
Organ Preservation with Histidine-Tryptophan- Ketoglutarate (HTK) Solution with an Emphasis on...
80
Organ Preservation with Histidine-Tryptophan- Ketoglutarate (HTK) Solution with an Emphasis on Non-Heart Beating Donors (NHBD) John J. Fung, M.D., Ph.D. Cleveland Clinic Foundation Transplant Center
-
Upload
melinda-rich -
Category
Documents
-
view
218 -
download
4
Transcript of Organ Preservation with Histidine-Tryptophan- Ketoglutarate (HTK) Solution with an Emphasis on...

Organ Preservation with Histidine-Tryptophan-Ketoglutarate (HTK) Solution with an Emphasis
on Non-Heart Beating Donors (NHBD)
John J. Fung, M.D., Ph.D.
Cleveland Clinic Foundation
Transplant Center

Organ Preservation
Preservation solutions are used to maintain the organ in optimal condition from the
time of explantation until transplantation

Ischemia
• Decreased mitochondrial function– Anaerobic conditions -
depletion of ATP– Alterations in ion permeability– Accumulation of lactate
• Accumulation of hypoxanthine• Cell swelling• Cytosolic calcium accumulation

Reperfusion
• Generation of reactive oxygen species
• Increased oxidative stress• Lipid peroxidation of cellular
membranes• Free radical formation leads to
cellular destruction• Results in macrophage/Kupffer
cell activation – Increased serum tumor
necrosis factor (TNF)• Damage can lead to prolonged
hypoxia after reperfusion

Principles of Liver Preservation
• Exsanguination to reduce intravascular thrombosis
• Hypothermia to reduce cellular metabolism
• Maintain cell membrane integrity to avoid cellular swelling
• Susceptibility to cold ischemic injury: vascular endothelium > hepatocytes

History of Organ Preservation
• Simple cooling with cold solution
• Continuous hypothermic perfusion
• Collins (1967)
• Euro-Collins (1980)
• University of Wisconsin - ViaSpan (1986)
• HTK - Custidiol (1980’s)
• Celsior - 1994

-
-
60
-
30
20
-
3
-
-
-
80
-
0.25
13
15
100
Celsior
310320355Osmolalrity (mOsm/L)
2--Tryptophan (mmol/L)
--194Glucose (mmol/L)
30--Mannitol (mmol/L)
-50-Starch (gm/L)
198--Histidine (mmol/L)
1--Ketoglutarate/Glutamic Acid (mmol/L)
-1-Allopurinol (mmol/L)
-3-Glutathione (mmol/L)
-5-Adenosine (mmol/L)
-30-Raffinose (mmol/L)
-2557Phosphate (mmol/L)
-100-Lactobionate (mmol/L)
-5-Sulfate (mmol/L)
0.015--Calcium (mmol/L)
45-Magnesium( mmol/L)
10120107Potassium (mmol/L)
154010Sodium (mmol/L)
HTKUWEurocollinsComponent

High potassium, glucose, and phosphate-based solution
Designed to mimic composition of intracellular fluid
Low cost
Poor preservation quality
Short preservation times achievable
Euro-Collins Solution

• Use of impermeant molecules, lactobionate and raffinose, in preventing cell swelling
• First developed for and applied in preservation of canine pancreas
• Hydroxyethyl starch to minimize interstitial edema during machine perfusion, not necessary during cold storage
• High [K+], low [Na+]
UW Solution

Southard and Belzer

• Glutathione is oxidized during storage: addition of fresh GSH immediately before use; other additives
• High viscosity
• Solution cannot be released into circulation (high K content)
• Huge particles ~ 100 µm in diameter contained in original solution: must use in-line filtration with 40 µm pore size.Particles caught in capillary bed of perfused organ, resulting in vascular constriction, impeded reperfusion, and reduction of functional recovery
UW Solution: Disadvantages

Crystals in UW solution stored at sub-zero temperatures (a )
perfused livers (b)
pancreas (c)
kidneys (d)
Tullius et al: AJT 2:627

M.M. Gebhard, H.J. Kirlum, C. Schlegel. Organ preservation with the solution HTK
• Developed as cardioplegia
• Low potassium, high sodium
• No colloid - viscosity equal to that of pure water from 1 to 350C, with mean flow rate 3X that of UW solution at equal perfusion pressure - organs exsanguinate and cool down to lower temperatures more rapidly than with UW
HTK Solution (Custodiol)
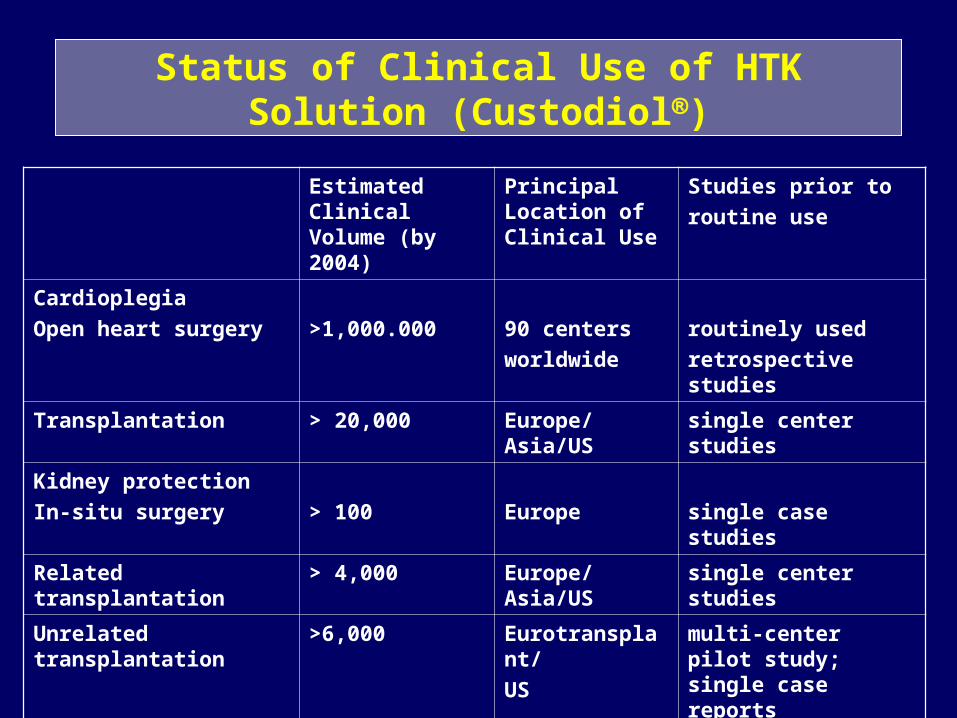
Status of Clinical Use of HTK Solution (Custodiol)
Estimated Clinical Volume (by 2004)
Principal Location of Clinical Use
Studies prior to
routine use
Cardioplegia
Open heart surgery >1,000.000 90 centers
worldwide
routinely used
retrospective studies
Transplantation > 20,000 Europe/Asia/US single center studies
Kidney protection
In-situ surgery > 100 Europe single case studies
Related transplantation > 4,000 Europe/Asia/US single center studies
Unrelated transplantation >6,000 Eurotransplant/
US
multi-center pilot study; single case reports
Liver protection > 600 Germany single center studies
Ex-vivo-surgery > 150 Germany single center studies
Pancreas transplantation > 1,000 US/Europe single case reports

Kidney Transplantation
• de Boer et al: Eurotransplant randomized multicenter kidney graft preservation study comparing HTK with UW and Euro-collins. Transplant Int, 1999, 12:447
• UW (168) vs EC (155) vs HTK (336),• DGF: 33% UW vs 43% EC* vs 31% HTK• 3-year Graft survival: UW (68%), HTK (73%),
EC (67%)• Conclusions: HTK is comparable to UW in its
preservative capabilities in cadaveric renal transplantation
Factors influencing DGF: Donor age, cause of death, CIT

J. De Boer, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK, UW and Euro-Collins (Transplant Int, 1999)

J. De Boer, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK, UW and Euro-Collins (Transplant Int, 1999)

J. De Boer, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK, UW and Euro-Collins (Transplant Int, 1999)

J. De Boer, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK, UW and Euro-Collins (Transplant Int, 1999)

Liver Transplantation
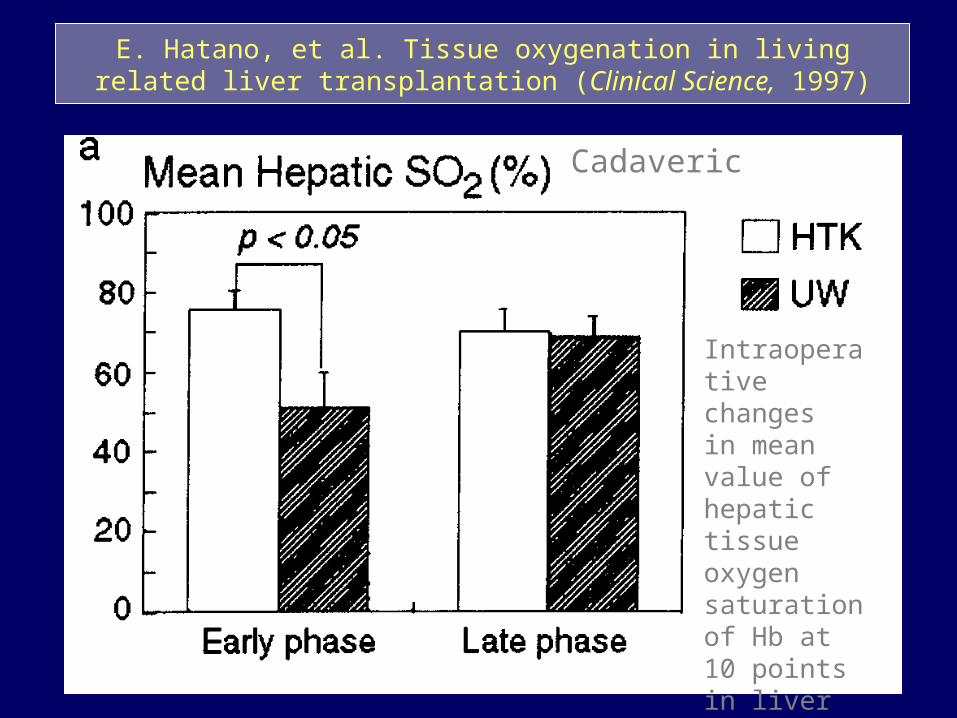
• Hatano et al: Hepatic preservation with histidine-tryptophan-ketoglutarate solution in living-related and cadaveric liver transplantation. Clinical Science (1997), 93:81
• LRD liver: HTK (15) vs UW (49)• CAD liver: HTK (30) vs UW (18)• Lower transaminases• Improved bile flow• No difference in survival or rejection rates

E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997)
Intraoperative changesin mean value of oxygen saturation of Hb at 10 points in liver graft
After reflow of operation
LRLT
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997)
Cadaveric
Intraoperative changesin mean value of hepatic tissue oxygen saturation of Hb at 10 points in liver graft

E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997)
CV of oxygen saturation of Hb at 10 points in liver graft, indicating heterogeneity of tissue oxygenation
After reflow of operation
LRLT
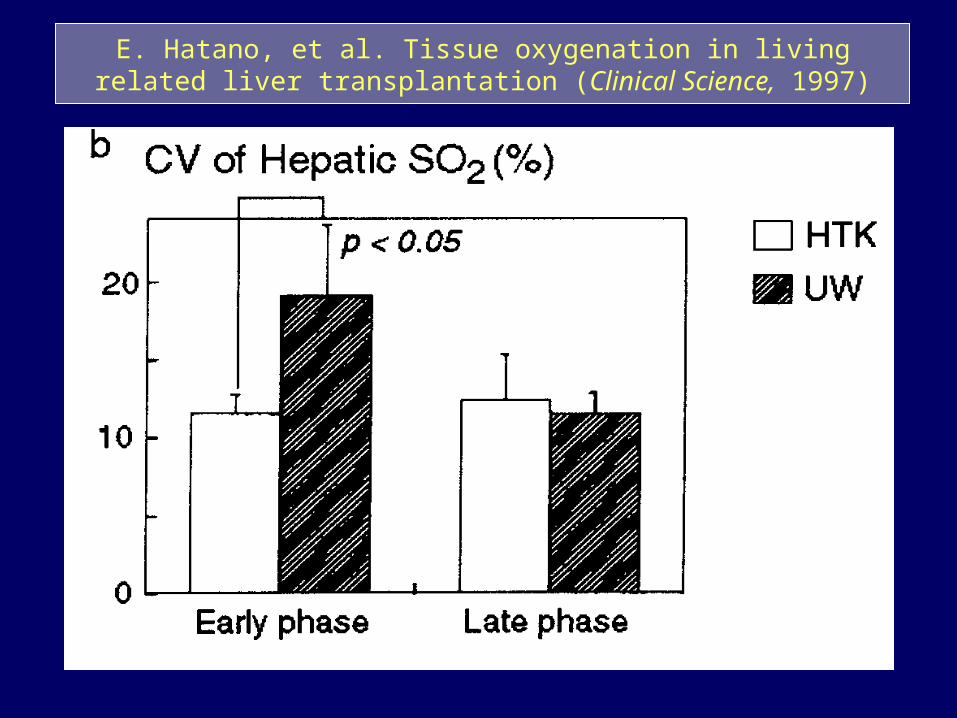
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997)

Liver Transplant Patient Survival Hannover (1988 - 2000)
0
20
40
60
80
100
0 1 2 3 4 5
%
years
HTK (n = 400)
UW (n =4 92)
P < 0.0331 (LogRank)
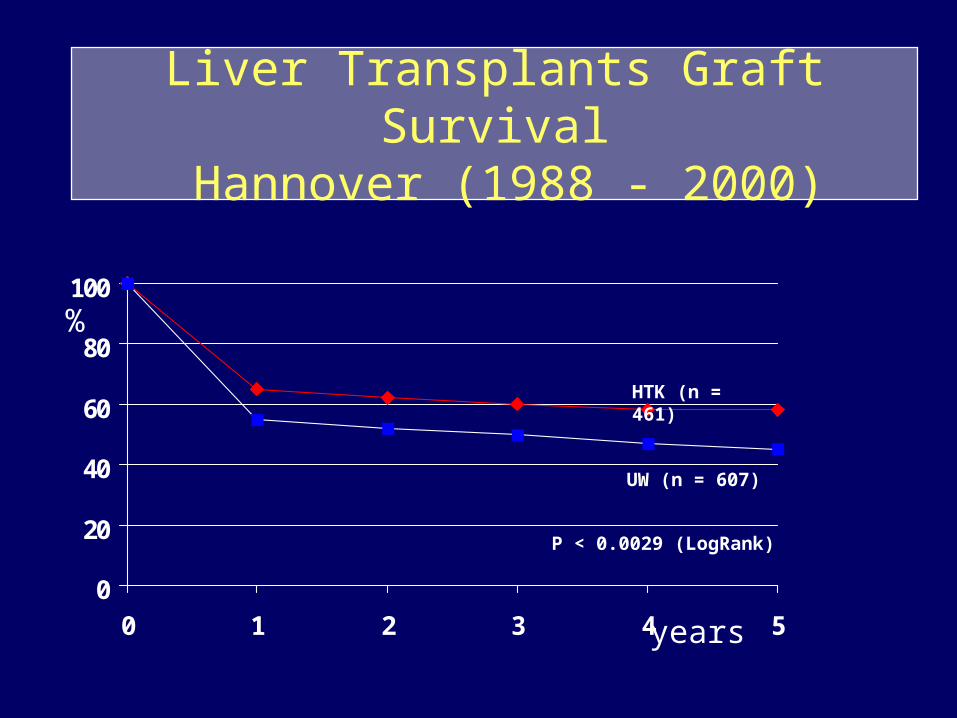
Liver Transplants Graft Survival Hannover (1988 - 2000)
0
20
40
60
80
100
0 1 2 3 4 5
%
years
HTK (n = 461)
UW (n = 607)
P < 0.0029 (LogRank)

HTK and UW for Liver Preservation
Hannover (1988 - 2000) n = 1068
< 5 days after transplantation HTK UW
• n 461 607
• PF 439 578
• INF 22 29
• INF % 4.8 % 4.8 %
p = 1.00

HTK and UW for Liver Preservation
Hannover (1988 - 1998) n = 836
Biliary Tract Complications HTK UW
• n 305 531
• BTC 39 65
• BTC % 12.8 12.2

HTK and UW for Liver Preservation
Hannover (1988 - 2000) n = 1068
CIT >15 hours HTK UW
• n 36 154
• PF 34 143
• INF 2 11
• INF % 5.6 7.1
p = 1.000
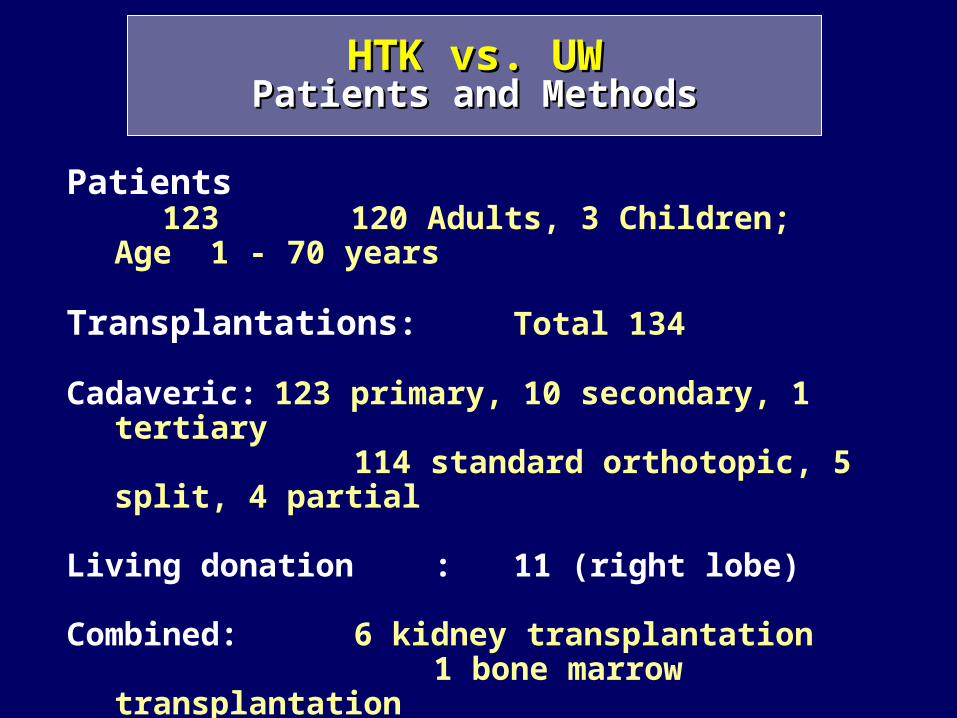
Patients 123 120 Adults, 3 Children; Age 1 - 70 years
Transplantations: Total 134
Cadaveric: 123 primary, 10 secondary, 1 tertiary114 standard orthotopic, 5 split, 4
partial
Living donation : 11 (right lobe)
Combined: 6 kidney transplantation1 bone marrow transplantation1 heart and kidney
transplantation
Preservation solution: 63 HTK und 71 UW
HTK vs. UWHTK vs. UWPatients and MethodsPatients and Methods

HTK UW
OLT total 63 71
Initial function (IF) 45 (71.5%) 43 (60.5%)
Initial dysfunction (IDF) 13 (20.6%) 26 (36.6%)
Initial nonfunction (INF) 5 (7.9%) 2 (2.8%)
HTK vs. UWHTK vs. UWInitial Liver FunctionInitial Liver Function

HTK UW
Bile duct necrosis 3 (16, 17, 485 d) 3 (44, 10, 8, 46 d)
Localized strictures 2 (72, 150 d) 2 (210, 305 d)
Diffuse strictures (ITBL) - 3 (610, 210, 365 d)
Total 5 8
ITBL = ischemic type biliary lesion
HTK vs. UWHTK vs. UWBiliary ComplicationsBiliary Complications

HTK UW
AST max (U/l) 1320 + 1254 1389 + 1214
“ pod 7 (U/l) 26.7 + 17.5 24.3 + 18.4
AP pod 7 (U/l) 159.7 + 94.6 214.8 + 109.2
GGT pod 7 (U/l) 81 + 52.9 84.6 + 59.5
Bilirubin pod 14 (mg/dL) 9.5 + 9.7 13.8 + 12.6
HTK vs. UWHTK vs. UWBiochemical ParametersBiochemical Parameters
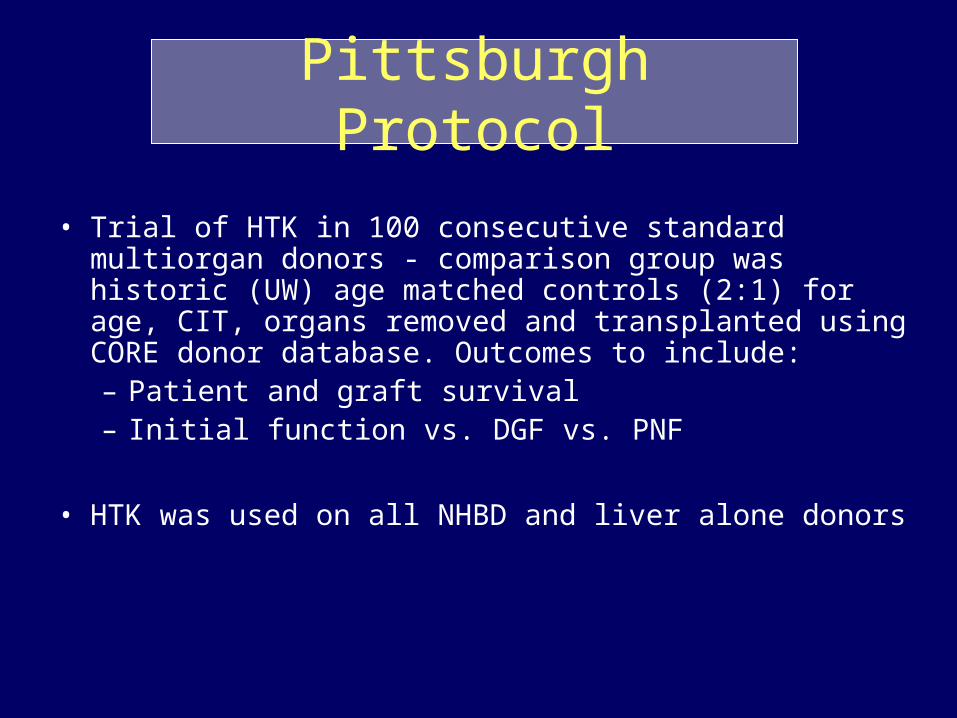
Pittsburgh Protocol
• Trial of HTK in 100 consecutive standard multiorgan donors - comparison group was historic (UW) age matched controls (2:1) for age, CIT, organs removed and transplanted using CORE donor database. Outcomes to include:– Patient and graft survival– Initial function vs. DGF vs. PNF
• HTK was used on all NHBD and liver alone donors

Patients
HTK UW
Donors 84 169Gender 49 M, 35 F 98 M, 71 F
Age 2 Wks - 75Y 3Y - 75Y
(47) (46)
(43.3 + 19) (43.7 + 18.8)
RecipientsGender 62 M, 22 F 101 M, 68 F
Age 2Y - 71Y 1Y - 73Y
(50) (52)
(49.7 + 13) (50.3 + 12.3)

Liver Transplantation, CadavericUW / HTK
Age D/R 43.7+18.8 (3-75) / 50.3+12.3 (1-73)
Age D/R 43.3+19 (1wk-75) / 49.7+13 (2-71)
CIT 619+191
CIT 616+193
AST1 1293+2907 Median: (597) (97-31490)
AST1 1489.2+2404 (595) (72-15750)
ALT1 834.9+1192 (483) (91-6552)
ALT1 914.8+1131.3 (450) (85-7016)
AST7 99.9+189.2 (51) (17-1969)
AST7 72.9+64.4 (55) (12-498)
ALT7 189.4+191.2 (137) (40-1408)
ALT7 178.9+145.6 (139) (22-568)
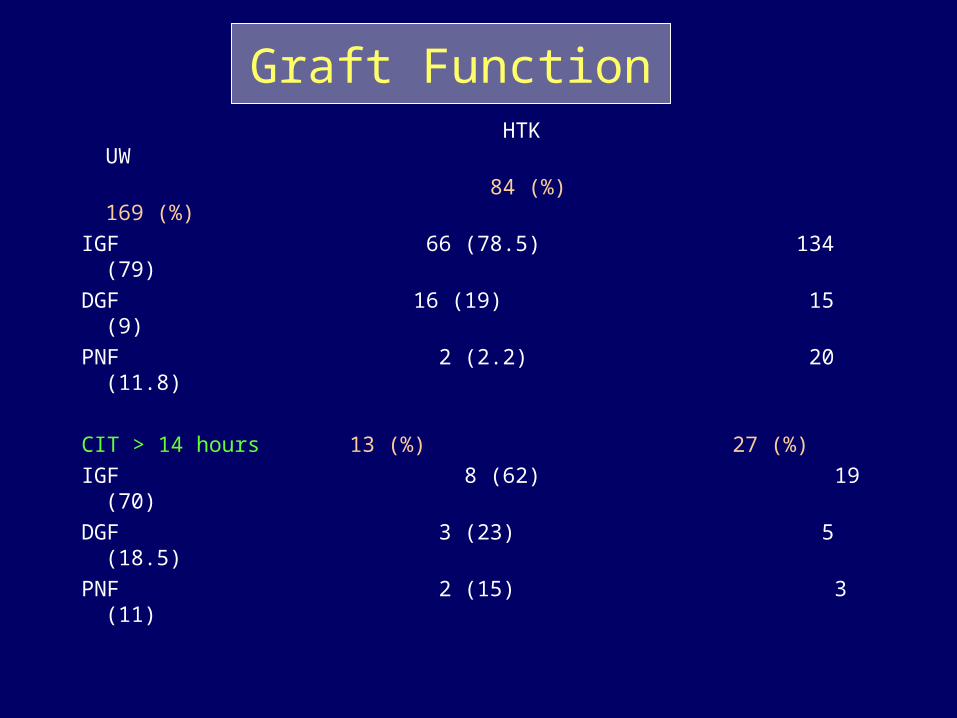
Graft Function HTK UW
84 (%) 169 (%)
IGF 66 (78.5) 134 (79)
DGF 16 (19) 15 (9)
PNF 2 (2.2) 20 (11.8)
CIT > 14 hours 13 (%) 27 (%)
IGF 8 (62) 19 (70)
DGF 3 (23) 5 (18.5)
PNF 2 (15) 3 (11)

30-day Survival
HTK UW
84 169
Graft 94% 83%
Patient 96% 89%
Re-OLTX 3 13in 30 days
HAT 2 4
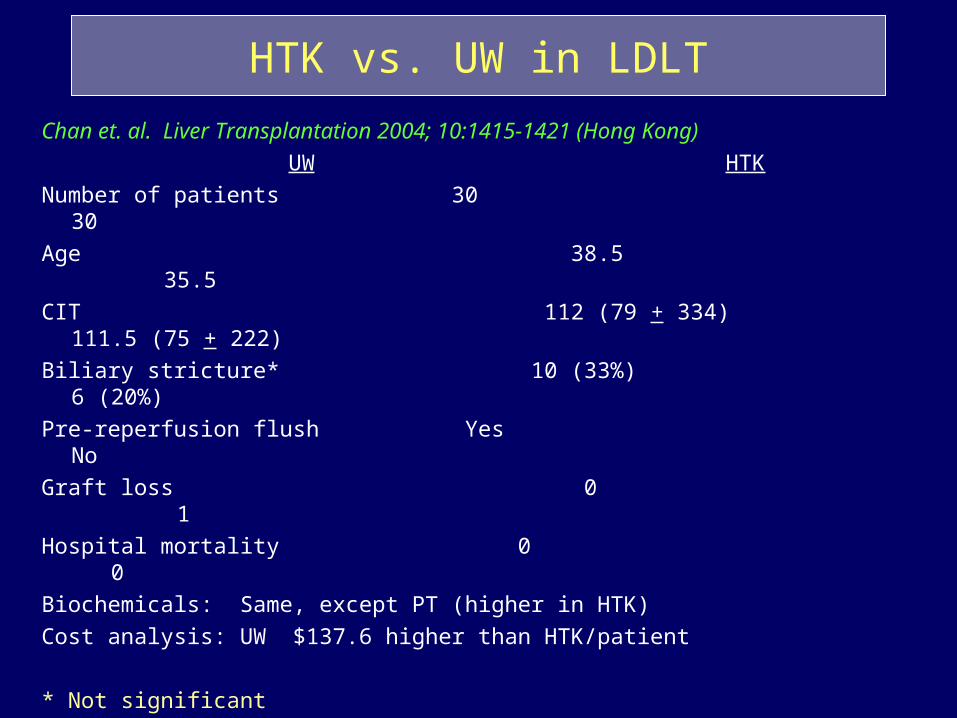
HTK vs. UW in LDLT
Chan et. al. Liver Transplantation 2004; 10:1415-1421 (Hong Kong)
UW HTK
Number of patients 30 30
Age 38.5 35.5
CIT 112 (79 + 334) 111.5 (75 + 222)
Biliary stricture* 10 (33%) 6 (20%)
Pre-reperfusion flush Yes No
Graft loss 0 1
Hospital mortality 0 0
Biochemicals: Same, except PT (higher in HTK)
Cost analysis: UW $137.6 higher than HTK/patient
* Not significant

HTK vs. UW in LDLTA Prospective Study
Testa et. al. Liver Transplantation 2003; 9:822-826 (Chicago and Essen)Donors: Right lobe Age: (33 + 10) 18 M, 12 FRecipients: Age: (49 + 9), 20 M, 10 F, MELD: 13.4 + 7.4
Mean Follow-up 13 + 7 months UW HTKPerfusion 14 16
Artery 1 mL/g 3 mL/gPortal vein 1 mL/g 1.5 mL/g
Pre-reperfusion flush Yes No (practical advantage)
CIT 147 + 44 144 + 40Patient survival 79% 88%Graft survival 72% 83%PNF 1 0HAT 1 1Liver biochemical values: SimilarNo intrahepatic biliary strictureOverall: Equally effective. HTK has practical and economical advantage

HTK solution for organ preservation in human liver transplantation
A prospective multi-center observation studyPokorny et. al. Transplant International 2004; 17:256-260 (Austria, Germany)
214 patients in 4 European centers (1996-1999)5 liters of HTK for preservation CIT 444 + 224All vascular anastomoses completed before reperfusionNo pre-reperfusion flushPNF 2.3%, Initial dysfunction 6.5%Graft dysfunction not correlated with CIT
1-year patient and graft survival 83% and 80% (unrelated to CIT)
HTK: safe and effective and easy to use. Comparable to UW with less cost.

HTK vs. UW in liver transplantationA meta analysis
Feng et.al. Liver Transplant, 2007

Patient Survival
Graft Survival
P= 0.87
RR 1.01
P= 0.86
RR 1.01
HTK vs. UW in liver transplantation A meta analysis
Feng et.al. Liver Transplant, 2007

HTK vs. UW in liver transplantationA meta analysis
Feng et.al. Liver Transplant, 2007

HTK vs. UW in liver transplantationA meta analysis
• Cost: HTK cheaper than UW• Biliary complications: Trend for less biliary strictures with HTK• PNF, PDF, DGF: No difference• Graft survival: No difference• Patient survival: No difference• Biochemical values: No difference
Feng et.al. Liver Transplant, 2007

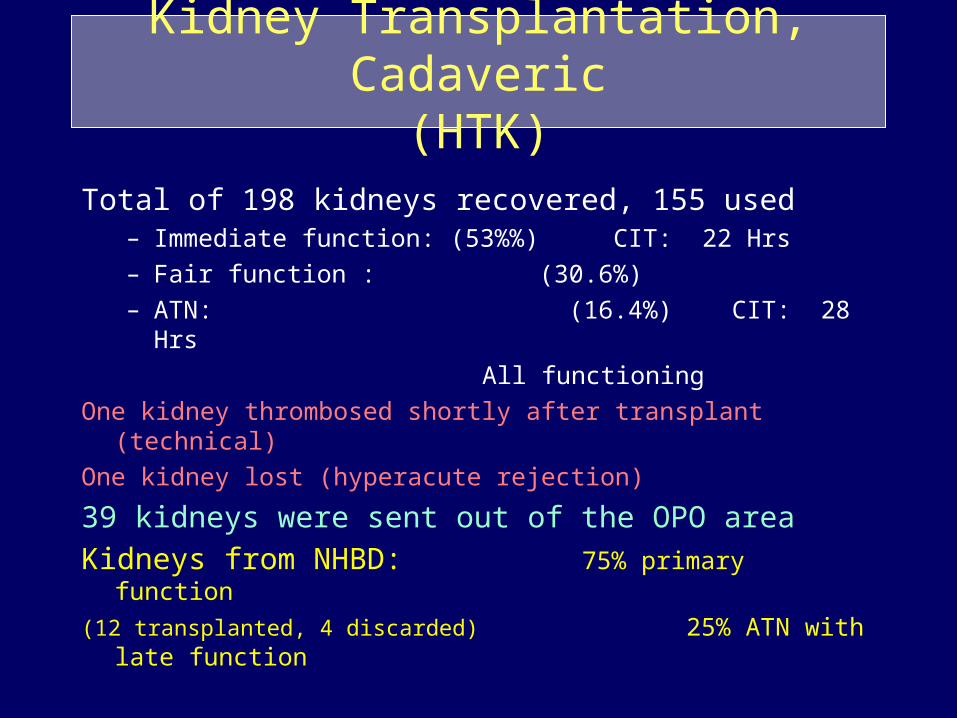
Kidney Transplantation, Cadaveric(HTK)
Total of 198 kidneys recovered, 155 used – Immediate function: (53%%) CIT: 22 Hrs
– Fair function : (30.6%)
– ATN: (16.4%) CIT: 28 Hrs
All functioning
One kidney thrombosed shortly after transplant (technical)
One kidney lost (hyperacute rejection)
39 kidneys were sent out of the OPO area
Kidneys from NHBD: 75% primary function
(12 transplanted, 4 discarded) 25% ATN with late function
Pancreas Transplantation, Cadaveric(HTK)
• 40 pancreata recovered– 20 used– 20 research
• 19 used locally
• One sent to another center (out of OPO) with kidney for K-P transplant with good function
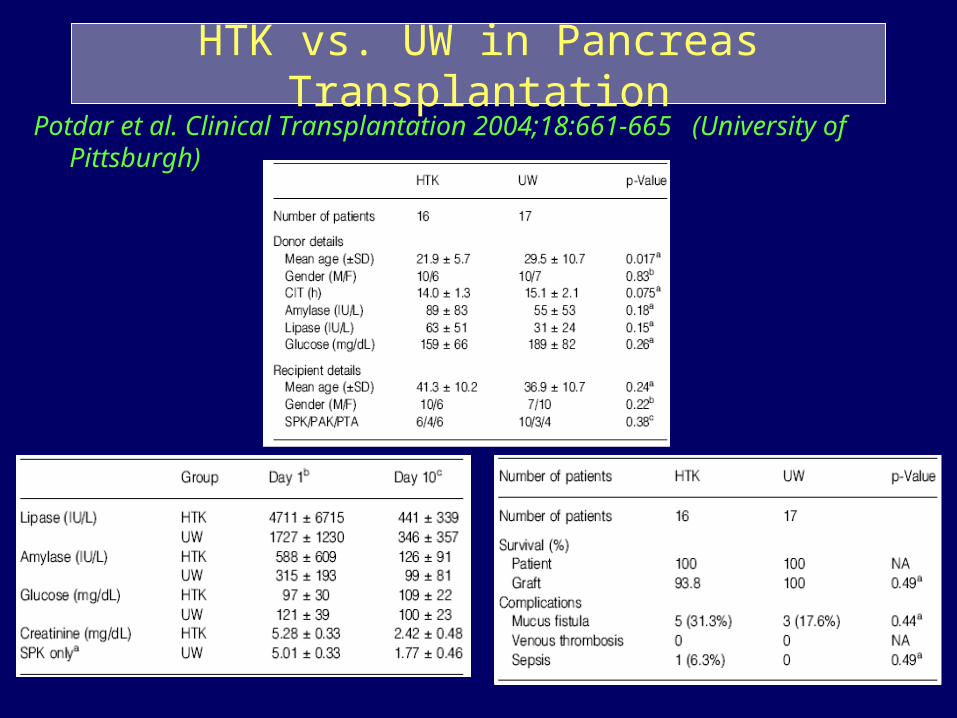
HTK vs. UW in Pancreas TransplantationPotdar et al. Clinical Transplantation 2004;18:661-665 (University of
Pittsburgh)
Kidney Transplantation, Cadaveric(HTK)
Total of 198 kidneys recovered, 155 used – Immediate function: (53%%) CIT: 22 Hrs
– Fair function : (30.6%)
– ATN: (16.4%) CIT: 28 Hrs
All functioning
One kidney thrombosed shortly after transplant (technical)
One kidney lost (hyperacute rejection)
39 kidneys were sent out of the OPO area
Kidneys from NHBD: 75% primary function
(12 transplanted, 4 discarded) 25% ATN with late function

Biliary Complications After Liver Transplantation

Long-term Biliary Complications(one year)
HTK UW
(76) (134)
Anastomotic stricture 3 5
Diffuse (ischemic) stricture 0 2
Bile leak 1 1

Post-liver Transplant Biliary Strictures
• Biliary strictures after liver transplantation: 10-30%
• Adequate flushing of peri-biliary arterial tree is important
• High viscosity preservation solutions might not completely flush the small donor peri-biliary plexus
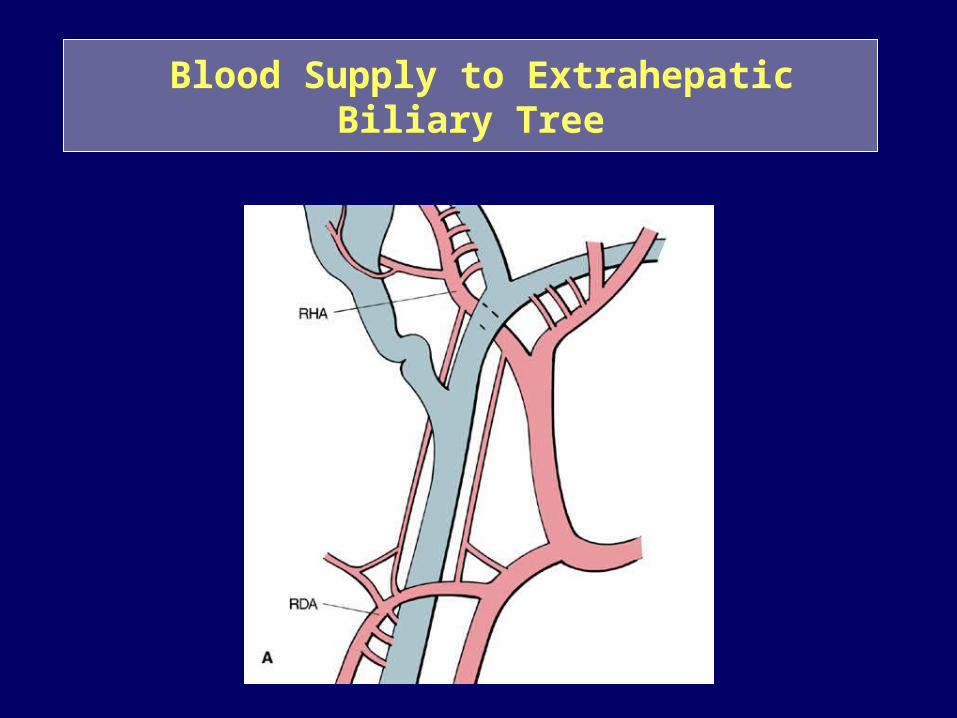
Blood Supply to Extrahepatic Biliary Tree

Peri-Biliary Vascular Plexus
Alpini et al.

Methacrylate Injection Replica of Peri-Biliary Capillary Plexus
Ohtani
NHBD and Liver Transplantation
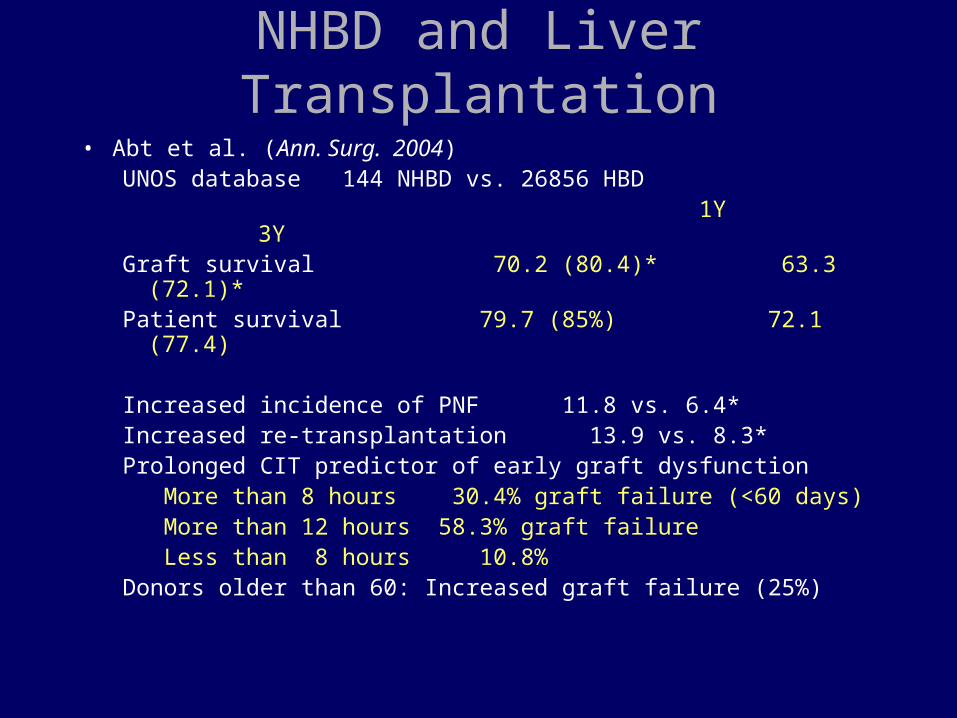
• Abt et al. (Ann. Surg. 2004)UNOS database 144 NHBD vs. 26856 HBD 1Y 3YGraft survival 70.2 (80.4)* 63.3 (72.1)*Patient survival 79.7 (85%) 72.1 (77.4)
Increased incidence of PNF 11.8 vs. 6.4*Increased re-transplantation 13.9 vs. 8.3*Prolonged CIT predictor of early graft dysfunction
More than 8 hours 30.4% graft failure (<60 days)More than 12 hours 58.3% graft failure Less than 8 hours 10.8%
Donors older than 60: Increased graft failure (25%)

Super Rapid Technique
A. Casavilla, Pittsburgh, 1995
Cannulation of aorta
Perfusion with HTK
Topical cooling
Thoracotomyaortic clamping
drainage IVC
En bloc removal and benchtable look for aberrant vessels

Liver Transplantation from NHBD1993-199621 donors 17 recovered 9 used (55%)Patient survival 4/9 (45%)
1997-200143 donors 37 recovered 23 used (62%)Patient survival 19/22 (86.5%)
1/02-12/0325 transplants (12 sent livers, 13 local) CIT sent vs. local 766 (min) : 590 (min) 2 DGF and one PNF (sent), one DGF (local)
Patient survival 20/25 (80%)
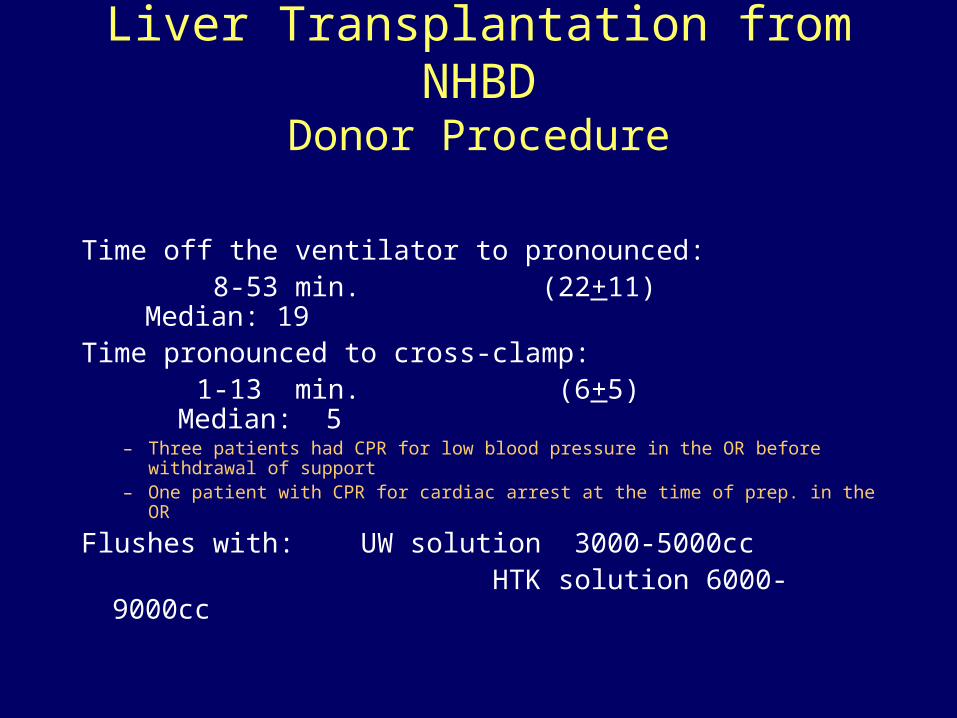
Liver Transplantation from NHBDDonor Procedure
Time off the ventilator to pronounced: 8-53 min. (22+11) Median: 19Time pronounced to cross-clamp: 1-13 min. (6+5) Median: 5
– Three patients had CPR for low blood pressure in the OR before withdrawal of support
– One patient with CPR for cardiac arrest at the time of prep. in the OR
Flushes with: UW solution 3000-5000cc HTK solution 6000-9000cc
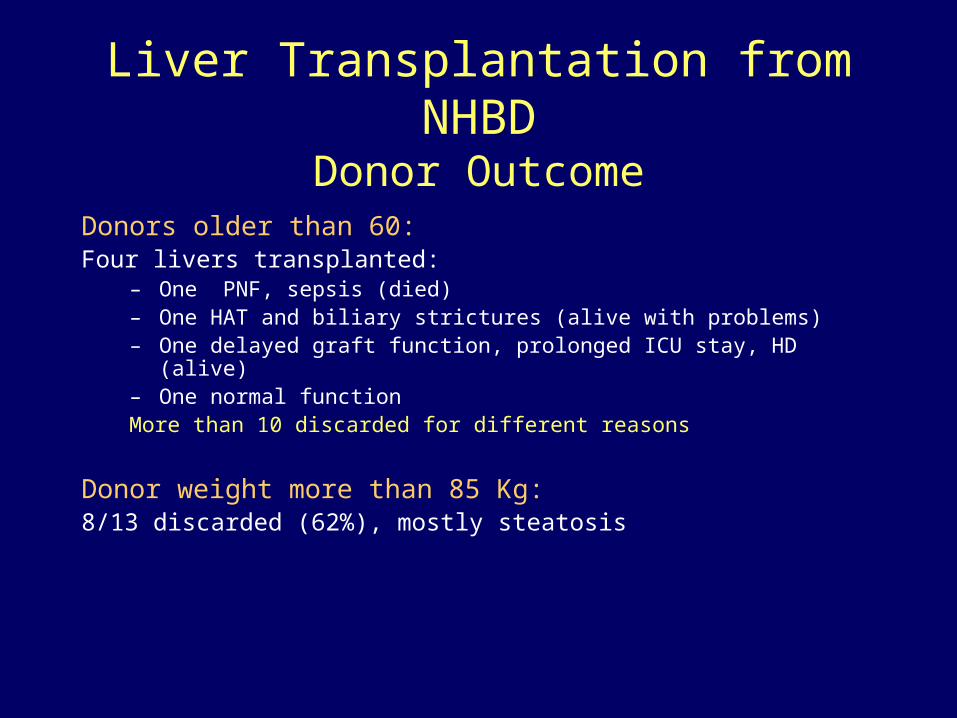
Liver Transplantation from NHBDDonor Outcome
Donors older than 60:Four livers transplanted:
– One PNF, sepsis (died)– One HAT and biliary strictures (alive with problems)– One delayed graft function, prolonged ICU stay, HD (alive)– One normal functionMore than 10 discarded for different reasons
Donor weight more than 85 Kg:8/13 discarded (62%), mostly steatosis

Liver Transplantation from NHBDRecipient Characteristics
Fifty-seven transplants in 56 recipients 32 males 24 females (One patient received 2 livers from NHBD)
Age: 18-69 y (50+11) Median: 50
Primary disease: HCV, PBC, AI, ETOH, …..
CIT (min): 630+144 (358-1056) Median: 600

Liver Transplantation from NHBD
Post-transplant labs.:
Range Mean+SD Median
AST(peak) 77-13692 3620+3973 2039
ALT(peak) 96-7245 1355+1825 504
AST(day7) 14-285 67+73 41
ALT(day7) 28-191 93+45 90
PT(day7) 11-15 13.1+1.1 12.8
T.Bili. D/C 0.3-1.7 0.9+0.4 0.95
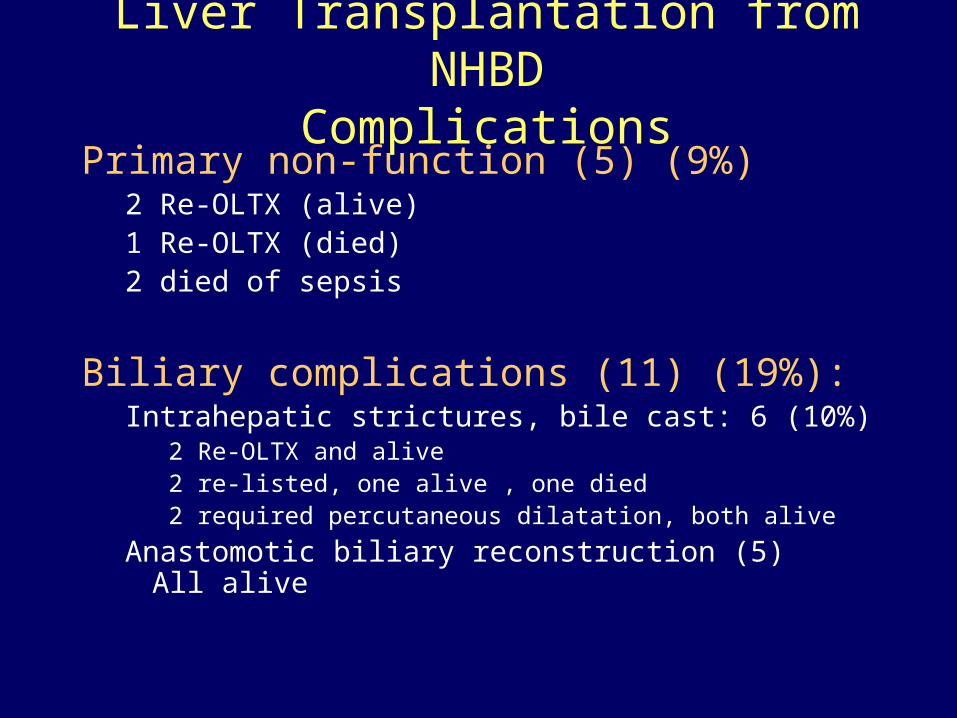
Liver Transplantation from NHBDComplications
Primary non-function (5) (9%)2 Re-OLTX (alive)1 Re-OLTX (died)2 died of sepsis
Biliary complications (11) (19%):Intrahepatic strictures, bile cast: 6 (10%)
2 Re-OLTX and alive2 re-listed, one alive , one died2 required percutaneous dilatation, both alive
Anastomotic biliary reconstruction (5) All alive

Liver Transplantation from NHBDComplications
Hepatic artery complications (8) (14%):
Hepatic artery stricture (2) Repaired Both alive
Hepatic artery thrombosis (6) (11%)Re-OLTX (3) Two died, one alive
Repaired (1) Alive
None (sepsis) (2) Died
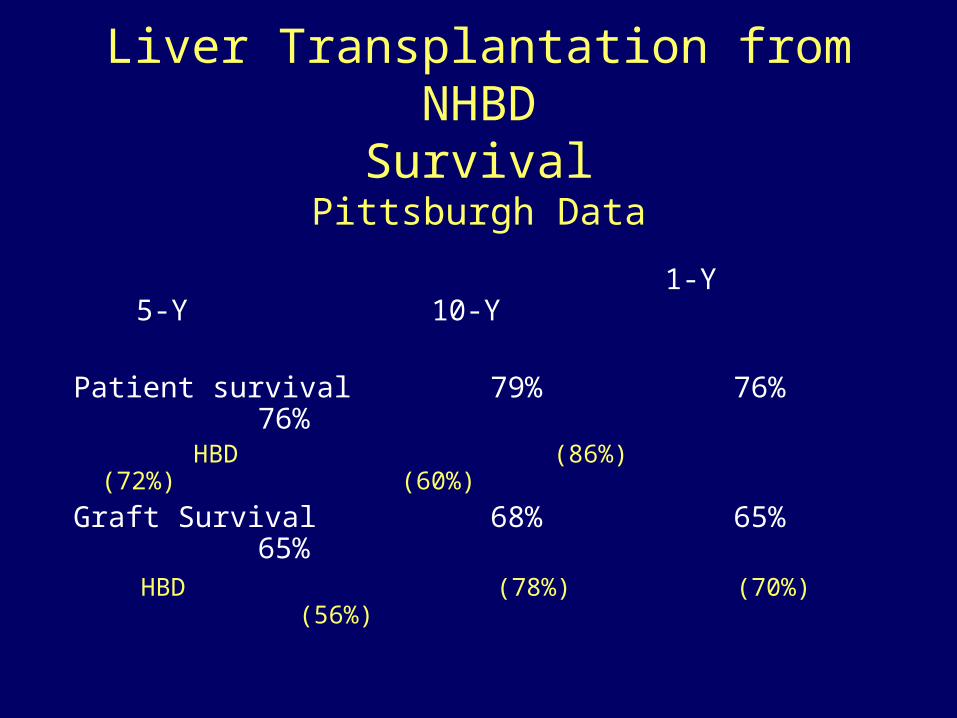
Liver Transplantation from NHBDSurvival
Pittsburgh Data
1-Y 5-Y 10-Y
Patient survival 79% 76% 76% HBD (86%) (72%) (60%)
Graft Survival 68% 65% 65% HBD (78%) (70%) (56%)

Non-Heart-Beating Donors HTK UW 8 15
IGF 8 12PNF 0 3
Biliary complications 1 3 Anastomotic 1 1 Diffuse 0 1 Bile leak 0 1

HTK (NHBD) UW
DCD Donor Liver Transplants1995 - 2004
0
50
100
150
200
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Nu
mb
er
of
Tran
sp
lan
ts . 184
Year of Transplant

Kaplan-Meier Adult Graft Survival Primary Deceased Donor Liver Transplants
1998-2003
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36Months Post Transplant
Su
rviv
al R
ate
(%
) .
Brain Dead DCD
N=303
N=22,199
Includes adult, primary, liver alone transplants

Kaplan-Meier Adult Graft Survival Primary Deceased Donor Kidney Transplants
1998-2003
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Months Post Transplant
Su
rviv
al R
ate
(%)
.
SCD DCD ECD
N=32,888
N=1,177
Includes adult, primary, kidney alone transplants
N=6,610

Yamauchi et al: Warm preflush with streptokinase improves microvascular procurement and tissue integrity in liver graft
retrieval from non-heart-beating donors.Transplantation. 2000, 69:1780
• After 30 min of warm ischemia, microvascular perfusion of UW solution was found markedly altered when compared with that of sham-operated living controls
• Preflush with RL (RL+UW) only slightly attenuated the perfusion disorder • the addition of SK (7500 IU/100 cc) to RL (SK/RL+UW) resulted in a
significant improvement of microvascular graft perfusion (P<0.05). • the increased enzyme release observed in solely UW-flushed livers after 24
hr cold preseravtion was only slightly influenced by preflush with RL, but markedly attenuated (P<0.05) by pre-flush with RL containing SK

Gok et al: How to improve the quality of kidneys from non-heart-beating donors: a randomised controlled trial of
thrombolysis in non-heart-beating donors.Transplantation. 2003 Dec 27;76(12):1714-9
• 2 groups of NHBD donors -streptokinase and placebo– 72% Maastricht II (uncontrolled), 28% Maastricht III (controlled)
• Streptokinase given at 1,500,000 units prior to preservation solution
• streptokinase-treated kidneys had a better appearance at procurement (P<0.001)
• performed better during machine preservation (P<0.001).
• higher proportion of kidneys transplanted through the use of streptokinase (63.6% with streptokinase vs. 42.6% with placebo)
• PNF - 0% streptokinase vs 17% placebo
• Graft function at one year - 93% streptokinase vs 83% placebo

• Abdominal Organ Recovery (Adult Donor):– Cannulate aorta, flush abdominal organs with 3-4 liters of ViaSpan– Cannulate portal, flush with 1-2 liters of ViaSpan– PRESERVATION TIME 12-15 MINUTES
– Flush 1 additional liter of ViaSpan through liver during preparation for transportation
– Store liver in 1 liter of ViaSpan– Kidneys stored in 1 liter of EuroCollins
– Solution Used: 6-8 liters of ViaSpan– 1 liter of Euro-Collins

• Abdominal Organ Recovery (Adult Donor):– Cannulate aorta, flush abdominal organs with 8-10 liters of HTK– No Portal Canulation– PRESERVATION TIME 4-7 minutes
– Flush 1 additional liter of HTK through liver during preparation for transportation, also used as storage solution
– Use 1 liter of HTK for storage of Kidneys
– Solution Used: 10-12 liters of Custodiol HTK

COST COMPARISONViaSpan/Eurocollins vs. Custodiol HTK
• ViaSpan with additives $327.00 Liter• EuroCollins with additives $ 37.50 Liter
• PER CASE COST:• 6-8 Liters of ViaSpan $1962.00-$2616.00• 1 Liter of EuroCollins $ 37.50• TOTAL $1963.50-$2653.50
• Custodiol HTK $150.00 Liter
• PER CASE COST:• 8-10 Liters of Custodiol HTK $1200-$1500
• POTINTIAL SAVINGS POTINTIAL SAVINGS $763.50-$1,153.50 PER CASE$763.50-$1,153.50 PER CASE

ANNUAL PROJECTED COST SAVINGS USING CUSTODIOL HTK
$73,000-$137,000Based on 130 Cases

HTK vs. UWCost analysis and savings
Englesbe et. al. Transplantation 2006;82:580-581 University of Michigan
Gift of Life, Michigan
Material costs of 77 consecutive kidney-pancreas recovered for transplantation
Significant cost reduction: 43% actual cost saving for Gift of Life Michigan
IDENTIFIED ADVANTAGES OF CUSTODIOL HTK
• No additives• Ready to use immediately for unstable donors• No discarding of solution if case is aborted• Packaging size• No apparent difference in organ function• Cost Savings• Transport/storage at room temperature• Approved for liver, kidney, pancreas and heart
preservation

Conclusions Comparison of HTK and UW
• Overall, logistical and cost benefits with HTK• Comparable PNF/PDF for livers and long-term
liver function tests– Too soon for any conclusion regarding long-term
biliary complications, but suggestion of less severe changes
• Similar early outcomes for kidneys and pancreases


















