our website at . These new physicians ... · our website at . These new physicians compliment our...
28
-
Upload
hoangkhanh -
Category
Documents
-
view
217 -
download
2
Transcript of our website at . These new physicians ... · our website at . These new physicians compliment our...



As the President of Commonwealth Orthopaedics, I am pleased to provide you with the fifth edition of Commonwealth Orthopaedics.
On behalf of our physicians and staff, I would like to introduce two new physicians to our practice: Sarah Pettrone, MD, a hand specialist, will be practicing out of our Reston and Lansd-owne offices. Amanda B. Trucksess, MD, specializing in physiatry, will be accepting new patients and consults out of the Reston and Herndon offices. You can learn more about them on page 12 and on our website at www.c-o-r.com. These new physicians compliment our team of leading orthopaedic surgeons who have a broad range of capabilities to treat most any orthopaedic injury or disease.
The focus of this issue of the magazine is on hand and upper extremity problems, an area of special-ization that requires extensive training and expertise. Not surprisingly, upper extremity injuries are extremely common in our practice and we treat hundreds of patients with these problems every year. In this issue, you will read several fascinating patient stories that describe how these hand, wrist and elbow injuries have been treated successfully by our Commonwealth Orthopaedic specialists.
We hope you will enjoy reading the articles in this issue and find them informative and interesting. We look forward to providing you and your family with the excellent orthopaedic care that Common-wealth Orthopaedics has become known for.
Sincerely,
Mark C. Hartley, MD
Welcoming Remarks
Corporate Office11240 Waples Mill Rd., Ste. 403
Fairfax, VA 22030(703) 383-6456 • (703) 383-6465 fax
www.c-o-r.com
Office Locations
AlexandriaArlington
BurkeFairfax
Herndon
LansdowneRestonSpringfieldTyson’s Corner
PresidentMark C. Hartley, MD
Chief Executive OfficerWilliam L. Harvey
Chief Operating OfficerMaureen M.R. Cook
Chief Financial OfficerRichard T. Givens
Director of Physical TherapyJo-Anne Burton, PT
Director of Human ResourcesBernadette McGavran
Directors of MarketingDeborah R. MartinSuzanne M. Kelly
Editorial Mission: Commonwealth Orthopaedics magazine is an educational and informative resource for physicians, health care professionals, employer groups, and the general public. This publication provides a forum for communicating news and trends involving orthopaedic-related diseases, injuries, and treatments, as well as other health-related topics of interest.
Commonwealth Orthopaedics magazine is designed and published by Custom Publishing Design Group, Inc. To advertise in an upcoming issue please contact: 800.246.1637 or MyCompanyMagazine.com This publication may not be reproduced in part or whole without the express written consent of Custom Publishing Design Group, Inc
ContentsThe Hand and Wrist In the forefront of sport injuries .............................................................4
Arthritis of the thumb Advances for reducing pain .....................................................................8
Physiatrists help patients achieve maximum recovery ................................................................. 11
New Physicians Join Commonwealth Orthopaedics ................... 12
New Lansdowne Office .......................................................................... 13
Helping the Hand Surgery offers patients a way out of carpal tunnel pain ............ 14
Taking a Break Commonwealth Orthopaedics offers treatments for wrist fractures .............................................................. 16
Cure Elbow Pain There are many ways to heal the joint ......................................................................................... 18
On the cover:
Hiko, an avid tennis player and confident skier, had an accident while skiing in Canada and suffered a de-tached thumb ligament. J. Mark Evans, MD, an ortho-paedic surgeon at Com-monwealth Orthopaedics specializing in trauma and reconstructive hand sur-gery, performed outpatient surgery on Hiko to re-pair the dislocation of the thumb joint.

4 Commonwealth Orthopaedics | www.c-o-r.com
After surgery to repair her detached thumb
ligament and physical therapy to increase her
strength and mobility, Hiko was able to return to
the tennis court exactly three months after her
surgery. She is playing regularly now and even
competing in national tournaments!

Commonwealth Orthopaedics | www.c-o-r.com 5
The hand and wrist -
An avid tennis player and confident skier, Hiko always enjoyed an active, athletic life with her husband
and children in Fairfax, Virginia. But when she decided to follow the Canadian national ski team on a downhill run during a family vacation several years ago, her bravado had unfortunate consequences. Hiko fell and failed to release her ski pole, severely pulling her thumb. Unaware of the gravity of her injury, she skied again the next day. It wasn’t until she was back home that she began to notice her thumb wasn’t functioning well. “It was difficult to perform simple tasks without pain,” she recalls. “And when I played tennis it really hurt. That’s when I knew I needed to see a hand specialist.”’
Hiko’s internet search led her to J. Mark Evans, MD, an orthopaedic surgeon specializing in trauma and reconstructive hand surgery at Commonwealth Orthopaedics. He took one look at her thumb and knew the ligament was detached. Outpatient surgery was scheduled for the next day. After several weeks in a cast, Hiko began rehabilitation and was able to return to the tennis court exactly three months after her surgery. “My experience at Commonwealth was overwhelmingly positive,” she says. “I’m playing tennis regularly again and even competing in national tournaments!”
Sports injuries of the hand are increasingly common among Northern Virginia’s growing and aging baby boomer population. With 27 bones and an advanced network of blood vessels, muscles, tendons
and nerves working together in an extremely tight space, the hand and wrist are among the most complex parts of the body, and extremely vulnerable to injury.“At Commonwealth Orthopaedics, we see a wide range of sports-related hand injuries – everything from minor problems such as tennis elbow and tendonitis, to a fracture or dislocation of the wrist or finger joint, such as Hiko’s,” explains Dr. Evans, “We offer the most advanced diagnostic and surgical techniques, including arthroscopic surgery, to treat and rehabilitate patients.”
Some of the most common hand and wrist injuries include:
Skier’s Thumb• – a high-energy injury in which the ligament at the base of the thumb is torn, usually as a result of a fall.
Tennis or Golfer’s Elbow• – in which a tendon in the forearm fails and begins to tear away from the bone, often sending pain down the arm.
De Quervain’s Tendonitis • – inflammation of the tendon that runs down the forearm, through the wrist, to the thumb, brought on by activities including using a keyboard, golfing or fishing. Other forms of tendonitis can develop when lifting weights or practicing yoga.
Wrist Fractures• – fractures can occur with many athletic activities, and are frequently seen in roller blading and snow boarding. The scaphoid is the most commonly fractured bone in the
wrist due to falling on an outstretched hand.
Dropped or Baseball Finger • – occurs when the tendon that straightens the finger gets pulled off of the bone making the end of the finger droop and it cannot be fully straightened. This can be treated with a splint.
PIP Dislocation• –commonly referred to as a “finger jam”, this occurs during athletic activities where the hand comes into contact with a ball and can range from a sprain or simple dislocation to a complex dislocation or joint fracture.
Regardless of the severity of the injury, prompt attention from an orthopaedist with special training in treating hand and wrist conditions is crucial for long-term recovery and a return to sports. “It’s really important to get an accurate diagnosis as soon as possible,” says Sarah Pettrone, MD, orthopedic surgeon and hand specialist. “The earlier the condition is identified and treated, the more likely it is to heal properly. Failure to get timely treatment can lead to long term complications, such as arthritis and chronic pain.” Fortunately, most sports injuries of the hand can be treated with simple procedures that yield excellent results. Jammed fingers
In the forefront of sport inju-
Fortunately, most sports injuries of the hand can be treated with simple procedures that yield excellent results.

can be put back in proper alignment, often in the office. If the finger is broken, the joint may need to be immobilized. Tendon injuries are usually treated with ultrasound or cortisone injections. If the condition persists, surgery to open the tendon and remove diseased tissue may provide relief. Treatment for fractures of the wrist or finger joints vary with the severity of the break, with high-impact fractures often the most complex. In extreme cases, joint fusion or replacement may be the only option.
Advances in arthroscopy
One of the newest and most advanced techniques for hand and wrist injuries is arthroscopy – a minimally invasive surgical procedure to diagnose and treat problems inside the joint. Surgeons make small incisions and insert a tiny camera (called an arthroscope) into the wrist to view the anatomic parts and their movements. The camera projects the images on a television monitor, enabling the surgeon to identify and correct problems with pinpoint precision.
“While knee and shoulder arthroscopy have been around for many years, wrist arthroscopy is relatively new,” Dr. Pettrone says. “The development of smaller, more refined cameras and instruments means we can now use this technique to directly view the complex wrist joint and connecting ligaments and make a more accurate diagnosis.”
Wrist arthroscopy is minimally invasive with numerous benefits to the patient, including smaller incisions, less post-
operative pain, bleeding and tissue trauma, fewer complications and faster recovery. It is usually an outpatient procedure, with patients returning home several hours after surgery.
As wrist arthroscopy has evolved, many conditions that traditionally required open surgery can now be treated arthroscopically, including chronic wrist pain, scaphoid fractures, instability, inflammation and infection, ligament tears and carpal tunnel syndrome. Diagnostic arthroscopy is often used in patients with wrist pain of unknown origin that has not improved with conservative treatment.
The decision to perform arthroscopic versus traditional surgery usually depends on the diagnosis. “Some conditions are amenable and others are not,” Dr. Pettrone explains. “Some are treated equally well either way and surgeons often differ on which approach is best. At Commonwealth, we take many factors into consideration when deciding how to proceed, including the patient’s age, condition and overall health.”
Keeping injuries to a minimum
Preventing a sports-related hand injury may not always be possible, but there are steps people can take to reduce the impact. Dr. Evans advises athletes to practice strengthening exercises on a regular basis, stretch before any activity, and never play through pain. “Stretching and strengthening exercises that protect the hands and wrists are simple to perform and don’t require any special equipment,”
6 Commonwealth Orthopaedics | www.c-o-r.com
Continued from page 5
Wrist arthroscopy is minimally invasive with numerous benefits to the patient, including smaller incisions, less post-operative pain, bleeding and tissue trauma, fewer complications and faster recovery.
“Stretching and strengthening exercises that protect the hands and wrists are simple to perform and don’t require any specia l equipment . Squeezing a ball in the hand, doing wrist curls with light weights, or extending the fingers against the resistance of rubber bands are all very effective.” - Mark Evans, MD

he explains. “Squeezing a ball in the hand, doing wrist curls with light weights, or extending the fingers against the resistance of rubber bands are all very effective.”
Additionally, he advises his patients who are treated for hand or wrist injuries not to return to sports prematurely. “It’s very important to do so under the advice and guidance of your physician,” he says. “Just because you feel better does not mean your injury has completely healed or your body is ready for sports again.”
Mark Evans, MD, earned a BA in Natural Sciences with a minor in Public Health from Johns Hopkins University in Baltimore, Maryland, before receiving his medical degree from the
University of Pennsylvania School of Medicine in Philadelphia. He went on to complete his orthopaedic residency at Downstate/Kings County Medical Center in Brooklyn, New York. Then, to conclude his formal medical training, Dr. Evans completed a year-long fellowship in hand surgery at Tufts/New England Medical Center in Boston.
Sarah Pettrone, MD, earned her medical degree from the University of Virginia School of Medicine in Charlottesville. She completed an orthopaedic surgery internship and
residency at New York University Hospital for Joint Diseases, as well as a hand fellowship at the University of Washington in Seattle.
Commonwealth Orthopaedics | www.c-o-r.com 7

8 Commonwealth Orthopaedics | www.c-o-r.com
Cheryl DeAntonio, who suffered from advanced arthritis of the thumb, is back to her beloved hobbies of needlepoint, cross-stitch and embroidery after having minimally invasive outpatient surgery called basal joint arthroplasty. This surgery removed part of her thumb joint and replaced it with a tendon graft from her arm.
Arthritis of the thumb

can be mendedAdvances for reducing pain
Commonwealth Orthopaedics | www.c-o-r.com 9
that cartilage deteriorates and its smooth surface roughens. The bones then rub against each other, resulting in friction and joint damage.
The initial symptom most people feel is pain at the base of the thumb when gripping, grasping, pinching or applying force. As the condition worsens, other symptoms may develop, including swelling, stiffness or tenderness, greater difficulty performing simple tasks involving the hands and wrists, an aching discomfort after prolonged use of the affected hand, and an enlarged, bony appearance at the thumb’s base.
“Arthritis of the thumb, as with osteoarthritis in general, is the result of a combination of factors,” says Dr. Evans. “Joint injury or stress, the aging process, family history, muscle weakness, and repetitive use all contribute to the condition. Patients with rheumatoid arthritis and other diseases that impact cartilage structure and function are also prone to develop osteoarthritis.” In the early stages, arthritis of the thumb usually responds well to a variety of nonsurgical treatments including activity modification, rest, daily application of heat or ice, anti-inflammatory medication such as aspirin or ibuprofen, or wearing a supportive splint to allow the joint to heal. Simple hand strengthening exercises are also effective.
Patients with advanced arthritis or who do not respond to conservative treatment may be candidates for surgical reconstruction.
“Recent advances in joint replacement surgery offer more minimally invasive treatment options to successfully reduce or eliminate pain and improve thumb
When Cheryl DeAntonio first felt pain in the base of her right thumb, she dismissed it as just
another minor ache. But as she pursued her beloved hobbies of needlepoint, cross-stitch and embroidery, the pain grew worse and more frequent. “Eventually I had pain all the time,” says the 60-year-old retired medical assistant, who lives in Oak Hill. “It got so bad I couldn’t do everyday things like turn a key or open a jar without it really hurting. I knew I had to do something about it.”
DeAntonio consulted J. Mark Evans, MD, an orthopaedic surgeon specializing in trauma and reconstructive hand surgery at Commonwealth Orthopaedics, who diagnosed arthritis of the thumb, a debilitating condition that causes hand pain, stiffness and weakness, limiting range of motion and making it increasingly difficult to perform simple tasks. After discussing her treatment options, DeAntonio initially chose cortisone injections. But when the pain returned she decided surgery was the answer, and Dr. Evans performed a basal joint arthroplasty in 2005.
“Arthritis of the thumb occurs when the basal joint at the wrist and base of the thumb develops osteoarthritis from wear and tear,” explains Alexander Croog, MD, a Commonwealth Orthopaedics surgeon specializing in the hand, wrist and elbow. “It is most common among post-menopausal women, with one in eight developing some form of the disease, but the condition occurs in men as well, usually as the result of a past injury.”
In a normal basal joint, cartilage covers the ends of the bones, acting as a cushion and allowing the bones to glide smoothly against each other. As arthritis develops,

10 Commonwealth Orthopaedics | www.c-o-r.com
Continued from page 9
position and function,” says Dr. Croog. “With the development of smaller, more refined cameras and miniature surgical instruments, arthroscopy is now a viable alternative for a majority of patients with arthritis of the thumb.”
During this procedure, the surgeon makes a very small incision in the area around the thumb joint and inserts a tubular instrument called an arthroscope with a tiny camera attached. The camera projects an enlarged 3-D image of the interior of the joint onto a video monitor, enabling the surgeon to identify the trouble and correct it if necessary, cleaning inflamed tissues and removing any damaged bone. Arthroscopy is also used to insert biodegradable spacers – one of the most exciting new advancements in joint reconstruction – which act like cushions and provide temporary relief while the space fills with tissue over time. As tissue re-grows, the spacers are re-absorbed into the body. B e caus e i t i s minima l ly invas ive , arthroscopy is less traumatic for patients than traditional surgery. Benefits include smaller incisions, less post-operative pain, bleeding and tissue trauma, fewer complications and faster recovery. It is usually an outpatient procedure, with patients returning home several hours after surgery.
For Cheryl DeAntonio, the answer was the removal of arthritic bone and joint reconstruction – a procedure known as basal joint arthroplasty. Dr. Evans removed part of her thumb joint and replaced it with a tendon graft from her arm. The
minimally-invasive, outpatient procedure took just a couple of hours, and DeAntonio was back home that afternoon. “It was quick and painless and the incisions were so small if I didn’t tell you they were there, you wouldn’t see them,” she says.
DeAntonio wore a cast from her hand to her elbow for six weeks following surgery, but was able to return to work after two weeks. When the cast came off, Dr. Evans gave her some hand-strengthening exercises to do and she did not need physical therapy because her range of motion was normal. The pain has never returned.
Other surgical options include joint fusion (arthrodesis), where surgeons permanently fuse bones in the thumb joint to increase stability and relieve pain; osteotomy, which repositions the thumb joint to realign deformities and move them away from joint-bearing areas; and trapeziectomy, the removal of the trapezium bone that sits adjacent to the thumb joint.
“The decision to perform one surgery over another depends on how severe the condition is, as well as the patient’s age and overall health,” Dr. Evans says. “It’s important that patients consult an orthopaedic surgeon specially trained in reconstructive hand surgery to determine which option is best for them.”
Dr. Croog agrees. “All of these surgeries have extremely good outcomes and high patient satisfaction in terms of pain relief and restoring function. It’s very disabling to have something wrong with your hand that interferes with daily living, and it’s an intricate and delicate system to treat. But
with the proper remedy and care, patients can and do get better.”
Cheryl DeAntonio says she is proof of this and urges others in similar circumstances to take action. “Don’t live with the pain,” she advises. “It’s not worth it.”
Alexander Croog, MD, earned his medical degree from the University of Virginia School of Medicine. He completed his residency in orthopaedic surgery at New York University Hospital for Joint Diseases.
J. Mark Evans, MD, earned a BA in Natural Sciences with a minor in Public Health from Johns Hopkins University in Baltimore, Maryland, before receiving his medical degree from the
University of Pennsylvania School of Medicine in Philadelphia. He went on to complete his orthopaedic residency at Downstate/Kings County Medical Center in Brooklyn, New York. Then, to conclude his formal medical training, Dr. Evans completed a year-long fellowship in hand surgery at Tufts/New England Medical Center in Boston.
Arthroscopy is also used to insert biodegradable spacers - one of the most exciting new advancements in joint reconstruction - which act like cushions and provide temporary relief while the space fills with tissue over time.

Commonwealth Orthopaedics | www.c-o-r.com 11
Physiatrists help patientsachieve maximum recoveryBy Amanda B. Trucksess, MD
What is a physiatrist? A physiatrist, or Physical Medicine and Rehabilitation physician, is a medical doctor who specializes in the non-operative treatment of disorders of nerves, muscles, and joints.
Physical Medicine and Rehabilitation has been practiced in the United States since the 1930s, but many patients, and even physicians, know little about this highly technical subspecialty. Physiatrists complete a four year residency program following medical school in their specialty. They are trained to coordinate the care of complex medical issues including sports injuries, musculoskeletal trauma, traumatic brain injuries, and nerve injuries including spinal cord injuries. The physiatrist’s goal is to restore the patient’s mobility and physical function, improve their quality of life, and relieve their pain.
Who should see a physiatrist? Patients experiencing pain or dysfunction related to sports injuries overuse injuries, or who have injuries that involve nerve damage – anything from a herniated disc to a major work-related or car accident – can benefit greatly from the help of a physiatrist. This specialist is skilled in diagnosing and managing a variety of musculoskeletal conditions that cause acute and chronic pain and neurological dysfunction.
What specialized testing does a physiatrist perform?The physiatrist’s first job is to establish the source of nerve-related injury. A patient experiencing weakness in the arm, for example, could be suffering from anything from a pinched nerve in the neck to carpal tunnel in the wrist. Using special electromyography (EMG) and nerve conduction studies (NCS), which use electrodes to monitor muscle and nerve activity and to detect irregular functioning, the physiatrist determines the location and severity of nerve injury. A physiatrist can also perform selective nerve root blocks to determine the location and cause of
a patient’s radicular pain. This specialist is skilled in diagnosing and managing a variety of musculoskeletal conditions that cause acute and chronic pain and neurological dysfunction.
What treatments does a physiatrist employ?After diagnosing the location of the injury, physiatrists will employ a conservative course of therapy focusing on nonsurgical treatment options such as exercise, physical therapy, biomechanical adaptations, medications, joint and trigger point injections, spinal epidural injections, and mobility devices to improve their patients’ function. For their patients with low back pain, particularly radicular pain or “sciatica”, physiatrists can administer lumbar epidural spinal injections to decrease the inflammation and provide pain relief. The epidural spinal injection is an outpatient procedure. Many patients with acute pain need only a few treatments to resume normal activity. Even those with chronic pain may benefit from well selected injections that can improve their function dramatically. These results can provide tremendous improvements in the lives of those suffering from pain.
The nervous system may be mystifying terrain for most patients and many physicians. But for physiatrists with specific training in pain, musculoskeletal, and nerve disorders, the complex neural network is as navigable as familiar back roads. The physiatrist often can be the best companion for patients with these disorders during their journeys from painful dysfunction to maximum achievable recovery.
Dr. Amanda Trucksess attended The College of William and Mary where she was a member of their Division I swim team. With a strong interest in athletics as well as human
biomechanics and physiology, Dr. Trucksess graduated cum laude with a major in kinesiology.
Conditions a physiatrist treats include:• Sportsrelatedinjuries• Arthritis• Tendonitis• Backpain• Myofascialpain
Physiatrists use nonsurgical treatment options including:• Exercise• Physicaltherapy• Heatorice• Electricalstimulation• Medications• Steroidinjections• Spinalepidurals• Mobilitydevices• TriggerPointInjections• BOTOXinjectionsforpainrelief
Physiatrists can coordinate health care teams of professionals including:• Physicaltherapists• Occupationaltherapists• Orthopedicphysicians• Rheumatologists• PrimaryCarePhysicians
Electromyography (EMG) testing: AnEMGtestdetermineswhetheramuscleworks normally. The physiatrist establishes this by inserting a fine Teflon-coated needle into selected muscles and listening to the sound of the electrical activity the muscle generates while also watching the impulses as they appearon the screenof theEMGmachine.
Nerve conduction studies (NCS): These studies involve taping metal electrodes to the skin over muscles and nerves and applying small amounts of electrical stimuli to those areas. The physiatrist evaluates the response from the nerve or muscle to determine whether conduction of the impulse was normal.
She went on to earn her medical degree from the Virginia Commonwealth University School of Medicine at the Medical College of Virginia in Richmond where she was named to the Alpha Omega Alpha Honor Society. Following medical school, she completed a four year residency in Physical Medicine and Rehabilitation at the University of Virginia in Charlottesville.

12 Commonwealth Orthopaedics | www.c-o-r.com
Sarah Pettrone, MD, Hand Specialist
The daughter of an orthopaedic surgeon, Dr. Sarah Pettrone remembers accompanying her father on hospital rounds on weekends when she was young. Although she was not initially inclined to follow in his footsteps, she noticed how much her father enjoyed his job. That observation along with her lifelong involvement in athletics eventually drew her in the direction of orthopaedics. After graduating summa cum laude, Phi Beta Kappa, from the University of Notre Dame with a BS in Biology, Dr. Pettrone earned her medical degree from the University of Virginia School of Medicine in Charlottesville, Virginia. While there, she was selected as a Bowman Scholar. Following medical school, Dr. Pettrone completed an orthopaedic surgery internship and residency at New York University-Hospital for Joint Diseases as well as a hand fellowship at the University of Washington in Seattle. She was selected as one of the Administrative Chief Residents in her 5th year of residency at NYU.
Her particular areas of interest include hand and wrist fractures as well as nerve and tendon injuries of the upper extremity.
Amanda B. Trucksess, MD, Physiatrist
A native Virginian, Dr. Amanda Trucksess attended The College of William and Mary where she was a member of their Division I swim team. With a strong interest in athletics as well as human biomechanics and physiology, Dr. Trucksess graduated cum laude with a major in kinesiology. She went on to earn her medical degree from the Virginia Commonwealth University School of Medicine at the Medical College of Virginia in Richmond where she was named to the Alpha Omega Alpha Honor Society. Following medical school, she completed a four year residency in Physical Medicine and Rehabilitation at the University of Virginia in Charlottesville.
Physical Medicine and Rehabilitation (known as physiatry) is a sub-specialty of medicine that focuses on the restoration of function and the non-operative treatment of nerve, muscle, and bone disorders. For more information, see page 11.
Her special interests within her field include the diagnosis and treatment of athletic injuries, running medicine and gait biomechanics, electromyography/nerve conduction studies, and the diagnosis and treatment of low back pain, including the use of epidural-steroid injections, trigger point injections and BOTOX injections for pain management.
New Physicians JoinCommonwealthOrthopaedics

Commonwealth Orthopaedics | www.c-o-r.com 13
(left-right) Dr. William C. Lennen, Dr. SarahPettrone,Dr.Matthew J. Levinepractice at Commonwealth’s newest office location in Lansdowne
NEWLANSDOWNEOFFICE
Commonwealth Orthopaedics newestoffice in Lansdowne brings additional orthopaedic and physical therapy services to the rapidly growing Loudoun County region. The office is located across the streetfromInovaLoudounHospitalat19450 Deerfield Ave., Suite 400, Leesburg, VA 20176.
William C. Lennen, MD., Matthew J. Levine, MD, and Sarah Pettrone, MD, provide comprehensive orthopaedic services at this new location.
To schedule a physician office appointment at the new Lansdowne office, call
703-810-5207
Foraphysicaltherapyappointment, call 703-810-5208
14 Commonwealth Orthopaedics | www.c-o-r.com
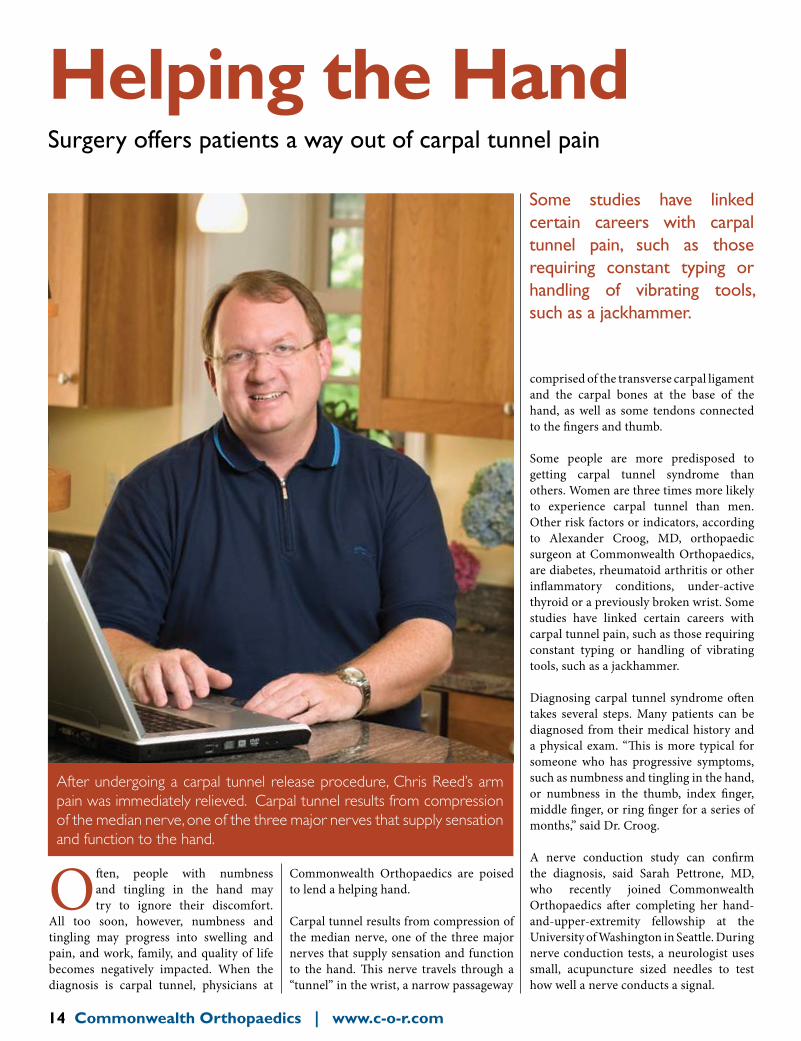
Helping the HandSurgery offers patients a way out of carpal tunnel pain
Some studies have linked certain careers with carpal tunnel pain, such as those requiring constant typing or handling of vibrating tools, such as a jackhammer.
Often, people with numbness and tingling in the hand may try to ignore their discomfort.
All too soon, however, numbness and tingling may progress into swelling and pain, and work, family, and quality of life becomes negatively impacted. When the diagnosis is carpal tunnel, physicians at
Commonwealth Orthopaedics are poised to lend a helping hand.
Carpal tunnel results from compression of the median nerve, one of the three major nerves that supply sensation and function to the hand. This nerve travels through a “tunnel” in the wrist, a narrow passageway
comprised of the transverse carpal ligament and the carpal bones at the base of the hand, as well as some tendons connected to the fingers and thumb.
Some people are more predisposed to getting carpal tunnel syndrome than others. Women are three times more likely to experience carpal tunnel than men. Other risk factors or indicators, according to Alexander Croog, MD, orthopaedic surgeon at Commonwealth Orthopaedics, are diabetes, rheumatoid arthritis or other inflammatory conditions, under-active thyroid or a previously broken wrist. Some studies have linked certain careers with carpal tunnel pain, such as those requiring constant typing or handling of vibrating tools, such as a jackhammer.
Diagnosing carpal tunnel syndrome often takes several steps. Many patients can be diagnosed from their medical history and a physical exam. “This is more typical for someone who has progressive symptoms, such as numbness and tingling in the hand, or numbness in the thumb, index finger, middle finger, or ring finger for a series of months,” said Dr. Croog.
A nerve conduction study can confirm the diagnosis, said Sarah Pettrone, MD, who recently joined Commonwealth Orthopaedics after completing her hand-and-upper-extremity fellowship at the University of Washington in Seattle. During nerve conduction tests, a neurologist uses small, acupuncture sized needles to test how well a nerve conducts a signal.
After undergoing a carpal tunnel release procedure, Chris Reed’s arm pain was immediately relieved. Carpal tunnel results from compression of the median nerve, one of the three major nerves that supply sensation and function to the hand.

is cut, so the median nerve (the one that is aggravated) has more room. Carpal tunnel is a type of compressive nerve injury, so relieving the compression relieves the symptoms. Usually, when patients return for their first visit after a week and a half, they notice significant improvement.”
In addition, Dr. Pettrone practices endoscopic carpal tunnel release. “The incision is located more proximally in the wrist rather than over the palm,” she said. “I use a special instrument that includes a camera and a blade. The camera is inserted into the carpal tunnel, and then the ligament is released with the blade.” She said the rehabilitation time may be a bit faster and the scar somewhat less noticeable with this technique.
Surgeons advise patients to return to normal activity as soon as possible after carpal tunnel release surgery. “When the stitches come out, the patients have no limitations,” Dr. Croog said.
Alexander Croog, MD, earned his medical degree from the University of Virginia School of Medicine. He completed his residency in orthopaedic surgery at New York University Hospital for Joint Diseases.
Sarah Pettrone, MD, earned her medical degree from the University of Virginia School of Medicine in Charlottesville. She completed an orthopaedic surgery internship and
residency at New York University Hospital for Joint Diseases, as well as a hand fellowship at the University of Washington in Seattle.
After completing the tests, the patient must decide whether to wait or request a carpal tunnel release procedure. “You can try other options first, such as wearing a velcro brace that holds your wrist in a little bit of extension,” Pettrone said. Another option is non-steroidal anti-inflammatory medications (such as ibuprofen).
Several types of surgery are available at Commonwealth Orthopaedics. Dr. Croog
performs a minimal-incision carpal tunnel release. For this technique, the incision, which is usually about three centimeters, is made on the palm, close to the wrist.
As Dr. Croog described the procedure, “The top of the tunnel closest to the skin
After a carpal tunnel procedure, surgeons advise patients to return to normal activity as soon as possible.
Commonwealth Orthopaedics | www.c-o-r.com 15
CarpalTunnelSurgeryWorks
neurologist for nerve tests and a rheumatologist to investigate other possible causes for the symptoms, such as diabetes. After examining the results, Dr. Croog recommended that Reed undergo carpal tunnel release procedure.
“My pain was immediately relieved aftersurgery,” said Reed. “With a small incision at the base of my palm; it seemed like I was in and out of surgery, with very little time spent in post-op,” he recalled. “To relieve the discomfort of the incision, I only took my prescribed pain medication for two days.”
The outpatient surgery took place on Thursday, and Reed returned to work on Monday.Tendays later, Dr. Croog removed the bandage and the stitches. Reed noted, “I was very surprised
that the scar was barely noticeable.”
Two months after surgery for his right hand, Reed had the same procedure on his left hand, which was starting to exhibit similar symptoms just before he had his first surgery.
Heofferedadviceforpeoplewithcarpaltunnelpain: “Do not fear that the surgery will put you out of commission for normal activities. Recovery is quick.” Recently, he took his own advice.“I installed the roof rack on my SUV,something I couldn’t have done last summer before the surgery.”
During the summer, Chris Reed started to develop numbness and tingling in some of the fingers of his right hand. At first, he chalked it up to the more than average amount of typing he does in his job as a law librarian, using power tools, mowing the yard, and playing with his 2-year-old son,Owen.He laternoticed someswelling in his palm and eventually felt pain radiating up his arm at night, depriving him of sleep. That was when he realized it was time to seek help.
After some rudimentary tests, his primary care doctor referred Reed to hand specialist Alexander Croog, MD.The swelling in Reed’spalm prompted Dr. Croog to quickly schedule anMRItoruleoutsuchpossibilitiesasahandtumor. Dr. Croog then also referred him to a

16 Commonwealth Orthopaedics | www.c-o-r.com
From a child falling during summer sports to a senior slipping on the winter
ice, no one is immune to wrist fractures. Surgeons at Commonwealth Orthopaedics are trained to recognize all of the different types and the latest methods of treating these breaks.
Most wrist fractures occur when people extend their arms to brace themselves while falling. In such situations, the part of the wrist most commonly fractured
by young people and elders is the distal radius bone, according to Commonwealth Orthopaedics surgeon Alexander Croog, MD. “We are starting to find that in the older population, we may have under-treated wrist fractures.”
During surgery for a distal radius fracture, the doctor pieces the break back together, restoring its intended anatomic position. Sometimes, the doctor attaches a plate and screws to the front or back side of the
wrist to compress the two ends of the bone together. The plates and screws remain permanently. According to Dr. Croog, less complicated breaks can be fixed back into position with temporary pins that stick out of the wrist and can be removed without additional surgery.
Some wrist breaks are riskier than others. “The scaphoid bone is notorious for not healing,” said Sarah Pettrone, MD, who recently joined Commonwealth
Taking a Break
Most wrist fractures occur when people extendtheir arms to brace themselves from a fall.
Commonwealth Orthopaedics offers treatments for wrist fractures
After slipping on a step and breaking her wrist, VilmaYosharhadoutpatientsurgerytorealignthe bone and have a plate inserted for stability. After physical therapy to regain strength and movement, she is 90% back to normal with her activities such as gardening.

Commonwealth Orthopaedics | www.c-o-r.com 17
Orthopaedics after completing a hand-and-upper-extremity fellowship at the University of Washington in Seattle, “Since the blood supply to this area is not as robust as it is to other wrist bones, the bone doesn’t heal well, causing a predictable progression of wrist arthritis and pain over the years.”
Non-displaced scaphoid fractures can be treated with a cast that extends above the elbow to prevent the wrist from rotating, flexing, or extending for approximately six weeks, followed by a short-arm cast for several more weeks.
If the scaphoid fracture is not displaced or only minimally so, percutaneous fixation surgery, which involves making a small incision to create just enough space to insert the screw, may be a treatment option, according to Dr. Pettrone. As she explained, percutaneous fixation sometimes necessitates arthroscopy, which involves putting a camera into the wrist to view the position of the fracture.
While surgery may seem more complicated, Drs. Croog and Pettrone noted that it in cases such as scaphoid fractures, surgery often results in quicker rehabilitation and recovery. Rather than just setting the wrist back into place, the doctors explained, “indications are that surgeries lead to quicker recovery, with better results and less pain.”
A less common fracture occurs when the triquetral bone becomes compressed or impacted by a fall. The recommended treatment for this injury is wrist immobilization in a short-arm cast for four to six weeks.
Another common fracture affects the hook of hamate, a small hook-shaped projection that protrudes from the bone. Also known as the golfer’s fracture, this can occur when a golf club hits the palm of the hand, near the wrist, fracturing off the hook part and resulting in tenderness or pain in the palm and numbness and tingling between the ring and small finger. While the injury can heal in a cast, the bone may have to be surgically removed if the hook is displaced (moved out of proper position) or is not discovered or treated for a long time.
Alexander Croog, MD, attended Harvard University as an undergraduate and earned his medical degree from the University of Virginia School of Medicine. He completed his residency
in orthopaedic surgery at New York University Hospital for Joint Diseases. Dr. Croog served as the Mary S. Stern Hand and Upper Extremity Fellow at the University of Cincinnati.
Sarah Pettrone, MD, earned her medical degree from the University of Virginia School of Medicine in Charlottesville. She completed an orthopaedic surgery internship and
residency at New York University Hospital for Joint Diseases, as well as a hand fellowship at the University of Washington in Seattle.
FixingaFall:APatient’sPerspective
VilmaYosharslippedonastepandfelldownthe stairs last spring. “I was holding something in my hand and fell on it sideways with my fist closed,” the 75-year-old woman recalled. “I knew right away that my hand was broken because it was not in the right position.”
After the emergency-room physician determined the break was bad enough to need surgery, Yoshar contactedCommonwealth Orthopaedics, where shemetAlexanderCroog,MD.
X-rays revealed she had a fracture to thedistal part of her radius bone. It was a “very badbreakandverypainful”Yosharsaid.
After outpatient surgery to realign the bone and put in a plate for stability and to help with healing,Yoshar wore a splint for fourweeks.Shethenvisitedthephysicaltherapistto regain strength and movement.
“I almost had to re-learn how to use my hand,” Yoshar said.“For eight weeks, the therapistand I worked together twice a week for an hour, stretching, pulling, and twisting, until I was back to about 90 percent normal. Dr. Croog was proud of my progress.”
Yoshar returnedto theCommonwealthOrthopaedicsseveral times toremovethestitchesandtakeadditionalx-raystomonitorherhealingprogress.BythefollowingJuly,shepassedherfinalexam.“IamsopleasedwithDr.Croog,”shesaid.“Hewassuchaniceyoungman,verypleasant. And everything went according to schedule.”

Did you know it’s physically impossible for you to lick your elbow? The length from your wrist
to your elbow is the same as the length of your foot? When you hit your funny bone you are not hitting a bone at all but the unprotected nerve near the ulna (one of the two bones that run from your wrist to your elbow).
While these may be interesting and fun facts, the reality is the elbow (a hinge joint composed of bone, cartilage, ligaments, and fluid) is the culprit for 3 to 4 million physician visits each year.
The primary cause of elbow pain is tendinitis, an inflammation or irritation of a tendon (a thick fibrous cord that attaches muscle to bone). Although two familiar terms for tendinitis of the elbow are tennis and golfer’s elbow, this type of injury is not limited to sports activities. It is common with many activities involving repetitive motion. Other causes of elbow pain include sprains, strains, fractures, dislocations, bursitis (inflammation of small, fluid-filled sacs that lubricate and cushion your joints), cellulitis (inflammation of the skin near the elbow related to an infection), cubital (ulnar nerve) and radial (radial nerve) tunnel
syndrome, arthritis, and ,rarely, tumors. Because all of these sources of elbow
pain share similar signs and symptoms (inflammation, redness, warmth, swelling, tenderness, local pain, and decreased range of motion) a physician’s advice is often necessary to obtain a correct diagnosis and formulate a treatment plan.
Treating elbow pain
Treating elbow pain often consists of the application of an ice pack or heating pad, rest, and the use of anti-inflammatory medications. It is sometimes helpful to wear a “counterforce” brace to ease the pressure on the inflamed elbow tendon while the injury is healing.
For chronic pain or severe inflammation, corticosteroid (cortisone; steroid) injections (usually no more than three) are sometimes given. If the problem is bursitis, your doctor may need to drain the fluid. Cellulitis or other severe infections generally require antibiotic treatment, either orally or intravenously. For early stage arthritis, physical therapy, activity modification, and pain relievers may be enough. Corticosteroid injections are also sometimes used to treat osteoarthritis (also known as wear-and-tear arthritis) symptoms.
Surgicalsolutions
Until recently, elbow pain has mostly been treated nonsurgically. Lately, however, clinical evidence is proving the benefit of arthroscopy. As in other joints, arthroscopy of the elbow involves the use of fiber optics and a tiny camera that is inserted through small incisions near the affected area. Through these small incisions, the surgeon removes any loose bone or cartilage and smooths irregular surfaces on the bone. Arthroscopy can be performed as an
outpatient procedure, and it is not unusual for patients to go back to work or school or resume daily activities within a few days. However, it takes several weeks for the joint to fully recover and your surgeon may recommend a specific activity and rehabilitation program to speed recovery and protect future joint function.
Patients with injury to the ulnar collateral ligament (UCL) located on the inside of the elbow joint often have a procedure called UCL reconstruction, which is more familiar as Tommy John surgery. Named after the Los Angeles Dodgers pitcher who, in 1974, was the first professional athlete to have this procedure performed, it involves replacing the ligament in the medial part of the elbow with a tendon taken from another location in the arm or the leg. The procedure, first performed by Frank Joeb, MD, takes about two hours, and can return full range of motion after two months. Although it takes about a year to return to high level throwing, UCL reconstruction can save a pitcher’s career. Alarmingly, more high school athletes and younger players are facing the prospect of having UCL reconstruction, mostly because of incorrect throwing mechanics.For patients with significant loss or damage
Cure elbow pain
18 Commonwealth Orthopaedics | www.c-o-r.com
The primary cause of elbow pain is tendinitis, an inflammation or irritation of a tendon (a thick fibrous cord that attaches muscle to bone). Although two familiar terms for tendinitis of the elbow are tennis and golfer’s elbow, this type of injury is not limited to sports activities.
“Until recently elbowpain has mostly been treated nonsurgically. Lately, however, clinical evidence is proving the benefit of arthroscopy. ”
–MatthewJ.Levine,MD
“The elbow (a hinge joint composed of bone, cartilage, ligaments, and fluid) is the culprit for 3 to 4 million physician visits each year. ”
–MatthewJ.Levine,MD
to areas of the elbow joint, the damaged bone and cartilage at the ends of the bones can be resurfaced, which entails replacing just the surface area with artificial materials made of metal alloys and polyethylene. It is even now possible to totally replace the elbow with an artificial joint. Elbow arthroplasty is reserved for severely damaged and painful elbow joints due to degenerative arthritis or elbow fractures, usually in aging adults. The artificial elbow is considered successful by more than 90 percent of patients who have elbow joint replacement.
And one more interesting fact: Almost everyone who reads that it is physically impossible to lick their own elbow, tries it.
Matthew J. Levine, MD, e a r n e d h i s m e d i c a l degree at the University of Pennsylvania. He completed his orthopaedic surgery residency at George Washington University and
fellowship in sports medicine and shoulder surgery at Duke University. Dr. Levine also completed a fellowship in shoulder and elbow reconstruction in Sydney, Australia. He is a life-long athlete and has extensive experience with sports medicine.
Cure elbow pain There are many ways to heal that joint
Commonwealth Orthopaedics | www.c-o-r.com 19

20 Commonwealth Orthopaedics | www.c-o-r.com

Commonwealth Orthopaedics | www.c-o-r.com 21

22 Commonwealth Orthopaedics | www.c-o-r.com

Commonwealth Orthopaedics | www.c-o-r.com 23

24 Commonwealth Orthopaedics | www.c-o-r.com
Commonwealth Orthopaedics | www.c-o-r.com 25
Mike KrzyzewskiDePuy Orthopaedics, Inc. Hip PatientCoach of the 2008 U.S. Olympic Team of Men’s Basketball
© D
ePuy
Ort
hopa
edic
s, In
c. 2
008
“My advice? Don’t wait as long as I did.” – Coach K
As a hands-on coach, movement is a big part of my life. But
ten years ago, the pain of hip arthritis nearly forced me into
early retirement. I even started coaching my team from a chair!
When I talked to my orthopaedic surgeon, he told me that
DePuy Orthopaedics, Inc., a Johnson & Johnson company,
has hip and knee solutions designed for more natural motion.
Today, I have two hip replacements from DePuy Orthopaedics
and I move more naturally than I ever thought possible. In fact,
these hips feel so good, I sometimes forget they’re not really mine.
My only regret is that I didn’t do it sooner.
My advice? Don’t wait for the pain of severe hip or knee arthritis to
take you out of the game. Ask your doctor about DePuy today.
And never stop moving.
Don’t wait. For a free information kit, visit www.depuyusa.com today, or call 1-866-256-1032.
Important Safety Information
Joint replacement is not for everyone. There are potential risks.
Recovery takes time and success depends on factors like age, weight
and activity level. You and your surgeon will know if surgery is right for you.
ART_00_DUP_CoachKAd_P89145E.indd 1 7/22/08 10:39:53 AM

26 Commonwealth Orthopaedics | www.c-o-r.com
DirectoryAct College .................................................................................................... 22
Breg,Inc. ..............................................................................................................7
BrentAssociates,Inc. ................................................................................. 22
DePuyMitek .....................................................................................................7
DePuyOrthopaedics,Inc. ...................................................................... 25
GenzymeBiosurgery ........................................................................ 20, 21
Kwik Kopy Printing 605 Carlisle Dr. Herndon,VA20170 (703)435-5502•(703)435•8194Fax
Kyphon, Inc. ..................................................................................................... 23
Lambert,Riddle,Schimmel&Company ...................................... 24
NascottRehabilitationServices ......................... inside front cover
OrthoCareRN ............................................................ inside back cover
Professional Risk Associates .................................................................. 19
RestonHospitalCenter ........................................................back cover
Smith&Nephew ........................................................................................ 20
SterlingServices,inc. ................................................................................. 26
SupremeOrthopedicSystems ........................................................... 20
SynergyOrthopedics ............................................................................... 24
The Washington Group .......................................................................... 24
Tysons Corner Diagnostic Image ....................................................... 22
WachoviaBank ............................................................................................ 24
WestFinancialServices,Inc. ................................................................ 26

Commonwealth Orthopaedics | www.c-o-r.com 27
703.481.1919 www.OrthoCareRN.com
“A Specialized Home Recovery Program for Orthopaedic Rehabilitation”

CommonwealthOrthopaedics 11240WaplesMillRd.,Ste.403 Fairfax,VA22030