Organ Transplantation: Ethical, Legal and Psychosocial ... · W. Weimar, M. A. Bos, J. J. V....
21
W. Weimar, M. A. Bos, J. J. V. Busschbach (Eds.) Organ Transplantation: Ethical, Legal and Psychosocial Aspects. Global Issues, Local Solutions P ABST
Transcript of Organ Transplantation: Ethical, Legal and Psychosocial ... · W. Weimar, M. A. Bos, J. J. V....

W. Weimar, M. A. Bos, J. J. V. Busschbach (Eds.)
Organ Transplantation: Ethical, Legal and Psychosocial Aspects.
Global Issues, Local Solutions
PABST


W. Weimar, M. A. Bos, J. J. V. Busschbach (Eds.)
Organ Transplantation: Ethical, Legal and Psychosocial
Aspects, Vol. IIIGlobal Issues, Local Solutions
Pabst science PublishersLengerich

Bibliographic information published by Die Deutsche NationalbibliothekDie Deutsche Nationalbibliothek lists this publication in the Deutsche Nationalbibliografie;detailed bibliographic data is available in the Internet at <http://dnb.ddb.de>.
This work is subject to copyright. All rights are reserved, whether the whole or part of the mate-rial is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in other ways, and storage in data banks. The use of registered names, trademarks, etc. in this publication does not imply, even in the absence of a spe-cific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.
The authors and the publisher of this volume have taken care that the information and recommen-dations contained herein are accurate and compatible with the standards generally accepted at the time of publication. Nevertheless, it is difficult to ensure that all the information given is entirely accurate for all circumstances. The publisher disclaims any liability, loss, or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents of this volume.
© 2014 Pabst Science Publishers · D-49525 Lengerich Internet: www.pabst-publishers.de, www.pabst-science-publishers.com E-mail: [email protected]
Print: ISBN 978-3-89967-931-1 eBook: ISBN 978-3-89967-932-8
Formatting: µPrinted in Germany by KM-Druck, D-64823 Gross-Umstadt

Contents
1. PrefaceW. Weimar . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2. Global Issues, Local Solutions/Global Outreach
Personal rights and the acquisition of organsTimothy M. Wilkinson . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Organ donation and transplantation in emerging economiesS. A. Anwar Naqvi, Mirza Naqi Zafar & S. Adibul Hasan Rizvi . . . . . . . . . . . . . . . . . . . . . . . . . 17
The Declaration of Istanbul on organ trafficking and transplant tourism: the first five yearsGabriel M. Danovitch . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
3. Cross-Border Transplants
Success factors to decrease foreign transplants in Colombia, South AmericaNéstor F. Pedraza, Fernando Girón, Alejandro Nino, Jorge E. Rodriguez, Yenny A. Baez . . . . . 33
International norms, local worlds:An ethnographic perspective on organ trafficking in the Israeli contextZvika Orr . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
The new crime of human organ trafficking in Spain. An approach to comparative lawClara Moya Guillem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
4. Increasing Living Donation
Improving cooperation between forensic pathologists and transplant teams in Belarus: A strategy for increasing transplant organs supplyAndrei Famenka . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Improving communication and consent for organ donation among minority ethnic groups: Development and evaluation of a hospital based interventionMyfanwy Morgan, Charlotte Kenten, Jessica Sims, Tim Newton . . . . . . . . . . . . . . . . . . . . . . . . 63
Nudges for organ donation. How do they work?Ana Manzano . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
5

Contents
Inter-institutional collaboration in order to reduce the opposition rate to organ donation in the population Simonetta Nieri, Paolo Maria Geraci, Massimo Abelli, Maurizio Campagnoli, Gianni Lodi, Carla Martinotti, Federica Meloni, Carlo Pellegrini, Elena Ticozzelli, Guido Fontana . . . . . . . . . 79
Consensus – a threat to public engagement Anne Hambro Alnæs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
5. Increasing Deceased Donation
Will the GABOiR data registry help to improve the health and risk stratification in ABO-incompatible living kidney transplantation? Silvia Hils, Marcel Geyer, Albrecht Kramer-Zucker, Przemyslaw Pisarski . . . . . . . . . . . . . . . . . . 93
Increase kidney transplantation. The Irish organ donors, mandatory consent choices era Arwa Nicola Shuhaiber . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
Transplant professionals’ views on the ethical challenges associated with altruistic unbalanced paired kidney exchange Céline Durand, Andrée Duplantie, Marie-Chantal Fortin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
Maximizing ‘0’pportunies for living kidney donation Robert Lam, Linda Wright, Michael Campbell, Olusegun Famure, S. Joseph Kim . . . . . . . . . . . 120
Attitudes towards living organ donation in two Romanian universities Harald Jung, Mihaela Frunză . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130
Living organ donation in Europe: Barriers and opportunities through the stakeholders’ eyes. Results from focus groups in four European countries Assya Pascalev, Yordanka Krastev, Adelina Ilieva . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 138
Ethical challenges in living organ donation Assya Pascalev, Yordanka Krastev, Adelina Ilieva . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
Legal issues in living organ donation in the member states of the EU Leonie L. Lopp . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 160
Reflections on the Israeli legislation on transplantation David M. Wood & David A. Frenkel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
6. Children as Donors and Recipients
The pediatric priority in organ allocation is not necessary and is counterproductive – proposal for an alternative ethical model Jean-Luc Wolff, Michel Carrier, Melanie Masse & Natacha Philippe . . . . . . . . . . . . . . . . . . . . . 177
Gift dynamics and identity construction within the family Karl-Leo Schwering, Isabelle Aujoulat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
6

Contents
7. Psychosocial Care
Health literacy and self-management among kidney transplant patientsLouise Maasdam, Emma K. Massey, Marleen C. de Haan-van Buren, Mirjam Tielen, Judith Kal-van Gestel, Michiel G. H. Betjes, Willem Weimar . . . . . . . . . . . . . . . . . . . . . . . . . . . 191
Pancreatic transplantation in patients with T1DM: a source of traumatic stress?Sue Jackson, Kate Gleeson, R. M. Smith . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197
Compliance to treatment and family support in kidney-pancreas transplantation recipientsSusana M. Bayardo, Silvia R. Groppa, Sung Ho Hyon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206
Psychosocial benefits of upper limb transplantationAdam Chełmoński, Katarzyna Kowal, Jerzy Jabłecki . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215
How can the past experience of donors and recipients inform the psychosocial screening of candidates for living kidney transplantation?Deborah Ummel & Marie Achille . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223
Who has extreme expectations of donation? Exploring the psychological profile of living kidney donorsLotte Timmerman, Mirjam Laging, Willij C. Zuidema, Jan N. M. IJzermans, Michiel G. H. Betjes, Jan J. V. Busschbach, Willem Weimar, Emma K. Massey . . . . . . . . . . . . . 230
Telemedically supported aftercare in living kidney recipients – an innovative project at the transplantation center Freiburg Design and first results of a prospective ongoing studySilvia Hils, Anja Schmid, Dieter Hauschke, Lioudmila Bogatyreva, Przemyslaw Pisarski . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240
Donors and recipients of living donor liver transplantation: How can a metasummary of their experience inform the psychosocial screening?Deborah Ummel & Marie Achille . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 248
8. Autonomy at the End of Life
Exploring organ donation with bereaved relatives, healthcare professional’s experiences in three European countriesBarbara Louise Neades . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257
Non-standard kidneys for transplant: Clinical margins, medical morality, and the lawAntonia J. Cronin & James F. Douglas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264
Rethinking the role of consent in relation to post mortem organ transplantationAusten AP Garwood-Gowers & Janine Moreton. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272
Non-standard resuscitation in refractory cardiac arrest: saving patients’ lives, first and, when not possible, preserving organsIván Ortega-Deballon & E. de la Plaza-Horche. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 279
7

Contents
Organ donation after euthanasia: views of professional community in SloveniaJana Šimenc, Danica Avsec . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284
DCDD: What are we waiting for?Alicia Pérez Blanco & Pablo de Lora . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 290
9. Donor Recruitment, Altruism and Compensation
Should postmortal donation be motivated by altruism?Govert den Hartogh . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
A regulated system of incentives for living donation: a challenge to define and understand the objectionsArthur J. Matas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
10. Anonymity
Ethics and the requirement of anonymity in organ donation: An uneasy and unsettled bondMedard T. Hilhorst . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 311
Contact between living anonymous donors and recipients: ethical issuesLinda Wright & Kyle W. Anstey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 317
11. Hot Topics in Allocation
Is it possible to transplant restored kidneys?Miyako Takagi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Corresponding authors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 333
Index of authors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
8

1. Preface
9
This book presents the proceedings of the third ELPAT congress held in Rotterdam, The Nether-lands, April 20-23, 2013.
ELPAT stands for the Ethical, Legal and Psychosocial Aspects of Transplantation and is part of ESOT, the European Society for Organ Transplantation.
The theme chosen for the third ELPAT congress was ‘Global Issues, Local Solutions’ and we thank the European Commission and The Transplantation Society for making this congress possible.
We were happy to welcome 360 delegates from 52 countries and we were able to accommodate 215 presentations.
Free communications, focus sessions and interactive workshops were organized according to the seven ELPAT working groups: Deceased Donation, Legal Boundaries, Living Donation, Organ Tour-ism, Trade and Trafficking, Children, Psychological Care and Public Issues.
During the congress the ELPAT Public Issues working group launched the first book on ‘Public En-gagement in Organ Donation’ while a special session was organized on the project ‘Living Organ Donation in Europe (EULOD)’, a Coordination Action, funded by the European Commission.
As can be seen from the content of this book all ELPAT topics have been explored and discussed. It is a reflection of the continuous debate on the Ethical, Legal and Psychosocial Aspects of Trans-plantation.
Willem WeimarErasmus MC University Hospital Rotterdam,
The Netherlands

10

2. Global Issues, Local Solutions/ Global Outreach
11

12

Personal rights and the acquisition of organsTimothy M. Wilkinson
University of Auckland, New Zealand
Organs for transplantation are an effective form of treatment for organ failure.1 At least in rich countries, they are also cost-effective. Public providers and private insurers are willing to fund more transplants than there are organs available. The major policy problem for transplantation is a short-age of its raw material, not a shortage of money. Acquiring the organs faces an ethical problem too: organs for transplant come from other people, dead or alive.
Here are some of the familiar ethical problems. When organs are taken from the dead, should the dead have to give consent, or should their families, or both, or neither? (In other words, these are questions about presumed consent and opt-in systems, about the family’s power of veto, and about the conscription of organs.) When organs are taken from living people, who thereby risk physical and psychological harm, who should be allowed to donate – only competent adults with close ties, or also strangers, or people who are on the margins of competence or even incompetent? Under what conditions, if any, should the organs of either the living or the dead be allowed to be bought? Any answers to these questions must take account of the, perhaps competing, interests of the people whose organs they are or were, the interests of their families, the needs of those with organ failure, the interests of the health professionals involved, and the feelings and beliefs of the wider society.
This paper tries to show that the key way to think through the ethical problems is in terms of people’s rights to determine what to do with their own bodies and, in particular, to veto bodily interference. According to this paper:(1) people do have rights over their bodies and these rights extend past their deaths;(2) thinking about what these rights require is the basis for the correct, or at least defensible, an-
swers to many of transplantation’s ethical problems; and(3) while rights may not always be the only basis for the correct answers they are in the case of the
conscription of organs after death.
Consider these three examples, which make a number of points about rights:(1) Suppose a man promises to donate a kidney to his son, and then refuses. With certain further
details, we would be justified in holding this man’s refusal to be morally wrong. Suppose too that society finds his behaviour repugnant. Nonetheless, few would say this man should be forced to submit to the removal of his kidney for transplant into his son.
(2) Suppose a competent woman refuses the removal of a cancerous kidney even though removal is necessary to save her life. It is widely accepted that her kidney may not be removed when she refuses even when it is in her interests to have the kidney removed.
1 A note on references: this paper brings into focus more clearly a theme in my book Ethics and the Acquisition of Organs (Oxford: Clarendon Press, 2011) and that book has all the references anyone could reasonably want for the claims made here. I would like this paper to be pleasantly readable so I have not cluttered it up with notes.
13

Timothy M. Wilkinson
14
(3) Consider some reasons for compulsorily taking the second kidneys of living people to allocate to those with renal failure. The loss to the person of one kidney would likely be outweighed by the gain to the recipient who has no functioning kidney; conscription would reduce the inequality between those with two kidneys and those with none; and conscription would help the worst off, since those with no kidneys are worse off than those with two, and worse off than those with two would be after one is taken off them. Yet virtually no one suggests conscripting so much as blood let alone kidneys. Our body parts may not be conscripted even when con-scription would do more good than harm and have apparently fairer outcomes.
Assuming our intuitions in these cases are right, we can conclude that people have rights and these rights are of considerable weight. In the first case, the right outweighs the needs of the son and society’s feelings of repugnance; in the second, the rights outweigh the woman’s own biological interests; and in the third, the right outweighs the greater needs of others. Rights can thus tell us how to decide between competing goods and claims.
However, while we may accept the intuitive conclusions in these three examples, what more can we learn? The examples are concerned with living people’s rights, so no conclusion can imme-diately be drawn about retrieval from the dead. And the examples involve bodily integrity; they are cases of vetoing retrieval. So no conclusion can immediately be drawn about whether people should be allowed to donate or sell their organs, since disallowing would not infringe upon the integrity of their bodies.
I think people do have rights that extend past their deaths. And I think people’s rights over their bodies go beyond the right to veto retrieval. I think people have rights of `personal sovereignty’ that includes a right to make consensual agreements with other people. Of course, I cannot persuade you in the space I have that we have such rights. What the rest of this paper does is indicate how a rights approach can help with some of the problems of transplantation and also to show why, in the case of organ conscription, thinking about rights is not just a help but essential.
Here is an indication of how a rights approach can help. Take some of the questions about taking organs from living people. Who should be allowed to donate or sell what organs? To what extent should people be allowed to act in ways that other people think likely to be against their interests? If people have rights of personal sovereignty, then a strong initial case is made against using legal coercion to prevent them freely selling their own body parts. The case is not decisive, but that they have rights will help us evaluate the considerations on the other side. For instance, it is sometimes argued that permitting sale is contrary to the value of altruism, but if people have rights to sell, that seems to rule out using legal coercion to uphold altruism.
Consider also the role of the family in retrieval from the dead. Virtually everywhere, the family have a de facto power to veto retrieval no matter how strongly the deceased had wanted to donate, and some people think this power violates the right of the deceased. But even assuming that people have rights past death, the right will not be a right to donate; it will only be a right to offer. A refusal of a clinically unsuitable organ does not infringe on a right. I have elsewhere argued that where the family’s de facto power is the result of a justified wish by transplant professionals to avoid bad publicity, the power does not infringe on the right of the deceased. Whether or not the argument is correct, the point is that we can make progress with this ethical problem by sharpening our thoughts about the rights people have. The sharpening also helps with the choice between opt in and opt out systems of retrieval. Some people think an opt out system is wrong because organs should not be taken without the consent of the deceased. We can evaluate that argument by think-ing through whether it is always the infringement of a right to interfere with a person’s body without

Personal rights and the acquisition of organs
15
that person’s consent. It is not, for instance, in the case of emergency treatment of unconscious patients.
These last few examples involve rights that supposedly extend past death. The challenge is to explain how a right could extend past death or, equivalently, how taking organs after death from a person opposed could infringe on her right given that she no longer exists. In essence, my argu-ment is that one can have interests in the success of one’s goals and their success does not depend only on what happens within one’s own biological life. Events after death can affect one’s interests too. People’s interests in what happens to their bodies are generally of great weight, and should be protected by a right. The interest in what happens to one’s organs is an interest in one’s body and it can be affected by what happens after death, so that interest is protected by a right. However, no one should be persuaded by the argument when it is set out in only a few sentences. All of those claims made are eminently disputable and require a lot of work in ethics and metaphysics to make them persuasive.
As a rule, it is best to avoid difficult foundational work in ethics and metaphysics if we are trying to solve practical problems. We can all agree, for instance, on the importance of informed consent in medicine without worrying about whether we are consequentialists, or Kantians, or virtue ethicists or something else. If different foundations have the same practical answers, why try to decide be-tween the foundations? Many writers on transplantation ethics have followed the generally sensible rule, noting (although with some inaccuracy) how societies respect wills and taking that as the non-foundational basis for following people’s wishes about their organs. In fact, the arguments above, which tried to show that the family veto and opt out systems need not infringe on the rights of the deceased, do not actually presuppose rights past death. They could be taken as arguing that even if the dead have rights, their rights would not be infringed upon. Obviously one could reach the same conclusion if the dead did not have rights at all. So they are cases where (if I am right) we can be helped with transplantation ethics by thinking through rights without having to decide whether anyone has the rights. But not every question can be answered in this non-committal way. The widespread rejection of conscription can only be based on an individual right to veto the retrieval of one’s organ after death and such a right cannot avoid the foundational challenge.
Although, as far as I know, every jurisdiction with a transplant program gives individuals the legal power to veto the retrieval of their organs, some writers say they should not have such a power. According to these writers, dead people do not need the organs while living people with organ failure need them so greatly that organs should be routinely taken even from people who opposed retrieval – in other words, the policy for organ acquisition should be conscription.
Here is one way to see the force of the greatest needs argument for conscription. Suppose a pilot knows his plane will crash and he can only steer it either into the paediatric wing of a hospital or into the mortuary, which at that time contains only dead people. Surely we would think he should steer the plane into the mortuary and we would not change our minds if it turned out that the people in the mortuary had all wanted to be buried intact while no one in the paediatric wing cared about their remains. In other words, when it is a choice between life and respect for posthumous wishes, life should win. By parallel, should we not then conscript organs regardless of the wishes of the dead?
A conscription policy does not follow directly from the crash-into-the-mortuary-conclusion. Per-haps conscription would not actually work to get more organs. But suppose it would. What could be so important about the individual’s power of veto that it should override the needs of potential recipients? One answer is: that individuals have rights over their bodies that extend past their deaths

Timothy M. Wilkinson
16
and these rights override the greater good that would be done if their organs were taken. Remember the earlier cases of rights against organ retrieval. At least for people whose organs could be taken while they were alive, their rights outweighed the greater good that could be done from organ real-location. If people’s rights extend past death, they could be the basis for a veto.
On the avoid-foundational-challenges approach, the argument I favour should be taken as just one potential reason for the individual veto and against conscription. Put another way, the metaphysics is dispensable. But I think the other supposed foundations for the individual veto either (a) do not support the individual veto but something else or (b) are not alternatives to the rights approach or (c) are not strong enough to support the veto against the claims of potential recipients.
Take an argument against conscription built on the needs of surviving family members. Some writ-ers believe conscription to be wrong because it would cause psychological harm to the deceased’s family. But no argument based on the family supports the individual veto in cases where the indi-vidual had no family or where the family want to donate and the individual did not. Nor, I think, are the interests of the deceased’s family strong enough to outweigh the needs of potential recipients especially when these are added to the interests of their families in their health and survival.
Take an argument that says people with strong religious objections should not have their organs taken because of the importance of religious freedom. This is one of those arguments that turns out not to be an alternative to the rights approach as we see when we ask: ‘Whose religious objections rule out retrieval?’ The answer is not just anyone’s. My religious objection to some stranger’s organ donation is simply irrelevant. The point is that religious freedom is at best insufficient until one has established on some other ground who is entitled to control what happens to the body.
Take an argument based on the fears of the living, for instance one that says if conscription were known to occur, living people would be upset and worried. This is one of those arguments simply not up to the job of supporting the individual veto against conscription (as before, assuming con-scription would get more organs than a system with an individual veto). Some people are frightened by the very existence of transplant programs, even ones that scrupulously respect individual wishes, because they believe doctors hasten death to get more organs. Such fears are not good enough reasons to close down the transplant programs. It is more important to treat organ failure than to allay fears. So, if conscription would provide more organs how could it be ruled out just because of any extra fear it creates?
The thesis that individual rights extend past death is not just one basis among several for the rejec-tion of conscription; it is the only defensible basis. But this thesis itself needs foundations to explain how people’s interests can be affected by posthumous events. Even then, it may be argued that posthumous rights are not absolute and the benefits of conscription outweigh respect for the rights. Such an argument deserves careful consideration, more indeed than it usually gets. But, to return to the point of this paper, it provides another example of how debates over transplantation ethics are advanced by thinking through individual rights and their limits.

17
Organ donation and transplantation in emerging economiesS. A. Anwar Naqvi, Mirza Naqi Zafar & S. Adibul Hasan Rizvi
Sindh Institute of Urology and Transplantation, Civil Hospital, Karachi, Pakistan
Abstract
Developing countries with emerging economies have low transplant (< 10 pmp) and still lower deceased donation (DD) rates (< 5 pmp) as compared to countries with developed economies with (> 40 pmp) transplant rate and (> 30 pmp) DD rates respectively. The reason for this dispar-ity is not entirely economic development. Inadequate transplant facilities in government sector hospital, high costs in private centres and inaccessibility due to rural dwelling renders the majority of the population disfranchised from transplantation. Moreover DD rates are low due to a lack of awareness about transplantation in general and brain death in particular, negative interpretation of religious rulings and cultural perspectives concerning the dead body. Organ trade in many coun-tries created mistrust of the professionals and affects transplant negatively. Availability of vendor kidneys reduced altruistic donation and in many countries delayed enactment of transplantation laws. Our institute created a model of community-government partnership to provide free dialysis and transplantation to the disfranchised populations with life long follow-up and medication. This model overcame major hurdles and brought forward living donors and initiated deceased donor program. The way forward in emerging economies is to provide transplantation to those who need it irrespective of cast, color or creed keeping transparency and equity in the forefront.
Introduction
Globally seen transplantation is the preferred treatment for end stage organ failure (ESOF) as it provides high quality life years to patients. Unfortunately, there are still many limitations to ac-cess transplantation, especially in emerging economies, and as a result transplant rates per million population (pmp) vary from 1.0 pmp in Africa to 46.6 pmp in America [1]. These transplantation rates with both living and deceased organ donors also equate with the human development index (HDI), a composite of life expectancy, education and purchasing power parity. High HDI countries have donation rates from > 30 to up to 60 pmp while low HDI countries have < 10 pmp [2]. In this report we highlight the hurdles that stand in the way of establishing viable deceased organ dona-tion and transplant programmes in emerging economies. These include economics, social and cultural issues. Religious impediments, professional attitudes and transplant commercialism are other reasons.
Economic issues
The Global Observatory on organ donation and transplantation has grouped countries accord-ing to transplant rates, while the World Health Organization (WHO) has divided the world into 6

S. A. Anwar Naqvi, Mirza Naqi Zafar & S. Adibul Hasan Rizvi
18
Figure 1: Global activities of solid organ transplants in 2011
Figure 2: Number of deceased and living donor kidney transplants in World Health Organization Member States in 2010, correlated with Human Development Index

Organ donation and transplantation in emerging economies
19
geographic administrative regions (Figure 1), where according to registry data the number of solid organs transplanted range from 1.0 pmp in Africa to 46.6 pmp in America’s [1]. Although this re-gional distribution does not take into account issues related to economics, social factors, culture or religion, the statistics however clearly show lower transplant rates in developing versus developed countries. Economics of countries play a major role in the establishment of transplant programs and also impact on organ donation rates for both the living and deceased (Figure 2) [2]. Countries with high HDI have higher transplant and donation rates as compared to low HDI countries. However, economics is not the only issue in emerging countries as other social and religious aspects con-found the economic factors, e.g. cultural reverence for the heart beating donor in Japan results in a deceased donor rate of < 1.0 pmp and a deceased donor kidney transplant rate of 1.64 pmp [1]. Religious issues in oil-rich Middle East countries result in low rates, although both Japan and Middle East region are high on the HDI [3].
Societal issues
A different aspect in understanding the emerging economies comes from two further sets of data on these countries: First freedom ranking and second the corruption index (Figure 3) [4, 5]. Freedom ranking is lowest and corruption rates highest in emerging countries. The ills of society are largely prevalent with human rights abuse, gender bias, absence of political and civil rights due to absolute monarchs, autocratic governments or military dictatorships [1]. Therefore of 132 countries classified as developing, only 47 perform transplantation. Of these countries some have become hubs for organ trade and transplant tourism [6].
Religious issues
Religious views on organ donation and transplantation vary according to religion as well as eco-nomic background. In the Islamic countries there are many rulings (fatwas) allowing organ donation and transplantation in Islam religion [7, 8]. The Middle Eastern perspective follows the Quran ver-dict ‘If anyone saves a life it shall be as though he had saved the life of all mankind’ [7]. Therefore
Ranking: Developed 1 & 2, Developing 6 & 7
Figure 3: Global Freedom Ranking and Corruption Index in 2012
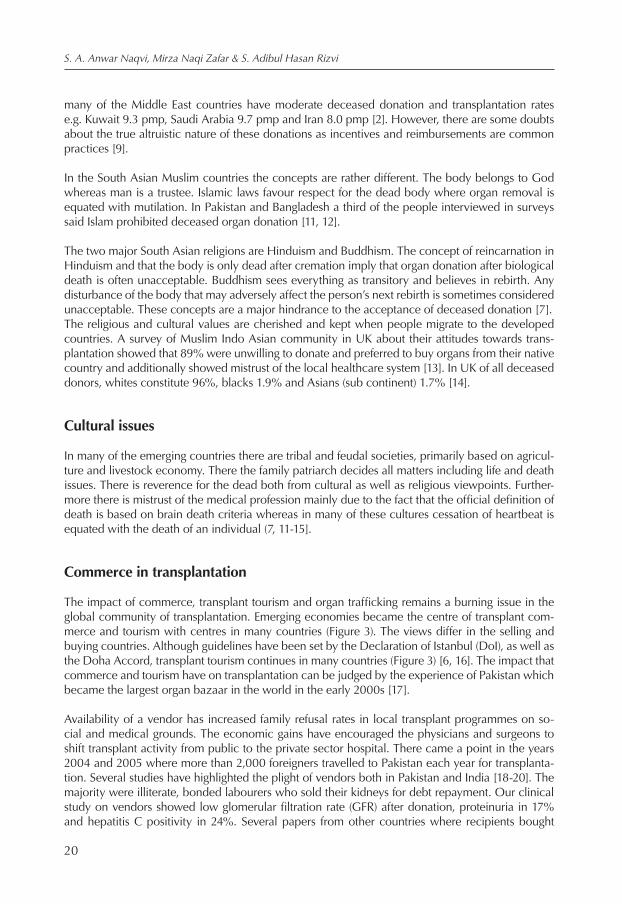
S. A. Anwar Naqvi, Mirza Naqi Zafar & S. Adibul Hasan Rizvi
20
many of the Middle East countries have moderate deceased donation and transplantation rates e.g. Kuwait 9.3 pmp, Saudi Arabia 9.7 pmp and Iran 8.0 pmp [2]. However, there are some doubts about the true altruistic nature of these donations as incentives and reimbursements are common practices [9].
In the South Asian Muslim countries the concepts are rather different. The body belongs to God whereas man is a trustee. Islamic laws favour respect for the dead body where organ removal is equated with mutilation. In Pakistan and Bangladesh a third of the people interviewed in surveys said Islam prohibited deceased organ donation [11, 12].
The two major South Asian religions are Hinduism and Buddhism. The concept of reincarnation in Hinduism and that the body is only dead after cremation imply that organ donation after biological death is often unacceptable. Buddhism sees everything as transitory and believes in rebirth. Any disturbance of the body that may adversely affect the person’s next rebirth is sometimes considered unacceptable. These concepts are a major hindrance to the acceptance of deceased donation [7].The religious and cultural values are cherished and kept when people migrate to the developed countries. A survey of Muslim Indo Asian community in UK about their attitudes towards trans-plantation showed that 89% were unwilling to donate and preferred to buy organs from their native country and additionally showed mistrust of the local healthcare system [13]. In UK of all deceased donors, whites constitute 96%, blacks 1.9% and Asians (sub continent) 1.7% [14].
Cultural issues
In many of the emerging countries there are tribal and feudal societies, primarily based on agricul-ture and livestock economy. There the family patriarch decides all matters including life and death issues. There is reverence for the dead both from cultural as well as religious viewpoints. Further-more there is mistrust of the medical profession mainly due to the fact that the official definition of death is based on brain death criteria whereas in many of these cultures cessation of heartbeat is equated with the death of an individual (7, 11-15].
Commerce in transplantation
The impact of commerce, transplant tourism and organ trafficking remains a burning issue in the global community of transplantation. Emerging economies became the centre of transplant com-merce and tourism with centres in many countries (Figure 3). The views differ in the selling and buying countries. Although guidelines have been set by the Declaration of Istanbul (DoI), as well as the Doha Accord, transplant tourism continues in many countries (Figure 3) [6, 16]. The impact that commerce and tourism have on transplantation can be judged by the experience of Pakistan which became the largest organ bazaar in the world in the early 2000s [17].
Availability of a vendor has increased family refusal rates in local transplant programmes on so-cial and medical grounds. The economic gains have encouraged the physicians and surgeons to shift transplant activity from public to the private sector hospital. There came a point in the years 2004 and 2005 where more than 2,000 foreigners travelled to Pakistan each year for transplanta-tion. Several studies have highlighted the plight of vendors both in Pakistan and India [18-20]. The majority were illiterate, bonded labourers who sold their kidneys for debt repayment. Our clinical study on vendors showed low glomerular filtration rate (GFR) after donation, proteinuria in 17% and hepatitis C positivity in 24%. Several papers from other countries where recipients bought

Organ donation and transplantation in emerging economies
21
kidneys from Pakistan show that they experienced serious infectious complications and early rejections [6].
Professional attitudes
Transplantation is still a very specialized field in many emerging economies. Paucity of intensive care unit (ICU) facilities and a negative attitude of physicians towards brain death and organ do-nation specially in emergency services and intensive care units, has held back deceased donor programmes. Non-availability of transplant services in the government sector and high costs in the private sector render the majority of the population disfranchised from dialysis and transplantation. The population seems to be unwilling to support deceased donation programmes due to several reasons. Firstly they cannot be beneficiary of deceased donation, further there is mistrust of doctors in the ICU situation for the fear of improper care and finally there is the perceived fear of sale of organs of the dying.
The way forward
Prevention strategies
Kidney transplantation and renal replacement therapies are costly interventions for the treatment of end stage renal disease (ESRD). In emerging economies funding for ESRD treatment should also be associated with funding for early detection by simple screening methods for hypertension and diabetes which can benefit a large proportion of the population specially those at high risk of de-veloping ESRD. Prevalence of chronic liver disease due to hepatitis B and hepatitis C is common in developing countries [21, 22]. There is an urgent need for cheap and effective vaccines for the prevention of Hepatitis. Funding should be made available for safe disposable syringes and simple screening tests for blood and blood products.
Awareness for organ donation and transplantation
There is generally a lack of awareness about organ donation and transplantation [2, 23]. Since there is poor access to transplantation both donation and transplant rates are low. The key to all these issues largely remain economics. To a poor population to be cut off from transplantation and deceased donation is irrelevant for the simple reason that they are not (economically) benefiting – when in need. A multitude of issues became barriers to donation and acceptance of transplantation including social, cultural, educational and religious concerns [24].
A transplantation model
Our institute in the mid 1980’s initiated a community government programme in the public sector to provide free dialysis and transplantation with life long follow-up and medications [25]. In the last 30 years over 4,000 transplants have been performed at our centre with 1 and 5 year graft survival rates of 96% and 85% respectively [25]. Each day over 750 patients are dialysed at 9 centres across the country with more than 110,000 sessions yearly. Over 1 million patients per year are offered free services in urology, nephrology, gastroenterology and hepatobiliary, oncology and transplanta-tion. The model has been sustained for over 3 decades where the guiding principle was transpar-