
Ovarian sarcoma
10
GYNECOLOGIC ONCOLOGY 26, 183-192 (1987) Ovarian Sarcoma’ BARRIE ANDERSON, M.D.,” DEBORAH A. TURNER, M.D., AND Jo BENDA, M.D.* Departments qf Obstetrics and Gyr~ecology~ und *Puthology, University qf Iowa Hospitals and Clinics, lo~u City, IONW 52242 Received October 29, 1985 A 30-year review of primary ovarian sarcomas seen at The University of Iowa Hospitals and Clinics and a review of the literature are presented. Stage at presentation and resectability were the most significant prognostic indicators. Most recurrences appeared outside the pelvis, indicating a need for systemic chemotherapy. With aggressive treatment, patients with early stage disease can have long term survival. A plea is made for multicenter protocols to develop effective programs of treatment. C 19X7 Academ,c Pre,\. Inc. Primary ovarian sarcomas are rare. Hanjani [l] found 193 reported cases and added 8 cases of his own. Morrow [2] published the GOG experience with 30 cases. Review of recent literature for this report yielded an additional 54 cases 13-201. The 14 cases described here bring the reported total to 299. Prognosis is described as poor with treatment varied and unorganized and response to treatment minimal. This report summarizes the literature and presents the experience with ovarian sarcomas at The University of Iowa Hospitals and Clinics. MATERIALS AND METHODS Records of all patients with ovarian sarcoma seen at The University of Iowa Hospitals and Clinics between 1952 and 1982 were reviewed. Data collected included age, race, gynecologic history, pregnancy history, presenting symptoms, history of current or prior second malignancy, treatment, and follow-up. All histologic slides were reviewed by one author (J.B.) for this report. RESULTS Fourteen patients with a diagnosis of sarcoma were seen and treated at The University of Iowa Hospitals and Clinics between 1952 and 1982. They ranged in age from 21 to 65, with a median age of 57.5 years (Table 1). All were white. During that same time 1353 patients with all ovarian cancers were seen with an age ’ Preliminary data presented at the Eleventh Annual Meeting of the Western Association of Gynecologic Oncologists, May, 1983. ’ To whom reprint requests should be addressed: Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, University of Iowa Hospitals and Clinics, Iowa City, Iowa 52242. 183 0090-8258187 $1 SO Copyright 0 1987 by Academic Press, Inc. All rights of reproductmn in any form reserved.
-
Upload
barrie-anderson -
Category
Documents
-
view
224 -
download
2
Transcript of Ovarian sarcoma
GYNECOLOGIC ONCOLOGY 26, 183-192 (1987)
Ovarian Sarcoma’
BARRIE ANDERSON, M.D.,” DEBORAH A. TURNER, M.D., AND Jo BENDA, M.D.*
Departments qf Obstetrics and Gyr~ecology~ und *Puthology, University qf Iowa Hospitals and Clinics, lo~u City, IONW 52242
Received October 29, 1985
A 30-year review of primary ovarian sarcomas seen at The University of Iowa Hospitals and Clinics and a review of the literature are presented. Stage at presentation and resectability were the most significant prognostic indicators. Most recurrences appeared outside the pelvis, indicating a need for systemic chemotherapy. With aggressive treatment, patients with early stage disease can have long term survival. A plea is made for multicenter protocols to develop effective programs of treatment. C 19X7 Academ,c Pre,\. Inc.
Primary ovarian sarcomas are rare. Hanjani [l] found 193 reported cases and added 8 cases of his own. Morrow [2] published the GOG experience with 30 cases. Review of recent literature for this report yielded an additional 54 cases 13-201. The 14 cases described here bring the reported total to 299. Prognosis is described as poor with treatment varied and unorganized and response to treatment minimal.
This report summarizes the literature and presents the experience with ovarian sarcomas at The University of Iowa Hospitals and Clinics.
MATERIALS AND METHODS
Records of all patients with ovarian sarcoma seen at The University of Iowa Hospitals and Clinics between 1952 and 1982 were reviewed. Data collected included age, race, gynecologic history, pregnancy history, presenting symptoms, history of current or prior second malignancy, treatment, and follow-up. All histologic slides were reviewed by one author (J.B.) for this report.
RESULTS
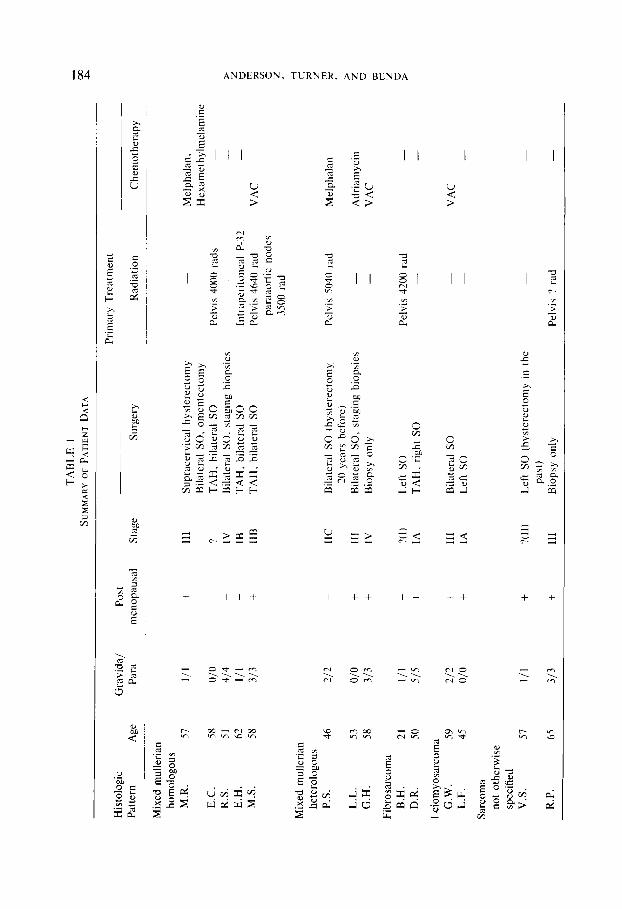
Fourteen patients with a diagnosis of sarcoma were seen and treated at The University of Iowa Hospitals and Clinics between 1952 and 1982. They ranged in age from 21 to 65, with a median age of 57.5 years (Table 1). All were white. During that same time 1353 patients with all ovarian cancers were seen with an age
’ Preliminary data presented at the Eleventh Annual Meeting of the Western Association of Gynecologic Oncologists, May, 1983.
’ To whom reprint requests should be addressed: Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, University of Iowa Hospitals and Clinics, Iowa City, Iowa 52242.
183 0090-8258187 $1 SO
Copyright 0 1987 by Academic Press, Inc. All rights of reproductmn in any form reserved.
TABL
E I
SUM
MAR
Y OF
PA
TIEN
T DA
TA
E
Prim
ary
Trea
tmen
t
Radi
atio
n Gr
avida
/ Pa
ra
Post
m
enop
ausa
l St
age
Surg
ery
Hist
olog
ic Pa
ttern
Ag
e
Mixe
d m
ulle
rian
hom
olog
ous
M.R
. 57
Chem
othe
rapy
Melp
halan
, He
xam
ethy
lmela
mine
-
VAC
l/l
+ 11
1 Su
prac
ervic
al hy
stere
ctom
y Bi
late
ral
SO,
omen
tecto
my
TAH,
bi
late
ral
SO
Bila
tera
l SO
, st
agin
g bi
opsie
s TA
H.
bila
tera
l SO
TA
H,
bila
tera
l SO
Pelvi
s 40
00
rads
Intrd
perit
onea
l P-
32
Pelvi
s 46
40
rad
para
aorti
c no
des
3500
ra
d
E.C.
58
R.
S.
51
E.H.
62
M
.S.
58
‘7 IV
+ IB
+
IIB
Mixe
d m
ulle
rian
hete
rolog
ous
P.S.
46
2/
2 IIC
+ 11
1 +
IV
Bila
tera
l SO
(h
yste
recto
my
20
year
s be
fore
) Bi
late
ral
SO,
stag
ing
biop
sies
Biop
sy
only
- ‘?(
I )
Left
SO
+ IA
TA
H,
right
SO
+ 11
1 +
IA
Bila
tera
l SO
Le
ft so
Pelvi
s 50
40
rad
-
Melp
halan
Adria
myc
in VA
C L.
L.
53
G.H.
58
Fibr
osar
com
a B.
H.
21
D.R.
so
Leiom
yosa
rcom
a G.
W.
59
L.F.
45
Sarc
oma
not
othe
rwise
sp
ecifie
d V.
S.
57
o/o
313 I/I
515
Pelvi
s 42
00
rad
-
212
O/O
VAC
-
111
3/3
+ ?(
11)
+ 11
1
Left
SO
(hys
tere
ctom
y in
th
e pa
st)
Biop
sy
only
Pelvi
s ?
rad
R.P.
65
Hist
olog
ic Pa
ttern
__
____
Mixe
d m
ulle
rian
hom
olog
ous
M.R
. E.
C.
R.S.
E.
H.
M.S
.
Mixe
d m
ulle
rian
hete
rolog
ous
P.S.
L.
L.
G.H.
Fibr
osar
com
a B.
H.
D.R.
Leiom
yosa
rcom
a G.
W.
L.F.
Sarc
oma
not
othe
rwise
sp
ecifie
d V.
S.
R.P
Age
Rem
issio
n tim
e (m
onth
s)
57
0
58
30
51
0 62
48
58
60
+
46
0
53
0
58
0
21
50
59
0
45
36
57
4 65
0 13
16
8
Recu
rrenc
e/
prog
ress
ion
treat
men
t
Adria
myc
in VA
C,
plat
inum
Adria
myc
in an
d Cy
toxan
Cy
toxan
(fo
r ac
quire
d Fa
ctor
VIII
defic
ienc
y,
no
tum
or
recu
rrenc
e)
PAC
Adria
myc
in
Pelvi
c tu
mor
37
50
rad
Actin
omyc
in-D
, ra
diat
ion
3000
ra
d to
ch
est
- -
Surv
ival
time
Pres
ent
(mon
ths)
st
atus
4 DO
D 48
DO
D 2
DOD
52
DOD
60+
Alive
NE
D
30
DOD
24
DOD
4 DO
D
19
DOD
168
Alive
NE
D
18
DOD
54
DOD
9 DO
D 1;
DO
D
Note
. SO
, sa
lping
-oop
hore
ctom
y; TA
H,
tota
l ab
dom
inal
hy
stere
ctom
y; VA
C,
vincr
istin
e,
actin
omyc
in-D,
cy
toxa
n;
PAC.
cis
-pla
tinum
, ad
riam
ycin,
cy
toxa
n;
DOD,
de
ad
of
dise
ase;
NE
D,
no
evide
nce
of
dise
ase.
-. -
-
186 ANDERSON, TURNER, AND BENDA
range of 3 to 93 and a median age of 56. Ninety-seven percent were white, and 1.0% black. Sarcomas, therefore, represented 1.0% of all ovarian cancers seen.
Review of the gynecologic history of the patients with ovarian sarcoma revealed that 93% had a history of regular menses and 57% were postmenopausal at the time of diagnosis. Twenty-one percent were nulliparous but 50% had had two or more children. Twenty-one percent had undergone prior gynecologic operative procedures for benign disease.
The primary presenting symptoms were abdominal discomfort, increase in abdominal girth, and change in GI or urinary habits. Only one patient had postmenopausal bleeding. Eleven (79%) had abdominal or pelvic masses appreciated at initial examination.
No patient had a prior history of radiation therapy and none had a history or concomitant finding of endometriosis. However, the malignant epithelial component was endometrioid in all the mixed mullerian tumors.
Two second malignancies were seen in these patients. One had a concomitant endometrioid carcinoma of the ovary. The other had had breast cancer treated surgically 8 years before the diagnosis of ovarian sarcoma with no evidence of recurrent breast disease.
Five patients presented with Stage I or 11 disease. Three were unstaged in that they had not had appropriate staging biopsies but, in reviewing their records, had no gross evidence of spread outside the pelvis at the time of surgery. Six were Stage III and IV.
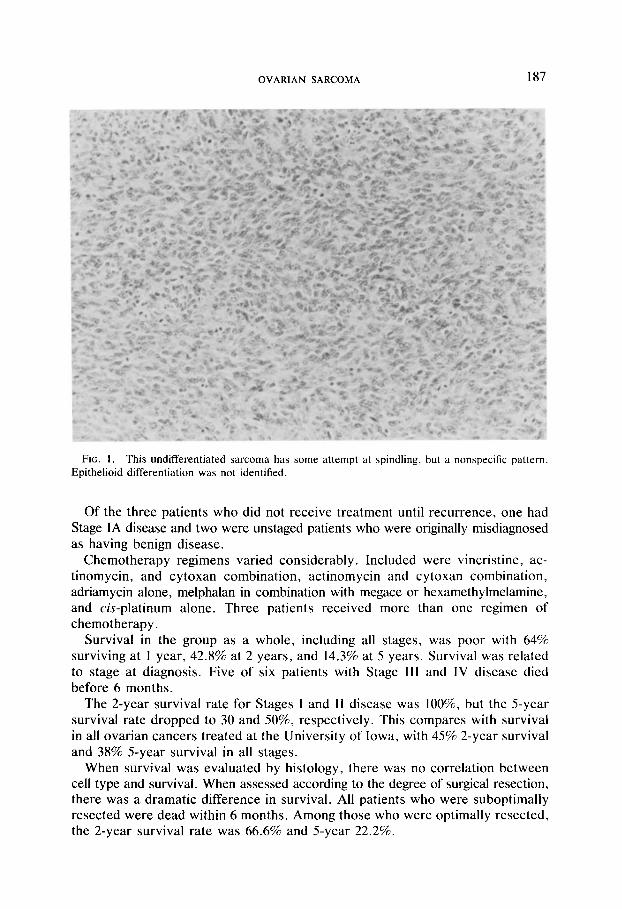
Five histopathologic patterns were identified. Two were undifferentiated sarcomas (Fig. 1); two were fibrosarcomas (Fig. 2); three were leiomyosarcomas (Fig. 3); and eight were mixed mullerian sarcomas, five homologous (Fig. 4) and three heterologous (Figs. 5 and 6).
One patient with fibrosarcoma was 21 and all the rest were over 40. No correlation between histologic pattern and menstrual status or stage at presentation was seen.
TREATMENT
All patients underwent primary surgical procedures which varied from total abdominal hysterectomy with bilateral salpingo-oophorectomy and omentectomy with varied biopsies, to biopsy only for unresectable disease. Nine were felt to be optimally resected and five suboptimally resected.
Following initial surgery, three patients received no further therapy; two were Stage III and IV and died before treatment could be initiated, and one had Stage IA disease.
Eleven patients received further therapy. Four received chemotherapy alone, five chemotherapy and radiotherapy, and two radiotherapy alone.
Eight of these eleven patients received treatment immediately postoperatively, while three were not treated until the time of recurrence. Of the patients treated initially, four were Stage III and IV and received chemotherapy, two were Stage IIB and received chemotherapy and pelvic radiation, one patient was Stage IA and received intraperitoneal P-32, and one unstaged patient received pelvic radiation.
OVARIAN SARCOMA 187
FIG. 1. This undifferentiated sarcoma has some attempt at spindling, but a nonspecific pattern. Epithelioid differentiation was not identified.
Of the three patients who did not receive treatment until recurrence, one had Stage IA disease and two were unstaged patients who were originally misdiagnosed as having benign disease.
Chemotherapy regimens varied considerably. Included were vincristine, ac- tinomycin, and cytoxan combination, actinomycin and cytoxan combination, adriamycin alone, melphalan in combination with megace or hexamethylmelamine, and &-platinum alone. Three patients received more than one regimen of chemotherapy.
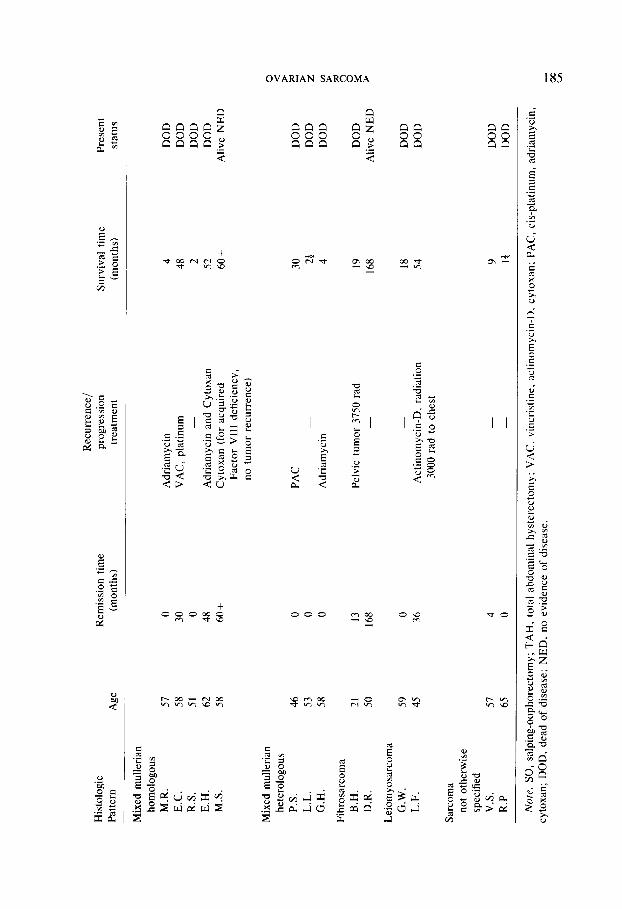
Survival in the group as a whole, including all stages, was poor with 64% surviving at 1 year, 42.8% at 2 years, and 14.3% at 5 years. Survival was related to stage at diagnosis. Five of six patients with Stage III and IV disease died before 6 months.
The 2-year survival rate for Stages I and II disease was lOO%, but the 5-year survival rate dropped to 30 and 50%, respectively. This compares with survival in all ovarian cancers treated at the University of Iowa, with 45% 2-year survival and 38% 5-year survival in all stages.
When survival was evaluated by histology, there was no correlation between cell type and survival. When assessed according to the degree of surgical resection, there was a dramatic difference in survival. All patients who were suboptimally resected were dead within 6 months. Among those who were optimally resected, the 2-year survival rate was 66.6% and 5-year 22.2%.
188 ANDERSON, TURNER, AND BENDA
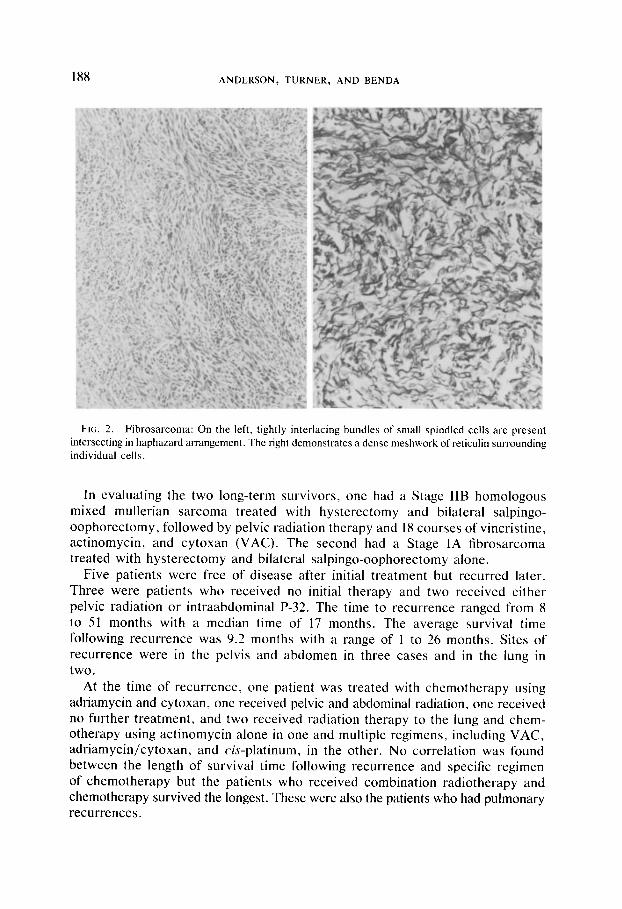
FIG. 2. Fibrosarcoma: On the left, tightly interlacing bundles of small spindled ceils are present intersecting in haphazard arrangement. The right demonstrates a dense meshwork of reticulin surrounding individual cells.
In evaluating the two long-term survivors, one had a Stage IIB homologous mixed mullerian sarcoma treated with hysterectomy and bilateral salpingo- oophorectomy, followed by pelvic radiation therapy and 1X courses of vincristine, actinomycin, and cytoxan (VAC). The second had a Stage IA fibrosarcoma treated with hysterectomy and bilateral salpingo-oophorectomy alone.
Five patients were free of disease after initial treatment but recurred later. Three were patients who received no initial therapy and two received either pelvic radiation or intraabdominal P-32. The time to recurrence ranged from 8 to 51 months with a median time of 17 months. The average survival time following recurrence was 9.2 months with a range of I to 26 months. Sites of recurrence were in the pelvis and abdomen in three cases and in the lung in two.
At the time of recurrence, one patient was treated with chemotherapy using adriamycin and cytoxan, one received pelvic and abdominal radiation, one received no further treatment, and two received radiation therapy to the lung and chem- otherapy using actinomycin alone in one and multiple regimens, including VAC, adriamycin/cytoxan, and c&platinum, in the other. No correlation was found between the length of survival time following recurrence and specific regimen of chemotherapy but the patients who received combination radiotherapy and chemotherapy survived the longest. These were also the patients who had pulmonary recurrences.
OVARIAN SARCOMA 189
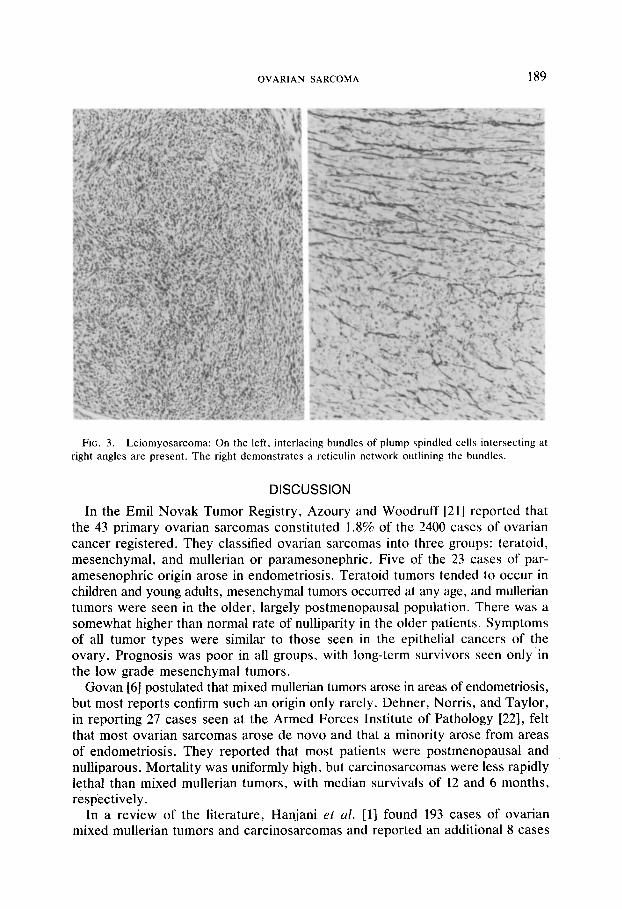
FIG. 3. Leiomyosarcoma: On the left, interlacing bundles of plump spindled cells intersecting at right angles are present. The right demonstrates a reticulin network outlining the bundles.
DISCUSSION
In the Emil Novak Tumor Registry, Azoury and Woodruff [21] reported that the 43 primary ovarian sarcomas constituted 1.8% of the 2400 cases of ovarian cancer registered. They classified ovarian sarcomas into three groups: teratoid, mesenchymal, and mullerian or paramesonephric. Five of the 23 cases of par- amesenophric origin arose in endometriosis. Teratoid tumors tended to occur in children and young adults, mesenchymal tumors occurred at any age, and mullerian tumors were seen in the older, largely postmenopausal population. There was a somewhat higher than normal rate of nulliparity in the older patients. Symptoms of all tumor types were similar to those seen in the epithelial cancers of the ‘. ovary. Prognosis was poor in all groups, with long-term survivors seen only m the low grade mesenchymal tumors.
Govan [6] postulated that mixed mullerian tumors arose in areas of endometriosis, but most reports confirm such an origin only rarely. Dehner, Norris, and Taylor, in reporting 27 cases seen at the Armed Forces Institute of Pathology [22], felt that most ovarian sarcomas arose de novo and that a minority arose from areas of endometriosis. They reported that most patients were postmenopausal and nulliparous. Mortality was uniformly high, but carcinosarcomas were less rapidly lethal than mixed mullerian tumors, with median survivals of 12 and 6 months, respectively.
In a review of the literature, Hanjani et al. [l] found 193 cases of ovarian mixed mullerian tumors and carcinosarcomas and reported an additional 8 cases
190 ANDERSON, TURNER, AND BENDA
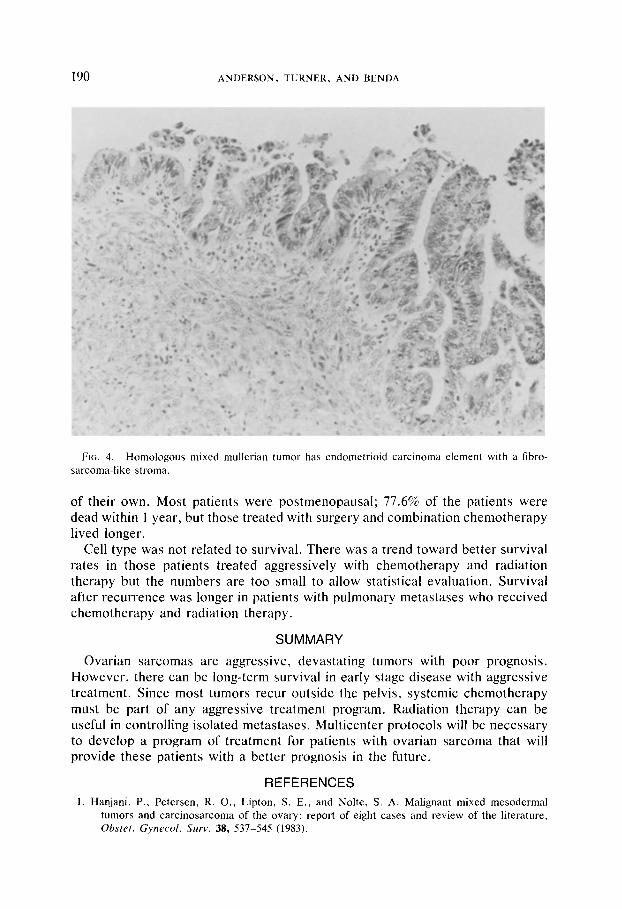
FIG. 4. Homologous mixed mullerian tumor has endometrioid carcinoma element with a fibro- sarcoma-like stroma.
of their own. Most patients were postmenopausal; 77.6% of the patients were dead within 1 year, but those treated with surgery and combination chemotherapy lived longer.
Cell type was not related to survival. There was a trend toward better survival rates in those patients treated aggressively with chemotherapy and radiation therapy but the numbers are too small to allow statistical evaluation. Survival after recurrence was longer in patients with pulmonary metastases who received chemotherapy and radiation therapy.
SUMMARY
Ovarian sarcomas are aggressive, devastating tumors with poor prognosis. However, there can be long-term survival in early stage disease with aggressive treatment. Since most tumors recur outside the pelvis, systemic chemotherapy must be part of any aggressive treatment program. Radiation therapy can be useful in controlling isolated metastases. Multicenter protocols will be necessary to develop a program of treatment for patients with ovarian sarcoma that will provide these patients with a better prognosis in the future.
REFERENCES
1. Hanjani, P., Petersen, R. 0.. Lipton, S. E., and Nolte, S. A. Malignant mixed mesodermal tumors and carcinosarcoma of the ovary: report of eight cases and review of the literature, Ohstet. Gynecol. Sum. 38, 537-545 (1983).

OVARIAN SARCOMA 191
FIG. 5. Heterologous mixed mullerian tumor has endometrioid carcinoma element with inset showing rhabdomyosarcoma differentiation of the stroma.
2. Morrow, C. P., d’Ablaing, G., Brady, L. W., Blessing, J. A., and Hreshchyshyn, M. M. A clinical and pathologic study of 30 cases of malignant mixed mullerian epithelial and mesenchymal ovarian tumors: a Gynecologic Oncology Group study, G~~necol. &co/. 18, 278-292 (1984).
3. Clement, P. B., and Scully, R. E. Extrauterine mesodermal (Mullerian) adenosarcoma. A clinico- pathologic analysis of five cases, A.J.C.P. 69, 276-283 (1978).
4. Connor, E. J., Aydinel, 0. H., Lee, J. S., and Homayouni, M. Leiomyosarcoma of the ovary. in Diagnosis and treatment of ovarian neoplastic alterations (de Watteville, H., et al. Ed.),
Excerpta Medica, Amsterdam (1975). 5. Fukui, H., and Taguchi, K. Mixed mesodermal tumor of the ovary, Ac,ta Pathol. Jupun. 23,
609-614 (1973). 6. Govan, A. D. T. Ovarian tumors: clinical and pathological features, C/in. Ohstet. Gynecol. 3,
89-152 (1976). 7. Ghosh, A. K. Bilateral fibrosarcoma of the ovary following hysterectomy, Amer. J. Obstet.
Gynecol. 112, 1136-1138 (1972). 8. Greenwald, E., Gregori, C. A., and Breen. J. L. Ovarian liposarcoma: a case report, J. Med.
Sot. N. J. 105-107 (1974). 9. Guerard, M. J., Ferenczy, A., and Arguelles, M. A. Ovarian Sertoli-Leydig cell tumor with
rhabdomyosarcoma: an ultrastructural study, Ultrastruc. Pathal. 3, 347-358 (1982). IO. Guerard, M. J., Arguelles, M. A., and Ferenczy, A. Rhabdomyosarcoma of the ovary: ultrastructural
study of a case and review of the literature, Gynecol. Oncol. 15, 325-339 (1983). Il. Hanada, M., Tsujimura, T., and Shimizu, H. Multiple malignancies (squamous cell carcinoma
and sarcoma) arising in a dermoid cyst of the ovary, Acta Pathol. Japan. 31, 681-688 (1981). 12. Nieminen, U., vonNumers, C., and Purola, E. Primary sarcoma of the ovary, Actn Obstet.
Gynecol. Stand. 48, 423-432 (1969). 13. Nunez, C., Abboud, S. L., Lemon, N. C., and Kemp, J. A. Ovarian rhabdomyosarcoma presenting
as leukemia: case report, Cancer 52, 297-300 (1983).

192 ANDERSON, TURNER, AND BENDA
FIG. 6. Heterologous mixed mullerian tumor has endometrioid carcinoma element (left) and stromal osteogenic sarcoma (right).
14. Prat, J.. and Scully, R. E. Sarcomas in ovarian mutinous tumors: a report of two cases. Crrncer 44, 1327-1331 (1979).
15. Prat, J., and Scully, R. E. Cellular fibromas and fibrosarcomas of the ovary: a comparative clinico-pathologic analysis of seventeen cases, Crrnc,er 47, 2663-2670 (198 I ).
16. Russell, P., Slavutin. L., Laverty, C. R., and Cooper-Booth, J. Extrauterine mesodermal (Mullet-tan) adenosarcoma: a case report, Pat/zo/og.v 11, 557-560 (1979).
17. Silverberg, S. G.. and Fernandez, F. N. Endolymphatic stromal myosis of the ovary: a report of three cases and literature review, Gvnc~col. On&. 12, 129-138 (1981).
18. Talerman, A., Anerbach, W. M., and VanMeurs, A. J. Primary chondrosarcoma of the ovary, Histopatldo~y 5, 319-324 (1981).
19. Waits, A. E., and Lichtenstein, 1. Primary leiomyosarcoma associated with serous cystadeno- carcinoma of the ovary, Gynr~col. Oncol. 5, 81-86 (1977).
20. Waxman, M., Vuletin, J. C., Urcuyo, R., and Belling. C. G. Ovarian low-grade stromal sarcoma with thecomatous features: a critical reappraisal of the so-called “malignant thecoma,” Ctrnc,rr 44, 2206-2217 (1979).
21. Azoury. R. S., and Woodruff. J. D. Primary ovarian sarcomas. Report of 43 cases from the Emil Novak Ovarian Tumor Registry, Oh,stet. G.yneco/. 37, 920-941 (1971).
22. Dehner, L. P., Norris, H. J., and Taylor. H. B. Carcinosarcomas and mixed mesodermal tumors of the ovary, Cuncrr 27, 207-216 (1971).
23. Carlson, J. A., Edwards, C., Wharton. J. T., Gallagher, H. S.. Delclos, L., and Rutledge. F. Mixed mesodermal sarcoma of the ovary. Treatment with combination radiation therapy and chemotherapy, Cancer 52, 1473-1477 (1983).












![UTERINE AND OVARIAN SARCOMAS: CLINICAL AND ... · Keywords: uterine sarcoma, ovarian sarcoma INTRODUCTION Sarcomas account for about 5% of uterine neo-plasms [1]. The most common](https://static.fdocuments.us/doc/165x107/5f8cf10c47e4f35e95087e30/uterine-and-ovarian-sarcomas-clinical-and-keywords-uterine-sarcoma-ovarian.jpg)



