OS206 Trans
4
OS 206: Abdomen and Pelvis KUB Radiologic Anatomy Dr. K. Baldivio 3 November 27, 2012 Page 1 / 4 Arielle, Nikki, Roger TOPIC OUTLINE I. Introduction II. X-ray A. Plain Film B. Excretory Urography/ Intravenous Pyelography C. Renal Angiography III. CT Scan IV. Normal physiological variations V. Pathology VI. Some Questions Legends: From the Powerpoint presentation From the lecturer From other sources (textbook, Internet, etc.)! I. INTRODUCTION RADIOLOGY • Radiology involves minimal or non-invasive anatomic evaluation • Modalities o X-ray o Ultrasound (not in the lecture) o CT Scan o MRI THE EXCRETORY SYSTEM Excretory organs Products eliminated Primary Secondary Kidneys Water, nitrogenous wastes, inorganic salts Heat, CO2 Lungs CO2 Heat, H2O Skin Heat CO2, H2O, Salts, Urea GI tract Solid wastes, secretions CO2, H2O, Salts, Urea The Urinary System • Helps keep the body in homeostasis • Controls composition and volume of blood Kidneys • Visualized due to perirenal fat • Fat wasting occurs in disease hence they become less visible. • To appreciate the kidneys, bowel preparation must be done. Otherwise, fecal material may obstruct the view. • Renal position o From level of T11-L3 (or T12-L4) o Axis of the kidneys lie parallel and lateral to the psoas muscle (psoas shadow) o Right kidney is 2 cm lower than the left because of the position of the liver. o The lower pole is more anterior relative to the superior pole o Kidneys are oriented down and out, its lateral borders has many humps. Embryologic indentations, called Dromedary humps. o In upright position, kidneys descend 2-3 cm and move moderately with respiration. • Coverings of the kidney: o Renal capsule Adherent to the kidney Protection from blunt trauma Continuous with the hilum o Perirenal fat Not seen normal unless fibrotic or inflamed Surrounds the kidneys and their vessels as it extends into their hollow centers, called the renal sinuses. Keeps kidneys in position In plain film, grey region around psoas major and kidney o Renal fascia Membranous layer that encloses the kidneys, perirenal fat and suprarenal glands Continues medially to ensheath the renal vessels o Pararenal Fat External to the renal fascia; the extraperitoneal fat of the lumbar region that is most obvious posterior to the kidney • Renal hilum o Medial indentation, which opens into the renal sinus o Versus renal pelvis: expansion of superior end of ureter o Exit and entry of the renal vein, renal artery, nerves, and tubules that drain urine from the kidney. • Renal Pelvis o It’s apex continuous with the ureter o Receives 2 or 3 major calyces, each of which divides into 2 or 3 minor calyces o Each minor calyx indented by renal papilla, the apex of renal pyramid. Ureters • Muscular ducts that run inferiorly from the apex of renal pelvis (Moore). • Not usually seen in plain film since collapsed Urinary Bladder • When empty, lies partially superior to the pubic bones. (Moore) • Not usually seen in plain film unless with contrast or if entirely filled with urine. X-RAY A. PLAIN FILM o No contrast or dye injected/ swallowed because it will obscure organs. o The general location, size and other pathologic findings are identified first before contrast is added. o Usually done in supine position, in deep inspiration. o Recall: The patient’s right side is on your left (Treat as if you are looking at the mirror). o Soft tissue mass/ fat: grey o Air or fluid: black o Other structures that may be observed o Bowel gas patterns o Track foreign bodies o Calcifications Phleboliths: Calcified pelvic veins, with lucent center and calcified walls. They appear as round structures in plain film. It is considered normal. Figure 1. Normal Plain Film of abdomen showing kidneys and urinary bladder Right kidney Right kidney Left kidney Left kidney Psoas line Psoas line Iliacus Iliacus Iliacus Iliacus Urinary bladder Urinary bladder
-
Upload
johna-mandac -
Category
Documents
-
view
18 -
download
4
Transcript of OS206 Trans

OS 206: Abdomen and Pelvis KUB Radiologic Anatomy Dr. K. Baldivio
3 November 27, 2012
Page 1 / 4 Arielle, Nikki, Roger
TOPIC OUTLINE I. Introduction II. X-ray
A. Plain Film B. Excretory Urography/ Intravenous Pyelography C. Renal Angiography
III. CT ScanIV. Normal physiological variationsV. Pathology VI. Some Questions
Legends: From the Powerpoint presentation From the lecturer From other sources (textbook, Internet, etc.)!
I. INTRODUCTION
RADIOLOGY • Radiology involves minimal or non-invasive anatomic evaluation• Modalities
o X-rayo Ultrasound (not in the lecture)o CT Scano MRI
THE EXCRETORY SYSTEM
Excretory organs Products eliminated Primary Secondary
Kidneys Water, nitrogenous wastes, inorganic
salts
Heat, CO2
Lungs CO2 Heat, H2O Skin Heat CO2, H2O, Salts,
Urea GI tract Solid wastes,
secretions CO2, H2O, Salts,
Urea
The Urinary System
• Helps keep the body in homeostasis• Controls composition and volume of blood
Kidneys • Visualized due to perirenal fat• Fat wasting occurs in disease hence they become less visible.• To appreciate the kidneys, bowel preparation must be done.
Otherwise, fecal material may obstruct the view.• Renal position
o From level of T11-L3 (or T12-L4)o Axis of the kidneys lie parallel and lateral to the psoas muscle
(psoas shadow)o Right kidney is 2 cm lower than the left because of the position
of the liver.o The lower pole is more anterior relative to the superior poleo Kidneys are oriented down and out, its lateral borders has
many humps.§ Embryologic indentations, called Dromedary
humps. o In upright position, kidneys descend 2-3 cm and move
moderately with respiration.
• Coverings of the kidney:o Renal capsule
§ Adherent to the kidney § Protection from blunt trauma § Continuous with the hilum
o Perirenal fat§ Not seen normal unless fibrotic or inflamed § Surrounds the kidneys and their vessels as it
extends into their hollow centers, called the renal sinuses.
§ Keeps kidneys in position § In plain film, grey region around psoas major and
kidney o Renal fascia
§ Membranous layer that encloses the kidneys, perirenal fat and suprarenal glands
§ Continues medially to ensheath the renal vessels
o Pararenal Fat§ External to the renal fascia; the extraperitoneal
fat of the lumbar region that is most obvious posterior to the kidney
• Renal hilumo Medial indentation, which opens into the renal sinuso Versus renal pelvis: expansion of superior end of uretero Exit and entry of the renal vein, renal artery, nerves, and
tubules that drain urine from the kidney.
• Renal Pelviso It’s apex continuous with the uretero Receives 2 or 3 major calyces, each of which divides into 2
or 3 minor calyceso Each minor calyx indented by renal papilla, the apex of renal
pyramid.
Ureters • Muscular ducts that run inferiorly from the apex of renal pelvis
(Moore).• Not usually seen in plain film since collapsed
Urinary Bladder • When empty, lies partially superior to the pubic bones. (Moore)• Not usually seen in plain film unless with contrast or if entirely filled with
urine.
X-RAY
A. PLAIN FILM o No contrast or dye injected/ swallowed because it will obscure
organs.o The general location, size and other pathologic findings are
identified first before contrast is added.o Usually done in supine position, in deep inspiration.o Recall: The patient’s right side is on your left (Treat as if you are
looking at the mirror).o Soft tissue mass/ fat: greyo Air or fluid: blacko Other structures that may be observedo Bowel gas patternso Track foreign bodieso Calcifications
§ Phleboliths: Calcified pelvic veins, with lucent center and calcified walls. They appear as round structures in plain film. It is considered normal.
Figure 1. Normal Plain Film of abdomen showing kidneys and urinary bladder
Right kidneyRight kidney
Left kidneyLeft kidney
Psoas linePsoas line
IliacusIliacusIliacusIliacus
Urinary bladderUrinary bladder
Page 2 / 4 Arielle, Nikki, Roger
KUB Radiologic Anatomy OS 206
A.
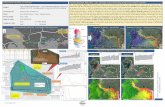
B. Figure 2. Close-up view of plain film showing natural contrast
between kidney and the low-density retroperitoneal fat that surrounds it.
B. EXCRETORY UROGRAPHY/ INTRAVENOUS PYELOGRAPHY (IVP)
• Serial films are obtained 15- 25 minutes as contrast is excreted bythe kidneys visualize the renal collecting system, ureters andbladder.o Ureters cannot generally be seen, except upon its entry into
the posterior trigone of the bladder.
• Phases1. Nephrographic phase: Renal tubules process the contrast
o A problem with a medulla will be manifested by a delayin the visualization of the contrast (eg. stab wound).
o Structures visualized:1. Renal tubules, seen as striations in the pyramids
(Note: Pyramids + cortex= parenchyma)2. Renal columns of Bertin3. Apex4. Renal papilla
2. Pyelographic phase:o Additional structures visualized, when the contrast
material reaches this phase:§ Minor calyx (6-14/ kidney according to Ma’am.)
- Dense peripheral and lucent center - Fornix and body connect to the major calyx.
§ Major calyx (3-4/ kidney) § Renal pelvis: Triangular beginning of the ureter
- Discharge of urine from the renal pelvis is accompanied by ureteral peristalsis
§ Ureter - Not seen completely - Narrow at certain areas, where stones are likely
to lodge: 1. Uretero-pelvic junction2. Uretero-vesical junction3. At the bifurcation of the common iliac
vessels§ Bladder
- Full: Egg shaped and smooth - Partially distended: irregular shape, and with air - Problem: Thick and irregular wall - Higher in females due to uterus
Figure 3. Intravenous Pyelography
Figure 2: 1 - Superior pole of kidney 8 - Right Kidney 2 - Twelfth rib 9 - Inferior pole of kidney 3 - Superior calyces 10 - Ureter 4 - Middle calyces 11 - Margin of psoas 5 - Renal calyces 12 - Distal ureter 6 - Inferior calyces 13 - Urinary bladder 7 - Left kidney
RENAL ANGIOGRAPHY
o Ma’am didn’t elaborate much on this.o A vascular catheter is inserted into the femoral artery
(percutaneous), to visualize blood vessels, malformations oradnormal enhancements.• Iodine-based.
CT SCAN
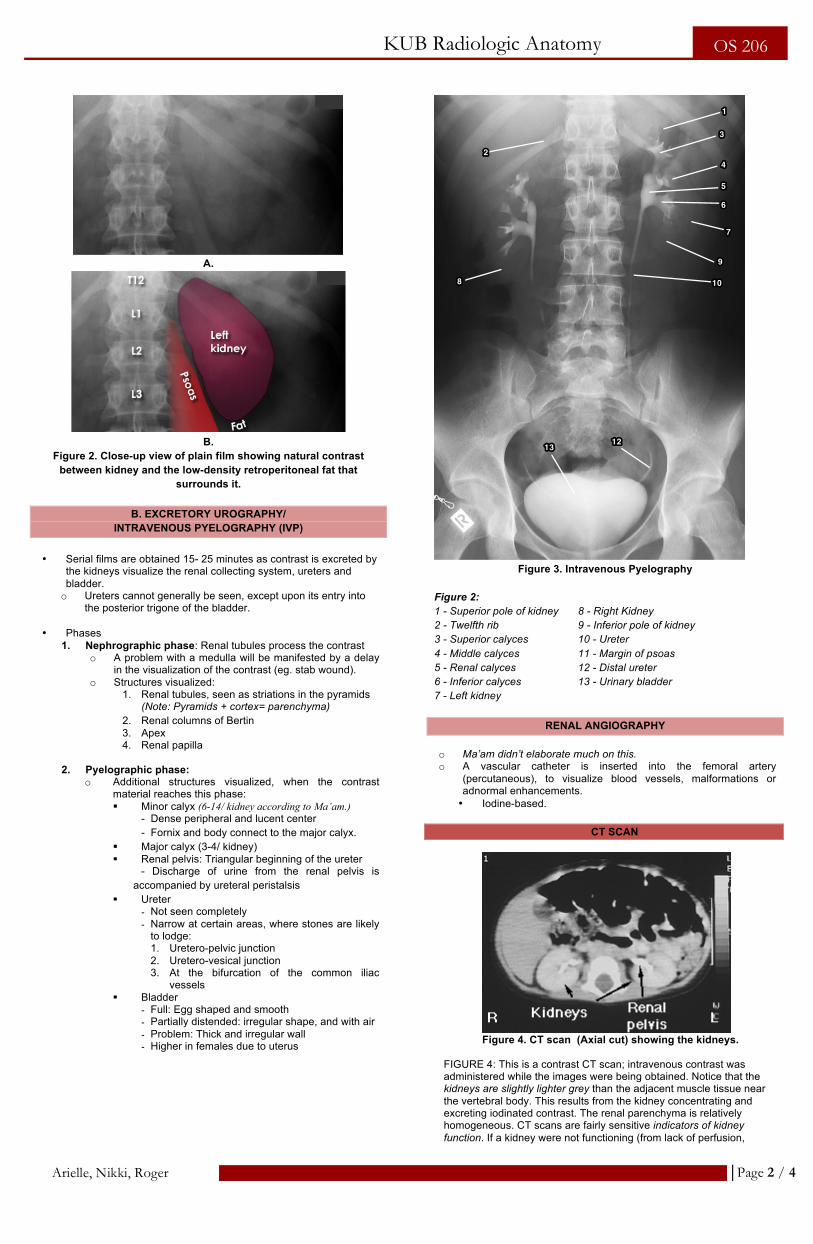
Figure 4. CT scan (Axial cut) showing the kidneys.
FIGURE 4: This is a contrast CT scan; intravenous contrast was administered while the images were being obtained. Notice that the kidneys are slightly lighter grey than the adjacent muscle tissue near the vertebral body. This results from the kidney concentrating and excreting iodinated contrast. The renal parenchyma is relatively homogeneous. CT scans are fairly sensitive indicators of kidney function. If a kidney were not functioning (from lack of perfusion,
11
33
44
55
66
77
1010
99
88
22
12121313
Page 3 / 4
Arielle, Nikki, Roger
KUB Radiologic Anatomy
OS 206
severe tubular dysfunction, etc.) then the kidneys wouldn't 'enhance' (appear lighter grey). The renal pelvis is white because iodinated contrast has filled the collecting system.
Figure 5. CT slice through the mid-abdomen showing multiple
normal-appearing organs, which are labeled.
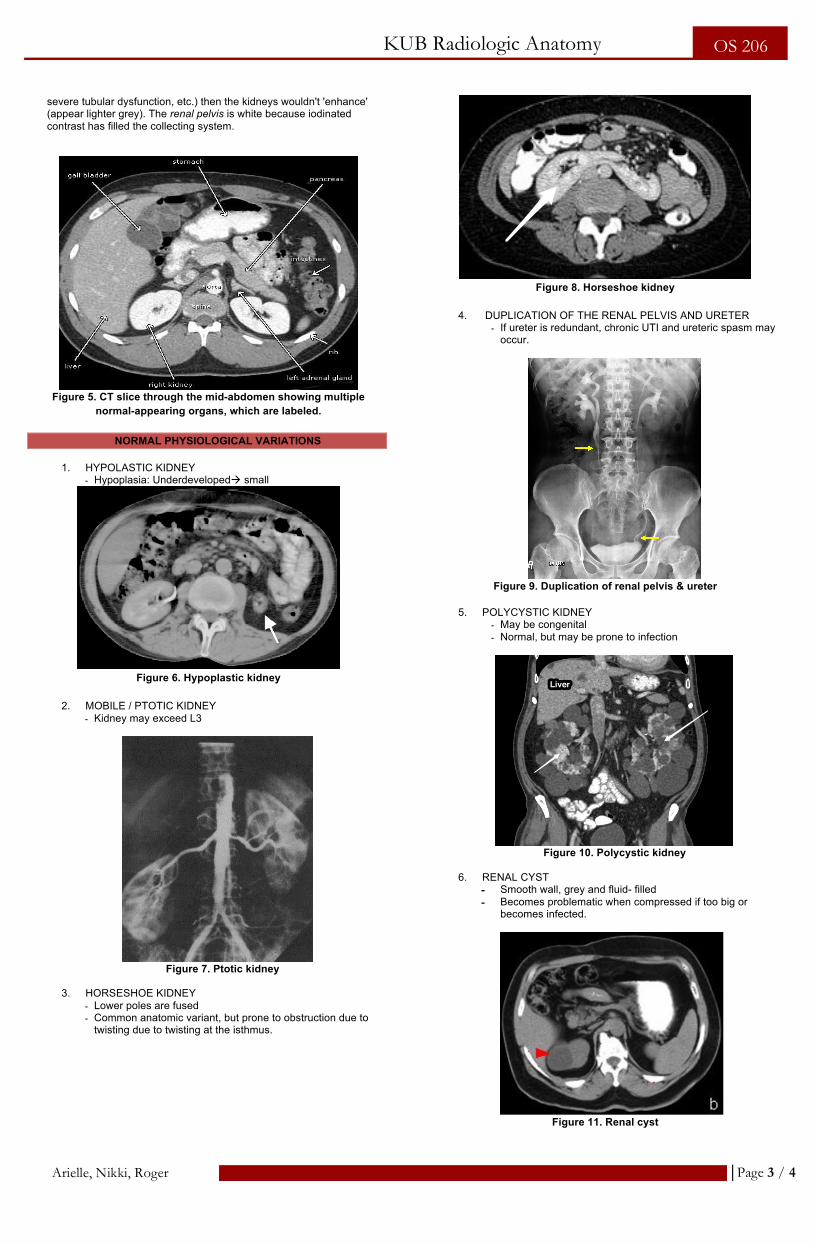
NORMAL PHYSIOLOGICAL VARIATIONS
1. HYPOLASTIC KIDNEY - Hypoplasia: Underdevelopedà small
Figure 6. Hypoplastic kidney
2. MOBILE / PTOTIC KIDNEY
- Kidney may exceed L3
Figure 7. Ptotic kidney
3. HORSESHOE KIDNEY
- Lower poles are fused - Common anatomic variant, but prone to obstruction due to
twisting due to twisting at the isthmus.
Figure 8. Horseshoe kidney
4. DUPLICATION OF THE RENAL PELVIS AND URETER
- If ureter is redundant, chronic UTI and ureteric spasm may occur.
Figure 9. Duplication of renal pelvis & ureter
5. POLYCYSTIC KIDNEY
- May be congenital - Normal, but may be prone to infection
Figure 10. Polycystic kidney
6. RENAL CYST
- Smooth wall, grey and fluid- filled - Becomes problematic when compressed if too big or
becomes infected.
Figure 11. Renal cyst
LiverLiver
Page 4 / 4
Arielle, Nikki, Roger
KUB Radiologic Anatomy
OS 206
PATHOLOGY
1. ABSCESSES AROUND THE KIDNEY:
- Collection of pus (debris)à soft tissue density - More dense than normal left hemi abdomen - Splinting: lumbar vertebrae displaced laterally - Extrinsic compression by a psoas abcess
2. OVARIAN MASS
- Ureter deviated medially - Pelvis is dilatedà hydronephrosis
3. URETERO- NEPHROLITHIASIS
- Appearing as dense structures due to calcium 4. FILLING DEFECT OF PELVIS 5. PELViCACTASIA SECONDARY TO AN OBSTRUCTED URETER
- Swelling of pelvis and calycesà pressure pushes it outward
- Obstructive uropathyà non functioning kidney
6. RENAL CELL CARCINOMA - Soft tissue mass extendingà lost normal architecture - Pelvo- calyceal system may be distendedà beginning of
hydronephrosis 7. BLASTIC BONES
- Abnormal deposition of bone, usually seen in prostate cancer. - Versus lytic bones: abnormal resorption
8. BLADDER CYSOCOELE - Outpouching of the bladder/ “Merry Christmas” - Weak pelvic floor, may be due to multiple births
9. LINEAR CALFICIFATION OF BOTH URETERS 10. URETHRAL STENOSIS/ NARROWING
- May be due to enlarged prostate - The narrowing may result in low bladder capacity
SOME QUESTIONS
RENAL TRANSPLANT Q: How do you visualize transplanted kidneys? Are they visible in plain film? (not verbatim)
o Some perirenal fat is retained around the transplanted kidney. o The best modality would be CT scan, paired with good history
taking. o Management is tailored based on what the patient has had. o Transplanted kidney should be shielded from radiation
therapy, if needed.
PA vs. AP VIEW
o Kidneys appear larger in PA view. This is because the kidneys are located posteriorly. Be careful on this in the clinics. Larger appearance in PA view doesn’t mean that the kidneys are actually enlarged. PA film only magnifies the kidney.
o When writing reports, indicate: “The kidneys are magnified, but not enlarged.”
End of Transcription
GREETINGS, GREETINGS!
Remo: Good Morning. Gusto ko po sanang batiin si Ma’am Mantaring, ehem ehem Good Morning! At sa lahat ng mga KulayNaBumubudoodoomBumubuhaySaMundoodoom J Hello nga pala kay Geoff haha mula kay Arielle.
Arielle: And if am flying solo, at least am flying free J
Good morning Roger! BOW! A million hugs and kisses to:
1. WAKA- bles. More gimmicks, movie nights and dine outs for my med life! Mah girlies Patring and Kei baybeh.
2. My brahs and brohs. I shall win Monopoly Deal in the future. 3. Med life crises- mates. Ith, you will find your glenoid fossa.
OR NOT! Am kidding, Joson loves you. GJ Empire will go down. OR UP! HAPPY BIRTHDAY! Johnny baby he is just there :>
4. My roommies, aka the internet less people. 5. My forever transmates, Ari Ni Roger. 6. Chorchor zebras. 7. MSSR lovabies. 8. Variable seatmates. GOOD MORNING APPENDIX! 9. POST IT! If there’s a Will, there’s a Kei. And then there’s
Aaron and Ith HAHA. 10. FUTURE 2018. I hope you enjoyed the Freshman Orientation
Program ;) Hello Pugad Sayk babies! MWAH MWAH. 11. TRP CHORALalaloopsies! 12. Psych Republiquans Meggie, Vince, Bernette, Pia, Chiong
and Kevin Kevins! Also hello to my library-mates! “Ano bang meron kang di ko mabitiwan. Di ako tinitigilan.” Arielle joke for the trans: What do you call a hipster med student? (ILIAC- CRESTer HIHI)
Nikki: Ihi ka ba? I like U-RINE kasi! Hello! Good luck sa ating lahat sa TRP and sa exams.