Origins of Sleep Apnea How Did We Get Here?
140
This presentation is intended for educational purposes only. Statements of facts and opinions expressed are those of the educator/doctor individually, and unless expressly stated to the contrary, are not the opinion of the course sponsor, Vivos Therapeutics, Inc. Origins of Sleep Apnea – How Did We Get Here? Presenter Name: Dr. Ben Miraglia, DDS
Transcript of Origins of Sleep Apnea How Did We Get Here?

This presentation is intended for educational purposes only. Statements of facts and opinions expressed are those of the educator/doctor individually, and unless expressly stated to the contrary, are not the opinion of the course sponsor, Vivos Therapeutics, Inc.
Origins of Sleep Apnea – How Did We Get Here?
Presenter Name: Dr. Ben Miraglia, DDS

This presentation is intended for educational purposes only. Statements of facts and opinions expressed are those of the educator/doctor individually, and unless expressly stated to the contrary, are not the opinion of the course sponsor, Vivos Therapeutics, Inc.
Statements of facts and opinions expressed are those of the educator/doctor individually, and unless expressly stated to the contrary, are not the opinion of Vivos Therapeutics, Inc.
Any use of the Vivos appliances outside of or “off label” from the FDA Cleared and/or Registered Indication(s) for use is the sole responsibility of the treating dentist at her/his clinical discretion and is not the teachings, guidelines, or recommendation of Vivos Therapeutics, Inc.
Vivos does not have an appliance to treat children diagnosed with Sleep Disordered Breathing. Any use of the Vivos appliances outside of or “off label” from the FDA Cleared and/or Registered Indication(s) for use is the sole responsibility of the treating dentist at her/his clinical discretion and is not the teachings, guidelines, or recommendation of Vivos Therapeutics, Inc.

HIPAA Please do not photograph or record any of the minor patients in this
presentation.
All patients shown are treated by Dr. Ben Miraglia
Any reproduction and use of the patient case content is a violation ofHIPAA

“This presentation is intended for educational purposes only. Statements of facts and opinions expressed are those of the educator/doctor individually, and unless expressly stated to the contrary, are not the opinion of the course sponsor, Vivos Therapeutics, Inc.”

WHY ARE WE HERE?
For the overall growth, development, health and longevity of our young
patients.
5

Children are struggling with symptoms…
ADHD
Bedwetting
Upper respiratoryinfections
Ear infections/tubes
Night terrors
Academic struggles
Hyperactivity
Aggressive behavior
Clenching/Grinding
Restless sleep/wakes
Asthma
Small/Delayed growth
Anxiety
Depression
Daytime sleepiness
Overweight
Obesity
Night sweats
GI distress/reflux
Emotional instability
Sensory issues
Snoring
Mouth breathing6

How did this child get here?What do we see?

How did this child get here?What do we see?
The most common orthodontic problem is a crowded malocclusion.

1. Improper Arch Form
Causes of Crowded Malocclusion
10

Causes of Crowded Malocclusion Improper vs. Proper Arch Form

1. Improper Arch Form
2. Improper Arch Width
1. Transverse Measurement
2. The Eyes
Causes of Crowded Malocclusion
12

Improper Arch Width
2. Improper Arch Width
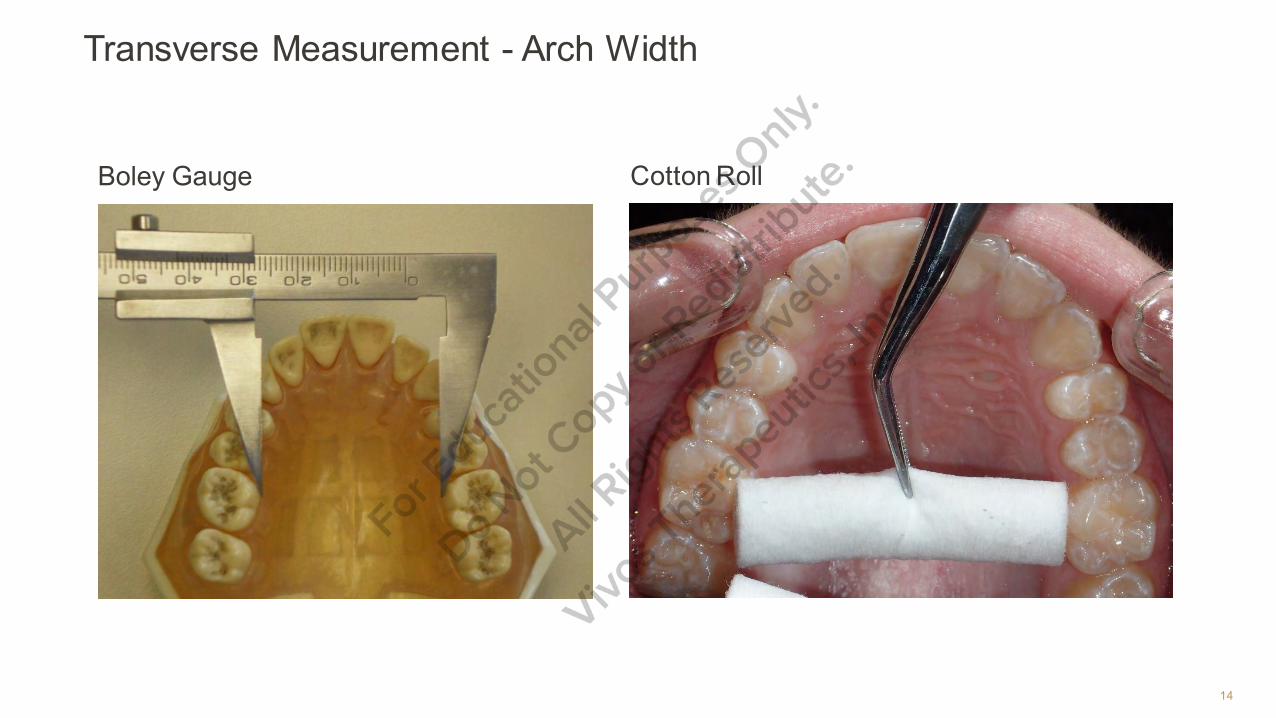
Transverse Measurement
The shortest distance between teeth 3 and 14.
Children who develop naturally without orthodontic intervention become adults who achieve a 35-39mm transverse measurement.
14
Transverse Measurement - Arch Width
Boley Gauge Cotton Roll

15
Transverse Measurement Arch Width
Boley Gauge Cotton Roll
37mm

PRIMARY TEETH

The Eyes
Venous Pooling - purple/blue discolorationunder the eyes
CO2 is a vasodilator
Mouth breathing reduces blood CO2
Less CO2 means less vasodilation or morevasoconstriction
The inferior orbital vein is a superficial vessel,when it contricts we see…
VENOUS POOLING
17

VENOUS POOLING
LET’S PUT SOME PIECES TOGETHER
Improper arch form and width are the result of underdevelopment of themaxilla and mandible.
I.E: An underdeveloped maxilla and mandible is the cause ofmalocclusion
An underdeveloped maxilla has an adverse effect on the position of themandible. It traps the mandible in a retruded position.

Craniofacial Growth & Development Normal growth is wide, forward and downward
Abnormal growth is narrow, backward and downward
Abnormal growth is underdevelopment
Professionally known as Craniofacial Deficiency

Ideal Craniofacial Growth & Development
21

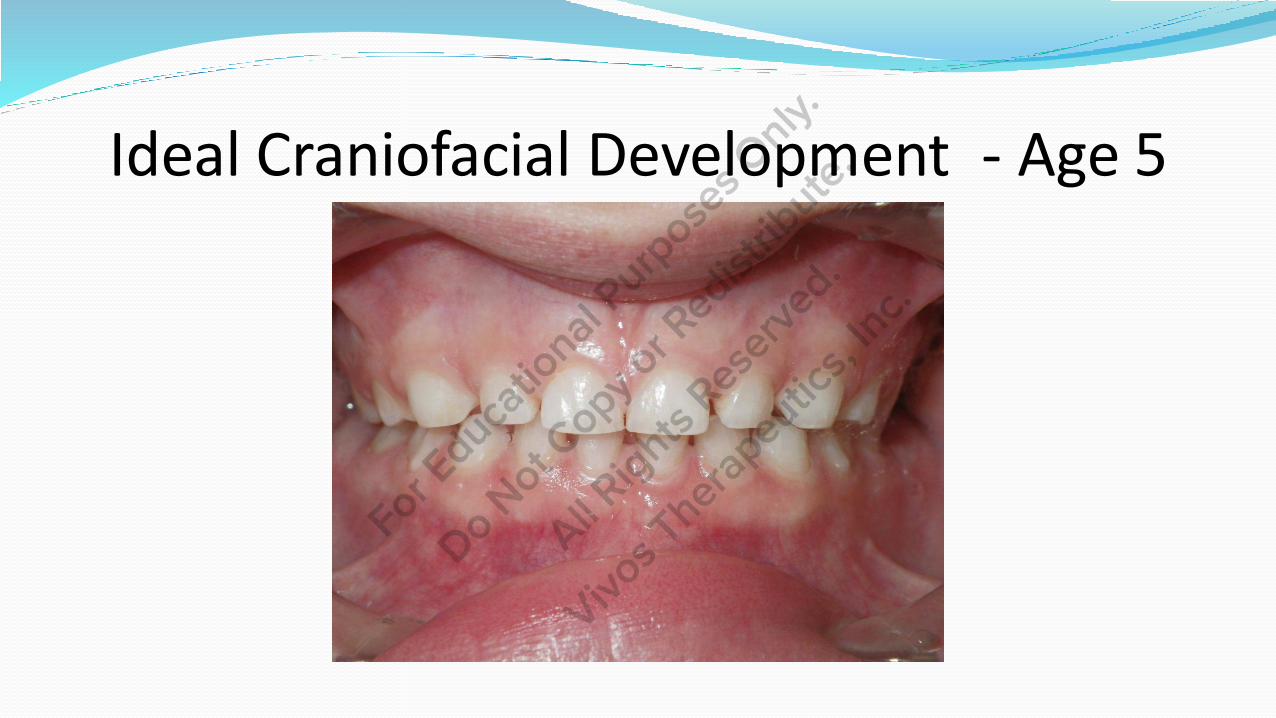
Ideal Craniofacial Development – Age 5
1. A significant space between all primary teeth2. A full view of the lower teeth when closed3. Forward growing

Ideal Craniofacial Development – Age 5
23
Ideal Craniofacial Development - Age 5

Ideal Craniofacial Development - Age 5
UNICORN

Ideal Craniofacial Development – Age 12
38mm

Ideal Craniofacial Development – Age 12

Craniofacial Growth & Development
When do we get our maxillary and mandibular growth?

29
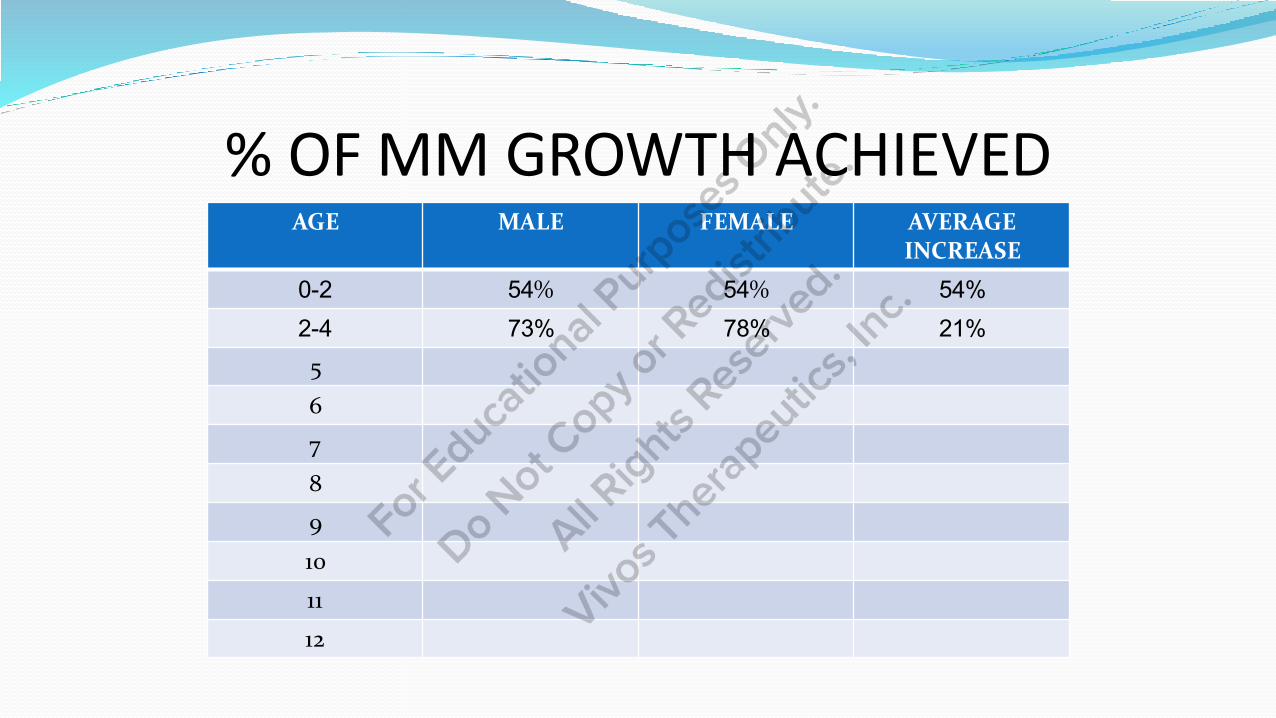
% OF MM GROWTH ACHIEVED AGE MALE FEMALE AVERAGE
INCREASE
0-2 54% 54% 54%2-4 73% 78% 21%5
6
7
8
9
10
11
12

% OF MM GROWTH ACHIEVED AGE MALE FEMALE AVERAGE
INCREASE
0-2 54% 54% 54%2-4 73% 78% 21%5 76% 81% 3%6 79% 84% 3%7 81% 85% 2%8 83% 87% 2%9 84% 89% 2%10 86% 91% 2%11 88% 93% 2%12 89% 94% 1%

Craniofacial Deficiency
Next question…
Why are the maxilla and mandible underdeveloped?

Anthropology Research
Four researchers: Dr. James Sim Wallace
Dr. Westin A. Price
Dr. Robert Corruccini
Dr. Jerome Rose

What do we tell parents when we see crowded/tight primary teeth?
35
“An early SOFT DIET prevents the development of the
muscle fibers of the TONGUE resulting in a WEAKER
TONGUE which can not drive the primary dentition out
into a spaced relationship with fully developed ARCHES
which will lead to more crowding of the permanent
teeth.”
JAMES SIM WALLACE, DDS - 1900’s

WESTON A. PRICE, DDS BORN IN 1870 RESEARCH DONE DURING THE EARLY 1900’S
10 YEAR PERIOD OF TRAVEL
14 COUNTRIES
100’S OF CITIES
LOOKING FOR SECRETS OF HEALTHY PEOPLES
STUDIED ISOLATED, PRIMITIVE GROUPS LIVING ON INDIGENOUS FOODS
ESKIMOS, NATIVE AMERICANS, AFRICAN TRIBES, AUSTRALIAN ABORIGINALS, POLYNESIANS ETC.

THE PEOPLE HE OBSERVED… DISPLAYED PHYSICAL EXCELLENCE
HAD PERFECT JAWS AND TEETH
EMOTIONAL STABILITY
NO ALLERGIES
COMMONALITIES BREASTFEEDING FOLLOWED BY A GRITTY, HARD DIET AT AN EARLY
AGE
NATURAL FOODS FROM SEA, PLANT AND MEAT
MOSTLY A RAW DIET WITH LITTLE COOKING OF THE FOOD
MEATS ARE DRIED AND CURED, SOME SALT
NO SUGAR, NO PRESERVATIVES, NO CHEMICALS,
NO CANNED OR PROCESSED FOODS
CHANGES OCCUR ONCE ISOLATION IS BROKEN

ESKIMOS DISPLAYED PERFECT OCCLUSION WITH EXCELLENT MAXILLARY
WIDTH
AFTER CONTACT WITH INDUSTRIALIZED SOCIETIES – A SHIFT TOSOFT FOODS AND REFINED SUGARS
MALOCCLUSION RATES ROSE TO OVER…
50% IN THE FIRST GENERATION!
WESTON A. PRICE, DDS All documented is his book
Nutrition and Physical Degeneration

Dr. Robert S. Corruccini

He wrote the book…

Mentor, Colleague, Friend…

Dr. Robert S. Corruccini ANTHROPOLOGIST
30+ YEARS OF RESEARCH
7 BOOKS
HUNDRES OF JOURNAL ARTICLES
FOSSIL STUDIES
POPULATION STUDIES
ANIMAL TESTING

PRIOR TO 400 YEARS AGO…

LITTLE TO NO EVIDENCE OF MALOCCLUSION

POPULATION STUDIES DR. CORRUCCINI TRAVELED THE WORLD
STUDIED ISOLATED RURAL PEOPLES
BREASTFEEDING
ALL HAD A HARD DIET
LITTLE TO NO INCIDENCE OF MALOCCLUSION OR OTHER DEGENERATIVE DISEASES
LITTLE TO NO VARIATION
ALSO STUDIED SEVERAL POPULATIONS AS THEY BECAME EXPOSED TO WESTERN CULTURES
ANIMAL STUDIES DECADES WORTH OF HARD-SOFT DIET STUDIES
RESULTS ALWAYS THE SAME:
SOFT-DIET ANIMALS
SMALLER BODY MASS
LESS DENSE BONE
SMALLER, WEAKER ORAL MUSCULATURE
NARROWER MAXILLA
SMALLER MANDIBLE
THINNER ALVEOLUS
SMALLER CONDYLES

BROKEN ISOLATION MALOCCLUSION SHOWS UP IN THE FIRST
GENERATION AFTER EXPOSURE TO PREPARED, PROCESSED AND PRESERVED FOODS
50%
MALOCCLUSION RATES RISE DRAMATICALLY INTO THE SECOND GENERATION
70%
AND THIRD GENERATION
85%
AND FOURTH GENERATION
>90%
VARIATION ALSO INCREASES

CONCLUSIONS BREASTFEEDING RESULTS IN PROPER TRAINING AND
DEVELOPMENT OF THE TONGUE
THEN THE EARLY HARD DIET CONTINUES THE PROCESS
WHEN THE TONGUE POSTURES, SWALLOWS AND SPEAKS PROPERLY, WEGET IDEAL GROWTH
MOST MALOCCLUSIONS ARE ACQUIRED, NOT INHERITED
MALOCCLUSION IS A DISEASE OF WESTERN SOCIETY

DR. CORRUCCINI “DIETARY CONSISTENCY AND TOUGHNESS PROMOTE PROPER
BONE GROWTH AND PROPER PERMANENT TOOTH ERUPTION, BRINGING ABOUT IDEAL OCCLUSION; WHEN NONRESISTANT PROCESSED FOODS BECOME UBIQUITOUS AFTER INDUSTRIALIZATION, AND THE ERUPTION AND CUSPAL COORDINATION OF TEETH LOSE THE CRITICAL PATHFINDER INFLUENCE OF VIGOROUS MASTICATORY PRESSURES, MALOCCLUSION SHOWS A RAPID RISE.” from: How Anthropology Informs the Orthodontic Diagnosis of Malocclusion’s Causes
Dr. Scott Bolding, Dr. Jerome Rose, Me

Dr. Jerome Rose
“95% of all malocclusions are acquired. Genetics play a role in only 5% of malocclusions. This is indisputable.”

Breastfeeding Trends in the USA The current rate is 70%
Drops to 50% at 6 months – partial/pumping
Bottle feeding/jar or blended food is different(soft)
Results:
Tongue is not trained properly – poor function
Tongue musculature is weaker – poor growth
Child misses the optimal growth and development of the maxilla and mandible during the first 2 years of life

56
Graduates ‘Puffs’. The nutritious snack that melts in baby’s mouth.
A BETTER CHOICE…
57


Craniofacial Deficiency Next question…
WHAT ARE THE RESULTS OF HAVING AN UNDERDEVELOPED MAXILLA AND MANDIBLE?
WE NEED TO LOOK AT OUR ANATOMY FOR THE ANSWERS.

MAXILLA

61
AIRWAY ANATOMY

Airway Anatomy
THE UNDERDEVELOPED MAXILLA AND MANDIBLE RESULT IN A CHILD WITH A
COMPROMISED…
AIRWAY

AGE 10 - AIRWAY
63

AGE 10 – AIRWAY?
64

CLASS I COMPARISON
AGE 10 AGE 10
Genetics
Twin Studies





COMPARE

12 MONTHS LATER

12 MONTHS LATER

12 MONTHS LATER

Airway Anatomy
Our airway anatomy is directly related to our craniofacial growth anddevelopment
The more ideal the craniofacial growth and development, the larger theairway space
Craniofacial deficiency includes airway compromise/deficiency
Airway compromise/deficiency results in compensation

NASAL BREATHING VS.
MOUTH BREATHING

77
DR. EGIL HARVOLD
• Director – Center for Craniofacial Anomalies –UCSF
• Research – Primate Center – UC – Davis• Rhesus monkeys• Blocked monkey’s noses with cotton rolls• Conducted airway studies• Nasal obstruction > mouth breathing >
lower tongue posture > malocclusion

Dr. Sten Linder-Aronson Dr. Sten Linder-Aronson – children
Research focus was the difference between nasalbreathing kids and mouth breathing kids
Same results – mouth breathers developdifferently
MOUTH BREATHING + POOR TONGUEPOSITION/FUNCTION = HIGH RATES OFMALOCCLUSION

FUNCTIONS OF THE NASAL CAVITY FILTER
HUMIDIFY
WARM
ACCELERATE
One Purpose:
Prepare the air for the lungs

PROPER NASAL BREATHING LIPS TOGETHER AND AT REST
TONGUE AT THE ROOF OF THE MOUTH
INVISIBLE
SILENT
NO MOVEMENT OF LIPS AND CHEEKS DURING SUBCONSCIOUS SWALLOW
END RESULT: NON-RESISTANT AIRFLOW

NASAL BREATHING DIAPHRAGMATIC BREATHING FILLS THE LUNGS WITH IDEAL AIR
LEADS TO OPTIMAL CO2, O2, NO BALANCE
END RESULT: A PROPERLY OXYGENATED, WELL BALANCED,HEALTHY CHILD
The perfect person breathes as if they do not breathe.
Sixth century B.C. philosopher
Lao Tzu
82
MOUTH BREATHERS DEVELOP POORLY


MOUTH BREATHERS INCREASE IN UPPER RESPIRATORY INFECTIONS
INCREASE IN ENT INFECTIONS
INCREASE IN ASTHMA
WHY?

MOUTH BREATHING COMPENSATION
OVERBREATHING, AKA HYPERVENTIALTING
DECREASED CO2 – CHEST BREATHING
DOES NOT FILL THE LUNGS WITH IDEAL AIR
IMBALANCE IN CO2, O2, NO
END RESULT: A POORLY OXYGENATED, IMBALANCED, ANDUNHEALTHY CHILD

MOUTH BREATHING
VENOUS POOLING
CO2 HAS A VASODILATORY EFFECT
MOUTH BREATHING REDUCES BLOOD CO2
INFERIOR ORBITAL VEIN CONSTRICTS
THE RESULT IS VENOUS POOLING
ALSO
NASAL BREATHING RELEASES NITRIC OXIDE FROM THE PARANASAL SINUSES
MOUTH BREATHERS REDUCE BLOOD NO
INFERIOR ORBITAL VEIN CONSTRICTS
THE RESULT IS VENOUS POOLING and…
87
MOUTH BREATHERS INCREASE IN UPPER RESPIRATORY INFECTIONS
INCREASE IN ENT INFECTIONS
INCREASE IN ASTHMA
WHY?
The decrease in NO
NO is antibacterial, antiviral and antifungal

Connecting the Dots…
“Mouth breathing has been linked to oral conditions such as craniofacial deformity, malocclusion and obstructive sleep apnea.”
García Triana, B., Hibatulla Ali, A., & Grau León, I. (2016). Mouth breathing and its relationship to some oral and medical conditions: physiopathological mechanisms involved. Revista Habanera De Ciencias MéDicas, 15(2).
Recuperadode

Connecting the Dots… “A narrow maxilla with high arched palate characterizes a phenotype of patients
with obstructive sleep apnea. This is associated with increased nasal airflow resistance and posterior displacement of the tongue.”
Johal A, Conaghan C. Maxillary morphology in obstructive sleep apnea: a cephalometric and model study. Angle Orthod. 2004;74:648-656.
Abdullantif J, Certal V, Zaghi S, et al. Maxillary expansion and maxillomandibular expansion for adult OSA: a systematic review and meta-analysis. J Craniomaxillofac Surg. 2016;44:574-578
90

Connecting the Dots… “Snoring is associated with straight profiles, V-shaped palatal morphology,
increased neck circumference, decreased upper arch length, and decreasedinter-first upper premolar distance.”
Al-Madani GH, Banabihl SM, El-Sakhawy MM. Prevalence of snoring and facial profile type, malocclusion class and dental archmorphology among snorer and nonsnorer university population. J Orthodont Sci 2015;4:108-12.
91

CONNECTING THE DOTS… “Patients with OSA had significantly narrower maxillary and mandibular arch
widths when compared to control groups. These findings support the notionthat a narrow maxilla or mandible may lead to airway obstruction because of
inadequate space for the tongue. Thus when the space in the oral cavity is inadequate, it is possible that a normal sized tongue can gravitate to the back of
the oro-pharynx.”
Banabilh SM, Suzina AH, et al. Dental arch morphology in south-east Asian adults withobstructive sleep apnoea: geometric morphometrics. Journal of Oral Rehabilitation 2009;36:184-
192.
92

ADENOIDS AND TONSILS
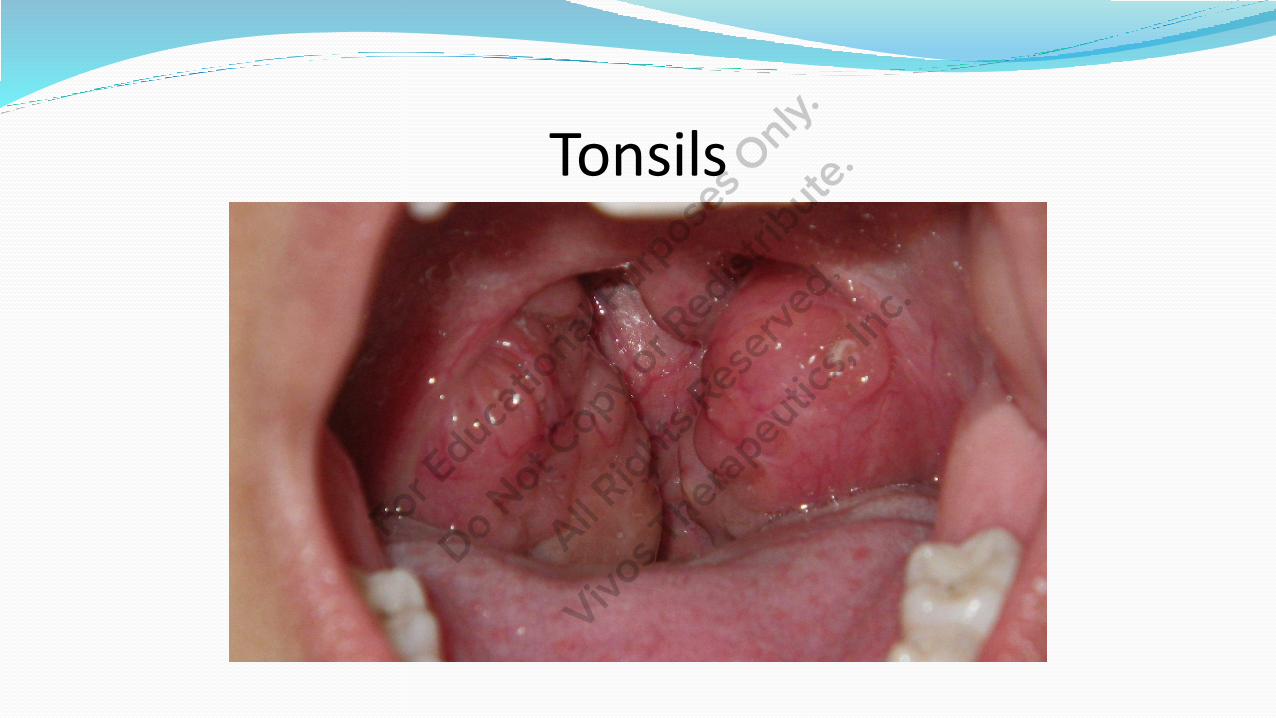
Tonsils
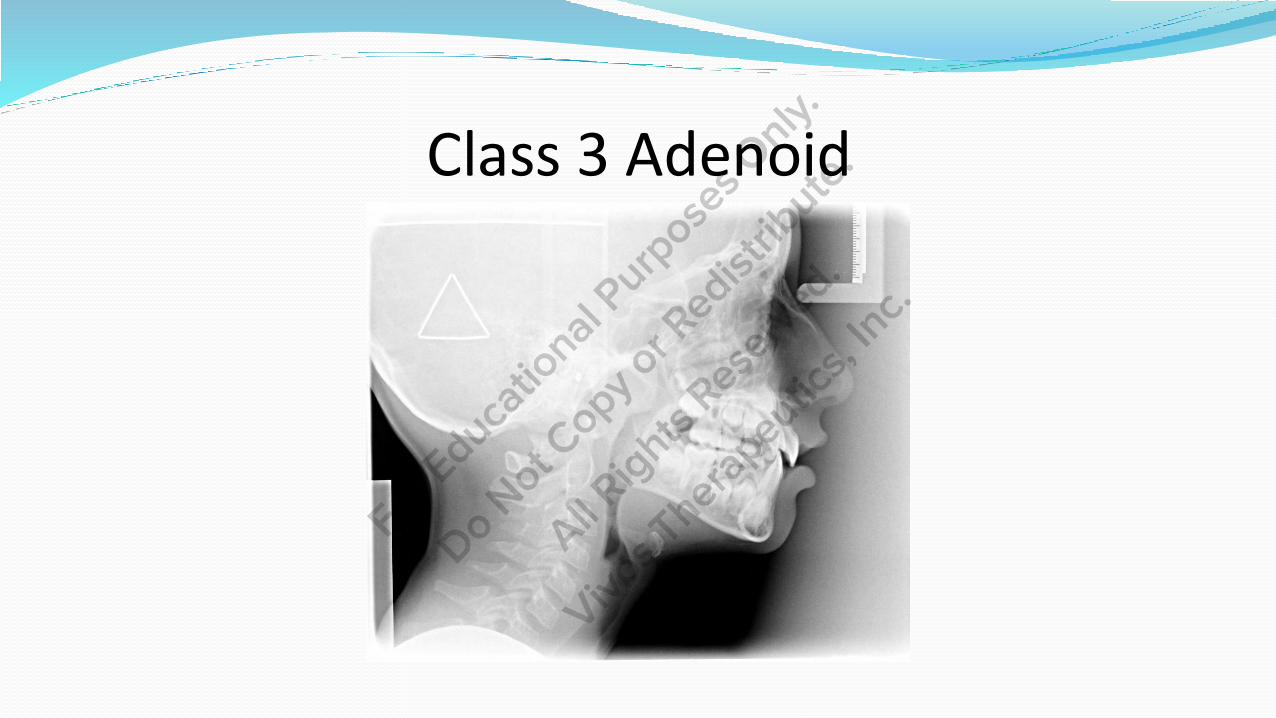
Class 3 Adenoid
Dr. Christian Guillemenault Stanford University
Childhood Sleep Disordered Breathing Research
Tonsil & Adenoid removal research
Unsuccessful 9-12 months post removal
Mouth vs. Nose
Conclusion: Nose breathing is the ultimate outcome
Connecting the Dots… In 98% of patients with OSAS, the condition is due to abnormal
anatomical features of the soft tissues and/or the structures of themaxillomandibular skeleton that cause a “disproportionate anatomy” of the airway,4,5 and in only 2% of adult patients is the condition due
to a space-occupying lesion, such as adenoidal, tonsillar or uvula hypertrophy, in which case resection would be curative.
Barceló X, Mirapeix RM, Bugés J, Cobos A, Domingo C. Oropharyngeal Examination to Predict Sleep ApneaSeverity. Arch Otolaryngol Head Neck Surg. 2011;137(10):990–996. doi:10.1001/archoto.2011.176
97

SLEEP DISORDERED BREATHING

99
SLEEP DISORDERED BREATHING (SDB)
Karen Bonuck, PhD.
Published research in 2012 that followed 11,000 kids for 6 years
Objective
Examine statistical effects of SDB symptom trajectories from 6 months to 7 years on subsequent behavior.
Youtube -Dr. Karen Bonuck Sleep Disordered Breathing Children

Results of Dr. Bonucks Research “A STRONG AND PERSISTENT ASSOCIATION BETWEEN
SLEEP DISORDERED BREATHING AND DIMINISHED IQ”
SLEEP DISORDERED BREATHING INCREASED THE RISKOF ADD/ADHD BY 50%
SLEEP DISORDERED BREATHING KIDS WERE 40-100%MORE LIKELY TO HAVE NEURO-BEHAVIORAL ISSUES

SDB/OSA ASSOCIATED WITH
INCREASED FACE HEIGHT
DECREASED NOSE PROMINENCE
DECREASED NOSE WIDTH
RETROGNATHIC MANDIBLE
THIS IS THE FACE OF SDB/OSA

SDB/OSA ASSOCIATED WITH NARROW ARCHES
HIGH VAULT
ELONGATED SOFT PALATE
RETROGNATHIC MAXILLA
RETRUDED MANDIBLE
THIS IS THE ORAL CAVITY OF SDB/OSA

“Hi, my name is Olaf and I like warm hugs.”
“I also wear a CPAP to bed. Can I get some nostrils?”

SLEEP DISORDERED BREATHING• Mouth breathing - Snoring - UARS - OSA
• Increased nasal airflow resistance
• Sympathetic Nervous System activation
• Altered biochemistry and physiology during sleep
• End result: sleep fragmentation or disruption of the reparative sleep
cycle delivers an unhealthy child who will grow up to be an unhealthy
adult

TONGUE TIE

Ankyloglossis
AKA – tongue-tie
Abnormal shortness of the lingual frenum causing limited movement of the tongue

TONGUE TIE RELATED TO DEVELOPMENT
“Restricted tongue mobility was associated with narrowing of themaxillary arch and elongation of the soft palate. These findings suggestthat variations in tongue mobility may affect maxillofacial development.”
Yoon AJ, Zaghi S, Ha S, Law CS, GuilleminaultC, Liu SY. Ankyloglosisas a risk factor for maxillary hypoplasia and soft palate elongation: A functional-morphological study. Orthod Craniofac Res.
2017;00:1-8.

ONE STEP FURTHER…
“Soft palate length is significantly greater in OSA patients and it is wellestablished that increased soft palate length is a prominent risk factor forupper airway collapsibility.”
Shigeta Y, Ogawa T, Tomoko I, Clark GT, Enciso R. Soft palate length and upper airway relationship in OSA and non-OSA subjects. Sleep Breath. 2010;14:353-358.
Sforza E, Bacon W, Weiss T, Thibault A,Petiau C, Krieger J. Upper airway collapsibility and cephalometric variables in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2000;161:347-352.
TIE it all together… “Children with untreated short frenulum developed abnormal tongue
function early in life with secondary impact on orofacial growth and sleep disordered breathing(SDB).”
“Short lingual frenulum may lead to abnormal orofacial growth early in life, a risk factor for development of SDB.”
Huang YS, Quo S, Berkowski JA, Guilleminault C (2015) Short Lingual Frenulum and Obstructive Sleep Apnea in Children. Int J Pediatr Res 1:003

PACIFIERS






Worth a Thousand Words?

NON-NUTRITIVE SUCKING
PACIFIER
FINGERS
SIPPY CUPS
STRAWS
119

NON-NUTRITIVE SUCKING FORM FOLLOWS FUNCTION
TONGUE
FACIAL MUSCLES
RESULTS OF NON-NUTRITIVE SUCKING
IMPROPER ARCH FORM
IMPROPER ARCH WIDTH
NARROW AND HIGH VAULTED PALATE
I.E. UNDERDEVELOPMENT
I.E. AIRWAY COMPROMISE
Behavior
Patient 3







Cognitive Development
Referred by pediatrician
Thumb habit
Struggling
Patient 4










Summary
The early soft diet results in muscle weakness and dysfunction
The soft tissue weakness and dysfunction results in underdevelopment
Craniofacial deficiency includes airway deficiency/compromise
Airway compromise leads to sleep disordered breathing
SDB results in sleep fragmentation
Ultimately compensatory breathing and sleep fragmentation deliverunhealthy children who struggle with a long symptom list
An unhealthy child grows up to be an unhealthy adult
Better to treat the craniofacial deficiency early

“It is evident that the next great step in medical progress in the line of preventive medicine should be made by the dentists.
The question is will they do it?”
Dr. Charles H. Mayo, M.D. (1865-1939)

THANK YOU!