
Ovarian cancer
37
Ovarian Cancer
-
Upload
muni-venkatesh -
Category
Education
-
view
265 -
download
0
Transcript of Ovarian cancer
Ovarian Cancer
Background Malignant lesions of the ovaries include primary lesions arising
from normal structures within the ovary and secondary lesions from cancers arising elsewhere in the body. Primary lesions include epithelial ovarian carcinoma (70% of all ovarian malignancies), germ-cell tumors, sex-cord stromal tumors, and other more rare types. Metastases to the ovaries are relatively frequent, with the most common being from the endometrium, breast, colon, stomach, and cervix. Although many histologic types of ovarian tumors have been described, more than 90% of ovarian malignancies are epithelial tumors. (See Pathophysiology.)
The precise cause of ovarian cancer is unknown, but several risk and contributing factors (including both reproductive and genetic factors) have been identified. (See Etiology.)
Ovarian cancer is the most common cause of cancer death from gynecologic tumors in the United States. Around the world, more than 200,000 women are estimated to develop ovarian cancer every year and about 100,000 die from the disease. The lifetime risk of a woman developing epithelial ovarian cancer is 1 in 70. (See Epidemiology.)
Early disease causes minimal, nonspecific, or no symptoms. Therefore, most cases are diagnosed in an advanced stage. The prognosis of ovarian cancer is closely related to the stage at diagnosis; thus, overall, prognosis for these patients remains poor. (See Clinical Presentation and Prognosis.)
Pathophysiology Most theories of the pathophysiology of ovarian
cancer include the concept that it begins with the dedifferentiation of the cells overlying the ovary. During ovulation, these cells can be incorporated into the ovary, where they then proliferate. Ovarian cancer typically spreads to the peritoneal surfaces and omentum.
Ovarian carcinoma can spread by local extension, lymphatic invasion, intraperitoneal implantation, hematogenous dissemination, and transdiaphragmatic passage. Intraperitoneal dissemination is the most common and recognized characteristic of ovarian cancer. Malignant cells can implant anywhere in the peritoneal cavity but are more likely to implant in sites of stasis along the peritoneal fluid circulation. As discussed later, these mechanisms of dissemination represent the rationale to conduct surgical staging, debulking surgery, and intraperitoneal administration of chemotherapy. In contrast, hematogenous spread is clinically unusual
Epithelial ovarian cancer
Epithelial tumors represent the most common histology (90%) of ovarian tumors. Other histologies include the following:
Sex-cord stromal tumors
Germ cell tumors
Primary peritoneal carcinoma
Metastatic tumors of the ovary
Epithelial ovarian cancer is thought to arise from epithelium covering the ovaries, which is derived from the coelomic epithelium in fetal development. This coelomic epithelium is also involved in formation of the Müllerian ducts, from which the Fallopian tubes, uterus, cervix, and upper vagina develop.
Five main histologic subtypes, which are
similar to carcinoma, arise in the epithelial
lining of the cervix, uterus, and fallopian tube,
as follows:
Serous (from fallopian tube)
Endometrioid (endometrium)
Mucinous (cervix)
Clear cell (mesonephros)
Brenner
Some variation is observed in the patterns of spread and
disease distribution within the various histologic subtypes
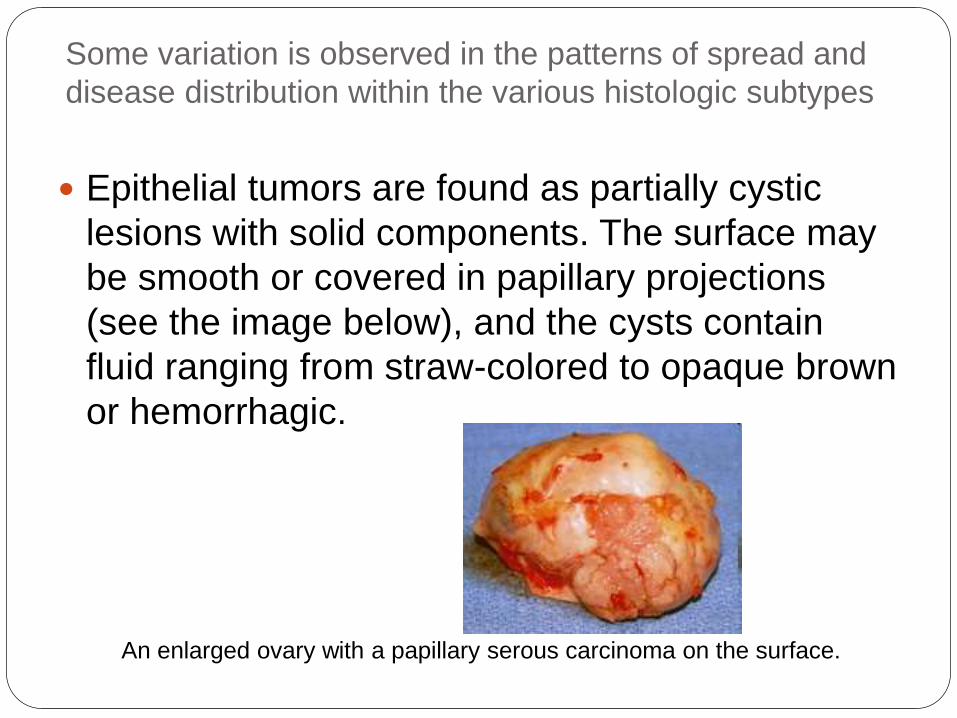
Epithelial tumors are found as partially cystic
lesions with solid components. The surface may
be smooth or covered in papillary projections
(see the image below), and the cysts contain
fluid ranging from straw-colored to opaque brown
or hemorrhagic.
An enlarged ovary with a papillary serous carcinoma on the surface.
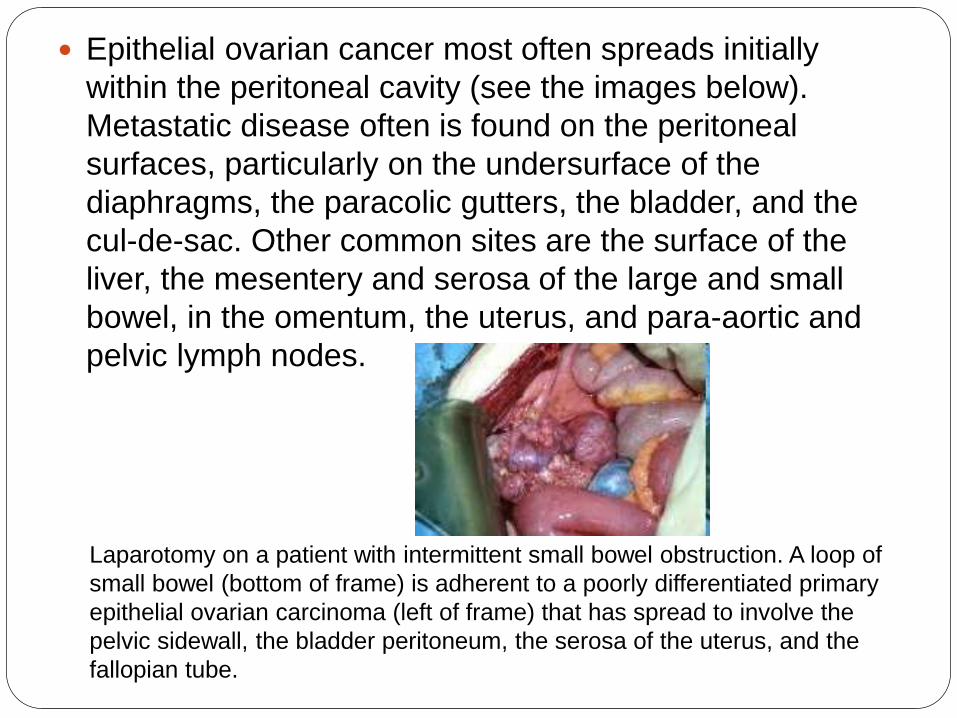
Epithelial ovarian cancer most often spreads initially
within the peritoneal cavity (see the images below).
Metastatic disease often is found on the peritoneal
surfaces, particularly on the undersurface of the
diaphragms, the paracolic gutters, the bladder, and the
cul-de-sac. Other common sites are the surface of the
liver, the mesentery and serosa of the large and small
bowel, in the omentum, the uterus, and para-aortic and
pelvic lymph nodes.
Laparotomy on a patient with intermittent small bowel obstruction. A loop of
small bowel (bottom of frame) is adherent to a poorly differentiated primary
epithelial ovarian carcinoma (left of frame) that has spread to involve the
pelvic sidewall, the bladder peritoneum, the serosa of the uterus, and the
fallopian tube.
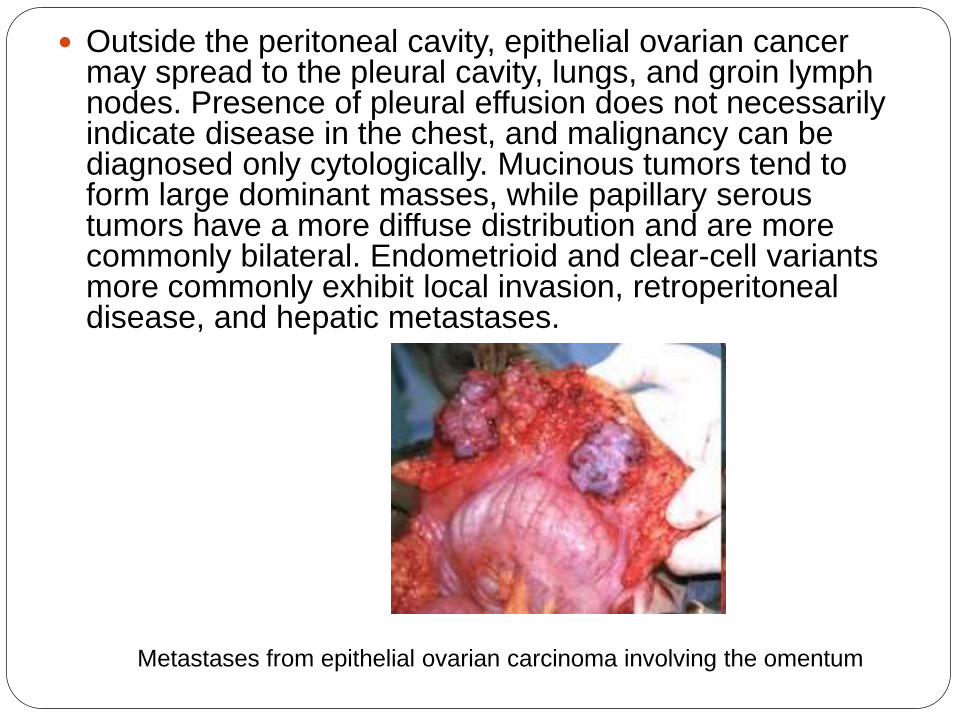
Outside the peritoneal cavity, epithelial ovarian cancer may spread to the pleural cavity, lungs, and groin lymph nodes. Presence of pleural effusion does not necessarily indicate disease in the chest, and malignancy can be diagnosed only cytologically. Mucinous tumors tend to form large dominant masses, while papillary serous tumors have a more diffuse distribution and are more commonly bilateral. Endometrioid and clear-cell variants more commonly exhibit local invasion, retroperitoneal disease, and hepatic metastases.
Metastases from epithelial ovarian carcinoma involving the omentum
Etiology The precise cause of ovarian cancer is
unknown, but several risk and contributing factors have been identified.
Hippisley-Cox and Coupland developed an algorithm to determine risk of breast cancer in women with and without symptoms.[2] , In their cohort study, 10% of women with the highest-predicted risk had 63% of all ovarian cancers diagnosed over the next 2 years.
Reproductive factors
Parity is an important risk factor. The risk of epithelial ovarian cancer is increased in women who have not had children and possibly those with early menarche or late menopause. Women who have been pregnant have a 50% decreased risk for developing ovarian cancer compared with nulliparous women. Multiple pregnancies offer an increasingly protective effect. Oral contraceptive use decreases the risk of ovarian cancer.
These factors support the idea that risk for ovarian cancer is related to ovulation. Two theories regarding this relationship have been proposed. The incessant ovulation theory suggests that repeated ovarian epithelial trauma caused by follicular rupture and subsequent epithelial repair results in genetic alterations within the surface epithelium. The gonadotropin theory proposes that persistent stimulation of the ovaries by gonadotropins, coupled with local effects of endogenous hormones, increases surface epithelial proliferation and subsequent mitotic activity.
Thus, the probability of ovarian cancer may be related to the number of ovulatory cycles, and conditions that suppress the ovulatory cycle may play a protective role. Ovulation suppression has been shown to decrease cancer incidence. Although treatment with agents that induce ovulation in women with infertility has been suggested to increase the incidence of epithelial ovarian cancer, this is unproven.
Genetic factors Family history plays an important role in the risk of developing ovarian
cancer. The lifetime risk for developing ovarian cancer is 1.6% in the general population. This compares with a 4-5% risk when 1 first-degree family member is affected, rising to 7% when 2 relatives are affected. From 5-10% of cases of ovarian cancer occur in an individual with a family history of the disease. Only a small percentage of these patients have an inherited genetic abnormality, and the risk of this occurrence increases with the strength of the family history. Hereditary epithelial ovarian cancer occurs at a younger age (approximately 10 years younger) than nonhereditary epithelial ovarian cancer, but the prognosis may be somewhat better.
At least 2 syndromes of hereditary ovarian cancer are clearly identified, involving either (1) disorders of the genes associated with breast cancer, BRCA1 and BRCA2, or (2) more rarely, genes within the Lynch II syndrome complex. Breast/ovarian cancer syndrome is associated with early onset of breast or ovarian cancer. Inheritance follows an autosomal dominant transmission. It can be inherited from either parent. Most cases are related to the BRCA1 gene mutation. BRCA1 is a tumor suppressor gene that inhibits cell growth when functioning properly; the inheritance of mutant alleles of BRCA1 leads to a considerable increase in risk for developing ovarian cancer.
Women with a history of breast cancer have an increased risk of epithelial ovarian cancer.
In a study by Rafner et al, whole-genome sequencing identified a rare
Previous hormone therapy
A nationwide prospective cohort study over 10 years that included all Danish women aged 50-79 years concluded that risk for ovarian cancer is increased with hormone therapy, regardless of duration of use, formulation, estrogen dose, regimen, progestin type, and administration route.[6] Nearly 1 million women without hormone-sensitive cancer or bilateral oophorectomy were followed. In an average of 8 years of follow-up, 3068 ovarian cancers were detected, of which 2681 were epithelial cancers.
Current users of hormones had incidence rate ratios for all ovarian cancers of 1.38 (95% confidence interval [CI], 11.26-1.51) compared with women who never took hormone therapy. Risk declined as years since last hormone use increased. Incidence rates in current and never users of hormones were 0.52 and 0.40 per 1000 years, respectively. This translates to approximately 1 extra ovarian cancer for approximately 8300 women taking hormone therapy each year
Other factors
Lactose consumption and the use
of talcum powder on the vulva and
perineum may be associated with
increased risk of epithelial ovarian
cancer.
Epidemiology
In the United States, the incidence of ovarian cancer is 33 cases per 100,000 women aged 50 years or older. The average patient age at diagnosis is 57 years. The estimated lifetime risk is 1 case in 70 women, which is a 1.4% lifetime incidence.
International statistics
Internationally, the incidence is 3.1 cases per 100,000 women in Japan and 21 cases per 100,000 women in Sweden. Around the world, more than 200,000 women are estimated to develop ovarian cancer every year and about 100,000 die from the disease. Epithelial ovarian cancer occurs most commonly in white women in the industrialized countries of northern and western Europe and North America and least
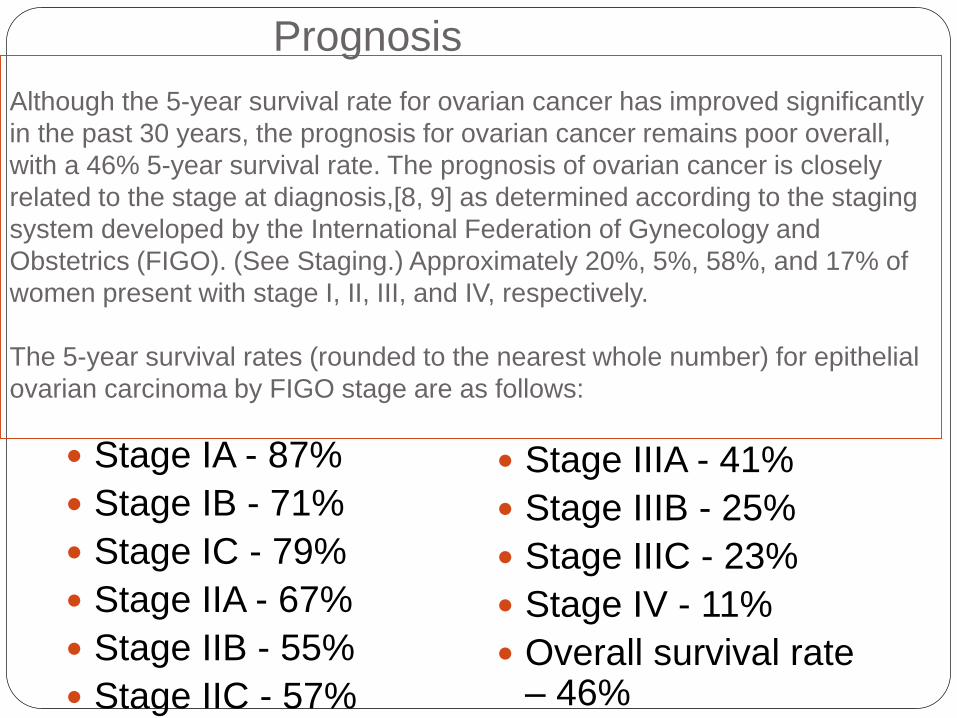
Although the 5-year survival rate for ovarian cancer has improved significantly
in the past 30 years, the prognosis for ovarian cancer remains poor overall,
with a 46% 5-year survival rate. The prognosis of ovarian cancer is closely
related to the stage at diagnosis,[8, 9] as determined according to the staging
system developed by the International Federation of Gynecology and
Obstetrics (FIGO). (See Staging.) Approximately 20%, 5%, 58%, and 17% of
women present with stage I, II, III, and IV, respectively.
The 5-year survival rates (rounded to the nearest whole number) for epithelial
ovarian carcinoma by FIGO stage are as follows:
Stage IA - 87%
Stage IB - 71%
Stage IC - 79%
Stage IIA - 67%
Stage IIB - 55%
Stage IIC - 57%
Stage IIIA - 41%
Stage IIIB - 25%
Stage IIIC - 23%
Stage IV - 11%
Overall survival rate – 46%
Prognosis
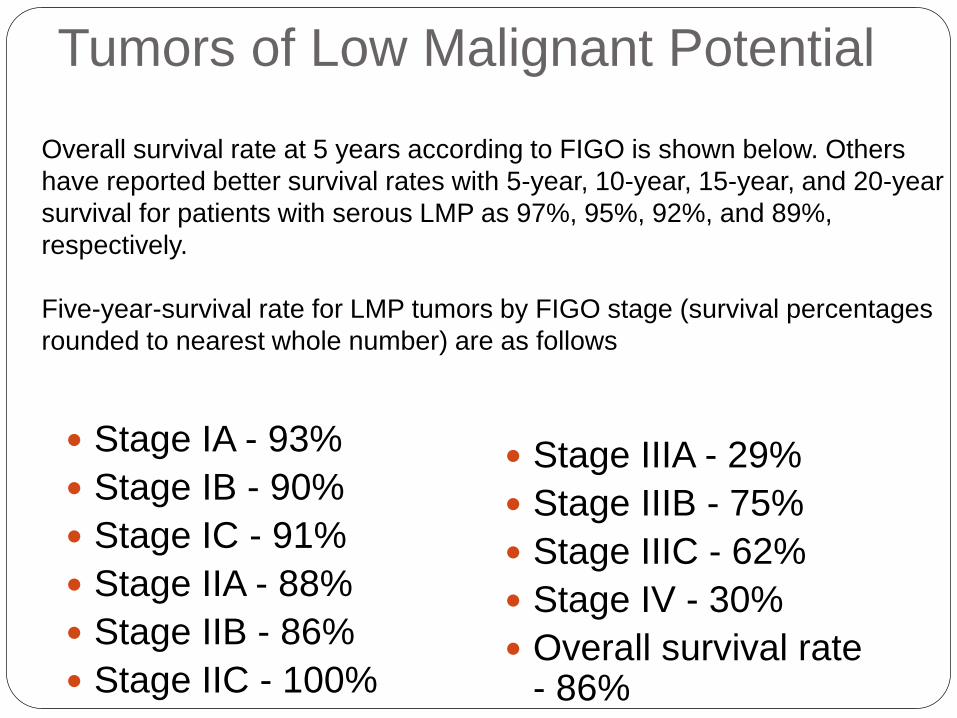
Tumors of Low Malignant Potential
Stage IA - 93%
Stage IB - 90%
Stage IC - 91%
Stage IIA - 88%
Stage IIB - 86%
Stage IIC - 100%
Stage IIIA - 29%
Stage IIIB - 75%
Stage IIIC - 62%
Stage IV - 30%
Overall survival rate - 86%
Overall survival rate at 5 years according to FIGO is shown below. Others
have reported better survival rates with 5-year, 10-year, 15-year, and 20-year
survival for patients with serous LMP as 97%, 95%, 92%, and 89%,
respectively.
Five-year-survival rate for LMP tumors by FIGO stage (survival percentages
rounded to nearest whole number) are as follows
Clinical Presentation History
Assessment of women for their risk of ovarian cancer necessitates obtaining a careful family history of both male and female relatives, including those relatives without cancer.
Carriers of mutations may be detected through laboratory analysis of the genetic structure of white blood cells.
Epithelial ovarian cancer presents with a wide variety of vague and nonspecific symptoms, including bloating, abdominal distension or discomfort, pressure effects on the bladder and rectum, constipation, vaginal bleeding, indigestion and acid reflux, shortness of breath, tiredness, weight loss, and early satiety. The patient may feel an abdominal mass.
A case-control study showed that symptoms independently associated with the presence of ovarian cancer were pelvic and abdominal pain, increased abdominal size and bloating and difficulty eating or feeling full.[13] Another study reported that gastrointestinal (GI) symptoms such as nausea and vomiting, constipation, and diarrhea, or other digestive disorders were associated with later-stage disease.[14] Presentation with swelling of a leg due to venous thrombosis is not uncommon. Paraneoplastic syndromes due to tumor-mediated factors lead to various presentations.
A prospective case-control study of 1,709 women visiting primary care clinics found that the combination of bloating, increased abdominal size, and urinary symptoms was found in 43% of those with ovarian cancer but in only 8% of those presenting to primary care clinics.[15]
Physical Examination
Physical findings are uncommon in
patients with early disease. Patients with
more advanced disease may present
with ovarian or pelvic mass, ascites,
pleural effusion, or abdominal mass or
bowel obstruction.
Diagnostic Considerations The normal functioning ovary produces a follicular cyst 6-7 times
each year. In most cases, these functional masses are self-limiting and resolve within the duration of a normal menstrual cycle. In rare situations, they persist longer or become enlarged. At this point, they represent a pathological condition.
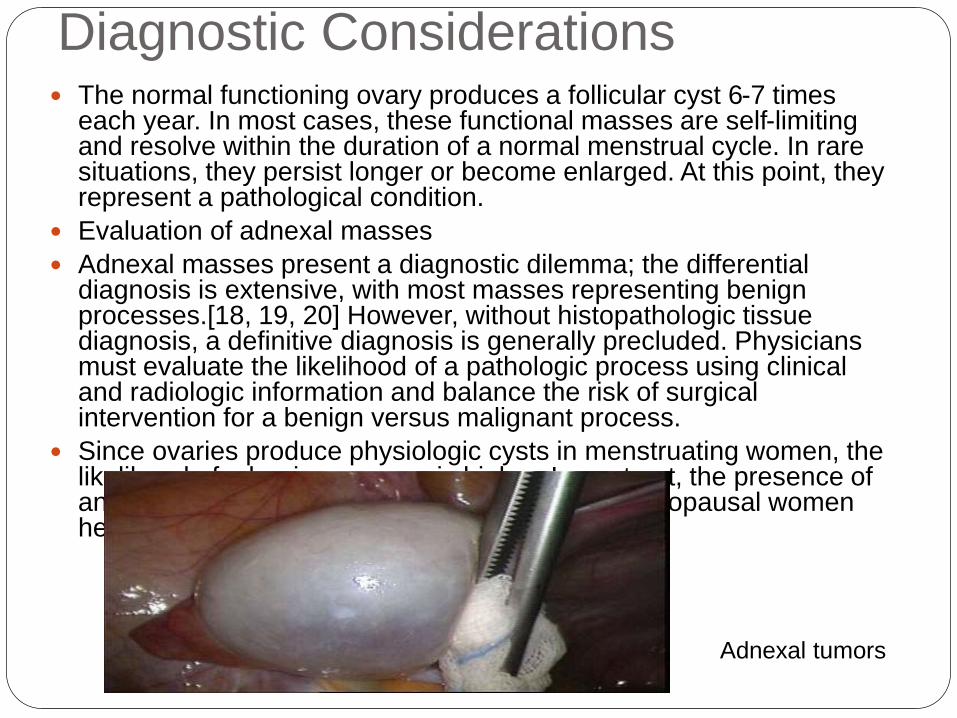
Evaluation of adnexal masses
Adnexal masses present a diagnostic dilemma; the differential diagnosis is extensive, with most masses representing benign processes.[18, 19, 20] However, without histopathologic tissue diagnosis, a definitive diagnosis is generally precluded. Physicians must evaluate the likelihood of a pathologic process using clinical and radiologic information and balance the risk of surgical intervention for a benign versus malignant process.
Since ovaries produce physiologic cysts in menstruating women, the likelihood of a benign process is higher. In contrast, the presence of an adnexal mass in prepubertal girls and postmenopausal women heightens the risk of a pathologic etiology.
Adnexal tumors
Presence of advanced ovarian cancer is often suspected on clinical grounds but can be confirmed only pathologically by removal of the ovaries or, when disease is advanced, by sampling tissue or ascitic fluid.
Routine imaging is not required in all patients in whom ovarian cancer is highly suggested. If diagnostic uncertainty is present, a pelvic ultrasound or CT scan of the abdomen and pelvis is warranted.
MRI can increase the specificity of imaging evaluation in cases where the ultrasound appearance of the lesion is
When imaging studies demonstrate an adnexal mass, the decision whether to observe the patient with repeat imaging or to proceed to surgical evaluation must take into account not only the imaging characteristics but also the patient's medical history, physical examination results, and cancer antigen 125 (CA125) level.[25] Tumor markers such as CA125 are not good discriminators of benign lesions from malignant lesions in premenopausal women but have better accuracy in postmenopausal women
Fine-needle aspiration (FNA) or percutaneous biopsy of an adnexal mass is not routinely recommended. In most cases, this approach may only serve to delay diagnosis and treatment of ovarian cancer. Instead, if a clinical suggestion of ovarian cancer is present, the patient should undergo a laparotomy for diagnosis and staging. An FNA or diagnostic paracentesis should be performed in patients with diffuse carcinomatosis
Screening
Ovarian cancer does not lend itself to screening because it has a relatively low prevalence within the general population and no proven precursor lesion exists that can be detected and treated to prevent the cancer from occurring. No approved screening method is available for ovarian cancer.
The U.S. Preventive Services Task Force (USPSTF) recommends against screening for ovarian cancer in the general population. The USPSTF found fair evidence that although screening with serum CA125 level or transvaginal ultrasonography can detect ovarian cancer at an earlier stage, earlier detection is likely to have a small effect, at best, on mortality from ovarian cancer. In addition, because of the low prevalence of ovarian cancer and the invasive nature of diagnostic testing, the USPSTF concluded that the potential harms outweigh the potential benefits.[26] A randomized trial in a US population found that simultaneous screening with ultrasonography and CA125 did not reduce ovarian cancer mortality, and evaluation of false-positive results was associated with
Currently, the National Cancer Institute (NCI) recommends that high-risk women should seek advice from their physician and consider having annual ultrasonographic examination, annual CA125 testing, and be considered for oophorectomy or participation in a clinical trial. The NCI recommends no screening methodology for women at normal risk for epithelial ovarian cancer, but these women should also be considered for research protocols seeking improved detection methods.
Urinalysis Urinalysis should be obtained to rule out
other possible causes of abdominal or pelvic pain, such as urinary tract infections
Imaging in Ovarian Cancer
Imaging studies used in ovarian cancer include ultrasonography, chest radiography, and magnetic resonance imaging (MRI). Positron emission tomography (PET) scanning does not have an established role in the diagnosis of primary ovarian malignancy.
Ultrasonography is the most useful initial investigation in a patient found to have a pelvic mass. This may define the morphology of the pelvic tumor. In addition, it can determine whether large masses are present in other parts of the abdomen, including in the liver. Chest radiography is useful in helping exclude pulmonary spread of malignant diseases of the ovary. The primary advantage of using MRI in the evaluation of ovarian masses is the ability to employ this modality in the characterization of tissue. The presence of fat, hemorrhage, mucin, fluid, and solid tissue within an ovarian mass can be determined with the aid of MRI. The ability to characterize tissue in this way is most useful in determining whether a mass is definitely benign.
Mammography
The preoperative workup also should include mammography for women older than 40 years who have not had one in the preceding 6-12 months. This is especially important in women with estrogen-producing tumors because these may increase the risk of breast malignancies.
Additionally, breast cancers can metastasize to the ovaries and are often bilateral. Mammography can help rule out the possibility of a nongynecologic
Treatment & Management In women who present with GI carcinomatosis but
without an obvious pelvic mass, an extensive search often fails to identify a primary tumor. These patients can be presumed to have ovarian carcinoma or primary peritoneal carcinoma and treated with cytoreductive surgery followed by platinum-based chemotherapy.
Surgery is the initial treatment of choice, provided patients are medically fit. Patients who are not fit for surgery may be given chemotherapy and considered for surgery later. The aim of surgery is to confirm the diagnosis, define the extent of disease, and resect all visible tumor. The role of cytoreduction was demonstrated by Griffiths in 1975 and has been confirmed by many others.
A retrospective analysis from Lin et al found that epidural anaesthesia and analgesia for ovarian serous adenocarcinoma surgery was associated
Choosing Appropriate Surgery Appropriate surgery depends on whether or not disease is visible
outside the ovaries. It is essential that where no disease is visible outside the ovaries, the patient be adequately surgically staged because the incidence of microscopic metastases is significant. Surgery for patients with stage IV disease should be individualized, particularly when disease is in the liver and above the diaphragm. Patients who are in stage IV because of small-volume disease in the liver, abdominal wall, or lung should undergo cytoreductive surgery if medically fit.
If there is no visible disease outside an ovary, aspirate ascitic fluid for cytology studies. Perform peritoneal washings for cytology if ascites is not present. Remove the ovary and ovarian tumor intact. Perform diaphragmatic scraping or biopsy for cytology studies. Obtain peritoneal biopsy specimens. Perform a subcolic omentectomy. Obtain bilateral para-aortic and pelvic node samples. Obtain biopsy samples of adhesions or other suspicious areas.
If the patient does not desire future fertility, perform a total abdominal hysterectomy and excise the opposite ovary. Remove the appendix if mucinous tumor is present.
If macroscopic disease is visible outside of the ovary, all visible tumor should be removed. This may require extensive surgery, including bowel resection, excision of peritoneal implants, liver resection, omentectomy, and splenectomy.
The extent of bowel resection should depend on the role this plays in
Cytoreductive Surgery
This should be performed by a gynecologic oncologist at the time of initial laparotomy. The volume of residual disease at the completion of surgery represents one of the most powerful prognostic factors. According to the 2011 National Comprehensive Cancer Network (NCCN) ovarian cancer guidelines, residual disease of less than 1 cm is evidence of optimal cytoreduction, although the greatest possible effort should be made to remove all obvious disease. As of this guideline, distal pancreatectomy may be considered in all stages for optimal surgical cytoreduction.[36]
Patients with advanced ovarian cancer are classified in 3 groups as follows, based on the postoperative residual tumor:
Good risk - Microscopic disease outside the pelvis (stage IIIa) or macroscopic disease less than 2 cm outside the pelvis (stage IIIb)
Intermediate risk - Macroscopic disease less than 2 cm outside the pelvis only after surgery
Laparoscopic Surgery
According to guidelines developed by the American College of Obstetricians and Gynecologists, laparoscopy may be used for diagnostic purposes in a patient with low risk for ovarian cancer and to remove cystic masses. The mass must be 10 cm or smaller as viewed by a sonogram, must have a distinct border and no solid parts, and must not be associated with ascites. The serum CA125 level must be normal (< 35 U/mL), and the patient must have no family history of ovarian cancer. If a chance exists that ovarian cancer may be present, surgery is best arranged in conjunction with a specialist in gynecologic cancer surgery. The patient can then undergo all necessary surgery for her cancer under a single anesthetic, without delay.
As part of initial treatment of epithelial ovarian cancer, laparoscopic surgery may be performed for early stage disease when no disease is visible outside of the ovaries. Its use in more advanced disease, when spread is visible outside the ovaries, is more limited due to the scope of cytoreductive surgery necessary and the risk of port-site recurrence. Laparoscopy also has a role in second-look inspection and in the staging of apparently early-stage disease found by chance during another surgery.
The 2011 NCCN ovarian cancer guidelines state that minimally invasive surgery may be considered in selected patients with Stage 1 disease. This is particularly true where an incidental finding of ovarian cancer was made during prophylactic oophorectomy.[36]
Secondary Surgery
An assessment by Park et al found that secondary cytoreductive surgery is safe and effective in patients with platinum-sensitive recurrent ovarian cancer. The surgery was most beneficial in patients who had remained disease free for more than 24 months after primary treatment and in those who achieved
Chemotherapy Regimens
Only a small percentage of women with epithelial ovarian cancer can be treated with surgery alone. These include patients with stage IA grade 1 and stage IB grade 1 serous, mucinous, endometrioid, and Brenner tumors. Clear-cell carcinomas are associated with a significantly worse prognosis in stage I, and patients with this histologic subtype should be considered for chemotherapy at all stages.
Patients not treated with chemotherapy should be monitored closely at regular intervals with clinical examination, serum CA125 estimation, and ultrasonography if an ovary is still present. Surgery to remove the uterus and residual ovary should be considered when the patient no longer desires to remain fertile.
The 2011 NCCN ovarian cancer guidelines recommend pelvic examinations at least every 2-3 cycles in women receiving primary chemotherapy.[36]
Higher-risk early-stage disease includes all histologic subtypes with stage IA and stage IB grade 2 and all stage I grade 3. These patients should be treated with front-line chemotherapy with a taxane/platinum combination for a minimum of 3 courses. They should consider participating in clinical trials.
All patients with stage II cancer and greater should receive front-line chemotherapy and should strongly consider participation in clinical
Radiation Therapy
Radiation has not been widely accepted as a
routine treatment modality in the initial
treatment of patients with epithelial ovarian
cancer, despite reports of efficacy for higher-
risk stage I and II disease and in stage III
disease where small-volume residual disease
is present after surgery. In selected cases,
pelvic diseases may respond to palliative
dosing regimens with minimal toxicity.
Estrogen Replacement Therapy
The safety of estrogen replacement therapy (ERT) after treatment for epithelial ovarian cancer has not been tested in a randomized trial, but current evidence suggests that the benefits of ERT outweigh the risks.
Younger women with endometrioid subtypes are of concern because these tumors theoretically are estrogen-sensitive. If estrogen is used in such patients, a progestogen probably should be given with it.
Management of Recurrent
Disease
In most patients presenting with advanced epithelial ovarian cancer, the disease recurs, and the prognosis for these patients is poor. The goal of further therapy is to achieve a response to treatment and to prolong meaningful quality survival.
Treatment of recurrent disease may involve surgery, chemotherapy, and radiation. Participation in clinical trials should be considered
Experimental Medications
The OCEANS phase III study reported that when bevacizumab (Avastin) was combined with chemotherapy, a 52% risk reduction for recurrence in disease progression was observed (HR=0.48, P < .0001) compared with women who received chemotherapy alone. The study included women with recurrent, platinum-sensitive ovarian, peritoneal, or fallopian tube carcinoma, who received bevacizumab in combination with carboplatin and gemcitabine followed by continued use of bevacizumab alone until disease progression. Other results of the trial include a median progression-free survival of 12.4 months, compared with 8.4 months in women who received chemotherapy alone. Additionally, the overall response rate of tumor shrinkage was 79% in women receiving the bevacizumab-based regimen, compared with 57% in those who received chemotherapy alone.[64]
A study by Stone et al concluded the presence of a paracrine circuit, wherein increased production of thrombopoietic cytokines in tumor and host tissues leads to a paraneoplastic thrombocytosis, which fuels tumor growth.
Deterrence and Prevention The risk of developing epithelial ovarian cancer is significantly reduced by bearing
children, using the combined oral contraceptive pill, undergoing tubal ligation, and undergoing bilateral oophorectomy.
Evidence suggests that taking the oral contraceptive pill for at least 5 years reduces the relative risk of developing EOC to 50% of the risk for a woman who has never taken it.
Prophylactic bilateral salpingo-oophorectomy is indicated in high-risk women. The American College of Obstetricians and Gynecologists recommends offering salpingo-oophorectomy to women with BRCA1 or BRCA2 mutations by age 40 years or when childbearing is complete (level A recommendation).[70] Surgical prophylaxis decreases the risk by at least 90%. Not all cases of ovarian cancer are prevented, as women are still at risk for developing primary peritoneal carcinomas.
The epithelial lining of the ovaries is embryologically identical with the lining of the peritoneal cavity, and similar cancers can develop from the peritoneum. Thus, while oophorectomy prevents a pure epithelial ovarian cancer from developing, a small risk still exists for developing carcinoma of the peritoneum, a disease that behaves similarly to epithelial ovarian cancer.
BRAC1 and BRAC2 mutations are common among women with invasive ovarian cancer; thus, women diagnosed with invasive, nonmucinous ovarian cancer are candidates for genetic testing.
For patients who are known carriers of BRCA1 or BRCA2 mutations, bilateral oophorectomy may be performed as soon as childbearing is complete, and probably before the patient is aged 35 years. This reduces the chance of developing EOC, but it does not prevent carcinoma of the peritoneum.
For women with BRCA1 and BRCA2 mutations who opt to not undergo early oophorectomy, the task force of the Cancer Genetics Studies Consortium
References http://emedicine.medscape.com/article/255771-
medication
www.cancer.org/downloads/STT/500809web.pdf. Accessed January 25, 2010.
http://www.ahrq.gov/clinic/3rduspstf/ovariancan/ovcanrs.htm. Accessed January 25, 2010.
http://www.merckmanuals.com/professional/resources/selected_links/selected_links.html?WT.z_resource=Selected%20Links- by David M. Gershenson, MD; Pedro T. Ramirez, MD, November 2008
American Cancer Society.: Cancer Facts and Figures 2012. Atlanta, Ga: American Cancer Society, 2012.


















