
Ovarian tumors and cysts
40
BENIGN CYSTS AND TUMORS OF OVARIES
-
Upload
muni-venkatesh -
Category
Education
-
view
272 -
download
1
Transcript of Ovarian tumors and cysts
BENIGN CYSTS
AND TUMORS OF
OVARIES

OVARIAN CYSTS
Follicular
Corpus luteum
Dermoid
Endometriomas
Types of cysts
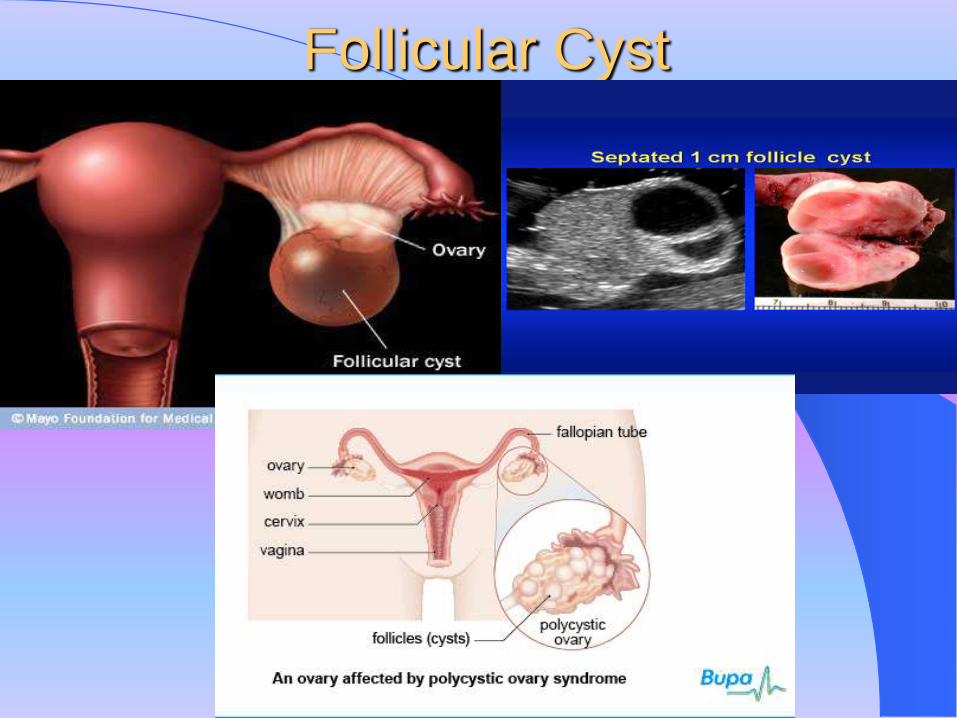
Follicular Cyst
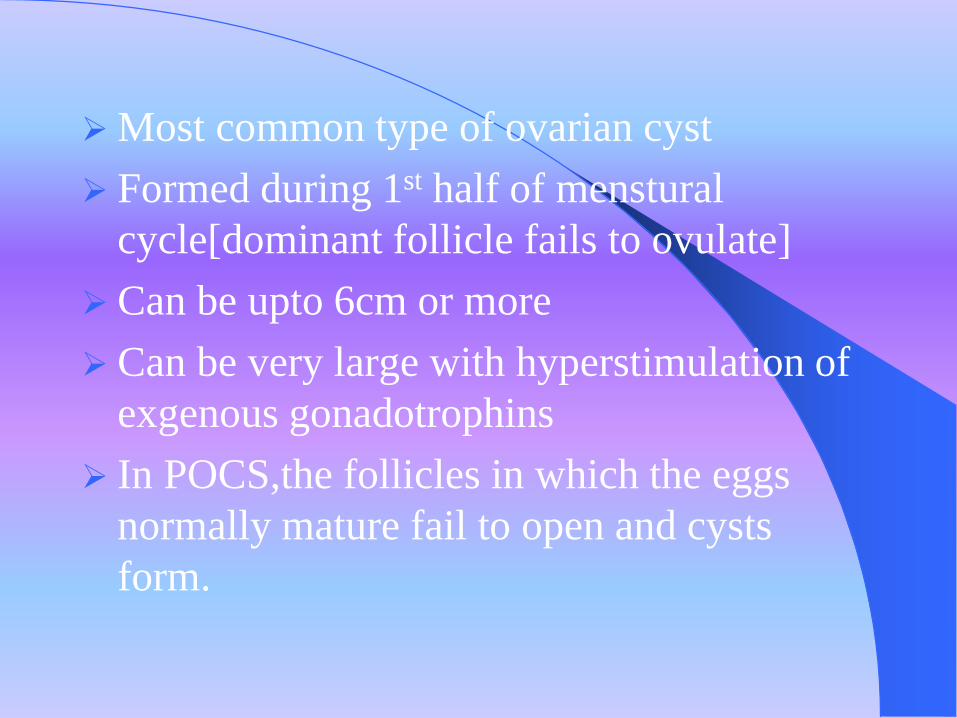
Most common type of ovarian cyst
Formed during 1st half of menstural
cycle[dominant follicle fails to ovulate]
Can be upto 6cm or more
Can be very large with hyperstimulation of
exgenous gonadotrophins
In POCS,the follicles in which the eggs
normally mature fail to open and cysts
form.
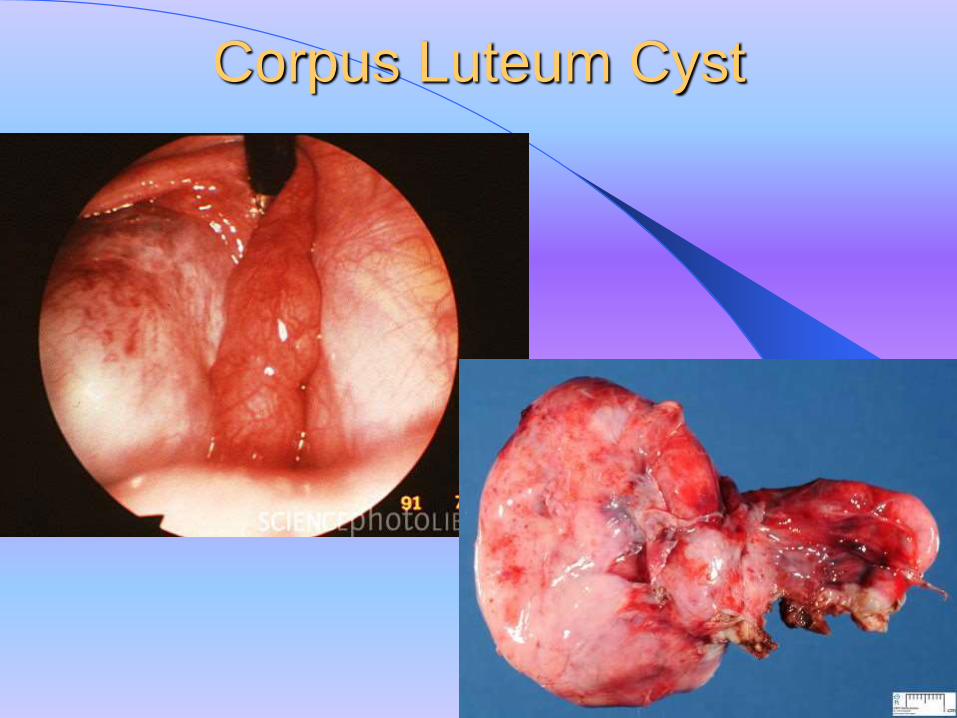
Corpus Luteum Cyst
Formed by hematoma or excessive growth of
corpus luteum
Less common but more clinically significant
than follicular cysts
Formed in the later half of the menstural
cycle
Not larger than 6cm
Formed due excess physiologic blessding
during the vasculization stage of corpus
luteum formation.
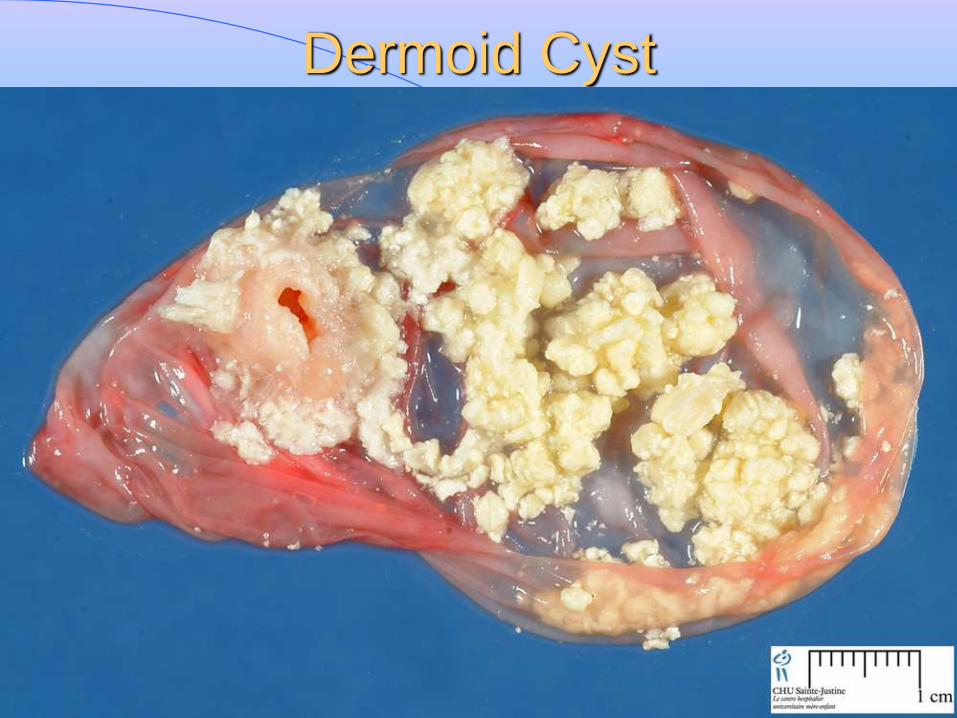
Dermoid Cyst
This type of cyst contains tissue similar to
that in other parts of the body. That
includes skin, hair, and teeth.
Benign cystic teratoma
Most common germ cell neoplasma and
mostly seen in women under 20yrs of age
18-25% of all ovarian tumors
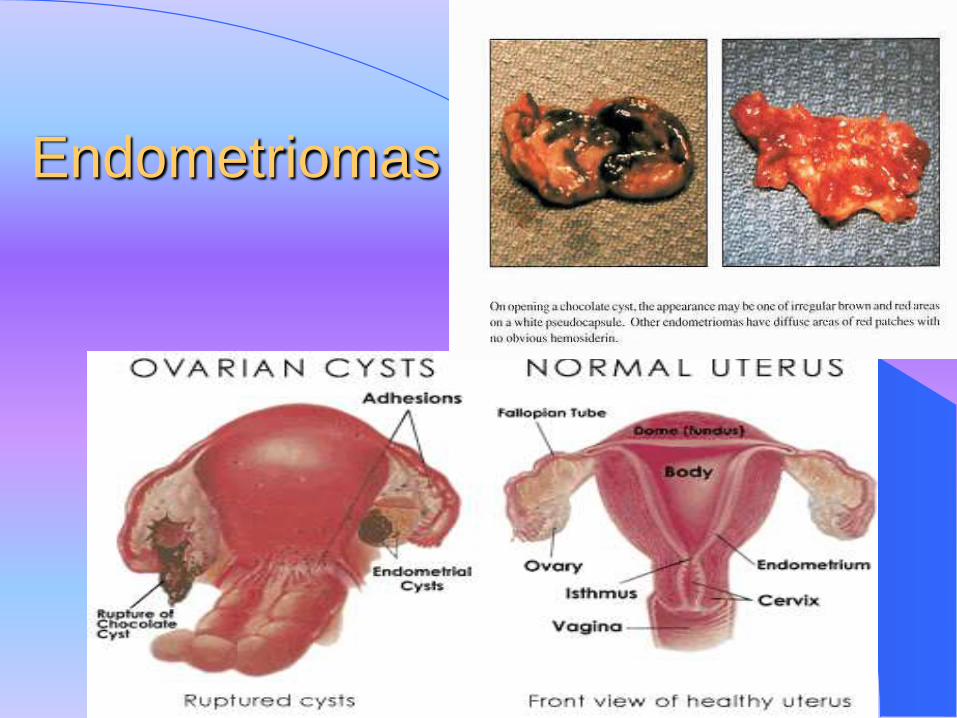
Endometriomas
In women with endometriosis,tissue from the
lining of the uterus grows in other areas of the
body. This includes the ovaries.
Endometriosis can be very painful and can
affect fertility
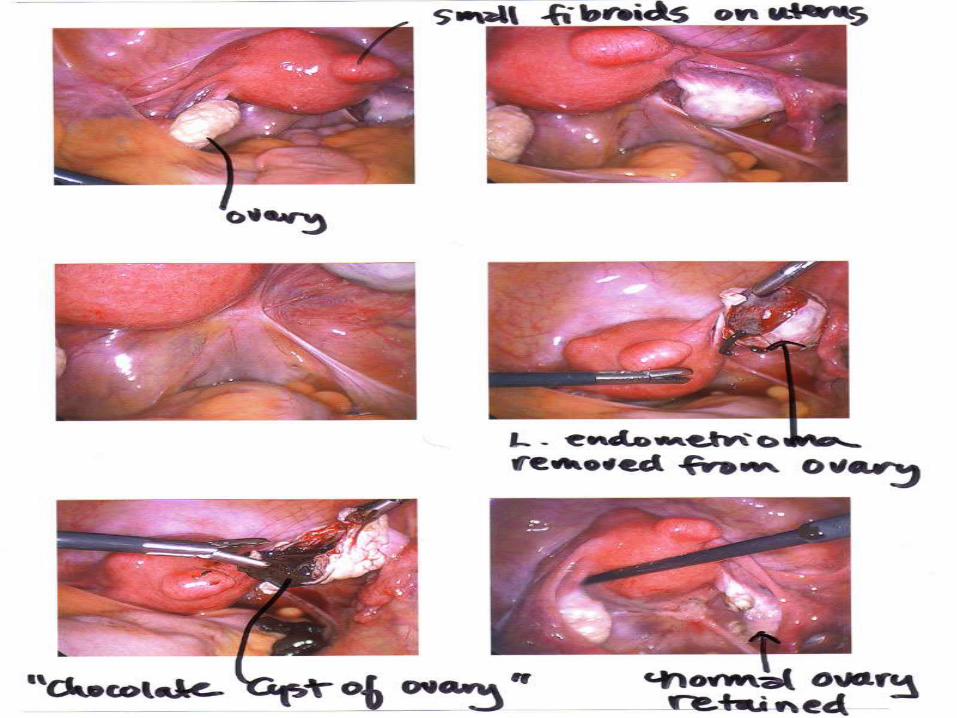
This chocolate cyst is caused by endometriosis,
and formed when a tiny patch of endometrial
tissue (the mucous membrane that makes up the
inner layer of the uterine wall) bleeds, sloughs
off, becomes transplanted, and grows and
enlarges inside the ovaries.

OVARIAN TUMORS
Ovarian Malignancies
Two Major Classifications
NON-EPITHELIAL
Germ cell tumors
Stromal tumors
EPITHELIAL
Epithelial cell tumor
Germ cell Tumors start in the cells that
produce the eggs.
They can either be benign
or cancerous.
Most are benign.
Derived from:
Ectoderm,Mesoderm and
endoderm or any
combination
Germ cell tumors can
be cancerous or non-
cancerous tumors
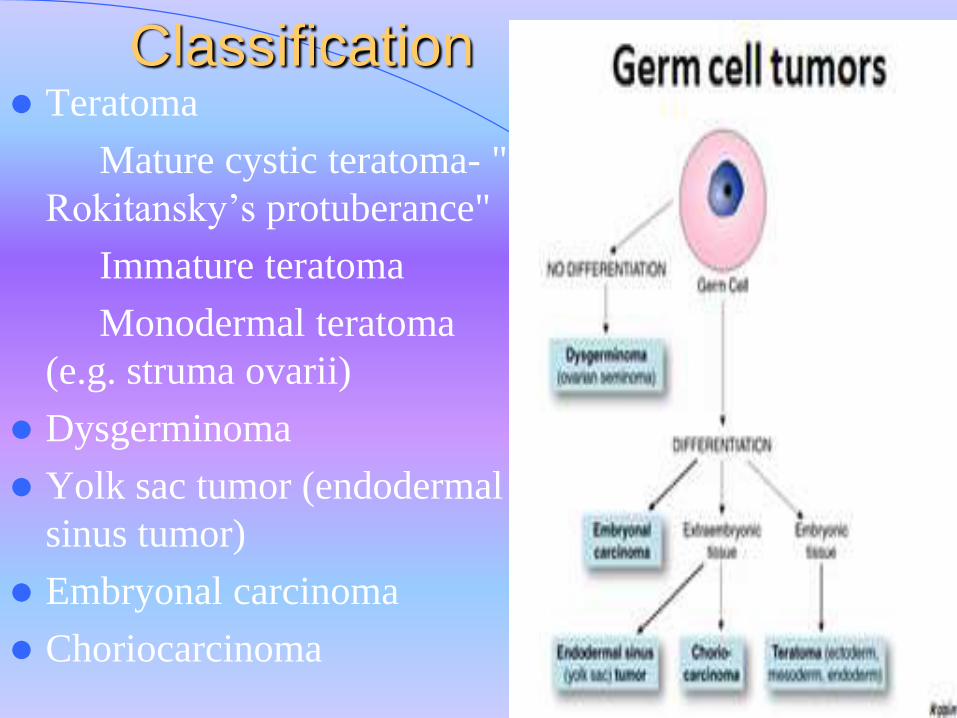
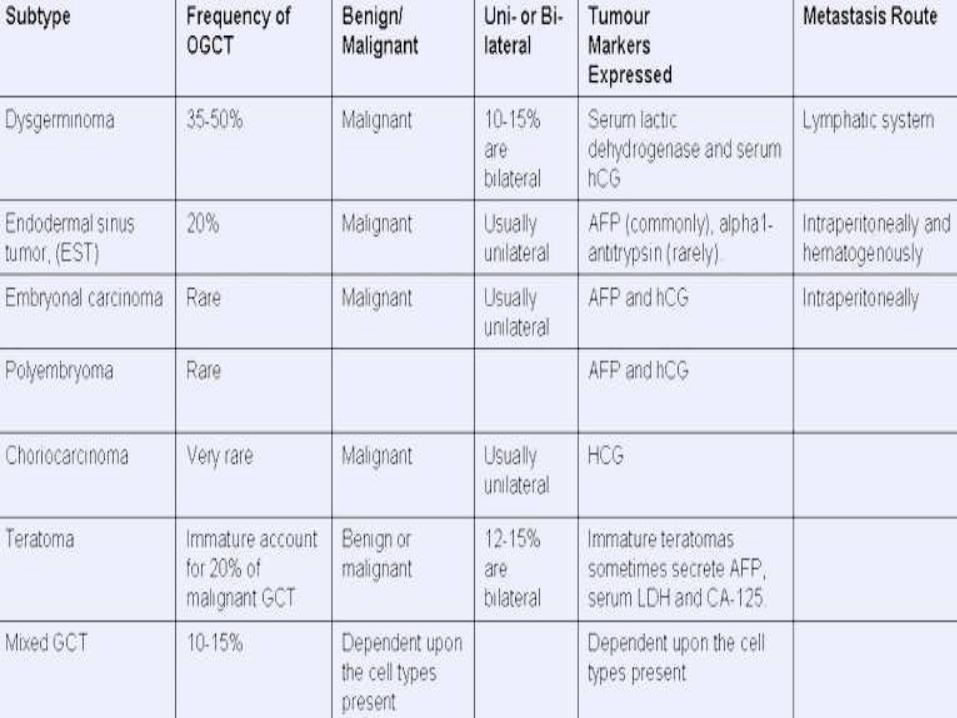
Classification Teratoma
Mature cystic teratoma- "
Rokitansky’s protuberance"
Immature teratoma
Monodermal teratoma
(e.g. struma ovarii)
Dysgerminoma
Yolk sac tumor (endodermal
sinus tumor)
Embryonal carcinoma
Choriocarcinoma
Mature cystic teratoma
most common ovarian teratoma and most
common ovarian germ cell tumor
cystic tumor with firm capsule, filled with
sebaceous material and hair (occasionally
teeth can be found)
thickened area from which hair and teeth
arise is called "Rokitansky's protuberance"
Monodermal teratoma
Monodermal teratoma is composed
predominantly of one tissue element
most common type is "struma ovarii",
which is mature thyroid tissue.
Immature teratoma
occurs in children and young adults
usually a unilateral, solid tumor
similar to mature teratoma but contains
immature or embryonal tissues
Malignant neoplasm
Dysgerminoma
most common malignant ovarian germ cell
tumor
typically occurs in 2nd and 3rd decades
typically a unilateral, solid, firm to fleshy
tumor composed of malignant germ cells,
similar to primordial germ cells
Yolk Sac Tumor
second most common malignant ovarian
germ cell tumor.
occurs in childhood, adolescence, and adult
life (most <30 years)can be pure or a
component of a mixed germ cell tumor
almost always a unilateral solid or solid and
cystic tumor
Embryonal Carcinoma
uncommon ovarian germ cell neoplasm
occurs in children and young adults
usually occurs in combination with yolk sac
tumor
typically a unilateral, solid tumor with
hemorrhage and necrosis composed of
undifferentiated, pleomorphic, large cells

Choriocarcinoma
very rare as a pure ovarian neoplasm or as a
component of a mixed germ cell tumor
occurs in children and young adults
associated with elevated serum hCG levels
typically a unilateral, solid, hemorrhagic
tumor composed of malignant
cytotrophoblast and syncytiotrophoblast
Stromal Cell Tumors
Also known as sex cord-stromal tumor is a
group of tumors of sex cord-derived tissues
of the ovary and testis.
originate in the cells that produce female
hormones.
This group of tumors is significantly less
common than testicular germ cell tumors in
men, and slightly less common than ovarian
germ cell tumours in women.
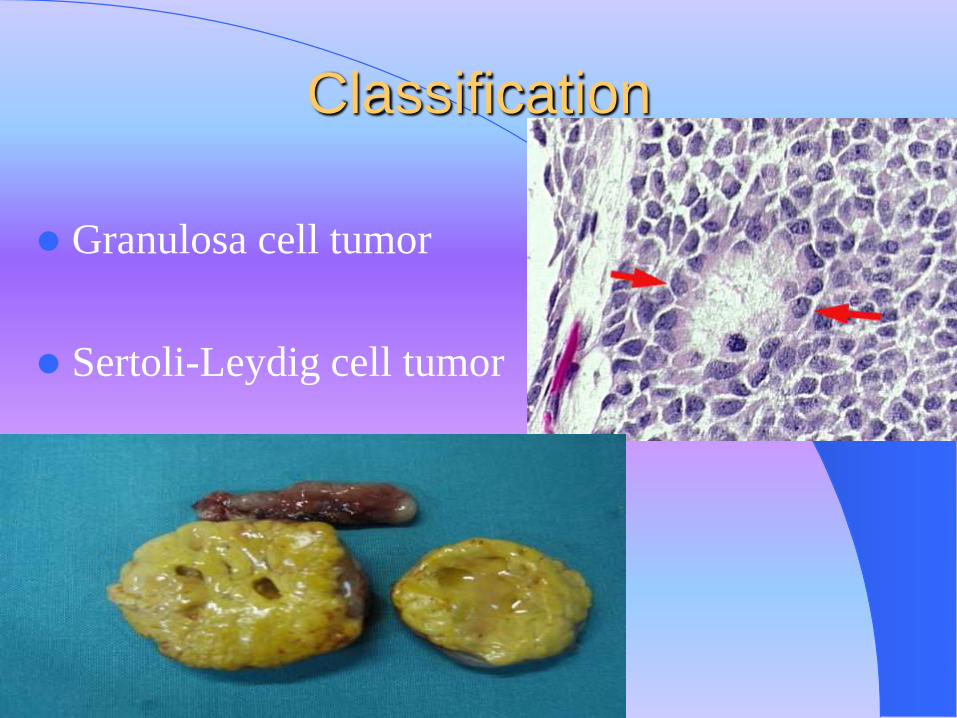
Classification
Granulosa cell tumor
Sertoli-Leydig cell tumor
Granulosa cell tumor
adult form typically occurs at any age after
puberty but is more common in postmenopausal
women
most common clinically estrogenic ovarian tumor
can present with abnormal vaginal bleeding
can be associated with endometrial hyperplasia
and carcinoma
typically a unilateral solid or solid and cystic
tumor, often with hemorrhagic areas
Sertoli-Leydig cell tumor
accounts for less than 0.5% of ovarian tumors
occurs in all age groups but encountered most
often in young women
present with virilization in ~1/3 of cases
(oligomenorrhea, amenorrhea, loss of female
secondary sex characteristics with hirsutism,
clitoromegaly, deepening of voice)
almost always a unilateral tumor that can be
solid, solid and cystic, or even papillary
Epithelial cell tumors start from the cells on the surface of the
ovaries,i.e. germinal epithelium or ovary.
This is the most common form of ovarian
cancer and occurs primarily in adults.
Accounts to 95% of ovarian tumors
Classification Serous
Mucinous
Endometroid
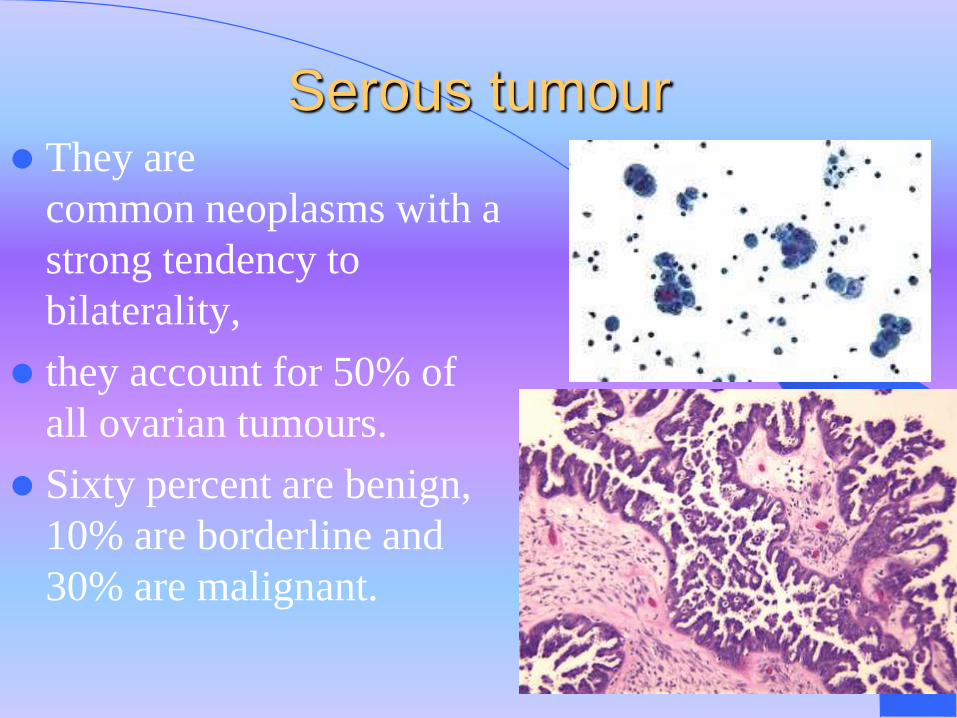
Serous tumour They are
common neoplasms with a
strong tendency to
bilaterality,
they account for 50% of
all ovarian tumours.
Sixty percent are benign,
10% are borderline and
30% are malignant.

Risk Factors
age -- specifically women who have gone through
menopause
smoking
obesity
not having children or not breastfeeding (however,
using birth control pills seems to lower the risk)
fertility drugs (such as Clomid)
hormone replacement therapy
family or personal history of ovarian, breast, or
colorectal cancer (having the BRCA gene can increase
the risk)

Symptoms
Pain or bloating in the abdomen
difficulty urinating, or frequent need to urinate
dull ache in the lower back
pain during sexual intercourse
painful menstruation and abnormal bleeding
weight gain
nausea or vomiting
loss of appetite, feeling full quickly
Complication of ovarian
tumors
Torsion
- common with dermoid/fibroma
- Severe abdominal pain/vomitting
Rupture
Haemorrhage
Impaction
infection
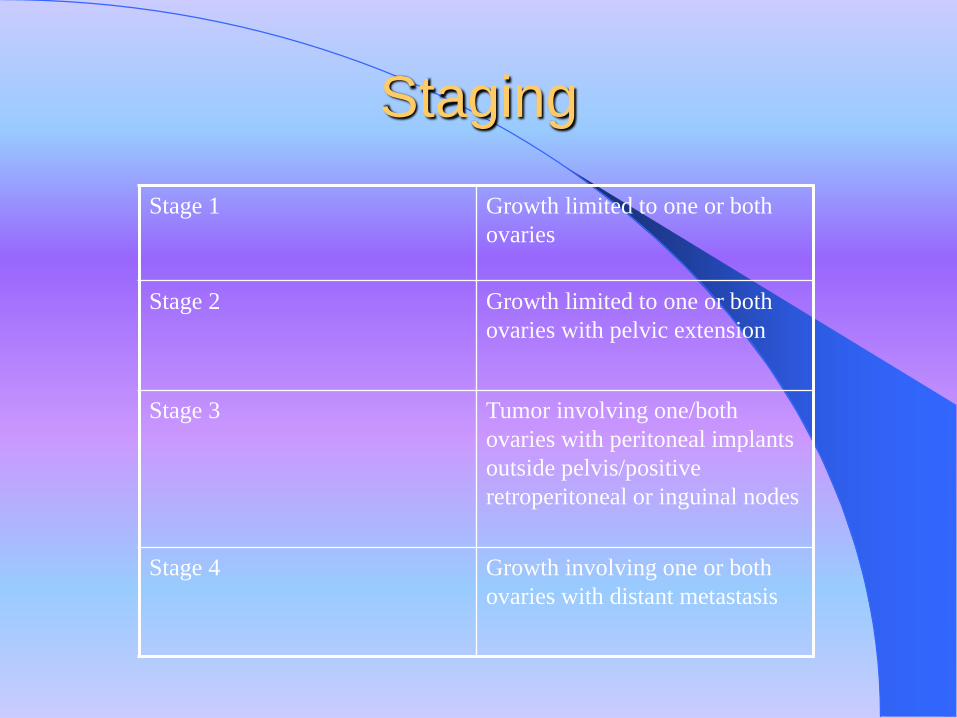
Staging
Stage 1 Growth limited to one or both
ovaries
Stage 2 Growth limited to one or both
ovaries with pelvic extension
Stage 3 Tumor involving one/both
ovaries with peritoneal implants
outside pelvis/positive
retroperitoneal or inguinal nodes
Stage 4 Growth involving one or both
ovaries with distant metastasis
Ovarian tumor and pregnancy
Found incidentally
Corpus luteal/dermoid
2% are malignant
If discover early and persist , surgery
around 16 weeks
If complicated …operate immediately
Physical signs
Benign:
- usually mobile.unless large or complicated
- Dermoid cyst anterior to bladder
• Malignant:
- Bilateral
- Ascites
- Hard deposit in pelvis
- Leg edema
- Signs of bowel obstruction ,of ureteric obstruction
Investigation
CT scan
Tumor markers(ca125,CEA,HCG,alpha FP)
Urea and electrolyte
Chest X ray
Ultrasound
PAP smear
Treatment The treatment of ovarian cancers based on the stage of
the disease which is a reflection of the extent or spread of the cancer to other parts of the body.
It also depends on histologic cell type, and the patient's age and overall condition.
There are basically three forms of treatment of ovarian cancer:– surgery
– Chemotherapy
– radiation treatment

Other Therapies
Vaccines
Gene therapy
Immunotherapy
Acupuncture
massage therapy
herbal supplements
vitamin supplements
special diets
meditation/relaxation therapy


















