Overcoming poor permeability: translating permeation enhancers for oral peptide delivery
7
TECHNOLOGIES DRUGDISCOVERY TODAY Overcoming poor permeability: translating permeation enhancers for oral peptide delivery Sam Maher, David J. Brayden * UCD School of Veterinary Medicine and UCD Conway Institute, University College Dublin, Belfield, Dublin 4, Ireland Demand for oral alternatives to parenteral delivery has led to renewed interest in excipient-like intestinal per- meation enhancers that improve oral drug bioavail- ability. Oral delivery of macromolecules including peptides and proteins is limited by pre-systemic degra- dation and poor penetration across the gut wall. Research on oral absorption enhancers that increase gut permeability was first undertaken 50 years ago, yet clinical success has yet to be achieved. Development has been hampered by lack of adequate reproducible efficacy as well as perceived safety concerns. We review some selected permeation-enhancing excipi- ents that are key components of peptide formulations in advanced clinical development and assess why trans- lation of such technologies is close to fruition. Section editor: Max Zeller – addc GmbH, Fuellinsdorf, Switzerland. Tom Alfredson – Gilead Sciences, Foster City, CA, USA. Introduction There is considerable interest in delivery platforms that improve oral bioavailability of poorly absorbed peptides, proteins and macromolecules. Not only does the oral route improve patient compliance, but reformulation can also extend intellectual property and reduce costs associated with sterile manufacturing and use of healthcare professionals. The oral route is also a more physiological means of deliver- ing certain molecules to liver and intestinal cell targets (e.g. insulin and glucagon-like peptide-1 (GLP-1)). There are over 60 peptides and 180 biologics marketed worldwide and they comprise a high percentage of candidates in pre-clinical discovery [1–3]. The continued success of injectable peptides and proteins is overshadowed on the oral side by suscept- ibility to intestinal pre-systemic degradation. A bigger pro- blem, due to relatively large molecular weights and hydrophilicity, is poor penetration across the intestinal epithelium (Fig. 1). Absorption enhancers One of the simplest approaches to overcome poor oral macro- molecule permeability is use of absorption enhancers which increase intestinal permeability as against impacting on molecule solubility [4]. They do this by either opening epithe- lial tight junctions (TJs) (paracellular route), mildly perturb- ing the mucosal surface (transcellular permeation enhancement), or by non-covalent complexation with the payload. Several formulations that use enhancers have pro- gressed to clinical trials to boost oral bioavailability of BCS 1 Class III drugs (high solubility, low permeability). Some enhancers have already been successfully used in non-oral formats: topical (dimethyl sulfoxide in Pennsaid 1 , Covidien, USA [6]), buccal (bile salts in Oral-Lyn 1 , Generex, Canada [7]) Drug Discovery Today: Technologies Vol. 9, No. 2 2012 Editors-in-Chief Kelvin Lam – Harvard University, USA Henk Timmerman – Vrije Universiteit, The Netherlands Formulation technologies to overcome poor drug-like properties *Corresponding author.: D.J. Brayden ([email protected]) 1 Biopharmaceutics Classification System: adopted by the FDA for bio-waivers for oral Class I molecules [5]. 1740-6749/$ ß 2011 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddtec.2011.11.006 e113
Transcript of Overcoming poor permeability: translating permeation enhancers for oral peptide delivery

TECHNOLOGIES
DRUG DISCOVERY
TODAY
Overcoming poor permeability:translating permeation enhancers fororal peptide deliverySam Maher, David J. Brayden*UCD School of Veterinary Medicine and UCD Conway Institute, University College Dublin, Belfield, Dublin 4, Ireland
Drug Discovery Today: Technologies Vol. 9, No. 2 2012
Editors-in-Chief
Kelvin Lam – Harvard University, USA
Henk Timmerman – Vrije Universiteit, The Netherlands
Formulation technologies to overcome poor drug-like properties
Demand for oral alternatives to parenteral delivery has
led to renewed interest in excipient-like intestinal per-
meation enhancers that improve oral drug bioavail-
ability. Oral delivery of macromolecules including
peptides and proteins is limited by pre-systemic degra-
dation and poor penetration across the gut wall.
Research on oral absorption enhancers that increase
gut permeability was first undertaken 50 years ago, yet
clinical success has yet to be achieved. Development
has been hampered by lack of adequate reproducible
efficacy as well as perceived safety concerns. We
review some selected permeation-enhancing excipi-
ents that are key components of peptide formulations
in advanced clinical development and assess why trans-
lation of such technologies is close to fruition.
Introduction
There is considerable interest in delivery platforms that
improve oral bioavailability of poorly absorbed peptides,
proteins and macromolecules. Not only does the oral route
improve patient compliance, but reformulation can also
extend intellectual property and reduce costs associated with
sterile manufacturing and use of healthcare professionals.
The oral route is also a more physiological means of deliver-
ing certain molecules to liver and intestinal cell targets (e.g.
insulin and glucagon-like peptide-1 (GLP-1)). There are over
*Corresponding author.: D.J. Brayden ([email protected])
1740-6749/$ � 2011 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddtec.2011.11.006
Section editor:Max Zeller – addc GmbH, Fuellinsdorf, Switzerland.Tom Alfredson – Gilead Sciences, Foster City, CA, USA.
60 peptides and 180 biologics marketed worldwide and they
comprise a high percentage of candidates in pre-clinical
discovery [1–3]. The continued success of injectable peptides
and proteins is overshadowed on the oral side by suscept-
ibility to intestinal pre-systemic degradation. A bigger pro-
blem, due to relatively large molecular weights and
hydrophilicity, is poor penetration across the intestinal
epithelium (Fig. 1).
Absorption enhancers
One of the simplest approaches to overcome poor oral macro-
molecule permeability is use of absorption enhancers which
increase intestinal permeability as against impacting on
molecule solubility [4]. They do this by either opening epithe-
lial tight junctions (TJs) (paracellular route), mildly perturb-
ing the mucosal surface (transcellular permeation
enhancement), or by non-covalent complexation with the
payload. Several formulations that use enhancers have pro-
gressed to clinical trials to boost oral bioavailability of BCS1
Class III drugs (high solubility, low permeability). Some
enhancers have already been successfully used in non-oral
formats: topical (dimethyl sulfoxide in Pennsaid1, Covidien,
USA [6]), buccal (bile salts in Oral-Lyn1, Generex, Canada [7])
1 Biopharmaceutics Classification System: adopted by the FDA for bio-waivers for oralClass I molecules [5].
e113

Drug Discovery Today: Technologies | Formulation technologies to overcome poor drug-like properties Vol. 9, No. 2 2012
2 FDA nomenclature indicates that use of an excipient in a marketed product is‘allowed’ as against ‘approved’.
and rectal (sodium caprate (C10) in Doktacillin1, MEDA,
Sweden [8]). Despite 50 years of research, the hurdles to
progression of oral enhancers include low and variable
efficacy as well as safety concerns. Clinical data from several
specialised oral drug delivery companies that have pio-
neered such platforms for BCS Class III agents suggest that
some of these hurdles are now being addressed and 2012
could see the first oral peptide approval since cyclosporin
and desmopressin.
Oral macromolecule formulations
Oral formulations of peptides using enhancers have reached
clinical phases (Table 1). Other macromolecules in develop-
ment for oral delivery include heparins, antibiotics, anti-
cancer agents and ONS. Peptides are labile in gastrointestinal
fluids and they need protection from degradation by gastric
and pancreatic juice, and this can be achieved by enteric
coating with pH-dependent methacrylate-based polymers.
An entrapped formulation also enables co-release of pepti-
dase inhibitors, mucoadhesives or absorption enhancers in
specific intestinal regions. The latter works best when
released at the mucosal surface at the same time as the pay-
load, as the compromised barrier may otherwise ‘close’ before
the payload reaches the epithelium [9]. The majority of
enhancers in clinical trials are amphiphilic membrane per-
turbants. They increase flux by altering phospholipid packing
in plasma membranes at the concentrations required to
increase permeability. Some can cause a degree of cell lysis
and solubilisation, as reflected by superficial but reversible
mucosal injury.
Example I: acylcarnitines and bile salts
Tarsa Therapeutics (USA), under licence from Unigene
Laboratories (USA), have developed Oracal1, an oral salmon
calcitonin (sCT) formulation for osteoporosis containing
citric acid in vesicles in a Eudragit1 enteric coating [10–
12]. Oracal1 reached the primary endpoint of increasing
bone mass density at the lumbar spine in a recent Phase III
clinical trial of 565 postmenopausal women with estab-
lished osteoporosis; this citric acid formulation is the most
advanced oral peptide in clinical trials [13], and it seems
that the citric acid protects sCT and acts as a permeation
enhancer with an EDTA-like mechanism. Unigene’s oral
PTH (Enteripep1) based on a similar construct was also
effective in increasing bone mass growth and compared
well with a PTH injectable in a Phase II trial. Unlike their
sCT formulation, the oral PTH formulation contains an
additional and more established enhancer, lauroyl carni-
tine. Medium and long chain fatty acid esters of L-carnitine
have ideal properties for enhancement including rapid and
reversible action [14]. Another component in some of Uni-
gene’s oral formulations is the bile salt, sodium taurocho-
late [10,11]. Bile salts can routinely reach concentrations
e114 www.drugdiscoverytoday.com
over 10 mM in the lumen in the fed state, which is high
enough to both increase intestinal permeability and
improve drug solubilisation [15]. Sodium taurocholate is
a constituent of the ‘allowed’2 excipient, sodium choleate
(derived from Ox bile extract, which also contains other bile
salts, glycocholate, deoxycholate and cholate). Sodium cho-
late is also present in the RapidMist1 spray being developed
for buccal delivery of insulin (Oral-lyn1, Generex) [7].
Actions of different bile salts often cause superficial mucosal
injury, but the barrier repairs within hours [16,17].
Example II: Eligen1
Emisphere Technologies Inc. (USA) has developed a family of
small carriers (Eligen1) that improve passage of hydrophilic
drugs across the intestinal epithelium by non-covalent com-
plexation [18]. In what is a controversial theory, the inter-
action helps protect the payload from digestive enzymes
and increases hydrophobicity so the moiety can passively
permeate, after which the complex dissociates into the
respective components. These formulations are therefore
not classed as new chemical entities (NCEs). The two
most advanced carriers are the acylated amino acids, SNAC
(n-(8-[2-hydroxybenzoyl]amino)caprylic acid) and 5-CNAC
(N-(5-chlorosalicyloyl)-8-aminocaprylic acid). Examples of
peptides that have been evaluated with SNAC in human
include GLP-1, sCT and PTH; non-peptides include fractio-
nated and unfractionated heparin. SNAC decreased transe-
pithelial electrical resistance (TEER) in Caco-2 monolayers,
which was accompanied by release of lactate dehydrogenase
(LDH), suggesting that transcellular enhancement might
also be part of its mechanism [19,20]. Despite suggestions
of in vitro cytotoxicity however, SNAC does not cause sig-
nificant pathology in rat intestinal instillations [19]. This is
further reflected in the paucity of side effects in clinical trials
as well as its provisional granting of generally regarded as safe
(GRAS) status.
The other advanced Eligen1 carrier, 5-CNAC, is licensed to
Novartis (Switzerland), who have performed clinical assess-
ments with Nordic Biosciences (Denmark). An enteric-coated
oral formulation for sCT containing 5-CNAC had greater
efficacy than the nasal format of the drug (Miacalcin1;
Novartis Ltd.) [21]. Unfortunately, there have been two failed
Phase III trials of oral 5-CNAC/sCT for osteoarthritis in 2011.
Whilst the Eligen1 formulation had some efficacy in both
trials, it was ineffective in the co-primary endpoint of joint
space narrowing. A recent proof-of-concept trial for oral
delivery of PTH with 5-CNAC failed several undisclosed end-
points and Novartis have terminated development. The
Phase III clinical programme with Eligen1-sCT for osteoporo-
sis is ongoing.

Vol. 9, No. 2 2012 Drug Discovery Today: Technologies | Formulation technologies to overcome poor drug-like properties
(a) (b)
(c)mucusgel
microvilli
epithelialcell
basementmembrane
laminapropria
blood vessel
liversinusoid
hepatocyte
Kupffer cells
liver(d)
Drug Discovery Today: Technologies
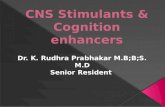
Figure 1. Barriers to the oral absorption of macromolecules. Gastric juice released from the stomach wall inactivates acid- and protease-labile drugs;
protection can be achieved by enteric coating or entrapment in micro- or nano-particulates. After leaving the stomach, the formulation enters the small
intestinal lumen (a) where the elevated pH causes dissolution of pH-dependent enteric coatings. Peptide-based macromolecules require protection from
pancreatic juice, achieved either by using citric acid to lower the optimal pH for enzymatic activity and/or by incorporation of a protease inhibitor. If
adequate protection is provided, the cargo reaches the small intestinal epithelium (b) which consists primarily of enterocytes and goblet cells. All BCS Class
III molecules require assistance with permeation to pass across the epithelial surface (c). Absorption enhancers can reversibly increase epithelial
permeability by the paracellular or transcellular routes, or by a combination of both. Macromolecules then enter sub-mucosal capillaries through endothelia
which drain into the hepatic portal vein, where the first pass effect may further reduce the fraction absorbed (d). If a macromolecule is encapsulated in a
nano- or micro-particulate, further barriers to absorption are the basement membrane, the endothelium of capillaries, the hepatic portal vein and the
Kupffer cells that line sinusoids. Figures (a) and (b) were produced using Servier Medical Art.
Example III: C10
Medium chain fatty acids have a long history of safe use as
dietary constituents in human, and have been extensively
studied as oral enhancers. C10 remains the only enhancer that
has been used clinically in the intestine for that purpose, albeit
in rectal suppositories [8]. It is one of the principal constituents
of gastrointestinal permeation enhancement technology
(GIPETTM; Merrion Pharmaceuticals, Ireland), an enteric-
coated solid dosage form currently designed to boost permea-
tion ofLMWH,pemetrexed,bisphosphonates andacyline [22].
GIPETTM is currently licensed to NovoNordisk (Denmark) for
oral formats of insulin and GLP-1 analogues. Isis Pharma (USA)
has also designed a different enteric-coated formulation of
C10 to improve bioavailability of antisense ONS. These were
effective in dogs and pigs as well as in preliminary clinical
studies [23]. The ISIS oral formulation comprises immediate
bolus release of payload and C10 followed by further gradual
release of C10 to extend the enhancement window [24], but
delivery of ONS has the disadvantage of requiring even higher
concentrations of C10 than that required for other molecules.
Numerous efforts have been made to determine the mechan-
ism that C10 increases gut permeability (reviewed in [8]). Low
concentrations increase paracellular permeability by activa-
tion of phospholipase C, calmodulin and myosin light chain
kinase, which leads to contraction of scaffolding proteins
required to maintain TJ integrity. However, the higher con-
centrations that are required for optimal enhancement in
animals and human, lead to transcellular perturbation as a
www.drugdiscoverytoday.com e115

Drug Discovery Today: Technologies | Formulation technologies to overcome poor drug-like properties Vol. 9, No. 2 2012
Table 1. Selected candidate oral absorption promoters in clinical trials
Candidate enhancer(s) Company(s) Proprietary name Most advanced phase
Citric acid � lauroylcarnitine Tarsa, USA (Unigene, USA) PeptelligenceTM Phase III complete (sCT)
SNAC, 5-CNAC Emisphere, USA Eligen1 Phase III (sCT)
Bile acids/salts (e.g. sodium cholate),
C10, formulated with alkyl-PEG–peptide
conjugates
Biocon, India IN-105 Phase III (insulin)
Sodium caprate in matrix tablets Merrion Pharma, Ireland GIPET1 Phase II (bisphosphonate)
Sodium caprylate in hydrophobic suspensions Chiasma, Israel TPE Phase I (octreotide)
Salts of EDTA Oramed Pharma, USA ORMD-0801
ORMD-0901
Phase I (exenatide/insulin)
Hydrophilic aromatic alcohols (e.g. phenoxy-,
benzyl- and phenyl-alcohols)
Proxima Concepts, UK Capsulin1 Capcitonin1 Phase I (insulin/sCT)
Alkylsaccharides (e.g. TDM and DDM) Aegis Therapeutics, USA Intravail1 Oral pre-clinical (octreotide);
Phase I (nasal, GLP-1 analogues)
result of its surfactant properties. In vivo this perturbative
action causes only mild mucosal injury that is rapidly reversed
and seems to be of little toxicological consequence to date. To
date, Merrion have administered GIPETTM to several hundred
patients without any major toxicity issues.
Example IV: transient permeability enhancer (TPE)
TPE (Chiasma, Israel) is an enteric-coated formulation con-
taining sodium caprylate (C8) in hydrophilic microparticles
that are mixed with castor oil or medium chain glyceride
(MCG) and/or caprylic acid, yielding an oily suspension [25].
Chiasma was granted orphan status by the FDA for their oral
format of the octapeptide, octreotide (Octreolin1). In a
Phase I trial of 12 individuals, octreolin1 performed simi-
larly to SC injection and had no adverse effects [26]. The
most effective molecular weight range of macromolecules
that TPE can deliver is 4–10 kDa [25]. Staggering the admin-
istration of TPE and cargo (FD4) gradually reduced the
window for enhancement, similar to other oral enhancers
(e.g. C10 [27]), the reasons being rapid intestinal epithelium
repair and likely absorption of the enhancer [17]. Increased
permeability with C8 is accompanied by altered membrane
fluidity of brush border membrane vesicles (BBMV) and
release of proteins from cells, both of which suggest trans-
cellular path enhancement [28]. Whilst the promoting
action of C8 is less than that of C10 and C12 per se, the
inventive step is its combination with other excipients in
an emulsion format to yield TPE and that format provides
increased oral bioavailability over that achieved with simple
admixed formats.
Example V: alcohol derivatives
Proxima Concepts (UK) is using food additives with GRAS
status and/or pharmacopoeia-listed excipients as absorption
enhancers [29]. Capsulin1 and Capcitonin1 are oral formats
of insulin and calcitonin containing enhancers that are being
e116 www.drugdiscoverytoday.com
evaluated under license by Diabetology Ltd. (UK) and Bone
Medical (Australia), respectively. Components include phe-
noxyethanol, benzyl- and phenyl-alcohols. These alcohol
derivatives are normally used as formulation preservatives
and solvents [30]. The Capsulin1 (150–300 IU) formulation
increased the glucose infusion rate when measured in
patients using the glucose clamp technique, although it
did not increase serum insulin level to the same degree as
the SC (12 IU) insulin counterpart [31].
Case VI: EDTA
Oramed Pharmaceuticals (USA) has tested oral and rectal
formulations for insulin (ORMD-0801) and GLP-1 analogues
(ORMD-0901) [32,33]. Assessment of five undisclosed ORMD-
0801 formulations showed reduction in baseline serum glu-
cose and c-met levels in eight patents [34]. An oral version of
exenatide (Eli Lilly, USA) demonstrated improved absorption
as indicated by a 28% increase in post-prandial serum insulin
[35]. Oramed’s enteric-coated oral formats contain a carrier
(e.g. omega-3 fatty acid), a protease inhibitor (e.g. soya bean
trypsin inhibitor) and an absorption enhancer (e.g. sodium
EDTA). Salts of EDTA are BCS Class III enhancers charac-
terised by strong-to-moderate enhancement with relatively
slow recovery of the barrier [14]. They increase paracellular
permeability by chelating the calcium that is required to form
intercellular junctions [36]. Sodium EDTA has widespread use
in topical, oral and parenteral formulations at concentrations
of 0.01–0.1% (w/v) [37]. It is considered non-toxic and non-
irritant at ‘allowable’ levels and is listed in the US Pharma-
copoeia-National Formulary (USP-NF). Oramed’s oral peptide
formulations were well tolerated in patients with only mild
gastrointestinal events. Although there are safety considera-
tions for some EDTA salts [38], the estimated daily acceptable
level of disodium EDTA is 2.5 mg/kg, and this is likely to be
much higher than the concentrations in Oramed’s oral for-
mulations.

Vol. 9, No. 2 2012 Drug Discovery Today: Technologies | Formulation technologies to overcome poor drug-like properties
Case VII: alkyl maltosides
Aegis Therapeutics (USA) use alkylmaltoside enhancers (col-
lectively termed Intravail1) that improve nasal and oral
delivery of macromolecules [39]. The most common enhan-
cers in Intravail1 are the amphiphilic surfactants, tetradecyl-
maltoside (TDM) and dodecylmaltoside (DDM). Whilst TDM
has been the more studied of the two enhancers for nasal
delivery, there are data showing improved oral delivery of
octreotide in rodents with DDM [40]. Intravail1 also
improved delivery of the synthetic peptide [D-Leu-4]-OB3
in rodents with an oral bioavailability of 47% relative to
SC [41]. Although ingredients of Intravail1 are GRAS-listed,
they probably cause some level of transcellular enhancement
as they are surfactants. This is reflected in studies showing
that increased nasal insulin bioavailability with DDM was
accompanied by mild morphological change [42].
Status of paracellular-specific peptide-based enhancers
Paracellular enhancers open the gaps between adjacent
epithelial cells by either (i) activating signalling cascades,
(ii) directly scrambling homophilic interactions between TJ
proteins or (iii) proteolytic cleavage of the extracellular por-
tions of TJ proteins [43–45]. By contrast, transcellular enhan-
cers may non-specifically affect the TJ by removing weakly
packed proteins or by directly perturbing the intestinal muco-
sae. In some cases the reversible opening of TJ is thought to be
a safer alternative than transcellular perturbation with sur-
factants. Nevertheless, for those that do not damage the
intestinal mucosa in pre-clinical animal models (e.g. C-term-
inal of Clostridium perfringens enterotoxin (C-CPE) [46]),
safety remains a key drawback. For instance, toxicological
assessment of C-CPE showed that whilst systemic delivery did
not increase biochemical markers of liver or kidney injury, it
caused an undesired immune response [47]. There are also
questions about whether specific TJ modulation can achieve
significant efficacy in human given the low overall surface
area in the intestine. Many are peptides or proteins them-
selves, and are likely to be digested in the GI lumen. The most
advanced specific TJ opening candidates to date are AT1002,
AT1006 and AT3227 (Alba Therapeutics, USA), which are
products of structure–function analysis of Zonula occludens
toxin (Zot), an enterotoxin produced by strains of Vibrio
cholera (reviewed in [48]). To our knowledge, no peptide-
based enhancer acting at TJs is currently in the clinic for oral
peptide delivery.
Hurdles to progression: efficacy considerations
A key issue in development of oral enhancer/macromolecule
formats is that oral bioavailability remains low and variable.
Low bioavailability is acceptable once the format can repro-
ducibly reach a threshold efficacy which is still cost effective:
this is the case with desmopressin, which has an oral bioa-
vailability of 0.16%. Traditionally, it was not financially
feasible to use 10- to 100-fold more peptide for oral delivery,
but there has been significant reduction in the cost of pro-
duction. For example, 0.8 mg of sCT was used in Phase III
clinical trials with 5-CNAC, which is almost 5000 times
higher than the current nasal dose (200 IU; 0.167 mg Miacal-
cin1; Novartis). Furthermore, the added cost of higher
amounts of active drug required when switching parenteral
peptides to oral formats can be partially offset by removing
the requirement for sterile injectable manufacturing and
increased revenue from new oral formulation patents.
In contrast to closed compartments like the nasal route, co-
presentation of the payload and enhancer at the intestinal
epithelium for a sufficient period is unpredictable because of
variability in intestinal transit, residence time, dilution in
intestinal fluids, diet and absorption of the enhancer itself.
Residence time in the small intestine is variable due to
wide-ranging peristaltic flow rates, so the enhancer and cargo
may have only short contact time with the wall [49]. Mucoad-
hesive polymers may slow formulation transit, although this
approach is limited by the high rate of mucous turnover [50].
Pharmacological inhibition of small intestinal peristalsis using
muscarinic antagonists [51], may improve understanding of
the contribution of residence time on efficacy of oral peptide
formulations. Furthermore, fluid volume in the small intestine
ranges from 45–320 ml (fasted) to 20–150 ml (fed) [52], so the
enhancer might never reach the threshold concentration for
enhancement, unless it is localised using novel formulation
design. The volume of solvent in which the formulation is
administered with also influences oral absorption: for 5-
CNAC/sCT, 50 ml water was more effective than 200 ml in
clinical studies [21]. A more concerted effort to understand the
effect of fluid volume and diet on enhancer action will assist
development of more effective oral platforms.
Another approach that could help overcome some of the
macromolecule permeability problems presented by the
small intestine is to target the colon, which is often shown
to be a more effective region for enhancement. When DDM
was formulated in colon-specific capsules, relative bioavail-
ability of carboxyflourescein (CF) in rats was 68.4% compared
with 16.9% and 29.3% in solution and uncoated gelatin
capsules, respectively [53]. Regional differences could be as
a result of (i) solvent drag effects in colon, (ii) differential
susceptibility to surfactants because the small intestine must
withstand regular exposure to bile salts and mixed micelles,
(iii) lower fluid volume in colon (4–13 ml), (iv) greater colonic
residence time (18–72 hours) and (v) reduced colonic pro-
teolysis [52–54]. A potential safety issue in targeting the colon
is the issue of increasing permeability in this bacteria-rich
environment.
Hurdles to progression: safety considerations
Since the first documented study on the use of intestinal
absorption enhancers, there has been concern about their
www.drugdiscoverytoday.com e117

Drug Discovery Today: Technologies | Formulation technologies to overcome poor drug-like properties Vol. 9, No. 2 2012
safety. Progression of enhancers that are either entirely NCEs
and/or have pharmacological actions are of greater toxico-
logical risk than substances with a history of safe use in
human. The FDA guidelines state that ‘if an excipient is
found to be pharmacologically active, this information
can influence subsequent development,’ so such substances
are likely to require a full battery of toxicological assess-
ments. Some paracellular enhancers have undesirable phar-
macology, for example, cytochalasin D which causes
hepatotoxicity [55] and C. perfringens enterotoxin (CPE),
which causes food poisoning [56]. These first-generation
TJ modulators helped delineate the structure and function
of epithelial TJs, and ultimately aided design of more selec-
tive second-generation paracellular enhancers which are
considered selective and potentially safer [43–45], although
their safety in human is unknown. Taking into account the
heavy financial investment developing the drug of interest,
Pharma has therefore focused on simple enhancers that have
a history of safe use including those with food additive status
or use of ‘allowed’ excipients that can be cheaply manufac-
tured. It is not yet clear whether these candidates will receive
any toxicological dispensation by regulatory authorities, but
their risk of failure because of unknown toxicity is signifi-
cantly reduced.
Of the candidate enhancers listed in Table 1, most have
demonstrated some capacity to superficially abrade the
intestinal mucosa. However, dilution, spreading and absorp-
tion of the enhancer itself prevent prolonged exposure in vivo.
Combined with the high turnover of enterocytes means that
the abrasive actions of enhancers are relatively mild [17].
Drugs (NSAIDs), established excipients (e.g. suppository
bases) and dietary constituents (alcohol, fatty and spicy
foods) can all cause mucosal injury, as do bile and gastric
secretions [15,16,57]. Aspirin causes gastrointestinal side
effects including ulceration and bleeding, but its damaging
action results from both mucosal perturbation and systemic
effects that are exacerbated by interference in mucosal repair
[58]. Whilst no such actions have been reported with enhan-
cers in recent clinical trials, repeated superficial mucosal
injury might be an issue for daily dosing regimes.
The possibility of bystander absorption during the
enhancement window is a valid concern. Taking into account
the precise conditions required for permeation enhance-
ment, as well as the difference in the molecular weight
between effective payloads (<10 kDa) and dangerous luminal
bystanders (�100 kDa), this concern may well be overstated.
Reversibility studies performed with C10 in human using the
lactulose:mannitol urinary excretion ratio (LMER), showed
that following intra-jejunal administration to human sub-
jects, the enhancer only increased permeability over the first
20 min and that the change in permeability is several orders
of magnitude lower than disease states [59]. Further studies
that rule out adverse events caused by bystander absorption
e118 www.drugdiscoverytoday.com
(both local and systemic) will improve the safety profile of the
candidate enhancer.
Conclusions and prospects
Oral formulations using absorption enhancers for poorly
absorbed peptides have matured with several technologies
progressing to clinical development. The positive outcome
from the Phase III trial of Tarsa’s Oracal1 sCT formulation
could result in the first oral peptide approval since cyclos-
porin and desmopressin. The most successful approaches
reaching clinical development are enteric-coated formula-
tions that encapsulate a peptide drug (<10 kDa) with protec-
tive carrier, peptidase inhibitors and an absorption enhancer
capable of rapidly and reversibly increasing epithelial perme-
ability. The most suitable enhancers are those with a history
of safe use in human either as food additives or ‘allowed’
pharmaceutical excipients that can be easily scaled to man-
ufacture and do not adversely affect peptide physicochemical
properties. The future is likely to see greater emphasis on
optimised micro- and nano-particulates with enhancers that
provide an added level of protection from degradation and
assist co-localised release. Achieving an adequate level of oral
efficacy is likely to be a bigger constraint than toxicity,
although safety of daily and long-term oral administration
regimes must be assessed.
Acknowledgements
Merrion Pharmaceuticals part-fund a PhD student and Novo-
Nordisk funds a postdoc in the lab of DB. Work in the lab is
mainly funded by Science Foundation Grant SRC/07/B1154
(The Irish Drug Delivery Network). SM is funded by Food-For-
Health Ireland.
References1 Chien, J.Y. and Ho, R.J. (2008) Drug delivery trends in clinical trials and
translational medicine. J. Pharm. Sci. 97, 2543–2547
2 Walsh, G. (2009) Market development of biopharmaceuticals. Genet. Eng.
Livest.: New Appl. Interdiscipl. Perspect. 34, 69–89
3 Vlieghe, P. et al. (2010) Synthetic therapeutic peptides: science and market.
Drug Discov. Today 15, 40–56
4 Swenson, S.E. and Curatolo, W.J. (1992) Means to enhance penetration:
(2) Intestinal permeability enhancement for proteins, peptides and other
polar drugs: mechanisms and potential toxicity. Adv. Drug Deliv. Rev. 8, 39–
92
5 Amidon, G.L. et al. (1995) A theoretical basis for a biopharmaceutic drug
classification: the correlation of in vitro drug product dissolution and in
vivo bioavailability. Pharm. Res. 12, 413–420
6 Moen, M.D. (2009) Topical diclofenac solution. Drugs 69, 2621–2632
7 Bernstein, G. (2008) Delivery of insulin to the buccal mucosa utilizing the
RapidMist system. Expert Opin. Drug Deliv. 5, 1047–1055
8 Maher, S. et al. (2009) Safety and efficacy of sodium caprate in promoting
oral drug absorption: from in vitro to the clinic. Adv. Drug Deliv. Rev. 61,
1427–1449
9 Baluom, M. et al. (2000) Synchronized release of sulpiride and sodium
decanoate from HPMC matrices: a rational approach to enhance sulpiride
absorption in the rat intestine. Pharm. Res. 17, 1071–1076
10 Lee, Y.H. and Sinko, P.J. (2000) Oral delivery of salmon calcitonin. Adv.
Drug Deliv. Rev. 42, 225–238

Vol. 9, No. 2 2012 Drug Discovery Today: Technologies | Formulation technologies to overcome poor drug-like properties
11 Sinko, P.J. et al. (1999) Biopharmaceutical approaches for developing and
assessing oral peptide delivery strategies and systems: in vitro permeability
and in vivo oral absorption of salmon calcitonin (sCT). Pharm. Res. 16,
527–533
12 Stern, W. and Gilligan, J.P. [Unigene Laboratories] (1999) Oral salmon
calcitonin pharmaceutical products. USP 5912014
13 http://www.tarsatherapeutics.com/news/091811.html (accessed
November 10th, 2011)
14 Muranishi, S. (1990) Absorption enhancers. Crit. Rev. Ther. Drug Carrier
Syst. 7, 1–33
15 Porter, C.J. et al. (2007) Lipids and lipid-based formulations: optimizing
the oral delivery of lipophilic drugs. Nat. Rev. Drug Discov. 6,
231–248
16 Gookin, J.L. et al. (2002) Inducible nitric oxide synthase mediates early
epithelial repair of porcine ileum. Am. J. Physiol. Gastrointest. Liver Physiol.
283, G157–G168
17 Blikslager, A.T. et al. (2007) Restoration of barrier function in injured
intestinal mucosa. Physiol. Rev. 87, 545–564
18 Goldberg, M. and Gomez-Orellana, I. (2003) Challenges for the oral
delivery of macromolecules. Nat. Rev. Drug Discov. 2, 289–295
19 Brayden, D. et al. (1997) Heparin absorption across the intestine:
effects of sodium N-[8-(2-hydroxybenzoyl)amino]caprylate in rat in
situ intestinal instillations and in Caco-2 monolayers. Pharm. Res. 14,
1772–1779
20 Hess, S. et al. (2005) Investigation of the enhancing mechanism of sodium
N-[8-(2-hydroxybenzoyl)amino]caprylate effect on the intestinal
permeability of polar molecules utilizing a voltage clamp method. Eur. J.
Pharm. Sci. 25, 307–312
21 Karsdal, M.A. et al. (2011) Lessons learned from the development of oral
calcitonin: the first tablet formulation of a protein in phase III clinical
trials. J. Clin. Pharmacol. 51, 460–471
22 Walsh, E. et al. (2011) Oral delivery of macromolecules: rationale
underpinning Gastrointestinal Permeation Enhancement Technology
(GIPET1). Ther. Deliv. 12, 1595–161010.4155/TDE.11.132
23 Hardee, G.E. et al. (2008) Routes and formulation for the delivery of
antisense oligonucleotides. In Antisense Drug Technology Principle, Strategies
and Applications (Crooke, S.T., ed.), pp. 217–236, CRC Press
24 Tillman, L.G. et al. (2008) Oral delivery of antisense oligonucleotides in
man. J. Pharm. Sci. 97, 225–236
25 Salama, P. et al. [Lando and Anastasi] (2010) Pharmaceutical combinations
and related methods of delivery. USP Application 01056275A1
26 Atsmon, J. et al. (2010) OctreolinTM, a safe oral alternative for parenteral
octreotide treatment; phase 1 study results. 14th European NeuroEndocrine
Association Congress, Liege, Belgium, 22–25 September (abstract OC-6.5)
27 Wang, X. et al. (2010) Restoration of rat colonic epithelium after in situ
intestinal instillation of the absorption promoter, sodium caprate. Ther.
Del. 1, 75–82
28 Sharma, P. et al. (2005) Absorption enhancement, mechanistic and
toxicity studies of medium chain fatty acids, cyclodextrins and bile salts as
peroral absorption enhancers. Farmaco 60, 884–893
29 New, R. [Axcess Limited] (2004) Absorption enhancers. USP 7303762
30 Storey, R.A. (2009) Benzyl alcohol. In Handbook of Pharmaceutical
Excipients (6th edn) (Rowe, R.C., Skeskey, P.J., Quinn, M.E., eds), pp. 64–
66, Pharmaceutical Press
31 Luzio, S.D. et al. (2010) The glucose lowering effect of an oral insulin
(Capsulin) during an isoglycaemic clamp study in persons with type 2
diabetes. Diabetes Obes. Metab. 12, 82–87
32 Kidron, M. [Oramed Ltd.] (2010) Methods and compositions for oral
administration of peptides. USP 0014247
33 Kidron, M. [Oramed Ltd.] (2011) Methods and compositions for oral
administration of exenatide. USP Application 0046053
34 Eldor, R. et al. (2010) Open-label study to assess the safety and
pharmacodynamics of five oral insulin formulations in healthy subjects.
Diabetes Obes. Metab. 12, 219–223
35 Eldor, R. et al. (2010) A single blind, two-period study to assess the safety
and pharmacodynamics of an orally delivered GLP-1 analog (Exenatide) in
healthy subjects. 70th Meeting of the American Diabetes Association, Florida,
USA, 25–29 June (abstract 6-LB)
36 LeCluyse, E.L. and Sutton, S.C. (1997) In vitro models for selection of
development candidates. Permeability studies to define mechanisms of
absorption enhancement. Adv. Drug Deliv. Rev. 23, 163–183
37 Thassu, D. (2009) Edetic acid. In Handbook of Pharmaceutical Excipients (6th
edn) (Rowe, R.C., Skeskey, P.J., Quinn, M.E., eds), pp. 247–250,
Pharmaceutical Press
38 Lanigan, R.S. and Yamarik, T.A. (2002) Final report on the safety
assessment of EDTA, calcium disodium EDTA, diammonium EDTA,
dipotassium EDTA, disodium EDTA, TEA–EDTA, tetrasodium EDTA,
tripotassium EDTA, trisodium EDTA, HEDTA, and trisodium HEDTA. Int. J.
Toxicol. 21 (Suppl. 2), 95–142
39 Maggio, E.T. (2006) Intravail: highly effective intranasal delivery of
peptide and protein drugs. Expert Opin. Drug Deliv. 3, 529–539
40 Maggio, E.T. and Grasso, P. (2011) Oral delivery of octreotide acetate in
Intravail1 improves uptake, half-life, and bioavailability over
subcutaneous administration in male Swiss Webster mice. Regul. Pept. 167,
233–238
41 Lee, D.W. et al. (2010) Oral delivery of mouse [D-Leu-4]-OB3, a synthetic
peptide amide with leptin-like activity, in male Swiss Webster mice: a
study comparing the pharmacokinetics of oral delivery to intraperitoneal,
subcutaneous, intramuscular, and intranasal administration. Regul. Pept.
160, 129–132
42 Arnold, J.J. et al. (2004) Correlation of tetradecylmaltoside induced
increases in nasal peptide drug delivery with morphological changes in
nasal epithelial cells. J. Pharm. Sci. 93, 2205–2213
43 Kondoh, M. et al. (2008) Targeting tight junction proteins – significance
for drug development. Drug Discov. Today 13, 180–186
44 Johnson, P.H. et al. (2008) Discovery of tight junction modulators:
significance for drug development and delivery. Drug Discov. Today 13,
261–267
45 Deli, M.A. (2009) Potential use of tight junction modulators to reversibly
open membranous barriers and improve drug delivery. Biochim. Biophys.
Acta 1788, 892–910
46 Kondoh, M. et al. (2005) A novel strategy for the enhancement of drug
absorption using a claudin modulator. Mol. Pharmacol. 67, 749–756
47 Suzuki, H. et al. (2011) A toxicological evaluation of a claudin modulator,
the C-terminal fragment of Clostridium perfringens enterotoxin, in mice.
Pharmazie 66, 543–546
48 Salama, N.N. et al. (2006) Tight junction modulation and its relationship
to drug delivery. Adv. Drug Deliv. Rev. 58, 15–28
49 Gutzeit, A. et al. (2010) Feasibility of small bowel flow rate measurement
with MRI. J. Magn. Reson. Imaging 32, 345–351
50 Varum, F.J. et al. (2008) Mucoadhesion and the gastrointestinal tract. Crit.
Rev. Ther. Drug Carrier Syst. 25, 207–258
51 Froehlich, J.M. et al. (2005) Small bowel motility assessment with
magnetic resonance imaging. J. Magn. Reson. Imaging 21, 370–375
52 Schiller, C. et al. (2005) Intestinal fluid volumes and transit of dosage
forms as assessed by magnetic resonance imaging. Aliment. Pharmacol.
Ther. 22, 971–979
53 Fetih, G. et al. (2005) Improvement of absorption enhancing effects of n-
dodecyl-beta-D-maltopyranoside by its colon-specific delivery using
chitosan capsules. Int. J. Pharm. 293, 127–135
54 Van den Mooter, G. (2006) Colon drug delivery. Expert Opin. Drug Deliv. 3,
111–125
55 O’Brien, P.J. et al. (2006) High concordance of drug-induced human
hepatotoxicity with in vitro cytotoxicity measured in a novel cell-based
model using high content screening. Arch. Toxicol. 80, 580–604
56 McDonel, J.L. (1986) Toxins of Clostridium perfringens types A, B, C, D, and
E. In Pharmacology of Bacterial Toxins (Dorner, F. and Drews, H., eds), pp.
477–517, Pergamon Press
57 Argenzio, R.A. et al. (1988) Restitution of barrier and transport function of
porcine colon after acute mucosal injury. Am. J. Physiol. 255 (Pt 1), G62–G71
58 Wallace, J.L. (2008) Prostaglandins, NSAIDs, and gastric mucosal
protection: why doesn’t the stomach digest itself? Physiol. Rev. 88,
1547–1565
59 Leonard, T.W. et al. (2006) Promoting absorption of drugs in humans
using medium-chain fatty acid-based solid dosage forms: GIPET. Expert
Opin. Drug Deliv. 3, 685–692
www.drugdiscoverytoday.com e119