Osteoporosis Rajesh Kataria, D.O. Southern Ohio Rheumatology.
57
Osteoporosis Osteoporosis Rajesh Kataria, D.O. Rajesh Kataria, D.O. Southern Ohio Southern Ohio Rheumatology Rheumatology
Transcript of Osteoporosis Rajesh Kataria, D.O. Southern Ohio Rheumatology.
OsteoporosisOsteoporosis
Rajesh Kataria, D.O.Rajesh Kataria, D.O.
Southern Ohio RheumatologySouthern Ohio Rheumatology

DisclosuresDisclosures
Speaker’s BureauSpeaker’s Bureau
NovartisNovartis
Warner ChilcottWarner Chilcott
ObjectivesObjectives
State the indications for bone mineral State the indications for bone mineral density testingdensity testing
Understand and describe the utility of Understand and describe the utility of the FRAX toolthe FRAX tool
List the medications that have proven List the medications that have proven reduction on nonvertebral fracturesreduction on nonvertebral fractures

OsteoporosisOsteoporosis
“…is a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture.”
Consensus Development Conference: Diagnosis, Prophylaxis, and Treatment of Osteoporosis, Am J Med 1993;94:646-650. WHO Study Group 1994.

Definition of Osteoporosis

Bone HealthBone Health

Bone Remodeling (Turnover)Bone Remodeling (Turnover)

Cells in Bone TissueCells in Bone Tissue

Bone Remodeling CycleBone Remodeling Cycle
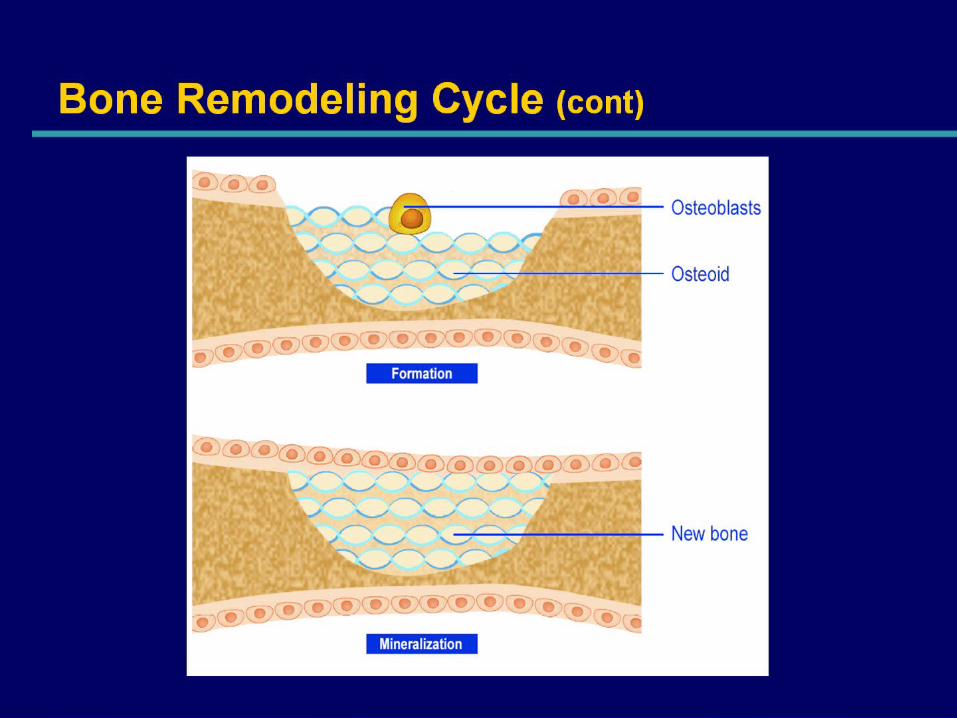
Bone Remodeling Cycle (cont)Bone Remodeling Cycle (cont)

Role of Modulators in Bone RemodelingRole of Modulators in Bone Remodeling

Unbalanced Remodeling in Menopause Leads to OsteoporosisUnbalanced Remodeling in Menopause Leads to Osteoporosis
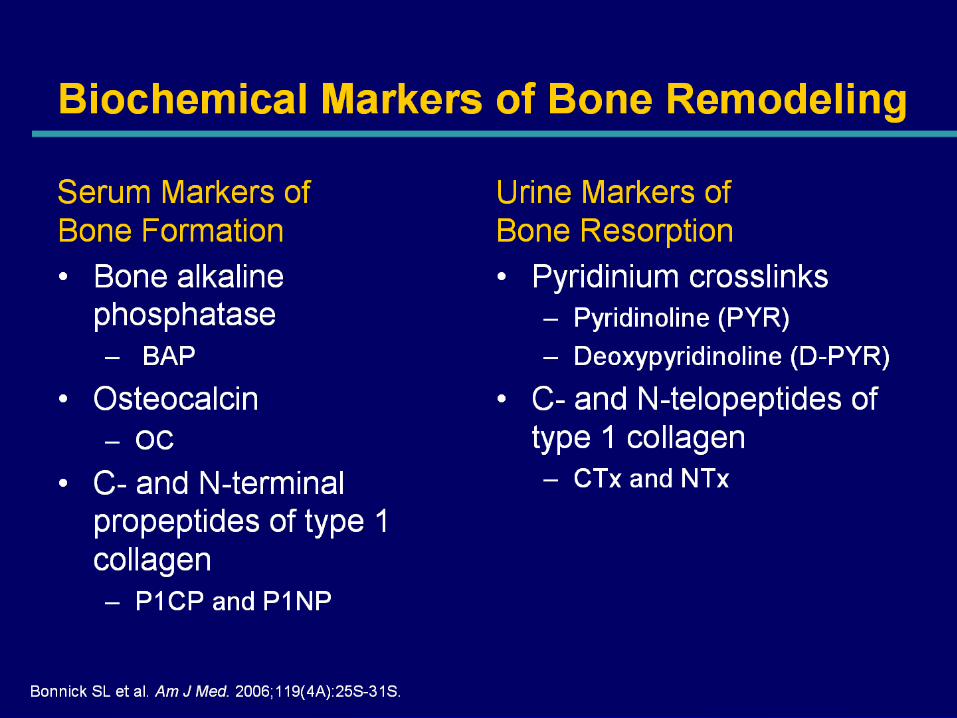
Biochemical Markers of Bone RemodelingBiochemical Markers of Bone Remodeling
Osteoporosis: A Common Problem in Osteoporosis: A Common Problem in the General Populationthe General Population
• In the United States, 10 million individuals are estimated to have osteoporosis
• 8 million are women
• 34 million more are estimated to have low bone mass (osteopenia)
• They have an increased risk for developing osteoporosis
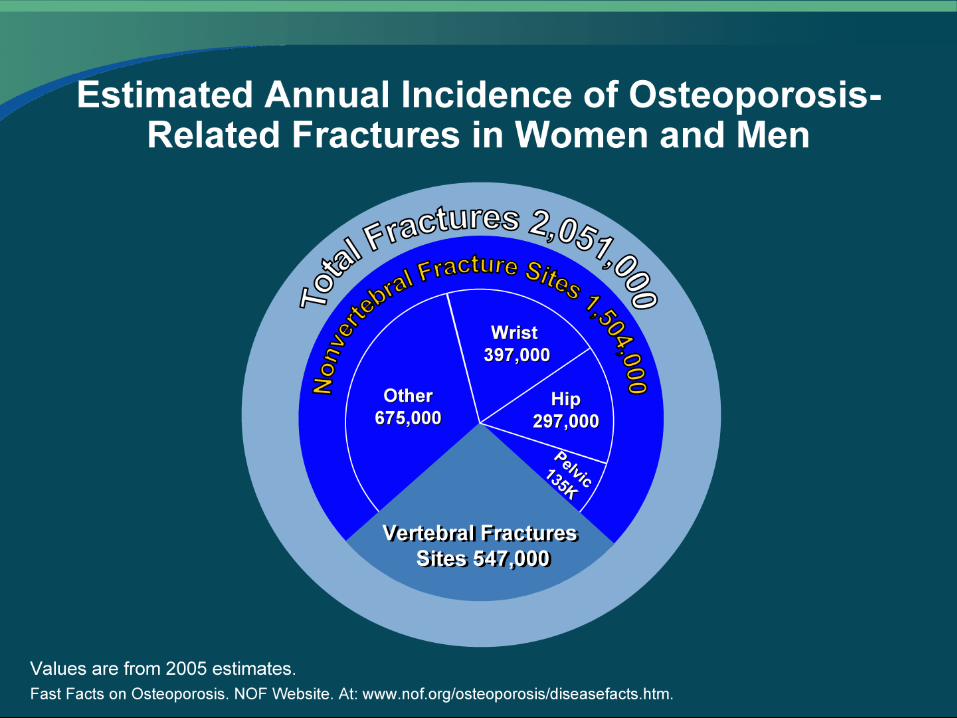
Estimated Annual Incidence of Osteoporosis-Related Fractures in Women and Men

Annual Incidence of Osteoporotic Fractures Higher Than Other Epidemic Annual Incidence of Osteoporotic Fractures Higher Than Other Epidemic DiseasesDiseases

OsteoporosisOsteoporosis
• Fractures• 1 in 2 females over age 50 will fracture• 1 in 4 males over age 50 will fracture

OsteoporosisOsteoporosis
• Fractures• Increased mortality seen after hip and
vertebral fractures• 20% mortality in first year after hip fracture• 25% require long-term nursing home care
after hip fracture• 80,000 male hip fractures annually
(2x mortality with age matched
females)

OsteoporosisOsteoporosis
• Cost
• Each hip fracture costs $40,000 (2001)• Fractures cost $13 billion per year (2005)• Expected costs to exceed $60 billion by
2030
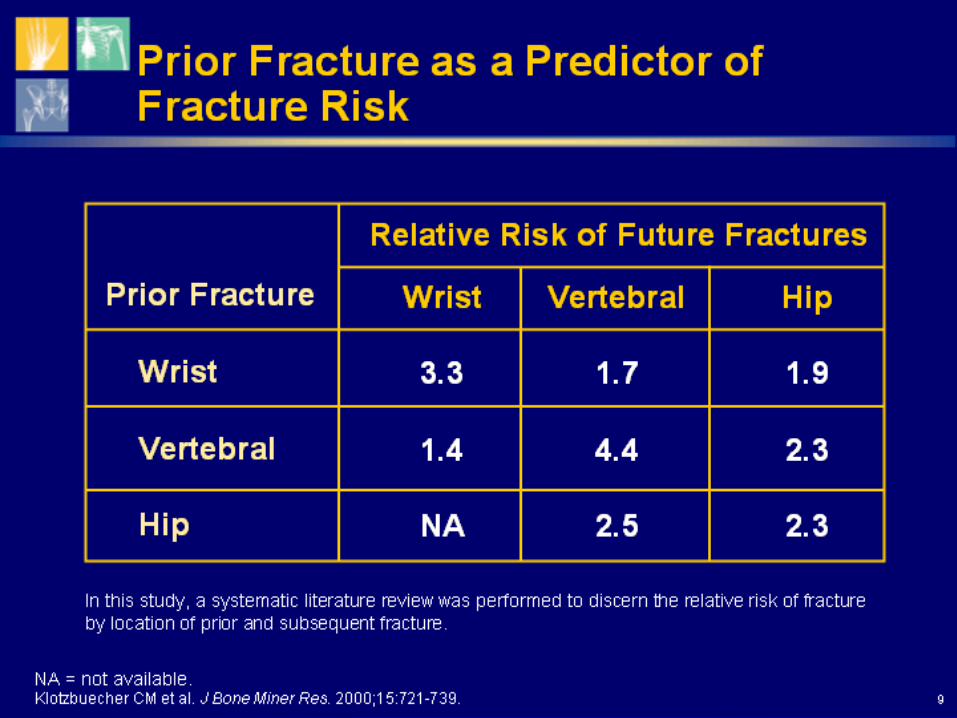
Prior Fracture as a Predictor of Fracture RiskPrior Fracture as a Predictor of Fracture Risk

Risk Factors for Osteoporotic FracturesRisk Factors for Osteoporotic Fractures

Vertebral Fractures Have Significant Consequences for Patients, Including Dorsal Vertebral Fractures Have Significant Consequences for Patients, Including Dorsal KyphosisKyphosis

Hip and Other Non-Vertebral Fractures Have Significant ConsequencesHip and Other Non-Vertebral Fractures Have Significant Consequences

Most Hip Fracture Patients Receive No Pharmacologic Treatment for Most Hip Fracture Patients Receive No Pharmacologic Treatment for OsteoporosisOsteoporosis

Clinical Presentation of OsteoporosisClinical Presentation of Osteoporosis

DXA
• “Gold-standard” for BMD (Bone Mineral Density) measurement
• Measures “central” or “axial” skeletal sites: spine and hip
• May measure other sites: total body and forearm
• Widely available (about 10,000 DXA machines in USA)

WHO Study Group. 1994.
27
Diagnostic Classification
Classification T-score
Normal -1 or greater
Osteopenia Between -1 and -2.5
Osteoporosis -2.5 or less
Severe Osteoporosis-2.5 or less and fragility fracture

Fracture Risk Doubles With Every SD Decrease in
BMD
0
5
10
15
20
25
30
35
-5.0 -4.0 -3.0 -2.0 -1.0 0.0 1.0
Bone Density (T-score)
Relative Risk
for Fracture
Fracture rate
60
50
40
30
20
10
0Fra
ctu
re p
er
100
0 P
ers
on
-Yea
rs
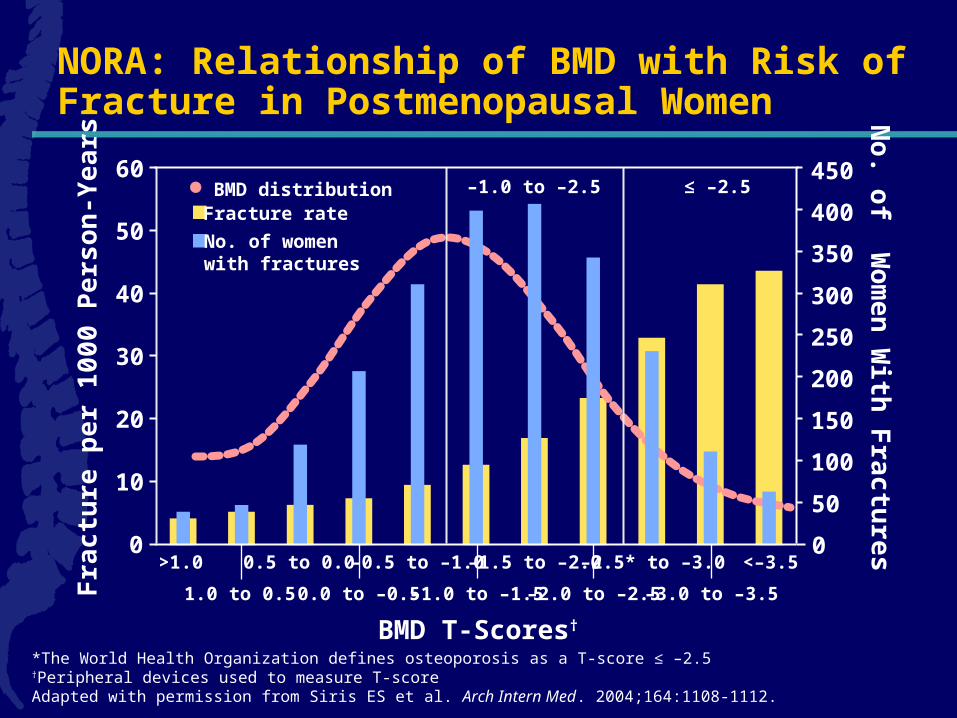
*The World Health Organization defines osteoporosis as a T-score ≤ –2.5 †Peripheral devices used to measure T-scoreAdapted with permission from Siris ES et al. Arch Intern Med. 2004;164:1108-1112.
BMD distribution
BMD T-Scores†
>1.0
1.0 to 0.5
0.5 to 0.0
0.0 to –0.5
–0.5 to –1.0
–1.0 to –1.5
–1.5 to –2.0
–2.0 to –2.5
–2.5* to –3.0
–3.0 to –3.5
<–3.5
No. of women with fractures
450
350
300
250
200
100
0
150
50
400
No
. of W
om
en
With
Fra
ctu
res
NORA: Relationship of BMD with Risk of Fracture in Postmenopausal Women
≤ –2.5–1.0 to –2.5
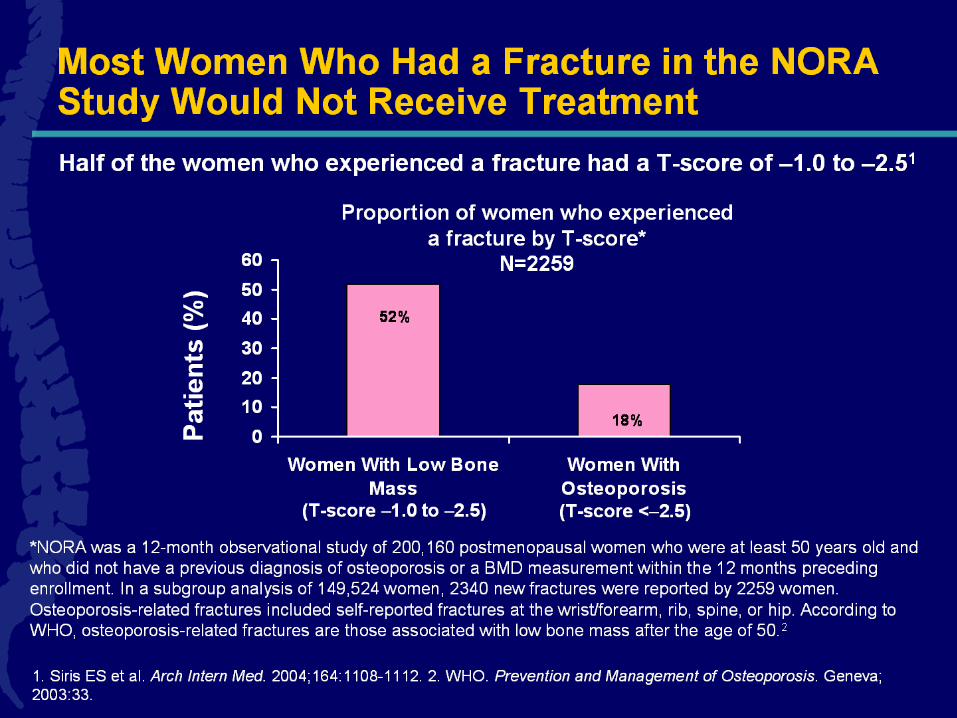
Most Women Who Had a Fracture in the NORA Study Would Not Receive Treatment

Indications For Bone Mineral Density (BMD) Testing
• Women aged 65 and older• Postmenopausal women under age 65 with risk factors• Men aged 70 and older• Adults with a fragility fracture• Adults with a disease or condition associated with low
bone mass or bone loss• Adults taking medications associated with low bone mass
or bone loss• Anyone being considered for pharmacologic therapy• Anyone being treated, to monitor treatment effect
Women discontinuing estrogen should be considered forbone density testing according to the indications listed above

Densitometric Vertebral Fracture Assessment (VFA)
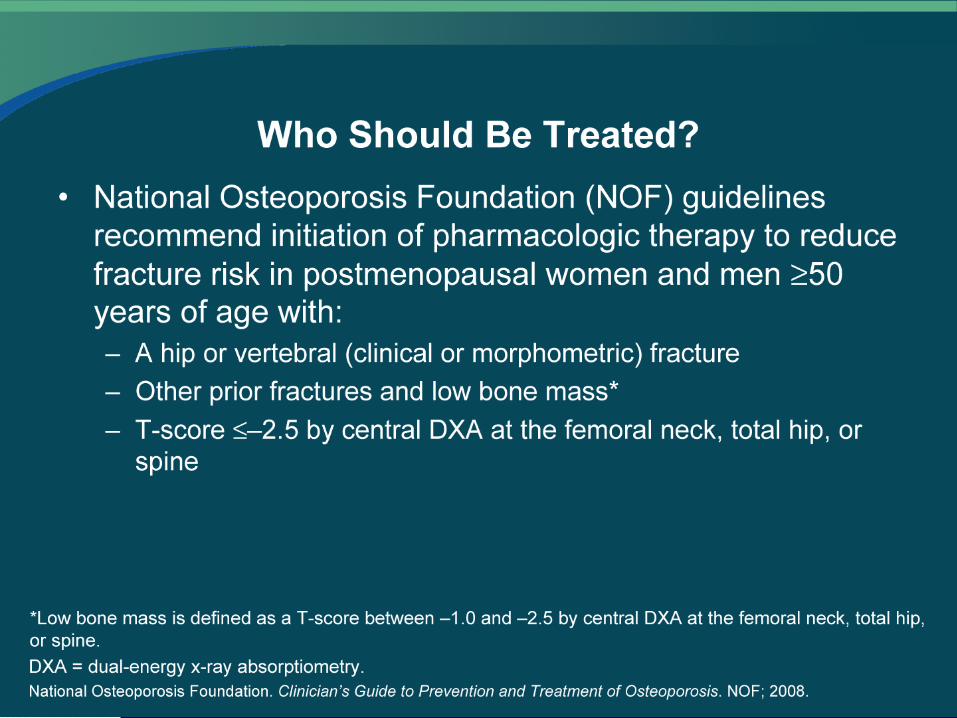
Who Should Be Treated?
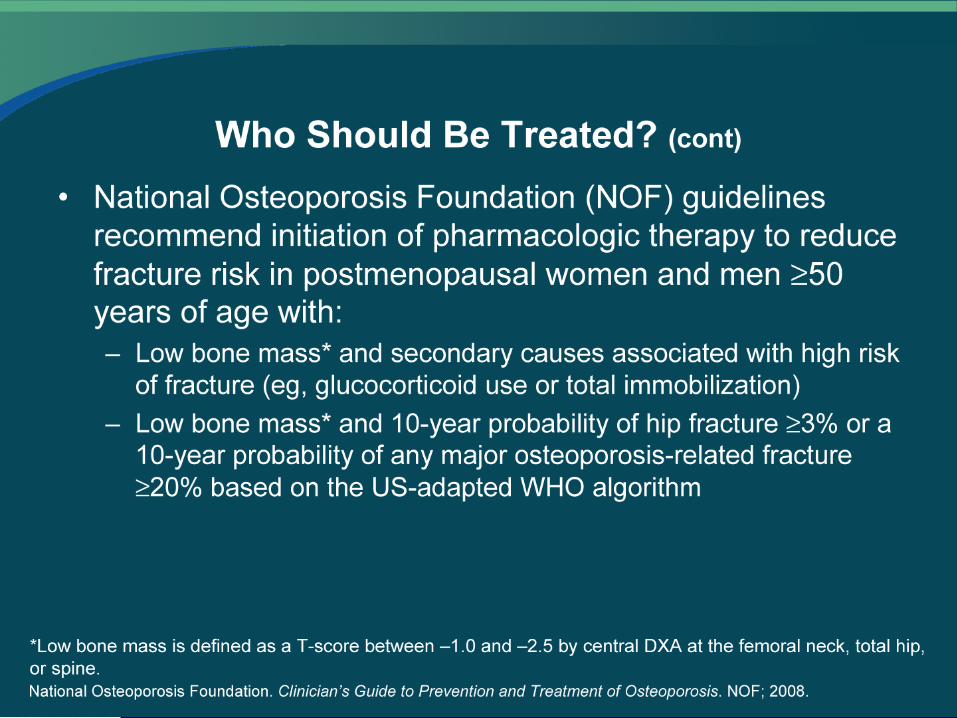
Who Should Be Treated? (cont)

Using the FRAX® Tool to Help Determine Fracture Risk in Treatment-Naïve Using the FRAX® Tool to Help Determine Fracture Risk in Treatment-Naïve Patients With Low Bone MassPatients With Low Bone Mass
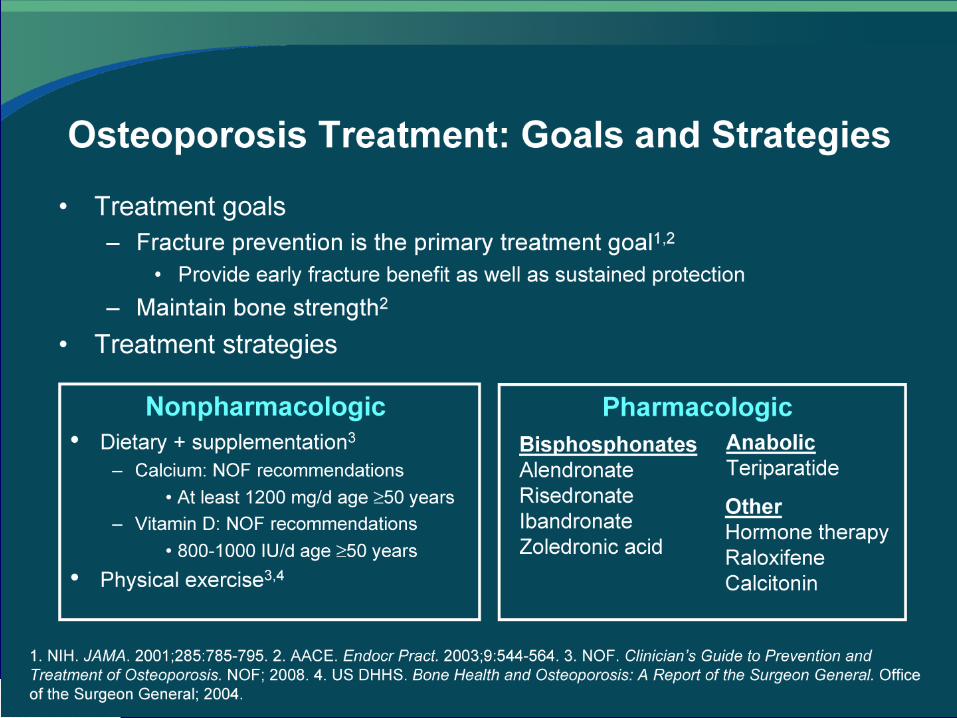
Osteoporosis Treatment: Goals and Strategies

Calcium and Vitamin D Supplementation

Calcium Purchase Habits in Households With Patients on Bisphosphonates
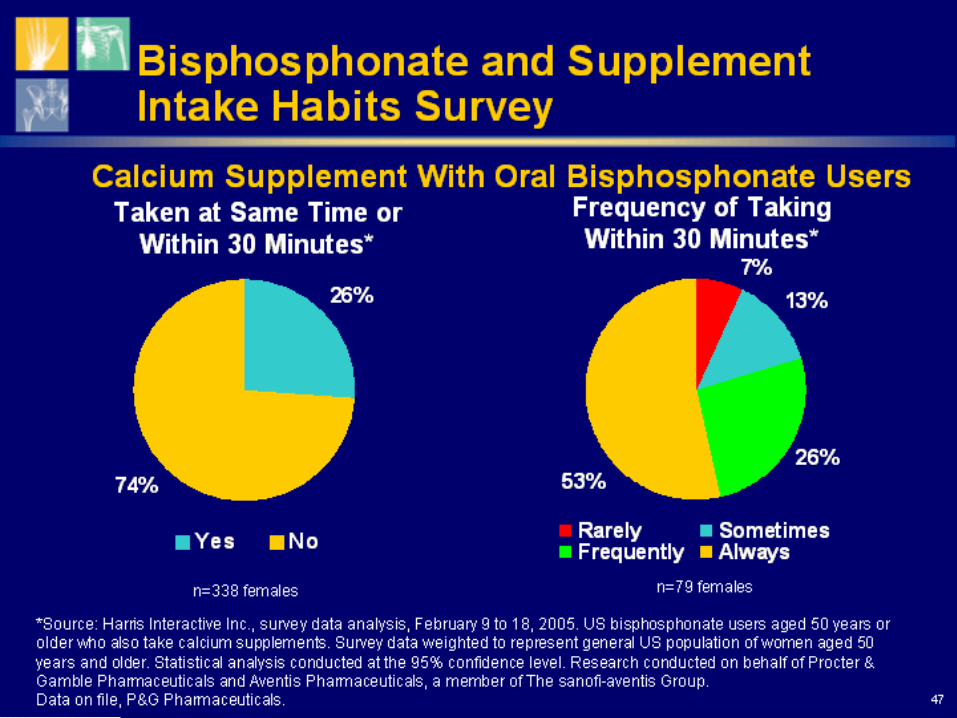
Bisphosphonate and Supplement Intake Habits Survey

Pharmacotherapy

Pharmacotherapy (cont)

OsteoporosisOsteoporosis
• Calcitonin (Miaclacin, Fortical)
• Daily nasal spray • Reduction in vertebral fractures• Short-term analgesic effect

OsteoporosisOsteoporosis
• Raloxifene (Evista)
• Selective estrogen receptor modulator (SERM)
• Reduction in vertebral fractures• Cholesterol reduction• Increased VTE, hot flushes, leg cramps

OsteoporosisOsteoporosis
• Teriparatide (Forteo)
• Anabolic agent (new bone formation)• Daily SQ injection• Reduction in vertebral and non-vertebral
fractures• Increased leg cramps

OsteoporosisOsteoporosis
• Denosumab (Prolia)
• Antibody to RANKL (osteoclast differentiating factor)
• q6 month SQ injection• Reduction in vertebral and non-vertebral
fractures• Increased eczema, cellulitis* & flatulence• Hypocalcemia in CKD
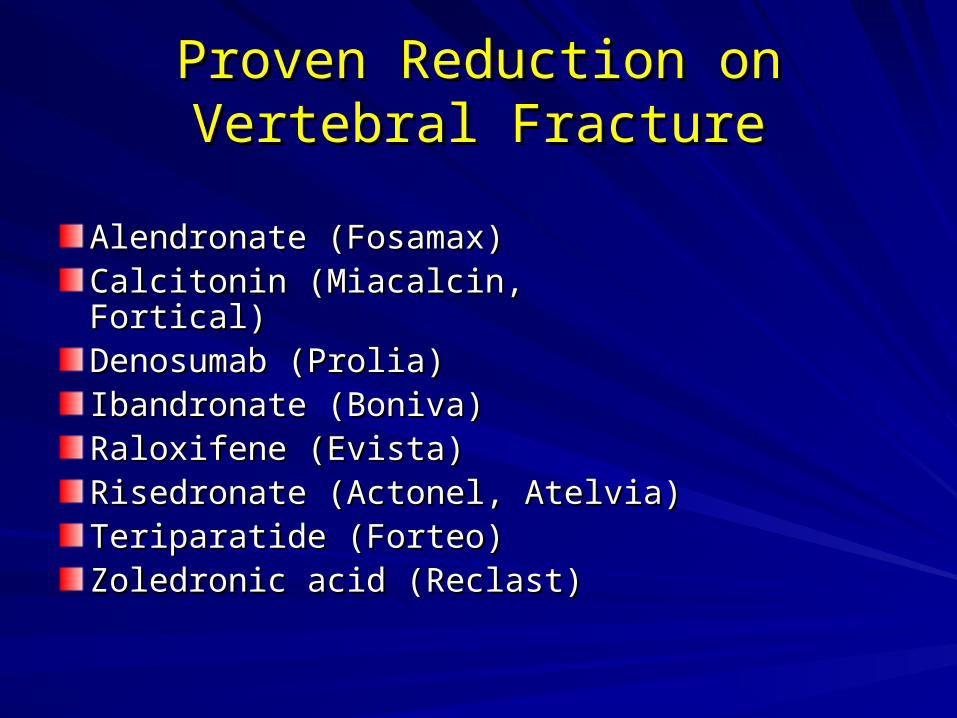
Proven Reduction on Vertebral Proven Reduction on Vertebral FractureFracture
Alendronate (Fosamax)Alendronate (Fosamax)Calcitonin (Miacalcin, Fortical)Calcitonin (Miacalcin, Fortical)Denosumab (Prolia)Denosumab (Prolia)Ibandronate (Boniva)Ibandronate (Boniva)Raloxifene (Evista)Raloxifene (Evista)Risedronate (Actonel, Atelvia)Risedronate (Actonel, Atelvia)Teriparatide (Forteo)Teriparatide (Forteo)Zoledronic acid (Reclast)Zoledronic acid (Reclast)
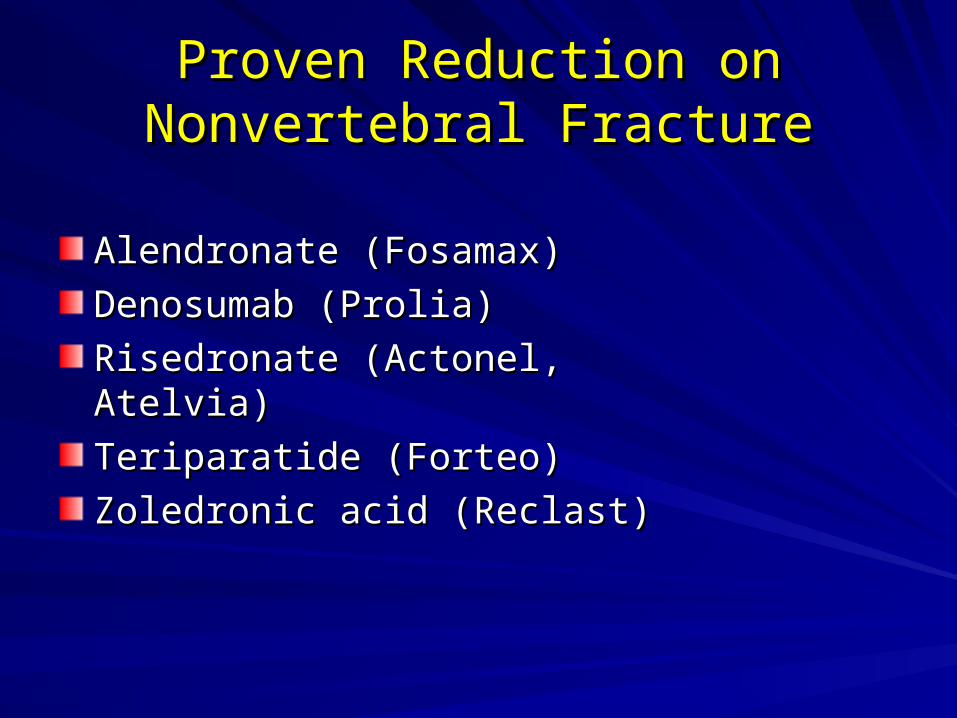
Proven Reduction on Nonvertebral Proven Reduction on Nonvertebral FractureFracture
Alendronate (Fosamax)Alendronate (Fosamax)
Denosumab (Prolia)Denosumab (Prolia)
Risedronate (Actonel, Atelvia)Risedronate (Actonel, Atelvia)
Teriparatide (Forteo)Teriparatide (Forteo)
Zoledronic acid (Reclast)Zoledronic acid (Reclast)


Osteonecrosis of the Jaws (ONJ)Osteonecrosis of the Jaws (ONJ)
• Bone exposure in the mandible, maxilla, or both
• Simulates dental abscesses, “toothaches”, denture sore spots or osteomyelitis

Osteonecrosis of the Jaws (ONJ)Osteonecrosis of the Jaws (ONJ)
• 368 reported cases (5/06)• 94% with intravenous bisphosphonate use
• (multiple myeloma or bone mets)
• 15 cases in patients taking bisphosphonates for osteoporosis
• 20 million users for osteoporosis• Risk is < 1/100,000

AAOMS, ADA & ASBMR AAOMS, ADA & ASBMR RecommendationsRecommendations
• Route dental exams & promotion of good oral hygiene
• Dental exam is not necessary prior to bisphosphonate therapy
• No alteration or delay in planned surgery is necessary
• Discuss benefits/risks of treatment

Safety Topics in the MediaSafety Topics in the Media
• Atrial Fibrillation• No cause and effect relationship
Safety Topics in the MediaSafety Topics in the Media
• Atypical subtrochanteric femur fracture• FDA (3/10): data have not shown a clear
connection with bisphosphonate use• Similar number of these fractures in those
not on bisphosphonates

Safety Topics in the MediaSafety Topics in the MediaTypical femur fractureTypical femur fracture Atypical femur fractureAtypical femur fracture
Associated with fall (95%)Associated with fall (95%) No fallNo fall
No prodromeNo prodrome Prodromal thigh painProdromal thigh pain
30-50% reduction with effective 30-50% reduction with effective bisphosphonatebisphosphonate
Often associated with Often associated with bisphosphonate/steroid usebisphosphonate/steroid use
Located at or above trochanterLocated at or above trochanter Below intertrochanteric lineBelow intertrochanteric line
General unilateralGeneral unilateral Uni or bilateralUni or bilateral
No cortical thickness changeNo cortical thickness change Increased femoral cortical Increased femoral cortical thicknessthickness
Generally spiral Generally spiral Transverse with medial spikeTransverse with medial spike

Safety Topics in the MediaSafety Topics in the Media
• Esophageal Cancer• 2 large studies in the UK with conflicting
results• FDA has not concluded that taking an oral
bisphosphonate increases the risk of esophageal cancer
• Would avoid bisphosphonates in patients with Barrett’s esophagus
Drug Holiday: FDADrug Holiday: FDA“ In light of all the risk-benefit challenges with the
bisphosphonate class, these data suggest that bisphosphonate therapy could be safely discontinued from an efficacy standpoint. However, additional long-term data would be needed to further define an appropriate duration of drug cessation and to determine if interim monitoring is appropriate on an individual basis.”
“There are no substantial data available to inform decision regarding the initiation or duration of a drug holiday.”
FDA Advisory Committee (9/9/11)