TBS903 Autumn2009 Subject Outline Subject Outline (Final Version)
Upload
duongthienCategory
view
217download
2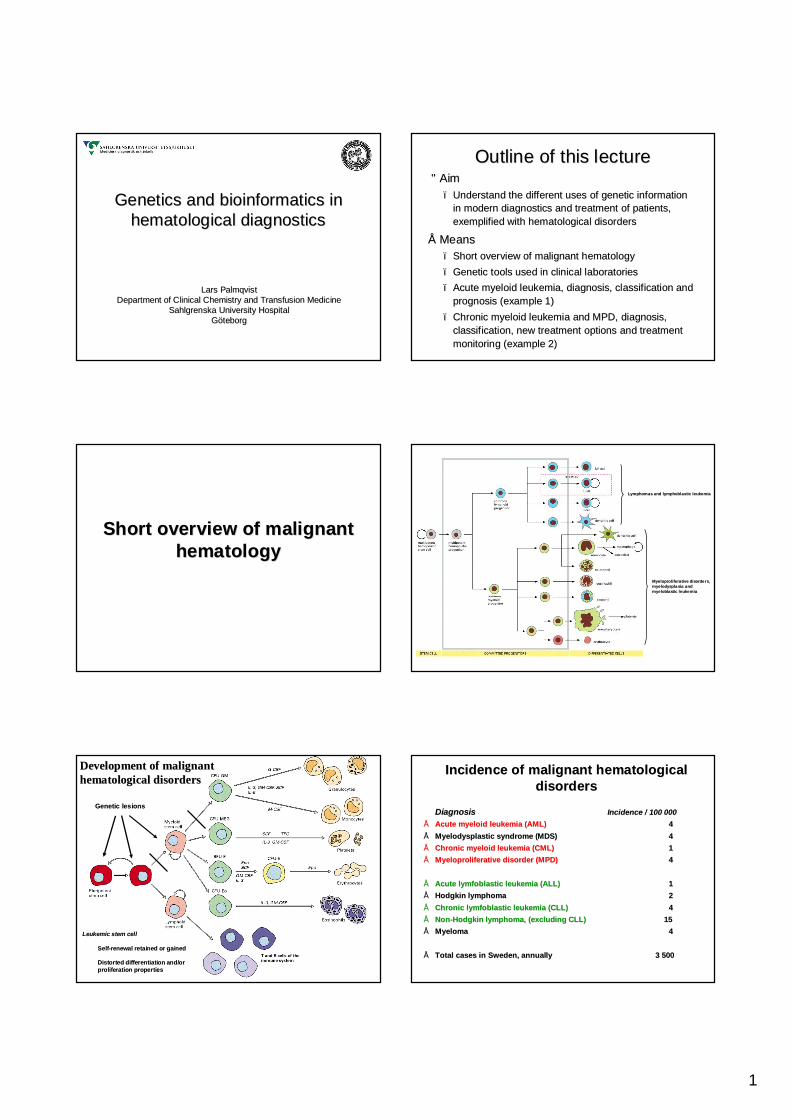
1
Genetics and bioinformatics in Genetics and bioinformatics in hematological diagnosticshematological diagnostics
Lars PalmqvistLars PalmqvistDepartment of Clinical Chemistry and Transfusion MedicineDepartment of Clinical Chemistry and Transfusion Medicine
Sahlgrenska University HospitalSahlgrenska University HospitalGGööteborgteborg
Outline of this lectureOutline of this lecture•• AimAim
–– Understand the different uses of genetic information Understand the different uses of genetic information in modern diagnostics and treatment of patients, in modern diagnostics and treatment of patients, exemplified with hematological disordersexemplified with hematological disorders
•• MeansMeans–– Short overview of malignant hematologyShort overview of malignant hematology–– Genetic tools used in clinical laboratoriesGenetic tools used in clinical laboratories–– Acute myeloid leukemia, diagnosis, classification and Acute myeloid leukemia, diagnosis, classification and
prognosis (example 1)prognosis (example 1)–– Chronic myeloid leukemia and MPD, diagnosis, Chronic myeloid leukemia and MPD, diagnosis,
classification, new treatment options and treatment classification, new treatment options and treatment monitoring (example 2)monitoring (example 2)
Short overview of malignant Short overview of malignant hematologyhematology
Lymphomas and lymphoblastic leukemiaLymphomas and lymphoblastic leukemia
MyeloproliferativeMyeloproliferative disorders, disorders, myelodyspla siamyelodyspla sia andandmyeloblasticmyeloblastic leukemialeukemia
HematopoiesisHematopoiesisDevelopment of malignant Development of malignant hematological disordershematological disorders
Genetic lesionsGenetic lesions
Leukemic stem cellLeukemic stem cell
SelfSelf--renewal retained or gainedrenewal retained or gained
Distorted differentiation and/or Distorted differentiation and/or proliferation propertiesproliferation properties
Incidence of malignant hematological Incidence of malignant hematological disordersdisorders
DiagnosisDiagnosis Incidence / 100 000Incidence / 100 000•• Acute myeloid leukemia (AML)Acute myeloid leukemia (AML) 4 4 •• MyelodysplasticMyelodysplastic syndrome (MDS)syndrome (MDS) 44•• Chronic myeloid leukemia (CML)Chronic myeloid leukemia (CML) 11•• MyeloproliferativeMyeloproliferative disorder (MPD)disorder (MPD) 44
•• Acute Acute lymfoblasticlymfoblastic leukemia (ALL)leukemia (ALL) 11•• Hodgkin lymphomaHodgkin lymphoma 22•• Chronic Chronic lymfoblasticlymfoblastic leukemia (CLL)leukemia (CLL) 44•• NonNon--Hodgkin lymphoma, (excluding CLL)Hodgkin lymphoma, (excluding CLL) 1515•• MyelomaMyeloma 44
•• Total cases in Sweden, annuallyTotal cases in Sweden, annually 3 5003 500
2
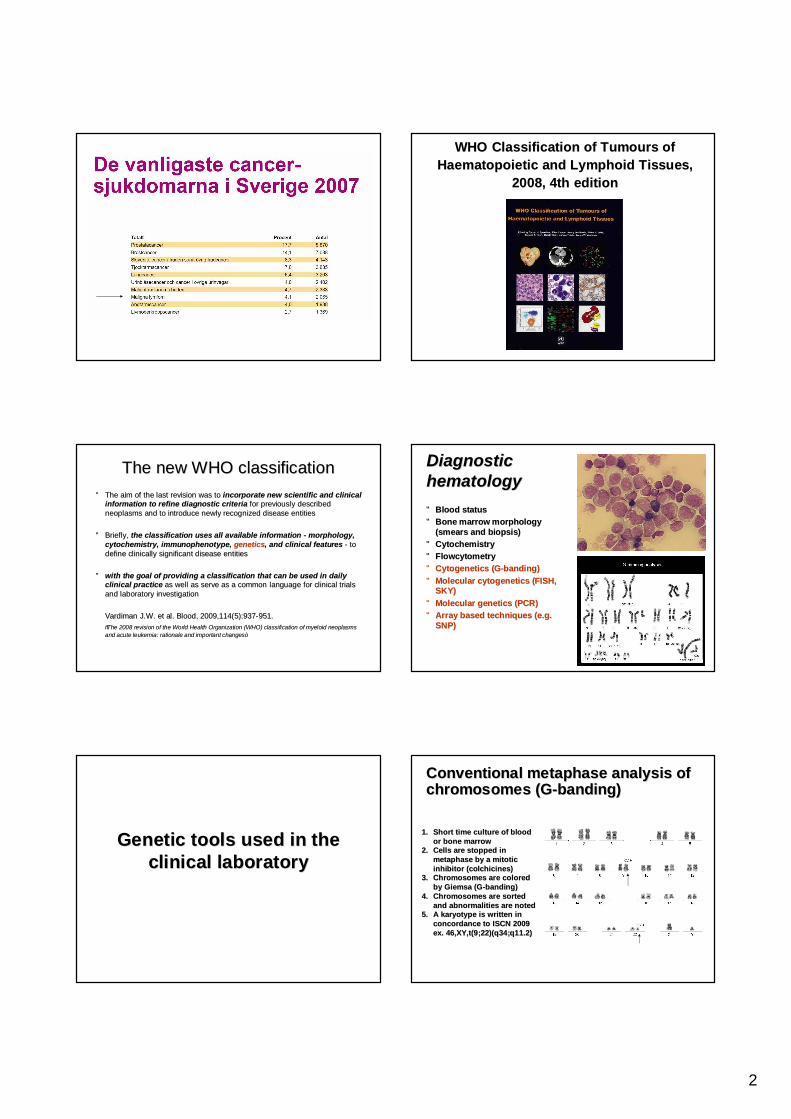
WHO Classification of WHO Classification of TumoursTumours of of HaematopoieticHaematopoietic and Lymphoid Tissues, and Lymphoid Tissues,
2008, 4th edition 2008, 4th edition
The new WHO classificationThe new WHO classification•• The aim of the last revision was to The aim of the last revision was to incorporate new scientific and clinical incorporate new scientific and clinical
information to refine diagnostic criteriainformation to refine diagnostic criteria for previously described for previously described neoplasmsneoplasms and to introduce newly recognized disease entitiesand to introduce newly recognized disease entities
•• Briefly, Briefly, the classification uses all available information the classification uses all available information -- morphology, morphology, cytochemistrycytochemistry, , immunophenotypeimmunophenotype, , geneticsgenetics, and clinical features, and clinical features -- to to define clinically significant disease entitiesdefine clinically significant disease entities
•• with the goal of providing a classification that can be used in with the goal of providing a classification that can be used in daily daily clinical practiceclinical practice as well as serve as a common language for clinical trials as well as serve as a common language for clinical trials and laboratory investigationand laboratory investigation
VardimanVardiman J.W. et al. Blood, 2009,114(5):937J.W. et al. Blood, 2009,114(5):937--951.951.““The 2008 revision of the World Health Organization (WHO) classifThe 2008 revision of the World Health Organization (WHO) classification of myeloid ication of myeloid neoplasmsneoplasmsand acute leukemia: rationale and important changesand acute leukemia: rationale and important changes””
Diagnostic Diagnostic hematologyhematology
•• Blood statusBlood status•• Bone marrow morphology Bone marrow morphology
(smears and (smears and biopsisbiopsis))•• CytochemistryCytochemistry•• FlowcytometryFlowcytometry•• CytogeneticsCytogenetics (G(G--banding)banding)•• Molecular Molecular cytogeneticscytogenetics (FISH, (FISH,
SKY)SKY)•• Molecular genetics (PCR)Molecular genetics (PCR)•• Array based techniques (e.g. Array based techniques (e.g.
SNP)SNP)
Genetic tools used in the Genetic tools used in the clinical laboratoryclinical laboratory
1.1. Short time culture of blood Short time culture of blood or bone marrowor bone marrow
2.2. Cells are stopped in Cells are stopped in metaphase by a mitotic metaphase by a mitotic inhibitor (colchicines)inhibitor (colchicines)
3.3. Chromosomes are colored Chromosomes are colored by by GiemsaGiemsa (G(G--banding)banding)
4.4. ChromosomesChromosomes are sorted are sorted and abnormalities are noted and abnormalities are noted
5.5. A A karyotypekaryotype is written in is written in concordance to ISCN 2009concordance to ISCN 2009ex. 46,XY,t(9;22)(q34;q11.2)ex. 46,XY,t(9;22)(q34;q11.2)
Conventional metaphase analysis of Conventional metaphase analysis of chromosomes (Gchromosomes (G--banding)banding)
3
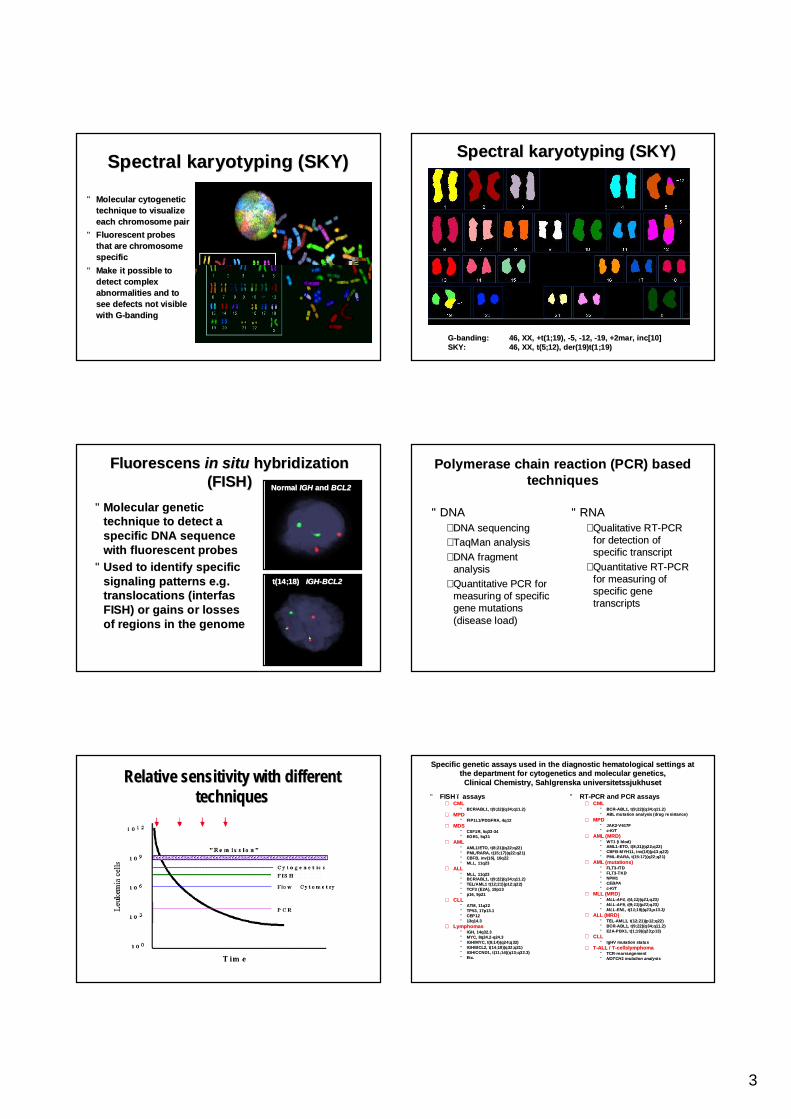
Spectral Spectral karyotypingkaryotyping (SKY)(SKY)
•• Molecular cytogenetic Molecular cytogenetic technique to visualize technique to visualize each chromosome paireach chromosome pair
•• Fluorescent probes Fluorescent probes that are chromosome that are chromosome specificspecific
•• Make it possible to Make it possible to detect complex detect complex abnormalities and to abnormalities and to see defects not visible see defects not visible with Gwith G--bandingbanding
Spectral Spectral karyotypingkaryotyping (SKY)(SKY)
GG--bandingbanding: : 46, XX, +t(1;19), 46, XX, +t(1;19), --5, 5, --12, 12, --19, +2mar, inc[10]19, +2mar, inc[10]SKY:SKY: 46, XX, t(5;12), der(19)t(1;19)46, XX, t(5;12), der(19)t(1;19)
Fluorescens Fluorescens in in situsitu hybridizationhybridization(FISH)(FISH)
•• Molecular genetic Molecular genetic technique to detect a technique to detect a specific DNA sequence specific DNA sequence with fluorescent probeswith fluorescent probes
•• Used to identify specific Used to identify specific signaling patterns e.g. signaling patterns e.g. translocations (translocations (interfasinterfasFISH) or gains or losses FISH) or gains or losses of regions in the genomeof regions in the genome
Normal Normal IGHIGH and and BCL2BCL2
t(14;18) t(14;18) IGHIGH--BCL2BCL2
Polymerase chain reaction (PCR) based Polymerase chain reaction (PCR) based techniquestechniques
•• DNA DNA –– DNA sequencingDNA sequencing–– TaqManTaqMan analysisanalysis–– DNA fragment DNA fragment
analysisanalysis–– Quantitative PCR for Quantitative PCR for
measuring of specific measuring of specific gene mutations gene mutations (disease load)(disease load)
•• RNARNA–– Qualitative RTQualitative RT--PCR PCR
for detection of for detection of specific transcriptspecific transcript
–– Quantitative RTQuantitative RT--PCR PCR for measuring of for measuring of specific gene specific gene transcriptstranscripts
Relative sensitivity with different Relative sensitivity with different techniques techniques
Specific genetic assays used in the diagnostic hematological setSpecific genetic assays used in the diagnostic hematological settings at tings at the department for the department for cytogeneticscytogenetics and molecular genetics, and molecular genetics,
Clinical Chemistry, Sahlgrenska Clinical Chemistry, Sahlgrenska universitetssjukhusetuniversitetssjukhuset
•• FISH FISH –– assaysassays–– CMLCML
•• BCR/ABL1, t(9;22)(q34;q11.2)BCR/ABL1, t(9;22)(q34;q11.2)–– MPDMPD
•• FIP1L1/PDGFRA, FIP1L1/PDGFRA, 4q124q12–– MDSMDS
•• CSF1R, 5q33CSF1R, 5q33--3434•• EGR1, 5q31EGR1, 5q31
–– AMLAML•• AML1/ETO, t(8;21)(q22;q22)AML1/ETO, t(8;21)(q22;q22)•• PML/RARA, t(15;17)(q22;q21)PML/RARA, t(15;17)(q22;q21)•• CBFB, inv(16), 16q22CBFB, inv(16), 16q22•• MLL, 11q23MLL, 11q23
–– ALLALL•• MLL, 11q23MLL, 11q23•• BCR/ABL1, t(9;22)(q34;q11.2)BCR/ABL1, t(9;22)(q34;q11.2)•• TEL/AML1 t(12;21)(p12;q22)TEL/AML1 t(12;21)(p12;q22)•• TCF3 (E2A), 19p13TCF3 (E2A), 19p13•• p16, 9p21p16, 9p21
–– CLLCLL•• ATM, 11q22ATM, 11q22•• TP53, 17p13.1TP53, 17p13.1•• CEP12CEP12•• 13q14.313q14.3
–– LymphomasLymphomas•• IGH, 14q32.3IGH, 14q32.3•• MYC, 8q24.2MYC, 8q24.2--q24.3q24.3•• IGH/MYC, t(8;14)(q24;q32)IGH/MYC, t(8;14)(q24;q32)•• IGH/BCL2, t(14;18)(q32;q21)IGH/BCL2, t(14;18)(q32;q21)•• IGH/CCND1, t(11;14)(q13;q32.3)IGH/CCND1, t(11;14)(q13;q32.3)•• Etc.Etc.
•• RTRT--PCR and PCR assaysPCR and PCR assays–– CMLCML
•• BCRBCR--ABL1, t(9;22)(q34;q11.2)ABL1, t(9;22)(q34;q11.2)•• ABL mutation analysis (drug re sistance)ABL mutation analysis (drug re sistance)
–– MPDMPD•• JAK2JAK2--V617FV617F•• cc--KITKIT
–– AML (MRD)AML (MRD)•• WT1 (i WT1 (i blodblod))•• AML1AML1--ETO, t(8;21)(q22;q22)ETO, t(8;21)(q22;q22)•• CBFBCBFB--MYH11, inv(16)(p13;q22)MYH11, inv(16)(p13;q22)•• PMLPML--RARA, t(15:17)(q22;q21)RARA, t(15:17)(q22;q21)
–– AML (mutations)AML (mutations)•• FLT3FLT3--ITDITD•• FLT3FLT3--TKDTKD•• NPM1NPM1•• CEBPACEBPA•• cc--KITKIT
–– MLL (MRD)MLL (MRD)•• MLLMLL--AF4, t(4;11)(q21;q23)AF4, t(4;11)(q21;q23)•• MLLMLL--AF9, t(9;11)(p22;q23)AF9, t(9;11)(p22;q23)•• MLLMLL--ENL, t(11;19)(q23;p13.3)ENL, t(11;19)(q23;p13.3)
–– ALL (MRD)ALL (MRD)•• TELTEL--AML1, t(12;21)(p12;q22)AML1, t(12;21)(p12;q22)•• BCRBCR--ABL1, t(9;22)(q34;q11.2)ABL1, t(9;22)(q34;q11.2)•• E2AE2A--PBX1, t(1;19)(q23;p13)PBX1, t(1;19)(q23;p13)
–– CLLCLL•• IgHVIgHV mutation statusmutation status
–– TT--ALL / TALL / T--cellslymphomacellslymphoma•• TCRTCR--rearrangementrearrangement•• NOTCH1 mutation analysisNOTCH1 mutation analysis
4
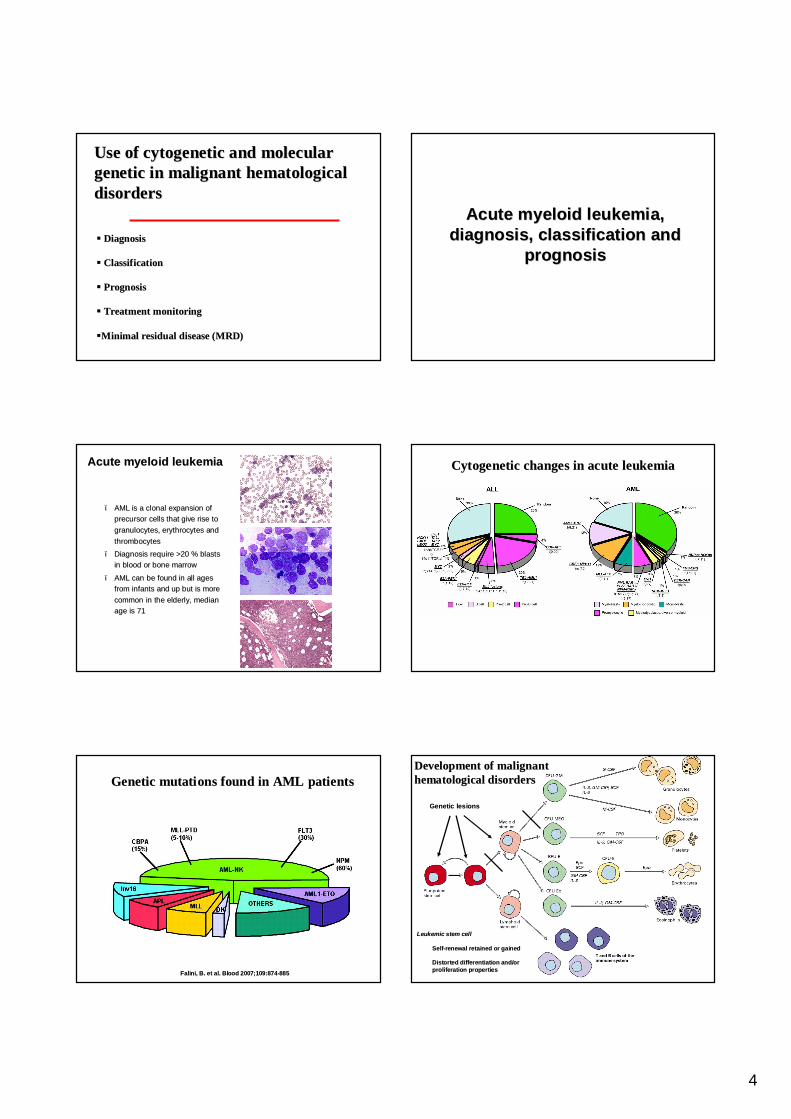
Use of cytogenetic and molecular Use of cytogenetic and molecular genetic in malignant hematological genetic in malignant hematological disordersdisorders
§§ DiagnosisDiagnosis
§§ ClassificationClassification
§§ Prognosis Prognosis
§§ Treatment monitoring Treatment monitoring
§§Minimal residual disease (MRD)Minimal residual disease (MRD)
Acute myeloid leukemia, Acute myeloid leukemia, diagnosis, classification and diagnosis, classification and
prognosisprognosis
–– AML is a clonal expansion of AML is a clonal expansion of precursor cells that give rise to precursor cells that give rise to granulocytes, erythrocytes and granulocytes, erythrocytes and thrombocytesthrombocytes
–– Diagnosis require >20 % blasts Diagnosis require >20 % blasts in blood or bone marrowin blood or bone marrow
–– AML can be found in all ages AML can be found in all ages from infants and up but is more from infants and up but is more common in the elderly, median common in the elderly, median age is 71age is 71
Acute myeloid leukemiaAcute myeloid leukemia Cytogenetic changes in acute leukemiaCytogenetic changes in acute leukemia
FaliniFalini, B. et al. Blood 2007;109:874, B. et al. Blood 2007;109:874--885885
Genetic mutations found in AML patientsGenetic mutations found in AML patients HematopoiesisHematopoiesisDevelopment of malignant Development of malignant hematological disordershematological disorders
Genetic lesionsGenetic lesions
Leukemic stem cellLeukemic stem cell
SelfSelf--renewal retained or gainedrenewal retained or gained
Distorted differentiation and/or Distorted differentiation and/or proliferation propertiesproliferation properties
5
BlasticBlastic plasmacytoidplasmacytoid dendriticdendritic cell neoplasmcell neoplasmMyeloid leukemia associated with Down syndromeMyeloid leukemia associated with Down syndrome
Transient abnormal Transient abnormal myelopoiesismyelopoiesis
Myeloid proliferations related to Down syndromeMyeloid proliferations related to Down syndromeMyeloid sarcomaMyeloid sarcoma
Acute Acute panmyelosispanmyelosis with with myelofibrosismyelofibrosis
Acute basophilic leukemiaAcute basophilic leukemia
Acute Acute megakaryoblasticmegakaryoblastic leukemialeukemia
ErythroleukemiaErythroleukemia, , erythroiderythroid/myeloid/myeloid
Pure Pure erythroiderythroid leukemialeukemia
Acute Acute erythroiderythroid leukemialeukemia
Acute Acute monoblastic/monocyticmonoblastic/monocytic leukemialeukemia
Acute Acute myelomonocyticmyelomonocytic leukemialeukemia
AML with maturationAML with maturation
AML without maturationAML without maturation
AML with minimal differentiationAML with minimal differentiation
Acute myeloid leukemia, not otherwise specifiedAcute myeloid leukemia, not otherwise specifiedTherapyTherapy--related myeloid related myeloid neoplasmsneoplasms **
Acute myeloid leukemia with Acute myeloid leukemia with myelodysplasiamyelodysplasia--related changesrelated changes
Provisional entity: Provisional entity: AML with mutated CEBPAAML with mutated CEBPA
Provisional entity: Provisional entity: AML with mutated NPM1AML with mutated NPM1
AML (AML (megakaryoblasticmegakaryoblastic) with ) with t(1;22)(p13;q13); t(1;22)(p13;q13); RBM15RBM15--MKL1MKL1
AML with AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); inv(3)(q21q26.2) or t(3;3)(q21;q26.2); RPN1RPN1--EVI1EVI1
AML with AML with t(6;9)(p23;q34); t(6;9)(p23;q34); DEKDEK--NUP214NUP214
AML with AML with t(9;11)(p22;q23); t(9;11)(p22;q23); MLLT3MLLT3--MLLMLL
APL with APL with t(15;17)(q22;q12); t(15;17)(q22;q12); PMLPML--RARARARA
AML with AML with inv(16)(p13.1q22) or t(16;16)(p13.1;q22); inv(16)(p13.1q22) or t(16;16)(p13.1;q22); CBFBCBFB--MYH11MYH11
AML with AML with t(8;21)(q22;q22); t(8;21)(q22;q22); RUNX1RUNX1--RUNX1T1RUNX1T1
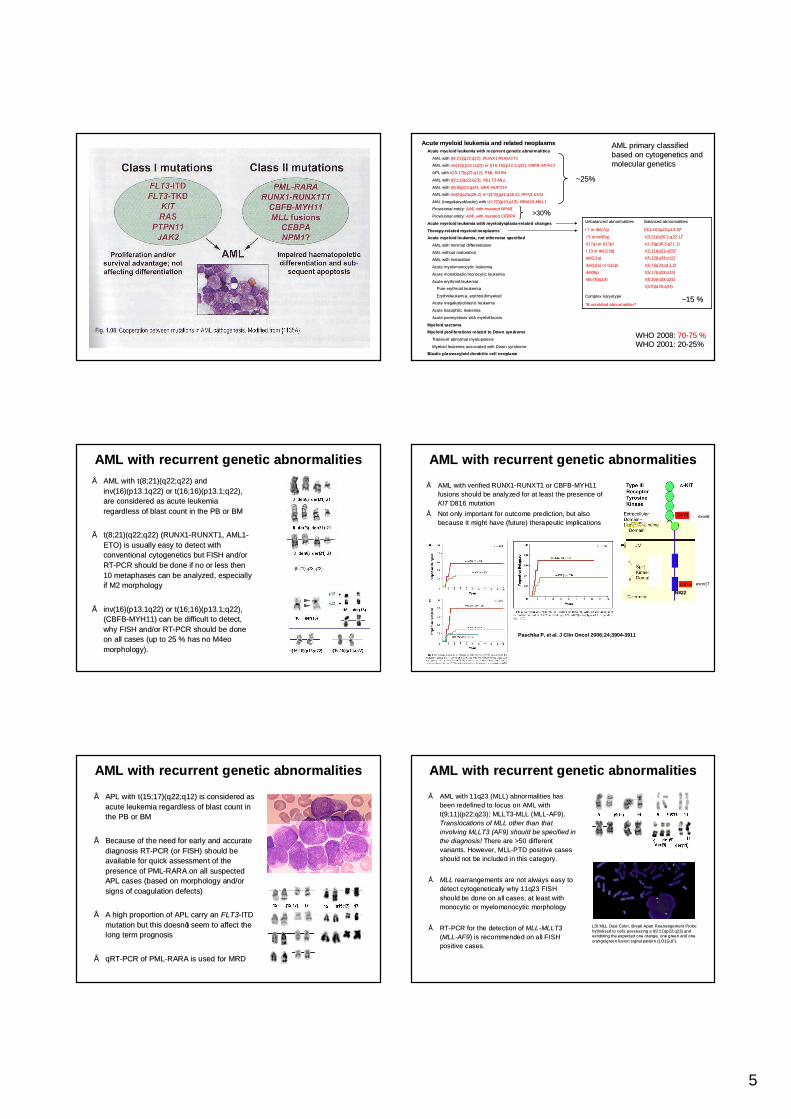
Acute myeloid leukemia with recurrent genetic abnormalitiesAcute myeloid leukemia with recurrent genetic abnormalities
Acute myeloid leukemia and related Acute myeloid leukemia and related neoplasmsneoplasms
t(3;5)(q25;q34)t(3;5)(q25;q34)
Complex Complex karyotypekaryotype
≥≥33 unrelated abnormalitiesunrelated abnormalities**
t(5;10)(q33;q21)t(5;10)(q33;q21)idic(X)(q13)idic(X)(q13)
t(5;17)(q33;p13)t(5;17)(q33;p13)del(9q)del(9q)
t(5;7)(q33;q11.2)t(5;7)(q33;q11.2)del(12p) or t(12p)del(12p) or t(12p)
t(5;12)(q33;p12)t(5;12)(q33;p12)del(11q)del(11q)
t(2;11)(p21;q23)t(2;11)(p21;q23)**––13 or del(13q)13 or del(13q)
t(1;3)(p36.3;q21.1)t(1;3)(p36.3;q21.1)i(17q) or t(17p)i(17q) or t(17p)
t(3;21)(q26.2;q22.1)t(3;21)(q26.2;q22.1)**––5 or5 or del(5q)del(5q)
Balanced abnormalitiesBalanced abnormalities
t(11;16)(q23;p13.3)t(11;16)(q23;p13.3)**
Unbalanced abnormalitiesUnbalanced abnormalities
––7 or del(7q)7 or del(7q)
AML primary classified AML primary classified based on based on cytogeneticscytogenetics and and molecular geneticsmolecular genetics
~15 %~15 %
WHO 2008: WHO 2008: 7070--75 %75 %WHO 2001: 20WHO 2001: 20--25%25%
~25%~25%
>30>30%%
AML with recurrent genetic abnormalities AML with recurrent genetic abnormalities •• AML with t(8;21)(q22;q22) and AML with t(8;21)(q22;q22) and
inv(16)(p13.1q22) or t(16;16)(p13.1;q22), inv(16)(p13.1q22) or t(16;16)(p13.1;q22), are considered as acute leukemia are considered as acute leukemia regardless of blast count in the PB or BMregardless of blast count in the PB or BM
•• t(8;21)(q22;q22) (RUNX1t(8;21)(q22;q22) (RUNX1--RUNXT1, AML1RUNXT1, AML1--ETO) is usually easy to detect with ETO) is usually easy to detect with conventional conventional cytogeneticscytogenetics but FISH and/or but FISH and/or RTRT--PCR should be done if no or less then PCR should be done if no or less then 10 metaphases can be analyzed, especially 10 metaphases can be analyzed, especially if M2 morphologyif M2 morphology
•• inv(16)(p13.1q22) or t(16;16)(p13.1;q22), inv(16)(p13.1q22) or t(16;16)(p13.1;q22), (CBFB(CBFB--MYH11) can be difficult to detect, MYH11) can be difficult to detect, why FISH and/or RTwhy FISH and/or RT--PCR should be done PCR should be done on all cases (up to 25 % has no M4eo on all cases (up to 25 % has no M4eo morphology).morphology).
AML with recurrent genetic abnormalities AML with recurrent genetic abnormalities
•• AML with verified RUNX1AML with verified RUNX1--RUNXT1 or CBFBRUNXT1 or CBFB--MYH11 MYH11 fusions should be analyzed for at least the presence of fusions should be analyzed for at least the presence of KITKIT D816 mutationD816 mutation
•• Not only important for outcome prediction, but also Not only important for outcome prediction, but also because it might have (future) therapeutic implicationsbecause it might have (future) therapeutic implications
PaschkaPaschka P, et al. J P, et al. J ClinClin OncolOncol 2006;24;39042006;24;3904--39113911
exon17exon17
exon8exon8
N822N822
AML with recurrent genetic abnormalities AML with recurrent genetic abnormalities
•• APL with t(15;17)(q22;q12) is considered as APL with t(15;17)(q22;q12) is considered as acute leukemia regardless of blast count in acute leukemia regardless of blast count in the PB or BMthe PB or BM
•• Because of the need for early and accurate Because of the need for early and accurate diagnosis RTdiagnosis RT--PCR (or FISH) should be PCR (or FISH) should be available for quick assessment of the available for quick assessment of the presence of PMLpresence of PML--RARA on all suspected RARA on all suspected APL cases (based on morphology and/or APL cases (based on morphology and/or signs of coagulation defects)signs of coagulation defects)
•• A high proportion of APL carry an A high proportion of APL carry an FLT3FLT3--ITD ITD mutation but this doesnmutation but this doesn ’’t seem to affect the t seem to affect the long term prognosislong term prognosis
•• qRTqRT--PCR of PMLPCR of PML--RARA is used for MRDRARA is used for MRD
AML with recurrent genetic abnormalities AML with recurrent genetic abnormalities
•• AML with 11q23 (MLL) abnormalities has AML with 11q23 (MLL) abnormalities has been redefined to focus on AML with been redefined to focus on AML with t(9;11)(p22;q23); MLLT3t(9;11)(p22;q23); MLLT3--MLL (MLLMLL (MLL--AF9). AF9). Translocations of MLL other than that Translocations of MLL other than that involving MLLT3 (AF9) should be specified in involving MLLT3 (AF9) should be specified in the diagnosis!the diagnosis! There are >50 different There are >50 different variants. However, MLLvariants. However, MLL--PTD positive cases PTD positive cases should not be included in this category.should not be included in this category.
•• MLLMLL rearrangements are not always easy to rearrangements are not always easy to detect cytogenetically why 11q23 FISH detect cytogenetically why 11q23 FISH should be done on all cases, at least with should be done on all cases, at least with monocyticmonocytic or or myelomonocyticmyelomonocytic morphologymorphology
•• RTRT--PCR for the detection of PCR for the detection of MLLMLL--MLLT3MLLT3((MLLMLL--AF9AF9) is recommended on all FISH ) is recommended on all FISH positive cases.positive cases.
LSI MLL Dual Color, Break Apart Rearrangement Probe LSI MLL Dual Color, Break Apart Rearrangement Probe hybridized to cells possessing a t(9:11)(p22;q23) and hybridized to cells possessing a t(9:11)(p22;q23) and exhibiting the expected one orange, one green and one exhibiting the expected one orange, one green and one orange/green fusion signal pattern (1O1G1F). orange/green fusion signal pattern (1O1G1F).

6
AML with recurrent genetic abnormalities AML with recurrent genetic abnormalities
•• Three new cytogenetically defined entities have been added: Three new cytogenetically defined entities have been added: –– (1) AML with t(6;9)(p23;q34); DEK(1) AML with t(6;9)(p23;q34); DEK--NUP214, NUP214, –– (2) AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); RPN1(2) AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); RPN1--EVI1; and EVI1; and –– (3) AML ((3) AML (megakaryoblasticmegakaryoblastic) with t(1;22)(p13;q13); RBM15) with t(1;22)(p13;q13); RBM15--MKL1.MKL1.
All are uncommon but associated All are uncommon but associated with distinct morphological and with distinct morphological and clinical featuresclinical features
These fusions can be detected in These fusions can be detected in selected cases by RTselected cases by RT--PCR if no PCR if no or only poor quality or only poor quality cytogeneticscytogeneticsis obtained. is obtained. FLT3FLT3--ITD is common ITD is common in t(6;9)(p23;q34)in t(6;9)(p23;q34)
AML with recurrent genetic abnormalitiesAML with recurrent genetic abnormalities-- gene mutationsgene mutations
•• Several specific mutations with prognostic impact have been founSeveral specific mutations with prognostic impact have been found in AMLd in AML–– FLT3 and NPM1 mutations are the most commonFLT3 and NPM1 mutations are the most common–– Mutations in CEBPA, KIT, RAS, WT1, RUNX1 and MLL are less frequeMutations in CEBPA, KIT, RAS, WT1, RUNX1 and MLL are less frequentnt–– These mutations are associated with few, if any, consistent morpThese mutations are associated with few, if any, consistent morphologic or clinical features hologic or clinical features –– They are not entirely mutually exclusive of each other or, partiThey are not entirely mutually exclusive of each other or, particularly in the case of FLT3, cularly in the case of FLT3,
of other wellof other well--recognized cytogenetic defectsrecognized cytogenetic defects
246 AML patients were 246 AML patients were analyzed for the analyzed for the presence of coexisting presence of coexisting mutationsmutations
Mrozek, K. et al. Blood 2007;109:431Mrozek, K. et al. Blood 2007;109:431--448448
AML with recurrent genetic abnormalitiesAML with recurrent genetic abnormalities-- gene mutationsgene mutations
•• FLT3 mutations occur in any AML but FLT3 mutations occur in any AML but especially t(15;17), t(6;9) and normal especially t(15;17), t(6;9) and normal karyotypekaryotypeAML. AML.
•• FLT3FLT3--ITD is associated with adverse outcome ITD is associated with adverse outcome in normal in normal karyotypekaryotype AML but AML but FLT3FLT3--TKD TKD mutations seem to be less somutations seem to be less so
Bienz, M. et al. Clin Cancer Res 2005;11:1416Bienz, M. et al. Clin Cancer Res 2005;11:1416--14241424
AML with recurrent genetic abnormalitiesAML with recurrent genetic abnormalities-- gene mutationsgene mutations
•• There are some reports that the There are some reports that the FLT3FLT3--ITD allelic burden has ITD allelic burden has a prognostic significance. Where patients with a a prognostic significance. Where patients with a FLT3FLT3--ITD/ITD/FLT3FLT3--wt ratio >50% have a worse prognosis.wt ratio >50% have a worse prognosis.
Gale, R. E., C. Green, et al. (2008) Blood, 111(5): 2776Gale, R. E., C. Green, et al. (2008) Blood, 111(5): 2776--84.84.
AML with recurrent genetic abnormalitiesAML with recurrent genetic abnormalities-- gene mutationsgene mutations
•• An An NPM1NPM1 mutation is found in 30% of de novo AML and ~50 % of normal mutation is found in 30% of de novo AML and ~50 % of normal karyotypekaryotype AML. Approx. 40 % have an AML. Approx. 40 % have an FLT3FLT3--ITD mutationITD mutation
•• Normal Normal karyotypekaryotype AML withAML with NPM1NPM1+/+/FLT3FLT3--ITDITD-- have comparable have comparable overall overall and disease free survival and disease free survival to t(8;21) and inv(16) AMLto t(8;21) and inv(16) AML
Thiede, C. et al. Blood 2006;107:4011Thiede, C. et al. Blood 2006;107:4011--40204020
AML with recurrent genetic abnormalitiesAML with recurrent genetic abnormalities-- gene mutationsgene mutations
•• CEBPA mutation is found in ~10% of de novo AML and ~15 % of normCEBPA mutation is found in ~10% of de novo AML and ~15 % of normal al karyotypekaryotype AML. Approx. ~25 % are AML. Approx. ~25 % are FLT3FLT3--ITD+ITD+
•• Normal Normal karyotypekaryotype AML withAML with CEBPACEBPA+/+/FLT3FLT3--ITDITD-- have comparable have comparable overall and disease free survival to t(8;21) and inv(16) AMLto t(8;21) and inv(16) AML
Bienz, M. et al. Clin Cancer Res 2005;11:1416Bienz, M. et al. Clin Cancer Res 2005;11:1416--14241424
7
AML with recurrent genetic abnormalitiesAML with recurrent genetic abnormalities-- gene mutationsgene mutations
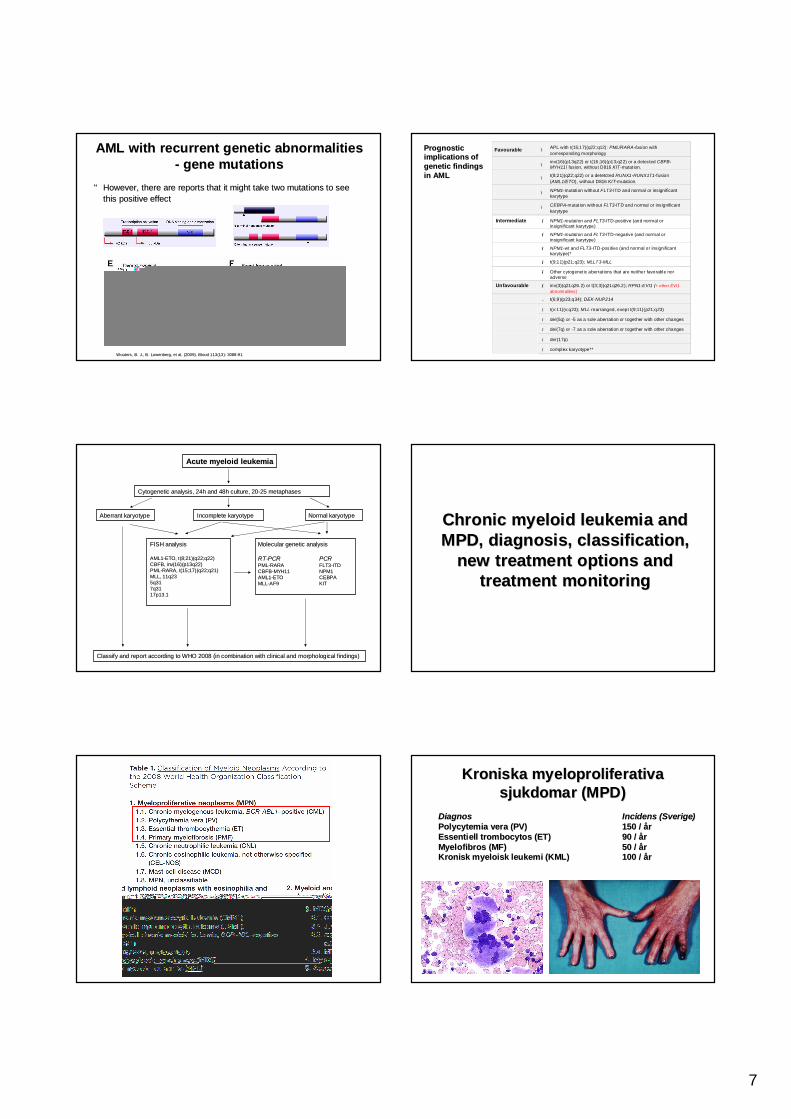
•• However, there are reports that it might take two mutations to sHowever, there are reports that it might take two mutations to see ee this positive effectthis positive effect
WoutersWouters, B. J., B. , B. J., B. LowenbergLowenberg, et al. (2009). Blood 113(13): 3088, et al. (2009). Blood 113(13): 3088--9191
Favourable – APL with t(15;17)(q22;q12): PML/RARA-fusion with corresponding morphology
– inv(16)(p13q22) or t(16;16)(p13;q22) or a detected CBFB-MYH11–fusion, without D816 KIT-mutat ion.
– t(8;21)(q22;q22) or a detetcted RUNX1-RUNX1T1-fusion (AML1/ETO), without D816 KIT-mutat ion.
– NPM1-mutation without FLT3-ITD and normal or insignificant karytype
– CEBPA-mutat ion without FLT3-ITD and normal or insignificant karytype
Intermediate – NPM1-mutation and FLT3-ITD-positive (and normal or insignificant karytype)
– NPM1-mutation and FLT3-ITD-negative (and normal or insignificant karytype)
– NPM1-wt and FLT3-ITD-positive (and normal or insignificant karytype)*
– t(9;11)(p21;q23); MLLT3-MLL
– Other cytogenet ic aberrations that are neither favorable nor adverse
Unfavourable – inv(3)(q21q26.2) or t(3;3)(q21q26.2); RPN1-EVI1 (+ other EVI1 abnormalities]
- t(6;9)(p23;q34); DEK-NUP214
– t(v:11)(v;q23); MLL rearranged, exept t(9;11)(p21;q23)
– del(5q) or -5 as a sole aberration or together with other changes
– del(7q) or -7 as a sole aberration or together with other changes
– der(17p)
– complex karyotype**
Prognostic Prognostic implications of implications of genetic findings genetic findings in AMLin AML
Acute myeloid leukemiaAcute myeloid leukemia
Cytogenetic analysis, 24h and 48h culture, 20Cytogenetic analysis, 24h and 48h culture, 20--25 metaphases25 metaphases
Molecular genetic analysisMolecular genetic analysis
RTRT--PCRPCR PCRPCRPMLPML--RARARARA FLT3FLT3--ITDITDCBFBCBFB--MYH11MYH11 NPM1NPM1AML1AML1--ETOETO CEBPACEBPAMLLMLL--AF9AF9 KITKIT
Aberrant Aberrant karyotypekaryotype Normal Normal karyotypekaryotypeIncomplete Incomplete karyotypekaryotype
Classify and report according to WHO 2008 (in combination with cClassify and report according to WHO 2008 (in combination with clinical and morphological findings)linical and morphological findings)
FISH analysisFISH analysis
AML1AML1--ETO, t(8;21)(q22;q22)ETO, t(8;21)(q22;q22)CBFB, inv(16)(p13q22)CBFB, inv(16)(p13q22)PMLPML--RARA, t(15;17)(q22;q21)RARA, t(15;17)(q22;q21)MLL, 11q23 MLL, 11q23 5q315q317q317q3117p13.117p13.1
Chronic myeloid leukemia and Chronic myeloid leukemia and MPD, diagnosis, classification, MPD, diagnosis, classification,
new treatment options and new treatment options and treatment monitoringtreatment monitoring
Kroniska Kroniska myeloproliferativamyeloproliferativasjukdomar (MPD)sjukdomar (MPD)
DiagnosDiagnos Incidens (Sverige)Incidens (Sverige)PolycytemiaPolycytemia veravera (PV)(PV) 150 / 150 / åårrEssentiell Essentiell trombocytostrombocytos (ET)(ET) 90 / 90 / åårrMyelofibrosMyelofibros (MF)(MF) 50 / 50 / åårrKronisk Kronisk myeloiskmyeloisk leukemi (KML)leukemi (KML) 100 / 100 / åårr

8
IntroductionIntroduction•• CML is characterized by CML is characterized by
elevated WBC counts and the elevated WBC counts and the presence of immature cells in presence of immature cells in peripheral blood peripheral blood
•• The Philadelphia chromosome The Philadelphia chromosome t(9;22)(q34;q11) is found in 95% t(9;22)(q34;q11) is found in 95% of patients and is caused by a of patients and is caused by a reciprocal translocation which reciprocal translocation which leads to a novel fusion protein leads to a novel fusion protein BCRBCR--ABL ABL
Cytogenetik och molekylCytogenetik och molekyläärgenetik vid rgenetik vid KMLKML
47,XY,+8,t(9;22)(q34;q11.2)47,XY,+8,t(9;22)(q34;q11.2)
BCRBCR--ABLABL
BCRBCR--ABL ABL fusion genefusion gene
ABL = ABELSON MURINE LEUKEMIA VIRAL ONCOGENE HOMOLOG 1 ABL = ABELSON MURINE LEUKEMIA VIRAL ONCOGENE HOMOLOG 1
BCR = BREAKPOINT CLUSTER REGION BCR = BREAKPOINT CLUSTER REGION
The leukemic effect of BCR/ABLThe leukemic effect of BCR/ABL
GlivecGlivec®® (STI571, (STI571, ImatinibImatinib ))
BcrBcr/Abl/Abl
STI571STI571
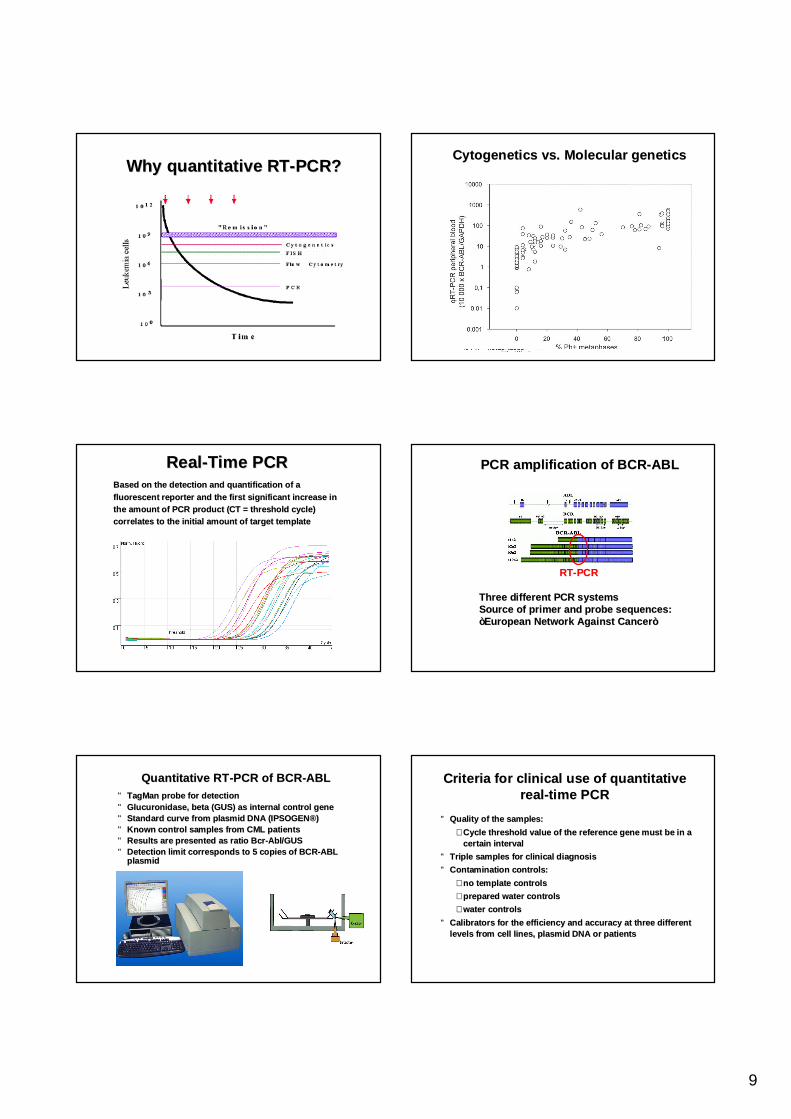
Why quantitative RTWhy quantitative RT--PCR of CML PCR of CML patients?patients?
•• For diagnosis and prognosisFor diagnosis and prognosis•• Treatment response and monitoringTreatment response and monitoring•• Early detection of relapseEarly detection of relapse•• Can be done on peripheral bloodCan be done on peripheral blood
9
Why quantitative RTWhy quantitative RT--PCR?PCR?CytogeneticsCytogenetics vs. Molecular geneticsvs. Molecular genetics
RealReal--Time PCRTime PCRBased on the detection and quantification of a Based on the detection and quantification of a fluorescent reporter and the first significant increase in fluorescent reporter and the first significant increase in the amount of PCR product (CT = threshold cycle) the amount of PCR product (CT = threshold cycle) correlates to the initial amount of target templatecorrelates to the initial amount of target template
PCR amplification of BCRPCR amplification of BCR--ABL ABL mRNAmRNA
RTRT--PCRPCR
Three different PCR systemsThree different PCR systemsSource of primer and probe sequences: Source of primer and probe sequences: ””European Network Against CancerEuropean Network Against Cancer””
Quantitative RTQuantitative RT--PCR of BCRPCR of BCR--ABLABL•• TagManTagMan probe for detectionprobe for detection•• GlucuronidaseGlucuronidase, beta (GUS) , beta (GUS) as internal control geneas internal control gene•• Standard curve from plasmid DNA (IPSOGENStandard curve from plasmid DNA (IPSOGEN®®))•• Known control samples from CML patientsKnown control samples from CML patients•• Results are presented as ratio Results are presented as ratio BcrBcr--Abl/GUSAbl/GUS•• Detection limit corresponds to 5 copies of BCRDetection limit corresponds to 5 copies of BCR--ABL ABL
plasmidplasmid
Criteria for clinical use of quantitative Criteria for clinical use of quantitative realreal--time PCRtime PCR
•• Quality of the samples: Quality of the samples: –– Cycle threshold value of the reference gene must be in a Cycle threshold value of the reference gene must be in a
certain intervalcertain interval•• Triple samples for clinical diagnosisTriple samples for clinical diagnosis•• Contamination controls:Contamination controls:
–– no template controlsno template controls–– prepared water controlsprepared water controls–– water controlswater controls
•• Calibrators for the efficiency and accuracy at Calibrators for the efficiency and accuracy at three different three different levels from cell lines, plasmid DNA or patientslevels from cell lines, plasmid DNA or patients

10
Clinical application in CMLClinical application in CML
•• RealReal--time Qtime Q--RTRT--PCR performed 4 times/year PCR performed 4 times/year for followfor follow--up up
•• Presently, over 100 CML patients under Presently, over 100 CML patients under ImatinibImatinib treatment or monitored after bonetreatment or monitored after bone--marrow transplantation at Sahlgrenskamarrow transplantation at Sahlgrenska
Time (months)
0 5 10 15 20 25 30 35
BCR
-ABL
/GAP
DH
-ratio
norm
aliz
ed to
bas
elin
e (%
)
0
50
100
150
200
Response on Response on ImatinibImatinibtreatmenttreatment
FISH 81,0% 20,0% 14,0% 2,0% 4,0% 3,0% 6,0%Cytogenetic nd nd nd nd nd nd nd
nd = not done
BloodMonths 0 3 6 9 12 15 18
PCR 30,78 20,14 5,36 2,15 3,54 3,45 3,12
Bone marrowMonths 0 3 6 9 12 15 18PCR 35,89 18,32 7,07 0,23 4,48 2,52 0,66
0
5
10
15
20
25
30
35
40
0 3 6 9 12 15 18
Months
Nor
mal
ized
BC
R-A
BL m
RN
A ex
pres
sion
Blood
Bone marrow
0
20
40
60
80
100
120
140
160
0 3 6 9 12 15 18 21 24 27
Months
No
rma
lize
d B
CR
-AB
L m
RN
A
exp
ress
ion
Blood
Bone marrow
BCRBCR--ABL expression in nonABL expression in non--responding CMLresponding CML
•• Primary resistance is defined as failure to achieve remission Primary resistance is defined as failure to achieve remission (hematologic 5% or cytogenetic 15%) in spite of therapeutic (hematologic 5% or cytogenetic 15%) in spite of therapeutic dosage of dosage of ImatinibImatinib in 3 and 6 month respectivelyin 3 and 6 month respectively
•• Secondary or acquired resistance is loss of established Secondary or acquired resistance is loss of established remission with a elevated remission with a elevated Bcr/AblBcr/Abl ratio with one log (10ratio with one log (10--fold fold increase)increase)
•• 48 month after diagnosis is the incidence of acquired 48 month after diagnosis is the incidence of acquired resistance 25% of patients in chronic phase CML, 75% of resistance 25% of patients in chronic phase CML, 75% of patients in accelerated phase and 95% of patients in blast patients in accelerated phase and 95% of patients in blast crisiscrisis
•• Only 30Only 30--50% of CML patients in blast crisis respond to 50% of CML patients in blast crisis respond to ImatinibImatinib
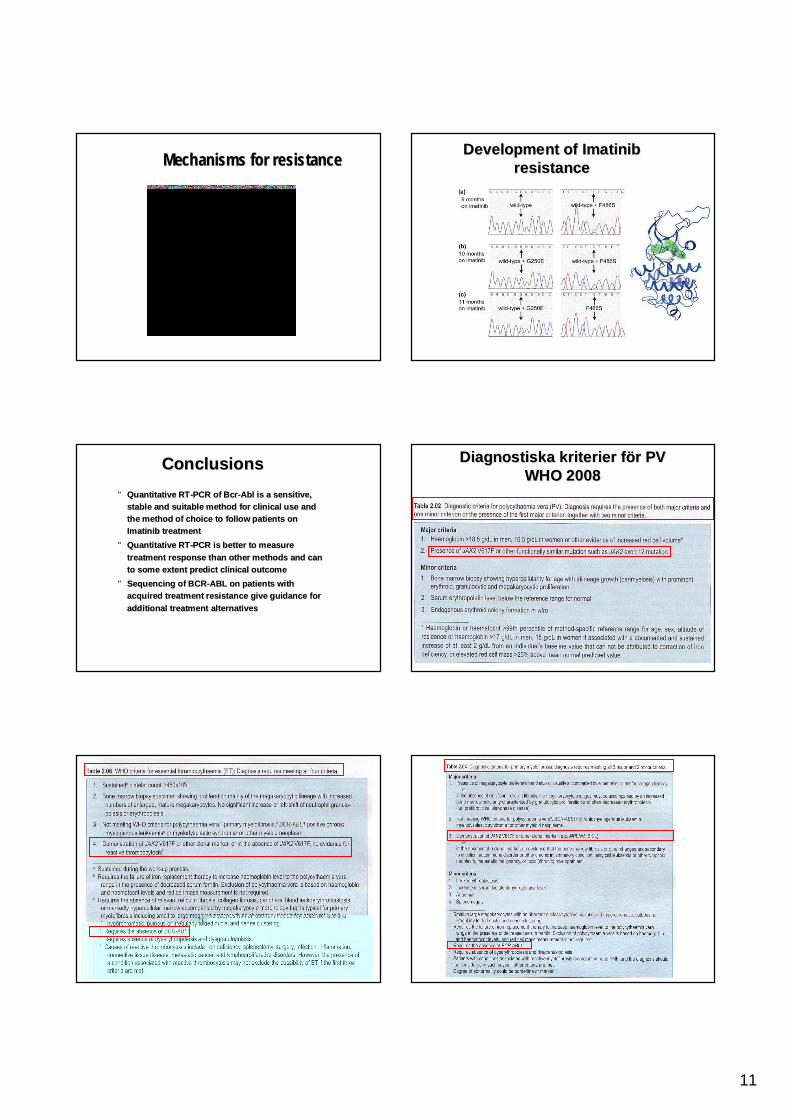
Treatment failure / Treatment failure / ImatinibImatinib resistanceresistance Development of Development of ImatinibImatinib resistanceresistance
•• 3535--90% depend on new point 90% depend on new point mutations in the kinase domain of mutations in the kinase domain of the the AblAbl genegene
•• Other mechanisms are gene Other mechanisms are gene amplification, new translocations amplification, new translocations and gene mutationsand gene mutations
•• Two new BCRTwo new BCR--ABL inhibitory ABL inhibitory drugs are now available which drugs are now available which have different resistance profilehave different resistance profile
11
Mechanisms for resistanceMechanisms for resistance Development of Development of ImatinibImatinibresistanceresistance
•• Quantitative RTQuantitative RT--PCR of PCR of BcrBcr--AblAbl is a sensitive, is a sensitive, stable and suitable method for clinical use and stable and suitable method for clinical use and the method of choice to follow patients on the method of choice to follow patients on ImatinibImatinib treatment treatment
•• Quantitative RTQuantitative RT--PCR is better to measure PCR is better to measure treatment response than other methods and can treatment response than other methods and can to some extent predict clinical outcometo some extent predict clinical outcome
•• Sequencing of BCRSequencing of BCR--ABL on patients with ABL on patients with acquired treatment resistance give guidance for acquired treatment resistance give guidance for additional treatment alternativesadditional treatment alternatives
ConclusionsConclusions Diagnostiska kriterier fDiagnostiska kriterier föör PV r PV WHO 2008WHO 2008
12
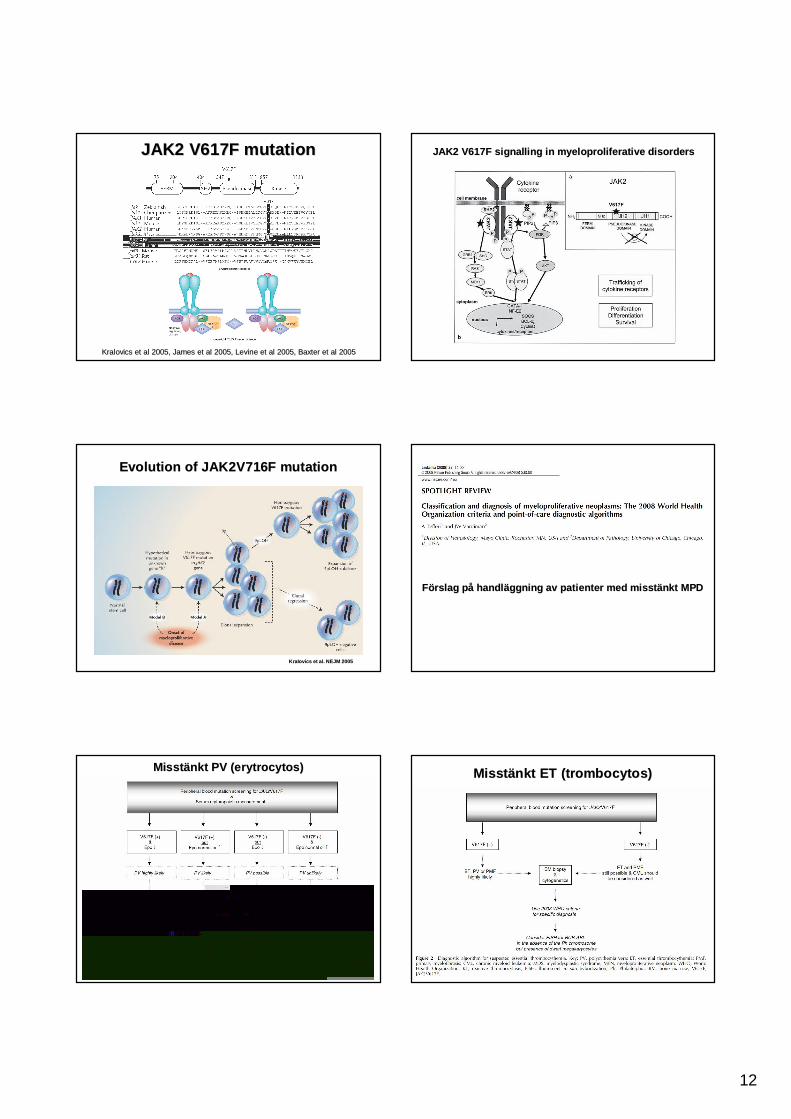
JAK2 V617F mutationJAK2 V617F mutation
KralovicsKralovics et al 2005, James et al 2005, Levine et al 2005, Baxter et al 2et al 2005, James et al 2005, Levine et al 2005, Baxter et al 2005005
JAK2 V617F JAK2 V617F signallingsignalling in in myeloproliferativemyeloproliferative disordersdisorders
KralovicsKralovics et al. NEJM 2005et al. NEJM 2005
Evolution of JAK2V716F mutation Evolution of JAK2V716F mutation
FFöörslag prslag påå handlhandlääggning av patienter med misstggning av patienter med misstäänkt MPDnkt MPD
MisstMisstäänkt PV (nkt PV (erytrocytoserytrocytos)) MisstMisstäänkt ET (nkt ET (trombocytostrombocytos))
13
MisstMisstäänkt nkt myelofibrosmyelofibros
Can JAK2V617F be used for treatment Can JAK2V617F be used for treatment monitoring?monitoring?
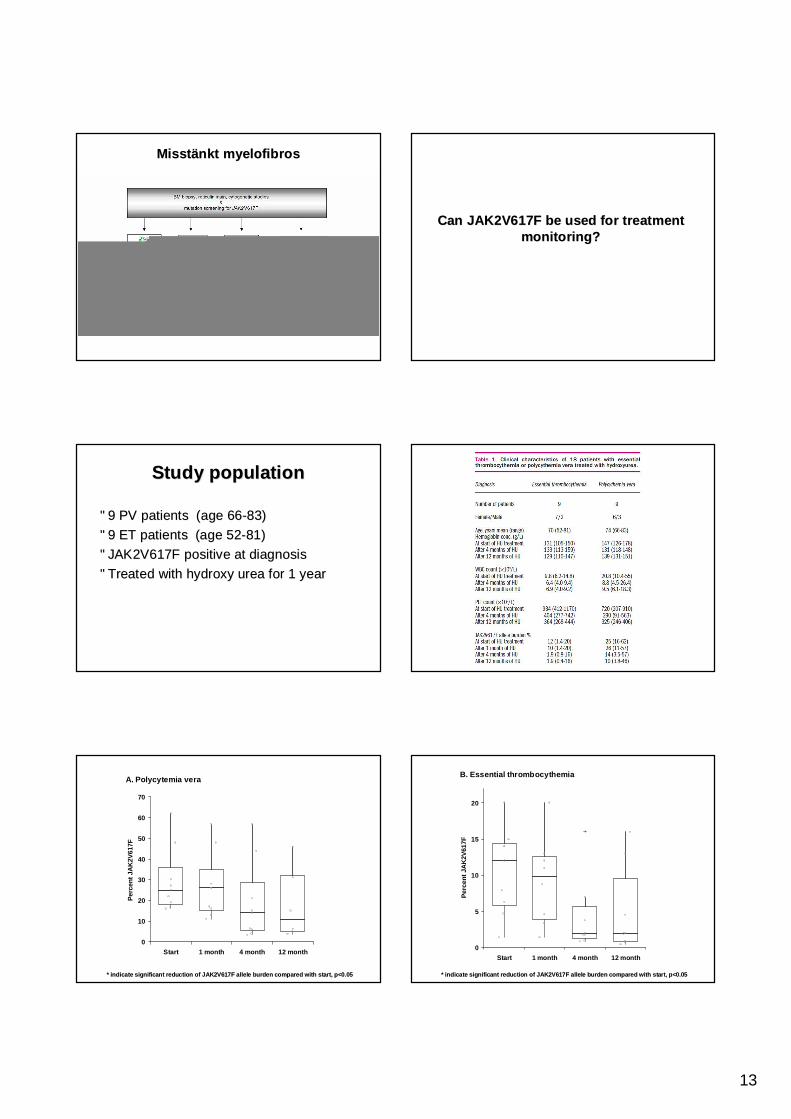
StudyStudy populationpopulation
•• 9 PV patients (age 669 PV patients (age 66--83)83)•• 9 ET patients (age 529 ET patients (age 52--81)81)•• JAK2V617F positive at diagnosisJAK2V617F positive at diagnosis•• Treated with Treated with hydroxyhydroxy urea for 1 yearurea for 1 year
* indicate significant reduction of JAK2V617F allele burden comp* indicate significant reduction of JAK2V617F allele burden compared with start, p<0.05ared with start, p<0.05
A. Polycytemia vera
0
10
20
30
40
50
60
70
Start 1 month 4 month 12 month
Perc
ent J
AK
2V61
7F
* indicate significant reduction of JAK2V617F allele burden comp* indicate significant reduction of JAK2V617F allele burden compared with start, p<0.05ared with start, p<0.05
B. Essential thrombocythemia
0
5
10
15
20
Start 1 month 4 month 12 month
Per
cent
JA
K2V
617F
14
ConclusionConclusion
•• SignifikantSignifikant reduction of JAKV617F reduction of JAKV617F allelallel burden burden after 4 month treatment with after 4 month treatment with HydroxyHydroxy urea for urea for both PV and ET patients both PV and ET patients
•• The reduction persisted up to 12 monthThe reduction persisted up to 12 month•• Five patients (3 PV and 2 ET) showed no signs Five patients (3 PV and 2 ET) showed no signs
of JAK2V617F reductionof JAK2V617F reduction•• The study showed that quantitative PCR can be The study showed that quantitative PCR can be
used for treatment followused for treatment follow--up of patents with up of patents with JAK2V617F mutationsJAK2V617F mutations
Summary and conclusionsSummary and conclusions
•• Diagnosis and classification of most if not all malignant Diagnosis and classification of most if not all malignant hematological disorders require at least some genetic investigathematological disorders require at least some genetic investigations ions and informationand information
•• Genetic information is also used to guide which treatment patienGenetic information is also used to guide which treatment patients ts will receive in many cases (e.g. will receive in many cases (e.g. allogenicallogenic transplantation or different transplantation or different cytotoxiccytotoxic regimes)regimes)
•• However, this is only the beginning. In the near future many canHowever, this is only the beginning. In the near future many cancer cer treatments will probably be truly individualized. treatments will probably be truly individualized.
•• Knowledge of activated Knowledge of activated kinasekinase pathways (e.g. BCRpathways (e.g. BCR--ABL, FLT3, KIT, ABL, FLT3, KIT, JAK2) is already used for classification but new drugs targetingJAK2) is already used for classification but new drugs targetingthese are in advanced clinical trials as we speak.these are in advanced clinical trials as we speak.