Overview of the Human Resources for Health Crisis in Developing · PDF file ·...
60
Overview of the Human Overview of the Human Resources for Health Crisis in Resources for Health Crisis in Developing Countries Developing Countries Way out of the crisis, implications for Way out of the crisis, implications for Nigeria Nigeria 31 October 2011 31 October 2011 First National Conference on HRH , Abuja First National Conference on HRH , Abuja Dr George W. Pariyo ( Dr George W. Pariyo ( MBChB MBChB , MSc, PhD) , MSc, PhD) Medical Officer, Country Facilitation Team Medical Officer, Country Facilitation Team Global Health Workforce Alliance Secretariat Global Health Workforce Alliance Secretariat
Transcript of Overview of the Human Resources for Health Crisis in Developing · PDF file ·...
Overview of the Human Overview of the Human
Resources for Health Crisis in Resources for Health Crisis in
Developing CountriesDeveloping CountriesWay out of the crisis, implications for Way out of the crisis, implications for
NigeriaNigeria31 October 201131 October 2011
First National Conference on HRH , AbujaFirst National Conference on HRH , Abuja
Dr George W. Pariyo (Dr George W. Pariyo (MBChBMBChB, MSc, PhD), MSc, PhD)
Medical Officer, Country Facilitation TeamMedical Officer, Country Facilitation Team
Global Health Workforce Alliance SecretariatGlobal Health Workforce Alliance Secretariat
Outline of the presentation
Overview of human resources for health global crisis
Part 1
Global Health Workforce AlliancePart 2
Country actions – a way out of the crisis
Part 3

Human Resources for Health:Shortages, Inequitable Distribution
A global crisis!
Part 1

In Sub-Saharan Africa…� 24% of global burden of disease but only 3% of
world's health workers
� 1 of 4 doctors and 1 of 20 nurses trained in Africa are working in developed countries.
Global health workforce crisis
Globally…� Shortfall of 4.3 million health workers globally
� Education and training insufficient
� Monthly wages: < $100 in some countries vs> $14 000 in other countries
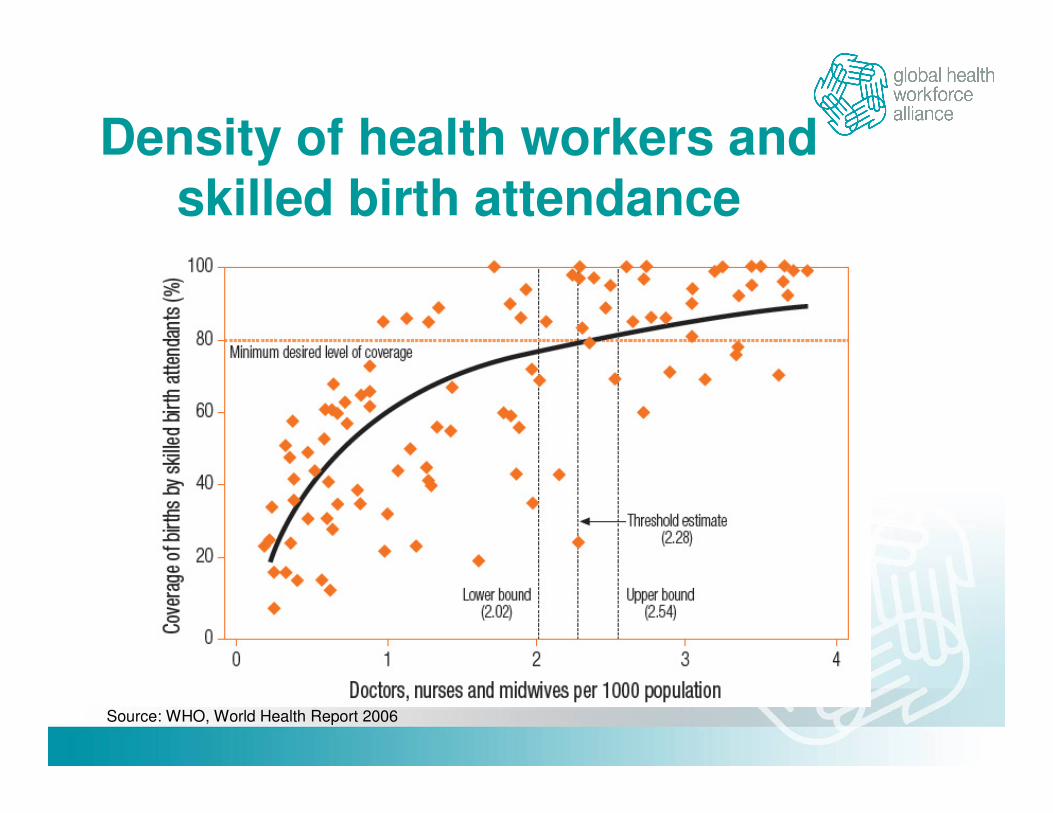
Density of health workers and skilled birth attendance
Source: WHO, World Health Report 2006

Countries with a critical HRH shortage Countries with a critical HRH shortage (< 2.3 nurses, midwives and doctors per 1,000 population)(< 2.3 nurses, midwives and doctors per 1,000 population)
[Source] WHO. (2006). World Health Report 2006. WHO: Geneva.

Uneven global distribution: nurses
Source: www.worldmapper.org and WHO Global Atlas Health WorkforceLegenda: the size of the countries is proportional to density of nurses

Uneven distribution of health workers within countries …
Source: WHO Global Atlas of the Health Workforce, 2009 update.
26 selected Countdown countries with urban/ rural distribution data available.

Africa has greatest burden of disease, least health workforce!

Countries with a critical HRH shortage
Of 57 HRH crisis countries, 39 (68%) are in Africa.
36 (63%) are in SSA
[Source] WHO. (2006). World Health Report 2006. WHO: Geneva.

19
29 30
45
62
131
142
0
20
40
60
80
100
120
140
160
Africa South-East Asia Eastern Mediterranean Western Pacific World Europe Americas
Health Service Providers (per 10,000 population) by WHO Region, 2005
Note:1. Data as reported by countries (compiled at WHO Regional offices and the Headquarter)
2. Reference year of data for some countries may differ from the reported year 2005
3. Health service providers include : (i) Physicians (ii) Nurses (iii) Midwives (iv) Dentists (v) Phramacists (vi) Environmental and public health personnel
(vii) Lab workers (viii) Community health workers (ix) other health workers
Number per 10,000 population
Global situation of health workforce
Source: WHO SEARO

Health workforce crisis in Africa
In Africa, there are, on average, only 1.08 doctors, In Africa, there are, on average, only 1.08 doctors, In Africa, there are, on average, only 1.08 doctors, In Africa, there are, on average, only 1.08 doctors, nurses and midwives per 1000 populationnurses and midwives per 1000 populationnurses and midwives per 1000 populationnurses and midwives per 1000 populationIn real terms, this means that there are 17 doctors, 71 In real terms, this means that there are 17 doctors, 71 In real terms, this means that there are 17 doctors, 71 In real terms, this means that there are 17 doctors, 71 nurses and 20 midwives for each 100,000 people in nurses and 20 midwives for each 100,000 people in nurses and 20 midwives for each 100,000 people in nurses and 20 midwives for each 100,000 people in AfricaAfricaAfricaAfrica1 in 4 doctors and 1 nurse in 20 trained in Africa is working in developed countriesThe current rate of health worker production in these The current rate of health worker production in these The current rate of health worker production in these The current rate of health worker production in these countries is such that the deficit will never be met and countries is such that the deficit will never be met and countries is such that the deficit will never be met and countries is such that the deficit will never be met and will only continue to growwill only continue to growwill only continue to growwill only continue to grow
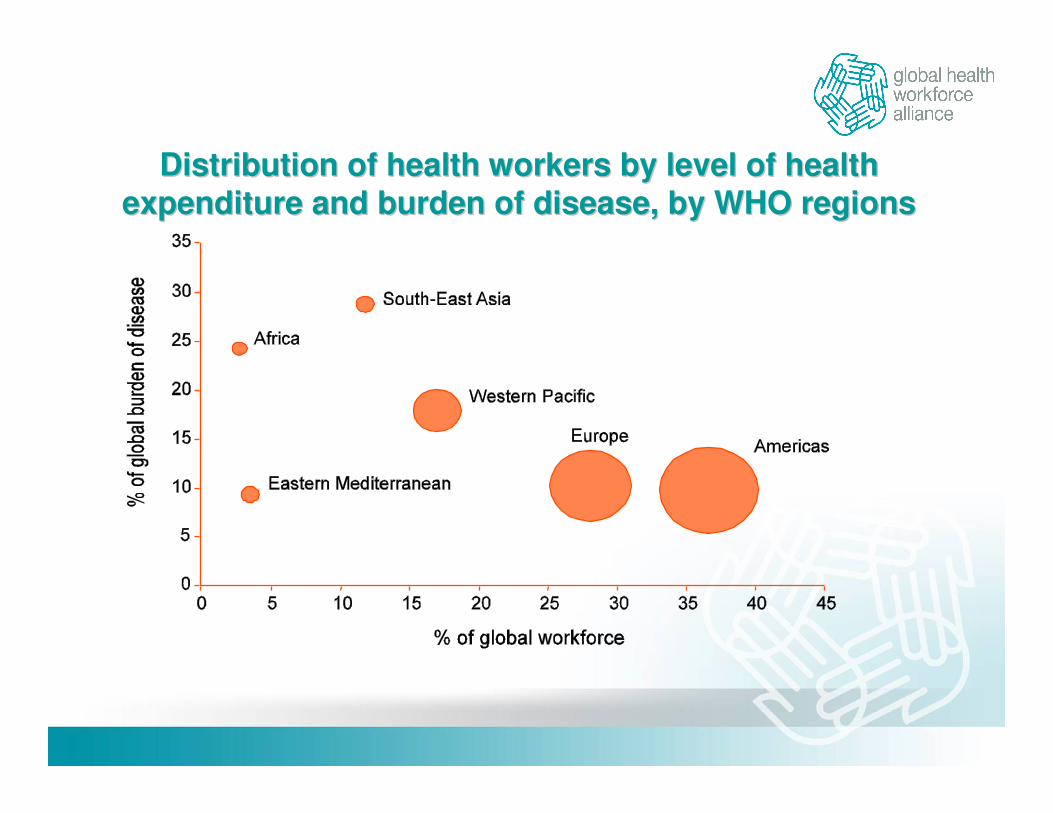
Distribution of health workers by level of healthDistribution of health workers by level of health
expenditure and burden of disease, by WHO regionsexpenditure and burden of disease, by WHO regions

Health Personnel in Asia
Pacific
Source: Asia-Pacific MDG Report 2010, 2010

Focus on Nigeria

Health worker availability and coverage of essential health services
Threshold = 2.3 HWs per 1000 pop
[Source] WHO. (2006). World Health Report 2006. WHO: Geneva.
Nigeria = 2.01 HWs per 1000 pop
Some Country Indicators
Population – 158 million
Density of Nurses, Midwives and Doctors per 1,000 population – 2.01
Number of maternal deaths – 50,000
Percent of all births registered – 33%
Health workforce shortage to attain 95% skilled birth attendance by 2015 – 6,790
Source: State of the World's Midwifery 2011, Nigeria Country Profile

Some MDG Indicators
Maternal Mortality Ratio (per 100,000 live births) - 840
Births attended by skilled health personnel – 39%
Under-5 Mortality Rate (per 1,000 live births) – 143
Source: Based on data in State of the World's Midwifery 2011, Nigeria Country Profile
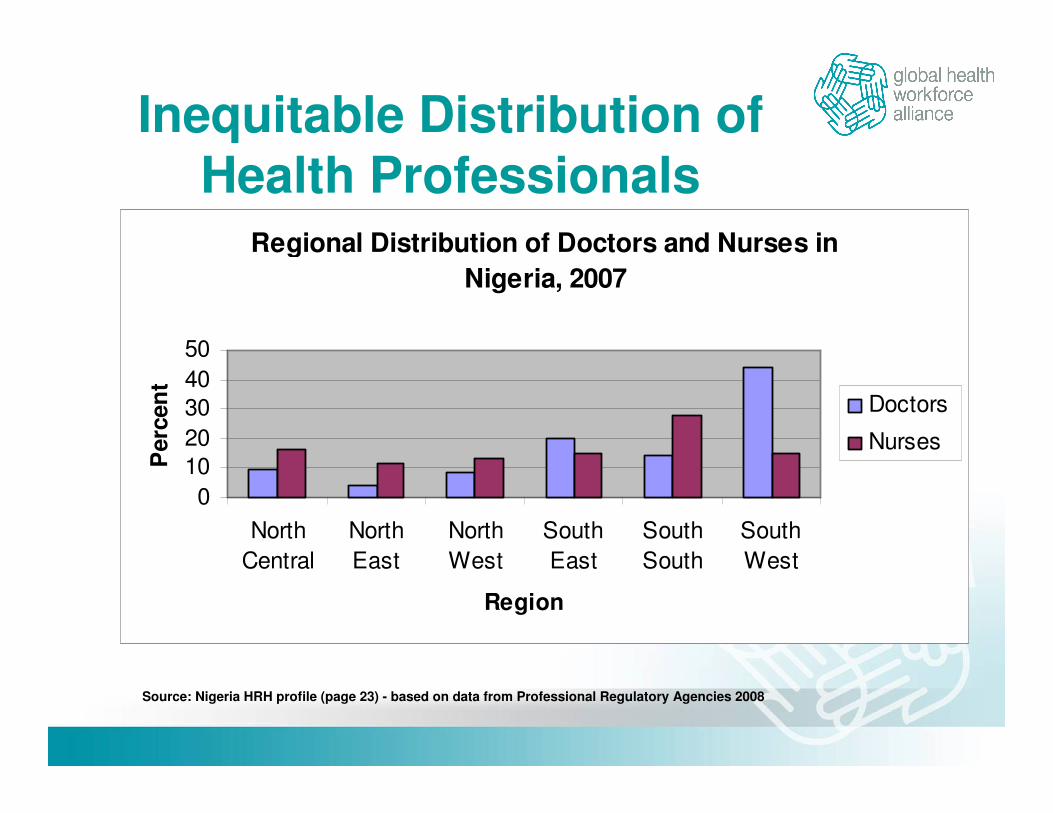
Inequitable Distribution of Health Professionals
Regional Distribution of Doctors and Nurses in
Nigeria, 2007
0
10
20
30
40
50
North
Central
North
East
North
West
South
East
South
South
South
West
Region
Perc
en
t
Doctors
Nurses
Source: Nigeria HRH profile (page 23) - based on data from Professional Regulatory Agencies 2008

Regional Disparities in Mortality
Distribution of Mortality by Geo-political Zones
050
100150200250300
N/Cent
ral
N/E
ast
N/West
S/E
ast
S/Sou
th
S/Wes
t
Zones
Mo
rtali
ty p
er
1,0
00 L
B
NNMR
PNNMR
IMR
CMR
U5MR
Source: Nigeria HRH profile (page 24) - based on data from NDHS Report 2003

Stagnant Production of Health Workers
Training Outputs from Health Training Institutions
from 2002 to 2005
0
2000
4000
6000
8000
10000
2002 2003 2004 2005
Year
Actu
al
An
nu
al
Ou
tpu
ts
Physicians
Nurses and midw ives
Pharmacists
Radiographers
Health records officers
Community health
practitioners
Source: Nigeria HRH profile (page 26) - based on data from National Universities Commission, Professional Regulatory Agencies, 2007

Need for Scaling Up Education
Rate of Increase of HRH Stock and Attrition Rate by
Cadre in the Nigerian Public Sector, 2006
05
101520
Docto
rs
Nurs
es a
nd
Mid
wiv
es
Labora
tory
Sta
ff
Pharm
acis
ts
and
technic
ians
CH
O/C
HE
Ws
Staff Category
Perc
en
t
Increase from New
Graduates
Attrition Rate
Source: Nigeria HRH profile (page 24) - based on data from National AIDS Control Agency, 2006

Slow progress towards MDG target
Source: Based on data in State of the World's Midwifery 2011, Nigeria Country Profile
Nigeria Trends in Maternal Mortality 1990-2015
1100 1100980
900 840
275
0
200
400
600
800
1000
1200
1990 1995 2000 2005 2010 2015
Year
Mate
rnal
death
s p
er
100,0
00 l
ive b
irth
s
Health Workers Save Lives!

Evidence base
Joint Learning Initiative on Human Resources for Health (JLI). Human Resources for Health: crises, strategies, sustainability. Cambridge, MA: Harvard University, Global Equity Initiative, 2004.
Link HRH policies to HRH availability: Dussault G, Dubois CA Human resources for health policies: a critical component in health policies. Hum Resour Health. 2003 1(1):1
Link health workers and health outcomes: Anand S, Bärnighausen T. Human resources and health outcomes: cross country econometric study. Lancet. 2004; 364(9445):1603-9
Chen, Lincoln, Timothy Evans, Sudhir Anand, Jo Ivey Boufford, Hilary Brown, MushtaqueChowdhury, Marcos Cueto, Lola Dare, Gilles Dussault, Gijs Elzinga, Elizabeth Fee, Demissie Habte, Piya Hanvoravongchai, Marian Jacobs, Christoph Kurowski, Sarah Michael, Ariel Pablos-Mendez, Nelson Sewankambo, Giorgio Solimano, Barbara Stilwell, Alex de Waal, Suwit Wibulpolprasert (2004). Human resources for health: overcoming the crisis (2004). The Lancet, Volume 364, Issue 9449, Pages 1984 - 1990, 27 November 2004 . doi:10.1016/S0140-6736(04)17482-5
Evidence base
Department for International Development, Management Sciences for Health and Management Solutions Consulting (2010). Evaluation of Malawi's Emergency Human Resources Programme. Final Report.
Global Health Workforce Alliance (2010). Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals: A Systematic Review, Country Case Studies, and Recommendations for Integration into National Health Systems. Global Health Workforce Alliance. Available online at http://www.who.int/workforcealliance/knowledge/publications/CHW_FullReport_2010.pdf
World Health Organization (2006). World Health Report 2006 - Working together for health. http://www.who.int/whr/2006/en/index.html. Accessed 02 May 2011.
Link HRH plans to HRH policy implementation: Global Health Workforce Alliance. Reviewing Progress, Renewing Commitment. Progress report on the Kampala Declaration and Agenda for Global Action; 2011, Geneva: WHO.

Density of health workers and skilled birth attendance
Source: WHO, World Health Report 2006
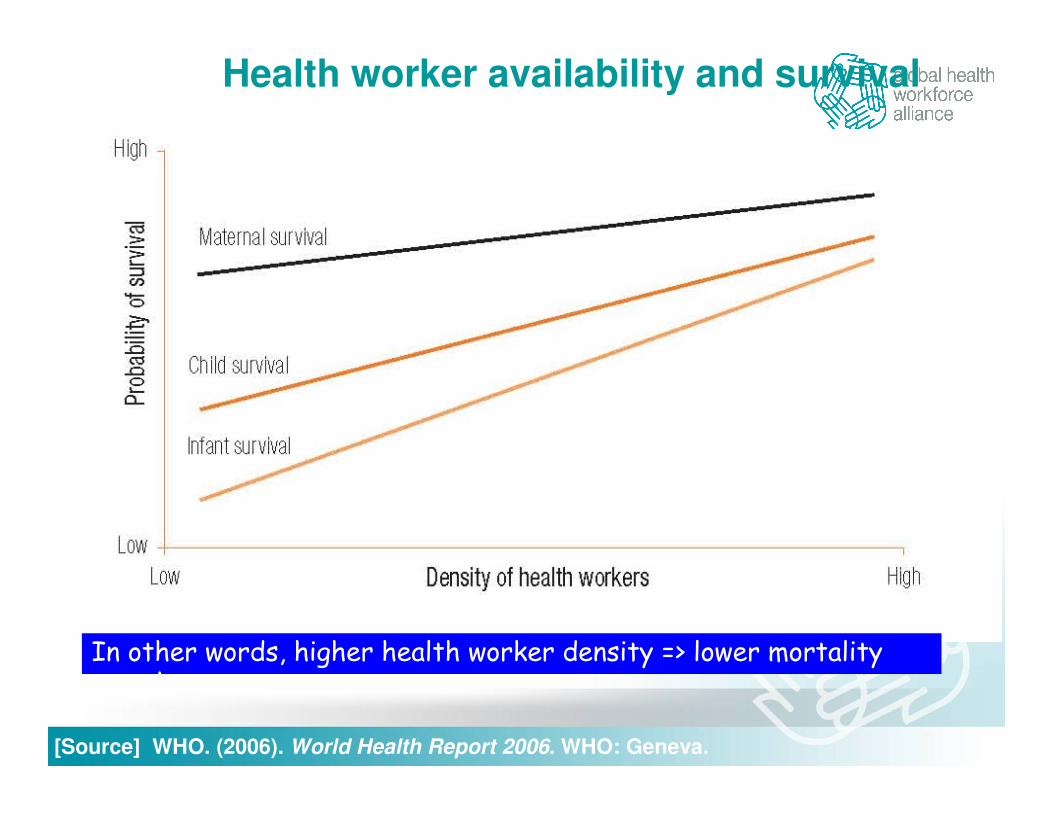
Health worker availability and survival
In other words, higher health worker density => lower mortality rate
[Source] WHO. (2006). World Health Report 2006. WHO: Geneva.

HRH availability and impact on
MDG targets
0
1
2
3
4
5
6
7
8
9
0 1 2 3 4 5
Density (workers per 1,000, log)
Mo
rtality
(p
er
1,0
00, lo
g)
Maternal
Infant
Under-5
Source: Anand & Source: Anand & BarnighausenBarnighausen 20042004
No health workforce, no health Millennium Development Goals!
MDG 4:MDG 4: reduce child mortality
MDG 5: MDG 5: reduce maternal mortality
MDG 6: combat HIV/ AIDS, malaria and other diseases
Future priorities: control chronic and non-communicable diseases

A Global Crisis Needs a Global Response!
Part 2
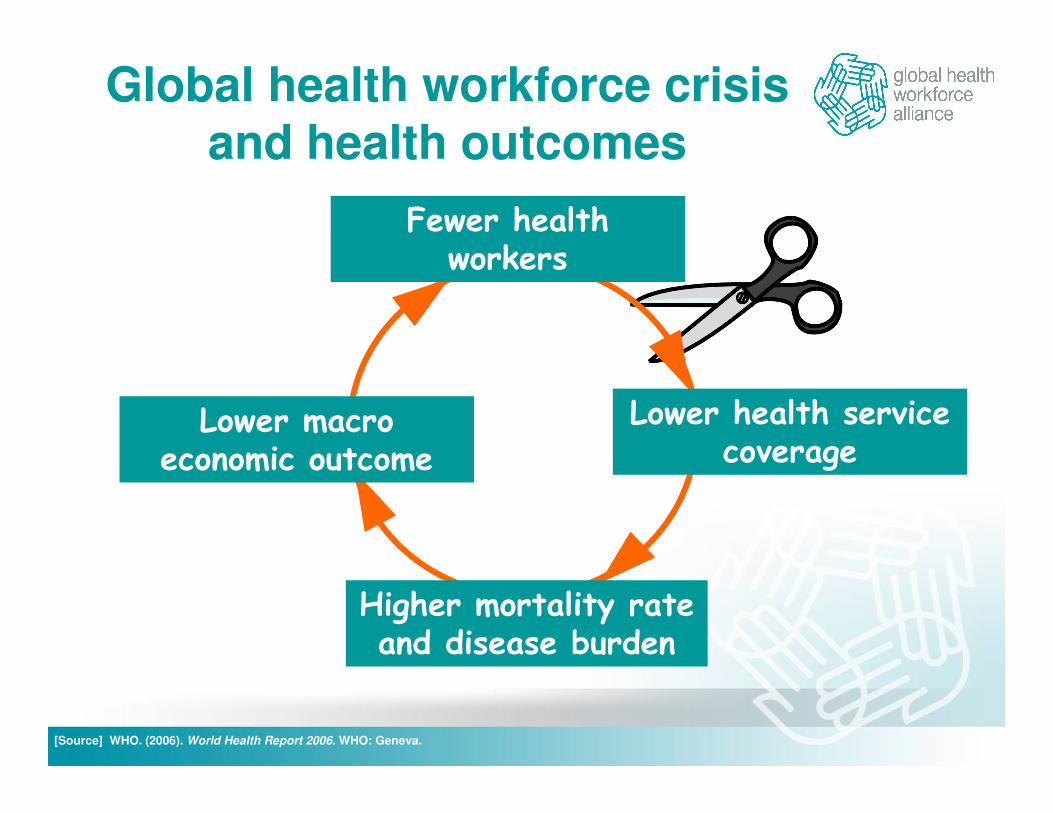
Global health workforce crisis and health outcomes
Lower health service coverage
Higher mortality rate and disease burden
Fewer health workers
Lower macro economic outcome
[Source] WHO. (2006). World Health Report 2006. WHO: Geneva.

The Global Health Workforce Alliance
"The Painful Fact
Worldwide, one billion people never see a health worker all their lives"
Amb. Sigrun Mogedal (former Chair, GHWA)
A global vision
“all people, everywhere, shall have access to a skilled, motivated and facilitated health worker within a robust health system” Kampala Declaration and Agenda for Global Action

The Roadmap: Kampala Declaration and The Roadmap: Kampala Declaration and
Agenda for Global ActionAgenda for Global Action
1. Building coherent national and global leadership for HW solution
2. Ensuring capacity for an informed responsebased on evidence and joint learning
3. Scaling up education and training
4. Retaining an effective, responsive and equitably distributed health workforce
5. Managing pressures of the international health workforce market and its impact on migration
6. Securing additional and more productive investment in the health workforce

� Vision: Access for all to a skilled, motivated, and supported health worker as part of a functioning health system
What is the Alliance?
� Mission: Mobilize all stakeholders to advocate and take appropriate actions to achieve access for all to health
workers, with a focus on the 57 countries in crisis.
� Composition: 336 Alliance Members and 27 Alliance
Partners from a variety of constituencies
� Organization: The Alliance is an international partnershiphosted by WHO, which brings together a variety of stakeholders� Government ministries and agencies, professional associations,
academia, civil society, UN agencies, donor agencies, private sector, etc
Three core functions “ABC”:
Core functions of GHWA
Convening all stakeholders => (1) CCF, (2) Global
consultation on community health workers.
Advocating for keeping HRH issues high on the global agenda => (1) Global forum on HRH, (2) High level
commitment at G8 – 2008, 2009, 2010 (3) Global code of practice on int’l recruitment of health personnel
Brokering knowledge => (1) Task forces, (2) technical tools, (3) community of practice, (4) knowledge centres, etc.

How does the Alliance work?
Allliance•Members •Partners •Secretariat•Board
Advocacy
Brokering knowledge Convening

Design, implement, monitor and evaluatea national comprehensive HRH plan
Academia
MoL
Civil
society
MoF
Prof Ass’n
MoH
Private
Sector
MoE
Convening: intersectoral coordination for integrated health workforce development
•19 countries have established/strengthened multi-sectoral HRH coordination mechanisms (as at October 2011)
Way Out of the Crisis, Country Actions and Progress
Part 3

The Roadmap: Kampala Declaration and The Roadmap: Kampala Declaration and
Agenda for Global ActionAgenda for Global Action
1. Building coherent national and global leadership for HW solution
2. Ensuring capacity for an informed responsebased on evidence and joint learning
3. Scaling up education and training
4. Retaining an effective, responsive and equitably distributed health workforce
5. Managing pressures of the international health workforce market and its impact on migration
6. Securing additional and more productive investment in the health workforce

The problem: HRH plans lacking or not costed or not implemented
57 priority countries
51 countries submitted data
43 countries had
evidence based HRH plans
29 countries were
implementing HRH plans
25 countries had
costed HRH plans
24 countries
had evidence basedand costed HRH
plans and were
implementing
them

Need to increase production
"…..with existing pre-service training patterns, countries would need:
36 years for physicians and 29 years for nurses and midwives - to reach the threshold of 2.28 health workers per 1,000 population, the level associated with at least 80% coverage of essential health services e.g., skilled birth attendance and fully immunized child…".
Kinfu et al BullWHO, 2009
The implication is that pre-service training of health workers needs to be expanded as well as combined with other measures to increase health worker inflow and reduce the rate of outflow.

45
Quantity
:
Pre
-serv
ice
train
ing
Quality:
In-service train
ing
Pro
fessional d
ev’t
Recruitment
Deployment &distribution
Migration & retention
Accred
itation
Soci
al rec
ognitio
n
MOH
MOLMOPS MOFA
MOE=>Education
MOF=> Investment
Health professional associations
Private sector
MOH
Civil society
NGOs
HRH as a complex polyhedronHRH as a complex polyhedron

Migration
Source: Nigeria HRH profile (page 30)
Destinations for Nurses Seeking Employment
Outside Nigeria, 2004 to 2007
0
500
1000
1500
2000
2500
3000
2004 2005 2006 2007
Year
Nu
mb
er
of
Nu
rse
s
United Kingdom
USA
Ireland
Australia
Canada
British Columbia
New Zealand
South Africa
Ghana
Botsw ana
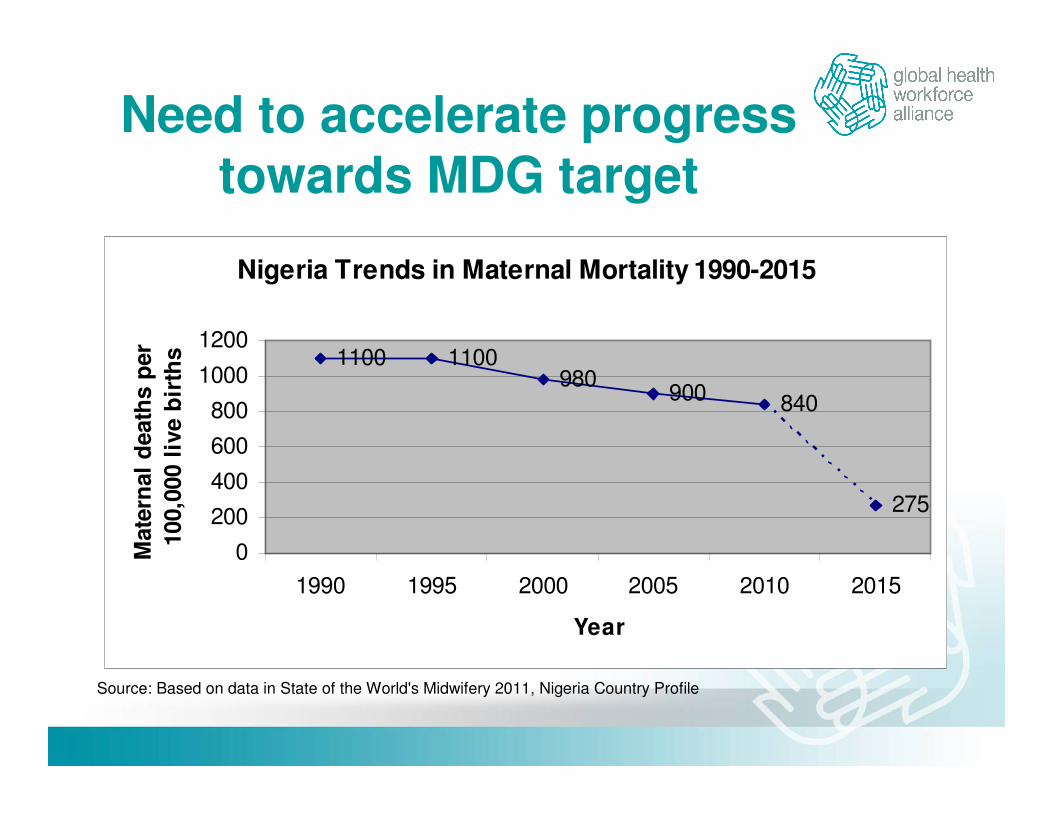
Need to accelerate progress towards MDG target
Source: Based on data in State of the World's Midwifery 2011, Nigeria Country Profile
Nigeria Trends in Maternal Mortality 1990-2015
1100 1100980
900 840
275
0
200
400
600
800
1000
1200
1990 1995 2000 2005 2010 2015
Year
Mate
rnal
death
s p
er
100,0
00 l
ive b
irth
s
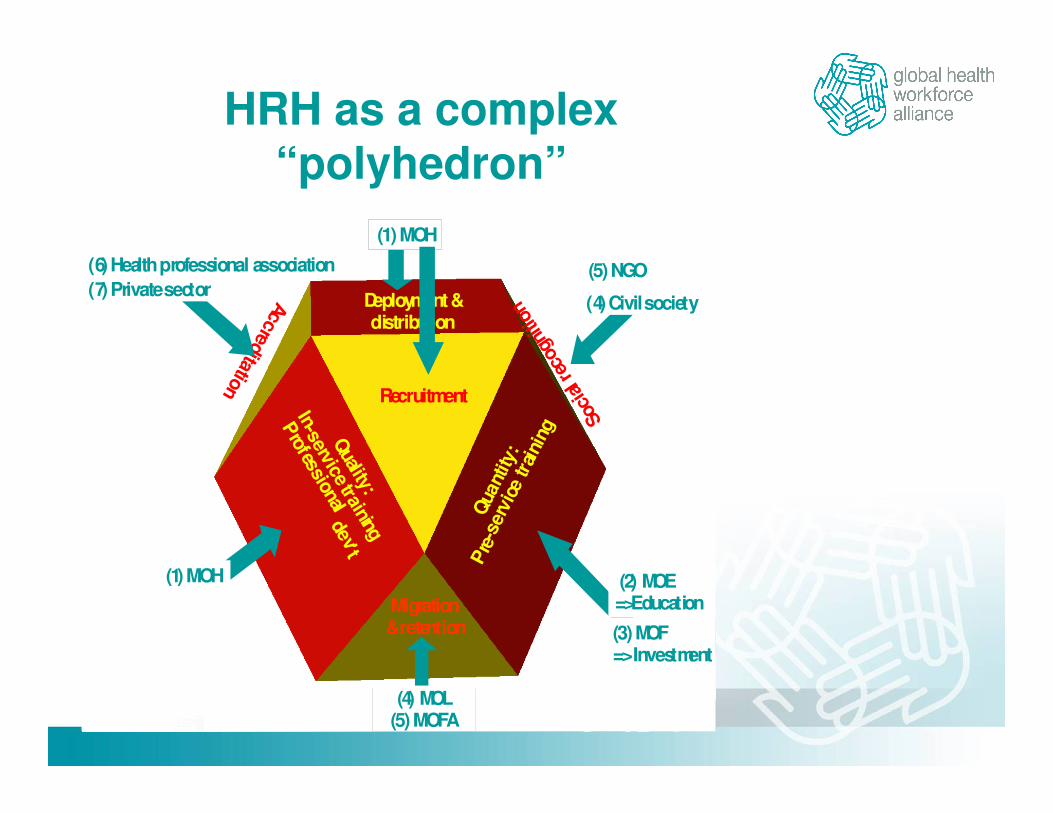
HRH as a complex “polyhedron”
Qua
ntity
:
Pre
-ser
vice
trai
ningQ
uality:
In-service training
Professional
dev’t
Recruitment
Deployment &distribution
Migration & retention
Accreditation
Soci
al rec
ogni
tion
(1) MOH
(4) MOL(5) MOFA
(2) MOE=>Education
(3) MOF=> Investment
(6) Health professional association
(7) Private sector
(1) MOH
(4) Civil society
(5) NGO
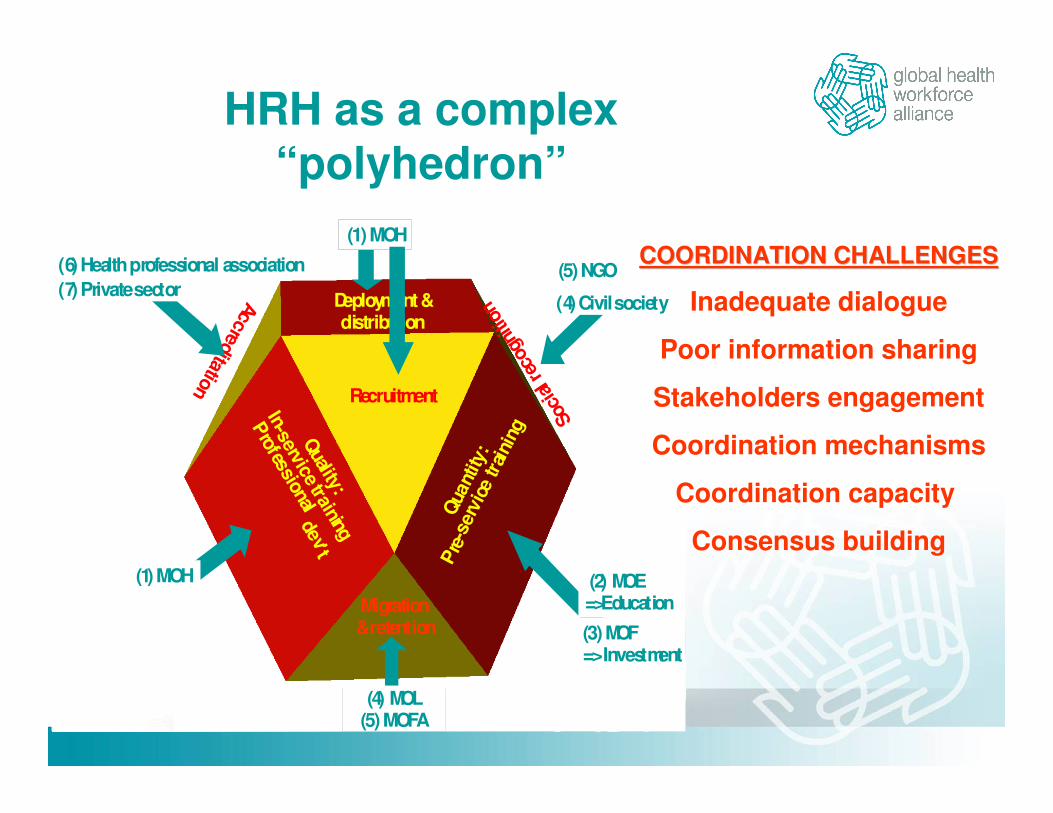
HRH as a complex “polyhedron”
Qua
ntity
:
Pre
-ser
vice
trai
ningQ
uality:
In-service training
Professional
dev’t
Recruitment
Deployment &distribution
Migration & retention
Accreditation
Soci
al rec
ogni
tion
(1) MOH
(4) MOL(5) MOFA
(2) MOE=>Education
(3) MOF=> Investment
(6) Health professional association
(7) Private sector
(1) MOH
(4) Civil society
(5) NGOCOORDINATION CHALLENGESCOORDINATION CHALLENGES
Inadequate dialogue
Poor information sharing
Stakeholders engagement
Coordination mechanisms
Coordination capacity
Consensus building

50
Design, implement, monitor and evaluatea national comprehensive HRH plan
Academia
MoL
Civil
society
MoF
Prof Ass’n
MoH
Private
Sector
MoE
National HRH committeeNational HRH committee
CCF
CC
FC
CF

The CCF
PROCESS
HRH PLANCompressive, Costed, Evidence-based
REDUCED HRH CRISIS
HRH COMMITTEE
Ministry of Health
Ministry of
Education
Ministry of
Labour
Ministry of
Finance
Ministry of
Local Govt.
Academia Researchers
Professional associations
Regulatory
bodies
NGOs and
civil society
Private
sector
UN agencies and International organizations
Other HRH related stakeholders
De
ve
lop
F
ina
nce
Implement
Mo
nito
r E
va
lua
te
Sta
ke
ho
lde
rs a
na
lys
is a
nd
id
en
tifi
ca
tio
n
Oth
er
HS
S c
oo
rdin
ati
on
me
ch
an
ism
s
Contributing to a Contributing to a
solutionsolution

Current status of CCF roll-out
21
14
43
0
5
10
15
20
25
Total Completed Under process Planned
Total Completed
Under process Planned
21
12
4 5
0
5
10
15
20
25
Total Completed Under
process
Planned
Total Completed
Under process Planned
HRH situation analysis
through the CCF process
Evidence based, and costed
HRH plan through the CCF process

Positive developments but….
but much remains to be
done!

A long-term monitoring agendaImportant evidence gaps persist
Factors underpinning quality and implementation of HRH plans and function of coordination mechanismsTraining curricula and competency frameworks Workforce movement, availability, distributionQuality and performance of health workforceTrends in health expenditure for HRH
Need to focus on results!
Shift from input and process to output indicators
New HRH benchmarks
Monitoring to be embedded in national mechanisms
Implementation of WHO Global Code
Implement the Roadmap
KD-AGA remains valid framework
Accelerate development, costing and implementation of multi-sector HRH plans
Enhance monitoring for improved tracking and use of data
Attention to quality of education

Role of Community Health Workers and Mid-Level Health Providers
Implement initiatives to favour retention (e.g. WHO guidelines)
Laws, systems and procedures to implement Code on International Recruitment
Investment: both domestic and international resources
Implement the Roadmap

A long-rough-winding road to reach our HRH vision
Inspired by dedicated health workers
“…There is no house in the village that I have not visited.”
“…There are many health workers like me, silently serving the communities... if one recognizes these silent heroes, give them opportunities, one could harness their talents and motivate them to serve better…our world will become a better and a healthy place to live.”
P.D. Lalitha Padmini
Public Health Midwife, Sri Lanka

Thanks for your attention
Contacts:
Dr. Mubashar SheikhDr. Mubashar Sheikh
Executive DirectorExecutive Director, , the the GHWAGHWA
Email: Email: [email protected]@who.int
URL: URL: http://http://www.who.int/workforcealliance/enwww.who.int/workforcealliance/en//
Dr. George PariyoDr. George Pariyo
Medical OfficerMedical Officer
Email: Email: [email protected]@who.int
http://http://www.who.int/workforcealliance/enwww.who.int/workforcealliance/en//


















