
oral mucosal diseases 2010
85
Wen Wen - - Chen Wang Chen Wang Common Oral Mucosal Diseases Assistant professor of Dept. of Oral Pathology, Faculty of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan Head of Dental Dept., Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan E-mail: [email protected] Wen-Chen Wang, DDS, MS, Ph.D
-
Upload
hai-trieu -
Category
Health & Medicine
-
view
12.520 -
download
0
Transcript of oral mucosal diseases 2010

WenWen--Chen WangChen Wang
Common Oral Mucosal Diseases
Assistant professor of Dept. of Oral Pathology, Faculty of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, TaiwanHead of Dental Dept., Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan E-mail: [email protected]
Wen-Chen Wang, DDS, MS, Ph.D
WenWen--Chen WangChen Wang
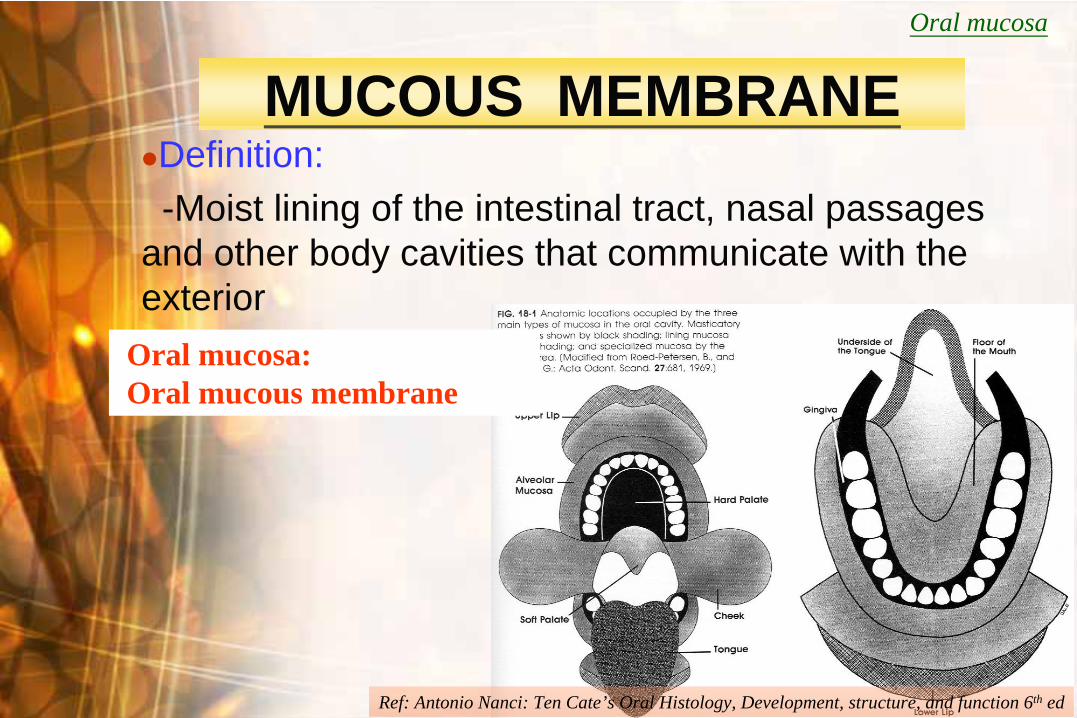
MUCOUS MEMBRANE
Definition:-Moist lining of the intestinal tract, nasal passages
and other body cavities that communicate with the exterior
Oral mucosa
Oral mucosa:Oral mucous membrane
Ref: Antonio Nanci: Ten Cate’s Oral Histology, Development, structure, and function 6th ed

WenWen--Chen WangChen Wang
STRUCTURE OF ORAL MUCOSA
Epithelium………………
..epidermis* Epithelial ridges, rete pegsLamina propria………...
..dermisSubmucosa……………...
..subcutaneous
Oral mucosa
--Similar to skinB.V. N.
Ref: BJ Orban:Orban’s oral histology and embryology,9th ed.
WenWen--Chen WangChen Wang
FUNCTIONAL CLASSIFICATION OF ORAL MUCOSA
Keratinized areas…Masticatory mucosa
hard palate & gingiva
vermilion border
Nonkeratinized areas…Lining or reflecting mucosa
lip, cheek, alveolar mucosa, vestibular fornix, mouth floor, soft palate, ventrum of tongue
Specialized mucosa
dorsum of tongue
Oral mucosa

WenWen--Chen WangChen Wang
FUNCTIONS OF ORAL MUCOSA
Protection
Sensation
Secretion
Thermal regulation
Oral mucosa
WenWen--Chen WangChen Wang
METHODS OF ORAL DIAGNOSIS
History taking
Inspection
Oral examination-Palpation-Percussion-Aspiration, -Auscultation
Radiographic examination
Laboratory examination

WenWen--Chen WangChen Wang
History Taking
What, where, when, how
Chief complaints
Present illness
Past medical historyFamily historySocial historyOccupational historyDental history
Review of symptoms by system

WenWen--Chen WangChen Wang
Chief Complaints
Pain
Soreness
Burning sensation
Bleeding
Loose teeth
Dry mouth
Swelling
Bad taste
Halitosis
Parthesia and anesthesia
Recent occlusal problem
Too much saliva
Delayed tooth eruption

WenWen--Chen WangChen Wang
1. Masses increase in size just before eating
ex. salivary retention phenomena, sialolithiasis
2. Slow-growing masses (duration of months to years)
1) Reactive hyperplasia 2) Chronic infection3) Cysts4) Benign tumors
Onset and Courses
WenWen--Chen WangChen Wang
3. Moderately rapid-growing masses (weeks to about 2 months)
1) Chronic infection2) Cysts 3) Malignant tumors

WenWen--Chen WangChen Wang
4. Rapidly growing masses (hrs to days)
1) Abscess (painful)2) Infected cyst (painful)3) Aneurysm4) Salivary retention phenomena 5) Hematomas
5. Masses with accompanying fever1) Infections2) lymphoma, leukemia

WenWen--Chen WangChen Wang
Inspection
Location
Contours
Color
Surfaces
WenWen--Chen WangChen Wang
ContoursNormal & variation
Masticatory mucosa vs lining mucosa
Color
WenWen--Chen WangChen Wang
Color
Normal: pinkish
Whitish :Epithelial hyperplasia, Hyperkeratosis
or dense collagen bundle
Reddish:atrophic epithelium、vessels dilatation
or hyperplasia
Blackish:nevus, tattoo, melanosis
Yellowish:Yellowish: adipose tissue, glandsadipose tissue, glands
Translucent blue :reflection of liquid
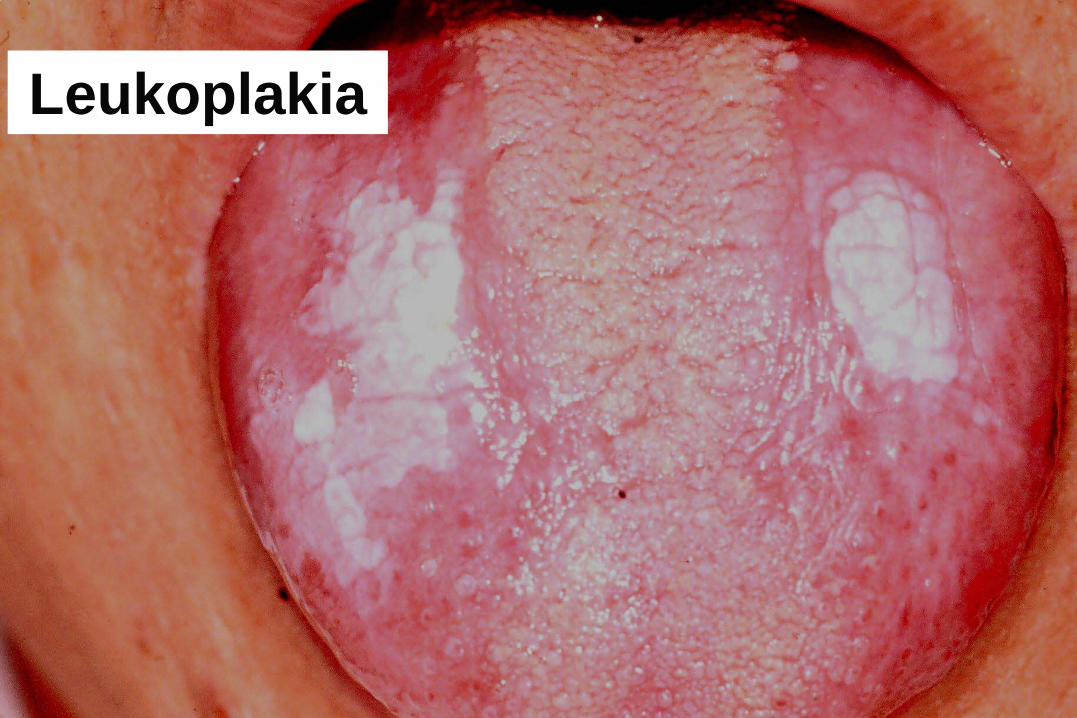
Leukoplakia
WenWen--Chen WangChen Wang
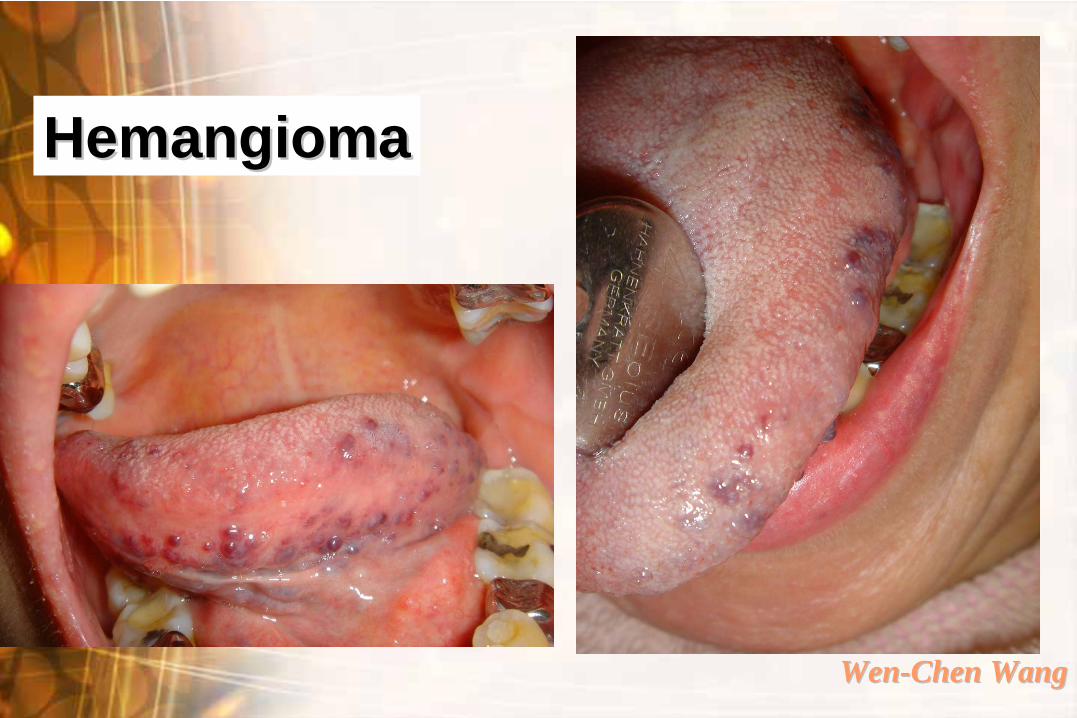
HemangiomaHemangioma

Peutz-Jegher’s syndrome
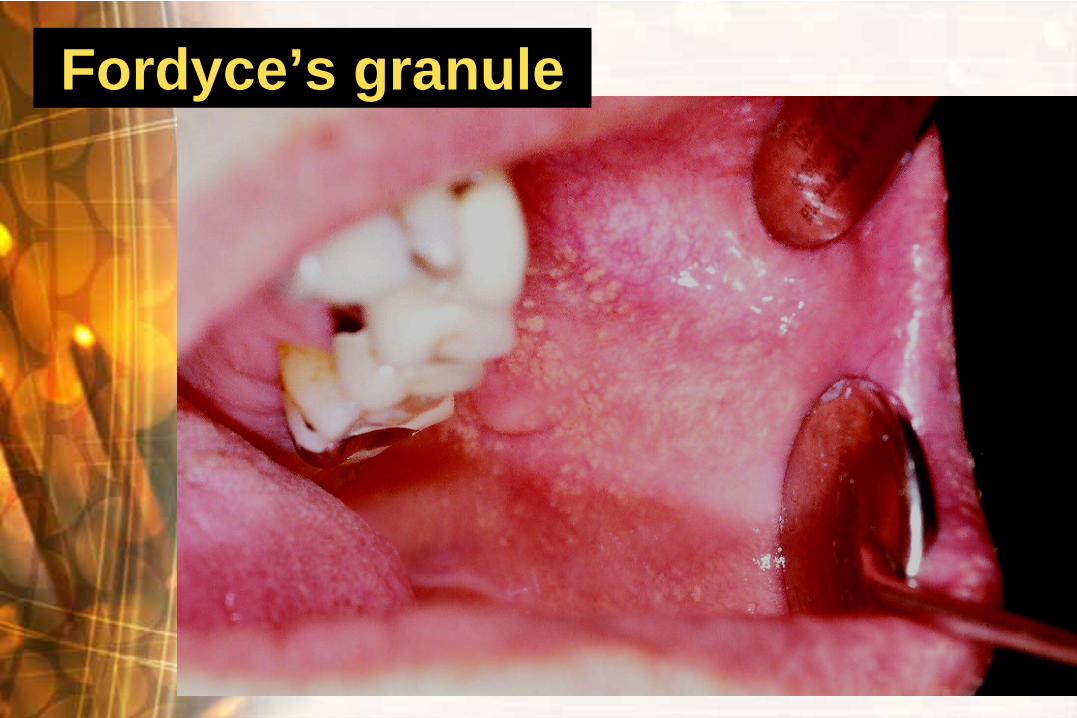
Fordyce’s granule

Mucocele
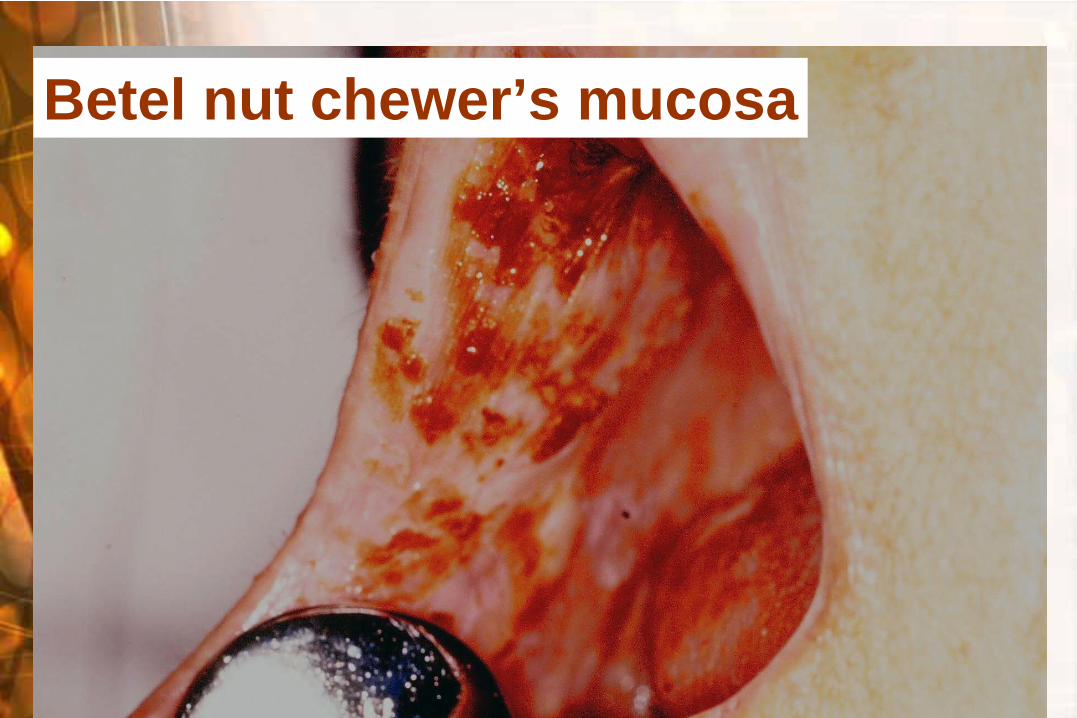
Betel nut chewer’s mucosa
WenWen--Chen WangChen Wang
Surfaces
Normal –smooth & glistening, except dorsal tongue, rugae & attached gingiva

WenWen--Chen WangChen Wang
Pathologic Mass May Be--
1) Smooth surface-arises beneath epi, originates from
mesenchyme
ex : benign & early maligant salivary gland tumors, benign & malig. mesenchymal T. ( fibroma, osteoma, hemangioma, myoma…), cellulitis, mucocele…

WenWen--Chen WangChen WangMixed tumor
irritation fibroma

WenWen--Chen WangChen Wang
2) Rough surface-except due to trauma, infection and maligancy, originates in the epithelium
ex: papilloma, VH V.ca, ulcerative & exophytic SCC
Ref: NK wood, PW Goaz: Differential diagnosis of oral and maxillofacial lesions 5th ed

WenWen--Chen WangChen Wang
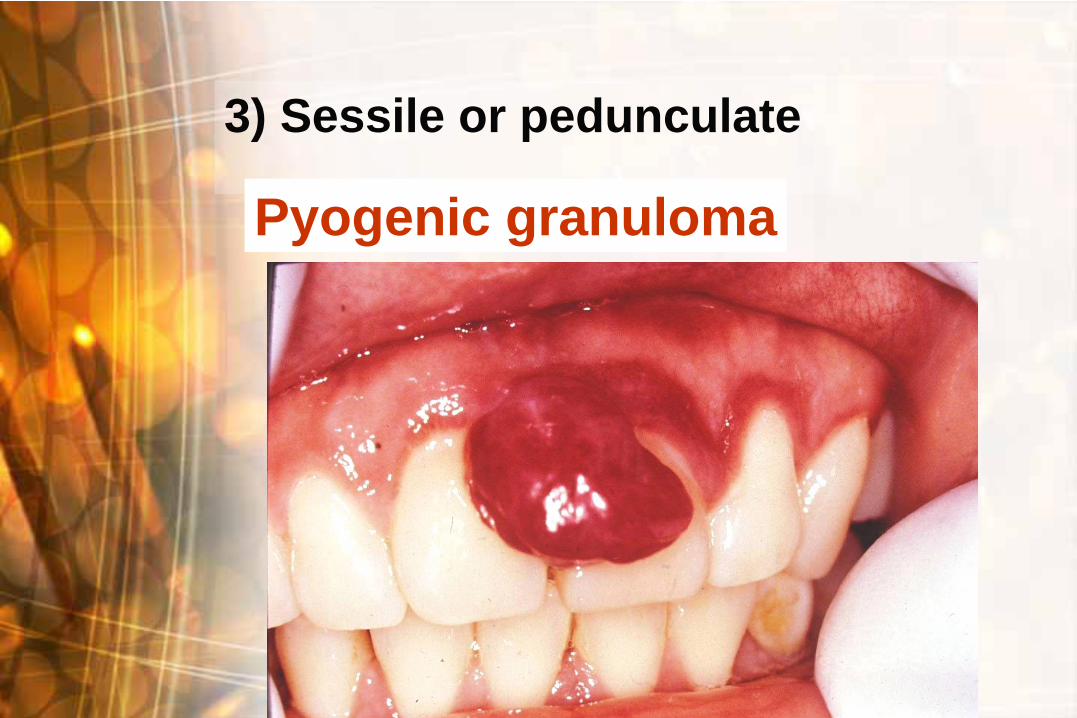
3) Sessile or pedunculate
Pyogenic granuloma

WenWen--Chen WangChen Wang
Palpation
--A third eye of clinical examination
Anatomic regions & planes involved
Mobility
Extent
Consistency
Painless, tender or painful
Unilateral or bilateral
Solitary or multiple

WenWen--Chen WangChen Wang
Anatomic Regions & Planes Involved
Locates a firm mass, superficial or deep
Difficult if swelling or painful
WenWen--Chen WangChen Wang
Mobility
1. free movable2. fixed to skin but not to the
underlying tissue 3. free movable to the skin but
fixed to the underlying tissue

WenWen--Chen WangChen Wang
4. bound to both skin or mucosa and to the underlying tissue
1) fibrosis-after a previous inflammation.2) malignant- from skin or mucosa invade
to underlying tissue 3) malignant- from deeper tissue invade to
surface epithelium4) malignant- from loose CT to both the
superficial & the deeper layers

WenWen--Chen WangChen Wang
Extent
Whether a mass has well defined, M-D or P-D borders will depend on :
-Border of the mass -Consistency of surrounding tissue -Thickness of overlying tissue -Sturdiness of underlying tissue
WenWen--Chen WangChen Wang
Fluctuation & emptiability: Fluid contented lesion
Soft: vein, loose CT, glandular tissue
Cheesy: sebaceous cyst, epidermoid cyst
Rubbery: relaxed muscle, glandular tissue with capsule, arteries
Firm: fibrous tissue, tensed muscle, large nerve
Bony hard: bone, cartilage, tooth structure
Consistency

WenWen--Chen WangChen Wang
Torus palatini

WenWen--Chen WangChen Wang
Painless, Tender or Painful
Pain1.inflammation-- mechanical trauma or
infection2.painful tumors--some neural tumors3.sensory nerve encroachmentTendernessLow-grade inflammation & internal pressure, chronic infection

WenWen--Chen WangChen Wang
Unilateral or bilateral
Solitary or multiple
•Solitary : A local benign or early malignancy
•Multiple : Systemic, disseminated diseases or syndrome

WenWen--Chen WangChen Wang
Erosive Lichen planus

WenWen--Chen WangChen Wang
Special Examination
Radiographic exam
Aspiration, smear cytological exam., biopsy
Laboratory exam…
(Suggested by attending drs.)

WenWen--Chen WangChen Wang
Common Oral Mucosal Diseases

WenWen--Chen WangChen Wang
Ulcerative Lesions
Ulcer-epithelium loss caused by any reason
Trauma, burn, infection, oral cancer…
Most of traumatic ulcers would be healed within 2 weeks spontaneously, otherwise, a further evaluation should be necessary.
WenWen--Chen WangChen Wang
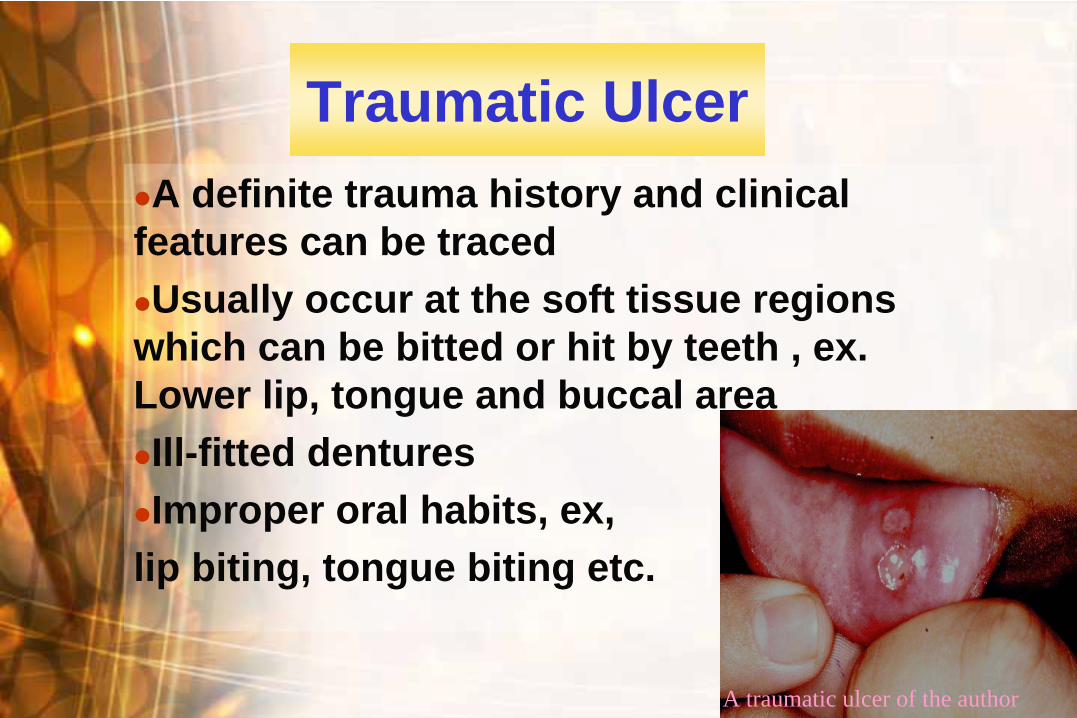
Traumatic Ulcer
A definite trauma history and clinical
features can be traced
Usually occur at the soft tissue regions
which can be bitted or hit by teeth , ex. Lower lip, tongue and buccal area
Ill-fitted dentures
Improper oral habits, ex,
lip biting, tongue biting etc.
A traumatic ulcer of the author

WenWen--Chen WangChen Wang
Burn
Chemicals or drugs, thermal
Suicide, psychiatric problems,
Placement an aspirin tablet in oral to relieve
toothache
Phenol, H2 O2 , NaHOCl used in dental practice

WenWen--Chen WangChen Wang
Recurrent Aphthous Ulcer
Commonest oral mucosal disease
Herpetiform RAU
WenWen--Chen WangChen Wang
Patients Can Be Grossly Classified As : 1.Primary immune dysregulation
-genetic, stress, congenital or acquired immunal disease (leukopenia, AIDS, endocrine etc. )
2.Decreased mucosal barrier-Trauma, blood diseases, nutritional
defficiency(Vit.B12、follic acid, iron)3. Increased antigenic expose-Bacteria, virus, etc.
WenWen--Chen WangChen Wang
Treatment of RAU
Topical steroid or NSAID therapy, local cauterization
Underline diseases or any possible etiology should be evaluated if suffered severely and recurred very often
WenWen--Chen WangChen Wang
Tuberculosis (TB)
Worldwide, chronic infectious disease, airborne droplets
Crowded or unsanitary environment
Opportunity infection, 5-10% progress into active disease
Immunocompromised patients, ex. DM, HIV infection
WenWen--Chen WangChen Wang
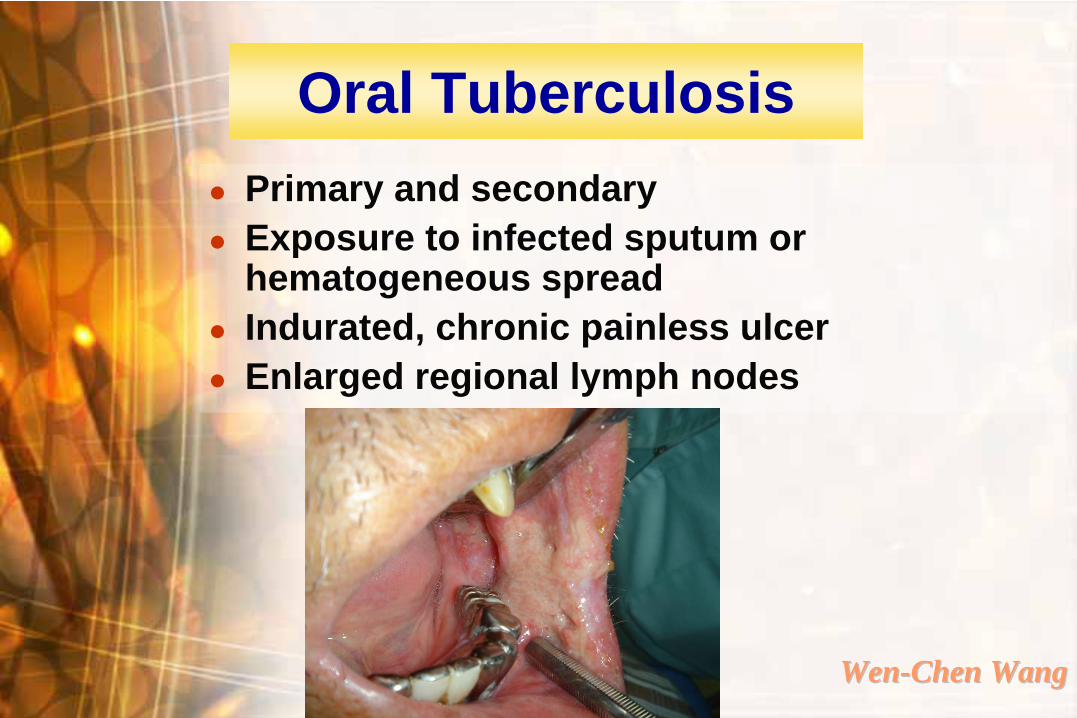
Oral Tuberculosis
Primary and secondary
Exposure to infected sputum or hematogeneous spread
Indurated, chronic painless ulcer
Enlarged regional lymph nodes

WenWen--Chen WangChen Wang
Herpes Simplex Virus Infection (HSV type 1)
Airborne droplets or direct contact
Primary and recurrent
Most primary HSV infections are asymptomatic, some suffered from primary herpetic gingivostomatitis
Usually in children and young adults

WenWen--Chen WangChen Wang
Clinical Characters of HSV Infection
Primary-upper respiratory tract infection oral symptoms,small vesicles/tiny ulcers Latency
Secondary- reactivation of latent virus after trauma, menstruation, systemic upsets, etc.
WenWen--Chen WangChen Wang
A discrete collection of vesicular swellings rupture erosion crusted
The commonest recurrent lesion is herpes labialis.
Attached gingiva, hard palate
Heal within 1-2 weeks without scarring
Secondary HSV Infection

WenWen--Chen WangChen Wang
Recurrent HSV infection

WenWen--Chen WangChen Wang
Oral White Lesions and Betel Nut Related Lesions

WenWen--Chen WangChen Wang
Lichen Planus
Reticular type (lace-like network of white lines, Wickham’s striae)
Erosive type
Asymptomatic or burning irritation in reticular type, symptomatic in erosive type
Middle-aged, F:M=3:2
Idiopathic, stress
Topical or systemic steroid therapy
Malignant potential is controversial

Lichen planus

WenWen--Chen WangChen Wang
Oral Candidiasis
Oral normal flora
Local irritation( ill-fitting or improper denture hygiene)
Antibiotics
Immuno-compromised, systemic disease patients
Complete denture of upper jaw

WenWen--Chen WangChen Wang
Oral Candidiasis
Oral manifestation:
Pseudomembranous type--creamy white
Atrophytic type-- reddish
Symptoms: varied, from mild to burning sensation, pain and dysphagia
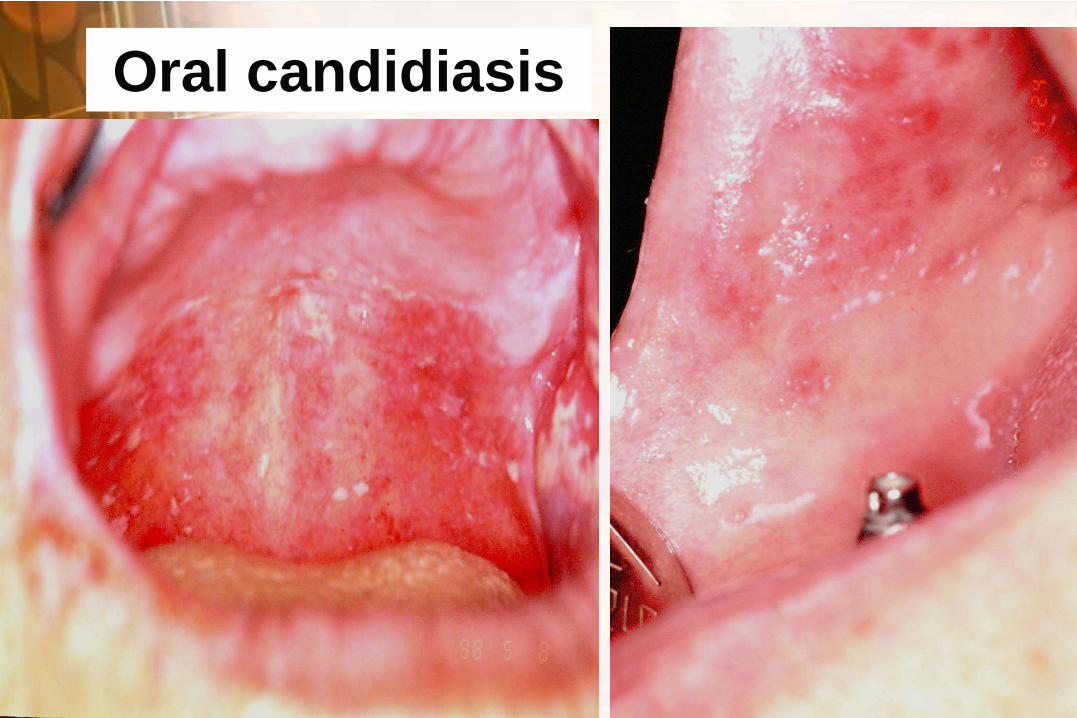
Oral candidiasis

WenWen--Chen WangChen Wang
Oral Cancer and Precancerous Lesions -Related to Betel Quid Chewing Habits

WenWen--Chen WangChen Wang
What is oral cancer?
WenWen--Chen WangChen Wang
Any cancer found in oral cavity
A cancer of the oral epithelial origin, ex. squamous cell carcinoma, verrucous carcinoma
Oral Cancer is-

WenWen--Chen WangChen Wang
Contributing factors of oral cancer?
Who is in high risk ?
WenWen--Chen WangChen Wang
Contributing Factors of Oral Cancer
--In betel nut (betel quid) consumption areas
Betel nut chewing habit ( 80% in Taiwan)
Others are:1. smoking 2. alcoholism3. radiation exposure 4. improper nutrition5. syphilis 6. candidiasis7. mutation of gene 8. immunodeficiency 9. improper denture
WenWen--Chen WangChen Wang
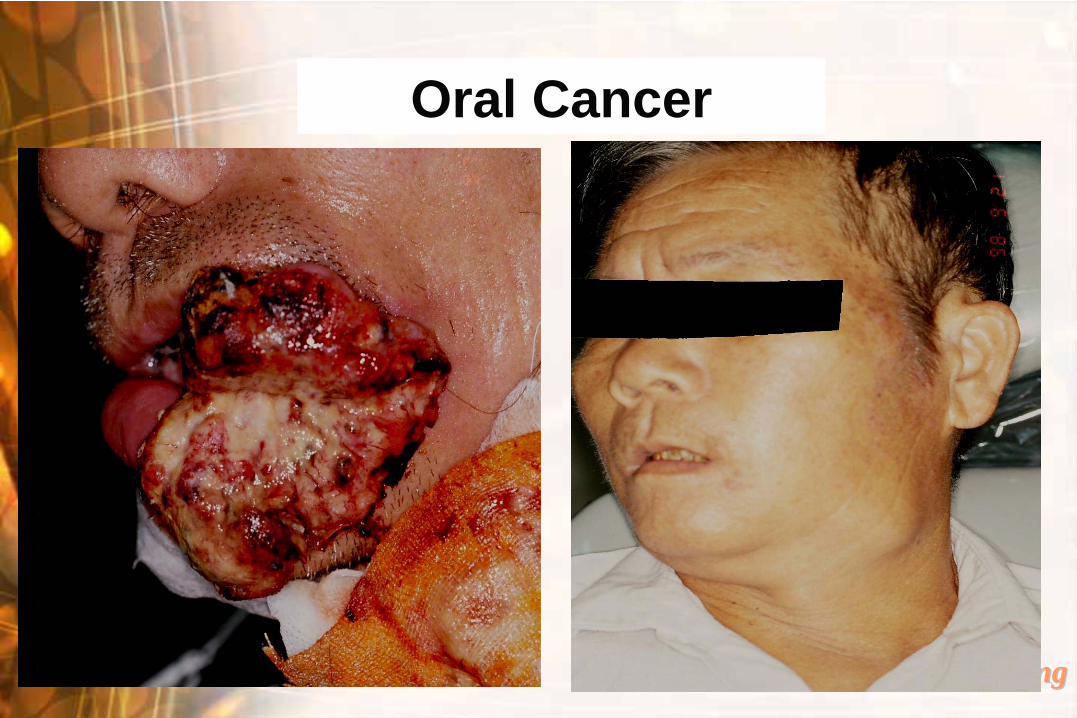
Oral Cancer
Early: may be a leukoplakia or erythroplakia
Tumor cells invade into connective tissue or grow exophytically
Clinical features: reddish or whitish ulcerative surfaces with induration, delayed healing process

WenWen--Chen WangChen Wang
Oral Cancer
Locations:
In Taiwan : buccal mucosa is the most common, followed by lateral border of tongue, retromolar, lower lip, palate and gingiva
In the world: lateral border of tongue is the most common

WenWen--Chen WangChen Wang
Oral Cancer
WenWen--Chen WangChen Wang
Oral Cancer

WenWen--Chen WangChen Wang
Visit your dentist as soon as possible if any oral ulcer doesn’t heal within 2 weeks !

WenWen--Chen WangChen Wang
What are Oral Precancerous Lesions ?

WenWen--Chen WangChen Wang
Oral Precancerous Lesions
Leukoplakia
Erythroleukoplakia
Erythroplakia
Oral submucous fibrosis
Verrucous hyperplasia
Erosive lichen planus*
*precancerous condition
WenWen--Chen WangChen Wang
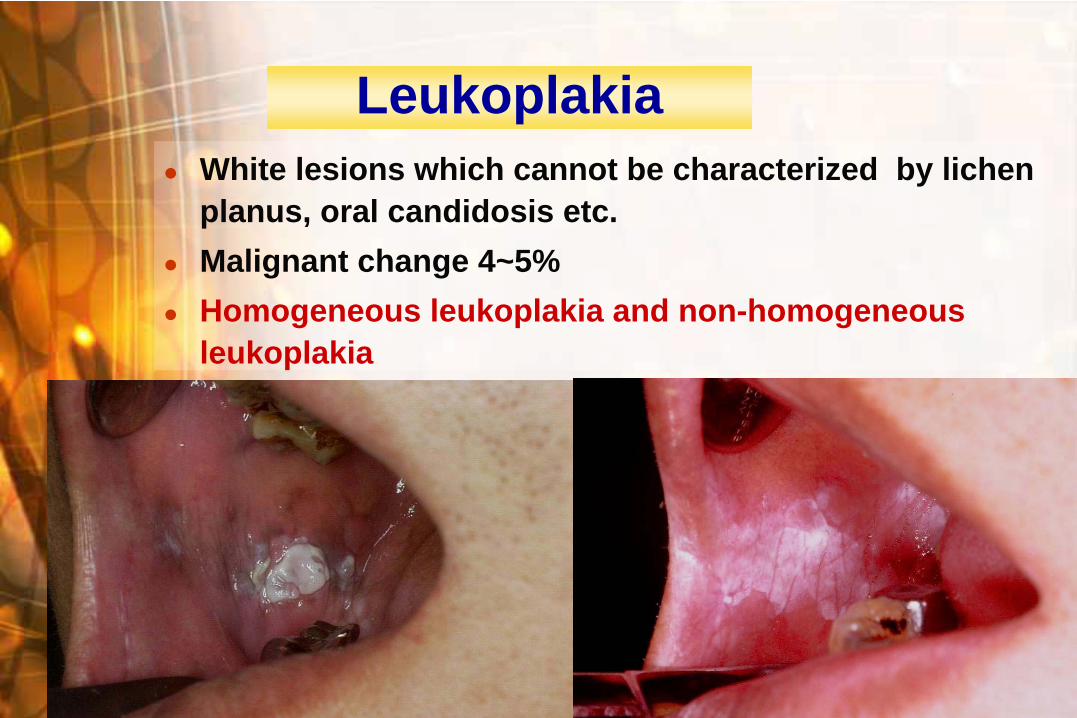
Leukoplakia
White lesions which cannot be characterized by lichen planus, oral candidosis etc.
Malignant change 4~5%
Homogeneous leukoplakia and non-homogeneous leukoplakia

WenWen--Chen WangChen Wang
Erythroleukoplakia
WenWen--Chen WangChen Wang
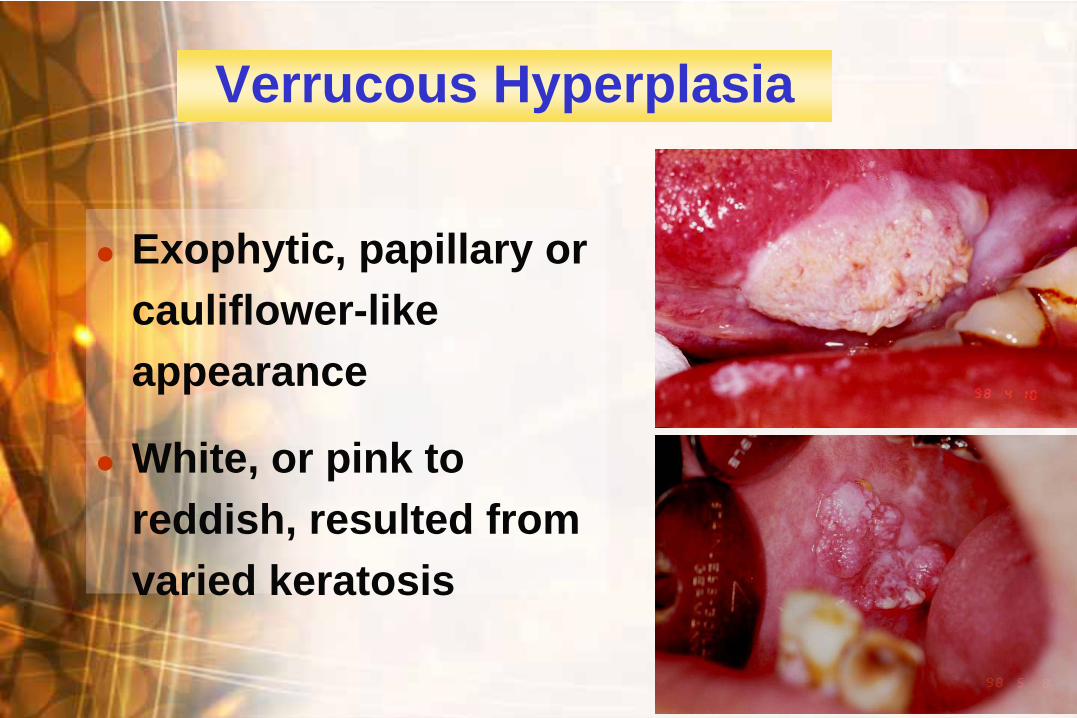
Verrucous Hyperplasia
Exophytic, papillary or cauliflower-like appearance
White, or pink to reddish, resulted from varied keratosis

WenWen--Chen WangChen Wang
20-40 y/o, male
Sites: oral mucosa, oropharynx, esophagus
Clinical characteristics:
-Dense collagen bundles, decreased vascularity, epithelium atrophy, whitening of the mucosa
-Trismus-Epithelium atrophy→ decreased protection,
sensitive to spicy foods
Oral Submucous Fibrosis (OSF)

WenWen--Chen WangChen Wang
Oral submucous fibrosis

WenWen--Chen WangChen Wang
Oral submucous fibrosis
WenWen--Chen WangChen Wang
Managements of OSF
Mouth opening exercise
Local cortical steroid injection
Surgical treatment combined with skin graft
Prognosis is not good in the severe OSF
patients

WenWen--Chen WangChen Wang
Oral Manifestations of Systemic Diseases

WenWen--Chen WangChen Wang
Burning Mouth Syndrome (BMS)
Bacterial or fungal infection
Dry mouth
Nutritional abnormality
Anemia
Endocrine disturbance, DM
Improper denture
Idiopathic
WenWen--Chen WangChen Wang
Clinical Features of BMS
Middle aged female or elder male
Burning sensation, esp. tongue and tongue tip; taste change
Normal appearance and color
Diagnosis and treatment depend on the etiology

WenWen--Chen WangChen Wang
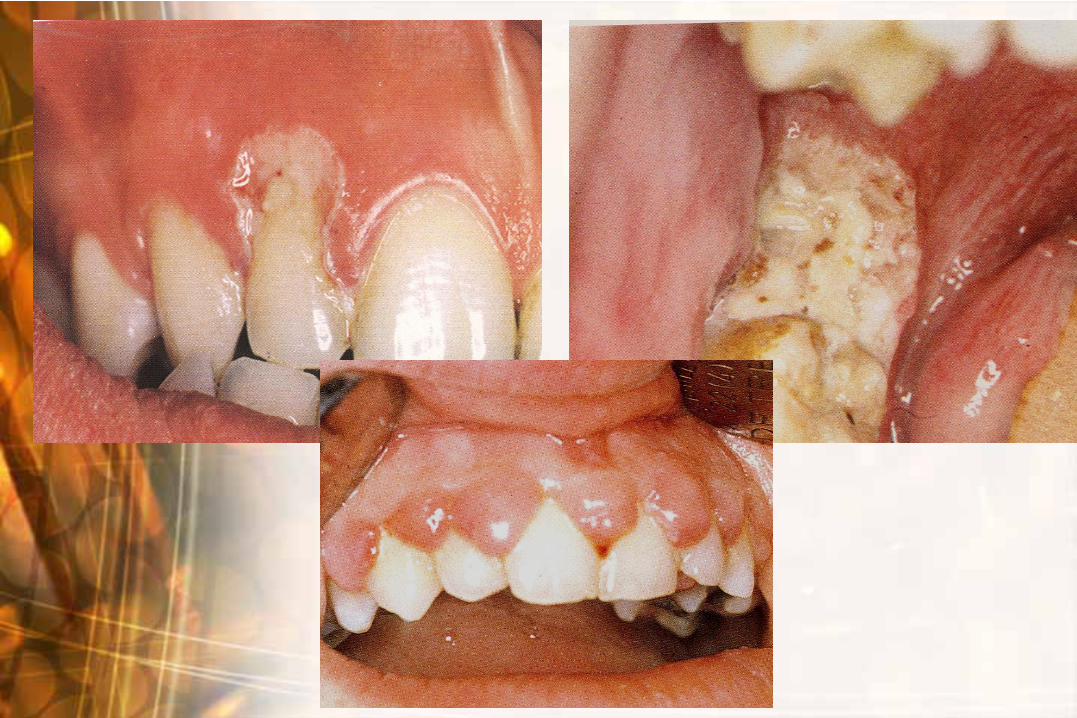
Vitamin Deficiency
Vit. A: keratosis
Vit. B: glossitis, angular cheilitis, burning mouth
Vit. C: generalized gingival swelling, bleeding tendency and ulcers, periodontitis

WenWen--Chen WangChen Wang
Vit. B12 deficiency
After treatment

WenWen--Chen WangChen Wang
Blood Diseases
Anemia-pale mucosa
Hemophilia-hematoma or petechiae
Coagulation problems associated with impaired liver function

WenWen--Chen WangChen Wang
Leukemia
Bleeding tendency
Idiopathic oral ulcers, necrotic gingival margin
Gingival swelling (chloroma)
Oral candidosis

WenWen--Chen WangChen Wang
Go for an oral and
dental examination
every 6 months!

WenWen--Chen WangChen Wang
References1. Antonio Nanci: Ten Cate's Oral Histology,
Development, structure, and function 6th ed. 2. BJ Orban:Orban's oral histology and
embryology,9th ed.3. NK wood, PW Goaz: Differential diagnosis of oral
and maxillofacial lesions 5th ed.4. BW Neville, DD Damm, CM Allen,JE Bouquot: Oral &
Maxillofacial pathology. 2nd ed.
Acknowledgement Clinical pictures were fully supported by Dept. of Oral Pathology, Kaohsinug Medical University
http://www.kmu.edu.tw/media/photos/001.jpg
Kaohsiung Medical University


















