Osteoporosis Management in Younger Premenopausal...
65
Osteoporosis Management in Younger Premenopausal Women: Challenging Cases Adi Cohen, MD, MHS Associate Professor or Medicine at Columbia University Medical Center
Transcript of Osteoporosis Management in Younger Premenopausal...

Osteoporosis Management in Younger Premenopausal
Women: Challenging Cases
Adi Cohen, MD, MHSAssociate Professor or Medicine at Columbia University Medical Center

Disclosures
Industry support for research from:
•Amgen• Eli Lilly & Company

Diagnosis based on fractures and low BMD:4.1 cases per 100,000 person‐yrs1
Fracture incidence is much lower in premenopausal women.
The incidence of distal radius fractures in menand women per 10,000 population per year and 95%confidence limits for Dorset residents2.
1. Khosla et al, Bone 19942. Thompson et al, Injury 2004
Premenopausal Osteoporosis is RARE
Diagnostic Criteria for Osteoporosis in PREmenopausal women
1. The diagnosis of “osteoporosis” is most secure in the context of low trauma fracture.
2. Osteoporosis cannot be diagnosed based on BMD alone.
International Society for Clinical Densitometry, Official Positions, 2015International Osteoporosis Foundation Committee of Scientific Advisors Working Group, 2012
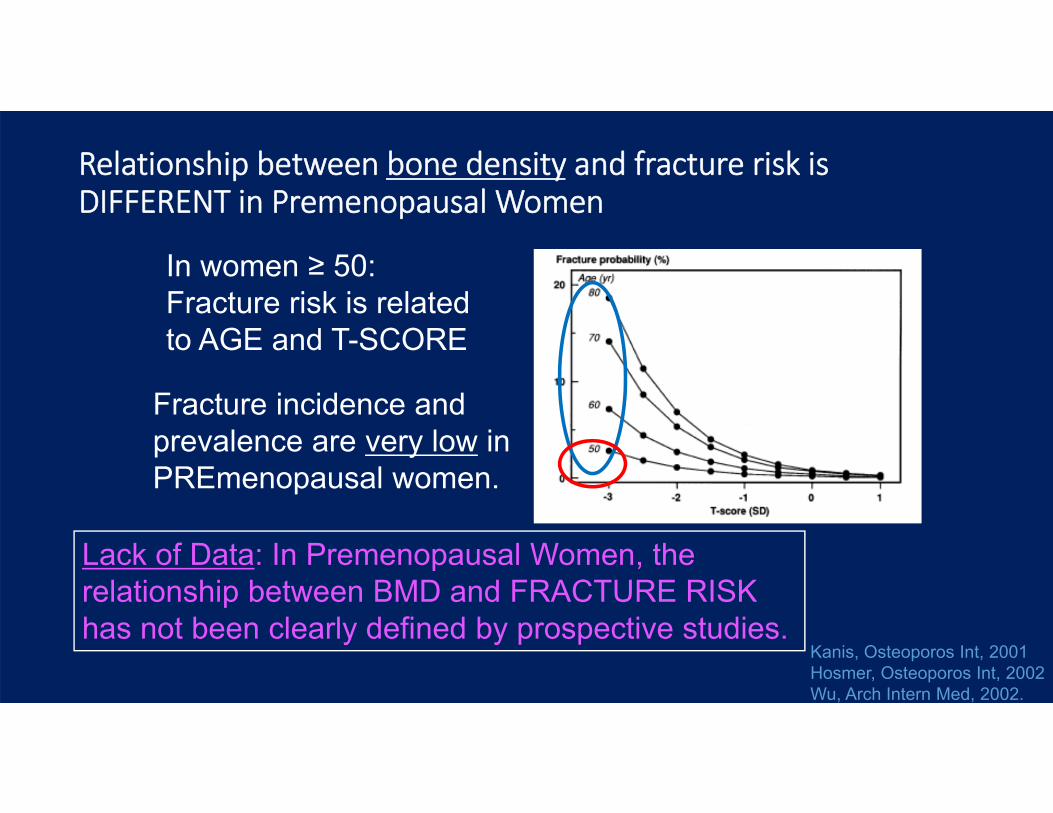
Relationship between bone density and fracture risk is DIFFERENT in Premenopausal Women
Kanis, Osteoporos Int, 2001 Hosmer, Osteoporos Int, 2002 Wu, Arch Intern Med, 2002.
In women ≥ 50: Fracture risk is related to AGE and T-SCORE
Fracture incidence and prevalence are very low in PREmenopausal women.
Lack of Data: In Premenopausal Women, the relationship between BMD and FRACTURE RISK has not been clearly defined by prospective studies.
Diagnostic Criteria for Osteoporosis in PREmenopausal women
1. The diagnosis of “osteoporosis” is most secure in the context of low trauma fracture.
2. Osteoporosis cannot be diagnosed based on BMD alone.
3. Screening BMD is not recommended• BMD measurement is indicated for those with fracture(s) or a
known secondary cause of bone loss.
International Society for Clinical Densitometry, Official Positions, 2015International Osteoporosis Foundation Committee of Scientific Advisors Working Group, 2012

Diagnostic Criteria for Osteoporosis in PREmenopausal women
4. Because of a lack of prospective data, DXA BMD (alone or as part of FRAX) cannot be used to:• Predict fracture risk• Make treatment decisions
5. Thus, to avoid the diagnostic and treatment implications of the T score, ISCD recommends reporting Z scores.
International Society for Clinical Densitometry, Official Positions, 2015International Osteoporosis Foundation Committee of Scientific Advisors Working Group, 2012
TERMINOLOGY –ISCD Recommendations
“Osteoporosis”‐ Applies only to those with
‐ Low trauma fracture‐ Secondary cause of bone loss
“Osteopenia”‐ Should not be used to describe BMD in premenopausal women
Exceptions• ISCD: T scores should be used for
perimenopausal women.
• IOF: Osteoporosis can be defined based on T score ≤ -2.5 in adult women with a known, ongoing secondary cause of bone loss or fragility.
International Society for Clinical Densitometry, Official Positions, 2015International Osteoporosis Foundation Committee of Scientific Advisors Working Group, 2012

Cases
• 30 yo woman slips off of a window seat and sustains a fracture of her left greater trochanter
• Fracture site biopsied to r/o cancer• No evidence of cancer on the biopsy
• DXA Z scores below expected range for age:• Spine ‐2.5• Total Hip ‐2.8• Femoral Neck ‐3.1
• Referred to our clinic for evaluation
Case #1
• 39 yo healthy premenopausal woman has a screening bone density because her mother has a history of osteoporosis with bilateral hip fractures.
• DXA Z scores are below expected range for age:• Spine ‐2.5
• Total Hip ‐2.3
• Femoral Neck ‐2.4
• Referred to our clinic for evaluation
Case #2
Which patient needs further evaluation?
• Case #1: Low trauma fracture + Very low BMD
• Case #2: Very low BMD, no fracture history

Evaluation for Secondary Causes
• Detailed history• Physical Examination• Laboratory Evaluation
Most premenopausal women with low BMD orlow‐trauma fracture have an underlying disorder or medication exposure
These SECONDARY CAUSES may:- Interfere with peak BMD acquisition
- or -- Cause excessive bone loss thereafter
How often can a secondary cause be found?
• In a population‐based study → 90% found to have 2o causes
• Khosla et al, 1994
• In series from tertiary referral populations →
44‐53% found to have 2o causes• Kulak et al, 2000, Peris et al, 2003, Cohen et al, 2006
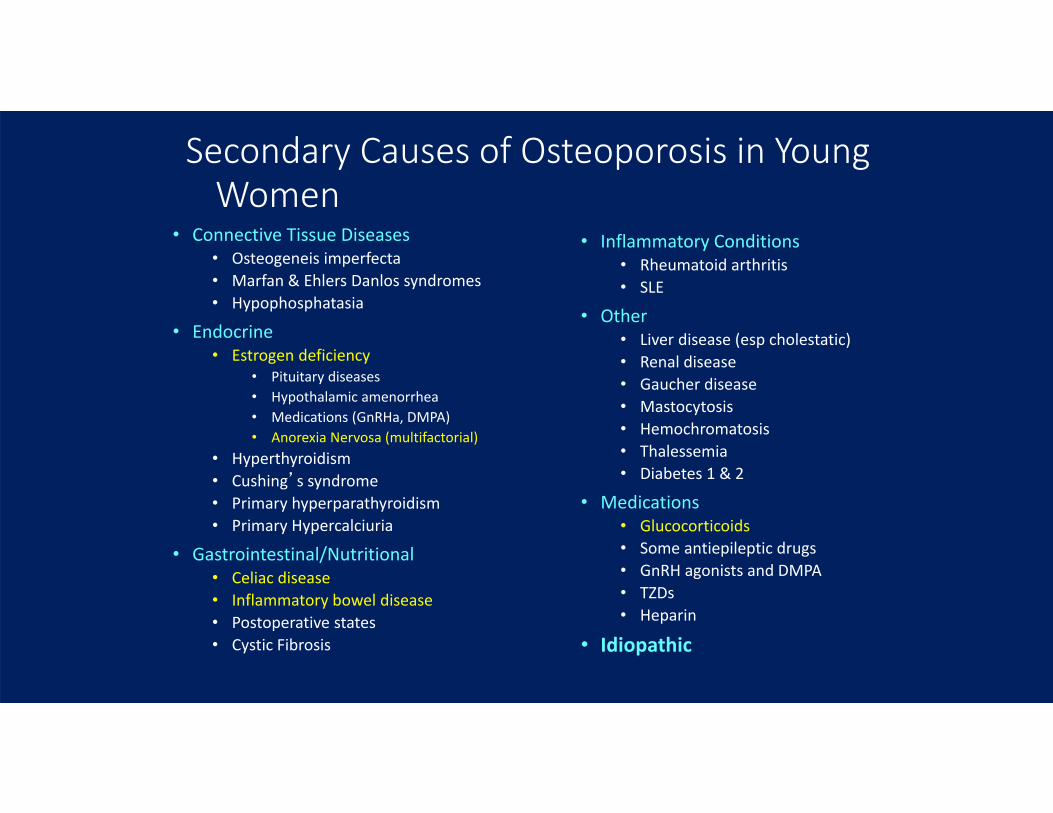
Secondary Causes of Osteoporosis in Young Women
• Connective Tissue Diseases• Osteogeneis imperfecta• Marfan & Ehlers Danlos syndromes• Hypophosphatasia
• Endocrine• Estrogen deficiency
• Pituitary diseases• Hypothalamic amenorrhea• Medications (GnRHa, DMPA)• Anorexia Nervosa (multifactorial)
• Hyperthyroidism• Cushing’s syndrome• Primary hyperparathyroidism• Primary Hypercalciuria
• Gastrointestinal/Nutritional• Celiac disease• Inflammatory bowel disease• Postoperative states• Cystic Fibrosis
• Inflammatory Conditions• Rheumatoid arthritis• SLE
• Other• Liver disease (esp cholestatic)• Renal disease• Gaucher disease• Mastocytosis• Hemochromatosis• Thalessemia• Diabetes 1 & 2
• Medications• Glucocorticoids• Some antiepileptic drugs• GnRH agonists and DMPA• TZDs• Heparin
• Idiopathic
• No significant medical history• Normal menarche (ages 15, 12)• No history of amenorrhea • Healthy diet, 2 servings dairy/day• Physically active• No medications• No tobacco• No excess ETOH• + FH osteoporosis
• 1: maternal aunt & grandmother• 2: mother and maternal grandmother
History – Case #1 and Case #2
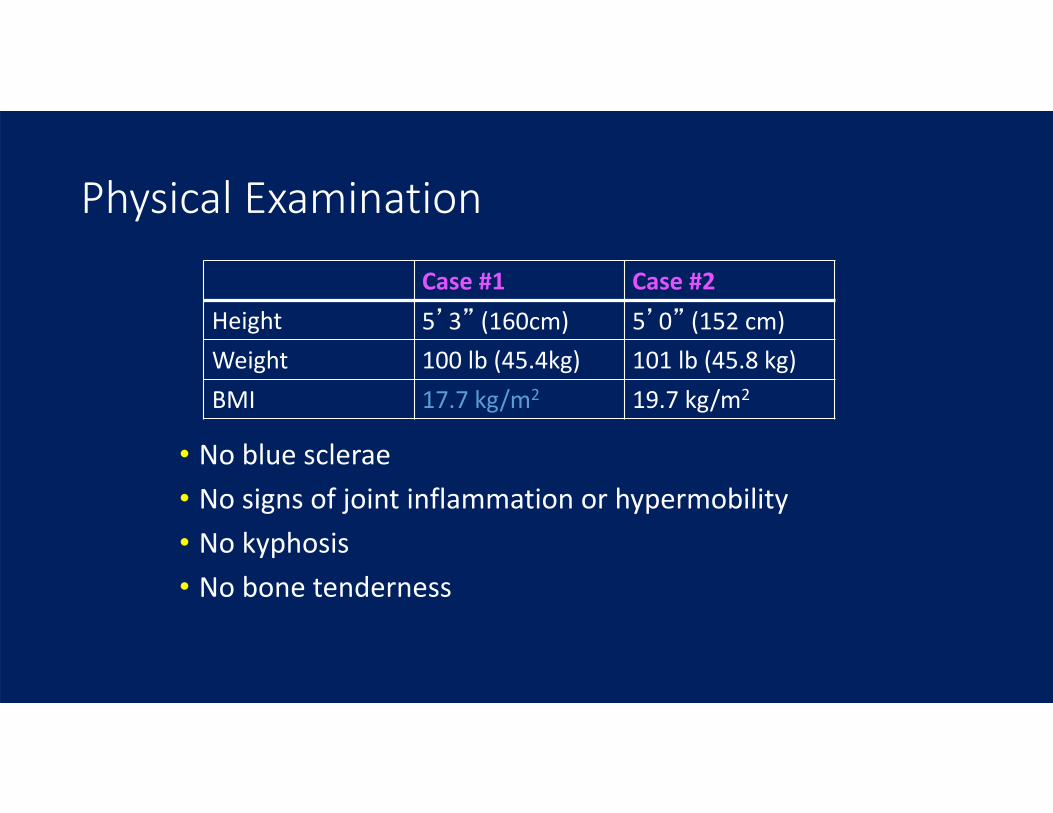
• No blue sclerae• No signs of joint inflammation or hypermobility• No kyphosis• No bone tenderness
Case #1 Case #2Height 5’3” (160cm) 5’0” (152 cm)Weight 100 lb (45.4kg) 101 lb (45.8 kg)BMI 17.7 kg/m2 19.7 kg/m2
Physical Examination
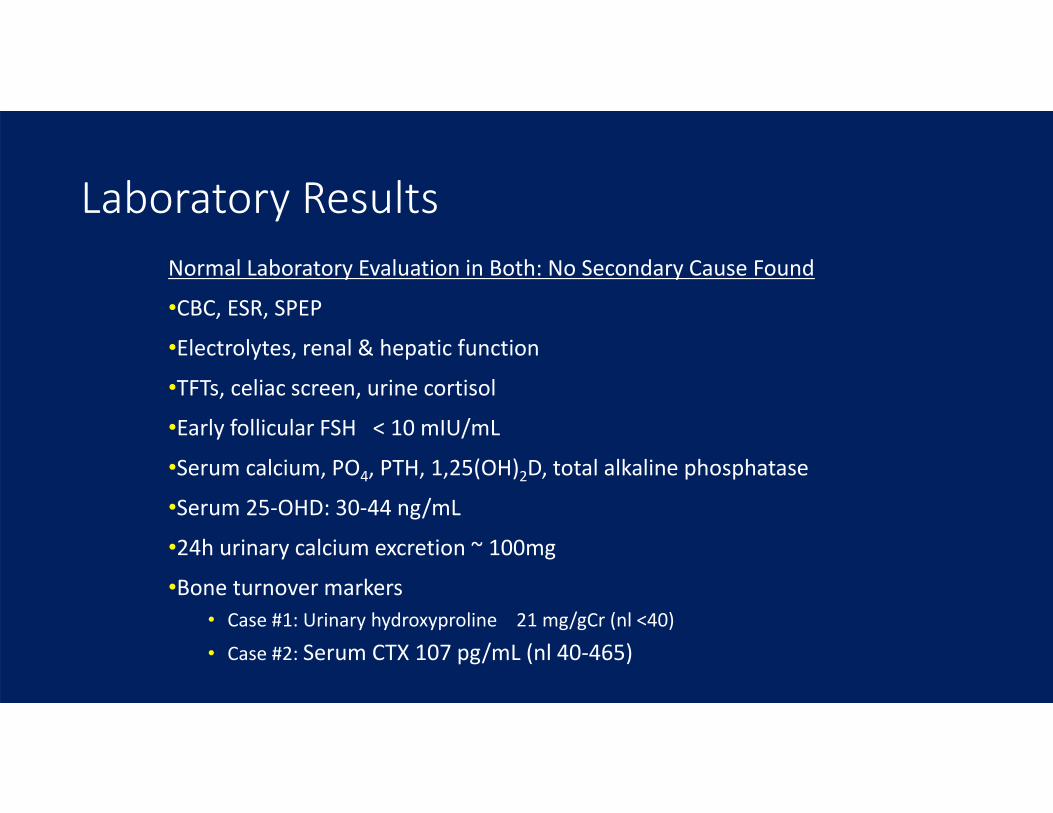
Normal Laboratory Evaluation in Both: No Secondary Cause Found
•CBC, ESR, SPEP•Electrolytes, renal & hepatic function•TFTs, celiac screen, urine cortisol•Early follicular FSH < 10 mIU/mL
•Serum calcium, PO4, PTH, 1,25(OH)2D, total alkaline phosphatase
•Serum 25‐OHD: 30‐44 ng/mL
•24h urinary calcium excretion ~ 100mg
•Bone turnover markers• Case #1: Urinary hydroxyproline 21 mg/gCr (nl <40)
• Case #2: Serum CTX 107 pg/mL (nl 40‐465)
Laboratory Results

Does Case #2 Have Osteoporosis?
Case #1: Idiopathic Osteoporosis• Low BMD Z ‐3.1• Clear clinical evidence of bone fragility
Case #2: Idiopathic Low BMD•Low BMD Z ‐2.5•No clinical evidence of bone fragility•No prospective data in premenopausal women:
• Cannot predict her Fx risk based on DXA alone
Can 3D imaging techniques define a microstructural defect in either or both cases?
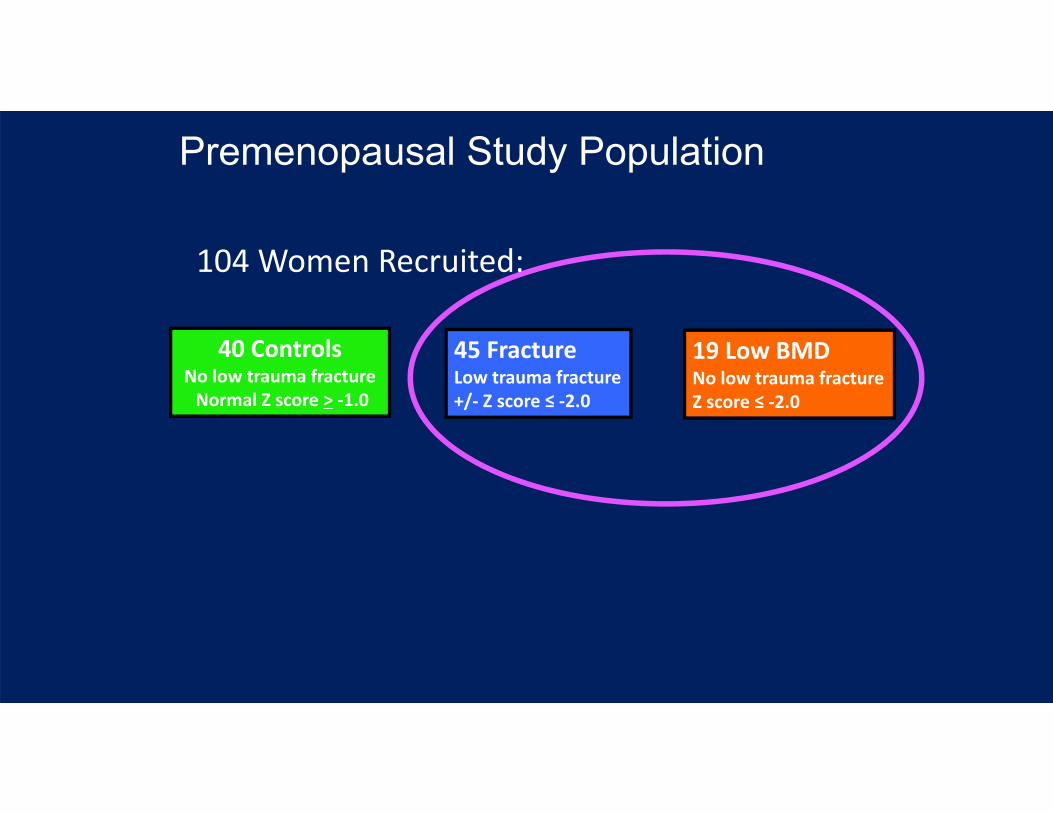
Premenopausal Study Population
45 FractureLow trauma fracture+/‐ Z score ≤ ‐2.0
19 Low BMDNo low trauma fractureZ score ≤ ‐2.0
40 ControlsNo low trauma fractureNormal Z score > ‐1.0
104 Women Recruited:
Bone Micro-architectural Defects
Cohen, Shane et al, JCEM 2009Cohen, Shane et al, JCEM 2011Cohen, Shane et al, JCEM 2012
Bone Structure Studies: Central QCT of the spine and hipPeripheral HRQCT of the radius and tibiaTransiliac bone biopsies ‐ obtained in all
Cortex:Density, ThicknessTrabecular Bone:3D Bone VolumeTb Number Tb Separation
45 FractureLow trauma fracture+/‐ Z score ≤ ‐2.0
19 Low BMDNo low trauma fractureZ score ≤ ‐2.0
40 ControlsNo low trauma fractureNormal Z score > ‐1.0
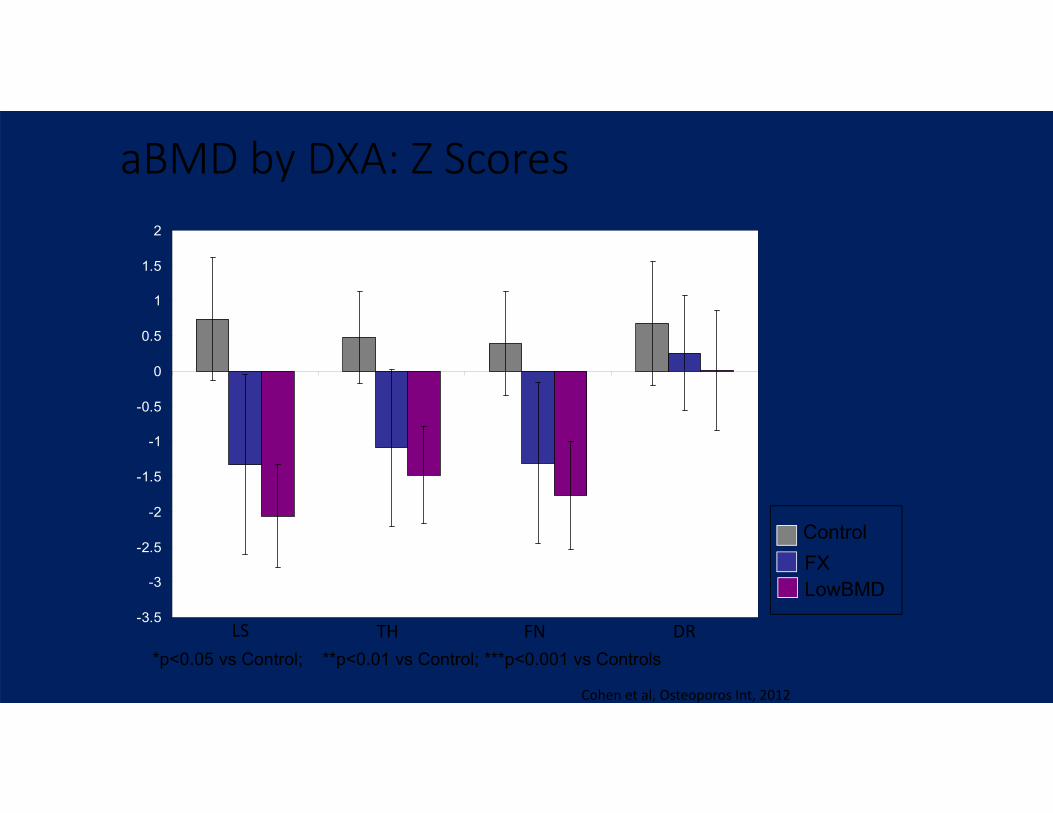
aBMD by DXA: Z Scores
ControlFXLowBMD
*p<0.05 vs Control; **p<0.01 vs Control; ***p<0.001 vs Controls
*
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
1.5
2
************
******
p<0.05
LS TH FN DR
***
Cohen et al, Osteoporos Int, 2012
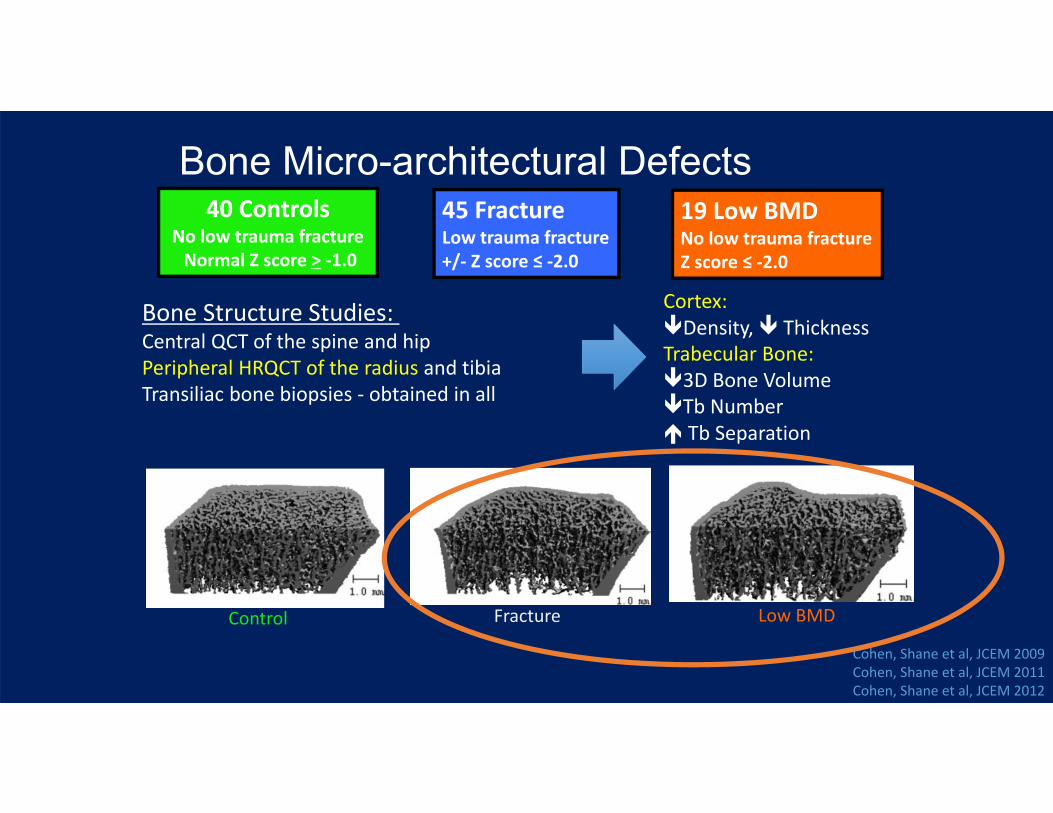
Bone Micro-architectural Defects
Bone Structure Studies: Central QCT of the spine and hipPeripheral HRQCT of the radius and tibiaTransiliac bone biopsies ‐ obtained in all
Cortex:Density, ThicknessTrabecular Bone:3D Bone VolumeTb Number Tb Separation
Control Fracture Low BMD
45 FractureLow trauma fracture+/‐ Z score ≤ ‐2.0
19 Low BMDNo low trauma fractureZ score ≤ ‐2.0
40 ControlsNo low trauma fractureNormal Z score > ‐1.0
Cohen, Shane et al, JCEM 2009Cohen, Shane et al, JCEM 2011Cohen, Shane et al, JCEM 2012
Bone Micro-architectural Defects
Bone Structure Studies: Central QCT of the spine and hipPeripheral HRQCT of the radius and tibiaTransiliac bone biopsies ‐ obtained in all
Cortex:Density, ThicknessTrabecular Bone:3D Bone VolumeTb Number Tb Separation
45 FractureLow trauma fracture+/‐ Z score ≤ ‐2.0
19 Low BMDNo low trauma fractureZ score ≤ ‐2.0
40 ControlsNo low trauma fractureNormal Z score > ‐1.0
Control Fracture Low BMD
Cohen, Shane et al, JCEM 2009Cohen, Shane et al, JCEM 2011Cohen, Shane et al, JCEM 2012

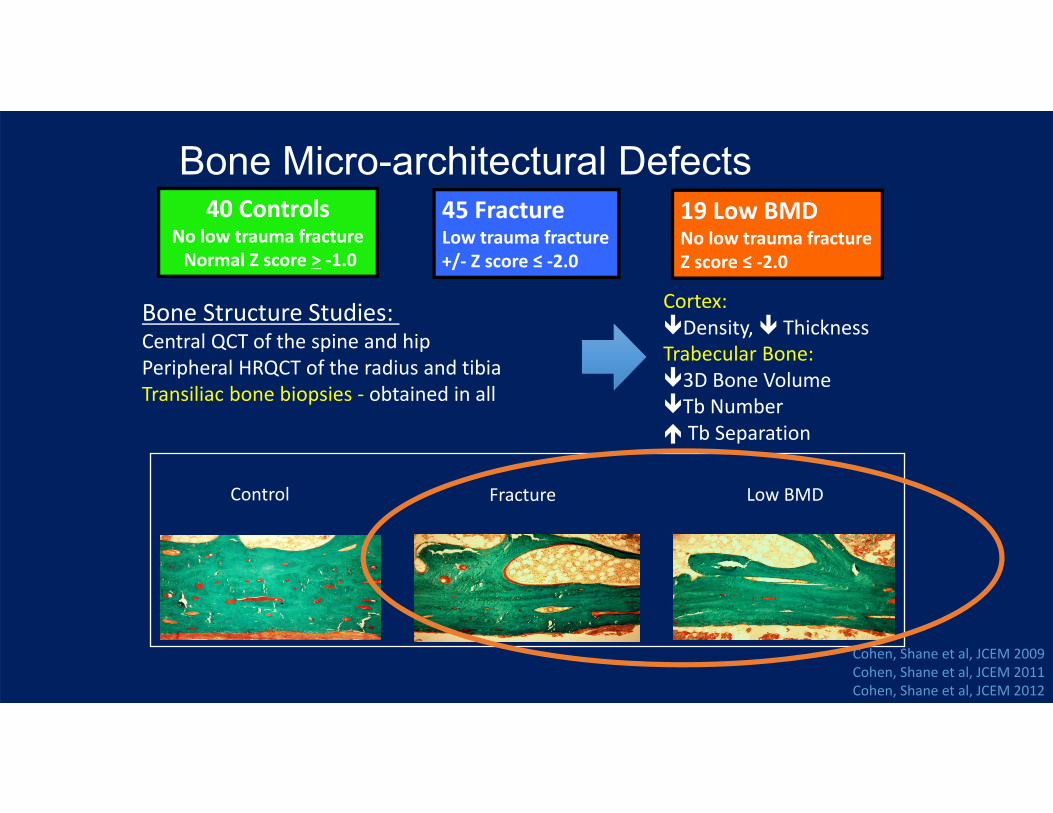
Bone Micro-architectural Defects
Bone Structure Studies: Central QCT of the spine and hipPeripheral HRQCT of the radius and tibiaTransiliac bone biopsies ‐ obtained in all
Cortex:Density, ThicknessTrabecular Bone:3D Bone VolumeTb Number Tb Separation
Control Fracture Low BMD
45 FractureLow trauma fracture+/‐ Z score ≤ ‐2.0
19 Low BMDNo low trauma fractureZ score ≤ ‐2.0
40 ControlsNo low trauma fractureNormal Z score > ‐1.0
Cohen, Shane et al, JCEM 2009Cohen, Shane et al, JCEM 2011Cohen, Shane et al, JCEM 2012

Summary: Case #1 and Case #2• Low trauma fractures (or low BMD) in premenopausal women should lead to an evaluation for secondary causes
• In some cases, no secondary cause can be found:• Idiopathic Osteoporosis (with fractures: IOP)• Idiopathic Low BMD (ILBMD)
• Bone structure deficits can be found in both cases
• Treatment recommendations DIFFER (opinion):• ILBMD: Treatment is rarely indicated for those with isolated low BMD since fracture risk is unknown
• Optimize bone health with nonpharmacologic lifestyle measures (Peris, Clin Rheumatol, 2007)
• IOP: Medical treatment can be considered on a case by case basis for young women with documented bone fragility, even in the absence of a known cause
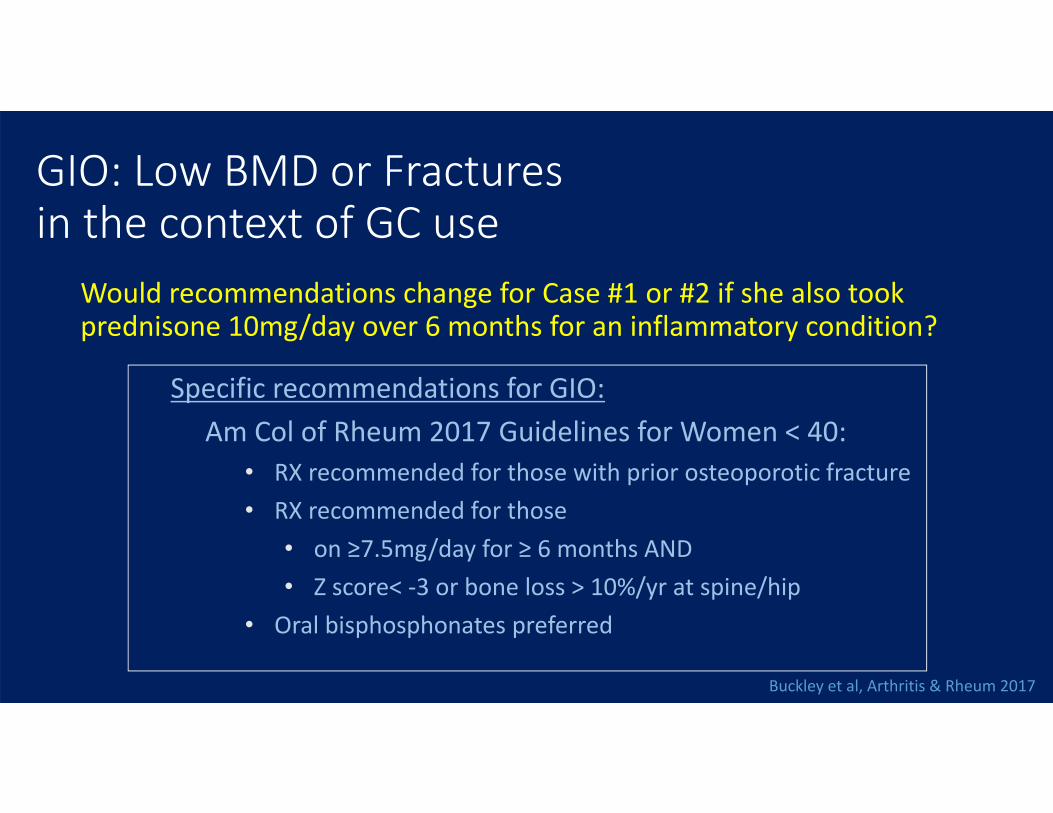
GIO: Low BMD or Fractures in the context of GC use
Would recommendations change for Case #1 or #2 if she also took prednisone 10mg/day over 6 months for an inflammatory condition?
Specific recommendations for GIO:Am Col of Rheum 2017 Guidelines for Women < 40:
• RX recommended for those with prior osteoporotic fracture• RX recommended for those
• on ≥7.5mg/day for ≥ 6 months AND • Z score< ‐3 or bone loss > 10%/yr at spine/hip
• Oral bisphosphonates preferred
Buckley et al, Arthritis & Rheum 2017
Treatment Options for Osteoporosis in Premenopausal Women
• Anti‐resorptive agents: • Estrogen• Bisphosphonates • SERMS (eg Raloxifene)• Denosumab
• Anabolic agents: • Teriparatide• Abaloparatide
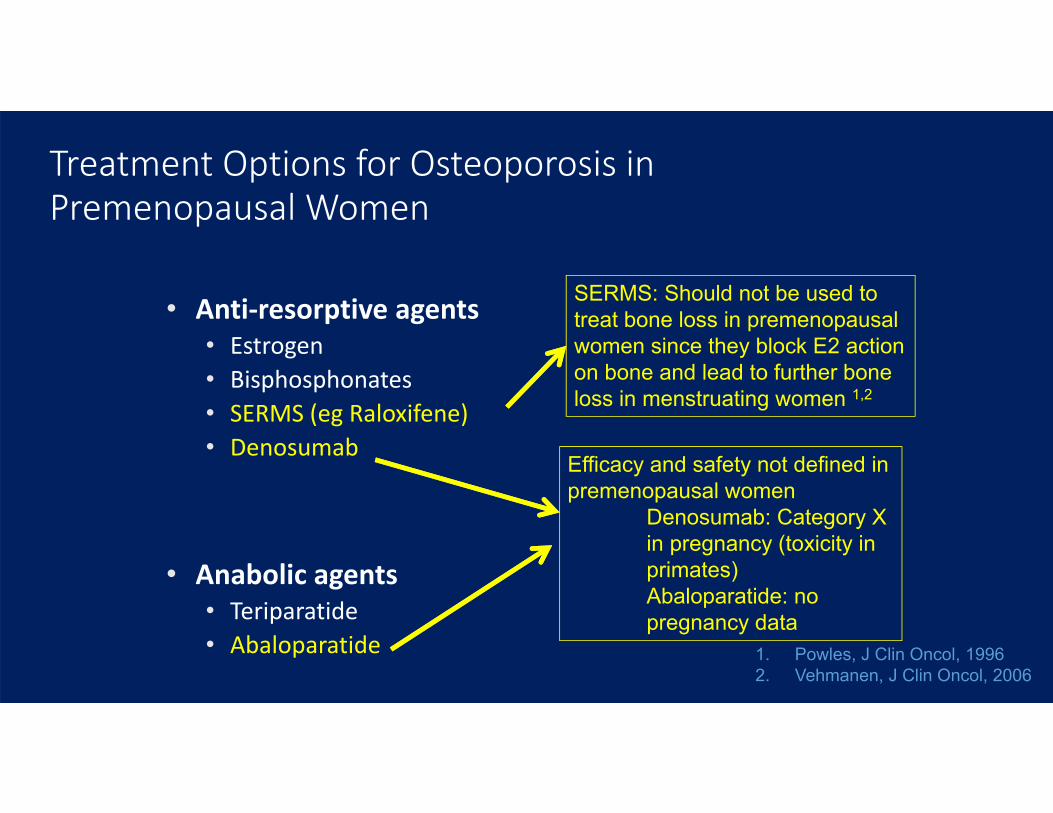
• Anti‐resorptive agents• Estrogen• Bisphosphonates • SERMS (eg Raloxifene)• Denosumab
• Anabolic agents• Teriparatide• Abaloparatide 1. Powles, J Clin Oncol, 1996
2. Vehmanen, J Clin Oncol, 2006
SERMS: Should not be used to treat bone loss in premenopausal women since they block E2 action on bone and lead to further bone loss in menstruating women 1,2
Efficacy and safety not defined in premenopausal women
Denosumab: Category X in pregnancy (toxicity in primates)Abaloparatide: no pregnancy data
Treatment Options for Osteoporosis in Premenopausal Women

Bisphosphonates:Short term BMD improvement in premenopausal women with•Lupus and other AI diseases•Pregnancy associated osteoporosis•GC exposure
Some are FDA approved for use in premenop women on GC•Alendronate, risedronate
Treatment not indicated in all:No fracture dataLong term risks are unknown
Nzeusseu Toukap Lupus 2005, Nakayamada J Rheumatol 2004, O’Sullivan OI 2006, Saag NEJM 1998, Wallach CTI 2000, Buckley Arth and Rheum 2017
Treatment Options for Osteoporosis in Premenopausal Women

• Anti‐resorptive agents: • Estrogen• Bisphosphonates • SERMS (eg Raloxifene)• Denosumab
• Anabolic agents: • Teriparatide
Treatment Options for Osteoporosis in Premenopausal Women
Parathyroid Hormone for Premenopausal Women
• Amenorrheic premenopausal women on GnRH agonists for endometriosis1: Prevents bone loss.
• Young women on GCs2: Increases BMD significantly more than alendronate.
• Premenopausal women with idiopathic osteoporosis3: Improves BMD/structure
• Anorexia nervosa: Improves BMD4
• Pregnancy associated osteoporosis: Improves BMD5,6
1. Finkelstein et al, JAMA 19982. Langdahl et al, Osteoporos Int 20093. Cohen et al, JCEM 20134. Fazeli et al, JCEM 20145. Choe et al, JBMM 20126. Hong et al, Cin Endoc 2018
Parathyroid Hormone for Premenopausal Women
•
•
•
••
Teriparatide for Premenopausal Women:Special Considerations
• Only approved in the setting of GIO.• Black Box Warning* re osteosarcoma risk:
• Documentation of fused epiphyses in young women < 25 yrs.
• Treatment plan post‐TPTD is unclear
“….It is not known if people who take FORTEO have a higher chance of getting osteosarcoma. Before you take FORTEO, you should tell your healthcare provider if you have Paget's disease of bone, are a child or young adult whose bones are still growing, or have had radiation therapy.”
*Document fused epiphyses in very young patients

Teriparatide for Premenopausal IOP/ILBMDA Pilot Open‐Label Treatment Study
• Investigator Initiated• Funded by Eli Lilly
21Premenopausal women with IOP
Teriparatide 20 µg SC daily
24 months
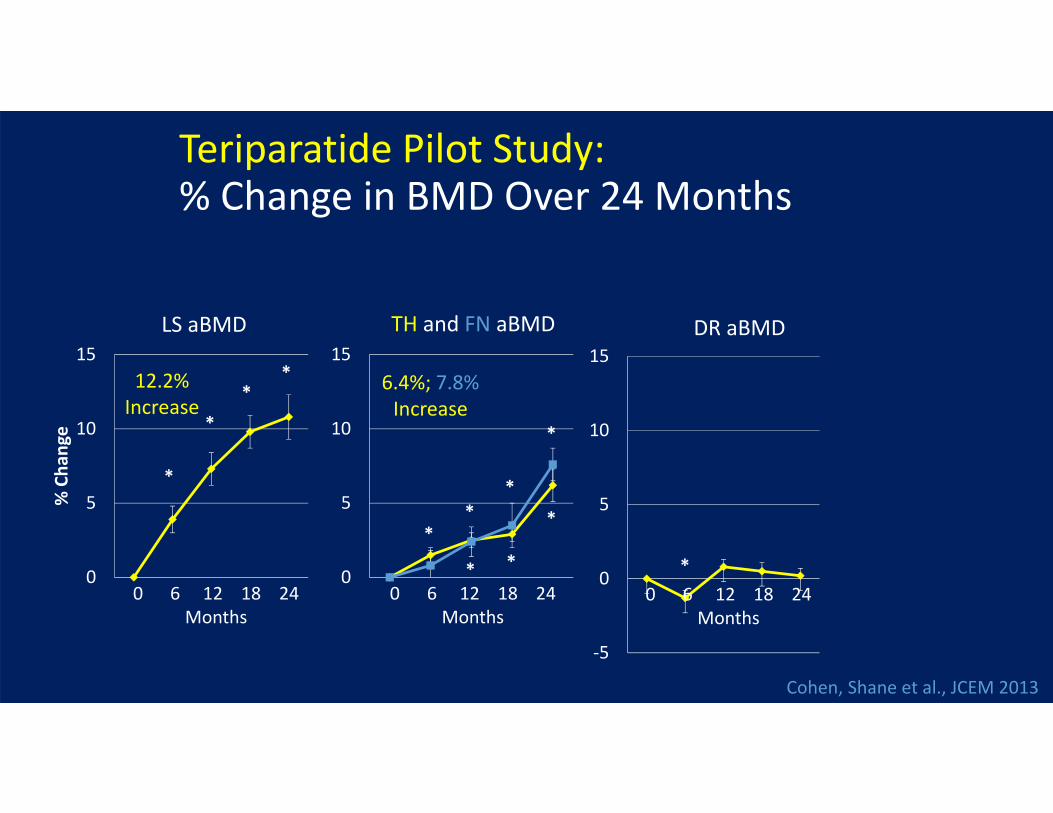
Teriparatide Pilot Study: % Change in BMD Over 24 Months
Cohen, Shane et al., JCEM 2013
0
5
10
15
% Cha
nge
LS aBMD
0
5
10
15TH and FN aBMD
‐5
0
5
10
15DR aBMD
**
*
*
**
*
*
*
0 6 12 18 24Months
0 6 12 18 24Months
0 6 12 18 24Months
*
**
12.2%Increase
6.4%; 7.8%Increase
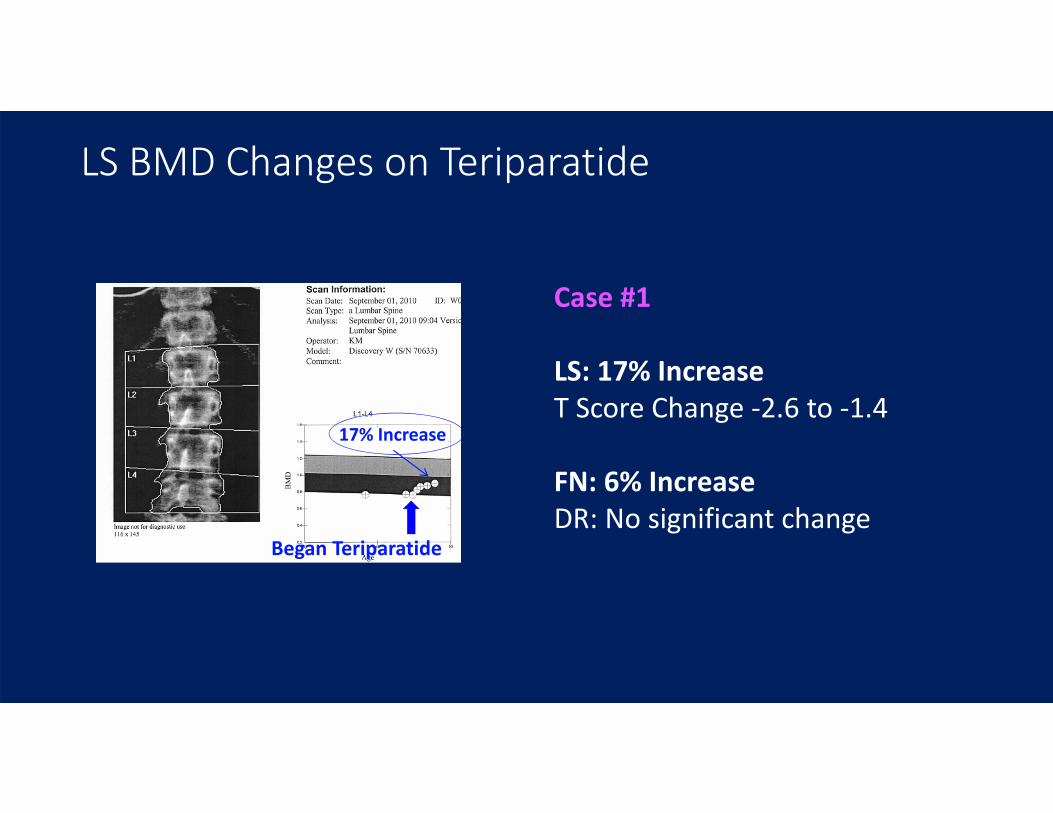
Began Teriparatide
Case #1
LS: 17% IncreaseT Score Change ‐2.6 to ‐1.4
FN: 6% IncreaseDR: No significant change
17% Increase
LS BMD Changes on Teriparatide
*
*
* *
*
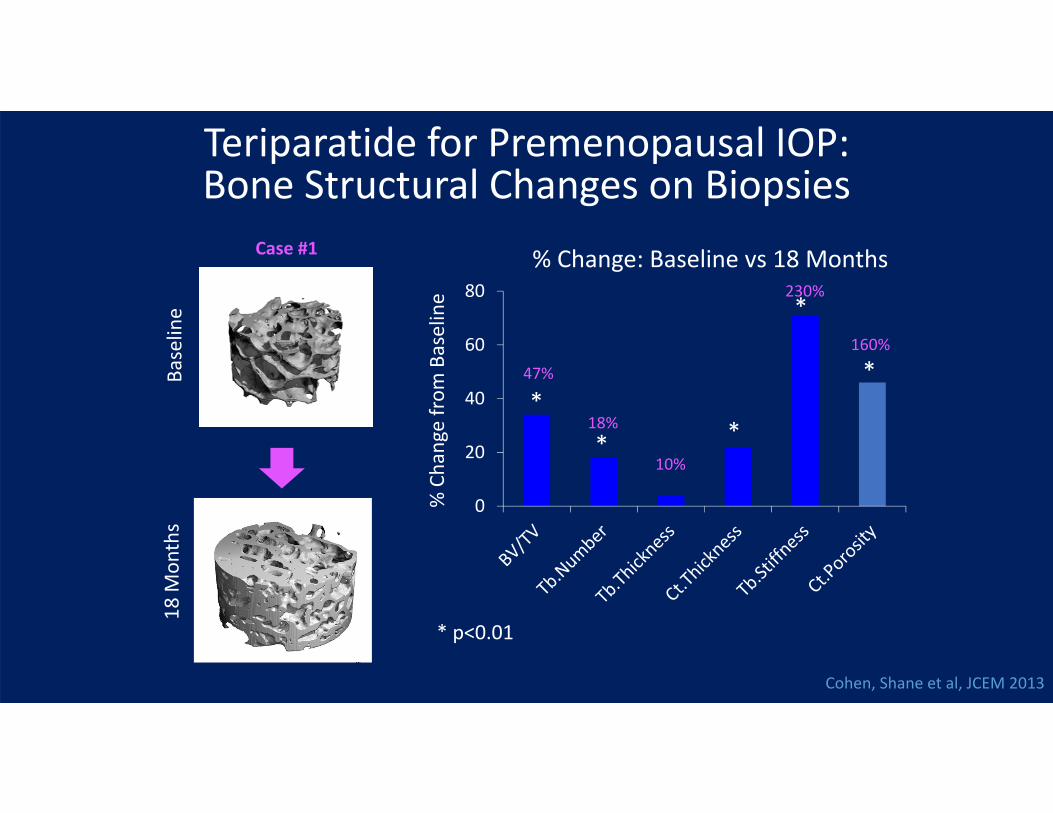
* p<0.01
% Change: Baseline vs 18 Months
% Cha
nge from
Baseline
0
20
40
60
80
Teriparatide for Premenopausal IOP: Bone Structural Changes on Biopsies
Baselin
e18
Mon
ths
Case #1
47%
18%
10%
230%
160%
Cohen, Shane et al, JCEM 2013
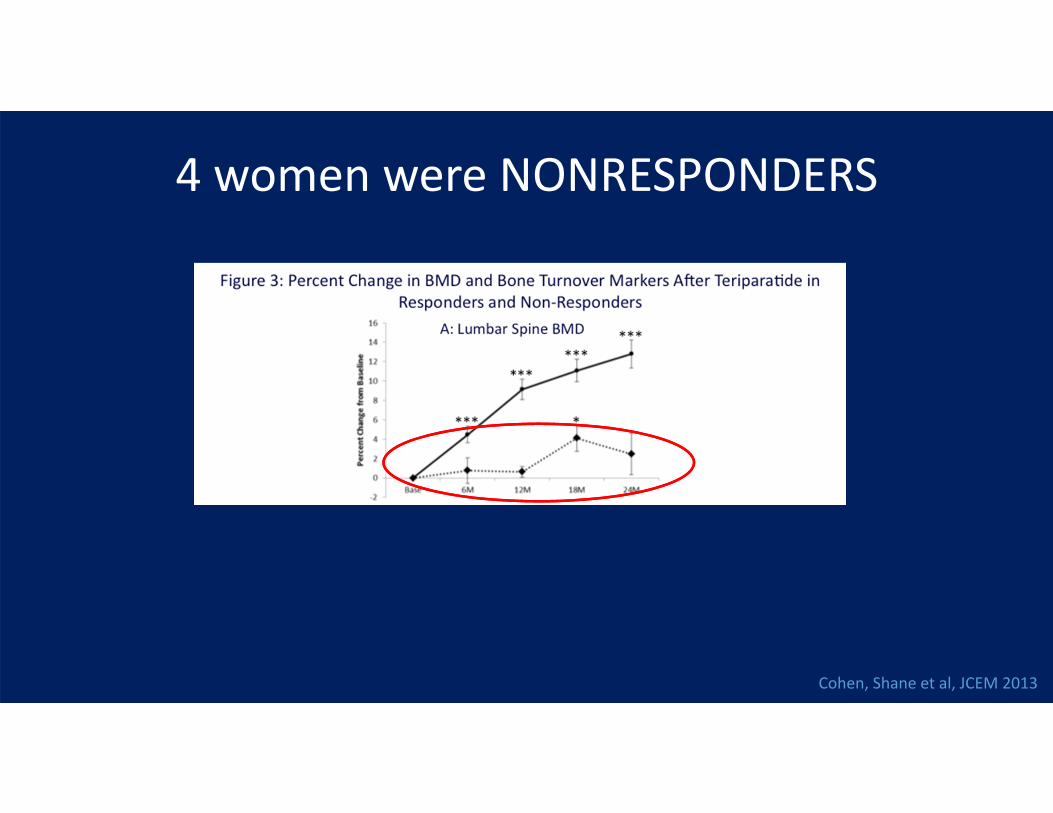
4 women were NONRESPONDERS
Cohen, Shane et al, JCEM 2013
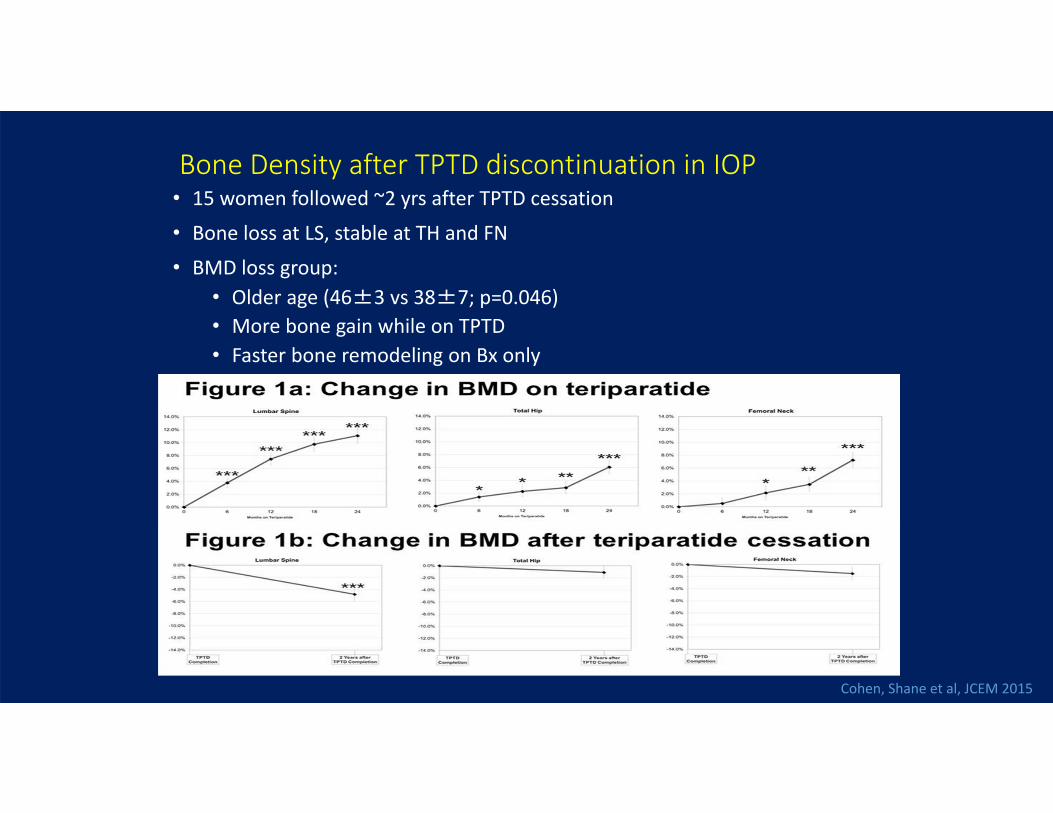
Bone Density after TPTD discontinuation in IOP• 15 women followed ~2 yrs after TPTD cessation
• Bone loss at LS, stable at TH and FN
• BMD loss group:• Older age (46±3 vs 38±7; p=0.046)• More bone gain while on TPTD• Faster bone remodeling on Bx only
Cohen, Shane et al, JCEM 2015

Premenopausal Women with Known Secondary Causes of Bone Loss/Bone Fragility

Case #3• 38 year old premenopausal woman• Diagnosed with celiac disease in the context of 2 years of GI symptoms and:
• dermatologic evaluation for a rash, biopsy consistent with dermatitis herpetiformis.• Iron deficiency• Infertility, undergoing treatment for one year
• Premenopausal with normal menarche and regular periods• NO fractures • Bone density is initially measured at the time of diagnosis (2007)
• Lumbar Spine T/Z ‐2.7• Total Hip T/Z ‐2.0• Femoral Neck T/Z ‐2.2• Distal Radius +0.4
• She is just starting a celiac diet
How should she be evaluated?
Should she be treated with a bone active agent?

Case #3
• Laboratory Evaluation (on CaCO3 500mg TID + Vit D 1000iu), • 4 months after diagnosis
• Calcium 9.3 mg/dL• PTH 55 pg/mL (normal range to 64 pg/mL)• 25D initially 21 ng/ML
corrected over 2 months to 29 ng/mL• Total alkaline phosphatase/BSAP 60 U/L / 14.6 ug/L• 24hour urine calcium 36 mg/24h• UNtx 18 nM BCE/mM Cr• No additional secondary cause found
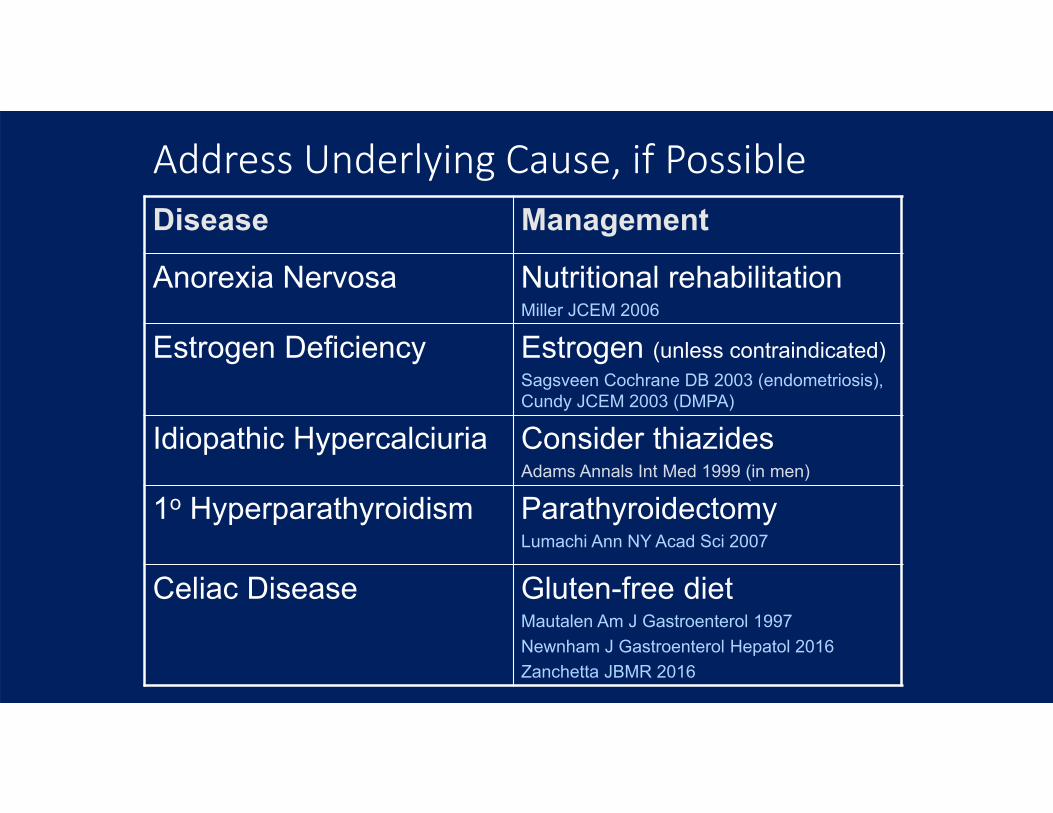
Address Underlying Cause, if PossibleDisease Management
Anorexia Nervosa Nutritional rehabilitationMiller JCEM 2006
Estrogen Deficiency Estrogen (unless contraindicated)Sagsveen Cochrane DB 2003 (endometriosis), Cundy JCEM 2003 (DMPA)
Idiopathic Hypercalciuria Consider thiazidesAdams Annals Int Med 1999 (in men)
1o Hyperparathyroidism ParathyroidectomyLumachi Ann NY Acad Sci 2007
Celiac Disease Gluten-free dietMautalen Am J Gastroenterol 1997Newnham J Gastroenterol Hepatol 2016Zanchetta JBMR 2016
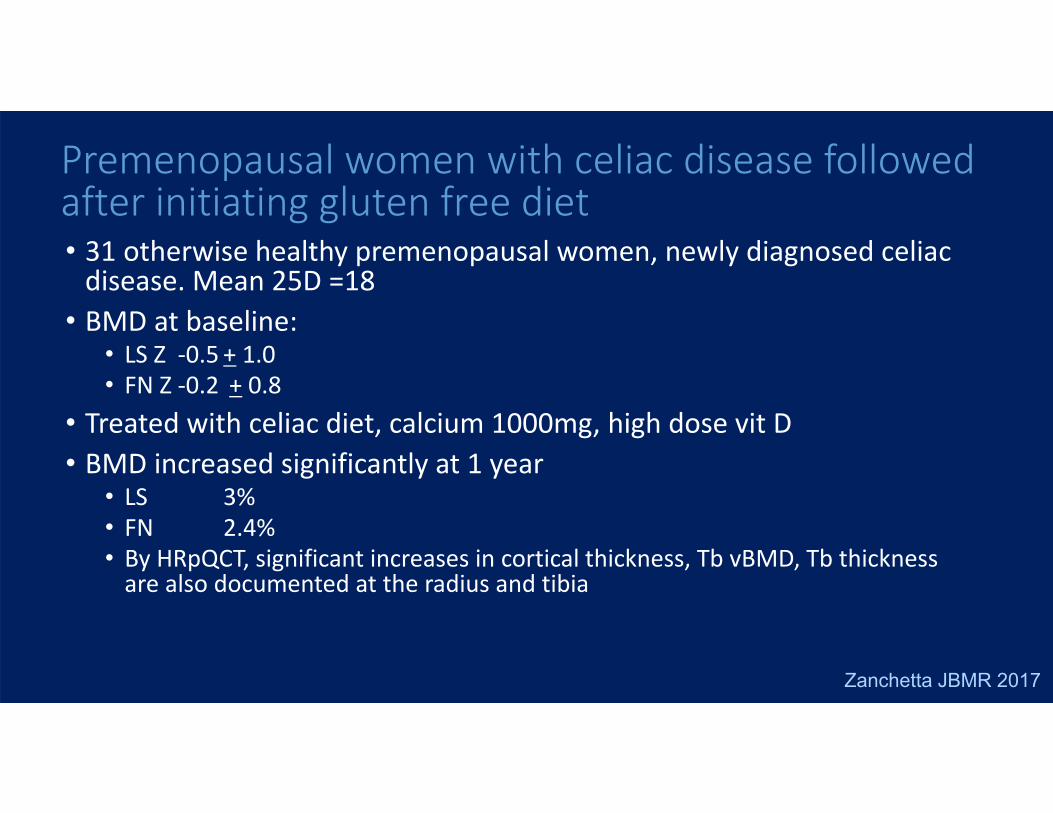
• 31 otherwise healthy premenopausal women, newly diagnosed celiac disease. Mean 25D =18
• BMD at baseline:• LS Z ‐0.5 + 1.0• FN Z ‐0.2 + 0.8
• Treated with celiac diet, calcium 1000mg, high dose vit D• BMD increased significantly at 1 year
• LS 3%• FN 2.4%• By HRpQCT, significant increases in cortical thickness, Tb vBMD, Tb thickness are also documented at the radius and tibia
Premenopausal women with celiac disease followed after initiating gluten free diet
Zanchetta JBMR 2017
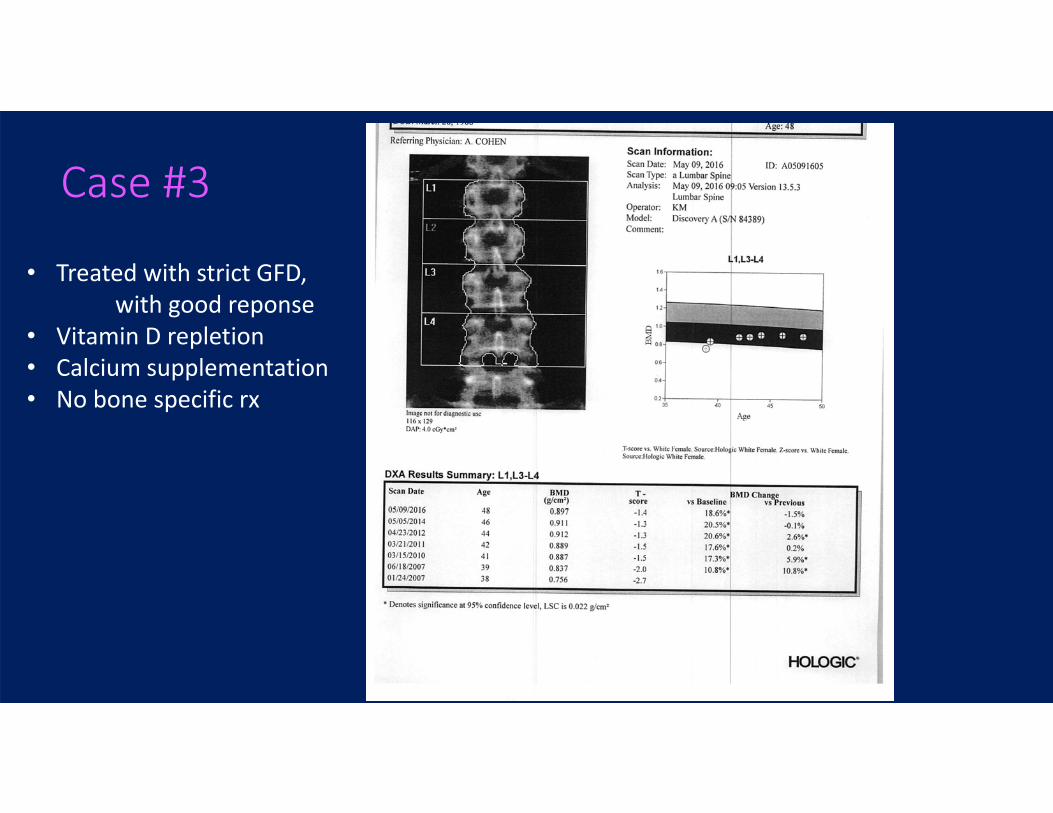
Case #3
• Treated with strict GFD, with good reponse
• Vitamin D repletion• Calcium supplementation• No bone specific rx

Case #3
• Treated with strict GFD, with good response
• Vitamin D repletion• Calcium supplementation• No bone specific rx
Interim Pregnancy

Bone Mass in the context of Pregnancy and Lactation
Case #4: LG• 37 year old woman seen for second opinion about
osteoporosis therapy• Healthy with normal menses• No Fractures
• 1st BMD done at age 34 by her request showed osteopenia• 2nd BMD done 2 years later decreased by ~6% and was
now in the osteoporosis range (T score -2.5)• Her PMD recommended Fosamax• She chose not to take the medication
• 3rd BMD done 1.5 years later shows an increase of ~6%• Everyone is puzzled…
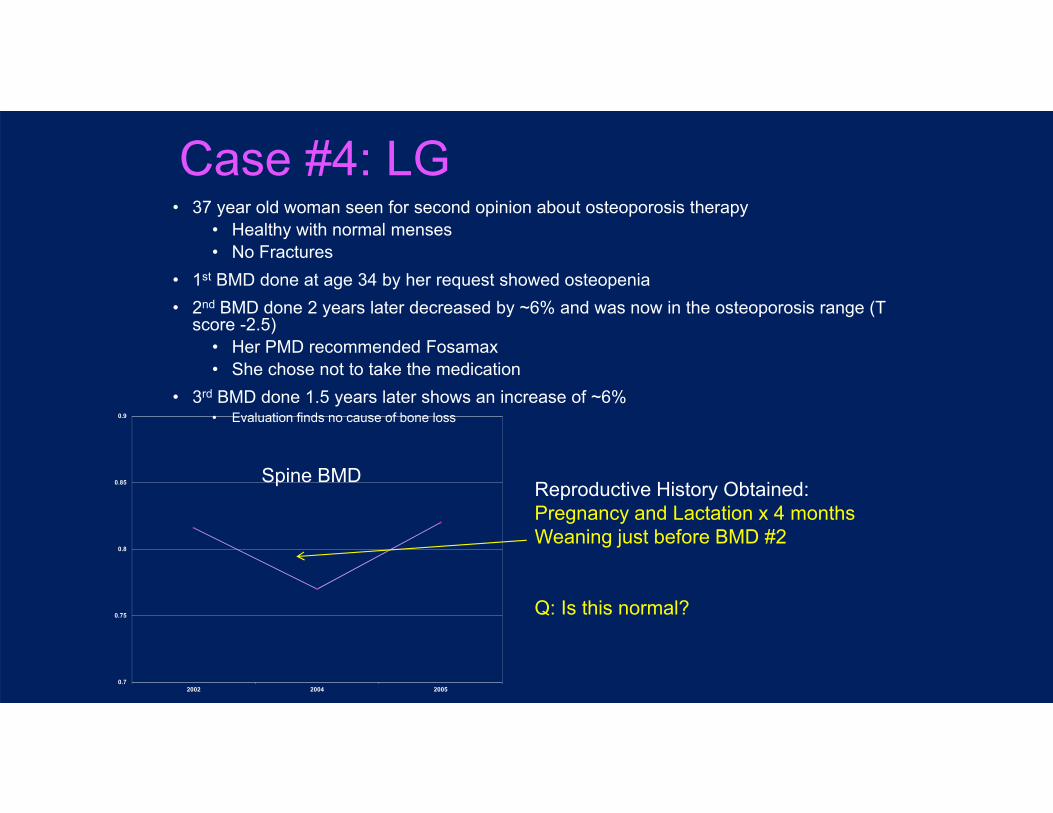
Case #4: LG• 37 year old woman seen for second opinion about osteoporosis therapy
• Healthy with normal menses• No Fractures
• 1st BMD done at age 34 by her request showed osteopenia• 2nd BMD done 2 years later decreased by ~6% and was now in the osteoporosis range (T
score -2.5)• Her PMD recommended Fosamax• She chose not to take the medication
• 3rd BMD done 1.5 years later shows an increase of ~6%• Evaluation finds no cause of bone loss
0.7
0.75
0.8
0.85
0.9
2002 2004 2005
Spine BMDReproductive History Obtained:Pregnancy and Lactation x 4 monthsWeaning just before BMD #2
Q: Is this normal?
Case #5: JZ• 30 year old woman, s/p NSVD of first child at 39wks• Pregnancy had been c/b preterm labor leading to rec for bedrest x 14 weeks
• She was well, breastfeeding, postpartum• At 6 weeks postpartum, while changing the sheets on a bed, she developed acute abdominal and back pain
• Initial imaging focused on abd pathology was negative• Spine MRI: Vert comp fx T8,T11‐L3 – 5 are acute
• One old fracture? She recalls a MVA followed by back pain 5 years ago

Case #5: JZ• BMD T/Z scores 4 months postpartum
• LS: ‐3.7• FN: ‐3.1
• Stops breastfeeding at 4 months postpartum
• BMD 6 months later has increased 9% at the spine, 3% at the hip. Additional follow up shows no change.
• T scores remain quite low: • LS ‐2.9• FN ‐3.0
• Q: Is this normal/expected?
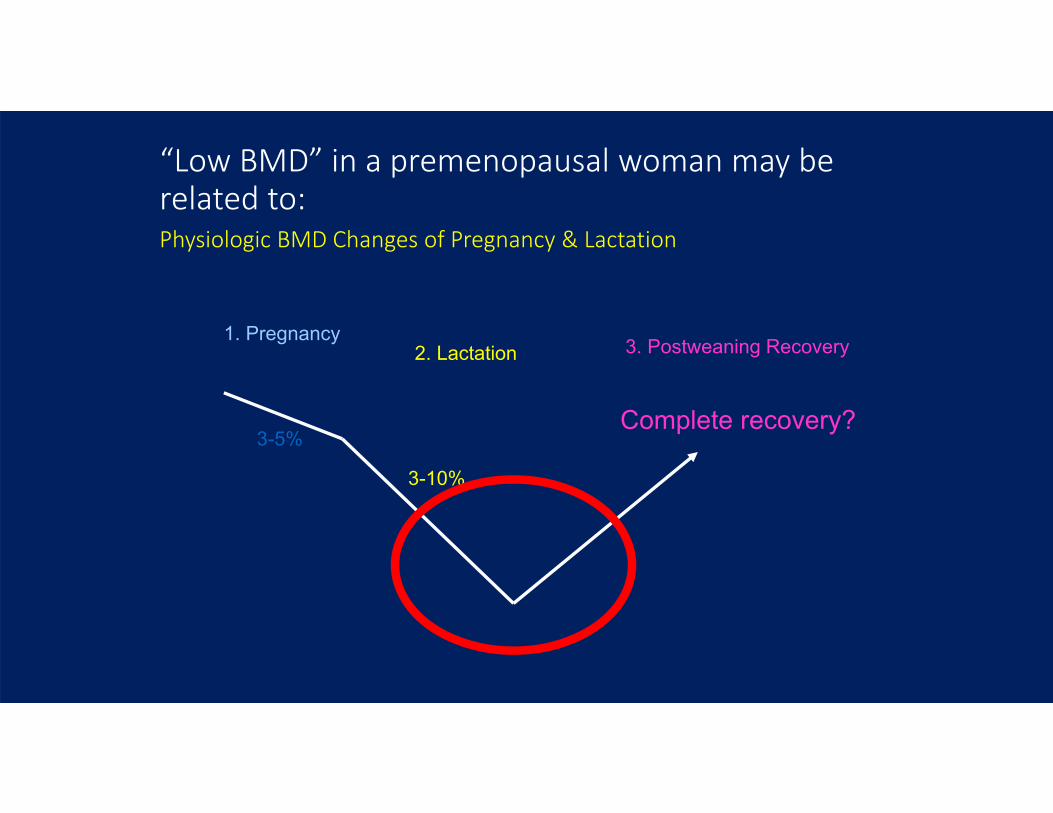
“Low BMD” in a premenopausal woman may be related to:Physiologic BMD Changes of Pregnancy & Lactation
Complete recovery?
1. Pregnancy2. Lactation 3. Postweaning Recovery
3-5%
3-10%

Lactation and BMD• Large Calcium Demand:
• All mammals supply calcium for milk production by mobilizing skeletal calcium stores.
• Ca is transferred mainly from bone → serum → breast milk under control of mammary PTHrP and other factors (CaR, prolactin)• 160 mg/day at 3 months with full lactation• 280‐400 mg/day at 6 months with full lactation
• BMD decline: • 3‐10% loss at the LS and Hip over 3‐6 months of lactation or ≈ 1‐3%/month• Even after correction for changes in soft tissue composition (and weight change).• This rate of change is much more than with estrogen deficiency alone
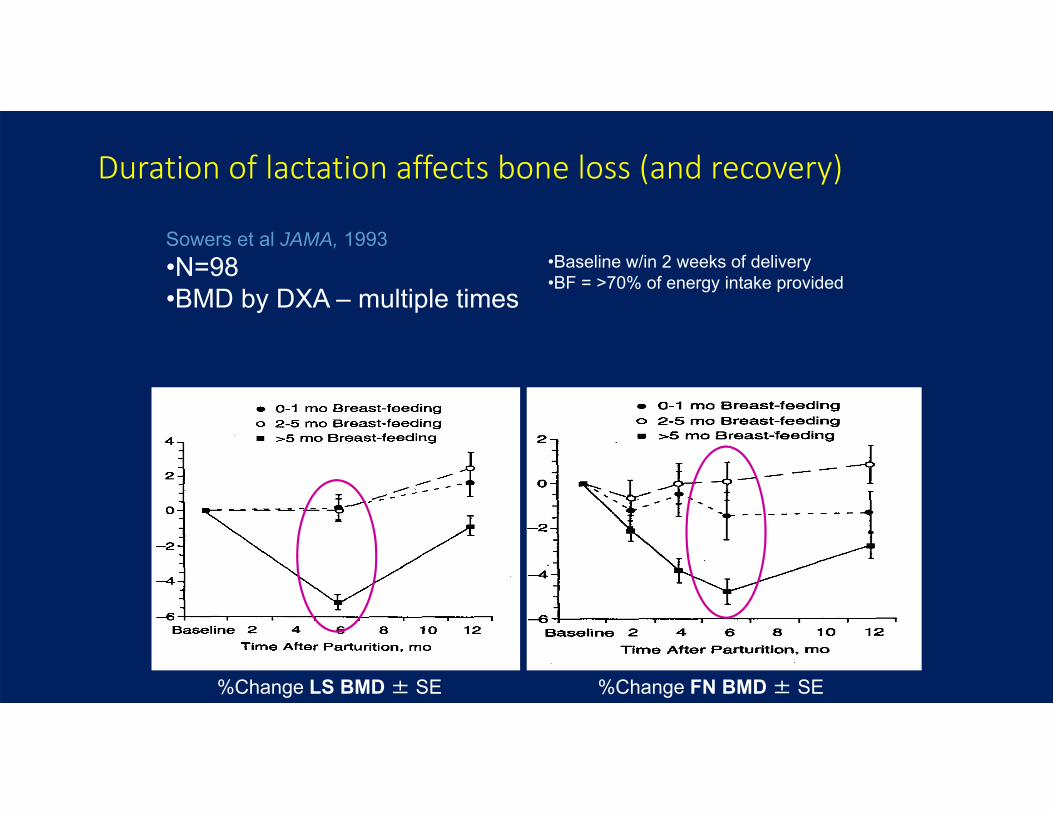
Duration of lactation affects bone loss (and recovery)
Sowers et al JAMA, 1993•N=98•BMD by DXA – multiple times
•Baseline w/in 2 weeks of delivery•BF = >70% of energy intake provided
%Change LS BMD ± SE %Change FN BMD ± SE
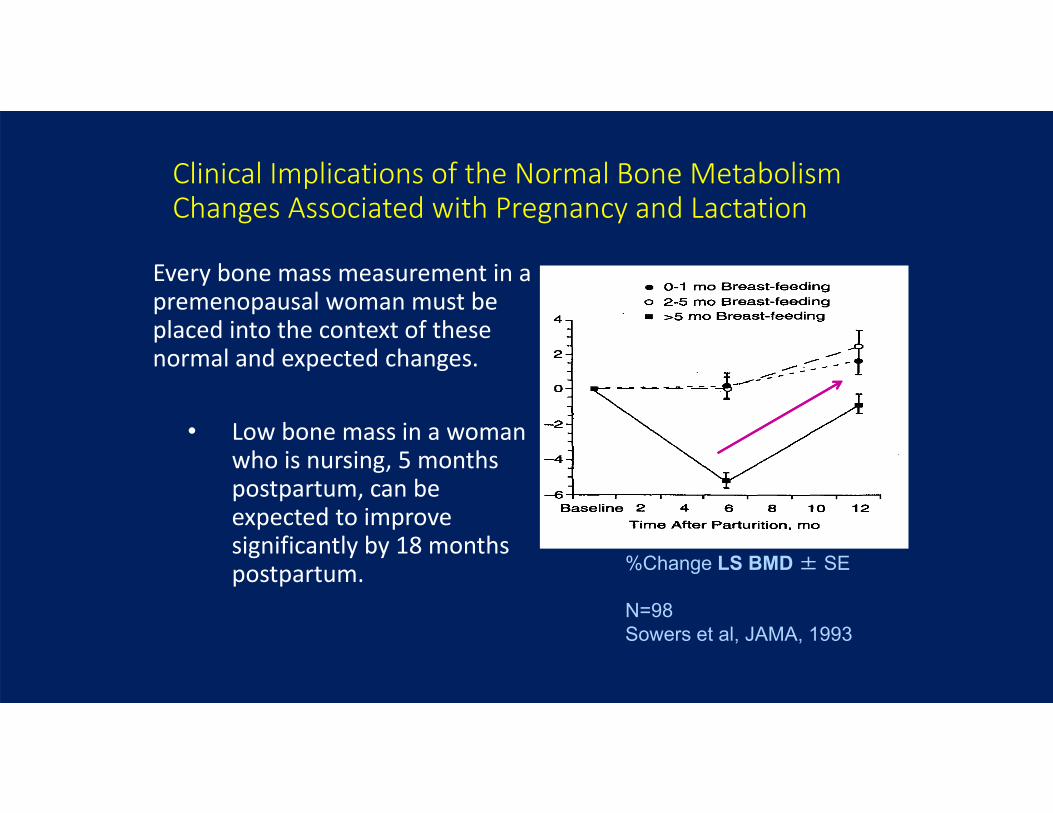
Clinical Implications of the Normal Bone Metabolism Changes Associated with Pregnancy and Lactation
Every bone mass measurement in a premenopausal woman must be placed into the context of these normal and expected changes.
• Low bone mass in a woman who is nursing, 5 months postpartum, can be expected to improve significantly by 18 months postpartum. %Change LS BMD ± SE
N=98Sowers et al, JAMA, 1993

Clinical Implications of the Normal Bone Metabolism Changes Associated with Pregnancy and Lactation
Rarely, fractures occur in the context of these expected bone mass changes.Pregnancy & Lactation Associated Osteoporosis (PLO or PAO):
•Low trauma or spontaneous fractures •Usually multiple vertebral fractures•During late pregnancy or lactation•Majority have no known predisposing condition•Very rare, described in case reports/case series•Subsequent fractures reported in 24% (Kyvernitakis et al, OI 2018)
•~100 subjects, mean follow up = 6 years
We are initiating a new FDA funded study to investigate etiologies, mechanisms of disease, and genetic characteristics (referrals welcome!)
36 year old woman presenting with back pain while breastfeeding
5 months postpartum
Choe et al JBMM 2012
PLO – What could we tell Case #5 about her prognosis?• Longitudinal study cohort evaluated in one recent study:
• 107 women with PLO diagnosis, median follow up 6 + 4 years• ~90% with vertebral fractures, Average #fx=4
• Subsequent fracture risk• 26/107 or 24% had subsequent fractures (25/26 had additional vert fx)• # of fractures at diagnosis predicted subsequent risk
• 30 women became pregnant again, 17 went on to delivery• All had received some rx with bisphosphonate or TPTD before pregnancy• 6/30 or 20% had disease recurrence: pregnancy associated fractures
• Bisphosphonate and teriparatide use has been reported in case series• Many questions remain regarding treatment options, and treatment timing
Kyvernitakis et al, OI 2018
• Routine BMD screening not recommended• Measure BMD in those with
• Known secondary causes of osteoporosis• History of low trauma fracture
• Interpret BMD in the context of growth and reproductive events.
• Look for secondary causes of osteoporosis in those with low BMD or low trauma fractures (regardless of BMD)
Summary: Diagnosis and Evaluation
1. Management recommendations:• Adequate Calcium/D/exercise• Treat secondary causes specifically
2. Drug Rx rarely justified for isolated low BMD• Repeat BMD in 1‐2 years to assess for ongoing bone
loss
Summary: Management
3. Consider drug treatment: • Long‐term glucocorticoids• Documented accelerated bone loss• Fragility fractures• Perimenopausal
4. Bisphosphonates and teriparatide are FDA approved only in the setting of GIO
5. No fracture data in this population
Summary: Management

Many Remaining Areas of Uncertainty• Which kinds of fractures represent true evidence of bone fragility?
• Spine and hip fractures• Foot fractures?• Stress fractures?
• What sort of fracture history should lead to a recommendation for medical treatment?
• Which medication(s) should be used?• How long should a course of treatment last in a premenopausal woman?