Outcome and Prognostic Factors of Uterine Sarcoma in 59 ... 2010/Can_2.pdf · sarcoma (18.6%) ....
10
ABSTRACT Purpose: Uterine corpus sarcomas are rare heteroge- neous tumors characterized by rapid progression and poor response to treatment. This series investigated treatment options, relapse pattern, survival and prognostic factors. Patients and Methods: A total of 59 patients were treated in the National Cancer Institute, Cairo University, (2000-2007). Leiomyosarcoma accounted for 42.2% fol- lowed by carcinosarcoma (35.5%) and endometrial stromal sarcoma (18.6%). 40.7% had FIGO stage I disease, 30.5% were II, 16.9% were III and 11.9% were IV. Surgery was the primary line of treatment for all cases with total abdominal hysterectomy and bilateral salpingoophorectomy in 88% of cases and 12% had less extensive surgery. Twenty-four (40.7%) patients had surgery alone, 24 (40.7%) had surgery and radiotherapy, 7 (11.9%) had surgery and chemo-irradiation and 4 (6.7%) had surgery and chemotherapy. Results: After 27.4 months mean follow-up (range: 2-69), relapses were detected in 32 patients (59.2%) including 19 (59%) systemic metastases. Stage, adjuvant irradiation, tumor size, myometrial invasion, vascular and cervix invasion were significant factors in univariate analysis; nevertheless, multivariate prognostic factors were only stage (p=0.04) and adjuvant irradiation (p=0.01). 5-year cumulative disease free survival for stage I was 63.6%, 41.2% for stage II, 10% for stage III and 0% in stage IV. Neither extent of surgery, chemotherapy, histo- logic type or grade had significant effect on survival. Adjuvant radiotherapy offered 62% 2-year cumulative overall survival versus 22% for surgery alone and surgery with chemotherapy. Salvage surgery for isolated relapses was performed for 9/32 recurrent patients (28%) including 5 lung metastatectomies and 4 local pelvic resections. Mean survival after pulmonary resections was 7.4 months (6-14). Conclusion: Diagnosis of uterine sarcoma is in itself a poor prognostic factor. Complete cytoreductive surgery Journal of the Egyptian Nat. Cancer Inst., Vol. 22, No. 2, June: 113-122, 2010 Outcome and Prognostic Factors of Uterine Sarcoma in 59 Patients: Single Institutional Results OMAYA ABDUL HAMEED NASSAR, M.D., F.R.C.S. (Ed.) 1 ; SHERIEF BAHAA-ELDEEN ABDUL MOATY, M.D. 1 ; EL-SAYED ASHRAF KHALIL, M.D., F.R.C.S.I. 1 ; MAHA MOHAMED EL-TAHER, M.D. 2 and MERVAT EL NAJJAR, M.D. 2 The Departments of Surgical Oncology 1 and Radiotherapy 2 , National Cancer Institute, Cairo University, Egypt 113 and adjuvant radiotherapy is essential for local control, provided tumor is limited to the uterus. Adjuvant irradiation showed survival benefit. Key Words: Uterine cancer – Uterine sarcoma – Uterine sarcoma treatment – Sarcoma irradiation – Sarcoma prognosis. INTRODUCTION Unlike epithelial tumors, which carry a rel- atively good prognosis, uterine sarcomas are generally associated with a poor prognosis because of high rates of local recurrence and metastases with reported 5-year survival rates of 30-48% [1,2]. These tumors are rare repre- senting 4-9% of all invasive uterine cancers; that is why, it is difficult to make randomized studies to guide treatment and analyze prognos- tic factors in detail [2,3]. WHO histologic classification suggested two main categories. Pure mesenchymal sarco- mas including leiomyosarcoma (LMS) and en- dometrial stromal sarcoma (ESS), and mixed epithelial and mesenchymal sarcomas including mixed müllerian tumors (carcinosarcoma) (CS). 3 Each group of tumors exhibits a different pattern of spread, prognostic factors, and prob- ably varied response to treatment [3-5]. Surgery constitutes the initial and reference treatment that enables precise staging. Total abdominal hysterectomy and bilateral salpin- goophorectomy (TAH & BSO) represents the standard treatment of uterine sarcomas provid- ed the disease is limited to the uterus [5,6] . Radiotherapy and chemotherapy (RTH & CTh) are used in the adjuvant setting or as primary Correspondence: Dr Omaya Abdul Hameed Nassar, M.D. 13, 287 th Street/Almaady Aljadeeda, Cairo, Egypt, [email protected]
Transcript of Outcome and Prognostic Factors of Uterine Sarcoma in 59 ... 2010/Can_2.pdf · sarcoma (18.6%) ....

ABSTRACTPurpose: Uterine corpus sarcomas are rare heteroge-
neous tumors characterized by rapid progression and poorresponse to treatment. This series investigated treatmentoptions, relapse pattern, survival and prognostic factors.
Patients and Methods: A total of 59 patients weretreated in the National Cancer Institute, Cairo University,(2000-2007). Leiomyosarcoma accounted for 42.2% fol-lowed by carcinosarcoma (35.5%) and endometrial stromalsarcoma (18.6%). 40.7% had FIGO stage I disease, 30.5%were II, 16.9% were III and 11.9% were IV. Surgery wasthe primary line of treatment for all cases with totalabdominal hysterectomy and bilateral salpingoophorectomyin 88% of cases and 12% had less extensive surgery.Twenty-four (40.7%) patients had surgery alone, 24(40.7%) had surgery and radiotherapy, 7 (11.9%) hadsurgery and chemo-irradiation and 4 (6.7%) had surgeryand chemotherapy.
Results: After 27.4 months mean follow-up (range:2-69), relapses were detected in 32 patients (59.2%)including 19 (59%) systemic metastases. Stage, adjuvantirradiation, tumor size, myometrial invasion, vascular andcervix invasion were significant factors in univariateanalysis; nevertheless, multivariate prognostic factorswere only stage (p=0.04) and adjuvant irradiation (p=0.01).5-year cumulative disease free survival for stage I was63.6%, 41.2% for stage II, 10% for stage III and 0% instage IV. Neither extent of surgery, chemotherapy, histo-logic type or grade had significant effect on survival.Adjuvant radiotherapy offered 62% 2-year cumulativeoverall survival versus 22% for surgery alone and surgerywith chemotherapy. Salvage surgery for isolated relapseswas performed for 9/32 recurrent patients (28%) including5 lung metastatectomies and 4 local pelvic resections.Mean survival after pulmonary resections was 7.4 months(6-14).
Conclusion: Diagnosis of uterine sarcoma is in itselfa poor prognostic factor. Complete cytoreductive surgery
Journal of the Egyptian Nat. Cancer Inst., Vol. 22, No. 2, June: 113-122, 2010
Outcome and Prognostic Factors of Uterine Sarcoma in59 Patients: Single Institutional Results
OMAYA ABDUL HAMEED NASSAR, M.D., F.R.C.S. (Ed.)1;SHERIEF BAHAA-ELDEEN ABDUL MOATY, M.D.1; EL-SAYED ASHRAF KHALIL, M.D., F.R.C.S.I.1;MAHA MOHAMED EL-TAHER, M.D.2 and MERVAT EL NAJJAR, M.D.2
The Departments of Surgical Oncology1 and Radiotherapy2, National Cancer Institute, Cairo University, Egypt
113
and adjuvant radiotherapy is essential for local control,provided tumor is limited to the uterus. Adjuvant irradiationshowed survival benefit.
Key Words: Uterine cancer – Uterine sarcoma – Uterinesarcoma treatment – Sarcoma irradiation –Sarcoma prognosis.
INTRODUCTION
Unlike epithelial tumors, which carry a rel-atively good prognosis, uterine sarcomas aregenerally associated with a poor prognosisbecause of high rates of local recurrence andmetastases with reported 5-year survival ratesof 30-48% [1,2]. These tumors are rare repre-senting 4-9% of all invasive uterine cancers;that is why, it is difficult to make randomizedstudies to guide treatment and analyze prognos-tic factors in detail [2,3].
WHO histologic classification suggestedtwo main categories. Pure mesenchymal sarco-mas including leiomyosarcoma (LMS) and en-dometrial stromal sarcoma (ESS), and mixedepithelial and mesenchymal sarcomas includingmixed müllerian tumors (carcinosarcoma) (CS).3 Each group of tumors exhibits a differentpattern of spread, prognostic factors, and prob-ably varied response to treatment [3-5].
Surgery constitutes the initial and referencetreatment that enables precise staging. Totalabdominal hysterectomy and bilateral salpin-goophorectomy (TAH & BSO) represents thestandard treatment of uterine sarcomas provid-ed the disease is limited to the uterus [5,6].Radiotherapy and chemotherapy (RTH & CTh)are used in the adjuvant setting or as primary
Correspondence: Dr Omaya Abdul Hameed Nassar, M.D.13, 287th Street/Almaady Aljadeeda, Cairo, Egypt,[email protected]

114
treatment in advanced disease with controvesialprognostic significance [1,2,5-7].
This retrospective study analyses clinico-pathologic prognostic factors and the impact ofsurgery and adjuvant treatment on our cases.
PATIENTS AND METHODS
Retrospective series of 59 patients withhistological diagnosis of uterine sarcoma weretreated in the National Cancer Institute, CairoUniversity (2000-2007). Median age was 55years (15-80) and 46 patients (77%) were post-menopausal (Table 1). Vaginal bleeding wasthe presenting symptom in 42 cases (71%),followed by pelviabdominal mass in 6 (11%)and abdominal pain in 5 (9%). Two patientspresented with systemic metastases.
Endometrial biopsy allowed preoperativediagnosis for 21 patients (35.6%) and 8 caseshad endometrial adenocarcinoma that provedafter hysterectomy to be CS (Table 2 and Fig.1). Other patients were diagnosed by CT andUS and confirmed their histological diagnosisafter surgery.
Lines of treatment:FIGO staging system 8 for uterine corpus
cancer was adopted and TAH & BSO togetherwith medial parametrium (type II hysterectomy)was the main technique for resection (Table 1).
Adjuvant RTH and/or CTh were indicatedto patients with stage III & IVa, involved mar-gins, deep mural invasion, tumor size >10cmand nodal metastases.
External beam whole pelvis irradiation(EBRT) was given using the four-field tech-nique. Brachytherapy in addition to EBRT wasindicated with involved vaginal margins and/orparametrium involvement with a vault applica-tion.
Follow-up and statistical analysis:Scheduled regular follow-up with clinical
and radiological investigation followed dis-charge. Local recurrence in patients with relapsefree period less than 6-months was considereddisease progression. Cases with isolated localor lung relapses were subjected to salvage sur-gery if amenable to complete resection.
The endpoints were the duration of overall(OS) and recurrence free (DFS) survivals. Datawas analyzed using SPSSwin statistical packageversion 12. Numerical data were expressed asmean ± standard deviation (SD), median, min-imum and maximum. Qualitative data wereexpressed as frequency and percentage. Chi-square test or Fisher’s exact test was used toexamine the relation between qualitative vari-ables. Survival analysis used Kaplan-Meiermethod. Comparison between two survivalcurves was done using Log-rank test. Multivari-ate analysis was done using Cox-regressionmethod for the significant factors affectingsurvival on univariate analysis.
RESULTS
Treatment:Table (1) showed treatment given; where 24
patients (40.7%) had surgery alone, 24 (40.7%)had surgery and post operative RTH, 7 (11.9%)had surgery and combined CTh & RTH and 4advanced and metastatic cases (6.7%) had sur-gery and CTh alone as palliative therapy.
(TAH & BSO) was performed in 52 patients(88%). Less extensive surgery was used in 7patients (11.8%) assuming benign condition.They had subtotal hysterectomy (n=3), vaginalhysterectomy (n=2) and TAH with unilateralsalpingoophorectomy (n=2). Subtotal and vag-inal hysterectomies had no further surgery basedon having clear margins.
TAH & BSO variations included completionto TAH & BSO after subtotal hysterectomy in3 cases and 15 patients (28.8%) had extendedTAH & BSO to other organs due to tumor ex-tension. Extended resection included bilateralpelvic nodal dissection (PND) and paraorticnodal sampling in 9 cases (17.3%), cystectomyin 3 patients (anterior pelvic excentration),partial colectomy in 2 patients and 9 cases(17.3%) had Infracolic omentectomy.
Three (5%) post operative mortalities (pul-monary embolism, myocardial infarction andperitonitis) and 4 morbidities (6.7%) were noted(one vesicovaginal fistula and 3 with abdominalwall sepses).
A total of 31 patients had EBRT with 5000cGy median dose (4140-5040) divided to 25fractions over 40 days median period (32-60).
Outcome & Prognostic Factors of Uterine Sarcoma in 59 Patients

Omay a A. Nassar, et al. 115
Brachytherapy was applied in 6 cases with adose of 500cGy in two vault applications.
Eleven cases had 3-6 cycles of CTh. Sevencases had holoxan (ifosfamid) associated withadriamycin or epirubcin. Two patients presentingwith systemic lesions had (CYVADIC) cyclo-phosphamid, vencristine-adriamycin and decar-bazen and (MAID) mysna, adriamycin, ifospha-mide, decarbazen. Two cases with rhabdomyo-sarcoma had vincristine, cyclophosphamid andactinomycin D.
No RTH or CTh related mortalities wereobserved.
Pathological findings:Table (2) shows confirmed post surgery
pathological results. LMS was the most frequenttype in 25 cases (42.4%) followed by CS (35.5%) and ESS (18.6%). Two patients (15 and 18years) had subserosal rhabdomyosarcoma (19and 16 cm in diameter) invading the body butnot the cervix. Both had ovarian invasion andone had omental deposits.
Cervix invasion was less frequent in LMS(24%) in contrast to CS (61%) and ESS (45%).It was present in 9/17(53%) of stages III & IV.
Parametrium invasion was associated withcervix tumor extension in 4/6 (66%) of LMScases, 8/13 (61%) of CS patients and 1/5 (20%)of ESS. 9 cases had bilateral pelvic nodal dis-section and only two cases with ESS had nodalmetastases.
Close or invaded surgical margin was foundin 17 cases (28.8%) where 9/17 (53%) werestage III & IV.
Survival and relapse:Mean and median follow-up period were
27.4±19.7 and 21 months respectively (range:2-69). A total of 54 patients were assessed fortumor relapse after exclusion of post operativemortalities and 2 primary metastatic patients.Table (3) shows pattern of relapse in the totalgroup in each histological type and for stagegrouping.
Local pelviabdominal relapse was seen in23 of total 32 relapsed patients (72%); whereas,19/32 (59%) had systemic metastases. Localrelapse had similar incidence with each tumortype, 66% for LM, 72% for CS and 75% for
ESS. Median time to relapse was short for CSand ESS in comparison to that for LM as seenin Table (3). Concerning local disease relapse16/23 (69.5%) were considered true recurrence;whereas, 7/23 had disease progression (30.5%).
Systemic metastases were mainly in lungsin 14/19 cases (73.7%) followed by the liver in4 (21%) and bone in 3 patients (15.8%).
Mean and median relapse free survival pe-riod were 24.6±3 and 20.5 months (1-69) andmedian survival after recurrence was 6 months(1-13).
Salvage surgery for isolated relapses wasperformed in 9/32 of total relapses (28%). Fivepatients had lung metastatectomy for isolatedmetastases (2 cases of CS and 3 of LMS aftera median disease free period of 2.5 months (2-23). Follow-up of these patients after secondsurgery showed median survival of 7.4 months(6-14) and all died of more lung metastases.
Four patients (2 ESS and 2 LMS) with cen-tral local recurrence at vaginal vault (n=3) andstump (n=1) had salvage resection. Three pa-tients had RTH due to involved resection marginin the prior surgery. Disease free periods were2, 2, 9 and 12 months and one patient hadcombined external and brachytherapy. Vaginalvault recurrences were resected with cystectomyin two patients and sigmoid colectomy in onepatient. Patients died of repeated abdominalrecurrences and lung deposits after 2-3 months.
5-year cumulative OS stratified with stagewas 77.3% for stage I, 52.9% for stage II, 10%for stage III and 0% for stage IV. 5-year diseasefree cumulative survival was 63.6% for stageI, 41.2% for stage II, 10% for stage III and 0%for stage IV.
Prognostic factors:Univariate analyses of prognostic factors
against median DFS and OS periods revealed6 significant factors namely, stage, adjuvantRTH, tumor size, depth of invasion, cervixextension and vascular invasion (Table 4). Tu-mor histology had nonsignificant prognosticvalue on survival (Fig. 2).
There was a significant increase in OS andDFS times when comparing stage I patientswith other stages (p=0.012 and 0.015 respec-tively) (Fig. 3).
116 Outcome & Prognostic Factors of Uterine Sarcoma in 59 Patients
Surgical margin status had no effect on OSmean with p-value (0.5); though, negative mar-gin cases had higher 2-year cumulative DFS(50.5% versus 40.9%).
No statistical significant effect for tumorgrade on OS was noticed (p=0.82) and also onconsidering tumor grade in each histologic type(p=0.8 for LMS, =0.9 for CS & =0.08 for ESS).
Depth of myometrial invasion whether, lessor more than inner half without regard to serosalinvasion had significant prognostic effect onOS and DFS (p=0.01 & 0.009 respectively).This effect was noticed for CS tumors only(p=0.023) and not for LMS (p=0.09) or ESS(p=0.3).
Vascular invasion was significant prognosticfactor on OS and DFS for the whole group andfor CS (p=0.019) whereas; LMS (p=0.08) andESS (p=0.29) had no significance.
Tumor size (largest diameter) had significantimpacts on both OS and DFS. Similar highsignificance OS effect has been found for CS(p=0.0007) and ESS (p=0.045) however, LMShad no effect (p=0.5).
Survival time (OS) after TAH & BSO showedno significance difference with less extensivesurgery (p=0.64); however, the mean survival(27.7 months), the median survival (16.0months) and 2-year cumulative survival (50.2%)were better than survival of less extensive pro-
cedures (mean and median = 20.2 and 10.2months respectively and cumulative=37.5%).DFS time after TAH & BSO showed highermean and median (26.30 & 18.60 months) ascompared with less surgical procedures meanand median (10.61 & 6.37 months) with stillinsignificant p-value (0.34).
Patients who received CTh showed worsemedian survival times (7.6 months versus 16for the no CTh patients) and cumulative 2-yearOS survival of 40% versus 53.3% for the noCTh group; however, this contradictory wasinsignificant (p=0.411).
There was significant increase in OS andDFS for postoperative RTh with p-value (0.002and 0.017 respectively) (Fig. 4). Mean andmedian survival periods were 32.7 and 30.6months in contrast to 12.93 and 5.5 for non-irradiated group. 2-year cumulative OS for RThgroup was 71.3% versus 26.59% for cases with-out RTh. Similarly, 2-year cumulative DFS washigh (62% versus 22%). Considering effect ofRTH in relation to stage grouping mean survivalfor FIGO I&II treated by RTH was 35.5±4.8months versus 14.17±4.3 months for same stagepatients not treated by irradiation. Similar resultswere seen for stages III & VI (20.6±9 vs. 15±5months).
Multivariate analyses of significant prognos-tic factors revealed stage and adjuvant RTH asthe only two independent factors for OS andDFS (Table 5).
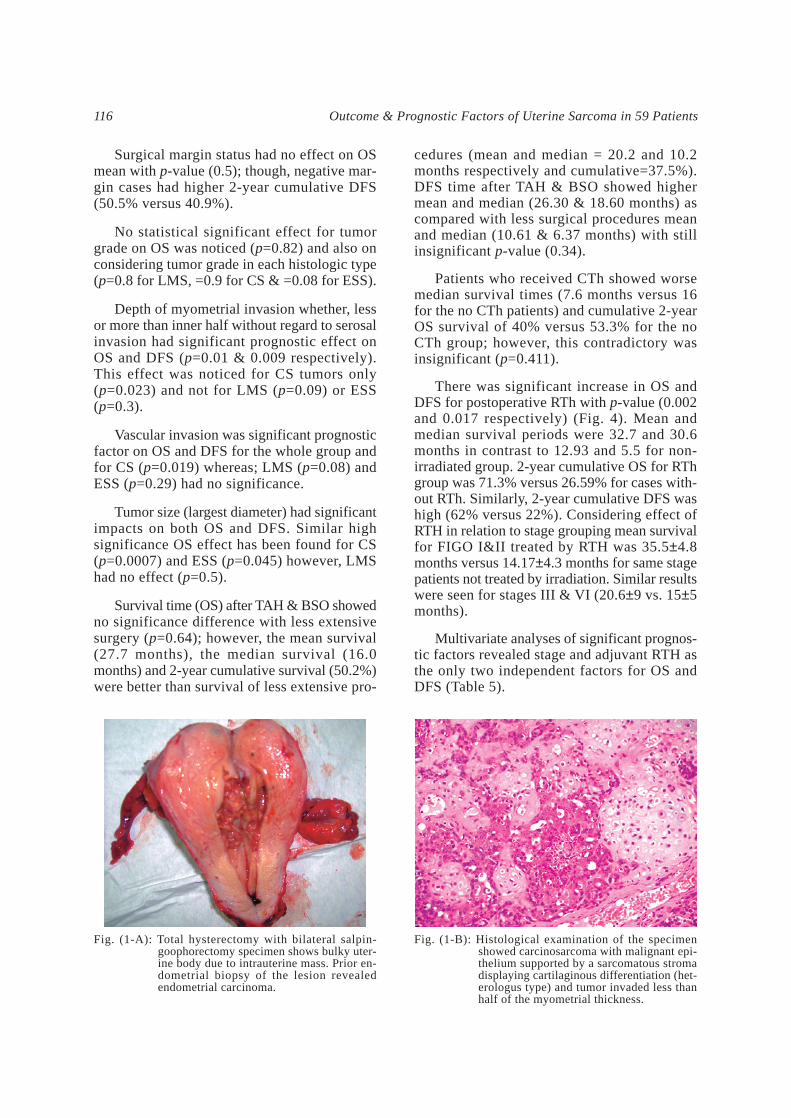
Fig. (1-A): Total hysterectomy with bilateral salpin-goophorectomy specimen shows bulky uter-ine body due to intrauterine mass. Prior en-dometrial biopsy of the lesion revealedendometrial carcinoma.
Fig. (1-B): Histological examination of the specimenshowed carcinosarcoma with malignant epi-thelium supported by a sarcomatous stromadisplaying cartilaginous differentiation (het-erologus type) and tumor invaded less thanhalf of the myometrial thickness.

Omay a A. Nassar, et al. 117
Table (1): Treatment offered to 59 patients with uterine sarcoma stratifiedwith stage grouping.
Surgery
TAH & BSO
Extended TAH & BSO
Less extensive
Adjuvant therapy
Radiotherapy
Chemotherapy
Treatment
TAH & BSO = Total abdominal hysterectomy and bilateral salpingoophorectomy.* = 2 patients with lung metastases at primary presentation (1 LMS and 1 CS) had
palliative resection and chemotherapy.~ = 2 patients with omental deposits (1 LMS and 1CS) had omentectomy in addition
to TAH & BSO and chemotherapy.
17 (100)
2 (11.8)*
12 (70.6)~
3 (17.6)
11 (64.7)
6 (35.3)
6 (35.3)*~
Stage III & IVNo. (%)
42 (100)
35 (83.3)
3 (7.1)
4 (9.5)
25 (59.5)
25 (59.5)
5 (11.9)
Stage I & IINo. (%)
59 (100)
37 (62.7)
15 (25.4)
7 (11.9)
36 (61)
31 (52.5)
11 (18.6)
TotalNo. (%)
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 7260
Time (months)
Overall Survival
p=0.884
Fig. (4): Disease free survival and adjuvantirradiation effect.
Pathological typeEndometrial stromalLeiomyosarcomaMixed müllerian
Fig. (2): Overall survivals for the main histologic typeswith no significance.
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 7260Time (months)
Disease Free Survival
p=0.017RTH
No
Yes
Fig. (3): Overall survivals with significant effect for tumorstage.
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 7260Time (months)
Overall Survival
p=0.026III
IIIIV
FIGO stage

118 Outcome & Prognostic Factors of Uterine Sarcoma in 59 Patients
Table (3): Pattern of relapses in relation to tumor type and stage in 54 evaluable uterine sarcoma patients.
Total relapse (%)
Local:
Recurrence
Progression
Systemic
Combined
Time to relapse
LMSCSESS*RMSm
13 (86.7%)
7 (46.7%)
2
5
2 (13.3%)
4 (26.7%)
9.8 (1-44)m
III & IV(n=15)*
19 (48.7%)
6 (15.4%)
4
2
7 (17.9%)
6 (15.4%)
10.6 (2-42)m
I & II(n=39)*
2 (100%)
1
1
–
–
1
–
RMS(n=2)
4 (40%)
1 (10%)
–
1
1 (10%)
2 (20%)
4.6 (2-12)m
ESS(n=10)*
11 (55%)
7 (35%)
3
4
3 (15%)
1 (5%)
3.9 (1-7)m
CS(n=20)*
15 (68.2%)
4 (18%)
2
2
5 (22.7%)
6 (27.3%)
15.9 (2-44)m
LM(n=22)*
32 (59.2%)
13 (24%)
6
7
9 (16.6%)
10 (18.5%)
10.5 (1-44)m
Total(n=54)*
Pathological type Stage
= Leiomyosarcoma,= Carcinosarcoma,= Endometrial stromal sarcoma,= Number of patients exclusive of 2 metastatic cases at presentation and 3 post operative mortalities.= Rhabdomyosarcoma,= Months.
Table (2): Pathological characteristics of 59 patients after surgery.
Median age
Grade:
1
2
3
FIGO Stage:
I
II
III
IV
Median tumor size
Myometrial invasion (>50%)
Cervix invasion
Vascular invasion
Involved surgical margin
Nodal metastases
* Include 2 rhabdomyosarcoma patients,LMSCSESS
= Leiomyosarcoma,= Carcinosarcoma,= Endometrial stromal sarcoma.
45
6 (55)
–
5 (45)
6 (55)
2 (18)
2 (18)
1 (9)
7cm (3-12)
7 (63)
5 (45)
5 (45)
3 (27)
2 (18)
ESS (n=11)No. (%)
63
1 (5)
17 (81)
3 (14)
8 (38)
9 (43)
3 (14)
1 (5)
7.9cm (4-14)
9 (43)
13 (61)
8 (38)
6 (28.5)
0
CS (n=21)No. (%)
50
2 (8)
14 (56)
9 (36)
10 (40)
7 (28)
4 (16)
4 (16)
12cm (3-35)
16 (64)
6 (24)
7 (28)
8 (32)
0
LMS (n=25)No. (%)
55
9 (15.3)
33 (55.9)*
17 (28.8)
24 (40.7)
18 (30.5)
10 (16.9)*
7 (11.9)*
10 (3-35)
32 (54)
24 (40.7)
21 (35.6)*
17 (28.8)
Total (n=59)*No. (%)

Omay a A. Nassar, et al. 119
Table (4): Clinico-pathological prognostic factors studied for the effect onoverall and disease free survival period (OS &DFS).
Age:>50<50
Pathology:LMSCSESS
Surgical margin:–ve+ve
Grade:12 & 3
Stage:IIIIIIIV
Radiotherapy:YesNo
Myometrial invasion:<50%>50%
Tumor size:<10cm>10cm
Cervix invasion:NoYes
Vascular invasion:NoYes
SE = Standard error. *Significant factors.Effects were similar on both survival types.
OS DFS
Univariate
Prognostic factor
0.483
0.6
0.10
0.31
0.015*
0.017*
0.009*
0.006*
0.010*
0.013*
p-value
19±3.6417±5.28
23±4.47±4.826±8.2
19±3.612±5.3
17.2518±3.37
34±4.796.5±48.5±8.15±5.9
30±4.365.5±3.28
33.5±4.415±3.37
28±3.677±4.13
30±3.765±3.72
28±3.775±4
Median±SE
0.426
0.8
0.5
0.82
0.012*
0.002*
0.010*
0.019*
0.005*
0.023*
p-value
21±3.1621±4.7
29±417±4.126±7.3
21±3.1717±4.7
20.5±4.2621±2.96
34±4.3618±313±78±5.57
30.6±3.913.5±2.8
35.6±3.8313±3.15
28.6±3.2812.5±3.82
30.5±5.3912±3.36
30±3.413±3.51
Median±SE
Table (5): Independent prognostic factors for overall and disease free survival.
OS
DFS
95% CI for OR
8.95.1
7.74.8
Upper
1.071.3
1.041
Lower
3.12.6
2.82.2
OR
0.040.01
0.040.05
p-value
0.540.35
0.50.4
SE
1.130.9
1.040.8
B
FIGO stageRadiotherapy
FIGO stageRadiotherapy
Independentfactors
: Regression coefficient.: Standard error.: Odds ratio.: Confidence interval (Lower = Stages II-IV & no radiation treatment).
BSEORCI

120
DISCUSSION
Only 59 verified cases of uterine sarcomawere documented over 7 years at our institute,a major cancer treatment center, illustrating therarity of cases. Even though several results aresuggestive and some of them fall short of sta-tistical significance.
Uterine corpus sarcoma behave in a moreaggressive fashion than endometrial carcinomaas suggested by the fact that in this series 54%of tumors invaded more than 50% of uterinewall, 35% and 40% had vascular and cervicalinvasion with a large median tumor size of10cm. Total relapse was uniformly high for thedifferent histologic types in spite of aggressivetreatment given to the patients and median timetill recurrence was short particularly for CS andESS. Incidence of relapse (48.7%) was high forstage I & II though 90% had TAH & BSO and60% had adjuvant RTH and 87% of stage III &VI had relapses in spite of having extendedTAH & BSO in 70.6% and adjuvant chemo-irradiation in 64.7%.
Diagnosis poses a special problem becauseclinical presentation was not specific and avail-able imaging procedures could not confirmdiagnosis particularly in early stage [9]. Endome-trial sampling was inconclusive and only 35%of our study group had preoperative pathologicaldiagnosis. For most women with CS, samplinglead to a correct diagnosis, although in 30%only the carcinomatous features were evidentand the diagnosis was endometrial adenocarci-noma. The reverse is also true, and occasionally,CS is suspected on endometrial biopsy, but nosarcomatous features appear in hysterectomyspecimen [10]. Symptomatic women with LMShave correct diagnosis in only 25-50% of casesand 75% of ESS is undetectable if the neoplasmis entirely intramural [10-13].
Age distribution of our patients was similarto that reported in literatures [12,13]; however,it was not a significant predictor of survivaland similarly several studies could not alsodocument such significance to age [4,14,15]. Onthe contrary others [1,7,16] found a favorablesurvival with patients <50 years.
In our study and other series [1,4,11,12] LMSwas the commonest histological diagnosis fol-lowed by CS and ESS. Histologic picture did
not have discriminating effect on survival inour group. EES showed little better median DFStime as compared to LMS & CS tumor however,this was insignificant (p=0.60) with no signifi-cance also for OS time possibly due to smallnumber of cases.
Other studies reported significant favorablesurvival for ESS in comparison to other types[1,4,11,14,15]. Sagae et al. [11] in a study on 106patient found that ESS had a favorable outcome(94.7% 5-year) in comparison to LMS and CS(78.8% and 63% respectively).
In this study there was no statistical signif-icant effect for grade on OS; however, Den-schlag et al. [15] were able to demonstrate asignificant association between tumor gradeand overall survival only in patients with ESS,but not in patients with LMS or CS. Livi et al.[1] found significant effect for grade on OS forall types. Chauveinc and colleagues [14] usedthe French grading system of soft tissue sarcomathat depends on tumor differentiation, mitoticcount and extent of tumor necrosis to grade 73cases. They found independent prognostic sig-nificance for this system on multivariate anal-ysis. Pautier et al. [4] could not reproduce thisprognostic significance with such grading sys-tem on survival or recurrence and even for anyhistologic type in a larger series (157 patients).
Tumor size had an impact on survival in ourseries but not as an independent factor as ob-served in other studies [7,16,17]. Callister et al.[18] found independent prognostic significancefor uterine length >10cm in 300 cases withmalignant mixed Müllerian tumors.
Depth of tumor invasion greater than 50%had a significant effect but it disappeared inmultivariate analysis in favor for tumor stage.Other authors [17,19] considered depth >50% anindependent factor for tumor with OS and DFS.
Cervix extension was significant on univari-ate analysis only. Similar result has been report-ed but with persistent significance on multivari-ate analysis [18].
Literatures [17,19] documented strong inde-pendent prognostic impacts on OS for lympho-vascular invasion particularly in early stages.Similar result was noticed in our study but thisvariable couldn’t stand in multivariate analysis.
Outcome & Prognostic Factors of Uterine Sarcoma in 59 Patients

Omay a A. Nassar, et al. 121
There is wide spread consensus in literaturesfor stage as an independent prognostic factor[1,2,4,6,14-16,19]. Comparing FIGO-I with otherstage was highly discriminating in our seriesfor both of incidence of relapse and survival.
A total of 57 in our study patients (96.6%)underwent abdominal surgical exploration andtwo patients had vaginal hysterectomy. 53 pa-tients had total hysterectomy (90%) whereas,6 cases had subtotal hysterectomy. Even though,extent of surgery was not translated in statisticalsignificance. Reports from eastern Asia [11,19,20]had stressed on complete cytoreductive surgeryas a strong prognostic factor principally forstages I & II.
The value of lymph node resection is highlycontroversial. Goff et al. [21] reported 47% and0% lymph node metastasis for early-stage LMSand ESS respectively. They found more frequentnode metastasis in LMS cases with recurrenceor peritoneal spread, and recommended system-atic lymphadenectomy for LMS. Leitao et al.[22] noted that survival in LMS has not beensignificantly affected by lymphadenectomy.On the other hand, Temkin et al. [23] concludedin their study that lymph node count in CScorrelated with the risk of recurrence and sur-vival.
There is general agreement for role of RTHregards local disease control; however, survivalbenefits are controversial with different conclu-sions [1,4,7,14-16,18]. In our study EBRT with orwithout intracavitary RTH improved DFS withbetter results in early stage. Also, significantincreased OS was observed in patients withpostoperative RTH (p=0.0017).
Le [24] and Gerszten et al. [25] showed im-provement of local disease control, with nostatistically significant difference in overallsurvival in patients treated with adjuvant pelvicRTH; whereas, others [17] found a statisticallysignificant impact on overall survival in patientswith CS, but not in the other histological sub-types. Some authors [1,26] reported increasedDFS for patients treated with high doses of 50-60Gy. Ferrer et al. [27] reported 5-year DFS andOS without RTH of 36% and 37%, respectively,in contrast with 76% and 73% when RTH wasgiven.
Adjuvant CTh had no significant impact onoverall survival in all of the histological subtypes
in our cases and other authors [15]. On the otherhand Wu et al. [6] reported DFS benefit for adju-vant CTh.
Salvage lung metastatectomy could offer amean survival of 7.4 months (6-14); however,all cases developed another lung deposits. Theshort mean survival period after metastatectomyand salvage resection of local recurrence in thisstudy can be explained by the short relapse freeperiod of these cases and the aggressive tumormetastatic potential. Levenback et al. [28] re-ported 43% 5-year survival after resection ofpulmonary metastases, while, for other study[29], survival did not exceed 26 months. In aseries of 41 cases of LMS, Leitao et al. [30]reported a 71% survival at 2-years after second-ary resection. Recurrence within the first fol-lowing year after surgery and the quality of theresection were the only two prognostic factors.
In conclusion: Tumor recurrence was rapidin spite of aggressive surgery and adjuvantchemo-irradiation. Surgery must consider themicro dissemination probability with iliac andparaortic nodal sampling together with oment-ectomy and the possibility of intraperitonealhyperthermia. Adjuvant RTH should be consid-ered for all stages taking in consideration thediagnosis of uterine sarcoma by itself as a poorprognostic factor.
REFERENCES
1- Livi L, Andreopoulou E, Shah N, Paiar F, Blake P,Judson I, et al. Treatment of uterine sarcoma at theRoyal Marsden Hospital from 1974 to 1998. ClinicalOncology. 2004, 16: 261-8.
2- Akahiara J, Tokunaga H, Toyoshima M, Takano T,Nagase S, Yoshinaga K, et al. Prognosis and prognosticfactors of carcinosarcoma, endometrial stromal sarco-ma and uterine leiomyosarcoma; a comparison withendometrial adenocarcinoma. Oncology. 2006, 71:333-40.
3- Hendrickson MR, Kempson RL, McCluggage WC.Mesenchymal tumors and related lesions. In: TavassoliFA, Devilee P, editors. WHO classification of tumors.Lyon: JARC Press. 2003, 233-44.
4- Pautier P, Genestie C, Rey A, Morice P, Roche B,Lhommé C, et al. Analysis of clinicopathologic prog-nostic factors for 157 uterine sarcomas and evaluationof a grading score validated for soft tissue sarcoma.Cancer. 2000, 88: 1425-31.
5- Giuntoli RL, Bristow RE. Uterine leiomyosarcoma:Present management. Curr Opin Oncol. 2004, 16:324-7.
122
6- Wu TI, Chang TC, Hsueh S, Hsu KH, Chou HH, HuangHJ, et al. Prognostic factors and impact of adjuvantChemo for uterine leiomyosarcoma. Gynecol Oncol.2006, 100: 166-72.
7- Winter R, Ostor A, Kapp K. Primary treatment ofuterine sarcomas. Gynecologic Cancer: Controversiesin management, Elsevier Churchill Livingstone. 2004,(22): 301-16.
8- Shepherd JH. Revised FIGO staging for gynecologicalcancer. Br J Obstet Gynaecol. 1989, 96 (8): 889-92.
9- Kido A, Togashi K, Koyama T, Yamaoka T, FujiwaraT, Fujii S, et al. Diffusely enlarged uterus: Evaluationwith MR imaging, Radiographics. 2003, 23: 1423-28.
10- Yang GC, Wan LMS, Del Priore G. Factors influencingthe detection of uterine cancer by suction curettageand endometrial brushing. J Reprod Med. 2002, 47:1005-12.
11- Sagae S, Yamashita K, Ishioka S, Nishioka Y, TerasawaK, Mori M, et al. Preoperative diagnosis and treatmentresults in 106 patients with uterine sarcoma in Hok-kaido, Japan. Oncology. 2004, 67: 33-9.
12- Benoit L, Arnould L, Cheynel N, Goui S, Collin F,Fraisse J, et al. The role of surgery and treatmenttrends in uterine sarcoma. EJSO. 2005, 31: 434-42.
13- Olah KS, Dunn JA, Gee H. Leiomyosarcomas havea poorer prognosis than mixed mesodermal tumourswhen adjusting for known prognostic factors: Theresult of a retrospective study of 423 case of uterinesarcoma. Br J Obstetric Gynecology. 1992, 99 (7):590-4.
14- Chauveinc L, Deniaud E, Plancher C, Satre X, AmsaniF, de la Rochefordiere A, et al. Uterine sarcomas: TheCurie institute experience. Prognosis factors andadjuvant treatments. Gynecol Oncol. 1999, 72: 232-7.
15- Denschlag D, Masoud I, Stanimir G, Gilbert L. Prog-nostic factors and outcome in women with uterinesarcoma Eur J Surg Oncol. 2007, 33 (1): 91-5.
16- Koivisto-Korander R, Butzow R, Koivisto AM, Lem-inen A. Clinical outcome and prognostic factors in100 cases of uterine sarcoma: Experience in HelsinkiUniversity Central Hospital 1990-2001. GynecolOncol. 2008, 111: 74-81.
17- Rovirosa A, Ascaso C, Ordi J, Albellana R, ArenasM, Lejarcegui JA, et al. Is vascular and lymphaticspace invasion a main prognostic factor in uterineneoplasms with a sarcomatous component? A retro-spective study of prognostic factors of 60 patientsstratified by stages. Int J Radiat Oncol Biol Phys.2002, 52: 1320-9.
18- Callister M, Ramondetta LM, Jhingran A, Burk TW,Eifel PJ. Malignant mixed Müllerian tumors of theuterus: Analysis of patterns of failure, prognostic
factors, and treatment outcome. Int J Radiat OncolBiol Phys. 2004, 58 (3): 786-96.
19- Park JY, Kim DY, Suh DS, Kim JH, Kim YM, KimYT, et al. Prognostic factors and treatment outcomesof patients with uterine sarcoma: Analysis of 127patients at a single institution, 1989-2007. J CancerRes Clin Oncol. 2008, 134 (12): 1277-87.
20- Kokawa K, Nishiyama K, Ikeuchi M, Ihara Y, Aka-matsu N, Enomoto, et al. Clinical outcomes of uterinesarcomas: results from 14 years worth of experiencein the Kinki district in Japan (1990-2003). Int J Gy-necol Cancer. 2006, 16 (3): 1358-63.
21- Goff BA, Rice LW, Fleischacker D, Muntz HG, Falk-enberry SS, Nikrui N, et al. Uterine leiomyosarcomaand endometrial stroma sarcoma: Lymph node me-tastases and site of recurrence. Gynecol Oncol. 1993,50: 105-9.
22- Leitao MM, Sonoda Y, Brennan MF, Barakat RR, ChiDS. Incidence of lymph node and ovarian metastasesin leiomyosarcoma of the uterus. Gynecol Oncol.2003, 91 (1): 209-12.
23- Temkin SM, Hellmann M, Lee YC, Abulafia O. Early-stage carcinosarcoma of the uterus: The significanceof lymph node count. Int J Gynecol Cancer. 2007, 17(1): 215-9.
24- Le T. Adjuvant pelvic RTH for uterine carcinosarcomain a high risk population. Eur J Surg Oncol. 2001, 27:282-5.
25- Gerszten K, Faul C, Kounelis S, Huang Q, Kelley J,Jones MW. The impact of adjuvant RTH on carcino-sarcoma of the uterus. Gynecol Oncol. 1998, 68: 1-13.
26- Hoffmann W, Schmandt S, Kortmann RD, SchiebeM, Dietl J, Bamberg M. RTH in the treatment ofuterine sarcomas. A retrospective analysis of 54 cases.Gynecol Obstet Invest. 1996, 42: 49-57.
27- Ferrer F, Sabater S, Farrus B, Guedea F, Rovirosa A,Anglada L, et al. Impact of RTH on local control andsurvival in uterine sarcomas: A retrospective studyfrom the Group Oncologic Català-Occità. Int J RadiatOncol Biol Phys. 1999, 44: 47-52.
28- Levenback C, Rubin SC, McCormack PM, HoskinsWJ, Atkinson EN, Lewis JL Jr. Resection of pulmonarymetastases from uterine sarcomas. Gynecol Oncol.1992, 45: 202-5.
29- Anderson T, Mc Mahon J, Nwogu C, Pombo MW,Urschel JD, Driscoll DL, et al. Pulmonary resectionin metastatic uterine and cervical malignancies. Gy-necol Oncol. 2001, 83: 472-6.
30- Leitao M, Brennan M, Hensley M, Sonoda Y, HummerA, Bhaskaran D, et al. Surgical resection of pulmonaryand extrapulmonary recurrences of uterine leiomyo-sarcoma. Gynecol Oncol. 2002, 87: 287-92.
Outcome & Prognostic Factors of Uterine Sarcoma in 59 Patients