Overview Internal review
49
Slide 1 © PharmOut 2015 Overview – Internal review • Presentation title: PDE Derivation for APIs – Case Study Venlafaxine • Track title: Contamination/ Toxicology • Speaker: Andrew Bartholomaeus • Date / Time: Tuesday • Time allotted: 1:30 – 2:30 • Dot point overview: • A worked case study deriving a PDE and OEL for venlafaxine
Transcript of Overview Internal review

Slide 1 © PharmOut 2015
Overview – Internal review• Presentation title: PDE Derivation for APIs – Case Study Venlafaxine
• Track title: Contamination/ Toxicology
• Speaker: Andrew Bartholomaeus
• Date / Time: Tuesday
• Time allotted: 1:30 – 2:30
• Dot point overview:
• A worked case study deriving a PDE and OEL for venlafaxine

R I S K I D E N T I F I C A T I O N F O R
M A N U F A C T U R E I N S H A R E D F A C I L I T I E S
PDE Derivation for APIsCase StudyVenlafaxine
BartCrofts Scientific Services Pty Ltd
Prof. Andrew BartholomaeusSchool of Pharmacy, University of Canberra
Therapeutic Research Centre, School of Medicine, University of QueenslandCEO, BartCrofts Scientific Services Pty Ltd
Email; [email protected]

BartCrofts Scientific Services Pty Ltd

1 . C L E A R L Y I D E N T I F Y T H E A P I
2 . G A T H E R A V A I L A B L E D A T A S O U R C E S
3 . I D E N T I F Y T H E K E Y H A Z A R D S
4 . E S T A B L I S H A N D R A N K O R D E R T H R E S H O L D S
5 . I D E N T I F Y U N C E R T A I N T I E S
6 . C A L C U L A T E P D E
BartCrofts Scientific Services Pty Ltd
Stepping Through the Process

C H E M I C A L A N D G E N E R I C N A M E
M A N U F A C T U R E R S R E S E A R C H C O D E S
BartCrofts Scientific Services Pty Ltd
Step 1 Identify the API

Identify the APIWhat is it
BartCrofts Scientific Services Pty Ltd
Generic Name Venlafaxene
Chemical Name (R/S)-1-[2-(dimethylamino)-1-(4-methoxyphenyl)ethyl]
cyclohexanol hydrochloride or (±)-1-[α- [(dimethyl-amino)methyl]-p-methoxybenzyl]cyclohexanol hydrochloride
MW 313.87
Structure
Brand Name Effexor
code name WY-45030 Early studies may use the code so this is important when searching
the literature

What does it do
BartCrofts Scientific Services Pty Ltd
Venlafaxine is an antidepressant that inhibits the reuptake of both 5-hydroxytryptamine (serotonin; 5-HT) and noradrenaline (NA). It is somewhat more potent as an inhibitor of the reuptake of 5-HT than NA. Its potency to inhibit the reuptake of 5-HT is comparable to that of tricyclic antidepressants (TCAs) such as amitriptyline or imipramine, but it is less potent than these drugs at inhibiting the reuptake of NA. ie the drug is quite receptor specific so any value that is
protective of the primary receptor is protective of less sensitive receptors

What is the normal human therapeutic Dose range
BartCrofts Scientific Services Pty Ltd
Maximum approved dose 225 mg/day
Minimum initiation dose 37.5 mg/day
This is a dose that does not produce side effects, or only minor effects, in most people
Unlikely to be pharmacologically active
Used to build tolerance to the drug before ramping up dosage to a pharmacologically active dose
Minimum daily dose 75 mg/day
The minimum shown to be therapeutically effective in clinical trials
A clear “effect” dose

BartCrofts Scientific Services Pty Ltd
Step 2 Gather Available Data Sources

Sources of Data
BartCrofts Scientific Services Pty Ltd
European Medicines Agency EPAR (European Public Assessment Reports - Summary of submission and evaluation)
http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/landing/epar_search.jsp&mid=WC0b01ac058001d124
Clinical reports – from mid 2016
US FDA Drugs@FDA
http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm
Australian TGA Product Information Documents
http://search-au.funnelback.com/s/search.html?collection=tga-artg
AusPARs (Australian Public Assessment Reports) https://www.tga.gov.au/browse-auspars-active-ingredient
Prescribing Medicine in Pregnancy http://www.tga.gov.au/prescribing-medicines-pregnancy-database
NIH TOXNET (collection of databases including DART, TOXLINE, HSDB)
http://toxnet.nlm.nih.gov/
DailyMed http://dailymed.nlm.nih.gov/dailymed/index.cfm
For Vitamins and Minerals use Nutrient Reference Values, Upper Levels Eg US IOM - http://ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx Australian NHMRC - https://www.nrv.gov.au/
Abstracting data bases, eg MEDLINE, PUBMED
Notes on Sources
BartCrofts Scientific Services Pty Ltd
No one source will give you all the information you need. Prescriber Information (PI) /labels evolve over time and different PI sheets for different brands of the same generic drug will include information from different studies
Studies available to one National Regulator may not be available to another so check at least 2 major regulators

Venlafaxine data
BartCrofts Scientific Services Pty Ltd
EMA - EPAR
FDA
Review
Product Label (prescriber Information)
TOXNET
HSDB summary
PUBMED
Published studies from development phase
√
√
√
√
X
X

BartCrofts Scientific Services Pty Ltd
Step 2 Identify Key Hazards

Pharmacokinetics
BartCrofts Scientific Services Pty Ltd
Well absorbed orally, plasma half life 5 hrs Volume of Distribution 7.5 L/kg, bioavailability 92%
This data can be used to estimate achieved systemic concentrations from a given exposure
Almost all API is metabolised to ODV and ODV conjugates, and then excreted in the urine Hepatic or renal impairment might increase systemic exposure by
delaying elimination Probably not a substantial concern at low exposures The ODV metabolite is biologically active

Pharmacology
BartCrofts Scientific Services Pty Ltd
IC50 values for neurotransmitter reuptake (concentration producing a 50% inhibition of target receptors) – a measure of potency – the lower the number the more potent for Noradrenaline is 300 nM For 5-Hydroxy-tryptamine is 50 nM (5-HT is also known as Serotonin )
Need a substantial proportion of the uptake inhibited for some period of time to produce a therapeutic or pharmacological effect
Calculate dose to achieve IC50 assuming 100% bioavalability and instant absorption (ie be conservative) Vd for a 50 kg person is 375 L MW 314 g/M Bioavailability essentially 100%
So, simplistically, 50 nM in body fluids would require a dose of
𝑑𝑜𝑠𝑒 = 50𝑛𝑀 ∗314𝑛𝑔
𝑛𝑀∗ 375𝐿 = 5.9 𝑚𝑔
Realistically absorption is not instantaneous and metabolism and excretion start immediately so achieved levels would be << than calculated and quite transient
Hence therapeutic dose is >> 6 mg (25 mg tid, 75 mg/day as a starting dose) Exposure of < 50% of the IC50 value (3 mg/day or 0.06 mg/kg bw/d) very unlikely to be
pharmacologically active
Clinical efficacy and IC50
BartCrofts Scientific Services Pty Ltd
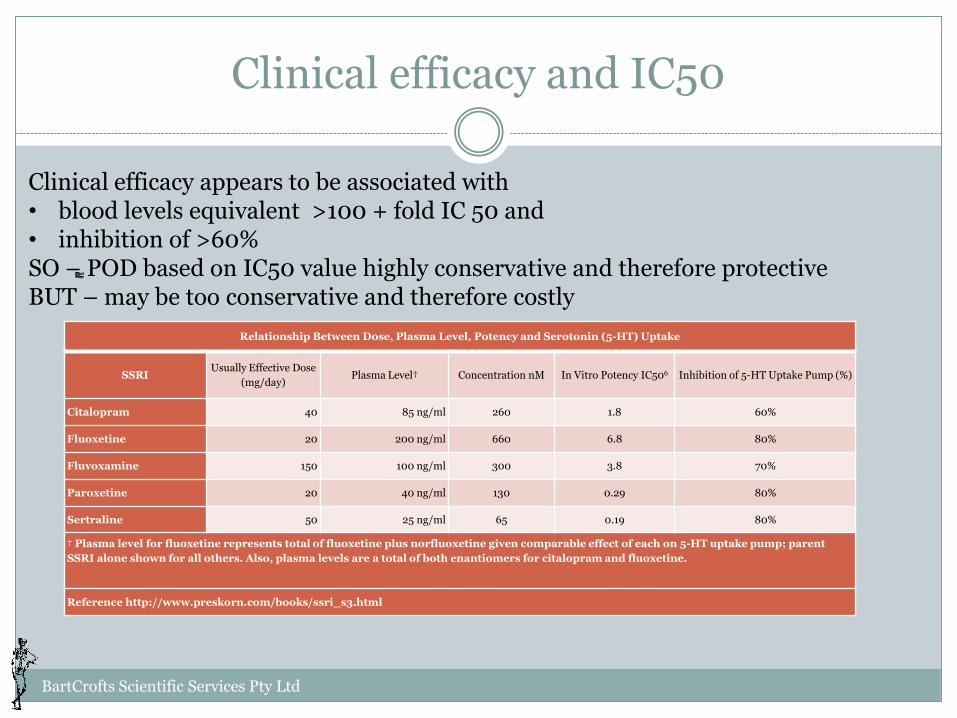
Relationship Between Dose, Plasma Level, Potency and Serotonin (5-HT) Uptake
SSRIUsually Effective Dose
(mg/day)Plasma Level† Concentration nM In Vitro Potency IC506 Inhibition of 5-HT Uptake Pump (%)
Citalopram 40 85 ng/ml 260 1.8 60%
Fluoxetine 20 200 ng/ml 660 6.8 80%
Fluvoxamine 150 100 ng/ml 300 3.8 70%
Paroxetine 20 40 ng/ml 130 0.29 80%
Sertraline 50 25 ng/ml 65 0.19 80%
† Plasma level for fluoxetine represents total of fluoxetine plus norfluoxetine given comparable effect of each on 5-HT uptake pump; parent
SSRI alone shown for all others. Also, plasma levels are a total of both enantiomers for citalopram and fluoxetine.
Reference http://www.preskorn.com/books/ssri_s3.html
Clinical efficacy appears to be associated with• blood levels equivalent >100 + fold IC 50 and • inhibition of >60%SO – POD based on IC50 value highly conservative and therefore protectiveBUT – may be too conservative and therefore costly
Carcinogenicity
BartCrofts Scientific Services Pty Ltd
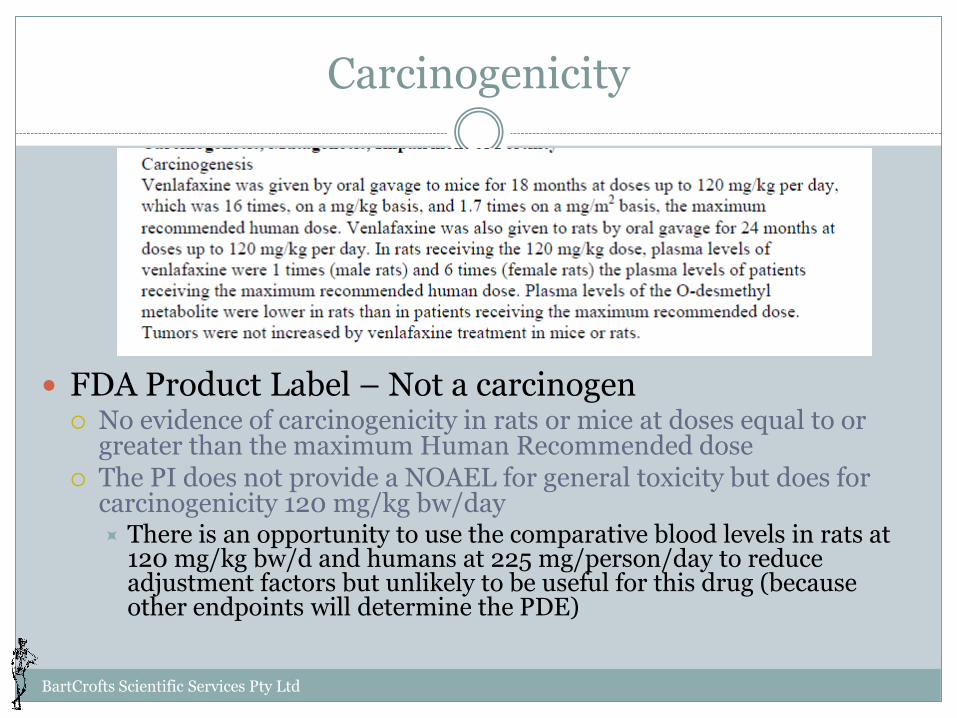
FDA Product Label – Not a carcinogen No evidence of carcinogenicity in rats or mice at doses equal to or
greater than the maximum Human Recommended dose The PI does not provide a NOAEL for general toxicity but does for
carcinogenicity 120 mg/kg bw/day There is an opportunity to use the comparative blood levels in rats at
120 mg/kg bw/d and humans at 225 mg/person/day to reduce adjustment factors but unlikely to be useful for this drug (because other endpoints will determine the PDE)

Genotoxicity
BartCrofts Scientific Services Pty Ltd
FDA Product Label venlafaxine not genotoxic
ODV mostly negative results but one study at high exposures relative to human therapeutics (& therefore contamination level) was positive
Weight of evidence indicates not a genotoxin at plausible exposure levels.

Reproduction and development - Fertility
BartCrofts Scientific Services Pty Ltd
The parent API had no effect but the metabolite reduced fertility in rats at a systemic exposure (AUC) = to 2-3 x the maximum human dose of 225 mg/day The comparison was based on exposure calculated from AUC Rat dose unknown and not readily calculated from this description The comparison is based on a LOAEL, the NOAEL is not given Could use human dose x 2 but then apply AFs to cover cross species extrapolation plus interindividual variation plus lack of NOAEL So
human dose 4.5 mg/kg bw/d x 2 = 9 mg/kg bw/d Very messy
BUT - US Pharmacopeial Convention MSDS indicates no fertility effect from venlafaxine in rats at up to 8 times max human dose (dose ≠AUC) – ie a NOEL NOEL for venlafaxine = 8 x 4.5 mg/kg bw/d = 36 mg/kg bw/day
There is no discordance between these 2 findings. Quite likely the rat required a dose >> 8 times human dose on mg/kg bw/d basis to achieve 2 X the AUC – this is a common finding

Foetal Development
BartCrofts Scientific Services Pty Ltd
TGA Categorization B2 Drugs which have been taken by only limited number of pregnant women and women of childbearing age, without
an increase in the frequency of malformation or other direct or indirect harmful effects on the human foetus having been observed. Studies in animals are inadequate or may be lacking, but available data show no evidence of an increased occurrence of foetal damage
Not a teratogen – no malformations ? Foetal survival reduced
But generally related to decreased maternal care resulting from pharmacological effects on the dam.
NOAEL 1.4 x human maximum dose of 225 mg/day Assume per EMA guidance a human bw of 50 kg Then dose in humans = 225÷50 = 4.5 mg/kg bw/day Rat NOAEL is therefore 1.4x4.5 = 6.3 mg/kg bw/day
Need to check post market literature for human experience to add or reduce weight to the other observations (reduced weight gain, stilborn)

Some discordant data
BartCrofts Scientific Services Pty Ltd
In a perinatal toxicity study in rats after oral dosing of dams with 30 mg/kg or more,
decreased pup survival following birth was observed. This effect is secondary to
treatment decreased maternal care, and is also seen with other antidepressants. (TGA PI)
In a developmental study in rabbits (Sloot et al., 2009) administered venlafaxine HCL at
0, 45, 90 or 135 mg/kg bw/d cardiovascular related malformations were observed
in 12/161 at 135 mg/kg bw/d and 5/161 at 90 mg/kg bw/d. The NOAEL for foetal development in this study appears to be 45 mg/kg bw/d. Skeletal malformations have also been
reported for this study but details are not available
Other rabbit studies apparently negative
Human prospective trial found no teratogenic or survival effect
Venlafaxine late in the 3rd trimester may result in functional and behavioural deficits in the newborn infant including respiratory distress, cyanosis, apnea, seizures, temperature instability, feeding difficulty, vomiting, hypoglycemia, hypotonia,
hypertonia, hyperreflexia, tremor, jitteriness, irritability, and constant crying.
The clinical features are consistent with either a direct toxic effect or drug discontinuation syndrome and, occasionally, may resemble a serotonin syndrome.
The complications may require prolonged hospitalization, respiratory support, and tube feeding (Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk)

What to do
BartCrofts Scientific Services Pty Ltd
Consider evidence Available human data indicates teratogenic risk is low at worst, Risk of Persistent Pulmonary Hypertension (PPH) from late
pregnancy exposure to therapeutic doses– dose relationship not characterised
Animal data largely negative in the rat, except reduced fertility at 2 X human exposure for the metabolite but we have a NOEL for the parent drug so use that
positive for malformations in at least one rabbit study. Rabbit NOAEL 45 mg/kg bw/d (?).
Strongest data is that in humans and most immediate risk appears to be PPH but need to ensure any PDE covers potential reduced fertility
Rabbit data has a high NOAEL so unlikely to influence PDE
Other Neonatal Effects
BartCrofts Scientific Services Pty Ltd
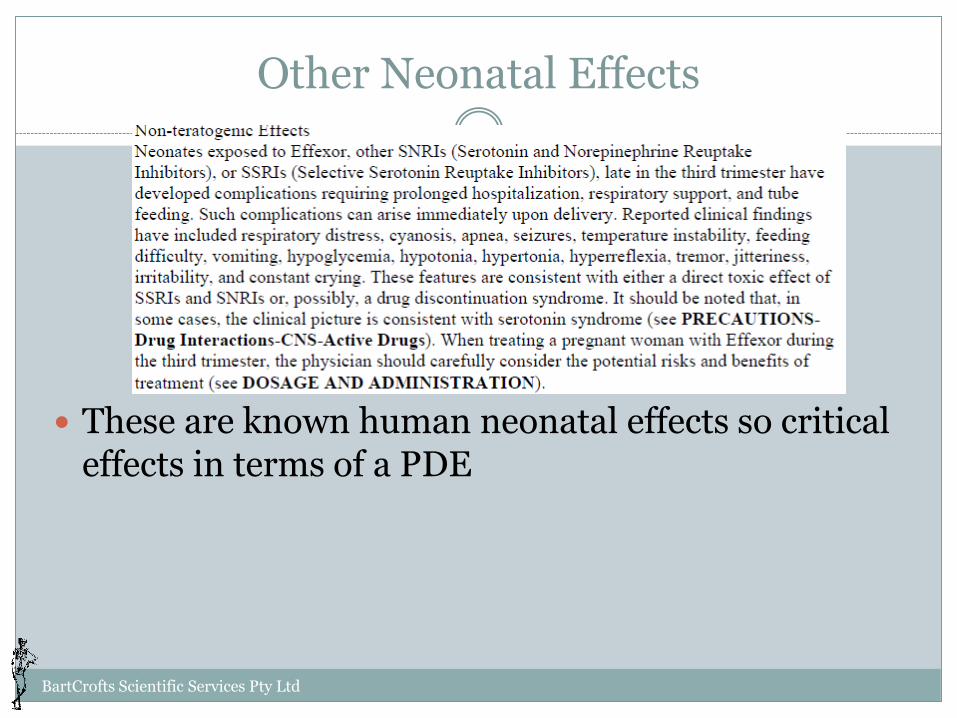
These are known human neonatal effects so critical effects in terms of a PDE

Breast feeding
BartCrofts Scientific Services Pty Ltd
This is important and needs careful consideration Ideally need data on the nature of the effect and the dose required to
produce it Unlikely to be readily available Need information on the levels in milk compared to maternal blood (higher,
lower or similar) Need to consider the mechanism
If pharmacological, which is most likely, then exposures below pharmacologically active levels unlikely to present a risk
Most of this is not available But… these effects occur at therapeutic doses so unlikely at contaminant levels –
need to check this at the end to ensure you are confident that this assumption is likely to remain true

Other Clinical Data
BartCrofts Scientific Services Pty Ltd
What side effects occurred at the lowest dose either at levels above placebo or not seen in placebo groups
Which of these are potentially serious (ie life threatening or irreversible)
Are any of these likely to be non pharmacological/idiosyncratic
Side effects at the lowest clinical trial dose of 75 mg/day appear to be pharmacological in nature and therefore unlikely to manifest at low exposures Effect Placebo 75 mg/day
Asthenia (lethargy) 3.3 16.9%
Vasodilatation 0 4.5%
Anorexia 2.2 14.6%
Nausea 14.1 32.6%
Insomnia 9.8 22.5%
Anxiety 4.3 11.2
Impotence 0 5.8

Other Clinical Data
BartCrofts Scientific Services Pty Ltd
No evidence of a strong sensitising potential
Isolated reports of sensitivity is not unusual for any drug/chemical
Cannot protect against random isolated events

First iteration of PDE - TTC
BartCrofts Scientific Services Pty Ltd
Venlafaxine is not carcinogenic or genotoxic so a Threshold of Toxicological Concern (TTC) approach would give a PDE of 1.5 µg/kg bw/day – 75 µg /person/day
Need to check that calculations from appropriate animal studies do not yield a lower value
Second Iteration PDE - Pharmacological
BartCrofts Scientific Services Pty Ltd
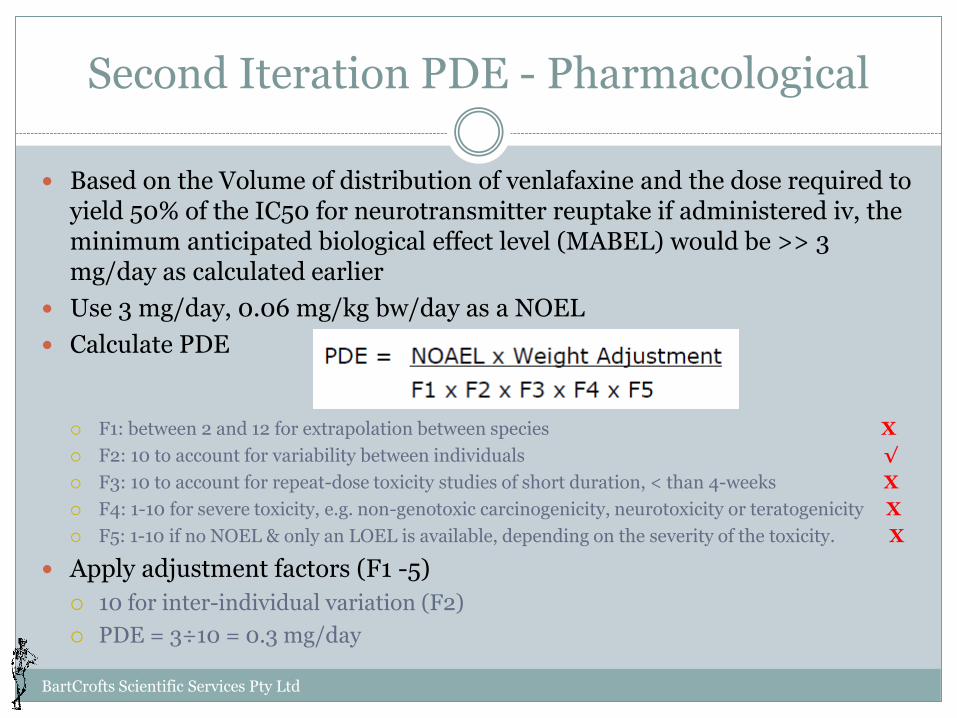
Based on the Volume of distribution of venlafaxine and the dose required to yield 50% of the IC50 for neurotransmitter reuptake if administered iv, the minimum anticipated biological effect level (MABEL) would be >> 3 mg/day as calculated earlier
Use 3 mg/day, 0.06 mg/kg bw/day as a NOEL
Calculate PDE
F1: between 2 and 12 for extrapolation between species X
F2: 10 to account for variability between individuals √
F3: 10 to account for repeat-dose toxicity studies of short duration, < than 4-weeks X
F4: 1-10 for severe toxicity, e.g. non-genotoxic carcinogenicity, neurotoxicity or teratogenicity X
F5: 1-10 if no NOEL & only an LOEL is available, depending on the severity of the toxicity. X
Apply adjustment factors (F1 -5)
10 for inter-individual variation (F2)
PDE = 3÷10 = 0.3 mg/day

Third iteration – Pharmacological –Minimum daily dose
BartCrofts Scientific Services Pty Ltd
Minimum daily therapeutic dose is 75 mg
This is a LOEL
Associated with side effects in clinical trials
? Relationship to neonatal effects at this dose
So need uncertainty factors for inter-individual variation and LOEL in place of NOEL
We’ll use 10 x 10
Calculate PDE
75/100 = 0.75 mg/day

Fourth Iteration – Toxicology and Adverse Effects
BartCrofts Scientific Services Pty Ltd
Critical effects Foetal survival – NOAEL 6.3 mg/kg bw/d Rabbit developmental study 45 mg/kg bw/d (?)
Calculate PDE Select POD - Use 6.3 mg/kg bw/d for foetal survival
Could start with the LOAEL for reduced fertility but the additional UF will yield approx the same value
Identify uncertainty factors F1 – 5 for rats to humans F2 – 10 for inter-individual variation F3 – 1 data includes life time studies F4 – 5, foetal death is a severe irreversible effect F5 – 1 we are using a NOAEL
Total UF = 250 PDE = (6.3 mg/kg bw/day * 50 kg/person)÷ 250 = 1.26 mg/person /day

Compare available PDEs
BartCrofts Scientific Services Pty Ltd
TTC Pharmacology -Receptor data
Pharmacology -Minimum Dose
Toxicology
Critical Effect Not mutagenic or carcinogenic
IC50 for neurotransmitter uptake, primary pharmacological mechanism
Minimum therapeutic dose of 75 mg/ day (25 mg tid)May be associated with neonatal effects
Reduced fertility in adult rats and foetal death, Rabbit development ?
Uncertainties Highly conservative (low)
Inter-individual variation Inter-individual variation, an effect (therapeutic ) dose
Rat to man, inter-individual, serious irreversible effect
Uncertainty Factor applied
Not applicable 10 100 (10 x 10) 250 (5 x 10 x 5)
PDE (/person/day)
75 µg 300 µg 750 µg 1260 µg
Comment Sets a lower bound Highly conservative assumptions
Simple, useful , calculation but need to check for other end points that may give lower values.tid dosing complicates the PK
Human clinical data takes precedence
Which to use ?• 300 µg/person/day is protective of toxicological endpoints and unlikely to be pharmacologically active• Should be protective of all normal subpopulations and avoids possible Cmax effects• ? Need to consider the follow on/receiving products to ensure there are not other issues that could impinge on PDE
selection
1 . S E L E C T A P P R O P R I A T E N O A E L O R P O D
2 . P L U G I N T O F O R M U L A
3 . D E T E R M I N E U F S
4 . C A L C U L A T E O E L
BartCrofts Scientific Services Pty Ltd
Worker Exposure Limits OEL

Calculate the OEL
BartCrofts Scientific Services Pty Ltd
𝑂𝐸𝐿 =𝑃𝑂𝐷
𝑚𝑔𝑑𝑎𝑦
(𝑈𝐹)(𝑆𝑆)(𝛼)(𝑣𝑜𝑙)
Where:POD = Point of Departure in dose per person per dayUF = combined uncertainty factorsSS = factor based on half life of the compoundα = bioavailability factor to convert from oral to inhalational bioavailabilityVol = volume of air breathed in a shift of work = 10 m3

Considerations for Venlafaxine OEL -1 -Pharmacological
BartCrofts Scientific Services Pty Ltd
POD is 300 µg/person per day based on a pharmacological end point and a body weight of 50kg as stipulated by EMA - however for occupational risk assessment 70 kg is used SO POD becomes 70/50 x 0.3 mg/d = 0.42 mg/d
Uncertainty and other adjustment factors F1: extrapolation between species
Data is in humans or for human receptors so no cross species adjustment
F2: variability between individuals Derivation is already based on conservative assumptions so x 5 is adequate
F3: account for repeat-dose toxicity studies of short duration, < than 4-weeks We have at least summaries for all relevant toxicological endpoints so not needed
F4: for severe toxicity, e.g. non-genotoxic carcinogenicity, neurotoxicity or teratogenicity End POD based on reversible pharmacological end point so not required
F5: if no NOEL & only an LOEL is available, depending on the severity of the toxicity. POD is based on a no effect level so not required
Half life is short so SS is 1 ie does not bio-accumulate and is quickly excreted
Oral bioavailability is high so α = 1 no need to adjust for a (potentially) greater absorption from lungs so
SO All adjustment factors combined = 5

Calculate OEL 1
BartCrofts Scientific Services Pty Ltd
𝑂𝐸𝐿 =0.42𝑚𝑔/𝑑
5𝑥10= 8 µg m-3
What if this is unachievable ?• Revisit each assumption and see if better, more accurate data is available• Consider if exposure is uniform across the working day – ie is exposure 2
hours not 8 & therefore the air breathed factor can be reduced• Can additional PPE be used during the high exposure period• Is the POD for cross contamination the appropriate one for occupational
exposure – eg if POD for PDE is based on a long term study or third trimester effects on the foetus is that applicable to your workforce ?

Calculate OEL 2 – Lowest Human Dose
BartCrofts Scientific Services Pty Ltd
OEL does not necessarily need to use the same POD as that for the PDE because the exposed population is different
Lowest human dose is 75 mg/kg bw/d Associated with only mild clinical side effects but need to consider possible reproductive effects Women in third trimester of pregnancy - ? working in pharmaceutical manufacture ? Uncertainty and other adjustment factors
F1: extrapolation between species Data is in humans
F2: variability between individuals x 5 Assuming women in late pregnancy not working with this material Children and geriatrics unlikely to be occupationally exposed
F3: account for repeat-dose toxicity studies of short duration, < than 4-weeks We have at least summaries for all relevant toxicological endpoints so not needed
F4: for severe toxicity, e.g. non-genotoxic carcinogenicity, neurotoxicity or teratogenicity POD based on reversible pharmacological effects – not required
F5: if no NOEL & only an LOEL is available, Based on a LOEL that is therapeutically sufficient for some patients x 10
Half life is short so SS is 1 ie does not bio-accumulate and is quickly excreted
Oral bioavailability is high so α = 1 no need to adjust for a (potentially) greater absorption from lungs so
SO All adjustment factors combined = 5

Calculate OEL 2
BartCrofts Scientific Services Pty Ltd
𝑂𝐸𝐿 =75𝑚𝑔/𝑑
10𝑥5𝑥10= 150 µg m-3
Which to use1. Occupationally exposed population unlikely to include the most
vulnerable1. The severely debilitated, 2. Elderly3. Neonates4. Women in late pregnancy (? Breast feeding may be an issue)
2. Use of a less conservative POD is reasonable in the absence of clear evidence of serious adverse effects
3. Side effects at the lowest therapeutic dose are mild4. Continuous exposure throughout a working day at the OEL = 1.5
mg/person -

N O W Y O U H A V E A P D E W H A T W I L L Y O U D O W I T H I T
BartCrofts Scientific Services Pty Ltd; [email protected]
38
Exposure Assessment

Over to You
BartCrofts Scientific Services Pty Ltd
The PDE is specific to an API and transferrable across manufacturing facilities
The Exposure assessment is specific to A specific manufacturing facility
Specific product manufacturing sequence
Specific to a cleaning protocol
So You can outsource or purchase the PDE determination
But the exposure assessment will require some in house consideration unless you want to have each production sequence risk assessed

Exposure Assessment
Exposure The amount of a substance an organism is exposed to through
ingestion, inhalation, or dermal application, etc.
Depending on context it may also be the Plasma or tissue concentration of a substance (esp for drugs)
Exposure in hazard characterisation Dose, route, frequency, duration
Plasma or tissue concentration
Exposure in the prospective human population ?? Source, route, magnitude (intake, absorption), duration
Specific populations: children, occupational exposure, general population
Plasma concentration (biological monitoring)
BartCrofts Scientific Services Pty Ltd; [email protected]
40

Exposure
The actual systemic exposure to a substance depends on the dose, absorption, clearance (elimination) and, for exposure of a particular tissue, tissue distribution
Plasma substance concentration is the best and most reliable determinant of systemic exposure
After oral ingestion exposure may vary & be different for Areas of the GIT Systemic sites Organs of excretion
Kidney Liver Gall bladder Urinary bladder
BartCrofts Scientific Services Pty Ltd; [email protected]
41

Determinants of exposure to a contaminating API
BartCrofts Scientific Services Pty Ltd
Quantity of API from donating product residual in equipment after clean up, or potentially mobile to follow on products
Size/volume of follow on product Both batch size and dose form size
Determines amount of contaminating API per unit dose
Eg large or small tablet Paracetamol (4 grams active per day) versus digoxin or thyroxine (100 µg/day)
Large or small volume injection Insulin versus normal saline for infusion
Frequency of administration of follow on product How many times a day ? Course of treatment – prn, a course of a week
WHO is exposed All ages and both sexes or just geriatrics, children, men only etc
May impact selection of PDE If a specific population sensitive to a critical effect that determined the PDE is not
treated with the follow-on product than a higher PDE may be available

Steps to Assess Exposure
BartCrofts Scientific Services Pty Ltd
1. Measure or estimate the maximum amount of API that could be residual on a piece of equipment or be introduced into a follow on product by whatever means
Residual material in equipment or cleaning materials Dust – ambient, fallout from surfaces, dust extractors etc Clothing of workers ????
2. For each potential follow on product estimate Maximum Amount of contaminating API per batch of follow on product Maximum amount of API contaminant per unit dose of follow on
product Maximum number of dose units per person for the most sensitive patient
sub population (children, pregnant women, patients in renal failure etc)
3. Compare theoretical maximum intake with appropriate PDE4. Determine risk management requirements

Highest risk
BartCrofts Scientific Services Pty Ltd
A low potency, high dose volume, high frequency product following on from a high potency low dose volume product
A small percentage contamination will lead to a larger exposure to contaminant because the amount of contaminated product taken is higher
Eg high potency long half life drug taken once a day as a very small tablet followed by a low potency drug in a large table taken 4 hourly

BartCrofts Scientific Services Pty Ltd
Risk Management
Extreme
High
Moderate
Low
Negligible
Nature and Severity of Effects
Potency (Min. dose) mg/dayOr PDE µg/person/day
mild, not acute, reversible
mild acute reversible
moderate not acute reversible
moderate acute reversible
severe not acute reversible
severe acute reversible
severe irreversible
Very High <0.1
High 1-10
Moderate 10-100
Low >100
Identifying High Risk APIs for Contamination ControlRisk Banding
Example of a possible in house risk banding approach to classification of API risk
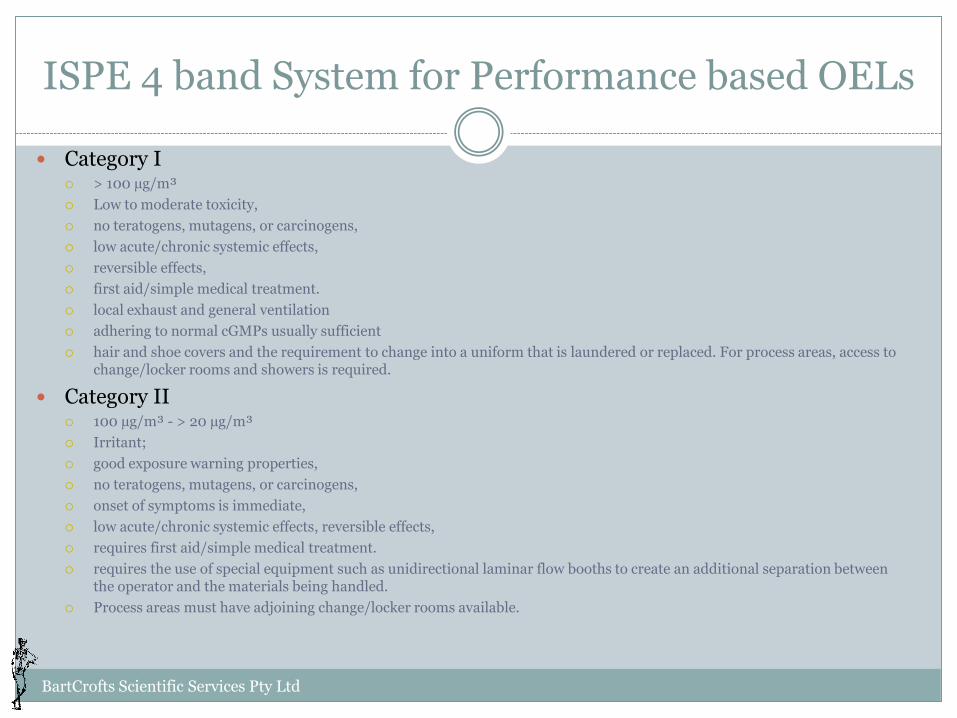
ISPE 4 band System for Performance based OELs
BartCrofts Scientific Services Pty Ltd
Category I > 100 µg/m³
Low to moderate toxicity,
no teratogens, mutagens, or carcinogens,
low acute/chronic systemic effects,
reversible effects,
first aid/simple medical treatment.
local exhaust and general ventilation
adhering to normal cGMPs usually sufficient
hair and shoe covers and the requirement to change into a uniform that is laundered or replaced. For process areas, access to change/locker rooms and showers is required.
Category II 100 µg/m³ - > 20 µg/m³
Irritant;
good exposure warning properties,
no teratogens, mutagens, or carcinogens,
onset of symptoms is immediate,
low acute/chronic systemic effects, reversible effects,
requires first aid/simple medical treatment.
requires the use of special equipment such as unidirectional laminar flow booths to create an additional separation between the operator and the materials being handled.
Process areas must have adjoining change/locker rooms available.
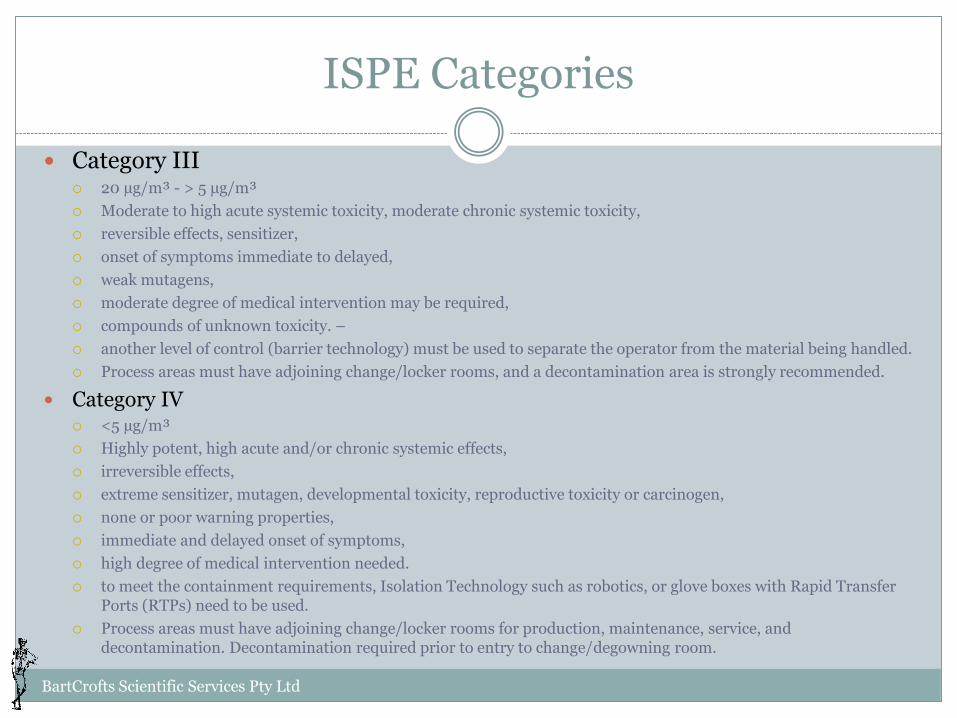
ISPE Categories
BartCrofts Scientific Services Pty Ltd
Category III 20 µg/m³ - > 5 µg/m³
Moderate to high acute systemic toxicity, moderate chronic systemic toxicity,
reversible effects, sensitizer,
onset of symptoms immediate to delayed,
weak mutagens,
moderate degree of medical intervention may be required,
compounds of unknown toxicity. –
another level of control (barrier technology) must be used to separate the operator from the material being handled.
Process areas must have adjoining change/locker rooms, and a decontamination area is strongly recommended.
Category IV <5 µg/m³
Highly potent, high acute and/or chronic systemic effects,
irreversible effects,
extreme sensitizer, mutagen, developmental toxicity, reproductive toxicity or carcinogen,
none or poor warning properties,
immediate and delayed onset of symptoms,
high degree of medical intervention needed.
to meet the containment requirements, Isolation Technology such as robotics, or glove boxes with Rapid Transfer Ports (RTPs) need to be used.
Process areas must have adjoining change/locker rooms for production, maintenance, service, and decontamination. Decontamination required prior to entry to change/degowning room.

Risk Management Options
BartCrofts Scientific Services Pty Ltd
A facility by facility consideration, for example.
Extreme Risk (eg micro dose genotoxin, teratogen, allergen,)
Dedicated, or highly product limited, facility or production line Enhanced and routinely QC/QA monitored cleaning protocols
High (eg low dose, allergen with moderate threshold, non genotoxic acute systemic toxicity, irreversible toxicity, teratogen, neurotoxin) Limited, pre designated production sequences Enhanced and QC/QA monitored cleaning protocols
Moderate (low dose, reversible but moderate acute systemic effects)
Broader pre-designated production sequences Some specific sequence constraints or exclusions Cleaning protocol validation plan
Very Low (low potency, low hazard, )
Largely unconstrained production sequences Routine cleaning validation
Negligible (low potency, low hazard, - low toxicity vitamins, food like supplements, antacids)
Unconstrained production sequences Routine cleaning validation

Unacceptable risk
Negligible risk
Acceptable Risk
Regulatory/Legal
Socio-Political
Practical
Commercial
Economic
Ethical
Potential for harm
Cost/Benefits
Factors Influencing ‘Acceptable’ Risk
BartCrofts Scientific Services Pty Ltd; [email protected]
49