Oregon Smile Survey 2007 - Oregon Health...
24
Oregon Smile Survey 2007
-
Upload
nguyenthuy -
Category
Documents
-
view
218 -
download
3
Transcript of Oregon Smile Survey 2007 - Oregon Health...
Oregon Smile Survey 2007


Public Health Division, Department of Human Services November 15, 2007
To the people of Oregon:
Tooth decay is the most common childhood disease, affecting five times more children than asthma. Tooth decay among children is a major concern for a number of reasons, often causing oral pain and infection, which in turn can affect a child’s school attendance and success, nutrition, self-esteem and general health.
“Smile Survey 2007” is an important step in addressing this problem. This survey is the second in a series of assessments and presents the findings of oral screenings of first-, second- and third-graders attending Oregon public schools in 2006-07. The first survey was conducted in 2002.
Identifying the current oral health of Oregon’s children is critical in identifying needs for targeting more early-stage prevention measures, including appropriate professional care and community-based interventions, all of which can significantly reduce the amount and severity of tooth decay.
In addition to addressing current problems, an accurate assessment of the oral health of Oregon’s children is important for reducing the challenges of the future. It is commonly recognized that untreated tooth decay worsens with age and eventually affects a person’s overall general health.
Taking a look at many of the same measurements addressed in the 2002 Smile Survey, this year’s report also provides an important tool for gauging changes in the oral health of Oregon’s children over the past five years, important for assessing trends in dental disease patterns.
The information found in this report can be used to develop and implement community-based prevention strategies designed to ensure all of Oregon’s children have a healthy smile.
Yours in oral health,
Gordon B. Empey, D.M.D., M.P.H.Executive dental health consultant, Oral Health Program, Office of Family Health
Katherine J. Bradley, Ph.D., R.N.Administrator, Office of Family Health


1
Acknowledgments
The Office of Family Health’s Oral Health Program would like to thank these individuals for their involvement in the Oregon Smile Survey 2007:
Sue Sanzi-Schaedel, R.D.H., M.P.H.Susan Castillo, Superintendent of Public InstructionShanie Mason, M.P.H., C.H.E.S.Andrew Osborn, M.B.A.Kathy Phipps, Dr. P.H.Ken Rosenburg, M.D., M.P.H.Melody Scheerer, B.S.D.H., R.D.H.
A special acknowledgment is extended to dental screeners who participated in the survey:
We would also like to thank the principals and staff of participating schools. Without their assistance, this report would not have been possible.
If you need this document in an alternate format, please call 971-673-0252
Oregon Department of Human Services Public Health Division Office of Family Health Oral Health Program
Melanie BreidenthalZina BurtCandis ClemensJeannnie CusterTricia GatesDorene Holmes
Laurie JohnsonLaurie KellyLinda MannAlicia RiedmanDarla Thompson

2
Table of Contents
Acknowledgments .............................................................. 1
Executive summary............................................................. 3
Fast facts from the 2007 Smile Survey ............................... 5
Survey findings ................................................................... 7
Recommendations ........................................................... 17Community water fluoridation .......................................18Early-childhood cavities prevention ...............................18School-based fluoride supplement programs .................18School-based dental sealant programs ..........................18

3
Executive summary
During the 2006-2007 school year, 3,865 first, second and third-graders in Oregon public schools participated in a statewide oral health survey conducted by the state’s Oral Health Program, an effort of the Office of Family Health. Using national Basic Screening Survey (BSS) criteria recommended by the Centers for Disease Control and Prevention and the Association of State and Territorial Dental Directors, specially trained dental hygienists performed a brief, simple visual screening of each child’s mouth. In addition, parents were invited to complete a questionnaire that included questions about the child’s age, race/ethnicity, participation in the Federal Free or Reduced Lunch (FRL) Program, language spoken at home, gender, medical insurance, dental insurance, and time since last dental visit. Approximately half of the parents returned the questionnaire.*
The results of the study were sobering. Nearly two-thirds of all students have already had a cavity, a dental condition that is 100 percent preventable. More than half of the children identified as ever having a cavity had untreated dental decay.
The survey also determined many children in Oregon do not get the dental care they need. At the time of the survey, more than one in four children had not seen a dentist in the previous year. More than one in three needed treatment the day they were examined by the survey hygienist.
Since the first Smile Survey conducted in 2002, every major measure of oral health among Oregon’s school children has worsened. Compared with the 32 other states with BSS data, Oregon ranks 25th – or seventh from the bottom, in percentage of children with untreated decay.
The survey also pointed out oral disease disparities exist in Oregon based on geographic residence, dental insurance coverage, income and race/ethnicity.
* A complete description of the survey methods and sampling is available at www.oregon.gov/DHS/ph/oralhealth/index.shtml.

4
Yet the reality is oral health among Oregon school children does not have to be this bad. There are several nationally recognized best practice strategies that rely on strong collaboration between dental providers, public health programs, schools and others with a vested interest in the oral health of children. The four key community-based preventive measures that have been proven effective in reducing tooth decay are:
Community water fluoridation •Early-childhood caries prevention programs •School-based dental sealant programs •School-based fluoride supplement programs •

5
Fast facts from the 2007 Smile Survey
Dental decay remains a significant public health •problem among Oregon’s children. What’s more, the 2007 Smile Survey found the oral health of Oregon’s youngsters is worsening.
Compared with a survey conducted five years ♦earlier, Oregon scored worse in every major measure of oral health for children. The proportion of school children with ♦untreated decay increased by 49 percent.
The oral health of Oregon’s school children lags behind those •of children in Washington, Idaho, Alaska and California. Of 32 states with similar reporting methods, Oregon ranks 25th, or seventh from the bottom, in the percent of school children with untreated decay.
Nearly two of every three children in first, second and third •grade in Oregon already have had a cavity. More than half of those children have untreated decay.
More than one in three children in Oregon need treatment •for tooth decay. At the time of the survey, an estimated 27 percent of Oregon’s children had not seen a dentist in the previous year.
Fewer than half of Oregon’s third-graders have sealants – a •simple, safe, effective, and low-cost method for preventing tooth decay.
School children who live outside of the Portland metropolitan •area experience more tooth decay, more untreated decay, and more decay severe enough to require urgent treatment than their urban counterparts.

6
Children without dental insurance have poorer oral health and •lower access to care. The estimated 24 percent of school children who are without dental insurance are more likely to have untreated decay, less likely to have visited a dentist in the previous year, and are less likely to have valuable, decay-preventing sealants on their teeth.
Low-income children suffer from poorer oral health and lower •access to care. Compared with those in the highest income bracket, children in the lowest bracket suffer twice the rate of untreated decay, almost three times the rate of rampant decay, and are 30 percent less likely to have seen a dentist in the previous year.
The racial and ethnic disparities in oral health are easing •somewhat. Compared with the 2002 Smile Survey:
All categories of children experienced worsening oral ♦health conditions.Children of Hispanic ethnicity continue to have a ♦substantially higher rate of oral disease than their White, non-Hispanic counterparts.The gap between Hispanic children and White, non- ♦Hispanic children has narrowed.

7
Dental decay remains a significant public health problem for Oregon’s children
In 2007 …
Nearly two in three children in first, second and third grades, representing 80,000 Oregon school children, have already had a cavity.*
One of every five children in this age group, representing more than 24,000 Oregon youngsters, have rampant decay, meaning decay in seven or more teeth
Nearly one in six youngsters in this age category – representing more than 21,000 Oregon children – have already had cavities in their permanent, ‘adult’ teeth. Decay in a permanent tooth requires a lifetime of re-treatment, often including larger fillings over the years, and perhaps a crown or an extraction. Decayed teeth also are not suitable for sealants, a highly effective, low-cost method for preventing cavities. (See page 11 for dental sealant rates.)
Cavities are 100% preventable.
Many children get their first cavity before they lose their first tooth.
* Includes children who have active decay, a previous filling or premature tooth extraction
8
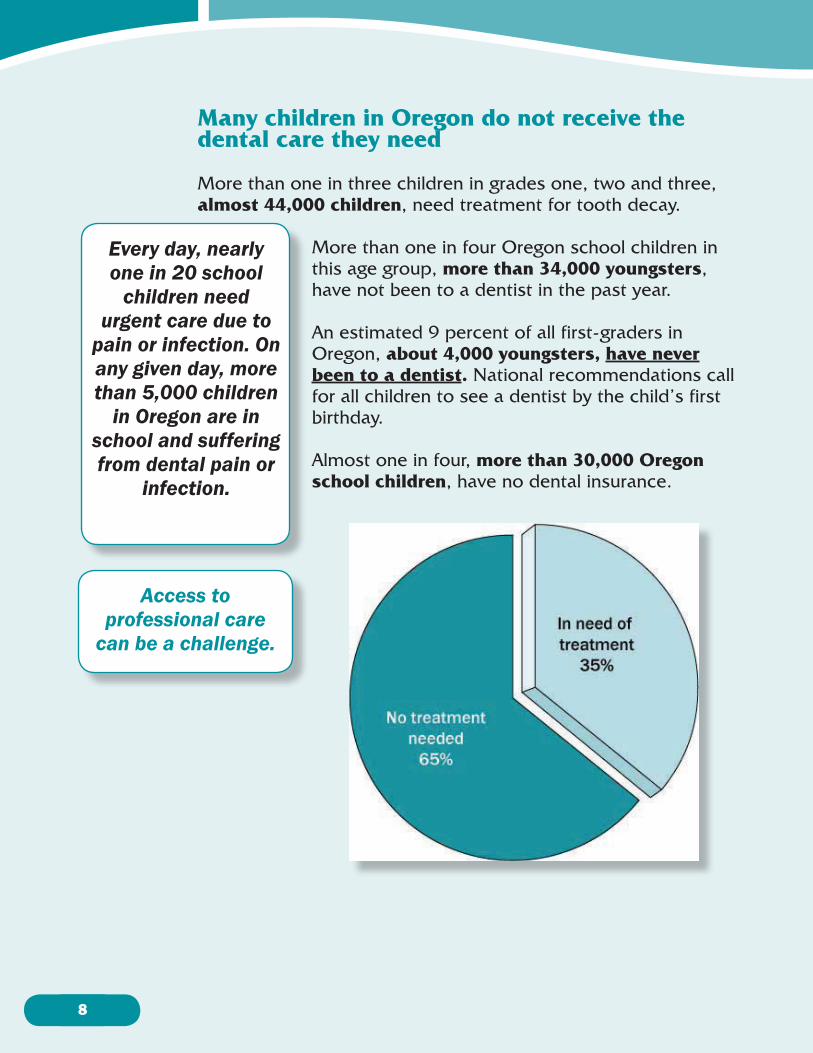
Many children in Oregon do not receive the dental care they need
More than one in three children in grades one, two and three, almost 44,000 children, need treatment for tooth decay.
More than one in four Oregon school children in this age group, more than 34,000 youngsters, have not been to a dentist in the past year.
An estimated 9 percent of all first-graders in Oregon, about 4,000 youngsters, have never been to a dentist. National recommendations call for all children to see a dentist by the child’s first birthday.
Almost one in four, more than 30,000 Oregon school children, have no dental insurance.
Every day, nearly one in 20 school
children need urgent care due to
pain or infection. On any given day, more than 5,000 children
in Oregon are in school and suffering from dental pain or
infection.
Access to professional care
can be a challenge.
9
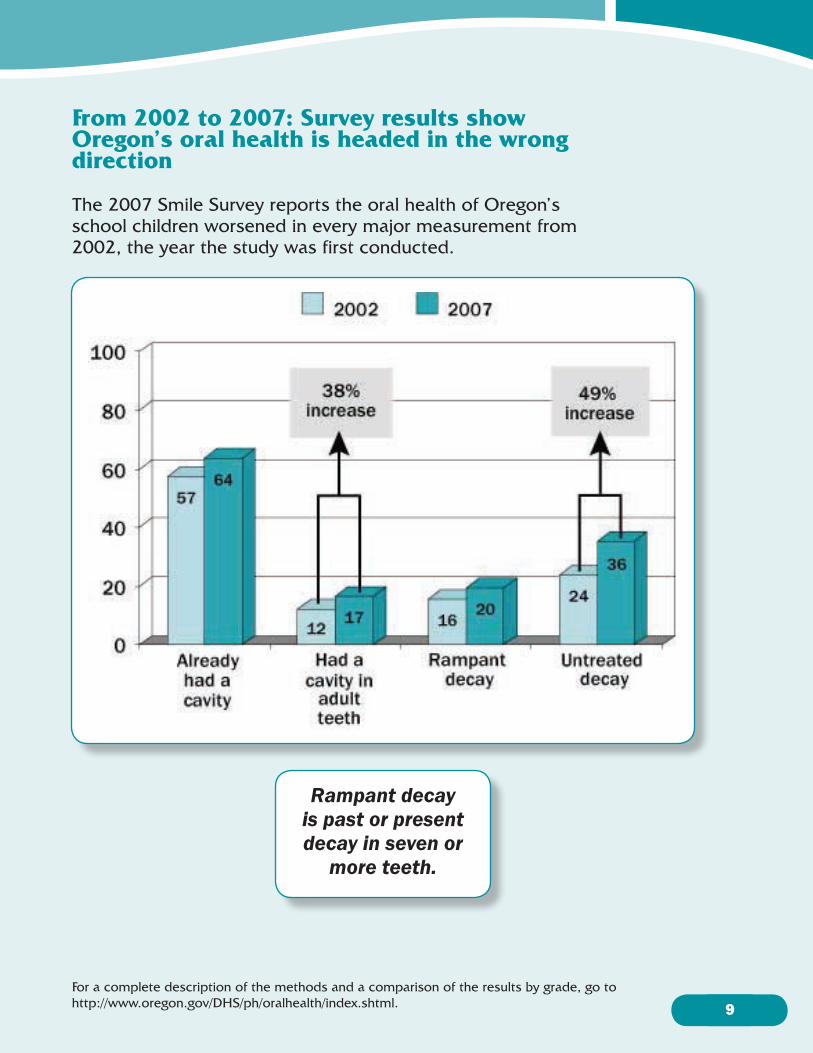
From 2002 to 2007: Survey results show Oregon’s oral health is headed in the wrong direction
The 2007 Smile Survey reports the oral health of Oregon’s school children worsened in every major measurement from 2002, the year the study was first conducted.
For a complete description of the methods and a comparison of the results by grade, go to http://www.oregon.gov/DHS/ph/oralhealth/index.shtml.
Rampant decay is past or present decay in seven or
more teeth.

10
The oral health of Oregon’s school children is poorer than that of children in neighboring states
Compared with neighboring states, Oregon has a higher rate of untreated decay among school children. In Oregon, almost two out of three first- through third-graders have already had a cavity. Furthermore, more than half of those children have untreated decay.
Preventing disease is always better than treating it. When dental decay occurs, prompt treatment is important. Left untreated, dental cavities can lead to severe pain or bacterial infection, which can cause additional tooth loss and other problems. The infection can become life-threatening if it spreads elsewhere in the body.
Nationally, Oregon ranks 25th –
seventh from the bottom – in the
percent of school children with
untreated decay.*
* Of the 32 states that report data using a similar method.
11
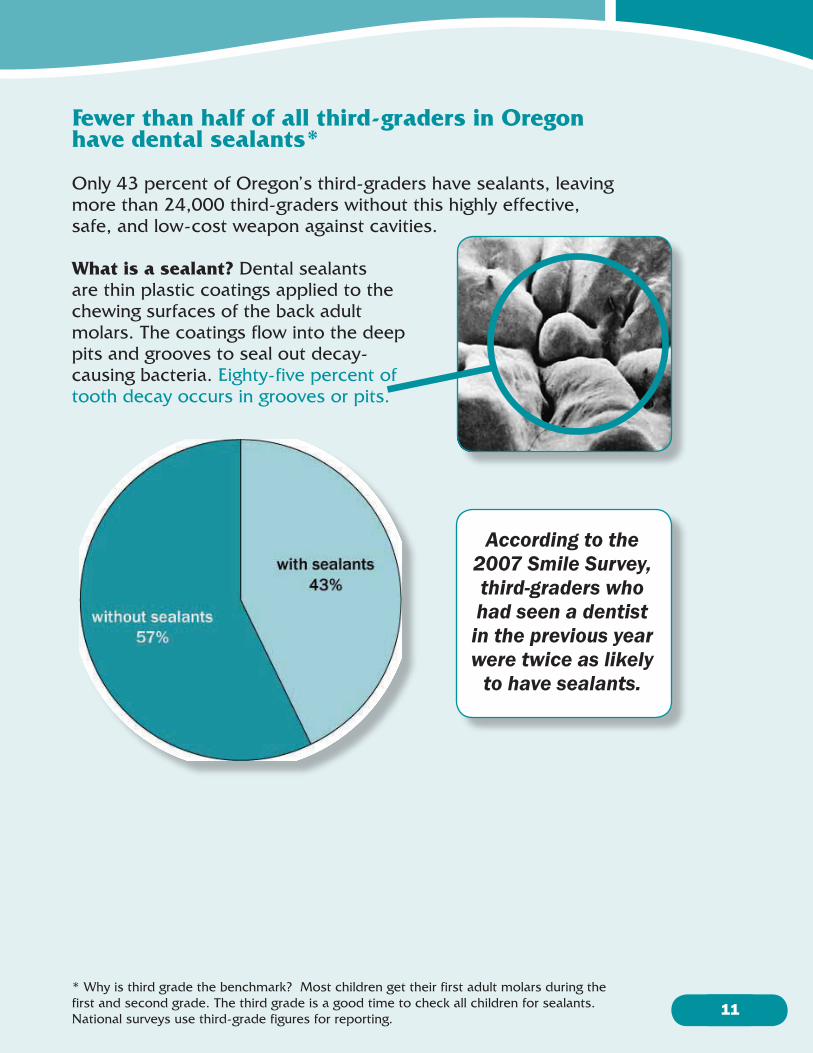
Fewer than half of all third-graders in Oregon have dental sealants*
Only 43 percent of Oregon’s third-graders have sealants, leaving more than 24,000 third-graders without this highly effective, safe, and low-cost weapon against cavities.
What is a sealant? Dental sealants are thin plastic coatings applied to the chewing surfaces of the back adult molars. The coatings flow into the deep pits and grooves to seal out decay-causing bacteria. Eighty-five percent of tooth decay occurs in grooves or pits.
According to the 2007 Smile Survey, third-graders who had seen a dentist in the previous year were twice as likely
to have sealants.
* Why is third grade the benchmark? Most children get their first adult molars during the first and second grade. The third grade is a good time to check all children for sealants. National surveys use third-grade figures for reporting.

12
Children living outside of metropolitan Portland* suffer from poorer oral health
Children in the Portland metropolitan area have less untreated tooth decay, are less likely to have ever had a cavity and are less likely to need urgent dental treatment.
In the Portland metropolitan area, more than half of third-graders – 51 percent – have sealants. Slightly less than a third of third-graders who live outside of the metropolitan area have sealants.
In the metropolitan area, one in 100 students require
urgent care due to pain or infection.
Outside of the metropolitan area, one in 17 students need urgent care.
* This report defines the Portland metropolitan area as Multnomah, Washington and Clackamas counties.

13
Children with dental insurance* have better oral health and access to care
One in four children do not have dental insurance. Oral disease and the care received for children with dental insurance compared to those without is strikingly different.
Insured school children have less untreated decay, are more likely to have sealants, and are more likely to have visited a dentist in the previous year.
* Data on dental insurance was extrapolated from questionnaires returned by 1,972 parents.

14
Low-income* children suffer from poorer oral health and have less access to care
The lowest income children, compared with the highest income, are more than twice as likely to have untreated decay, almost three times as likely to have rampant decay, and see the dentist annually 30 percent less of the time.
Information on household income was not collected in this survey. A proxy for income was used instead – the percent of children in a school that participate in the Federal Free and Reduced Lunch Program. Schools fell in to one of four categories:
Higher income < 25 percent •25.0 – 49.9 percent •50.0 – 74.9 percent •Lower income is ≥ 75 percent •
* Eligibility for the Free and Reduced Lunch Program is a household income at or below 130% (Free) and between 130–185% (Reduced) of the federal poverty level.

15
Racial and ethnic disparities ease
Comparing the 2007 Smile Survey results with those of 2002, there is evidence that oral disease disparities are easing to some degree.
Oral disease increased for school •children in every race/ethnicity category.Hispanic school children have •a disproportionately higher rate of oral disease than White, non-Hispanic school children.The rate of increase for some types •of oral disease increased more slowly among Hispanic children than among White, non-Hispanic school children.
16

17
Recommendations
Dental public health professionals have long championed the practice of disease prevention and health promotion on the part of individuals, health care providers and the community at large. The simple reason is these thoughtful approaches can significantly improve oral health. When efforts by individuals, providers and the community at large join to form partnerships, the outcome is even further enhanced. The Oregon Public Health Division recommends the following strategies that focus on public-private partnerships to address the issue of dental disease in children.
Improve the oral health of infants, children and adolescents •by setting guidelines for prevention and care.Improve the partnerships between dental professionals •and other health professionals to promote the oral health of children.Create partnerships between dental care professionals and •families to promote an understanding of the importance of oral health care. Create partnerships between dental care professionals and •public health professionals.Promote a seamless system of care that includes community- •based health education and preventive interventions.
There are four community-based preventive measures that have been proven effective in reducing tooth decay through partnerships between public health and the professional.
Community water fluoridation •Early-childhood cavities prevention programs •School-based fluoride supplement programs •School-based dental sealant programs •

18
Community water fluoridationWater fluoridation is the controlled addition of a fluoride compound to a public water supply to achieve a concentration optimal for tooth decay prevention. The practice of community water fluoridation has been recognized as one of the great public health achievements of the 20th century because of its impressive record of safety and effectiveness. Nearly 70 percent of U.S. citizens on public water supplies drink fluoridated water compared with less than 20 percent of Oregon residents. This ranks Oregon 48th out of 50 states. The Public Health Division advocates the fluoridation of community water supplies to reduce tooth decay.
Early-childhood cavities preventionDental treatment for pregnant women plus preventive care beginning as early as age one has been shown to reduce tooth decay in young children. The Public Health Division in partnership with dental and medical care providers supports early-childhood cavity prevention programs.
School-based fluoride supplement programsFor communities without community water fluoridation, participation in school-based fluoride supplement programs is recommended. The Public Health Division, partnering with elementary schools around the state, recommends and implements a school-based fluoride supplement program.
School-based dental sealant programsA dental sealant is a plastic coating applied to the chewing surfaces of molar teeth for the purpose of preventing tooth decay. School-based dental sealant programs have been shown to be a best practice in decay prevention. The Public Health Division, in partnership with communities, elementary schools, and dental care professionals, promotes and implements a school-based dental sealant program.


Oregon Department of Human ServicesPublic Health DivisionOral Health Program800 NE Oregon Street, Suite 825Portland, Oregon 97232www.oregon.gov/DHS/ph/oralhealth/