
Overview Early Recognition & Significance of the … of the Problem Defining the continuum...
17
1 Kathleen M. Vollman RN, MSN, CCNS, CCRN, FCCM Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING [email protected] Dearborn, Michigan www.vollman.com Early Early Recognition & Recognition & Management of Management of Severe Sepsis Severe Sepsis © Vollman 2006 Overview Significance of the Problem Significance of the Problem Defining the continuum Defining the continuum Pathophysiologic Pathophysiologic derangements derangements Prevention Prevention Early Recognition & Resuscitation Early Recognition & Resuscitation Early Treatment Early Treatment Supportative care Supportative care Surviving Sepsis Campaign Public & Professional Awareness Evidence Based Guidelines Implementation Change Packet * Based on data for septicemia †Reflects hospital-wide cases of severe sepsis as defined by infection in the presence of organ dysfunction 1 Sands KE, et al. JAMA 1997;278:234-40. 2 National Vital Statistics Reports. 2005. 3 Angus DC, et al. Crit Care Med 2001;29:1303-10. Severe Sepsis: A Significant Healthcare Challenge Major cause of morbidity and mortality Major cause of morbidity and mortality worldwide worldwide Leading cause of death in noncoronary Leading cause of death in noncoronary ICU (US) ICU (US) 1 10th leading cause of death overall (US) 10th leading cause of death overall (US) 2 * More than 750,000 cases of severe sepsis More than 750,000 cases of severe sepsis in the US annually in the US annually 3 In the US, more than 500 patients die In the US, more than 500 patients die of severe sepsis daily of severe sepsis daily 3† * Calculated data based on information compiled from the American Heart Association, American Cancer Society, National Center for Health Statistics and the US Census Bureau (1995-1999). † Severe sepsis mortality rates range from 28%-50% (79/100,000 to 141/100,000 population). Severe Sepsis Is Common* Rate per 100,000 Population 0 50 100 150 200 250 300 Severe Sepsis† Stroke Breast Cancer Lung Cancer Incidence Mortality Surviving Sepsis Campaign Public & Professional Awareness Evidence Based Guidelines Implementation Change Packet
Transcript of Overview Early Recognition & Significance of the … of the Problem Defining the continuum...

1
Kathleen M. Vollman RN, MSN, CCNS, CCRN, FCCMClinical Nurse Specialist/Educator/Consultant
ADVANCING [email protected]
Dearborn, Michiganwww.vollman.com
Early Early Recognition & Recognition & Management of Management of Severe SepsisSevere Sepsis
© Vollman 2006
Overview
Significance of the ProblemSignificance of the ProblemDefining the continuumDefining the continuumPathophysiologicPathophysiologic derangementsderangementsPreventionPreventionEarly Recognition & ResuscitationEarly Recognition & ResuscitationEarly Treatment Early Treatment
Supportative careSupportative care
Surviving Sepsis Campaign
Public & ProfessionalAwareness
Evidence BasedGuidelines
ImplementationChange Packet
* Based on data for septicemia †Reflects hospital-wide cases of severe sepsis as defined by infection in the presence of organ dysfunction
1 Sands KE, et al. JAMA 1997;278:234-40.2 National Vital Statistics Reports. 2005.3 Angus DC, et al. Crit Care Med 2001;29:1303-10.
Severe Sepsis: A Significant Healthcare Challenge
Major cause of morbidity and mortality Major cause of morbidity and mortality worldwideworldwide
Leading cause of death in noncoronary Leading cause of death in noncoronary ICU (US)ICU (US)11
10th leading cause of death overall (US)10th leading cause of death overall (US)22**More than 750,000 cases of severe sepsis More than 750,000 cases of severe sepsis in the US annuallyin the US annually33
In the US, more than 500 patients dieIn the US, more than 500 patients dieof severe sepsis dailyof severe sepsis daily33††
*Calculated data based on information compiled from the American Heart Association, American Cancer Society, National Center for Health Statistics and the US Census Bureau (1995-1999).† Severe sepsis mortality rates range from 28%-50% (79/100,000 to 141/100,000 population).
Severe Sepsis Is Common*
Rat
e pe
r 10
0,00
0 P
opul
atio
n
0
50
100
150
200
250
300
Severe Sepsis† Stroke Breast Cancer Lung Cancer
IncidenceMortality
Surviving Sepsis Campaign
Public & ProfessionalAwareness
Evidence BasedGuidelines
ImplementationChange Packet

2
Begin Proven Care Strategies
Early appropriate antibiotic useEarly appropriate antibiotic useEGDT: Early GoalEGDT: Early Goal--Directed TherapyDirected TherapyLowLow--tidal volume ventilation/ARDS/ALItidal volume ventilation/ARDS/ALIXigrisXigris if not contraindicatedif not contraindicatedTight Tight glycemicglycemic controlcontrolLowLow--dose steroid administration for refractory dose steroid administration for refractory septic shock particularly in patients with relative septic shock particularly in patients with relative adrenal insufficiencyadrenal insufficiency
Implementation Through Proven Implementation Through Proven Change StrategiesChange Strategies
IHI/VHA Change StrategyCare BundlesCare Bundles
Grouping of care elements Grouping of care elements for particular symptoms, for particular symptoms, procedures or treatmentsprocedures or treatmentsStrong science, good Strong science, good methodology, poor processmethodology, poor processBundle characteristicsBundle characteristics
Solid evidenceSolid evidenceRelatively easy & Relatively easy & inexpensiveinexpensiveIndividual components Individual components defined welldefined wellProcess not defined wellProcess not defined well
Bone RC, et al. Chest 1992;101:1644-55.
Sepsis: 1991 ACCP / SCCM Sepsis: 1991 ACCP / SCCM DefinitionsDefinitions
InfectionInfectionInflammatory response to microorganisms, orInflammatory response to microorganisms, orInvasion of normally sterile tissuesInvasion of normally sterile tissues
Systemic Inflammatory Response Syndrome Systemic Inflammatory Response Syndrome (SIRS)(SIRS)
Two or more of the following:Two or more of the following:Core temperature Core temperature >38>38°°C or <36C or <36°°C (>100.4C (>100.4°°F or F or
<96.8<96.8°°F)F)Elevated heart rate (>90 beats/min)Elevated heart rate (>90 beats/min)Respiratory rate >20 breaths/min or PaCORespiratory rate >20 breaths/min or PaCO22 <32 mm <32 mm
Hg or mechanical ventilation for acute respiratory Hg or mechanical ventilation for acute respiratory processprocess
WBC count >12,000/mmWBC count >12,000/mm33 or <4,000/mmor <4,000/mm33 or or >10% immature >10% immature neutrophilsneutrophils
Signs & Symptoms of Sepsis
31
PlateletsBandsSkin perfusionUrine output
Skin mottlingPoor capillary refillHyperglycemiaPurpura/petechia
ChillsAlteration in LOCTachypneaUnexplained metabolicacidosis
Heart rateAltered blood pressure
Levy M, et al. Crit Care Med 2003;31:1250-6.
Bone RC, et al. Chest 1992;101:1644-55.
SepsisSepsisKnown or suspectedKnown or suspectedinfection, plusinfection, plus≥≥2 SIRS criteria2 SIRS criteria
Severe SepsisSevere SepsisSepsis plusSepsis plus≥≥1 1 organ dysfunctionorgan dysfunction
Septic ShockSeptic ShockSepsis withSepsis withHypotension despite Hypotension despite fluid resuscitation, fluid resuscitation, andandPerfusion Perfusion abnormalitiesabnormalities
Severe SepsisSevere SepsisSepsisSepsisSIRSSIRSInfection/Infection/TraumaTrauma Severe SepsisSevere SepsisSepsisSepsisSIRSSIRSInfection/Infection/TraumaTrauma
Sepsis: 1991 ACCP / SCCM Sepsis: 1991 ACCP / SCCM Definitions (cont)Definitions (cont)
Identifying Acute Organ Dysfunction as a Marker of Severe Sepsis
TachycardiaSBP<90mmHgMAP < 70mmHg (despite fluid)Need for Vasopressors
Unexplained metabolic acidosis•pH<7.30 or Base deficit > 5.0 mEq/l•Lactate > 1.5 times upper normal
PaO2/FiO2 ≤200 if lung only dysfunction/site of infectionPaO2/FiO2 ≤250 with other organ dysfunction/lung not site of infection UO >0.5 ml/kg per hr
(despite fluid)
Platelets <80,000/mm3
Decline in platelet count of 50% over 3 days
RespiratoryRespiratory
MetabolicMetabolic
CardiovascularCardiovascular
RenalRenal
HematologicHematologic

3
PaO2/FiO2 Ratio
User friendly toolUser friendly toolCrude assessment of the Crude assessment of the severity of lung injuryseverity of lung injuryUsed in the definition of Used in the definition of ALI/ARDSALI/ARDS
ALI: ALI: << 300 regardless 300 regardless of PEEPof PEEPARDS: ARDS: << 200 200 regardless of PEEPregardless of PEEP
PaO2 = 70 torrPaO2 = 70 torrFiO2 = 60% or .60FiO2 = 60% or .60P/F Ratio = 70/.60P/F Ratio = 70/.60Answer: 117Answer: 117
© Vollman 2001
Identifying Acute Organ Dysfunction as a Marker of Severe Sepsis
TachycardiaSBP<90mmHgMAP < 70mmHg (despite fluid)Need for Vasopressors
Unexplained metabolic acidosis•pH<7.30 or Base deficit > 5.0 mEq/l•Lactate > 1.5 times upper normal
PaO2/FiO2 ≤200 if lung only dysfunction/site of infectionPaO2/FiO2 ≤250 with other organ dysfunction/lung not site of infection UO >0.5 ml/kg per hr
(despite fluid)
Platelets <80,000/mm3
Decline in platelet count of 50% over 3 days
RespiratoryRespiratory
MetabolicMetabolic
CardiovascularCardiovascular
RenalRenal
HematologicHematologic
Homeostasis
Homeostasis Is Unbalanced in Severe Sepsis
Carvalho AC, Freeman NJ. J Crit Illness 1994;9:51-75.Kidokoro A, et al. Shock 1996;5:223-8.Vervloet MG, et al. Semin Thromb Hemost 1998;24:33-44.
COAGULATIONCOAGULATIONINFLAMMATIONINFLAMMATION
FIBRINOLYSISFIBRINOLYSIS
SEVERE SEPSIS PATHOPHYSIOLOGY
Microvascular dysfunction↑ Inflammation↑ Coagulation↓ Fibrinolysis
Hypoperfusion/hypoxiaMicrovascular thrombosisEndothelial dysfunction
Organ dysfunctionGlobal tissue hypoxiaDirect tissue damage
→ →
1. www.opsimaging.net. Accessed April 2004. 2. Spronk PE, et al. Lancet. 2002;360:1395-1396.
MICROCIRCULATION: SUBLINGUAL BLOOD FLOW
Healthy Healthy VolunteerVolunteerBP: 120/80 mm HgBP: 120/80 mm HgSaOSaO22: 98%: 98%
Septic Shock Septic Shock Patient Patient
Resuscitated with fluids and Resuscitated with fluids and dopaminedopamine
HR: 82 BPMHR: 82 BPMBP: 90/35 mmHgBP: 90/35 mmHgSaOSaO22: 98%: 98%CVP: 25 mmHgCVP: 25 mmHg
Pathophysiologic Characteristics in Severe Sepsis
Maldistribution of blood flowMaldistribution of blood flow
Imbalance of oxygen supply & demandImbalance of oxygen supply & demand
Metabolic alterations & activation of the Metabolic alterations & activation of the stress responsestress response
© Vollman 2001

4
Maldistribution of Blood FlowMechanical obstructionMechanical obstruction
MicroMicro--emboliemboliIncreased blood viscosityIncreased blood viscosityCompressionCompression
Systemic & local mediator & Systemic & local mediator & ion influenceion influence
Constriction vs. dilationConstriction vs. dilationLoss of regulatory Loss of regulatory activities/endothelial cell injuryactivities/endothelial cell injury
Reactive hyperemiaReactive hyperemiaAnticoagulationAnticoagulation
Imbalance of Oxygen Supply & Demand
SUPPLY
DEMAND
O 2 Supply/Demand Compensatory Mechanisms
Improve pulmonary gas exchangeImprove pulmonary gas exchange
Increase oxygen deliveryIncrease oxygen delivery
Alter the distribution of blood flowAlter the distribution of blood flow
O2 Supply Debt
Metabolic Alterations & The Stress Response
Initiation of the Stress ResponseInitiation of the Stress Response
Sympathetic Nervous Sympathetic Nervous System ActivationSystem Activation
Hypothalamus Activation
Metabolic Alterations & The Stress Response
SNS ActivationSNS ActivationGut hypothesisGut hypothesis↑↑ BMRBMRInhibition of Inhibition of insulin secretioninsulin secretionInhibition of Inhibition of glucose uptake glucose uptake by the tissuesby the tissues
Hypothalamus Hypothalamus ActivationActivation
Adrenal cortex Adrenal cortex stimulationstimulationChanges in Changes in carbohydrate, protein carbohydrate, protein & fat metabolism & fat metabolism resulting in resulting in ↑↑ glucose glucose concentrationconcentration
5
Except on few occasions, Except on few occasions, the patient appears to die from the patient appears to die from the body's response to infection the body's response to infection rather than from it."rather than from it."
Sir William Osler – 1904The Evolution of Modern Medicine
Cornerstones of Management
PreventionPreventionEarly recognition & resuscitationEarly recognition & resuscitationEarly antibiotic administrationEarly antibiotic administrationEarly resuscitationEarly resuscitationTransport to appropriate care area for early Transport to appropriate care area for early treatment using evidence based caretreatment using evidence based care
PREVENTING THE INVASION
Oral careOral care
Line care Line care
HandwashingHandwashing
HOBHOB
Michigan Keystone Prevention of Infection (127 ICU’s)
VAPVAP’’ssMarch 2004 March 2004 5.44/per 1000 ventilator days5.44/per 1000 ventilator days
July 2004 July 2004 5.36/per 1000 ventilator days5.36/per 1000 ventilator days
December 2004 December 2004 4.14 per/1000 ventilator days4.14 per/1000 ventilator days
1/3 hospitals 5 months with no 1/3 hospitals 5 months with no VAPVAP’’ssPrevented 73 deathsPrevented 73 deathsCost saved $2,000,000.00Cost saved $2,000,000.00
March 14th, 2005 Keystone Meeting
Michigan Keystone Prevention of Infection (103 ICU’s data reported)
BSIBSI’’ssJune 2004/BaselineJune 2004/BaselineMedian 2.7 (mean 7.7) /per 1000 catheter Median 2.7 (mean 7.7) /per 1000 catheter days days
At 18 monthsAt 18 monthsMedian 0 (mean 1.4) per/1000 catheter Median 0 (mean 1.4) per/1000 catheter daysdays
66% reduction using the BSI bundle concept66% reduction using the BSI bundle concept
Pronovost P et al N Engl J of Med 2006;355(26):2725-32
EARLY MANAGEMENT
Early RecognitionEarly Recognition/Screening/Screening
ICU/Additional EvidenceICU/Additional EvidenceBased TherapiesBased Therapies
Source Control/Source Control/
Early AntibioticsEarly Antibiotics
Prompt/Aggressive Prompt/Aggressive ResuscitationResuscitation
6
Screening for Severe Sepsis
Screen for Severe SepsisYes
No
Standard careStandard care
Monitor Q24H floor; Monitor every shift
in the ICU
Surviving Sepsis Guidelines
Confirm Diagnosis of Severe Sepsis
“Triggers” for Identifying Severe SepsisComputerized Alert Message
Manual Alert Message
Standard Procedure
Location/Trigger Type
•Upon pharmacy entry of vasopressor/antibiotic
•Upon withdrawal of med from Automated Dispensing Cabinet
•Upon scanning of medication at bedside
Concurrent coder or case manager
•Order sheets antibiotic/vasopressor
•Change in lab values (lactate)
•Triage: Criteria-Based Early Response
•Lactate as a screen
•Change in lactate
Emergency Department
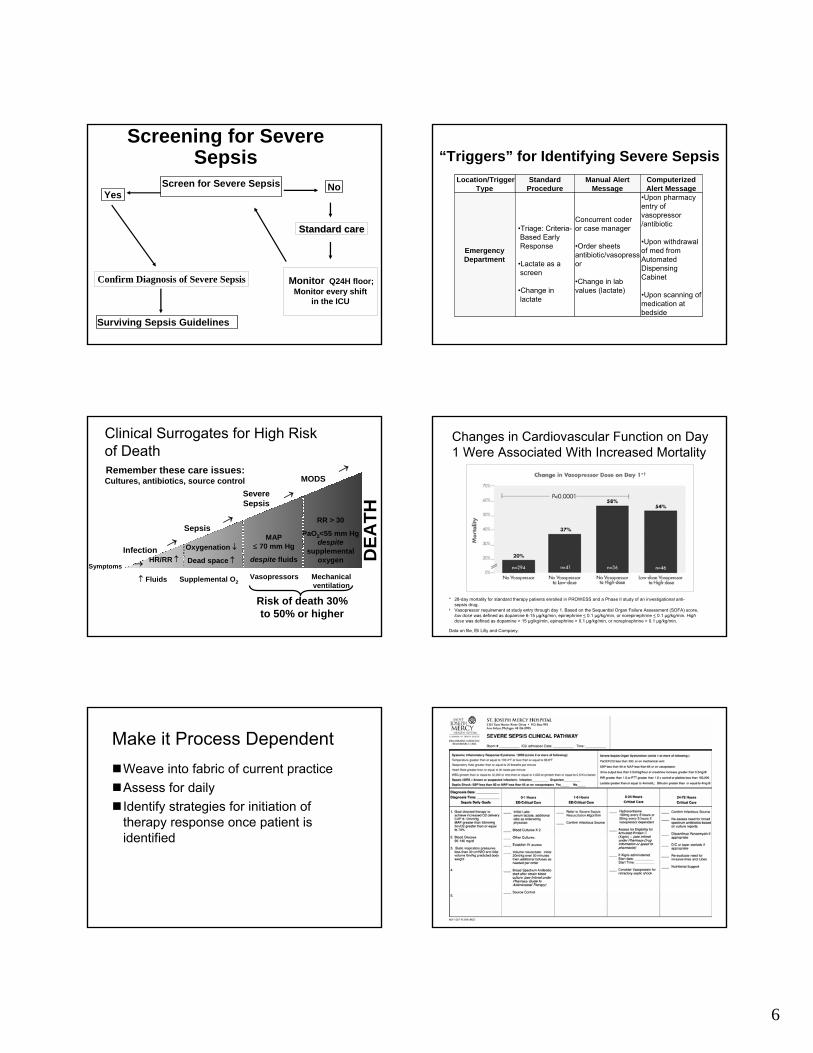
Remember these care issues:Remember these care issues:
↑↑ FluidsFluids Supplemental O2
HR/RR ↑Oxygenation ↓
Dead space ↑
MAP ≤ 70 mm Hg
despite fluids
RR > 30
PaO2<55 mm Hg despite
supplemental oxygen
→
Risk of death 30% to 50% or higher
→Symptoms
Cultures, antibiotics, source control
Vasopressors Mechanical ventilation
→
→
→
Infection
Sepsis
SevereSepsis
MODS
DEA
TH
Clinical Surrogates for High Risk of Death
Changes in Cardiovascular Function on Day 1 Were Associated With Increased Mortality
* 28-day mortality for standard therapy patients enrolled in PROWESS and a Phase II study of an investigational anti-sepsis drug.
† Vasopressor requirement at study entry through day 1. Based on the Sequential Organ Failure Assessment (SOFA) score, low dose was defined as dopamine 6-15 µg/kg/min, epinephrine < 0.1 µg/kg/min, or norepinephrine < 0.1 µg/kg/min. High dose was defined as dopamine > 15 µg/kg/min, epinephrine > 0.1 µg/kg/min, or norepinephrine > 0.1 µg/kg/min.
Data on file, Eli Lilly and Company.
Make it Process DependentWeave into fabric of current practiceWeave into fabric of current practiceAssess for dailyAssess for dailyIdentify strategies for initiation of Identify strategies for initiation of therapy response once patient is therapy response once patient is identifiedidentified

7
Reaching Outside The ICU: Early Recognition Models
Shock Program Shock Program MET TeamMET TeamCritical Care Nurse Consultant Critical Care Nurse Consultant ServiceService
Case Study: Early Identification and Intervention
Initial VS:Initial VS:Temp: 101.6 FTemp: 101.6 FRR: 31RR: 31HR: 109, HR: 109, atrialatrial fib with occasional SVTfib with occasional SVTB/P: 79/51B/P: 79/512L of O2, O2 sat of 96%2L of O2, O2 sat of 96%
Positive Screen for severe sepsis:Positive Screen for severe sepsis:SIRS: HR >90; RR> 20; Temp > 38SIRS: HR >90; RR> 20; Temp > 38Organ dysfunction: SBP<90mmHgOrgan dysfunction: SBP<90mmHg
Early TreatmentEarly TreatmentIV startedIV startedReceived 500cc NS bolus over 30 minutesReceived 500cc NS bolus over 30 minutesLabs drawnLabs drawn
Advanced Treatment GuidelinesDepartment of Emergency Services
PURPOSE:PURPOSE: To provide prompt, consistent nursing interventions for the pTo provide prompt, consistent nursing interventions for the patient with SIRS or atient with SIRS or sepsis prior to physician evaluation, to enable rapid diagnosis sepsis prior to physician evaluation, to enable rapid diagnosis and slow the and slow the progression of illness. progression of illness.
IMPLEMENTATION:IMPLEMENTATION:The nursing staff may implement these interventions for patientsThe nursing staff may implement these interventions for patients who present with who present with all threeall threeof the following criteria. The nurse should take into consideraof the following criteria. The nurse should take into consideration the patienttion the patient’’s baseline vital s baseline vital signs when evaluating as a potential candidate. Also, these intsigns when evaluating as a potential candidate. Also, these interventions should not conflict erventions should not conflict with the patient/family goals. (i.e. DNR, comfort care)with the patient/family goals. (i.e. DNR, comfort care)
1.1. Clinical suspicion of systemic infection Clinical suspicion of systemic infection
2.2. At least two of the following:At least two of the following:–– Hyperthermia :Temperature greater than 38 Hyperthermia :Temperature greater than 38 °°C (100.4 C (100.4 °°F)F)–– Hypothermia: Temperature less than < 36 Hypothermia: Temperature less than < 36 °°C (96.8 C (96.8 °°F)F)–– Tachycardia Pulse > 90 Tachycardia Pulse > 90 bpmbpm–– TachypneaTachypnea RR > 20RR > 20
3. 3. SBP < 90SBP < 90
Patients who meet all three criteria will be placed in a room imPatients who meet all three criteria will be placed in a room immediately after mediately after consultation with charge nurse and/or attending.consultation with charge nurse and/or attending.
Advanced Treatment GuidelinesDepartment of Emergency Services
TREATMENTTREATMENT
1.1. Notify Physician Notify Physician 2.2. Place Intermittent Infusion Device (large bore catheter) in 2 Place Intermittent Infusion Device (large bore catheter) in 2
sitessites3.3. Place on cardiac monitorPlace on cardiac monitor4.4. Continuous pulse Continuous pulse oximetryoximetry5.5. Vital signs every 15 minutesVital signs every 15 minutes6.6. Administer oxygen at 2 L/min per nasal Administer oxygen at 2 L/min per nasal cannulacannula if O2 sat <92%if O2 sat <92%7.7. Draw and Draw and hold hold blood cultures x 2, Type & screenblood cultures x 2, Type & screen8.8. Draw and Draw and holdhold tube for serum lactate and place ontube for serum lactate and place on iceice..9.9. Collect CCMS urine sample in the nonCollect CCMS urine sample in the non--menstruating patient. menstruating patient.
Send for Urinalysis and urine culture.Send for Urinalysis and urine culture.10.10. Portable CXRPortable CXR11.11. Intravenous hydrationIntravenous hydration: Administer 500ml bolus of normal : Administer 500ml bolus of normal
saline over 15 minutes.saline over 15 minutes.
Case Study: Early Identification and Intervention
Labs:Labs:WBC: 11.5WBC: 11.5HgbHgb: 15.8: 15.8HctHct: 47.4: 47.4BUN: 28 Creatinine:1.6BUN: 28 Creatinine:1.6Glucose:158Glucose:158BNP:78 (moderate CHF); troponin:0.03BNP:78 (moderate CHF); troponin:0.03Lactic acid: 4.6Lactic acid: 4.6U/A: positive for bacteriaU/A: positive for bacteriaScvO2: 49.1%ScvO2: 49.1%Blood cultures X 2 drawnBlood cultures X 2 drawn
Case Study: Early Identification and Intervention
CXR:CXR: RLL consolidationRLL consolidation
Additional Interventions:Additional Interventions:Broad spectrum antibiotics given within 3 hours of Broad spectrum antibiotics given within 3 hours of presentationpresentationLactic acid >4mmol/L so CVP insertedLactic acid >4mmol/L so CVP insertedFluid resuscitation continued Fluid resuscitation continued Foley insertedFoley inserted
Received total of Received total of 3 Liters of NS3 Liters of NS during 3 hour ED during 3 hour ED staystayED diagnosis:ED diagnosis: Severe sepsis, Pneumonia , UTI, Severe sepsis, Pneumonia , UTI, CHFCHFTransferred to MICUTransferred to MICU

8
Case Study: Early Identification and Intervention--MICU
Additional Interventions: Day 1Additional Interventions: Day 1Continued fluid resuscitationContinued fluid resuscitation——7 L7 LLow dose Low dose vasopressorvasopressorLow dose steroidsLow dose steroidsRemained on 2 L nasal Remained on 2 L nasal canulacanulaNot eligible for Not eligible for XigrisXigris (renal failure resolved and (renal failure resolved and vasopressorvasopressor weaned off within 12hours after ICU weaned off within 12hours after ICU admission)admission)
Labs:Labs:ScvO2: 72.8 (after resuscitation)ScvO2: 72.8 (after resuscitation)Lactic acid: 4 hours after ICU admission: 6.7Lactic acid: 4 hours after ICU admission: 6.7
12 hours after ICU admission: 3.012 hours after ICU admission: 3.0
Bleeding is most common adverse effect associated with Xigris therapy, please see important safety information in this presentation
Case Study: Early Identification and Intervention
Day 2:Day 2:VasopressorVasopressor weaned offweaned offLasixLasix to assist with fluid mobilizationto assist with fluid mobilizationLactic acid: 3.0Lactic acid: 3.0
Day 3:Day 3:Lactic acid: 1.2Lactic acid: 1.2O2 sat 93% on room airO2 sat 93% on room airCentral line discontinuedCentral line discontinued
Transferred to intermediate care on Day 3Transferred to intermediate care on Day 3Discharged from hospital on day 7Discharged from hospital on day 7
“Triggers” for Identifying Severe SepsisComputerized Alert
MessageManual Alert MessageStandard Procedure
Location/Trigger Type
• Upon pharmacy entry of vasopressor/antibiotic
• In note field on computerized MAR
• In note field of vasopressor computerized label
• Upon withdrawal of med from Automated Dispensing Cabinet
• Upon scanning of medication at bedside
• From concurrent coder or case manager
• Nurse MAR reviewantibiotic/vasopressor)
• Change in lab values (lactate or surrogate)
• Place on all ICU charts, daily
• Upon admission• By nurse at shift
change• Change in lactate or
surrogate• During MD, RN,
RPh, round• Criteria-Based Early
Response
ICU
“Triggers” for Identifying Severe SepsisComputerized Alert
MessageManual Alert
MessageStandard
ProcedureLocation/Trigger
Type
• Upon pharmacy entry of antibiotic
• In note field on computerized MAR
• In note field of vasopressor computerized label
• Upon withdrawal of med from Automated Dispensing Cabinet
• Upon scanning of medication at bedside
•From concurrent coderor case manager•Nurse MAR reviewfor antibiotic•Change in patient hemodynamics
•Need to mobilize MET•Change in lab values (e.g. elevated WBC, decreased platelet count)
• Upon admission• During MD, RN,
RPh, rounds• Criteria-Based
Early Response teams
Patient Care Units
Seeking Best Practices for Identifying Seeking Best Practices for Identifying Severe Sepsis PatientsSevere Sepsis Patients
9
EARLY MANAGEMENT
Early RecognitionEarly Recognition/Screening/Screening
ICU/Additional EvidenceICU/Additional EvidenceBased TherapiesBased Therapies
Source Control/Source Control/
Early AntibioticsEarly Antibiotics
Prompt/Aggressive Prompt/Aggressive ResuscitationResuscitation
Early Treatment: Source Control(grade E: case series, uncontrolled studies, expert opinion)
Appropriate cultures including 2 blood Appropriate cultures including 2 blood cultures prior to initiation of antibioticscultures prior to initiation of antibioticsEarly aggressive surgical intervention Early aggressive surgical intervention Early fracture fixationEarly fracture fixation
Start intravenous antibiotic therapy within the Start intravenous antibiotic therapy within the first hour of recognition of severe sepsis after first hour of recognition of severe sepsis after obtaining appropriate cultures obtaining appropriate cultures Grade EGrade E
Empirical choice of antimicrobials should include Empirical choice of antimicrobials should include one or more drugs with activity against likely one or more drugs with activity against likely pathogens, both bacterial or fungal pathogens, both bacterial or fungal Grade DGrade D
–– Penetrate presumed source of infectionPenetrate presumed source of infection–– Guided by susceptibility patterns in the community Guided by susceptibility patterns in the community
and hospitaland hospital–– Continue broad spectrum therapy until the Continue broad spectrum therapy until the
causative organism and its susceptibilities are causative organism and its susceptibilities are defineddefined Kreger BE. Am J Med 1980;68:344-355.
Ibrahim EH. Chest 2000;118:146-155. Hatala R. Ann Intern Med 1996;124-717-725.
Antibiotic Therapy
Dellinger, et. al. Crit Care Med 2004, 32: 858-873.
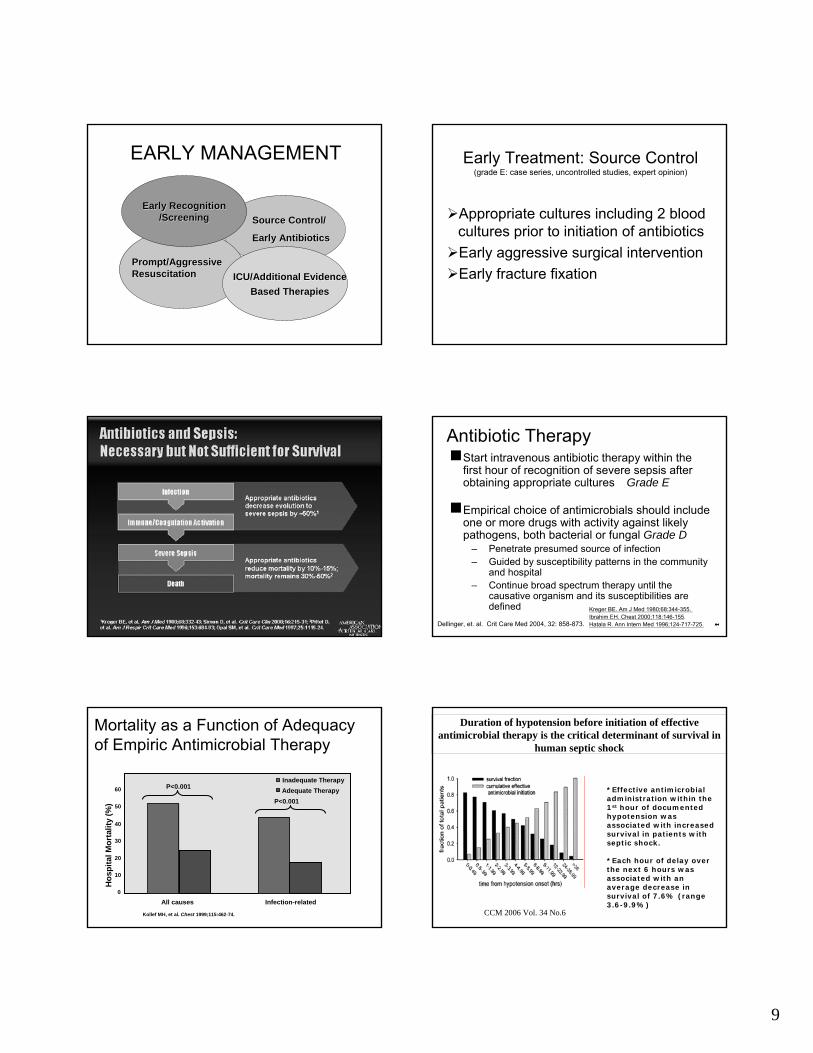
Mortality as a Function of Adequacyof Empiric Antimicrobial Therapy
Hos
pita
l Mor
talit
y (%
)
All causes Infection-related
P<0.001Inadequate TherapyAdequate Therapy60
50
40
30
20
10
0
P<0.001
Kollef MH, et al. Chest 1999;115:462-74.
Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in
human septic shock
*Effective antimicrobial administration within the 1st hour of documented hypotension was associated with increased survival in patients with septic shock.
*Each hour of delay over the next 6 hours was associated with an average decrease in survival of 7.6% (range 3.6-9.9%)
CCM 2006 Vol. 34 No.6

10
Antibiotic ChallengesAppropriate selection – determined based upon consensus guidelines and pathogen sensitivity at your institution
Timing issuesHow? Delivery time challenges of antibioticsPossible solutions
Sepsis Resuscitation Bundle(To be accomplished as soon as possible over first 6 hours):
1. Serum lactate measured.2. Blood cultures obtained prior to antibiotic administration.3. From the time of presentation, broad-spectrum antibiotics administered within 3 hours for ED admissions and 1 hour for non-ED ICU admissions.4. In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl):a) Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent*).b) Apply vasopressors for hypotension not responding to initial fluid resuscitation tomaintain mean arterial pressure (MAP) > 65 mm Hg.5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/orlactate > 4 mmol/L (36 mg/dl):a) Achieve central venous pressure (CVP) of > 8 mm Hg.b) Achieve central venous oxygen saturation (ScvO2) of > 70%.**
““Early Goal Directed TherapyEarly Goal Directed Therapy””
PROMPT AGGRESSIVE PROMPT AGGRESSIVE RESUSCITATIONRESUSCITATION
Early Goal Directed Therapy
Early GoalEarly Goal--Directed Directed Therapy (EGDT)Therapy (EGDT)
Continuous ScvO2 Continuous ScvO2 monitoring & monitoring & txtx with fluids, with fluids, blood, blood, inotropesinotropes &/or &/or vasoactivesvasoactives to maintain:to maintain:
ScvO2 ScvO2 >>70%, SaO2 70%, SaO2 >>93%, 93%, HctHct >> 30%, CI/VO230%, CI/VO2
CVP CVP >> 88--1212MAP MAP >> 6565UO UO >> .5ml/kg/hr.5ml/kg/hr
Standard TherapyStandard TherapyCVP CVP >> 88--1212MAP MAP >> 6565UO UO >>.5ml/kg/hr.5ml/kg/hr
Rivers et. al. N Engl J Med. 2001;345;19:1368-1377.
Methodology: 263 severe sepsis patients
49.2%
33.3%
0
10
20
30
40
50
60
Standard Therapyn=133
EGDTn=130
P = 0.01*
*Key difference was in sudden CV collapse, not MODS
28-day Mortality
Rivers E. N Engl J Med 2001;345:1368-77.
Early Goal-Directed Therapy Results NNT = 7-8
Evidence of Early Goal Directed Therapy
First 6 hours of EGDT:First 6 hours of EGDT:1500cc more fluid 1500cc more fluid 64% received blood products vs. 64% received blood products vs.
18.5%18.5%13.7% received 13.7% received inotropesinotropes vs. 0.8%vs. 0.8%No difference in No difference in vasopressorvasopressor use or use or
mechanical ventilationmechanical ventilationRivers et. al. N Engl J Med. 2001;345;19:1368-1377.

11
Resuscitation should begin as soon as severe sepsis or sepsis induced tissue hypoperfusion is recognizedElevated Serum lactate identifies tissue hypoperfusion in patients at risk who are not hypotensive
Rivers E. N Engl J Med 2001;345:1368-77.
Initial Resuscitation (Grade B)
Dellinger, et. al. Crit Care Med 2004, 32: 858-873.
-
EGDT: RevisitedOutcomes Survey: 12 programsOutcomes Survey: 12 programs1,298 patients with severe sepsis and septic 1,298 patients with severe sepsis and septic shockshockTreated with EGDT and/or the sepsis bundlesTreated with EGDT and/or the sepsis bundlesPre implementation mortality: 44.8 Pre implementation mortality: 44.8 ++ 7.8%7.8%Post implementation mortality: 24.5 Post implementation mortality: 24.5 ++ 5.5 %5.5 %
Otero RM. et al Chest; 2006:130:1579-1595
20.3% Reduction in Mortality, NNT 5
EGDT: RevisitedCost Effectiveness of EGDT/Guideline Based Cost Effectiveness of EGDT/Guideline Based Care (ED, ICU or RRT initiated)Care (ED, ICU or RRT initiated)
23.4% reduction in hospital cost (incorporated 23.4% reduction in hospital cost (incorporated additional training, personnel and equipment) additional training, personnel and equipment) Huang et al Huang et al CritCrit Care Med 2003:7(suppl S116)Care Med 2003:7(suppl S116)
Henry Ford Hospital: Henry Ford Hospital: 4 day 4 day Hospital LOS Hospital LOS (32.6% reduction)(32.6% reduction)Reduction in hospital charges from $135,199 Reduction in hospital charges from $135,199 to $82,233 (39.2% reduction) to $82,233 (39.2% reduction) TrzeciakTrzeciak S et al, Chest S et al, Chest 2006:129:2252006:129:225--232232
Otero RM. et al Chest; 2006:130:1579-1595
Challenges to Adequate Fluid Resuscitation
How does your institution do fluid boluses?Is low urine output still measured by < 30cc/hr?Are resuscitation goals based on CVP, MAP & UO and do your practitioners still believe this is adequate?

12
Challenges to Adequate Fluid Resuscitation
What are your average wait times for an ICU bed?Will you be able to shorten those?Initiation of EGDT must be earlyDo you routinely measure lactate, and how?What resources and education/training is required? (catheter, fluid administration per kg & dobutamine use)
EARLY MANAGEMENT BUNDLE
Early RecognitionEarly Recognition
ICU/Additional EvidenceICU/Additional EvidenceBased TherapiesBased Therapies
Source Control/Source Control/
Early AntibioticsEarly Antibiotics
Prompt/Aggressive Prompt/Aggressive ResuscitationResuscitation
Intravenous corticosteroids are Intravenous corticosteroids are recommended in patients with septic shock who, recommended in patients with septic shock who, despite adequate fluid therapy, require despite adequate fluid therapy, require vasopressor therapy to maintain adequate blood vasopressor therapy to maintain adequate blood pressurepressure
Administer intravenous hydrocortisone Administer intravenous hydrocortisone 200200--300 mg/day for 7 days in three or four 300 mg/day for 7 days in three or four divided doses by continuous infusiondivided doses by continuous infusionShown to reduce mortality rate and reverse Shown to reduce mortality rate and reverse shock in patients with relative adrenal shock in patients with relative adrenal insufficiencyinsufficiencyNNT=17NNT=17
Grade C
Corticosteroids In Septic Shock:SSC Recommendations
Dellinger RP, et al. Crit Care Med. 2004;32:858-873.Annane D et al. JAMA 2000;283:1038-1045
Xigris (drotrecogin alfa[activated]) in Severe Sepsis: Indication
Drotrecogin alfa (activated) is indicated for the Drotrecogin alfa (activated) is indicated for the reduction of mortality in adult patients with severe reduction of mortality in adult patients with severe sepsis (sepsis associated with acute organ sepsis (sepsis associated with acute organ dysfunction) who have a high risk of death (e.g., as dysfunction) who have a high risk of death (e.g., as determined by APACHE II*)determined by APACHE II*)
DrotrecoginDrotrecogin alfaalfa (activated) is not indicated in adult (activated) is not indicated in adult patients with severe sepsis and lower risk of death. patients with severe sepsis and lower risk of death. Safety and efficacy have not been established in Safety and efficacy have not been established in pediatric patients with severe sepsis.pediatric patients with severe sepsis.
*APACHE (Acute Physiology And Chronic Health Evaluation). For more information on using the APACHE II scoring system, please see http://www.sfar.org/scores2/scores2.html.
See important safety information in this presentation.
THE ROLE OF ENDOGENOUS ACTIVATED PROTEIN C IN SEVERE SEPSIS
Endothelium
Neutrophil
Monocyte
IL-6
IL-6
Activated Protein C
Inactivation
Inactivation
Inactivation
Activated Protein CPAI-1
SuppressedfibrinolysisActivated
Protein C
Reductionof Rolling
Inhi
bitio
nIn
hibi
tion
Activated Protein C
Factor VIIIaTissue Factor
COAGULATION CASCADE
Factor Va
THROMBIN
Fibrin
Fibrin clotTissue Factor
Organisms
Inflammatory Responseto Infection
Thrombotic Responseto Infection
Fibrinolytic Responseto Infection
Recombinant human Activated Protein C Recombinant human Activated Protein C [Drotrecogin alfa (activated)] is recommended in [Drotrecogin alfa (activated)] is recommended in patients at a high risk of deathpatients at a high risk of death Grade BAPACHE II score APACHE II score ≥≥ 25, or25, orSepsisSepsis--induced multiple organ failure, orinduced multiple organ failure, orSeptic shock, orSeptic shock, orSepsis induced acute respiratory distress syndromeSepsis induced acute respiratory distress syndrome
Treatment with drotrecogin alfa (activated) should Treatment with drotrecogin alfa (activated) should begin as soon as possible once a patient has been begin as soon as possible once a patient has been identified as being at high risk of deathidentified as being at high risk of deathPatients should have no absolute or relative Patients should have no absolute or relative contraindication related to bleeding risk that contraindication related to bleeding risk that outweighs the potential benefit of rhAPCoutweighs the potential benefit of rhAPC
Recombinant human Activated Protein C
Dellinger, et. al. Crit Care Med 2004, 32: 858-873.

13
*as defined by APACHE II ≥25†relative risk reduction at 28 daysData on file, Eli Lilly and Company.
PROWESS 28-Day Mortality –High Risk of Death Patients*
44%
31%
0%
10%
20%
30%
40%
50%
60%
Placebo Drotrecoginalfa
(activated)
Absolute Risk Reduction
= 13%
Mor
talit
y R
ate
Drotrecogin Alfa (Activated) In Severe Sepsis: PROWESS Results
29% reduction in relative risk of death with Xigris†
See important safety information in this presentation.
Survival Benefit Consistent across High-risk Severe Sepsis Patients
The 95% relative risk confidence interval for each subgroup included the point estimate for the overall PROWESS population (0.80). The point estimate of relative risk of death in each subgroup is indicated by a solid circle, and the 95% confidence interval is indicated by the horizontal lines. Note the consistency between the overall trial result and the subgroup analyses.
*APACHE (Acute Physiology And Chronic Health Evaluation). For more information on using the APACHE II scoring system, please seehttp://www.sfar.org/scores2/scores2.html †Nonprospectively defined population 1. Barie P, et al. Am J Surg. 2004; 188:212-220. 2. Dhainaut JF MD, PhD, et al. For the PROWESS Study Group. Intensive Care Med. 2003;29(6):894-903.3. Laterre P-F et al. Crit Care Med.2005;33(5):952-961. 4. Data on file, Eli Lilly and Company. 6. Dhainaut JF, Yan SB, Joyce DE, et al. J Thromb Haemost 2004; 2:1924-33.
Xigris® (drotrecogin alfa [activated]) benefits consistent
See Important Safety Information in this presentation.
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 Relative Risk of Death (95% CI)
FAVORS XIGRIS FAVORS PLACEBO TOTAL RELATIVE RISK XIGRIS PLACEBO(CONFIDENCE
INTERVAL)
APACHE II* ≥ 251 817 0.70(0.59 - 0.85) 30.9 43.7
ORGAN DYSFUNCTION ≥22 1271 0.78(0.66 - 0.93) 26.5 33.9
CAP WITH APACHE II ≥253 321 0.60(0.44 - 0.82) 26.2 43.5
CAP S. PNEUMONIAE 92 0.40(0.20 - 0.78) 18.0 45.2WITH APACHE II ≥254
INTRA-ABDOMINAL SURGERY 116 0.60(0.36 - 1.00) 26.8 45.0WITH APACHE II ≥251
OVERT DIC6 454 0.71(0.55 - 0.91) 30.5 43.0
28-DAY MORTALITY
6
Safety ProfileLow incidence of serious bleeding events*Rate of serious bleeding events during infusion in high-risk patients:
PROWESS: 2.2% (9 of 414) in drotrecogin alfa (activated) patients vs 0.7% (3 of 403) in standard therapy patients
Rate of ICH in high-risk patients during infusion:PROWESS: 0.2% (1 of 414) in drotrecogin alfa (activated) patients
Associated with severe thrombocytopenia (platelet count < 30,000/mm3)†
Not associated with other adverse events*Serious bleeding events were defined as any intracranial hemorrhage, any life-threatening bleeding, any bleeding event requiring the administration of ≥3 units of packed red blood cells per day for 2 consecutive days, or any bleeding event assessed as a serious adverse event.†At the time of enrollment in the PROWESS study, the patient had a platelet count above 30,000/mm3. The patient’s platelet count fell to less than 30,000/mm3 after drotrecogin alfa (activated) therapy was initiated.Data on file, Eli Lilly and Company
See important safety information and full prescribing information in this presentation.
CONTRAINDICATIONS
Active internal bleedingActive internal bleedingRecent (within 3 months) hemorrhagic strokeRecent (within 3 months) hemorrhagic strokeRecent (within 2 months) intracranial or intraspinal Recent (within 2 months) intracranial or intraspinal surgery, or severe head traumasurgery, or severe head traumaTrauma with an increased risk of lifeTrauma with an increased risk of life--threatening threatening bleedingbleedingPresence of an epidural catheterPresence of an epidural catheterIntracranial neoplasm or mass lesion or evidence of Intracranial neoplasm or mass lesion or evidence of cerebral herniationcerebral herniation
See full Prescribing Information available at this presentation.
Important Safety InformationImportant Safety Information
Drotrecogin alfa (activated) increases the risk of bleeding. Drotrecogin alfa(activated) is contraindicated in patients with the following clinical situations in which bleeding could be associated with a high risk of death or significant morbidity.
DrotrecoginDrotrecogin alfaalfa (activated) is contraindicated in patients with known (activated) is contraindicated in patients with known hypersensitivity to hypersensitivity to drotrecogindrotrecogin alfaalfa (activated) or any component of this product.(activated) or any component of this product.
Drotrecogin Alfa (Activated) Has a Favorable Risk/Benefit Profile
8 times more likely to save an additional life than observe an additional serious bleeding event *
* Based on a 13% 28-day survival benefit and a serious bleeding rate during infusion attributable to Xigris of 1.5% (13% ÷ 1.5% = 8.7) in patients with an APACHE II score > 25.Data on file, Eli Lilly and Company.
Fine-Tuning Xigris Therapy in AdultHigh-Risk Severe Sepsis PatientsRight Patient, Right Drug, Right Time
New: Clinical trials to help advance care of adultpatients with severe sepsis at high risk of death:
Contact 1-800-LILLY-RX for more information.
RESPOND Targeted Enrollment = 500 RESPOND Targeted Enrollment = 500 Enrollment started in Nov. 2006Enrollment started in Nov. 2006
Phase 2 trial investigating a biomarker (Protein C) to help guidPhase 2 trial investigating a biomarker (Protein C) to help guide e Xigris therapy in adult patients with severe sepsis at high riskXigris therapy in adult patients with severe sepsis at high risk of death.of death.
NEW Placebo Controlled Trial NEW Placebo Controlled Trial in Adult Highin Adult High--Risk Severe SepsisRisk Severe Sepsis
Help clinicians better identify patients who are most likely to Help clinicians better identify patients who are most likely to benefit benefit from Xigris, as well as to further clarify the benefit/risk proffrom Xigris, as well as to further clarify the benefit/risk profile of the drug.ile of the drug.
Please see Important Safety Information in this presentation and accompanying full Prescribing Information.Bleeding is the most common adverse effect associated with Xigris therapy.

14
Low Tidal Volume Ventilation: SSC Recommendations
High tidal volumes, >6 High tidal volumes, >6 mLmL/kg, coupled /kg, coupled with high plateau pressures, >30 cm with high plateau pressures, >30 cm HH22O, should be avoidedO, should be avoided
HypercapniaHypercapnia can be tolerated in patients can be tolerated in patients with ALI/ARDS if required to minimize with ALI/ARDS if required to minimize plateau pressures and tidal volumesplateau pressures and tidal volumes
A minimum amount of positive end A minimum amount of positive end expiratory pressure should be used to expiratory pressure should be used to prevent lung collapse at endprevent lung collapse at end--expirationexpiration
Grade B
Grade C
Grade E
Dellinger RP, et al. Crit Care Med. 2004;32:858-873.
0
5
10
15
20
25
30
35
40
6 ml/kg12 ml/kg
% M
orta
lity
ARDSnetMechanical Ventilation Protocol
Results: Mortality
The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:1301-1378
Potential Advantages of Norepinephrine
Minimal tachycardia responseMinimal tachycardia responseNo interference with hypothalamic No interference with hypothalamic pituitary axispituitary axisEvidence of increased cardiac output, Evidence of increased cardiac output, renal blood flow and urine output when renal blood flow and urine output when used in septic shockused in septic shockMore potent agent than dopamine in More potent agent than dopamine in refractory septic shockrefractory septic shock
Dellinger RP Crit Care Med 2003;31(3):946-955
Following initial stabilization of patients with severe Following initial stabilization of patients with severe sepsis, maintain blood glucose to sepsis, maintain blood glucose to <150 mg/<150 mg/dLdLGlycemicGlycemic control strategy should include a nutrition control strategy should include a nutrition protocol with the preferential use of the protocol with the preferential use of the enteralenteral routeroute
Minimize the risk of hypoglycemia by providing Minimize the risk of hypoglycemia by providing a continuous supply of glucose substrate a continuous supply of glucose substrate Accomplished by using 5% or 10% dextrose IV Accomplished by using 5% or 10% dextrose IV infusion and followed by initiation of feeding infusion and followed by initiation of feeding preferably by preferably by enteralenteral routeroute
Grade D
Grade E
Glucose Control: SSC Recommendations
Dellinger RP, et al. Crit Care Med. 2004;32:858-873.
Intensive Insulin Therapy in the Critically Ill
Hyperglycemia & insulin resistance are Hyperglycemia & insulin resistance are commoncommonIn diabetics with acute myocardial infarct, In diabetics with acute myocardial infarct, therapy to maintain the blood glucose level < therapy to maintain the blood glucose level < 215mg/dL improves long term outcomes 215mg/dL improves long term outcomes In the SICU, tight In the SICU, tight glycemicglycemic control to maintain control to maintain a blood glucose of < 110mg/dL reduces a blood glucose of < 110mg/dL reduces morbidity & mortality (Grade B)morbidity & mortality (Grade B)The greatest reduction in mortality involves The greatest reduction in mortality involves deaths due to multiple organ failure with a deaths due to multiple organ failure with a proven septic focus.proven septic focus.
Van den Berghe G. et al. N Engl J Med 2001;345:1359-67

15
10.9%
7.2%
0%
5%
10%
15%
8.0%
4.6%
0%
5%
10%
15%
Mortality During Intensive Care
In-Hospital Mortality
Mor
talit
y (%
)
p = 0.01p < 0.04 (adjusted)
n=783 n=765Conventional Intensive Insulin
n=783 n=765
van den Berghe G. N Engl J Med 2001;345:1359-1367.
Glucose Control – Intensive Insulin
NNT=29
Medical ICU Glycemic Management
1200 MICU patients1200 MICU patientsMaintain serum glucose levels 80Maintain serum glucose levels 80--110mg/dl110mg/dlMeasure 28 day mortality for patients >3 days in the ICUMeasure 28 day mortality for patients >3 days in the ICUMeasured morbidity factors: renal failure/dialysis use, Measured morbidity factors: renal failure/dialysis use, vent days & ICU LOSvent days & ICU LOS
Methodology
ResultsNo difference in mortality within looking at all patientsNo difference in mortality within looking at all patients> 3 days in the ICU with effective glucose control > 3 days in the ICU with effective glucose control demonstrated improved mortalitydemonstrated improved mortality (43% (43% vsvs 52.5% 52.5% (p=0.009)(p=0.009)Reduce use of dialysis, earlier weaning & discharge Reduce use of dialysis, earlier weaning & discharge from the ICU in pts receiving from the ICU in pts receiving glycemicglycemic controlcontrol
Van den Berghe G et al. N Engl J of Med 2006;354:449-461
Sepsis Evidence ImplementationSepsis Evidence Implementation
Making it a RealityMaking it a RealitySepsis BundleSepsis Bundle
Sepsis BundlesScreen for Severe SepsisYes No
Management Sepsis Bundle (24 hour)
•• Maintain serum glucose levels on Maintain serum glucose levels on average < 150 mg/dl. (8.3 average < 150 mg/dl. (8.3 mmolmmol/L )/L )
•• DrotrecoginDrotrecogin alfaalfa (activated) (activated) administered in accordance with administered in accordance with hospital guidelineshospital guidelines
•• Steroids given for septic shock Steroids given for septic shock requiring continued use of requiring continued use of vasopressorsvasopressors for equal to or greater for equal to or greater than 6 hoursthan 6 hours
•• Adoption of a lung protective strategy Adoption of a lung protective strategy (tidal volumes (tidal volumes < < 6ml/kg) with plateau 6ml/kg) with plateau pressures of 30 cm H2O for pressures of 30 cm H2O for mechanically ventilated patientsmechanically ventilated patients
Resuscitation Sepsis Bundle (6-Hour)
••Obtain Cultures before antibiotic administrationObtain Cultures before antibiotic administration••Lactate LevelLactate Level••Board spectrum antibiotics administered Within 3 hours of Board spectrum antibiotics administered Within 3 hours of presentationpresentation••In the event of hypotension (SBP < 90, MAP < 70) or lactate In the event of hypotension (SBP < 90, MAP < 70) or lactate > 4 > 4 mmolmmol/L, begin initial fluid resuscitation with 20/L, begin initial fluid resuscitation with 20--40 ml of 40 ml of crystalloid (or colloid equivalent) per estimated kg of body crystalloid (or colloid equivalent) per estimated kg of body weightweight••VasopressorsVasopressors employed for hypotension ((MAP) Less than employed for hypotension ((MAP) Less than 65 mm Hg) during and after initial fluid resuscitation65 mm Hg) during and after initial fluid resuscitation••In the event of septic shock or lactate > 4 In the event of septic shock or lactate > 4 mmolmmol/L, CVP and /L, CVP and ScvO2 or SVO2 measured. ScvO2 or SVO2 measured. ••In the event of septic shock or lactate > 4 In the event of septic shock or lactate > 4 mmolmmol/L, CVP /L, CVP maintained 8maintained 8--12 12 mmhgmmhg••InotropesInotropes (and/or (and/or PRBCPRBC’’ss if if hematocrithematocrit <= 30 percent) <= 30 percent) delivered for ScvO2 < 70delivered for ScvO2 < 70 percent or SVO2 < 65 percentpercent or SVO2 < 65 percent if if CVP >= 8 CVP >= 8 mmhgmmhg
Standard careStandard care
If on Antibiotic, then Monitor Q24H FL Monitor Per shift ICU
Develop Protocols & Order Sets to Implement Resuscitation in Medical-Surgical Area
Draw bloodDraw bloodLactate LevelLactate LevelObtain blood cultures before administration of Obtain blood cultures before administration of antibioticantibiotic
Broad spectrum antibiotics administered within three Broad spectrum antibiotics administered within three hours of presentationhours of presentationIn the event of hypotension (SBP < 90, MAP < 70) or In the event of hypotension (SBP < 90, MAP < 70) or lactate > 4 lactate > 4 mmolmmol/L, begin initial fluid resuscitation with /L, begin initial fluid resuscitation with 2020--40 ml of crystalloid (or colloid equivalent) per 40 ml of crystalloid (or colloid equivalent) per estimated kg of body weightestimated kg of body weightVasopressorsVasopressors employed for hypotension ((MAP) employed for hypotension ((MAP) Less than 65 mm Hg) during and after initial fluid Less than 65 mm Hg) during and after initial fluid resuscitationresuscitation
www.ihi.org
Within 6 hrs (Transport is ICU is Key)
In the event of septic shock or lactate > 4 In the event of septic shock or lactate > 4 mmolmmol/L, CVP and ScvO2 or SVO2 /L, CVP and ScvO2 or SVO2 measured. (line inserted)measured. (line inserted)In the event of septic shock or lactate > 4 In the event of septic shock or lactate > 4 mmolmmol/L, CVP maintained 8/L, CVP maintained 8--12 12 mmhgmmhgInotropesInotropes (and/or (and/or PRBCPRBC’’ss if if hematocrithematocrit<= 30 percent) delivered for S<= 30 percent) delivered for ScvcvO2 < O2 < 7070 percent or Spercent or SVVO2 < 65 percentO2 < 65 percent if CVP if CVP >= 8 >= 8 mmhgmmhg
www.ihi.org

16
Maintain serum glucose levels on average Maintain serum glucose levels on average < 150 mg/dl. (8.3 < 150 mg/dl. (8.3 mmolmmol/L) /L) DrotrecoginDrotrecogin alfaalfa (activated) administered in (activated) administered in accordance with hospital guidelinesaccordance with hospital guidelinesSteroids given for septic shock requiring Steroids given for septic shock requiring continued use of continued use of vasopressorsvasopressors for equal to for equal to or greater than 6 hoursor greater than 6 hoursAdoption of a lung protective strategy (tidal Adoption of a lung protective strategy (tidal volumes volumes < < 6ml/kg) with plateau pressures 6ml/kg) with plateau pressures of 30 cm H2O for mechanically ventilated of 30 cm H2O for mechanically ventilated patientspatients
Develop Protocols & Order Sets to Implement Management 24-Hour Severe Sepsis Bundles
www.IHI.org
Sepsis Measurement tool found at www.ihi.org & www.survivingsepsis.org
Severe Sepsis Bundle Implementation Results
EnglandEnglandGermanyGermanySt. Louis, MissouriSt. Louis, MissouriColorado CoalitionColorado CoalitionTICUTICU
Severe Sepsis Protocol in UseGermany
Retrospective cohort study in 10 bed mixed ICU in GermanyRetrospective cohort study in 10 bed mixed ICU in Germany60 patients (30 consecutive receiving SOP severe sepsis 60 patients (30 consecutive receiving SOP severe sepsis management compared to historical controls)management compared to historical controls)Measured: Primary endpoint 28 day mortalityMeasured: Primary endpoint 28 day mortalityMeasured: Secondary endpoints; Measured: Secondary endpoints; ABGABG’’ss, lactate, glucose, , lactate, glucose, creatcreat, WBC, Plat, time to , WBC, Plat, time to dxdx & 7am on day 2 & 4 SOFA & 7am on day 2 & 4 SOFA scoresscoresResults: In SOP group: Results: In SOP group: ↑↑ use of use of dobutaminedobutamine, glucose , glucose control, steroids & control, steroids & rhAPCrhAPCMortality: Control Mortality: Control vsvs SOP (53% vs. 27% p <.05)SOP (53% vs. 27% p <.05)Independent predictors of survival: lactate on admission, age, Independent predictors of survival: lactate on admission, age, gender, blood glucose < 150 mg/dl, gender, blood glucose < 150 mg/dl, admadm of of rhAPCrhAPC & steroids& steroids
Kortgen A et al. Crit Care Med, 2006:34:943-949
Standardized Order Set-Sepsis BundlesSt. Louis, Missouri
BeforeBefore--after study design with prospective consecutive after study design with prospective consecutive data collection of 120 patientsdata collection of 120 patients1,200 bed academic medical center1,200 bed academic medical centerPrimary endpoint: 28 day mortalityPrimary endpoint: 28 day mortalityOther measures: hospital LOS, IV fluid intact for shock, Other measures: hospital LOS, IV fluid intact for shock, appropriate antibioticappropriate antibioticResults: after group: received more IV fluids in ED Results: after group: received more IV fluids in ED (p=0.002); more likely to receive >20ml/kg of fluid prior to (p=0.002); more likely to receive >20ml/kg of fluid prior to vasopressorsvasopressors; had lower risk of mortality (48.3% ; had lower risk of mortality (48.3% vsvs 30%, 30%, p=0.04); lower hospital LOS (12.1 p=0.04); lower hospital LOS (12.1 vsvs 8.9 days, p=0.038)8.9 days, p=0.038)Independent predictors of survival: increased pt age and Independent predictors of survival: increased pt age and not receiving >20 ml/kg of IV fluid prior to not receiving >20 ml/kg of IV fluid prior to vasopressorsvasopressors
Micek, Scott et al., Critical Care Medicine, 2006; 34:2707-2714
Colorado Coalition: Statewide Network
27%27%15%15%1371371161162121Management Management BundleBundle
19%19%11%11%989887871111Resuscitation Resuscitation BundleBundle
100%100%22%22%509509399399110110Mortality: Mortality: All PatientsAll Patients
% Total % Total ChartsCharts
% died % died who got who got the the bundlebundle
Total Total Receiving Receiving BundleBundle
AliveAliveDeceasedDeceased
Presented by Dr. M. Levy at ASPEN National Meeting, 1/07

17
VHA Sepsis Composite Profile (19 ICU’s)
(Sepsis Population: On ICU Admission)
43.5
84.2
61.5
77.4
36
48.1
57.7
48.5
58.7
90.9
67.661.9
86.790
85.387
0
10
20
30
40
50
60
70
80
90
100
VancoReceived
BS AbxReceived
Bld CulturesCollected
SteriodsReceived
CSTCompleted
APC EligAssessed
APC Received Vanco Discont
Baseline (Sept03- Nov03) 3rdQ04
Presented at MI Keystone Oct 2004Presented at SCCM 2005
VHA TICU: Sepsis(n= 19 ICUs)
Mortality
13.1
21.9
41.8
0.0
10.0
20.0
30.0
40.0
50.0
Oct - Dec2003
Mar - May2004
July - Sept2004
%
69% Reduction (p < 0.001)
ICU LOS
6.27.6
10.0
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
Oct - Dec2003
Mar - May2004
July - Sept2004
Day
s
36% Reduction (NS)
Presented at MI Keystone Oct 2004Presented at SCCM 2005
The Nurses RoleEarly recognition of Early recognition of patients with signs of patients with signs of sepsissepsisEarly initiation of Early initiation of evidence based practice evidence based practice therapies appropriate for therapies appropriate for your area of practice your area of practice (antibiotics, fluids/blood & (antibiotics, fluids/blood & pressorspressors))Swift disposition to care Swift disposition to care areas where the rest of areas where the rest of the bundle can be started.the bundle can be started.


















