
OVERVIEW OF EmONC NEEDS ASSESSMENTS - MCHIP UNICEF... · Essential Drugs, Equipment and ......
22
OVERVIEW OF EmONC NEEDS ASSESSMENTS Patsy Bailey, DrPH, AMDD/FHI 360 Maternal & Newborn Health Services Measurement Meeting Arusha, Tanzania 14 January 2013
Transcript of OVERVIEW OF EmONC NEEDS ASSESSMENTS - MCHIP UNICEF... · Essential Drugs, Equipment and ......
OVERVIEW OF EmONC NEEDS ASSESSMENTS Patsy Bailey, DrPH, AMDD/FHI 360 Maternal & Newborn Health Services Measurement Meeting Arusha, Tanzania 14 January 2013

EmONC Needs Assessments • Facility-based cross sectional surveys • Measure current functioning and capacity of a health system to
provide maternal and newborn services • Usually national in scope • Census of all hospitals and health centers, sometimes a
“systematic selection” of lower level facilities (all do deliveries) • Tool kit contains:
• Modules and Manual for data collectors • 4 additional tools to support planning and implementation of
the NA • Available for download at www.amddprogram.org

In the context of other service provision surveys …
• Scope and Purpose • Data are fed back to lower levels to be used for planning at
facility and district level. Thus, sampling discouraged. • Characteristics
• Questionnaires adaptable and dynamic (making some cross-country comparisons difficult)
• Local ownership (public access to data can be sketchy – no one repository for databases)

EmONC Needs Assessments by current status (as of December 2012)
Completed – pre-2005 Completed – 2005 and later Ongoing

Data Collection Modules (adapted by each country)
0. National Level Information 1. Identification of Facility & Infrastructure 2. Human Resources 3. Essential Drugs, Equipment and
Supplies 4. Facility Case Summary / Service
statistics 5. EmONC Signal Functions & Other
Important Services 6. Partograph Chart Review 7. Provider Knowledge & Competency
Interview 8. Cesarean Delivery Chart Review 9. Maternal Death Chart Review 10. Neonatal Death Chart Review 11. Referral

EmONC assessments collect the data for the EmOC indicators • Availability and distribution
of facilities fully functioning at EmONC levels
• Institutional delivery rate • Met need • Population-based cesarean
rate • Direct obstetric case
fatality rate • Intrapartum stillbirth and
early neonatal death rate • % maternal deaths due to
indirect causes

Selected topics for this meeting
• Pre-eclampsia and eclampsia • Postpartum hemorrhage • Obstructed labor • Newborn birth asphyxia • Low birth weight newborns

Human resources • Which health worker cadres
• Administer parenteral anticonvulsants • Administer parenteral uterotonics and misoprostol • Perform manual removal of placenta • Perform MVA • Perform cesarean delivery • Complete partographs • Perform newborn resuscitation • Perform immediate newborn care (including skin-to-skin care)
• Cadre availability on duty & on call 24/7
Equipment, supplies, drugs and guidelines
• Availability & stock out frequency of magnesium sulfate, oxytocin, misoprostol
• Cost of magnesium sulfate and oxytocin to patient • Availability of blank partographs • Equipment: MVA, D&C, ambu bag & mask plus other
essential and specialist’s equipment • Requisites for functioning operating theatre • Availability of explicit clinical guidelines for treatment
of obstetric complications, neonatal resuscitation, kangaroo mother care

Current functioning status and recent performance
• Administration of parenteral anticonvulsants/ uterotonics in last 3 & 12 months, if not, why not, and if ‘yes,’ what drugs were administered
• Same question for manual removal of placenta, removal of retained products, neonatal resuscitation, cesarean delivery and completion of partograph
• Number of cases by month over last 12 months for: • Treated cases of PE/E, PPH, retained placenta, prolonged/
obstructed labor • Maternal deaths by cause • Intrapartum stillbirths & early neonatal deaths (by birth weight) • Vaginal and cesarean deliveries

Availability of anticonvulsants among facilities that had used them in the last 12 months, Angola 2007
0%10%20%30%40%50%60%70%80%90%
100%
Kuanz
a Sul
Malange
Cabind
aUige
Bengo Bié
Luan
da
Huambo
Lund
a Nort
eZaire
Nation
alHuil
a
Kuanz
a Nort
e
Bengu
ela
Cunene
Kuand
o Kubang
o
Lund
a Sul
Moxico
Namibe
Mag Sulfate Diazepam Both

Case fatality rates for PE/E, Angola 2007
9.0%
1.4%
5.6%
1.1%
0% 2% 4% 6% 8% 10%
15 provinces
Huila + Benguela
17 provinces
Luanda
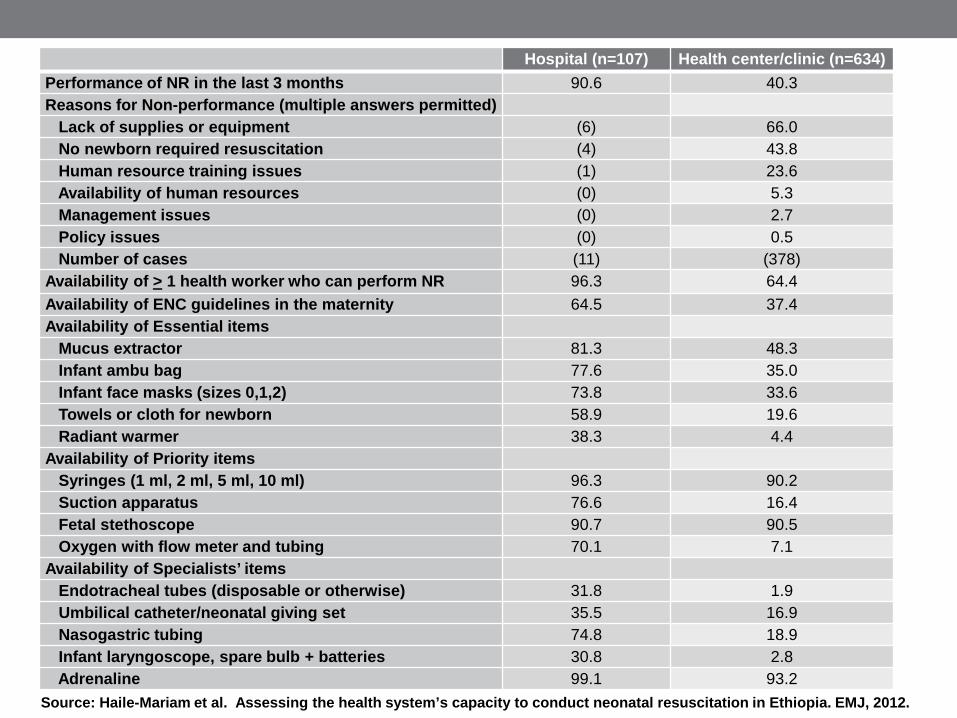
Hospital (n=107) Health center/clinic (n=634) Performance of NR in the last 3 months 90.6 40.3 Reasons for Non-performance (multiple answers permitted) Lack of supplies or equipment (6) 66.0 No newborn required resuscitation (4) 43.8 Human resource training issues (1) 23.6 Availability of human resources (0) 5.3 Management issues (0) 2.7 Policy issues (0) 0.5 Number of cases (11) (378) Availability of > 1 health worker who can perform NR 96.3 64.4 Availability of ENC guidelines in the maternity 64.5 37.4 Availability of Essential items Mucus extractor 81.3 48.3 Infant ambu bag 77.6 35.0 Infant face masks (sizes 0,1,2) 73.8 33.6 Towels or cloth for newborn 58.9 19.6 Radiant warmer 38.3 4.4 Availability of Priority items Syringes (1 ml, 2 ml, 5 ml, 10 ml) 96.3 90.2 Suction apparatus 76.6 16.4 Fetal stethoscope 90.7 90.5 Oxygen with flow meter and tubing 70.1 7.1 Availability of Specialists’ items Endotracheal tubes (disposable or otherwise) 31.8 1.9 Umbilical catheter/neonatal giving set 35.5 16.9 Nasogastric tubing 74.8 18.9 Infant laryngoscope, spare bulb + batteries 30.8 2.8 Adrenaline 99.1 93.2
Source: Haile-Mariam et al. Assessing the health system’s capacity to conduct neonatal resuscitation in Ethiopia. EMJ, 2012.


Provider knowledge & competency • Provider knowledge + guided interview
• Observations made when monitoring a woman in labor • Actions taken during AMTSL • Signs looked for if woman has heavy bleeding • Actions taken if a woman has heavy bleeding • Actions taken if retained placenta • Special care provided when newborn weighs less than 2.5 kgs • How to diagnose birth asphyxia • Steps of neonatal resuscitation
• Provider training and performance in last 3 months • AMTSL • Manual removal of placenta • External and internal bimanual uterine compression • Suture episiotomy, vaginal lacerations, cervical lacerations • MVA • D&C • NR • Complete and use a partograph
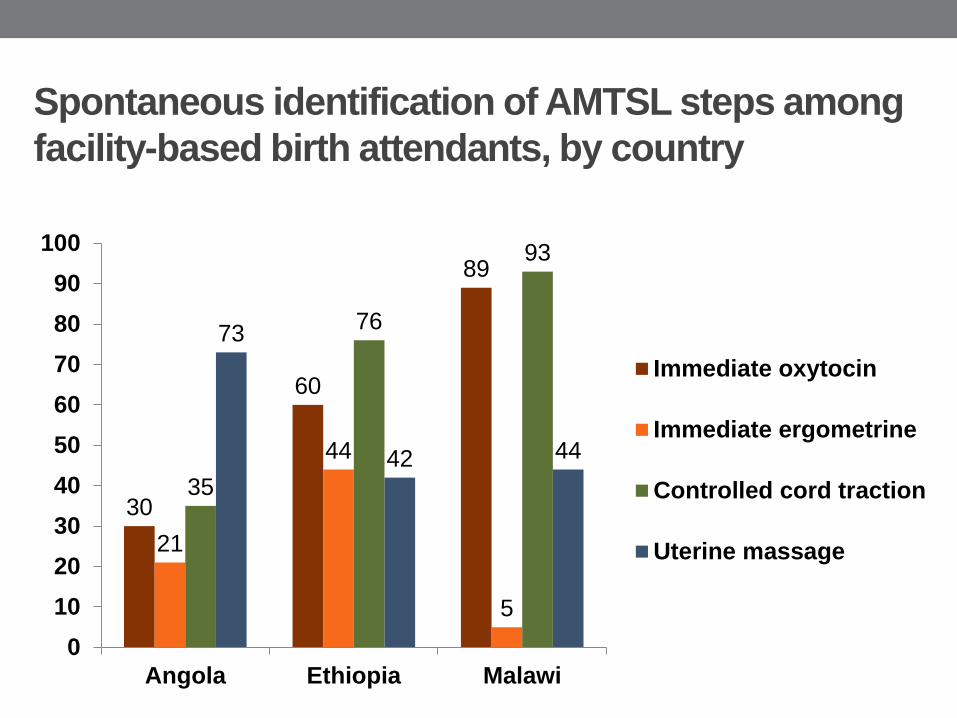
Spontaneous identification of AMTSL steps among facility-based birth attendants, by country
30
60
89
21
44
5
35
76
93
73
42 44
0102030405060708090
100
Angola Ethiopia Malawi
Immediate oxytocin
Immediate ergometrine
Controlled cord traction
Uterine massage

Chart reviews • Partograph review (23 questions)
• Type used, if not used, why not • Dilatation when started, times temperature, BP, pulse
recorded, if fetal HR and contractions recorded hourly, etc. • When did delivery occur, if augmentation was done, type of
delivery and perinatal outcomes • Cesarean delivery review (23 questions)
• Who performed • Emergency / elective, indication • Use of antibiotics, wound infection, partograph used • Time from decision to incision • Maternal and newborn outcomes

Percentage of partographs reviewed with admission dilatation charted correctly
96
94
88
84
81
63
45
0 20 40 60 80 100
Benin
Malawi
Ghana
Niger
Guyana
Madagascar
Ethiopia
n=32
n=2092
n=878
n=1195
n=398
n=1163
n=231
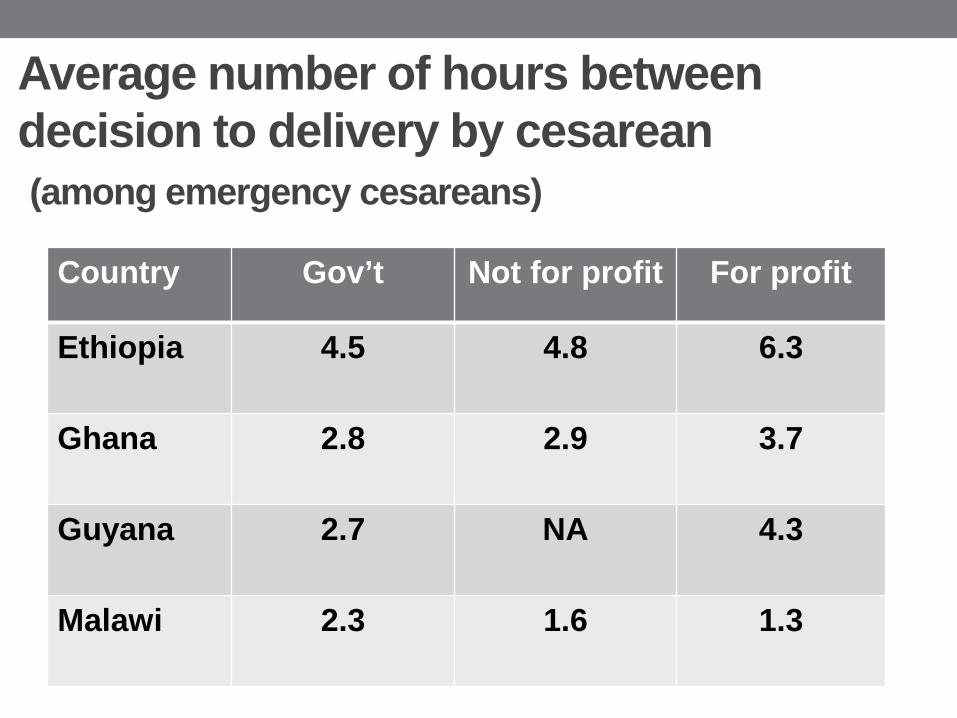
Average number of hours between decision to delivery by cesarean (among emergency cesareans)
Country Gov’t Not for profit For profit
Ethiopia 4.5 4.8 6.3
Ghana 2.8 2.9 3.7
Guyana 2.7 NA 4.3
Malawi 2.3 1.6 1.3

Stillbirth and early neonatal death rate among institutional births
121
49 45 42
29 23
16
0
20
40
60
80
100
120
140
Madagascar Ethiopia Niger Angola Malawi Guyana Ghana

Lessons Learned regarding the NAs
• Demand for data on quality of services goes beyond infrastructure • Guided interview on neonatal resuscitation to proxy
simulation • Data quality issues have led to audits to improve
recording • Timing (fresh or macerated) of fetal death often unrecorded • Birth weight often unrecorded, especially of stillbirths • Reporting of fetal death vs. early neonatal death may not be accurate
• Fact sheets & GIS powerful tools for planning, implementation and dissemination

Implications of adding an observational component • An additional module means extending each facility
visit, or dropping current modules • Revisiting the profile and training of data collectors • IRB considerations • Could restrict observational component to a sample
of facilities • Jhpiego NA in Afghanistan seems to have been
successful in adding observational components on newborn resuscitation and cesarean delivery


















