

Overview of the Merit Based Incentive Payment System
33
An Overview of MACRA Quality Payment Programs PART 1: The Merit Based Incentive Payment System
-
Upload
groupone-health-source-inc -
Category
Healthcare
-
view
69 -
download
3
Transcript of Overview of the Merit Based Incentive Payment System

An Overview of MACRA Quality Payment Programs
PART 1: The Merit Based Incentive Payment System

AGENDAThe Quality Payment ProgramMIPS Categories OverviewFinancial Impact

April 18, 2015- President Obama signed the Medicare Access and Children’s Health Insurance
Program Reauthorization Act (MACRA)

Replaces the Sustainable Growth Rate
Adjusts payments based on individual performance
Switches Medicare Part B payments from fee-for-service to fee-for-value
QUALITY PAYMENT PROGRAM
APMsMIPS


WHAT IS MIPS?
New program that combines PQRS, VBM, and Meaningful Use
Adds a fourth component to promote ongoing improvement and innovation to clinical activities
QUALITYACICOST CPIA
MIPS allows Medicare clinicians to be paid for providing high quality, efficient care through success in four performance categories:

What is MIPS?
Quality25%
50%15%
10%
ACI
CPIA
Cost
These 4 categories all contribute to a MIPS Composite Performance Score or CPS of up to 100 points
Certain circumstances may require a category to be 0% of the MIPS CPS
Clinicians choose to be rated on either an individual-clinician basis or as a group of clinicians (Identified by Tax ID number)
Relative weights of Quality & Cost categories will change

QUALITY
Clinicians would choose to report six measures instead of the nine measures currently required under PQRS
There are multiple reporting options to choose from in order to accommodate differences in specialty and practices
Quality would be worth 50% of the total score in year 1
Replaces PQRS and the quality component of the value modifier program
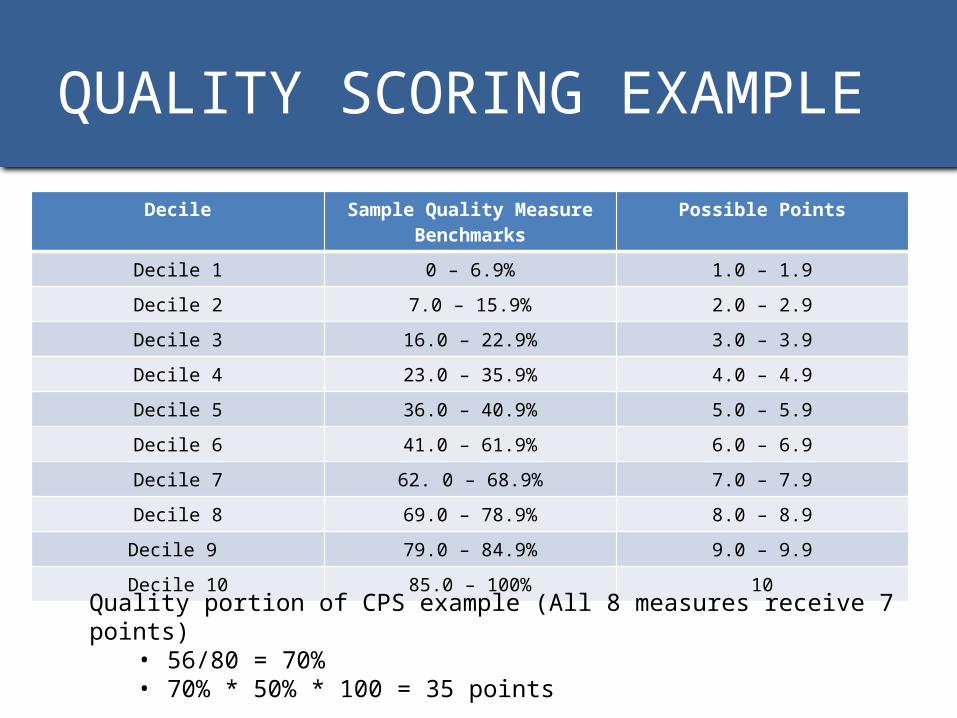
QUALITY SCORING EXAMPLEDecile Sample Quality Measure
BenchmarksPossible Points
Decile 1 0 – 6.9% 1.0 – 1.9Decile 2 7.0 – 15.9% 2.0 – 2.9Decile 3 16.0 – 22.9% 3.0 – 3.9Decile 4 23.0 – 35.9% 4.0 – 4.9Decile 5 36.0 – 40.9% 5.0 – 5.9Decile 6 41.0 – 61.9% 6.0 – 6.9Decile 7 62. 0 – 68.9% 7.0 – 7.9Decile 8 69.0 – 78.9% 8.0 – 8.9Decile 9 79.0 – 84.9% 9.0 – 9.9Decile 10 85.0 – 100% 10
Quality portion of CPS example (All 8 measures receive 7 points)• 56/80 = 70%• 70% * 50% * 100 = 35 points

COST/RESOURCE USE
The score would be based on Medicare claims (PQRS reporting), which means no additional reporting requirements for this program
This category will use more than 40 episode-specific measures to account for differences among specialties
Cost would be worth 10% of the total score in year 1
Replaces the cost component of the Value Modifier Program

COST/RESOURCE USE
Each measure can earn up to 10 points 20 points possible
Cost portion of CPS example (each measure receives 8 points) 16/20 = 80%
80% * 10% * 100 = 8 points
SCORING EXAMPLE

ADVANCING CARE INFORMATION
Clinicians would choose to report customizable measures
Unlike the existing Meaningful Use program, this category would not require all-or-nothing EHR measurement or quarterly reporting
ACI would be worth 25 percent of the total score in year 1
Replaces Meaningful Use

ADVANCING CARE INFORMATION
There is a total of 131 points available for this category Base score
• Protect Patient Health Information (“Yes” required)• Public Health and Clinical Data Registry Reporting (“Yes” required)• Electronic Prescribing (Numerator/Denominator)• Patient Electronic Access (Numerator/Denominator)• Coordination of Care Through Patient Engagement (Numerator/Denominator)• Health Information Exchange (Numerator/Denominator)
Performance score• Patient Electronic Access• Coordination of Care Through Patient Engagement• Health Information Exchange
Bonus point• Immunization required• Additional point for reporting beyond immunization category
POINTS DESCRIPTION

ADVANCING CARE INFORMATION
SCORING EXAMPLE
ACI portion of CPS example (only receives base score of 50 points)
50/100 = 50%
50% * 25% * 100 = 12.5 points contributed by the ACI category
CPIA
Clinicians would be rewarded for clinical practice improvement activities such as activities focused on care coordination, beneficiary engagement, and patient safety
Clinicians may select activities that match their practices’ goals from a list of more than 90 options
Additionally, clinicians would receive credit in this category for participating in Alternative Payment Models and in Patient-Centered Medical Homes
CPIA would be worth 15 percent of total score in year 1

CPIA
There are 60 possible points and 4 possible ways to get those points:• Any combination of “high” and/or “medium” activities• Special rules for non-patient facing, small practices (15 or fewer), rural
practice areas, or practices in a HPSA All activities are worth 30 points• APM participation automatically earn 30 points • Participation in certain medical home models automatically earns the
full 60 points
CPIA portion of CPS example (one “high” weight activity and two “medium” weight activities)• 40/60 = 67.7%• 67.7% * 15% * 100 = 10 CPS points contributed from the CPIA category
SCORING EXAMPLE

CALCULATING TOTAL CPS
Quality (56 of 80 points) * 50% weight * 100 = 35 points
Cost (16 of 20 points) * 10% weight * 100 = 8 points
ACI (50 of 100 points) * 25% weight * 100 = 12.5 points
CPIA (40 of 60 points) * 15% weight * 100 = 10 points
Total CPS score of 35 + 8 + 12.5 + 10 = 65.5 CPS Score out of a possible 100

PERFORMANCE THRESHOLD
• Each year CMS will calculate Composite Performance Scores (CPS)• Scores renewed annually• A clinician’s CPS will be compared to the Performance Threshold
CPS = 50CPS = 70 CPS = 20 CPS = 85
50+70+20+85 = 225225/4=56.25PT=56.25
12 3 4
-- + +The amount which they are above or below the PT will determine the size of the incentive payment or penalty.

PERFORMANCE/PAYMENT YEARS
2017 2019
Performance year is the year the providers’ performance is judged Payment year will occur two years later & is based on the
performance year data The 2016 performance year and 2018 payment year will be the final
separate payment adjustments for the programs individually
First Payment Year
First Performance Year

WHO IS ELIGIBLE?Years 3+Years 1 & 2
Physical and occupational therapists, speech-language pathologists, audiologists, nurse midwives, clinical social workers, clinical psychologists, & dietitians or nutrition professionals
Physicians, physician assistants, nurse practitioners, clinical nurse specialists, & nurse anesthetists
20192017 & 2018

WHO IS EXCLUDED?Advanced APM
Low Volume
1st Time Medicare Enrollees
Providers participating in an Advanced Alternative Payment Model.
CMS has defined a low volume threshold that is described as Medicare billing charges less than or equal to $10,000 and providing care to 100 or fewer Medicare patients in one year
Providers who enroll in Medicare for the first time during a performance year are exempt from MIPS until the subsequent year.

DATA SUBMISSIONQuality and Resource Use
Individual Reporting Group Reporting QCDR Qualified Registry EHR Administrative Claims (No
submission required) Claims
Administrative Claims (No submission required)
Administrative Claims (No submission required)
QCDR Qualified Registry EHR Administrative Claims (No
submission required) CMS Web Interface (Groups of 25 or more) CAHPS for MIPS Survey
Quality
Resource Use

DATA SUBMISSIONAdvancing Care Information and CPIA
Individual Reporting Group Reporting
Attestation QCDR Qualified Registry EHR Vendor
Attestation QCDR Qualified Registry EHR Vendor Administrative Claims (No
submission required)
Attestation QCDR Qualified Registry EHR Vendor CMS Web Interface (Groups of 25 or more)
Attestation QCDR Qualified Registry EHR Vendor CMS Web Interface (Groups of 25 or more)
ACI
CPIA

FINANCIAL IMPACT

MIPS “BASE” PAYMENT ADJUSTMENT
2017 2018 2019 2020 2021 2022 +/-4%
+/-5%
+/-7%
+/-9%
The performance year will be the year in which providers’ performance is judged. The payment year will occur two years later and is based on the performance year data.
2017 = First performance year2019 = First payment year

BUDGET NEUTRALITY
• Incentive money paid to those with high MIPS scores will be funded
by the penalties applied to those with low MIPS scores
• The amount of this available revenue (penalties) determines the actual bonus reimbursement rate each year

BUDGET NEUTRALITY EXAMPLE
For example:If only relatively few clinicians attain high MIPS scores – and conversely, a great deal of clinicians attain low MIPS scores – the incentives available to the high performers could be increased by a factor of up to 3, which in 2019 could result in a maximum of 12 percent increase in reimbursements. Potential for3x
4%
12%
In 2022, high MIPS scores could be rewarded with a maximum 27% increase in reimbursement.
adjustment

BASE & BUDGET NEUTRALITY ILLUSTRATION

BONUS CMS has also ensured that all providers who score
above the MIPS performance threshold will receive a reimbursement bonus, even if there are no low-performers in a given year
A special “Additional Incentive Payment” account has been created by CMS and will be funded with $500 Million each year from 2019 to 2024
If there are an adequate number of low performers, this “Additional Incentive Payment” will go to the exceptional performers

EXCEPTIONAL BONUS
$500M available each year from 2019 – 2024 for this pool

PUTTING IT ALL TOGETHER

TAKE AWAY POINTS
1. MIPS allows Medicare clinicians to be paid for providing high quality, efficient care through success in four performance categories
2. MIPS replaces PQRS, Meaningful Use, and the value based modifier programs.
3. Medicare Part B clinicians will participate in the MIPS, unless they are in their 1st year of Part B participation, become QPs through participation in Advanced APMs, or have a low volume of patients.
4. 2017 is the first performance year with payment adjustments and bonuses starting in 2019.


















