 (4):209-221. (No original data)
Engel, C. C., Jr., X. Liu, B. D. McCarthy, R. F. Miller, and R. Ursano. 2000. Relationship of physical symptoms to posttraumatic stress disorder among veterans seeking care for gulf war-related health concerns. Psychosomatic Medicine 62(6):739-745. (Does not describe an intervention to
treat or manage illness/symptoms)
Escobar, J. I. 2006. An effective intervention for medically unexplained symptoms in primary care. World Psychiatric Association, International
Congress. (Meeting abstract only)
Escobar, J. I., M. Gara, I. Alex, L. Allen, A. Diaz-Martinez, and M. Warman. 2004. Treatment of patients presenting with unexplained physical symptoms in primary care. Neuropsychopharmacology 29(1). (Meeting abstract only)
Flynn. 2011. Management of medically unexplained symptoms (chronic pain and fatigue) (structured abstract). Health Technology Assessment
Database(4). (Abstract only)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 7
Fritzsche, K., H. Sandholzer, E. Wetzler-Burmeister, A. Hartmann, M. Cierpka, H. C. Deter, R. Richter, B. Schmidt, M. Harter, C. Hoger, and M. Wirsching. 2010. Symptom presentation, interventions, and outcome of emotionally-distressed patients in primary care. Psychosomatics 51(5):386-394. (Does not describe an intervention used to treat or manage illness/symptoms- cross-sectional study design)
Fritzsche, K., Z. Xudong, K. Anselm, S. Kern, M. Wirsching, and R. Schaefert. 2011. The treatment of patients with medically unexplained physical symptoms in china: A study comparing expectations and treatment satisfaction in psychosomatic medicine, biomedicine, and traditional chinese medicine. International Journal of Psychiatry in Medicine 41(3):229-244. (Does not describe an intervention used to treat or manage
illness/symptoms- Cross-sectional study design)
Glass, J. M., A. K. Lyden, F. Petzke, P. Stein, G. Whalen, K. Ambrose, G. Chrousos, and D. J. Clauw. 2004. The effect of brief exercise cessation on pain, fatigue, and mood symptom development in healthy, fit individuals. Journal of Psychosomatic Research 57(4):391-398. (Does not
describe an intervention to treat or manage illness/symptoms)
Gottschalk, J. M., G. Bleichhardt, W. Hiller, M. Berking, and W. Rief. 2011. Cognitive-behavioral therapy enriched with emotion regulation training (encert) in patients with multiple somatoform symptoms: Preliminary findings. Verhaltenstherapie Conference: 13. Kongress der Deutschen Gesellschaft fur Verhaltensmedizin und Verhaltensmodifikation - DGVM Luxemburg Luxembourg. Conference Start: 20110929 Conference End: 20111001 Sponsor: Medtronic. Conference Publication: (var.pagings). 21:36-37. (Meeting abstract only)
Guarino, P., P. Peduzzi, S. T. Donta, C. C. Engel, D. J. Clauw, D. A. Williams, J. S. Skinner, A. Barkhuizen, L. E. Kazis, and J. R. Feussner. 2001. A multicenter two by two factorial trial of cognitive behavioral therapy and aerobic exercise for gulf war veterans' illnesses: Design of a veterans affairs cooperative study (csp #470). Controlled Clinical Trials 22(3):310-332. (Other- No results presented; Link to Donta et al. 2003 (#130)
and Mori et al. 2006 (#210))
Guilleminault, C., and R. Dave. 2003. Upper airway resistance syndrome, insomnia, and functional somatic syndromes. Chest 123 (1):12-14. (No
original data)
Gutman, S. A., H. Diamond, S. E. Holness-Parchment, D. N. Brandofino, D. G. Pacheco, M. Jolly-Edouard, and S. Jean-Charles. 2004. Enhancing independence in women experiencing domestic violence and possible brain injury: An assessment of an occupational therapy intervention. Occupational Therapy in Mental Health 20 (1):49-79. (Only describes existing syndromes)
Halpern, J., M. Cohen, and G. Kennedy. 2010. Yoga for improving sleep and life quality in the elderly population. Sleep and Biological Rhythms Conference: 22nd Annual Scientific Meeting of the Australian Sleep Association and Australian Sleep Technologists Association: Sleep Down Under 2010 - Biodiversity of Sleep Christchurch New Zealand. Conference Start: 20101021 Conference End: 20101023. Conference Publication: (var.pagings). 8:A41. (Meeting abstract only)
Hassett Al, S. S. V. 2008. A computer-based intervention for medically unexplained physical symptoms [nct00468013]. ClinicalTrials.gov
[www.clinicaltrials.gov]. (Other- No results presented)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 8
Hatcher, S., and B. Arroll. 2008. Assessment and management of medically unexplained symptoms. BMJ 336(7653):1124-1128. (No original
data)
Heijmans, M., T. C. Olde Hartman, E. van Weel-Baumgarten, C. Dowrick, P. L. B. J. Lucassen, and C. van Weel. 2011. Experts' opinions on the management of medically unexplained symptoms in primary care. A qualitative analysis of narrative reviews and scientific editorials. Family
Practice 28(4):444-455. (No original data)
Henningsen, P., H. Sattel, H. Gndel, E. Guthrie, J. Kruse, C. Lahmann, M. Noll-Hussong, C. Ohmann, J. Ronel, M. Sack, N. Sauer, and G. Schneider. 2010. Brief psychodynamic-interpersonal psychotherapy for patients with pain-predominant multisomatoform disorder: A randomized controlled trial. Journal of Psychosomatic Research Conference: 13th Annual Meeting of the European Association for Consultation-Liaison Psychiatry and Psychosomatics, EACLPP, 28th European Conference on Psychosomatic Research, ECPR Innsbruck Austria. Conference Start: 20100630 Conference End: 20100703. Conference Publication: (var.pagings). 68 (6):631-632. (Meeting abstract only)
Henningsen, P., S. Zipfel, and W. Herzog. 2007. Management of functional somatic syndromes. Lancet 369(9565):946-955. (No original data)
Hillert, L., P. Savlin, A. Levy Berg, A. Heidenberg, and B. Kolmodin-Hedman. 2002. Environmental illness--effectiveness of a salutogenic group-intervention programme. Scandinavian Journal of Public Health 30(3):166-175. (Does not address CMI)
Hoedeman, R., A. H. Blankenstein, C. M. van der FeltzCornelis, B. Krol, R. Stewart, and J. W. Groothoff. 2009. Consultation letters for medically unexplained physical symptoms in primary care. Cochrane Database of Systematic Reviews(1). (Other- Same publication as Hoedeman et al.
2010)
Hoedeman, R., A. H. Blankenstein, C. M. van der Feltz-Cornelis, B. Krol, R. Stewart, and J. W. Groothoff. 2010. Consultation letters for medically unexplained physical symptoms in primary care. Cochrane Database of Systematic Reviews 12:CD006524. (Does not describe an
intervention to treat or manage illness/symptoms)
Hunt, S. C., R. D. Richardson, and C. C. Engel, Jr. 2002. Clinical management of gulf war veterans with medically unexplained physical symptoms. Military Medicine 167(5):414-420. (No original data)
Jackson, J. L., S. George, and S. Hinchey. 2009. Medically unexplained physical symptoms. Journal of General Internal Medicine 24(4):540-542. (No original data)
Jackson, J. L., and K. Kroenke. 2006. Managing somatization: Medically unexplained should not mean medically ignored. Journal of General
Internal Medicine 21(7):797-799. (No original data)
Jacob, K. S. 2004. A simple protocol to manage patients with unexplained somatic symptoms in medical practice. National Medical Journal of
India 17(6):326-328. (No original data)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 9
Kawana, N., S.-i. Ishimatsu, and K. Kanda. 2001. Psycho-physiological effects of the terrorist sarin attack on the tokyo subway system. Military
Medicine 166(12,Suppl 2):23-26. (Does not describe an intervention to treat or manage illness/symptoms)
Khattak, T., S. Farooq, and B. Jan. 2006. Behavior therapy in dissociative convulsions disorder. Jcpsp, Journal of the College of Physicians &
Surgeons - Pakistan 16(5):359-363. (Does not address CMI)
Kolk, A., S. Schagen, and G. Hanewald. 2004. Multiple medically unexplained physical symptoms and health care utilization: Outcome of psychological intervention and patient-related predictors of change. Journal of Psychosomatic Research 57(4):379-389. (Does not describe an
intervention)
Kroenke, K., I. Benattia, J. Musgnung, J. Graepel, and S. Stahl. 2004. Short-term treatment of depressed and anxious primary care patients with multiple, unexplained somatic symptoms: A pilot study. Neuropsychopharmacology 29(1). (Meeting abstract only)
Labys, C. A. 2010. The treatment of gulf war syndrome with cognitive behavioral therapy a case comparison study. Dissertation: Thesis (Psy.D.), Rutgers University. (Case study or case series)
Lacour, M., T. Zunder, M. Dettenkofer, S. Schonbeck, R. Ludtke, and C. Scheidt. 2002. An interdisciplinary therapeutic approach for dealing with patients attributing chronic fatigue and functional memory disorders to environmental poisoning - a pilot study. International Journal of Hygiene
and Environmental Health 204(5-6):339-346. (Does not address CMI)
Lamberg, L. 2005. New mind/body tactics target medically unexplained physical symptoms and fears. JAMA: Journal of the American Medical
Association 294(17):2152-2154. (No original data)
Larisch, A., A. Schweickhardt, M. Wirsching, and K. Fritzsche. 2004. Psychosocial interventions for somatizing patients by the general practitioner - a randomized controlled trial. Journal of Psychosomatic Research 57(6):507-514. (Does not describe an intervention to treat or
manage illness/symptoms; Link to Schweickhardt 2005 #1549)
Laugharne, J., and A. Janca. 2007. Icd-10 telepsychiatry education in western australia: Bridging the distance. Primary Care & Community
Psychiatry 12(3-4):145-149. (Does not describe an intervention to treat or manage illness/symptoms)
Lehrer, P. M., M. Karavidas, M. Gara, A. Kotay, J. Mayers, J. Sawaya, N. Breach, A. Gonzalez-Restrepo, R. Liu, and J. Escobar. 2010. Exploratory pilot study, randomized controlled blinded trial on medically unexplained physical symptoms (mups). Biological Psychology 85(3):517-517. (Meeting abstract only)
Lein, C., and C. E. Wills. 2007. Using patient-centered interviewing skills to manage complex patient encounters in primary care. Journal of the
American Academy of Nurse Practitioners 19(5):215-220. (No original data)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 10
Levenstein, S. 2009. The evidence for treatments for somatoform disorders: A view from the trenches. In Somatic presentations of mental
disorders: Refining the research agenda for dsm-v. Arlington, VA: American Psychiatric Publishing, Inc ; US. Pp. 165-169. (No original data)
Li, C. T., T. P. Su, and J. C. Hsieh. 2011. Rtms efficacy in relieving medically unexplained pain in depressive patient is independent of its antidepressant effect. Biological Psychiatry Conference: 66th Annual Meeting of the Society of Biological Psychiatry San Francisco, CA United States. Conference Start: 20110512 Conference End: 20110514. Conference Publication: (var.pagings). 69 (9 SUPPL. 1):277S. (Meeting abstract
only)
Lincoln, A. E., D. A. Helmer, A. I. Schneiderman, M. Li, H. Copeland, M. K. Prisco, M. T. Wallin, H. K. Kang, and B. H. Natelson. 2006. The war-related illness and injury study centers: A resource for deployment-related health concerns. Military Medicine 171(7):577-585. (Case study or
case series)
Lipsitt, D. R., and V. Starcevic. 2006. Psychotherapy and pharmacotherapy in the treatment of somatoform disorders. Psychiatric Annals 36(5):341-348. (No original data)
Luo, Z., J. Goddeeris, J. C. Gardiner, and R. C. Smith. 2007. Costs of an intervention for primary care patients with medically unexplained symptoms: A randomized controlled trial. Psychiatric Services 58(8):1079-1086. (Does not describe an intervention to treat or manage
illness/symptoms; Link to Lyles 2003 #127 & Smith 2006 #946)
Luttermoser, G. 2003. Cognitive behavioral therapy and exercise minimally help gulf war veterans' illnesses. Journal of Family Practice 52 (6):441-442. (No original data)
Lyles, J. S., A. Hodges, C. Collins, C. Lein, C. W. Given, B. Given, D. D'Mello, G. G. Osborn, J. Goddeeris, J. C. Gardiner, and R. C. Smith. 2003. Using nurse practitioners to implement an intervention in primary care for high-utilizing patients with medically unexplained symptoms. General Hospital Psychiatry 25(2):63-73. (Does not describe an intervention to treat or manage illness/symptoms; Link to Smith 2006 #946 &
Luo 2007 #104)
Margalit, A. P. A., and A. El-Ad. 2008. Costly patients with unexplained medical symptoms: A high-risk population. Patient Education &
Counseling 70(2):173-178. (Does not describe an intervention to treat or manage illness/symptoms)
Maunder, R., and J. Hunter. 2004. An integrated approach to the formulation and psychotherapy of medically unexplained symptoms: Meaning- and attachment-based intervention. American Journal of Psychotherapy 58(1):17-33. (No original data)
Meerman, E. E., B. Verkuil, and J. F. Brosschot. 2011. Decreasing pain tolerance outside of awareness. Journal of Psychosomatic Research 70(3):250-257. (Does not describe an intervention used to treat or manage illness/symptoms)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 11
Moene, F. C., P. Spinhoven, K. A. Hoogduin, and R. van Dyck. 2002. A randomised controlled clinical trial on the additional effect of hypnosis in a comprehensive treatment programme for in-patients with conversion disorder of the motor type. Psychotherapy and Psychosomatics 71(2):66-76. (Does not address CMI)
———. 2003. A randomized controlled clinical trial of a hypnosis-based treatment for patients with conversion disorder, motor type. The
International journal of clinical and experimental hypnosis 51(1):29-50. (Does not address CMI)
Morriss, R., C. Dowrick, P. Salmon, S. Peters, G. Dunn, A. Rogers, B. Lewis, H. Charles-Jones, J. Hogg, R. Clifford, C. Rigby, and L. Gask. 2007. Cluster randomised controlled trial of training practices in reattribution for medically unexplained symptoms. British Journal of Psychiatry 191:536-542. (Does not describe an intervention to treat or manage illness/symptoms)
Mosek, A., D. Yoel, A. Aylon, Z. Hybloom, F. Broitman, M. Kfir, and M. Bloch. 2011. The treatment of resistant, chronic, headaches and facial pain patients in a comprehensive multidisciplinary clinic. Cephalalgia Conference: 15th Congress of the International Headache Society Berlin Germany. Conference Start: 20110623 Conference End: 20110626. Conference Publication: (var.pagings). 31:177. (Meeting abstract only)
Mousavi, S. G., J. Rahimi, and H. Afshar. 2008. Comparison of four different treatment options in the management of acute conversion disorder. Iranian Journal of Psychiatry and Behavioral Sciences 2 (1):21-25. (Does not address CMI)
Neimark, G., S. N. Caroff, and J. L. Stinnett. 2005. Medically unexplained physical symptoms. Psychiatric Annals 35(4):298-305. (No original
data)
Nickel, R., K. Ademmer, and U. T. Egle. 2010. Manualized psychodynamic-interactional group therapy for the treatment of somatoform pain disorders. Bulletin of the Menninger Clinic 74(3):219-237. (No original data)
Oakley, A. M. M., and M. H. Rennie. 2004. Retrospective review of teledermatology in the waikato, 1997-2002. Australasian Journal of
Dermatology 45 (1):23-28. (Does not address CMI)
O'Malley, P. G. 2002. Treatment trials of unexplained symptom syndromes: Time for larger and longer trials to address the complexities. American Journal of Medicine 112 (3):237-239. (No original data)
O'Malley, P. G., J. L. Jackson, J. Santoro, and J. Price. 2000. Review: Antidepressants are effective for clinical improvement in unexplained physical symptoms and syndromes. Evidence-Based Medicine 5 (5):143. (Published prior to 2000)
Payne, H. 2009. The bodymind approach (bma) to psychotherapeutic groupwork with patients with medically unexplained symptoms (mus): A review of the literature, description of approach and methodology for a pilot study. European Journal of Psychotherapy and Counselling 11(3):287-310. (Other: No results presented, methods only (Payne 2009 #762; Payne et al 2010 #914))

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 12
Peters, S., C. C. Graham, and C. Dowrick. 2008. Psychological treatments for medically unexplained symptoms (mus) delivered by health professionals: Using qualitative methodologies to understand the story behind the numbers. Journal of Psychosomatic Research 64(6):668-668. (Meeting abstract only)
Pols, R. G., and M. W. Battersby. 2008. Coordinated care in the management of patients with unexplained physical symptoms: Depression is a key issue. Medical Journal of Australia 188(12 Suppl):S133-137. (Does not describe an intervention to treat or manage illness/symptoms)
Poole, N. A., A. Wuerz, and N. Agrawal. 2010. Abreaction for conversion disorder: Systematic review with meta-analysis. British Journal of
Psychiatry 197(2):91-95. (Does not address CMI)
Rasmussen, N. H., J. W. Furst, D. M. Swenson-Dravis, D. C. Agerter, A. J. Smith, M. A. Baird, and S. S. Cha. 2006. Innovative reflecting interview: Effect on high-utilizing patients with medically unexplained symptoms. Disease Management 9(6):349-359. (Does not describe an
intervention to treat or manage illness/symptoms)
Rosendal, M., F. Olesen, P. Fink, T. Toft, I. Sokolowski, and F. Bro. 2007. A randomized controlled trial of brief training in the assessment and treatment of somatization in primary care: Effects on patient outcome. General Hospital Psychiatry 29(4):364-373. (Does not describe an
intervention to treat or manage illness/symptoms)
Ruddy, R., and A. House. 2005. Psychosocial interventions for conversion disorder. Cochrane Database of Systematic Reviews(4):CD005331. (Other- Updated by Ruddy et al 2009)
Ruddy, R., and A. House. 2009. Psychosocial interventions for conversion disorder. Cochrane Database of Systematic Reviews(1). (Does not
address CMI. Review comparing Ataglou 2003, Moene 2002, and Moene 2003)
Russell, M. C. 2008. War-related medically unexplained symptoms, prevalence, and treatment: Utilizing emdr within the armed services. Journal
of EMDR Practice and Research 2(3):212-225. (Case study or case series)
Saenz Guerrero, A., C. Mugica Samperio, M. Avellanet Viladomat, and J. Obiols Llandrich. 2001. [conversion disorders: A therapeutic approach]. Medicina Clinica 117(20):798. (No original data)
Samarasekera, D., and D. Abbott. 2009. Addressing functional symptoms in neurology: Can outpatient intervention make a difference? Journal of
Neurology, Neurosurgery and Psychiatry Conference: Section of Neuropsychiatry (SoN) Royal College of Psychiatrists and British Neuropsychiatry Association: Joint Conference at the British Neuropsychiatry Association - 22nd Annual General Meeting London United Kingdom. Conference Start: 20090204 Conference End: 20090204. Conference Publication: (var.pagings). 80 (7):827. (Meeting abstract only)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 13
Samarasekera, S., and R. J. Abbott. 2010. Addressing functional symptoms in neurology: Can outpatient intervention make a difference? Journal
of Neurology, Neurosurgery and Psychiatry Conference: Association of British Neurologists Annual Meeting 2010, ABN Bournemouth United Kingdom. Conference Start: 20100511 Conference End: 20100514. Conference Publication: (var.pagings). 81 (11):e41. (Meeting abstract only)
Schilte, A. F., P. J. Portegijs, A. H. Blankenstein, H. E. van Der Horst, M. B. Latour, J. T. van Eijk, and J. A. Knottnerus. 2001. Randomised controlled trial of disclosure of emotionally important events in somatisation in primary care. BMJ 323(7304):86. (Does not describe an
intervention to treat or manage illness/symptoms)
Schroder, A., and P. Fink. 2011. Functional somatic syndromes and somatoform disorders in special psychosomatic units: Organizational aspects and evidence-based treatment. Psychiatric Clinics of North America 34(3):673-687. (No original data)
Schroeder, A., E. Rehfeld, E. Oernboel, M. Sharpe, R. W. Licht, and P. Fink. 2010. A novel treatment approach for people with severe functional somatic syndromes (stress-1): Randomized trial. Journal of Psychosomatic Research Conference: 13th Annual Meeting of the European Association for Consultation-Liaison Psychiatry and Psychosomatics, EACLPP, 28th European Conference on Psychosomatic Research, ECPR Innsbruck Austria. Conference Start: 20100630 Conference End: 20100703. Conference Publication: (var.pagings). 68 (6):664. (Meeting abstract
only)
Schwarz, D., J. Giessing, J. Heider, A. Zaby, and A. Schroder. 2009. Physical exercise in the treatment of somatoform symptoms: A literature review. Zeitschrift Fur Sportpsychologie 16(4):117-130. (ILL could not retrieve)
Schweickhardt, A., A. Larisch, and K. Fritzsche. 2005. Differentiation of somatizing patients in primary care - why the effects of treatment are always moderate. Journal of Nervous and Mental Disease 193(12):813-819. (Does not describe an intervention to treat or manage
illness/symptoms; Link to Larish 2004 #1169)
Schweickhardt, A., A. Larisch, M. Wirsching, and K. Fritzsche. 2007. Short-term psychotherapeutic interventions for somatizing patients in the general hospital: A randomized controlled study. Psychotherapy and Psychosomatics 76(6):339-346. (Does not describe an intervention to treat
or manage illness/symptoms)
Shapiro, A. P., and R. W. Teasell. 2004. Behavioural interventions in the rehabilitation of acute v. Chronic non-organic (conversion/factitious) motor disorders. British Journal of Psychiatry 185:140-146. (Case study or case series)
Sharpe, M., I. Butcher, A. Carson, J. Walker, J. Cavanagh, and C. Williams. 2008. A randomised controlled trial of a guided self-help intervention for patients with medically unexplained neurological symptoms. Journal of Psychosomatic Research 64(6):673-673. (Meeting abstract only)
Smith, R. C., J. C. Gardiner, Z. Luo, S. Schooley, L. Lamerato, and K. Rost. 2009. Primary care physicians treat somatization. Journal of General
Internal Medicine 24(7):829-832. (Does not describe an intervention to treat or manage illness/symptoms)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 14
Smith, R. C., C. Lein, C. Collins, J. S. Lyles, B. Given, F. C. Dwamena, J. Coffey, A. Hodges, J. C. Gardiner, J. Goddeeris, and C. Given. 2003. Treating patients with medically unexplained symptoms in primary care. Journal of General Internal Medicine 18(6):478-489. (No original data)
Smith, R. C., J. Lyles, and J. C. Gardiner. 2004. Effective primary care treatment for patients with medically unexplained symptoms - a clinical trial. Journal of General Internal Medicine 19:148-148. (Meeting abstract only)
Smith, R. C., J. S. Lyles, J. C. Gardiner, C. Sirbu, A. Hodges, C. Collins, F. C. Dwamena, C. Lein, C. Given, B. Given, and J. Goddeeris. 2006. Primary care clinicians treat patients with medically unexplained symptoms: A randomized controlled trial. Journal of General Internal Medicine 21(7):671-677. (Does not describe an intervention to treat or manage illness/symptoms; Link to Luo 2007 #127 & Lyles 2003 #127)
Smith, R. C., J. S. Lyles, J. Goddeeris, J. C. Gardiner, A. Hodges, C. Collins, C. Sirbu, C. Lein, F. C. Dwamena, C. W. Given, and B. Given. 2005. Primary care clinicians effectively treat patients with medically unexplained symptoms: A clinical trial. Psychosomatics 46(2):182-183. (Meeting
abstract only)
Smits, F. T. M., K. A. Wittkampf, A. H. Schene, P. J. E. Bindels, and H. C. P. M. Van Weert. 2008. Interventions on frequent attenders in primary care. A systematic literature review. Scandinavian Journal of Primary Health Care 26(2):111-116. (Does not address CMI)
Spaans, J. A., L. Veselka, P. Luyten, and M. E. F. Buhring. 2009. [bodily aspects of mentalization: A therapeutic focus in the treatment of patients with severe medically unexplained symptoms]. Tijdschrift voor Psychiatrie 51(4):239-248. (No original data)
Steele, R. E., E. De Leeuw, and D. O. Carpenter. 2009. A novel and effective treatment modality for medically unexplained symptoms. Journal of
Pain Management 1 (4):401-412. (Case report or case series)
Stuart, S., R. Noyes Jr, V. Starcevic, and A. Barsky. 2008. An integrative approach to somatoform disorders combining interpersonal and cognitive-behavioral theory and techniques. Journal of Contemporary Psychotherapy 38 (1):45-53. (No original data)
Timmer, B., G. Bleichhardt, and W. Rief. 2006. Importance of psychotherapy motivation in patients with somatization syndrome. Psychotherapy
Research 16(3):348-356. (Does not describe an intervention to treat or manage illness/symptoms; Link to Bleichhardt 2005 #1680; Bleichhardt
2004 #2044, and Rief 2002 #1722)
Toft, T., M. Rosendal, E. Ornbol, F. Olesen, L. Frostholm, and P. Fink. 2010. Training general practitioners in the treatment of functional somatic symptoms: Effects on patient health in a cluster-randomised controlled trial (the functional illness in primary care study). Psychotherapy &
Psychosomatics 79(4):227-237. (Does not describe an intervention to treat or manage illness/symptoms)
Tyrer, H., P. Tyrer, and I. Lovett. 2011. Adapted cognitive-behavior therapy for medically unexplained symptoms in secondary care reduces hospital contacts. Psychosomatics 52(2):194-196. (Case series)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 15
van Bokhoven, M. A., H. Koch, T. van der Weijden, R. P. T. M. Grol, A. D. Kester, P. E. L. M. Rinkens, P. J. E. Bindels, and G.-J. Dinant. 2009. Influence of watchful waiting on satisfaction and anxiety among patients seeking care for unexplained complaints. Annals of Family Medicine 7(2):112-120. (Does not describe an intervention to treat or manage illness/symptoms)
Van Der Feltz-Cornelis, C., P. Van Oppen, H. Ader, and R. Van Dyck. 2006. Collaborative care for medically unexplained physical symptoms in general practice. [dutch]. Huisarts en Wetenschap 49 (7):342-347. (Other- Translation of van der Feltz-Cornelis 2006 #334)
van der Feltz-Cornelis, C. M., P. van Oppen, H. J. Ader, and R. van Dyck. 2006. Randomised controlled trial of a collaborative care model with psychiatric consultation for persistent medically unexplained symptoms in general practice. Psychotherapy & Psychosomatics 75(5):282-289. (Does not describe an intervention to treat or manage illness/symptoms)
Wessely, S. 2004. The long aftermath of the 1991 gulf war. Annals of Internal Medicine 141 (2):155-156. (No original data)
Woolfolk, R. L., L. A. Allen, and J. E. Tiu. 2007. New directions in the treatment of somatization. Psychiatric Clinics of North America 30(4):621-644. (No original data)
Zonneveld, L. N. L., H. J. Duivenvoorden, J. Passchier, and A. van 't Spijker. 2010. Tailoring a cognitive behavioural model for unexplained physical symptoms to patient's perspective: A bottom-up approach. Clinical Psychology & Psychotherapy 17(6):528-535. (No original data)
Zonneveld, L. N. L., A. van 't Spijker, J. Passchier, J. J. van Busschbach, and H. J. Duivenvoorden. 2009. The effectiveness of a training for patients with unexplained physical symptoms: Protocol of a cognitive behavioral group training and randomized controlled trial. BMC Public
Health 9:251. (Other- No results presented)

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 16
Gulf War and Health: Treatment for Chronic Multisymptom Illness
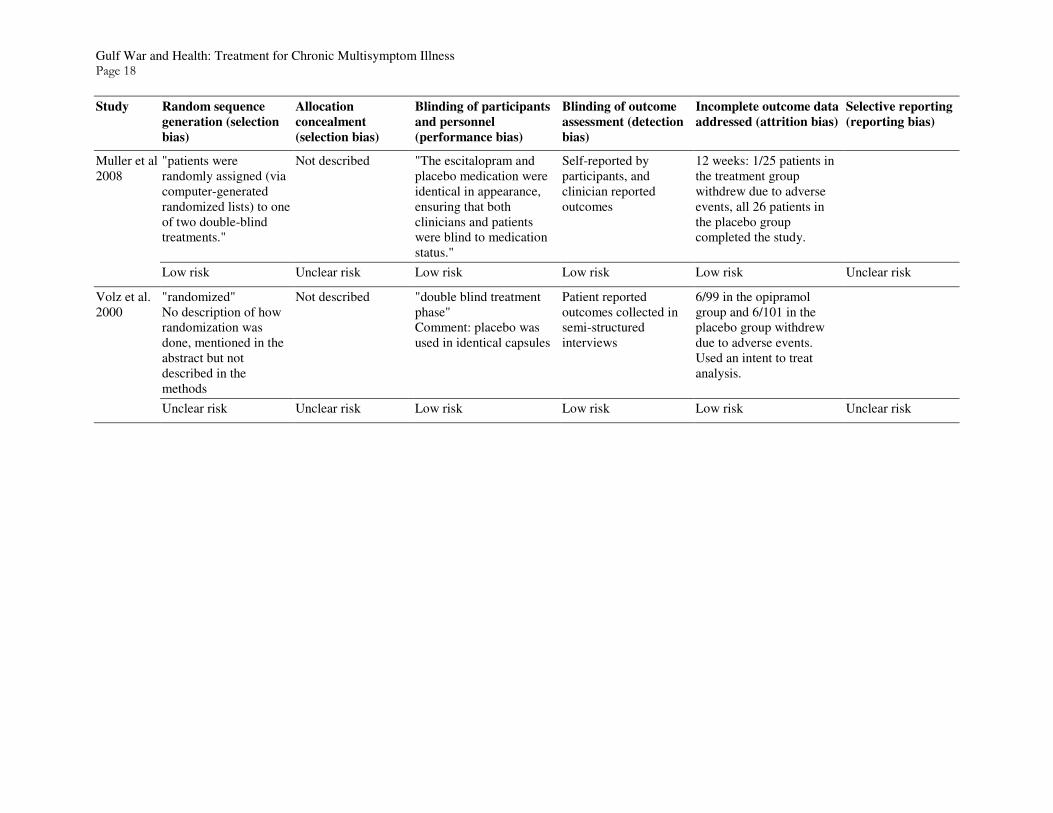
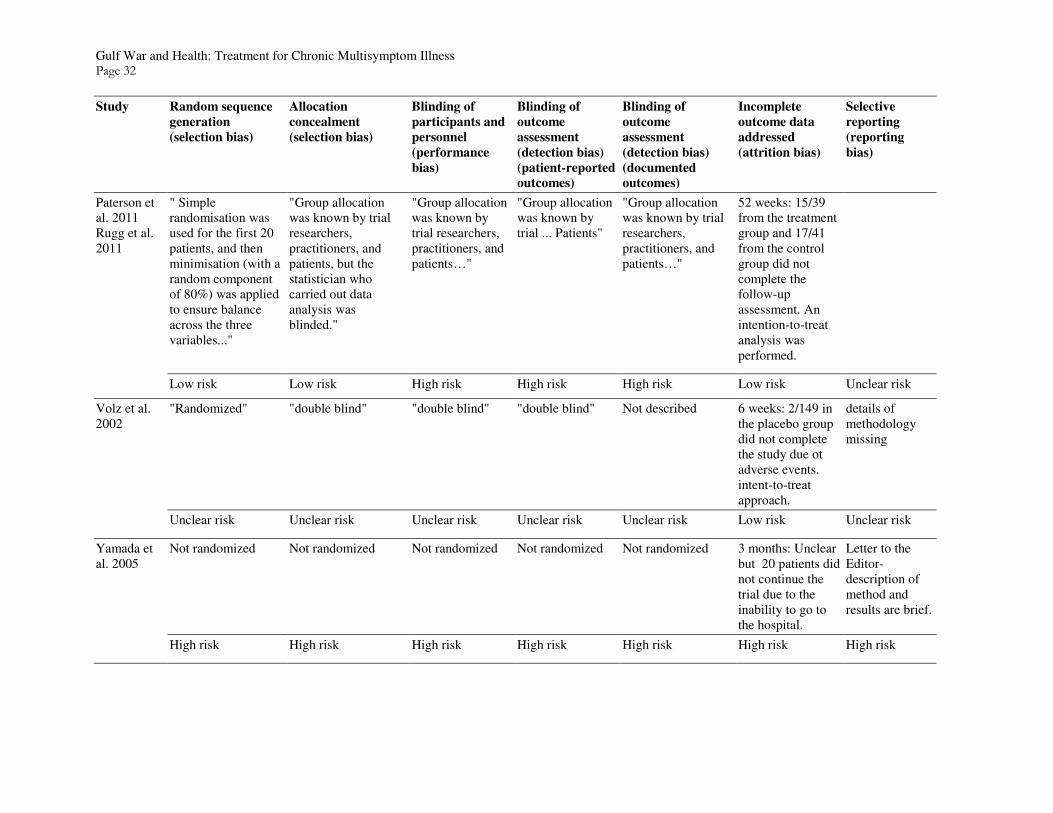
Risk of Bias for Included Studies The following tables show how the committee rated studies that met criteria for inclusion as described in the report. The risk of bias was determined based on guidance outlined in the Cochrane Handbook for Systematic Reviews of Interventions1. The committee constructed the following tables in their assessment. Studies are listed alphabetically by the type of intervention as presented in the report. A table of systematic reviews included in the committee’s evaluation of treatments is last and follows guidance provided by AMSTAR (Shea et al., 2007).
Pharmacologic Treatments
Study Random sequence
generation (selection
bias)
Allocation
concealment
(selection bias)
Blinding of participants
and personnel
(performance bias)
Blinding of outcome
assessment (detection
bias)
Incomplete outcome data
addressed (attrition bias)
Selective reporting
(reporting bias)
Altamura et al. 2003
Not described Not described Placebo was used to blind the participants; no description of blinding of personnel
Not described 22/74 dropped out during treatment with levosulpiride; 12/74 dropped out during treatment with placebo.
Results after 4 weeks are described but not after 8 weeks.
Unclear risk Unclear risk Unclear risk Unclear risk High risk High risk
Donta et al 2004
"Randomization was performed seperately for each site by using varying block sizes. The site coordinator randomly assigned participants by calling into a central, automated telephone randomization system"
"A treatment kit was randomly assigned. The kit number corresponded to a treatment kit located in the facility's pharmacy."
"…those assigned to the placebo group received identically matched lactose capsules."
"double-blind" 49/238 in the treatment group and 43/243 in the placebo group who completed baseline assessment did not complete the 12 month assessment, most voluntarily withdrew, reasons were similar between the groups.
Low risk Low risk Low risk Low risk Low risk Unclear risk
Garcia-Campayo et al 2002
Open trial- no randomization
Pre-post design, no control group and no allocation
Open trial, no blinding Open trial, no blinding 6 months: 8/35 patients dropped due to side effects or patient perceived lack of efficacy
1 The Cochrane Collaboration. 2011. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. Available at: http://www.cochrane-handbook.org/

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 17
Study Random sequence
generation (selection
bias)
Allocation
concealment
(selection bias)
Blinding of participants
and personnel
(performance bias)
Blinding of outcome
assessment (detection
bias)
Incomplete outcome data
addressed (attrition bias)
Selective reporting
(reporting bias)
High risk High risk High risk High risk High risk Unclear risk
Han et al 2008 (#1699)
"computer generated randomization code"
Not described "open-label" "open-label" 12 weeks: 11/50 mirtazapine and 13/45 venlafaxine patients dropped out. Reasons for drop out are not clear. LOCF population of 77/95 originally enrolled.
Low risk Unclear risk High risk High risk High risk Unclear risk
Han et al 2008 (#744)
Open trial- no randomization
Pre-post design, no control group and no allocation
Open trial, no blinding Open trial, no blinding 8 weeks: 2/22 patients were lost to follow-up.
High risk High risk High risk High risk Low risk Unclear risk
Kroenke et al 2006
"This was a randomized, double-blind, placebo controlled study…" and "…followed by randomization to treatment…"
Not described "placebo controlled study." Number of capsule of placebo matched number of capsule of treatment drug.
“double-blind”. 12 weeks: 18/55 missing from treatment group, 4 due to adverse events and 4 due to protocol violation; 20/57 missing from the control group, 10 due to unsatisfactory response. Withdrawals not significantly different.
Unclear risk Unclear risk Low risk Low risk High risk Unclear risk
Menza et al 2001
Open trial- no randomization
Pre-post design, no control group and no allocation
Open trial, no blinding Open trial, no blinding 8 weeks: 1/22 patients dropped out due to adverse events.
High risk High risk High risk High risk Low risk Unclear risk
Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 18
Study Random sequence
generation (selection
bias)
Allocation
concealment
(selection bias)
Blinding of participants
and personnel
(performance bias)
Blinding of outcome
assessment (detection
bias)
Incomplete outcome data
addressed (attrition bias)
Selective reporting
(reporting bias)
Muller et al 2008
"patients were randomly assigned (via computer-generated randomized lists) to one of two double-blind treatments."
Not described "The escitalopram and placebo medication were identical in appearance, ensuring that both clinicians and patients were blind to medication status."
Self-reported by participants, and clinician reported outcomes
12 weeks: 1/25 patients in the treatment group withdrew due to adverse events, all 26 patients in the placebo group completed the study.
Low risk Unclear risk Low risk Low risk Low risk Unclear risk
Volz et al. 2000
"randomized" No description of how randomization was done, mentioned in the abstract but not described in the methods
Not described "double blind treatment phase" Comment: placebo was used in identical capsules
Patient reported outcomes collected in semi-structured interviews
6/99 in the opipramol group and 6/101 in the placebo group withdrew due to adverse events. Used an intent to treat analysis.
Unclear risk Unclear risk Low risk Low risk Low risk Unclear risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 19
Other Biologic Treatments
Study Random sequence
generation (selection
bias)
Allocation
concealment (selection
bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment (detection
bias)
Incomplete outcome
data addressed
(attrition bias)
Selective reporting
(reporting bias)
Fontani et al 2011
"…computerized randomization by an outside operator.'
”external operation” "Group B subjects received placebo treatment, ie, inactive REAC, in a specific room…"
"single-blind" and "…we used an electronic version [of the PSM questionnaire] to collect and process data, and to analyze the results." Comment: no discussion about investigator involvement
Not described The descriptions provided do not allow for a thorough assessment of the study
Low risk Low risk Low risk Low risk Unclear risk Unclear risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 20
Cognitive Behavioral Interventions
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
Allen et al 2006
“…using a computer-generated random number sequence.”
Not described No participant blinding due to nature of the treatment- CBT Results not likely influenced by performance bias- Patient’s expectation of improvement were assessed- the treatment and control groups did not differ significantly in their expectations of improvement.
“Study personnel conducting assessments were masked as to the participants treatment condition…” “To assess the success of blinding and index was 0.85 (95% CI 0.78-0.92) indicating a high level of blindedness.”
15 months: 8/43 missing from intervention group (all 8 withdrew from the study); 4/41 missing from control group (all 4 withdrew from the study). Difference in attrition rates not significantly different between groups.
Low risk Unclear risk Low risk Low risk N/A Low risk Unclear risk
Arnold et al 2009
"Randomization of practices was not considered feasible because of the number of practices needed. The family physicians had no influence on selection of their patients since the family-physician-researcher (IAA) contacted their patients if they met the inclusion criteria."
"Names of the participants were not revealed to the control family-physicians."
"All eligible participants… were only informed about their allocation after they had signed the informed consent form." The family physicians administering the treatment had to be trained to deliver the treatment and supervised by a qualified cognitive-behavioral therapist.
None Health care utilization and prescription medication info from electronic medical records provided by the participating physicians. Participants reported mental health treatment or assessment.
12 Months: final outcome assessment available for all participants. 100% included in both samples for dta analysis ITT employed.

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 21
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
High risk High risk High risk High risk Unclear risk Low risk Unclear risk
Bleichhardt et al. 2004/Rief et al. 2002
Waiting list not randomized-"waiting controls selected during the first year by screening "randomly" no description of how.
"randomly" no description of how
Not described No information on blinding of interviewers
1 year follow-up: 34/191 did not complete the last follow-up. Checked for differences with dropout--none found, no impact on results.
Solid battery of all expected measures. (SCL-90, Depression, Anxiety, QOL, and life satisfaction)
High risk Unclear Risk Unclear risk High risk Low risk Low Risk
Donta et al 2003 Mori et al. 2006
"Randomization was centrally performed by the coordinating center after verification of eligibility criteria" "…to 1 of 4 treatment arms using a permuted block design with a block size of 8"
"Treatment assignment was unmasked"
No blinding All outcomes were self-reported. "Treatment assignment was unmasked except for a masked assessor of study outcomes at each site" "Research assistants who were masked to treatment assignment administered all primary and secondary outcome assessments."
12 months: 25/266 CBT+Exercise; 24/265 Exercise; 25/286 CBT; and 15/270 Usual care patients completed the study. 44 refused follow-up, 3 died, 1 was released for safety reasons. No differences between groups noted. Used an intent-to-treat approach.
Low risk Low risk High risk High risk N/A Low risk Unclear risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 22
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
Escobar et al. 2007
"Patients were assigned to the intervention or control group using a computer-generated random number sequence generated by the study statistician before the study."
Not described "Study personnel conducting assessments were blinded to the participants’ study group…" Blinding of participants was not described.
"The blind was considered as possible broken for a total of 17 patients, 12 of 87 (13.8%) in the intervention group and 5 of 85 (5.9%) in the control group. Eliminating these patients from the analyses did not change the significant benefits of the intervention described above." "Study personnel conducting assessments were blinded to the participants’ study group…"
6 month follow-up: 36/87 treatment and 41/85 control participants did not complete the last assessment. No differential drop 58% versus 51%. ITT approach utilized.
Low risk Unclear risk High risk Low risk N/A Low risk Unclear risk
Lidbeck 2003 Lidbeck 1997
"Randomization was carried out independently by a nurse who was not participating in the study,"
Not described Not described Not described Only one dropout, all included in the analysis
Methods described in more detail in Lidbeck 1997
Low risk Unclear risk Unclear risk Unclear risk N/A Low risk Low risk
Martin et al. 2007
"Randomization was based on a predefined list of
"Study assistants enrolled and
Not blinded Not described 6-month follow-up: 11/70 in the treatment group and 11/70 in the

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 23
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
binary variables, using blocking procedures to ensure comparable sample sizes."
assigned participants to the groups according to the randomization list."
control group did not complete the study. Intent to treat analysis conducted.
Low risk Low risk High risk Unclear risk N/A Low risk Unclear risk
Sharpe et al. 2011
"...randomly assigned in a 1:1 ratio to either the usual care alone or usual care plus GSH. The randomization sequence was computer-generated... "
"Trial doctors obtained the treatment allocation after providing each patient's data to a remote telephone-based randomization system."
"Participants could not be masked to treatment allocation."
Outcomes were self-reported by participants who were not blinded. "…questionnaire data were obtained by dictation to a research assistant who was blind to treatment allocation."
3 month follow-up: 59/64 treatment and 63/63 control participants completed the last assessment. Intent-to-treat approach was used.
Low risk Low risk High risk High risk N/A Low risk Unclear risk
Sumathipala et al. 2000
"The patients were allocated to the intervention and non-intervention groups by simple randomization... by random numbers generated from a calculator."
"These were available in 68 sealed opaque envelops bearing sequential registration numbers on the outside of the envelope."
"The participant was registered at the time of enrolment into the study, but the corresponding sealed envelope was not opened until the end of the baseline assessment." "The non-clinical research assistant and the second psychiatrist remained blind to the group status throughout
Not blinded.. "A random sample was co-rated by the second psychiatrist (blinded) during their follow-up assessment. The non-clinical research assistant (blinded) administered BSI and case vignettes for SEMI." Patient not blinded
3 month follow-up: 10/34 treatment and 13/34 control patients did not complete the last assessment. An intent-to-treat approach was used.

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 24
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
the study."
Low risk Low risk High risk Unclear N/A Unclear risk Unclear risk
Sumathipala et al. 2008
"The doctors were allocated at random to deliver CBT or structured care" "Trial participants were first randomised to the two intervention groups using a random permuted block design... Randomisation codes were generated by a statistician in the UK and passed on to the independent epidemiologist..."
"...the independent epidemiologist (M.R.N.A.) in Sri Lanka, who executed the random allocation of treatment condition."
"...the physician (PI) and the research assistants for the project remained masked to the group status of the patients. Details of allocation of all patients were concealed from them until the end of the trial. The research assistants did not know which primary care doctors provided which treatment." "Neither the primary care doctors who delivered the interventions nor the patients who received them could be masked to their allocation because of the nature of the interventions."
Outcomes were reported by participants (not blinded) "Throughout the study both the physician and research assistants remained masked to the group status of the participants.
12 month follow-up: 15/75 treatment and 22/75 control participants were lost to follow-up or violated the study protocol. Mixed effects models used to handle missing data; sensitivity analyses showed no impact of missing data on results.
Low risk Low risk Unclear risk Unclear risk N/A Low risk Unclear risk
Zaby et al. 2008
"randomized assignment to one of the two groups…based on drawing lots."
Not described Not described Not described; All measures written self-report instruments. No interview or document measures
8 weeks: 2/77 dropped out, no difference between groups. All analysis intent to treat
Good battery of measures reported -- all reported.

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 25
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
"All patients for whom the period of time until the start for the respective group treatment was greater than 4 weeks and less than three months were assigned to a waiting group.”
Low risk Unclear risk Unclear Risk High risk N/A Low risk Low risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 26
Psychodynamic Psychotherapies
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of
outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete
outcome data
addressed
(attrition bias)
Selective
reporting
(reporting bias)
Abbass et al. 2009 (#1103)
None None None None Number of ED visit was abstracted from hospital databases
Not fully described- 20/50 patients only attended 1 session. Sensitivity analysis conducted on outcome p. 532; reported analyses for those who completed two or more sessions (n = 26). More than half sample missing for analyses
Only one self report measure reported. Seems unlikely that more measures weren't included.
High risk High risk High risk High risk Low risk High risk Unclear risk
Aiarzaguena et al 2002
High risk High risk High risk High risk High risk Low risk High risk
Posse 2004 Patients were randomly assigned to treatment or control groups
None None None None Not described
Low risk High risk High risk High risk High risk Unclear risk Unclear risk
Rembold 2011 Not described. Most likely not randomized, "another 20 patients served as the control
Not described Not described Not described; self report and primary care physician report measures. Primary care physician not
Not described; Dropout not reported. No discussion of handling of missing data
"Abundance of results allows only a selective presentation of individual selected data here." No

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 27
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of
outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete
outcome data
addressed
(attrition bias)
Selective
reporting
(reporting bias)
group." blinded. standard statistical analyses.
High risk Unclear risk Unclear risk High risk N/A High risk High risk
Reuber et al. 2007
None None None All outcomes self-report measures.
post-treatment: 28/91 patients did not finish the treatment. Both ITT and completer analyses reported. No difference between dropout and not. 6-month follow-up: 57/91 patients did not complete the 6-month post-treatment follow-up. Intent to treat analysis used for 91 patients.
High risk High risk High risk High risk N/A Low risk Unclear risk
Sattel et al. 2012
"A computer program generated a blocked randomisation list and the Coordination Centre for Clinical Trials covertly applied this list
"The therapist disclosed the groups assignment to the patient and began treatment." This is after they were entered in the trial. On their consort, all who were given informed consent went into the trial and
"...neither the study personnel nor the patients had been masked to randomisation, and recommendations regarding future therapeutic procedures had been a part of the
"As the outcome assessment consisted of self-report measures, masking procedures were not applicable." all self-report measures.
Health care utilization appears to be self-report but not clear.
9 months post treatment: 11/107 treatment group patients and 16/104 control group patients did not complete the last assessment. Intent to treat analysis

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 28
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of
outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete
outcome data
addressed
(attrition bias)
Selective
reporting
(reporting bias)
to the sample." randomization happened after informed consent so unlikely selection bias
protocol." Study tested whether or not unhappy with assignment and found no effect on outcome.
Low risk Unclear risk Unclear risk High risk Unclear risk Low risk Unclear risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 29
Biofeedback Risk of Bias
Study Random
sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of
outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete
outcome data
addressed
(attrition bias)
Selective
reporting
(reporting bias)
Katsamanis et al. 2011
"Participants were randomly assigned to PCI or PT+PCI using a computer-generated random number sequence."
Not described Not described Not described "Study personnel conducting assessments were masked to participants’ treatment condition…"
Duration unknown: 10 participants dropped out of the study for various reasons (e.g. relocation and medical issues difficulty). An intent-to-treat approach was used.
Scores are presented but significance of changes and comparisons to other groups (except for HAM-A) are not discussed
Low risk Unclear risk Unclear risk Unclear risk Low risk Unclear risk High risk
Nanke et al. 2003 "…randomly assigned…"
Not described No blinding No blinding No blinding Not described
Unclear risk Unclear risk High risk High risk High risk Unclear risk Unclear risk
Saldanha et al. 2007
Not described Not described Not described Not described Not described 1 year: Drugs- 2/30; Biofeedback- 7/30; Drugs/biofeedback- 3/30 withdrew. No reasons listed. No corrective methods were indicated
Incomplete reporting.
Unclear risk Unclear risk Unclear risk Unclear risk Unclear risk Unclear risk High risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 30
Cognitive Rehabilitation Therapy Risk of Bias
Study Random
sequence
generation
(selection
bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance bias)
Blinding of outcome
assessment (detection
bias) (patient-
reported outcomes)
Blinding of outcome
assessment (detection
bias) (documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective reporting
(reporting bias)
Jacksy 2002
Not randomized
Not described Not described Not described Not described 6-weeks: 3/10 treatment and 3/10 controls did not complete the study. No method of adjusting for missing data was described.
High risk High risk High risk High risk High risk High risk Unclear risk

Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 31
Complementary and Alternative Therapies Risk of Bias
Study Random sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of
outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete
outcome data
addressed
(attrition bias)
Selective
reporting
(reporting
bias)
Muller et al. 2004
"Computer-aided randomization and preparation of a coding list was performed in blocks of 6 by the independent Quality Assurance Unit of the sponsor."
"Blistered study medication and medication containers were labeled sequentially according to the coding list by the manufacturing department of the sponsor and provided to the investigators in blocks of six."
"All investigators, personnel of contracted partners and of the sponsor who were actively involved in the trial were blinded to group assignment until lock of database at the end of the trial."
"double blind" "All investigators, personnel of contracted partners and of the sponsor who were actively involved in the trial were blinded to group assignment until lock of database at the end of the trial."
6 weeks: 11/175 participants did not complete the study or had major protocol violations. The authors used an intent-to-treat approach.
Low risk Low risk Low risk Low risk Low risk Low risk Unclear risk
Nickel et al. 2006
"…using randomized numbers generated by an Excel table."
"clinic administration conducted randomization confidentially.""
No blinding No blinding No blinding 6 weeks: 9/64 drop outs- no discussion of why, what treatment groups they were in or how the analysis accounted for them.
Low risk Low risk High risk High risk High risk High risk Unclear risk
Payne et al. 2010 Payne 2009
Not randomized No allocation concealment
No blinding No blinding No blinding 18/31 completed the treatment, only those 18 were included in the analysis.
unclear description of the intervention
High risk High risk High risk High risk High risk High risk High risk
Gulf War and Health: Treatment for Chronic Multisymptom Illness Page 32
Study Random sequence
generation
(selection bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of
outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of
outcome
assessment
(detection bias)
(documented
outcomes)
Incomplete
outcome data
addressed
(attrition bias)
Selective
reporting
(reporting
bias)
Paterson et al. 2011 Rugg et al. 2011
" Simple randomisation was used for the first 20 patients, and then minimisation (with a random component of 80%) was applied to ensure balance across the three variables..."
"Group allocation was known by trial researchers, practitioners, and patients, but the statistician who carried out data analysis was blinded."
"Group allocation was known by trial researchers, practitioners, and patients…"
"Group allocation was known by trial ... Patients"
"Group allocation was known by trial researchers, practitioners, and patients…"
52 weeks: 15/39 from the treatment group and 17/41 from the control group did not complete the follow-up assessment. An intention-to-treat analysis was performed.
Low risk Low risk High risk High risk High risk Low risk Unclear risk
Volz et al. 2002
"Randomized" "double blind" "double blind" "double blind" Not described 6 weeks: 2/149 in the placebo group did not complete the study due ot adverse events. intent-to-treat approach.
details of methodology missing
Unclear risk Unclear risk Unclear risk Unclear risk Unclear risk Low risk Unclear risk
Yamada et al. 2005
Not randomized Not randomized Not randomized Not randomized Not randomized 3 months: Unclear but 20 patients did not continue the trial due to the inability to go to the hospital.
Letter to the Editor- description of method and results are brief.
High risk High risk High risk High risk High risk High risk High risk

Exercise Intervention Risk of Bias
Study Random sequence
generation (selection
bias)
Allocation
concealment
(selection bias)
Blinding of
participants and
personnel
(performance
bias)
Blinding of outcome
assessment
(detection bias)
(patient-reported
outcomes)
Blinding of outcome
assessment (detection
bias) (documented
outcomes)
Incomplete outcome
data addressed
(attrition bias)
Selective
reporting
(reporting
bias)
Donta et al 2003 Mori et al. 2006
"Randomization was centrally performed by the coordinating center after verification of eligibility criteria" "…to 1 of 4 treatment arms using a permuted block design with a block size of 8"
"Treatment assignment was unmasked"
"Treatment assignment was unmasked"
"Treatment assignment was unmasked except for a masked assessor of study outcomes at each site"
"Research assistants who were masked to treatment assignment administered all primary and secondary outcome assessments."
12 months: 25/266 CBT+Exercise; 24/265 Exercise; 25/286 CBT; and 15/270 Usual care patients completed the study. 44- Refused follow-up, 3 died, 1 was released for safety reasons. No differences between groups noted. Used modified intent-to-treat analysis.
Low risk Low risk High risk High risk Low risk Low risk Unclear risk
Peters et al. 2002
"Consecutive patients were randomly allocated to either an aerobic exercise or stretching programme" Method of randomization not indicated.
Not described "It was not feasible to blind therapists or research assistants to randomization. However, throughout the study, patients remained blind to the hypothesis and the content of the alternative exercise programme."
"...patients remained blind to the hypothesis and the content of the alternative exercise programme."
"It was not feasible to blind therapists or research assistants to randomization."
Number of participants to drop out after starting the treatment was not provided. An intention-to-treat model was used.
Unclear risk Unclear risk High risk Low risk High risk Unclear risk Unclear risk

Gulf War and Health: Treatment of Chronic Multisymptom Illness Page 34
Systematic Reviews
The following AMSTAR items were used to evaluate the methodological quality of systematic reviews (Shea et al. 2007). A table of systematic reviews meeting the committees criteria assessed by these items follows.
1. Was an ‘a priori’ design provided? The research question and inclusion criteria should be established before the conduct of the review.
2. Was there duplicate study selection and data extraction? There should be at least two independent data extractors and a consensus procedure for disagreements should be in place.
3. Was a comprehensive literature search performed? At least two electronic sources should be searched. The report must include years and databases used (e.g. Central, EMBASE, and MEDLINE). Key words and/or MESH terms must be stated and where feasible the search strategy should be provided. All searches should be supplemented by consulting current contents, reviews, textbooks, specialized registers, or experts in the particular field of study, and by reviewing the references in the studies found.
4. Was the status of publication (i.e. grey literature) used as an inclusion criterion? The authors should state that they searched for reports regardless of their publication type. The authors should state whether or not they excluded any reports (from the systematic review), based on their publication status, language etc.
5. Was a list of studies (included and excluded) provided? A list of included and excluded studies should be provided.
6. Were the characteristics of the included studies provided? In an aggregated form such as a table, data from the original studies should be provided on the participants, interventions and outcomes. The ranges of characteristics in all the studies analyzed e.g. age, race, sex, relevant socioeconomic data, disease status, duration, severity, or other diseases should be reported.
7. Was the scientific quality of the included studies assessed and documented? ‘A priori’ methods of assessment should be provided (e.g., for effectiveness studies if the author(s) chose to include only randomized, double-blind, placebo controlled studies, or allocation concealment as inclusion criteria); for other types of studies alternative items will be relevant.
8. Was the scientific quality of the included studies used appropriately in formulating conclusions?
The results of the methodological rigor and scientific quality should be considered in the analysis and the conclusions of the review, and explicitly stated in formulating recommendations.
9. Were the methods used to combine the findings of studies appropriate? For the pooled results, a test should be done to ensure the studies were combinable, to assess their homogeneity (i.e. Chi-squared test for homogeneity, I²). If heterogeneity exists a random effects model should be used and/or the clinical appropriateness of combining should be taken into consideration (i.e. is it sensible to combine?).
10. Was the likelihood of publication bias assessed? An assessment of publication bias should include a combination of graphical aids (e.g., funnel plot, other available tests) and/or statistical tests (e.g., Egger regression test).

Gulf War and Health: Treatment of Chronic Multisymptom Illness Page 35
11. Was the conflict of interest stated? Potential sources of support should be clearly acknowledged in both the systematic review and the included studies.
AMSTAR Items
Study 1 2 3 4 5 6 7 8 9 10 11
Abbass et al. 2009 (#85)
Yes Yes/No (Did not discuss procedure for handling disagreements)
Yes No No Yes Yes Yes Yes Yes No
Allen et al. 2002
Yes Can't answer Yes No No Yes No No Yes No Yes
Kleinstauber et al. 2011
Yes No Yes Yes No Yes Yes Yes Yes Yes No
Kroenke 2000
Yes Cannot answer (Did not discuss procedure for handling disagreements)
No (Only Medline, bibliographies, reviews, and monographs)
Cannot Answer
No (Only included studies)
Yes No Yes No No No
Kroenke 2007
Yes Can't answer No (Only medline and references)
Can't answer No Yes No Yes Yes No No
Looper 2002 No Cannot answer (Not described)
Yes Cannot Answer
No (Only included studies)
Yes (Not for all studies)
Yes Yes Yes No No
Nezu et al. 2001
Yes Cannot answer (Not described)
Yes (decade range)
Yes No (Only included studies)
Yes Yes Yes Yes No No
Sumathipala 2007
Yes Yes Yes Can't answer No Yes No Yes Yes No No
van Rood and Roos, 2009
Yes Yes (study selection), No (data extraction)
Yes No No Yes No No Can't answer
No No

Gulf War and Health: Treatment of Chronic Multisymptom Illness Page 36


















