



Organizing pneumonia
47
ORGANIZING PNEUMONIA BRONCHIOLITIS OBLITERANS ORGANISING PNEUMONIA Presented by Dr. Mohamed A/Aziz Omer Mustafa Consultant chest physician MD Respiratory medicine SMSB
-
Upload
amr-eldakroury -
Category
Health & Medicine
-
view
109 -
download
4
Transcript of Organizing pneumonia

ORGANIZING PNEUMONIA
BRONCHIOLITIS OBLITERANS ORGANISING PNEUMONIA
Presented by
Dr. Mohamed A/Aziz Omer Mustafa
Consultant chest physician
MD Re spirato ry me dicineSMSB

Idiopathic
BRONCHIOLITIS OBLITERANS ORGANISING PNEUMONIA (BOOP)
CRYPTOGENIC ORGANISING PNEUMONIA (COP)
SECONDRY ORGANIZING PNEUMONIA (SOP)
Terms
• Bronchiolitis
Bronchiolitis obliterans (BO)
Obliterative bronchiolitis (OB)
Constrictive bronchiolitis(CB)
• Bronchiolitis obliterans syndrome (BOS)
• Pneumonia
• Organizing pneumonia
• Idiopathic interstitial pneumonia ( diffuse alveolar damage)
Bronchiolitis
• Is an inflammatory reaction that follows damage to the bronchiolar epithelium of the small conducting airways
Subsequent healing leads to excessive proliferation of granulation tissue within the airway walls , lumen or both.
Depending on disease stage the repair process may cause narrowing and distortion of the small airway (constrictive bronchiolitis ) or complete obliteration ( bronchiolitis obliterans)

BRONCHIOLITIS OBLITERANS
• Rare form of non-reversible Obstructive lung disease
• Scarring
• Polyploidy obliteration of the lumen of the bronchioles without involving of the distal lung parenchyma.
• Infants - adenovirus
BRONCHIOLITIS OBLITERANS
• Rare form of non-reversible Obstructive lung disease
• Scarring
• Polyploidy obliteration of the lumen of the bronchioles without involving of the distal lung parenchyma.
• Infants - adenovirus
BRONCHIOLITIS OBLITERANSSYMPTOMS & SIGNS
• Dry cough
• SOB
• WHEEZES
• FEV1 16-21%
• Desaturation

BRONCHIOLITIS OBLITERANSCAUSES
• Viruses
• Collagen vascular diseases
• Transplant rejection
• Stevens-Jonson's syndrome
• Pneumocystis Juversi pneumonia
• Drug reaction
• Aspiration
• Bronchopulmonary dysplasia-prematurity
• Toxic fumes

BOS
a distinct clinical entity
occurring in the transplanted lung
involves the small airways primarily
should not be confused with BO or BOOP
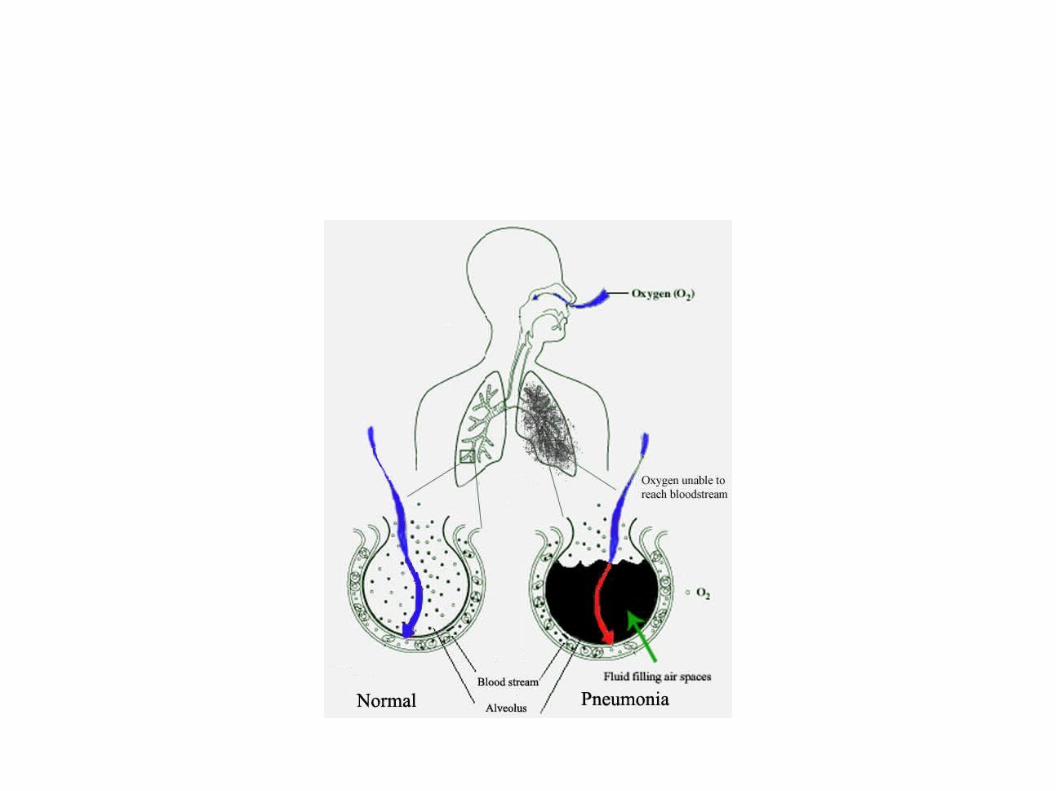
PNEUMONIA - PNEUMONITIS
• Inflammatory condition of the lung affecting primarily the microscopic airspaces known as alveoli .
• Congestion , hepatization , resolution
• …. Viruses , bacteria ,fungi , parasites
• > 100 strains identified
• Mixed infection 45% children : 15% adults
• Isolation of causative agent 50% despite careful testing

Pneumonitis
• Certain drugs
• Chemical burns
• Autoimmune diseases
• Radiation
• Thermal injuries
HISTORY• HIPPOCRATES 460-370 BC
• 12 November world pneumonia day
• 450 million /year
• 4 million deaths /year
• 7% world’s total deaths
• Greatest < 5 >75 yrs
• 8th leading death in the states 2009
PNEUMONIA IMAGING
• CXR does not always match the severity of pneumonia
• Not reliably separate between bacterial infection and viral infection
• CXR typically clear within one month

Pneumonic patch
Interstitial lung disease
• Is a class of diffuse lung diseases .
• It is a common pathological response of the lung to a wide variety of known & unknown cause .
• It is often referred to interstitial pneumonia , IP or interstitial lung disease ILD
• Until 1960 IPF remained largely a clinical diagnosis considered as a single entity
• Has been felt to be a terminal disease with poor prognosis
because of lack of response to immunosuppressive therapy only 30% respond
• only 30% histopathology done

ILD
Several acute and chronic lung disorders with variable degrees of pulmonary fibrosis ,variable degree of disease progression & variable response to treatment.
Retrospective review of clinical & histopathology data allows IPF to be classified into distinct subsets that differ in clinical course , prognosis & response to treatment .

ILD
• NSIP , LIP , DIP ,RBI lung disease , UIP , OP
• In some ILDs , the small airways- the respiratory and terminal bronchioles- are primarily affected .
respiratory bronchiolitis-associated interstitial lung disease (RBILD)
idiopathic , smoking related in contrast to BO .

Known factors or insults lead toInterstitial lung disease
• Drugs : antineoplastic (bleomycin , methotrexate )
: antimicrobial (nitrofrantoin , penicillin )
:amidorone
: hydroclorothiazide
• Hypersensitivity pneumonia
Farmer’s lung , pigeon breeder’s lung
. Dusts:
Asbestos , silica
Viral agents … mycoplasma pneumonia
. CD
ILD
.
It is important to differentiate terms used to define clinical entities and terms describing the pathologic lesions of these disorders .
Clinical syndromes IPF,CFA ,idiopathic BOOP,COP,BO,BOS ,Hamman-Rich syndrome .
Pathological:UIP , LIP , giant cell interstitial pneumonitis , diffuse alveolar damage, non classifiable interstitial pneumonia , BOOP .

D\DILD
• Clinical setting:-
• First: requires consideration of a variety of other pathological processes that mimic the interstitial disorders in appropriate clinical setting
• Second: Physician should be aware of at least 150 other clinical entities & situations associated with ILD
• Third: Owing the broad D\D & the availability of various evolving invasive & non-invasive diagnostic techniques, the best approach to use is to establish a specific diagnosis which is frequently difficult to determine
• Fourth: In a significant proportion of patients a conclusive cause can't be ascertained even when the most invasive diagnostic pathways are taken.
• Finally , even when a specific diagnosis is made, an effective therapeutic regimen is not available for many patients with ILD
????????BOOP
Bronchiolitis obliterans organizing pneumonia
Is a type of diffuse INTERSTITIAL LUNG DISEASE that affects the distal bronchioles , respiratory bronchioles , alveolar ducts and alveolar wall.
Type of lung injury and repair
Failure of resolution of acute pneumonia
The primary area of injury is within the alveolar wall.

BOOP Hx
• As a distinct clinical entity 1st described by Davison in 1983
• Gary Epler 1985 gave the name BOOP
• Inflammation of the bronchioles & surrounding tissue in the lung.
• Non infectious- infectious
• Complication of an existing chronic inflammatory disease such as RA
• Side effect of certain medication such as amidarone
• M\F 1:1
• Age 50-60 \ 20-80
• No relation to smoking

Organizing pneumonia
• Refers to unresolved pneumonia in which alveolar exudates persists & eventually undergo fibrosis .
. presence of buds of granulation tissue progressing from fibrin exudates to loose collagen containing fibroblast.
Accessory finding in other inflammatory diseases such as vasculitis
. It may also be a feature of organizing stage of ARDS
• A complication of an existing chronic inflammatory disease
or a side effect of certain medication .
• organizing Pneumonia of determined causes
• organizing Pneumonia of unknown cause occurring in a specific context causes
• Cryptogenic organizing pneumonia
Undetermined causes of organizing Pneumonia
• RA , Sjorgen syndrome---------- SLE ,SS
• Sweet”s disease
• HCV thyroiditis
• Crhons disease…..UC
• Behcets”s …. Wegener”s granulomatosis ….PN
• Polymyalgia Rheumatica
• Myelodysplasia
• Leukemia ….. Cancer
• Mesangiocapillary GN
• Chronic rejection …. Graft versus host disease
Determined causes of organizing Pneumonia
• Infection
• Drugs
• Radiation
• It was long been known that radiation may induce radiation pneumonitis
• However a syndrome similar to COP has been identified recently
• It differs strikingly from usual radiation pneumonitis in that the pulmonary infiltrate occur or migrate outside the radiation fields add respond good to steroids.
• Interestingly, unilateral breast irradiation, whether or not it results in pneumonitis , has been shown to induce bilateral lymphocytic alveolitis with activated CD4+Tcells

Infectious causes of organising pneumonia
• Bacteria Chlamydia pneumoniae
Coxiella burnetii
Legionella pneumophila
Mycoplasma pneumoniae
Nocardia asteroides
Pseudomonas aeruginosa
Serratia marcescens
Staphylococcus aureus
Streptococcus group B (newborn treated by extracorporeal oxygenation)
Streptococcus pneumoniae
Infectious causes of organising pneumoniacont…..
• Viruses Herpes virus
Human immunodeficiency virus
Influenza virus
Parainfluenza virus
• Parasites Plasmodium vivax
• Fungi Cryptococcus neoformans
Penicillium janthinellum
Pneumocystis carinii (in AIDS )
Clinical approach
• Medical Hx , environmental factors, occupational exposures, medication & drug usage, FH
• Age , smoking, sex
• Onset & Duration of symptoms
• Rate of disease progression
• Extra pulmonary symptoms

Clinical approach …cont.
• Acquired immunodeficiency & transplant
• Diffuse neoplasia
• CHF
• Pulmonary vascular disorder
• CBC, ESR, LFT, electrolytes, RFT

BOOP diagnosis
• Diagnosis is suspected after no response to multiple antibiotics & blood & sputum cultures are –ve for organisms
. Clinical picture & radiological images resemble infectious pneumonia
• CXR similar to an extensive pneumonia wide spread white patches
small nodular opacities 50% & large nodules in 15%
• Preservation of normal lung volume
• Migrate
• Persists or progresses

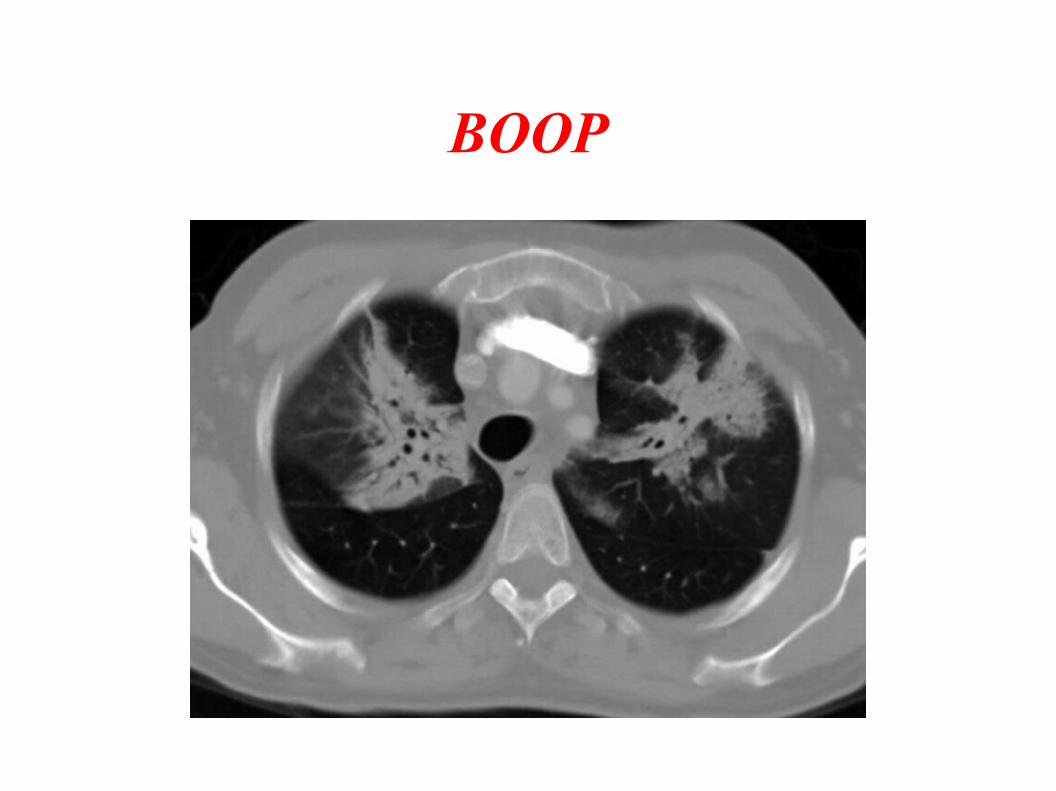
BOOP – CT
• CT may be used to confirm the diagnosis ( findings are typical enough to allow the doctor to make the diagnosis without ordering additional tests)
• …airspace consolidation with airbronchogram , lower zone predominance , sub pleural or peribronchial distribution 50%.
• Ground glass appearance in most pt , honeycombing in some
• Diffuse bilateral infiltratation
• as a solitary focal lesion associated usually with subacute or chronic inflammatory illness, it occurs in the upper lobes and may cavitate.
• .

BOOP - histopathology• Confirmation
• Broncoscopic biopsy !
• VATS
• Histology: presence of polyploidy plugs of loose organizing connective tissue
( Masson bodies ) within the alveolar ducts , alveoli , bronchioles .
• Intraluminal polyps in respiratory bronchioles , alveolar ducts , alveolar spaces .
• Accompanied by organizing pneumonia in the more distant parenchyma ( proliferative bronchitis)

Diagnosis of exclusion• COP is a diagnosis of exclusion .
• Once confirmation done , physician has to rule out :-
Chronic esinophilic pneumonia
Hypersensitivity pneumonia
Bacterial …. Viral
CD
Drug reaction

TREATMENT
• Spontaneous
• Macroloids
• Steroids
• Cytotoxic drugs
• Transforming growth factor , pirfenidone
BOOP
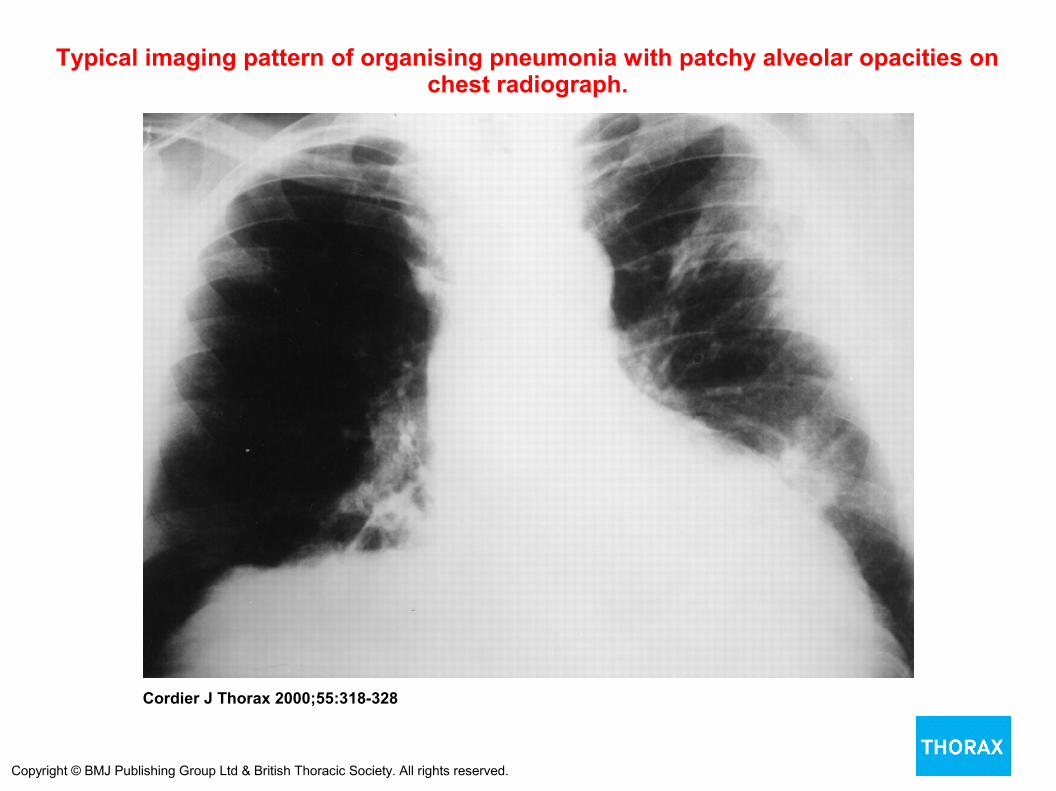
Typical imaging pattern of organising pneumonia with patchy alveolar opacities on chest radiograph.
Cordier J Thorax 2000;55:318-328
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.




THANK YOU








![Organizing pneumonia in mice and men - Home - Springer · 2017-08-29 · Organizing pneumonia in mice and men ... cause [2] and (2) secondary organizing pneumonia (SOP), based on](https://static.fdocuments.us/doc/165x107/5e2d47a8a9bbe92dcc272487/organizing-pneumonia-in-mice-and-men-home-springer-2017-08-29-organizing-pneumonia.jpg)









