ORAL MANIFESTATIONS OF SYSTEMIC DISEASES Dr.Shahzadi Tayyaba Hashmi [email protected].
Upload
ramesh-parajuliCategory
view
46download
2
Oral Manifestations of Oral Manifestations of Systemic DiseasesSystemic Diseases
Dr.Ramesh Parajuli MS(Otorhinolaryngology,Head and Neck surgery)Dr.Ramesh Parajuli MS(Otorhinolaryngology,Head and Neck surgery)Chitwan Medical College Teaching Hospital, Bharatpur-10, Chitwan, NepalChitwan Medical College Teaching Hospital, Bharatpur-10, Chitwan, Nepal
Oral cavity- window to the bodyOral cavity- window to the body
Lesions of oral mucosa, tongue, Lesions of oral mucosa, tongue, gingiva, dentition, periodontium, gingiva, dentition, periodontium, salivary gland, facial skeleton, & salivary gland, facial skeleton, & extraoral skinextraoral skin
Appropriate diagnosis & Appropriate diagnosis & treatmenttreatment

ClassificationClassification
1.Systemic Infectious diseases 1.Systemic Infectious diseases
2.Connective tissue disorders2.Connective tissue disorders
3.Granulomatous diseases3.Granulomatous diseases
4.Gastrointestinal diseases4.Gastrointestinal diseases
5.Respiratory diseases5.Respiratory diseases
6.Haematological diseases6.Haematological diseases
7.Endocrine diseases7.Endocrine diseases
8.Neurologic diseases8.Neurologic diseases
9.Nutritional deficiency9.Nutritional deficiency
10.Immunodeficiency diseases10.Immunodeficiency diseases
11.Drug reactions/radiotherapy11.Drug reactions/radiotherapy
12.Dermatological diseases12.Dermatological diseases
13.Metabolic disorders13.Metabolic disorders
14.Neoplastic diseases14.Neoplastic diseases
Infective diseasesInfective diseases
1.Viral infection1.Viral infection
2.Bacterial infection2.Bacterial infection
3.Fungal infection3.Fungal infection
4.Protozoal infection4.Protozoal infection
Viral infectionsViral infections
1.Herpes Simplex Stomatitis1.Herpes Simplex Stomatitis2.Herpes Zoster2.Herpes Zoster3.Herpangina 3.Herpangina 4.Hand Foot Mouth Disease4.Hand Foot Mouth Disease5.Cytomegalovirus Infection5.Cytomegalovirus Infection6.Measles6.Measles7.Infectious Mononucleosis7.Infectious Mononucleosis8.Mumps8.Mumps9.HIV9.HIV

Herpes Simplex StomatitisHerpes Simplex Stomatitis
HSV-1HSV-1: : Primary herpetic GingivostomatitisPrimary herpetic Gingivostomatitis Recurrent herpes labialisRecurrent herpes labialis HSV-2HSV-2:: Primary herpetic Gingivostomatitis:Primary herpetic Gingivostomatitis: -most frequent cause of acute stomatitis in -most frequent cause of acute stomatitis in
children children -varies in severity, many infections --varies in severity, many infections -
subclinicalsubclinical -misdiagnosed as “teething”-misdiagnosed as “teething” -malaise, anorexia, irritability, fever, -malaise, anorexia, irritability, fever,
anterior cervical lymphadenopathy, diffuse, anterior cervical lymphadenopathy, diffuse, purple, boggy gingivitis purple, boggy gingivitis
-multiple vesicles -multiple vesicles scarred ulcers(1-3mm)scarred ulcers(1-3mm) -occasionally in adults-occasionally in adults

Diagnosis:Diagnosis:
-clinically-clinically
-scrapping or smears from the lesion-scrapping or smears from the lesion
-immunofluorescent staining-immunofluorescent staining
-exfoliative cytology- typical -exfoliative cytology- typical multinucleated giant cellsmultinucleated giant cells
Treatment:Treatment:
-symptomatic-symptomatic
-acyclovir (systemic)-severe cases-acyclovir (systemic)-severe cases

Recurrent Intraoral Herpes Simplex InfectionRecurrent Intraoral Herpes Simplex Infection::
-may affect healthy individual-may affect healthy individual
-persistent lesions in immunocompromised-persistent lesions in immunocompromised
--chronic ulcer, raised, white borderchronic ulcer, raised, white border
-esp. at sites of trauma-esp. at sites of trauma
-acyclovir-acyclovir

Herpes zoster (Shingles)Herpes zoster (Shingles)
Reactivation of Varicella –Zoster virusReactivation of Varicella –Zoster virus Predisposing factor: Predisposing factor:
Immunocompromised statusImmunocompromised status One dermatome affected (trigeminal One dermatome affected (trigeminal
nerve)nerve) UnilateralUnilateral Ulcers in the distribution of dermatomeUlcers in the distribution of dermatome Mandibular nerve: ulceration of one side Mandibular nerve: ulceration of one side
of tongue, floor of the mouth, lower labial of tongue, floor of the mouth, lower labial & buccal mucosa& buccal mucosa
Maxillary nerve: one side of palate, the Maxillary nerve: one side of palate, the upper gingiva, buccal sulcusupper gingiva, buccal sulcus
Lesions persists for 2-3 wksLesions persists for 2-3 wks
Lesions on lips and chin
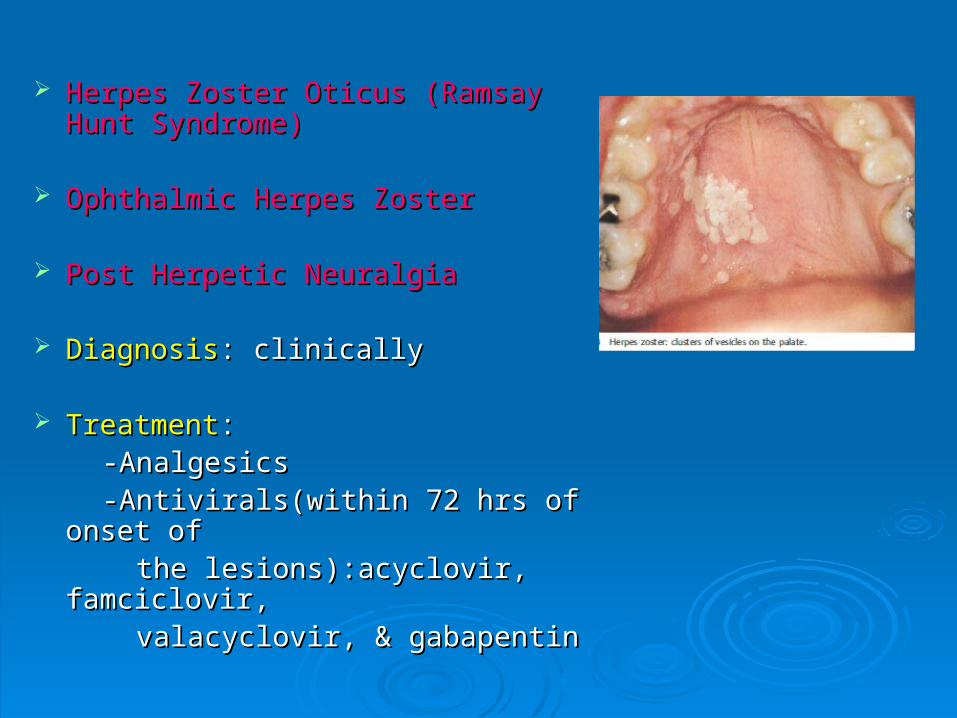
Herpes Zoster Oticus (Ramsay Herpes Zoster Oticus (Ramsay Hunt Syndrome)Hunt Syndrome)
Ophthalmic Herpes ZosterOphthalmic Herpes Zoster
Post Herpetic NeuralgiaPost Herpetic Neuralgia
DiagnosisDiagnosis: clinically: clinically
TreatmentTreatment:: -Analgesics-Analgesics -Antivirals(within 72 hrs of onset of-Antivirals(within 72 hrs of onset of the lesions):acyclovir, famciclovir, the lesions):acyclovir, famciclovir, valacyclovir, & gabapentinvalacyclovir, & gabapentin

HerpanginaHerpangina
Common in childrenCommon in children Coxsackie virus group A, Coxsackie virus group A,
Enteroviruses(30 & 71)Enteroviruses(30 & 71) Self limiting vesicular eruptions in Self limiting vesicular eruptions in
the oropharynx eg. soft palate, the oropharynx eg. soft palate, uvula, tonsillar pillars, posterior uvula, tonsillar pillars, posterior pharyngeal wallpharyngeal wall
Similar to herpes simplex except Similar to herpes simplex except the lesions more commonly in the lesions more commonly in oropharynx rather than oral cavityoropharynx rather than oral cavity
Diagnosis:Diagnosis: Clinically Clinically Treatment:Treatment: Supportive Supportive
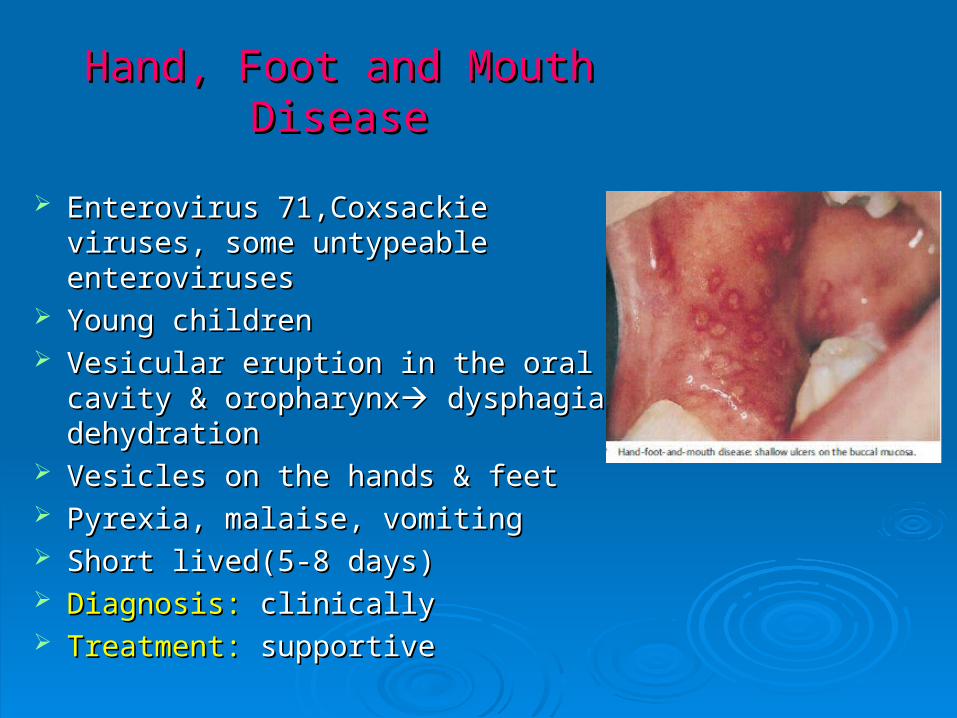
Hand, Foot and Mouth DiseaseHand, Foot and Mouth Disease
Enterovirus 71,Coxsackie viruses, Enterovirus 71,Coxsackie viruses, some untypeable enterovirusessome untypeable enteroviruses
Young childrenYoung children Vesicular eruption in the oral cavity & Vesicular eruption in the oral cavity &
oropharynxoropharynx dysphagia, dehydration dysphagia, dehydration Vesicles on the hands & feetVesicles on the hands & feet Pyrexia, malaise, vomitingPyrexia, malaise, vomiting Short lived(5-8 days)Short lived(5-8 days) Diagnosis:Diagnosis: clinically clinically Treatment:Treatment: supportive supportive
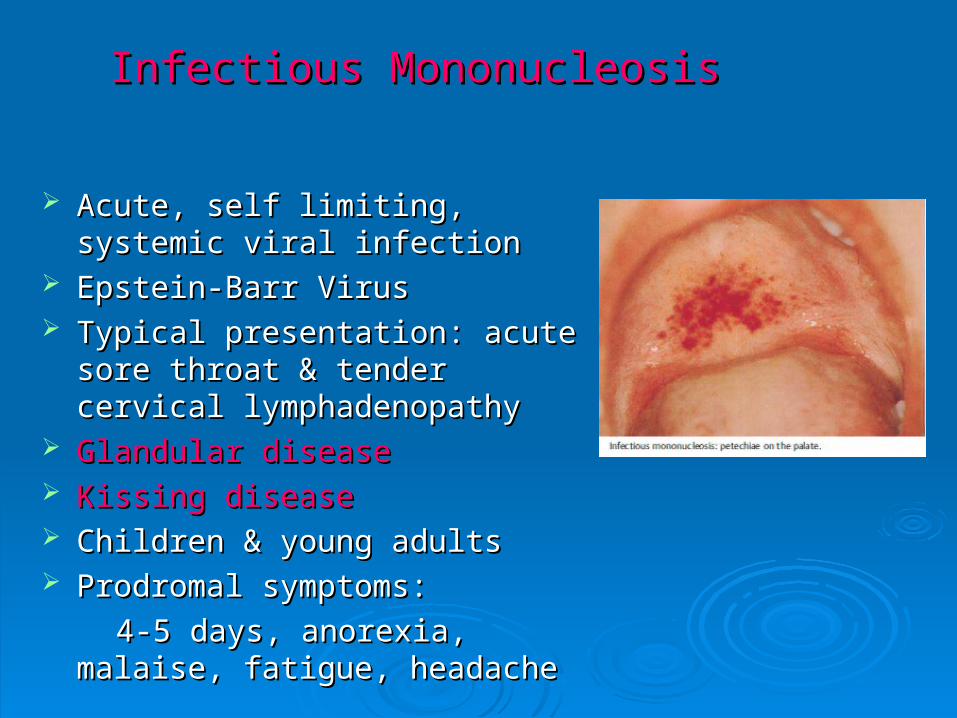
Infectious MononucleosisInfectious Mononucleosis
Acute, self limiting, systemic viral Acute, self limiting, systemic viral infectioninfection
Epstein-Barr VirusEpstein-Barr Virus Typical presentation: acute sore Typical presentation: acute sore
throat & tender cervical throat & tender cervical lymphadenopathylymphadenopathy
Glandular diseaseGlandular disease Kissing diseaseKissing disease Children & young adultsChildren & young adults Prodromal symptoms: Prodromal symptoms:
4-5 days, anorexia, malaise, 4-5 days, anorexia, malaise, fatigue, headachefatigue, headache
Clinical features:-Clinical features:- Oral manifestationsOral manifestations - early and common- palatal - early and common- palatal
petechiae, uvular edema, tonsillar exudate, gingivitis, petechiae, uvular edema, tonsillar exudate, gingivitis,
& rarely ulcers & rarely ulcers -Generalized lymphadenopathy, hepatosplenomegaly, -Generalized lymphadenopathy, hepatosplenomegaly,
maculopapular skin rashmaculopapular skin rash
Laboratory testsLaboratory tests:: Heterophile antibody(Paul Bunnel test, Monospot test)Heterophile antibody(Paul Bunnel test, Monospot test)
Treatment:Treatment: -Mild to moderate cases: Symptomatic-Mild to moderate cases: Symptomatic -Severe disease: Famciclovir-Severe disease: Famciclovir Anti-EBV compounds: MaribavirAnti-EBV compounds: Maribavir
Ampicillin based antibiotics should be avoidedAmpicillin based antibiotics should be avoided

Cytomegalovirus InfectionCytomegalovirus Infection
Relatively rare Relatively rare Cytomegalovirus (CMV)Cytomegalovirus (CMV) HIV infection and immunocompromisedHIV infection and immunocompromised
Clinical features:Clinical features: asymptomaticasymptomatic Oral lesionsOral lesions -nonspecific painful -nonspecific painful
ulcerations- gingiva & tongueulcerations- gingiva & tongue -Enlargement of parotid & -Enlargement of parotid &
submandibular glands, dry mouth, submandibular glands, dry mouth, fever, malaise, myalgia, headachefever, malaise, myalgia, headache
Laboratory tests: Laboratory tests: HPE/ImmunochemistryHPE/Immunochemistry Treatment: Treatment: -Resolve spontaneously-Resolve spontaneously -Ganciclovir (Persistent case)-Ganciclovir (Persistent case)
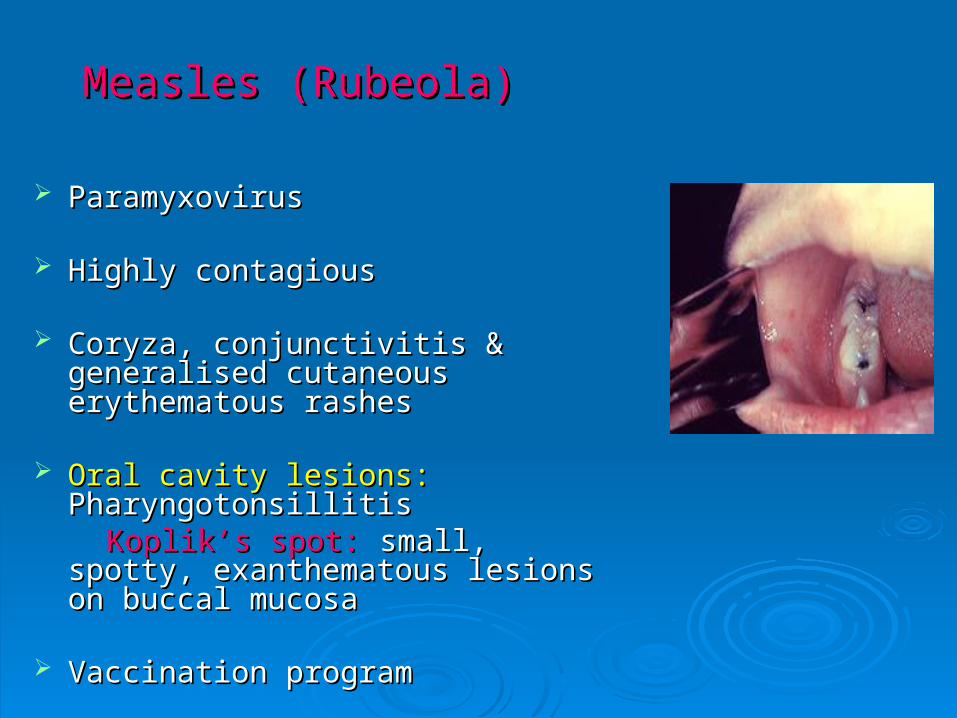
Measles (Rubeola)Measles (Rubeola)
Paramyxovirus Paramyxovirus
Highly contagious Highly contagious
Coryza, conjunctivitis & generalised Coryza, conjunctivitis & generalised cutaneous erythematous rashescutaneous erythematous rashes
Oral cavity lesions:Oral cavity lesions: Pharyngotonsillitis Pharyngotonsillitis Koplik’s spot:Koplik’s spot: small, spotty, small, spotty,
exanthematous lesions on buccal exanthematous lesions on buccal mucosamucosa
Vaccination programVaccination program

MumpsMumps
Common viral illnessCommon viral illness
Incubation period: 2-3 weeksIncubation period: 2-3 weeks
Fever, malaise, myalgia, headache, & Fever, malaise, myalgia, headache, & painful parotid gland swellingpainful parotid gland swelling
Self limitingSelf limiting
Complications: SNHLComplications: SNHL
Diagnosis:Diagnosis: Clinical Clinical
Treatment:Treatment: Supportive Supportive

Bacterial InfectionsBacterial Infections
1.1. TuberculosisTuberculosis
2.2. SyphilisSyphilis
3.3. LeprosyLeprosy

Tuberculosis Tuberculosis
Chronic, granulomatous, infectious Chronic, granulomatous, infectious diseasedisease
Mycobacterium tuberculosisMycobacterium tuberculosis Clinical featuresClinical features:: Oral lesions – rare Oral lesions – rare secondary tosecondary to pulmonary tuberculosispulmonary tuberculosis Pharynx- not commonPharynx- not common
Primary infection (Tonsils, Adenoids)Primary infection (Tonsils, Adenoids)
Secondary to coughing heavily of Secondary to coughing heavily of infected sputuminfected sputum
UlcerUlcer: multiple, painful, irregular, : multiple, painful, irregular, undermined borderundermined border, granulating floor, , granulating floor, usually covered by a gray-yellowish usually covered by a gray-yellowish exudate, inflamed & indurated exudate, inflamed & indurated surrounding tissuesurrounding tissue
Dorsum of the tongue - most commonly Dorsum of the tongue - most commonly affected- lip, buccal mucosa, & palateaffected- lip, buccal mucosa, & palate
TB Esophagitis:TB Esophagitis: -swallowed sputum or direct spread from -swallowed sputum or direct spread from
adjacent lymph nodesadjacent lymph nodes -stricture, fistula, mucosal irregularities-stricture, fistula, mucosal irregularities
Granulomatous Cheilitis-Granulomatous Cheilitis- rare rare
Laboratory tests:Laboratory tests: Sputum culture, HPE, Sputum culture, HPE, CXRCXR
Treatment:Treatment: ATTATT

SyphilisSyphilis
Treponema pallidumTreponema pallidum -Acquired -Acquired -Congenital-Congenital
1.1. Primary SyphilisPrimary Syphilis
2.2. Secondary SyphilisSecondary Syphilis
3.3. Tertiary SyphilisTertiary Syphilis

Primary SyphilisPrimary Syphilis
Lips, tongue, buccal mucosa, & tonsilsLips, tongue, buccal mucosa, & tonsils
Site of inoculation- 3 weeks after the Site of inoculation- 3 weeks after the infection, Papule, breaks down to form infection, Papule, breaks down to form an ulcer (chancre)an ulcer (chancre)
Oral chancre:Oral chancre: painless ulcer with a painless ulcer with a smooth surface, raised borders, & smooth surface, raised borders, & indurated marginindurated margin
Non tender cervical lymphadenopathyNon tender cervical lymphadenopathy
Spontaneous healingSpontaneous healing

Secondary SyphilisSecondary Syphilis
Most infectiousMost infectious
Secondary stage – after 6–8 Secondary stage – after 6–8 weeks & lasts for 2-10 weeksweeks & lasts for 2-10 weeks
Clinical features:Clinical features: Malaise, low-grade fever, Malaise, low-grade fever,
headache, lacrimation, headache, lacrimation, sore throat, weight loss, sore throat, weight loss,
myalgia,arthralgia, & myalgia,arthralgia, & generalized lymphadenopathygeneralized lymphadenopathy
Mucous patches

Hyperemia and inflammation of Hyperemia and inflammation of pharynx & soft palatepharynx & soft palate
Snail Track ulcer :-Snail Track ulcer :-
-Oral cavity & oropharnyx-Oral cavity & oropharnyx
-Ulcerated lesion covered with -Ulcerated lesion covered with
grayish white membranegrayish white membrane
which when scraped has pink base which when scraped has pink base with no bleeding with no bleeding

Syphilitic PharyngitisSyphilitic Pharyngitis
May be congenital or acquired by May be congenital or acquired by sexual intercoursesexual intercourse
Secondary stage most likelySecondary stage most likely
HIV positive patientsHIV positive patients

Tertiary SyphilisTertiary Syphilis
Tertiary syphilis - after a period of 4–7 yearsTertiary syphilis - after a period of 4–7 years
Typically painlessTypically painless
No lymphadenopathy unless secondary No lymphadenopathy unless secondary infectioninfection
Gumma:Gumma: -Characteristic lesion-Characteristic lesion -Hard palate, Nasal septum, Tonsil, PPW, or -Hard palate, Nasal septum, Tonsil, PPW, or LarynxLarynx
VDRL may be negativeVDRL may be negative
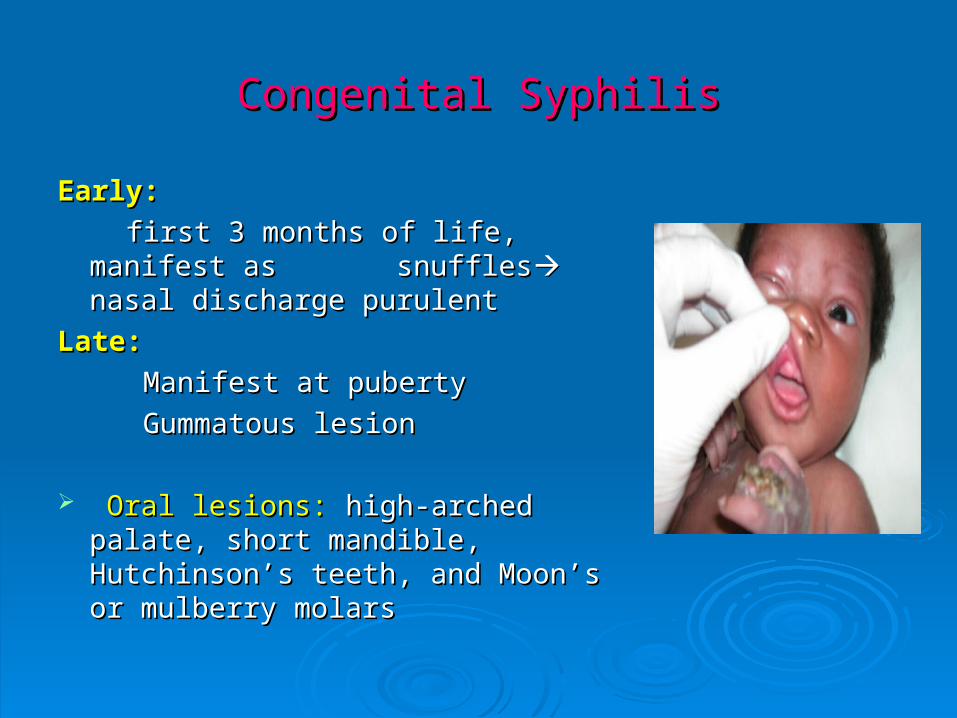
Congenital SyphilisCongenital Syphilis
Early:Early:
first 3 months of life, manifest as first 3 months of life, manifest as snufflessnuffles nasal discharge purulent nasal discharge purulent
Late: Late:
Manifest at pubertyManifest at puberty
Gummatous lesionGummatous lesion
Oral lesions:Oral lesions: high-arched palate, high-arched palate, short mandible, Hutchinson’s teeth, short mandible, Hutchinson’s teeth, and Moon’s or mulberry molarsand Moon’s or mulberry molars

Diagnosis:Diagnosis:
1.Immunoflurorescence or dark field microscopy1.Immunoflurorescence or dark field microscopy
2. Biopsy2. Biopsy
3.Serology3.Serology
Non-treponemal antibody testsNon-treponemal antibody tests: :
-VDRL, RPR-VDRL, RPR
-For screening and treatment follow up-For screening and treatment follow up
Treponema specific antibody tests:Treponema specific antibody tests:
-FTA-ABS test, TPHA-FTA-ABS test, TPHA
-For confirmation-For confirmation
-Usually remains positive for life-Usually remains positive for life
Treatment: Treatment: Penicillin( DOC)Penicillin( DOC)
Ceftriaxone, Erythromycin, or DoxycyclineCeftriaxone, Erythromycin, or Doxycycline
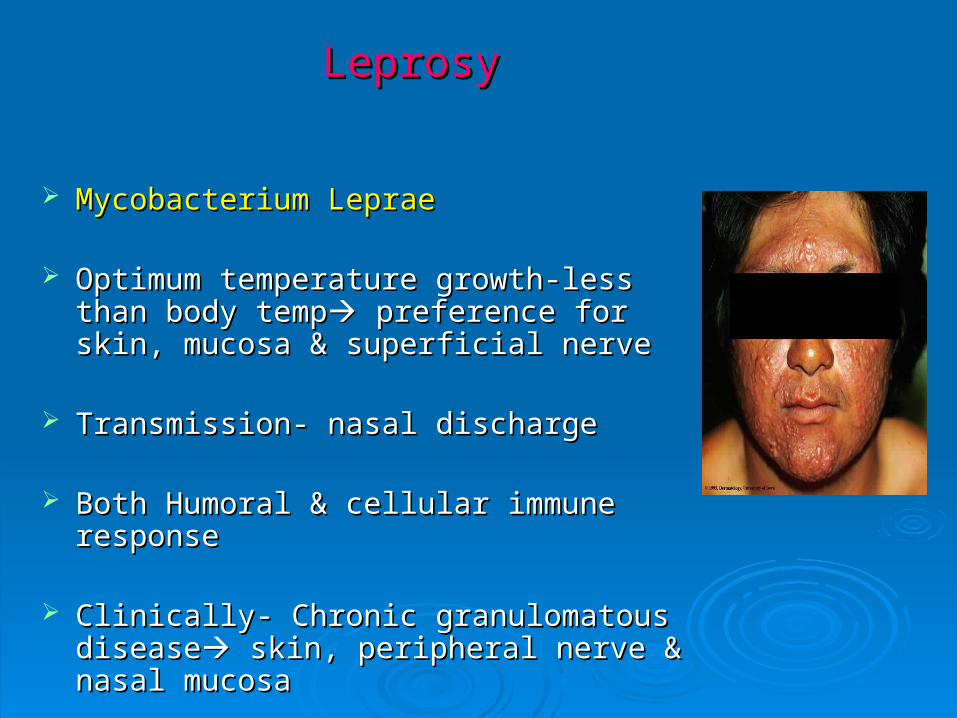
LeprosyLeprosy
Mycobacterium LepraeMycobacterium Leprae
Optimum temperature growth-less than Optimum temperature growth-less than body tempbody temp preference for skin, mucosa & preference for skin, mucosa & superficial nervesuperficial nerve
Transmission- nasal discharge Transmission- nasal discharge
Both Humoral & cellular immune responseBoth Humoral & cellular immune response
Clinically- Chronic granulomatous Clinically- Chronic granulomatous diseasedisease skin, peripheral nerve & nasal skin, peripheral nerve & nasal mucosamucosa
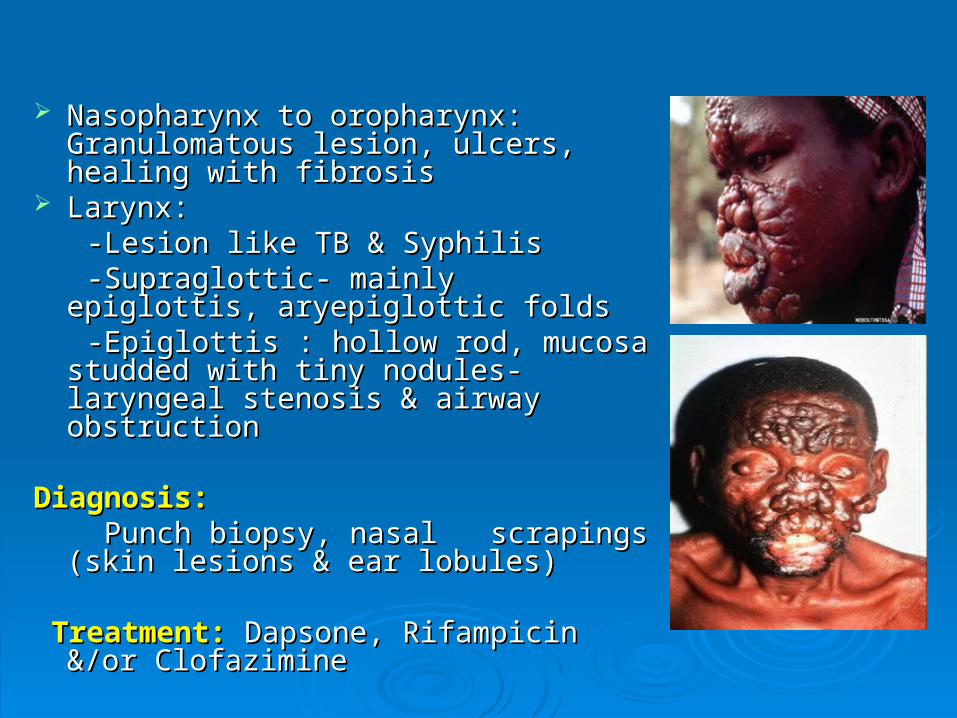
Nasopharynx to oropharynx: Nasopharynx to oropharynx: Granulomatous lesion, ulcers, healing Granulomatous lesion, ulcers, healing with fibrosiswith fibrosis
Larynx:Larynx: -Lesion like TB & Syphilis-Lesion like TB & Syphilis -Supraglottic- mainly epiglottis, -Supraglottic- mainly epiglottis,
aryepiglottic foldsaryepiglottic folds -Epiglottis : hollow rod, mucosa studded -Epiglottis : hollow rod, mucosa studded
with tiny nodules- laryngeal stenosis & with tiny nodules- laryngeal stenosis & airway obstructionairway obstruction
Diagnosis:Diagnosis: Punch biopsy, nasal scrapings (skin Punch biopsy, nasal scrapings (skin
lesions & ear lobules)lesions & ear lobules)
Treatment:Treatment: Dapsone, Rifampicin &/or Dapsone, Rifampicin &/or ClofazimineClofazimine

Protozoal infectionProtozoal infection
1.1. Toxoplasmosis Toxoplasmosis
2.2. LeshmaniasisLeshmaniasis
Toxoplasmosis Toxoplasmosis
Toxoplasm gondiiToxoplasm gondii ZoonosisZoonosis Self limitingSelf limiting
Immunocompetent: asymptomaticImmunocompetent: asymptomatic
Immunocompromised: Immunocompromised:
sore throat, malaise, fever, cervical sore throat, malaise, fever, cervical lymphadenopathylymphadenopathy
Multiple organs involvementMultiple organs involvement
(lungs, liver, skin, spleen, myocardium, (lungs, liver, skin, spleen, myocardium, eyes, skeletal muscles, braineyes, skeletal muscles, brain

Transplacental infection: Transplacental infection:
about 45 %about 45 %
subclinical infection- intrauterine deathsubclinical infection- intrauterine death
DiagnosisDiagnosis:: serological serological
Treatment:Treatment:
-usually unnecessary-usually unnecessary
-combination of pyrimethamine & -combination of pyrimethamine & sulphadiazinesulphadiazine

Leshmaniasis involving Lips

Fungal infectionFungal infection
1.1. CandidiasisCandidiasis
2.2. HistoplasmosisHistoplasmosis
3.3. CryptococcosisCryptococcosis
4.4. AspergillosisAspergillosis
5.5. MucormycosisMucormycosis
6.6. Paracoccidomycosis Paracoccidomycosis
7.7. Blastomycosis Blastomycosis
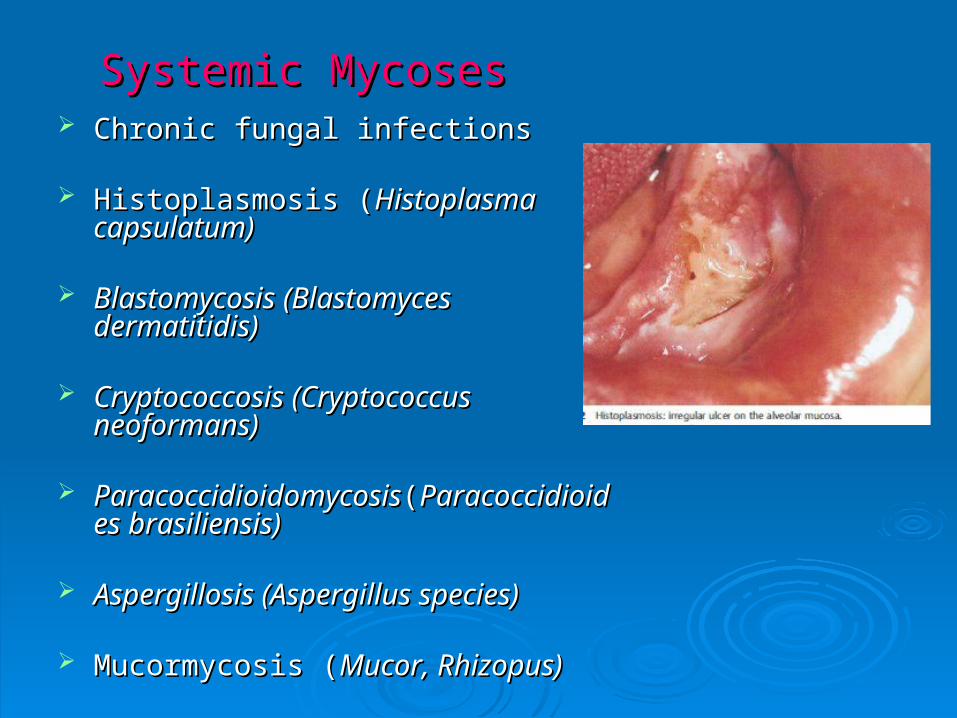
Systemic MycosesSystemic Mycoses Chronic fungal infectionsChronic fungal infections
Histoplasmosis (Histoplasmosis (Histoplasma Histoplasma capsulatum)capsulatum)
Blastomycosis (Blastomyces Blastomycosis (Blastomyces dermatitidis)dermatitidis)
Cryptococcosis (Cryptococcus Cryptococcosis (Cryptococcus neoformans)neoformans)
ParacoccidioidomycosisParacoccidioidomycosis((ParacoccidioidParacoccidioides brasiliensis)es brasiliensis)
Aspergillosis (Aspergillus species)Aspergillosis (Aspergillus species)
Mucormycosis (Mucormycosis (Mucor, Rhizopus)Mucor, Rhizopus)

Predisposing Predisposing conditionsconditions: : -Immunocompromised status-Immunocompromised status eg. HIV infection eg. HIV infection
Clinical features:Clinical features: Oral lesions – rareOral lesions – rare chronic, irregular chronic, irregular ulcerulcer
Candidiasis rarely produces ulcersCandidiasis rarely produces ulcers
Deep mycosis: chronic lumps & Deep mycosis: chronic lumps & ulcersulcers
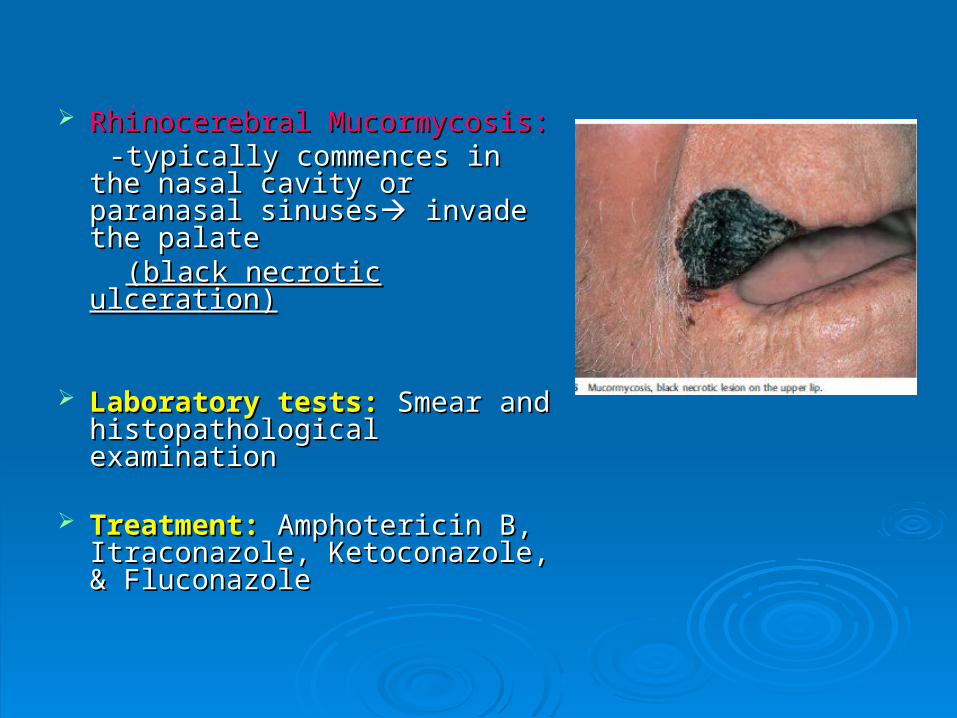
Rhinocerebral Mucormycosis: Rhinocerebral Mucormycosis: -typically commences in the -typically commences in the
nasal cavity or paranasal nasal cavity or paranasal sinusessinuses invade the palate invade the palate
(black necrotic ulceration)(black necrotic ulceration)
Laboratory tests: Laboratory tests: Smear and Smear and histopathological examinationhistopathological examination
Treatment:Treatment: Amphotericin B, Amphotericin B, Itraconazole, Ketoconazole, & Itraconazole, Ketoconazole, & FluconazoleFluconazole

Collagen-Vascular & Granulomatous DisordersCollagen-Vascular & Granulomatous Disorders1.1. Sjogren’s SyndromeSjogren’s Syndrome2.2. Systemic Lupus Erythematous (SLE)Systemic Lupus Erythematous (SLE)3.3. SclerodermaScleroderma4.4. Dermatomyositis-PolymyositisDermatomyositis-Polymyositis5.5. SarcoidosisSarcoidosis6.6. Wegner’s GranulomatosisWegner’s Granulomatosis7.7. Behcet’s SyndromeBehcet’s Syndrome8.8. Reiter’s SyndromeReiter’s Syndrome9.9. Sweet SyndromeSweet Syndrome10.10. Cogan’s SyndromeCogan’s Syndrome11.11. Amyloidosis Amyloidosis 12.12. Kawasaki DiseaseKawasaki Disease13.13. Rheumatoid Arthritis (RA)Rheumatoid Arthritis (RA)14.14. Polyarteritis Nodusa (PAN)Polyarteritis Nodusa (PAN)15.15. Sturge- Weber SyndromeSturge- Weber Syndrome16.16. Ehlers-Danlos SyndromeEhlers-Danlos Syndrome17.17. Cowden’s DiseaseCowden’s Disease

Sjogren’s SyndromeSjogren’s Syndrome
Autoimmune Autoimmune Female Female Primary Sjogren’s Syndrome:Primary Sjogren’s Syndrome: Secondary Sjogren’s SyndromeSecondary Sjogren’s Syndrome: :
associated with RA, SLE, Scleroderma, associated with RA, SLE, Scleroderma, Polymyositis, Polyarteritis NodusaPolymyositis, Polyarteritis Nodusa
Presents with xerostomia & parotid Presents with xerostomia & parotid enlargementenlargement
Oral findings:Oral findings: -Due to decreased saliva-Due to decreased salivadysphagia, dysphagia,
disturbances in taste & speech, burning disturbances in taste & speech, burning pain of mouth & tongue, increased pain of mouth & tongue, increased dental caries, increased predisposition dental caries, increased predisposition to infection (candidiasis)to infection (candidiasis)

Mucosal changes: dry, red & wrinkled Mucosal changes: dry, red & wrinkled mucosamucosa
Fissured tongue, atrophy of tongue Fissured tongue, atrophy of tongue papillae and redness of tongue, cracked papillae and redness of tongue, cracked & ulcerated lips & ulcerated lips
Diagnosis:Diagnosis: -Minor salivary gland biopsy (mucosa of -Minor salivary gland biopsy (mucosa of
lower lip)lower lip) -Periductal lymphocytic infiltrate-Periductal lymphocytic infiltrate -Serum: Autoantibodies (ANA, antilacrimal -Serum: Autoantibodies (ANA, antilacrimal
& antithyroid antibodies, RA factor)& antithyroid antibodies, RA factor)
Treatment :Treatment : -Steroid & immunossuppresive drugs-Steroid & immunossuppresive drugs -Artificial saliva-Artificial saliva -Constant dental evaluation-Constant dental evaluation
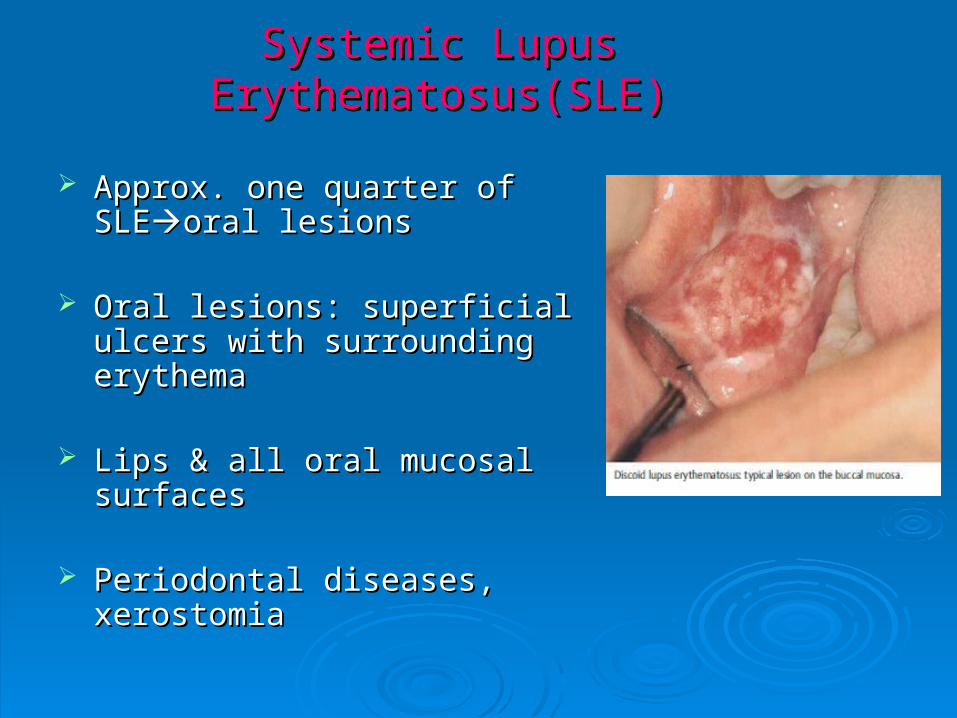
Systemic Lupus Erythematosus(SLE)Systemic Lupus Erythematosus(SLE)
Approx. one quarter of SLEApprox. one quarter of SLEoral oral lesionslesions
Oral lesions: superficial ulcers Oral lesions: superficial ulcers with surrounding erythemawith surrounding erythema
Lips & all oral mucosal surfacesLips & all oral mucosal surfaces
Periodontal diseases, xerostomiaPeriodontal diseases, xerostomia
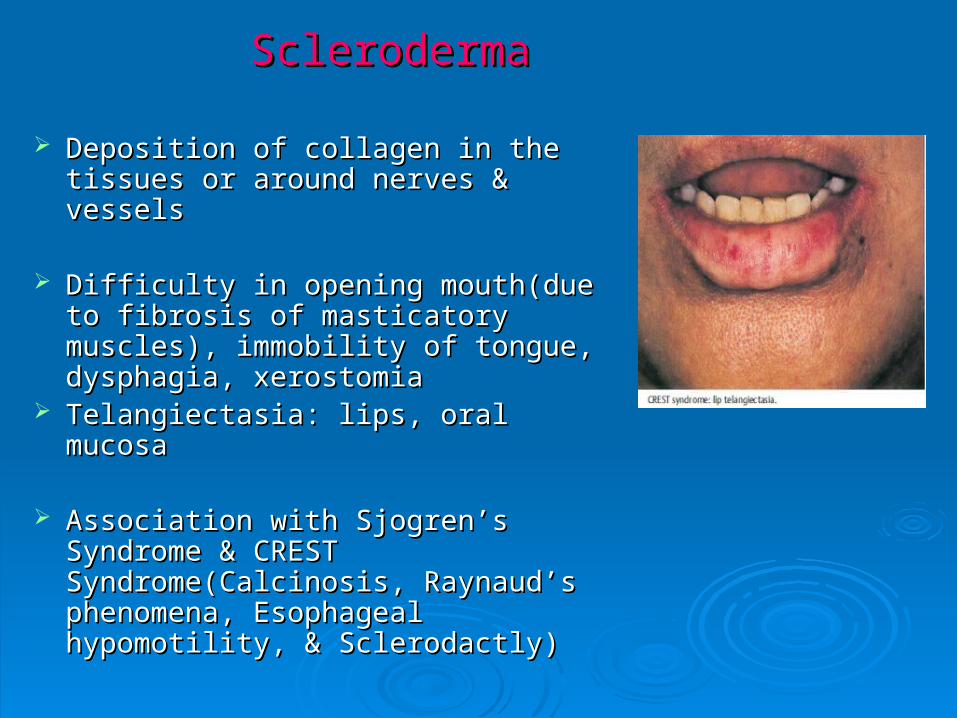
Scleroderma Scleroderma
Deposition of collagen in the tissues Deposition of collagen in the tissues or around nerves & vesselsor around nerves & vessels
Difficulty in opening mouth(due to Difficulty in opening mouth(due to fibrosis of masticatory muscles), fibrosis of masticatory muscles), immobility of tongue, dysphagia, immobility of tongue, dysphagia, xerostomiaxerostomia
Telangiectasia: lips, oral mucosaTelangiectasia: lips, oral mucosa
Association with Sjogren’s Syndrome Association with Sjogren’s Syndrome & CREST Syndrome(Calcinosis, & CREST Syndrome(Calcinosis, Raynaud’s phenomena, Esophageal Raynaud’s phenomena, Esophageal hypomotility, & Sclerodactly)hypomotility, & Sclerodactly)
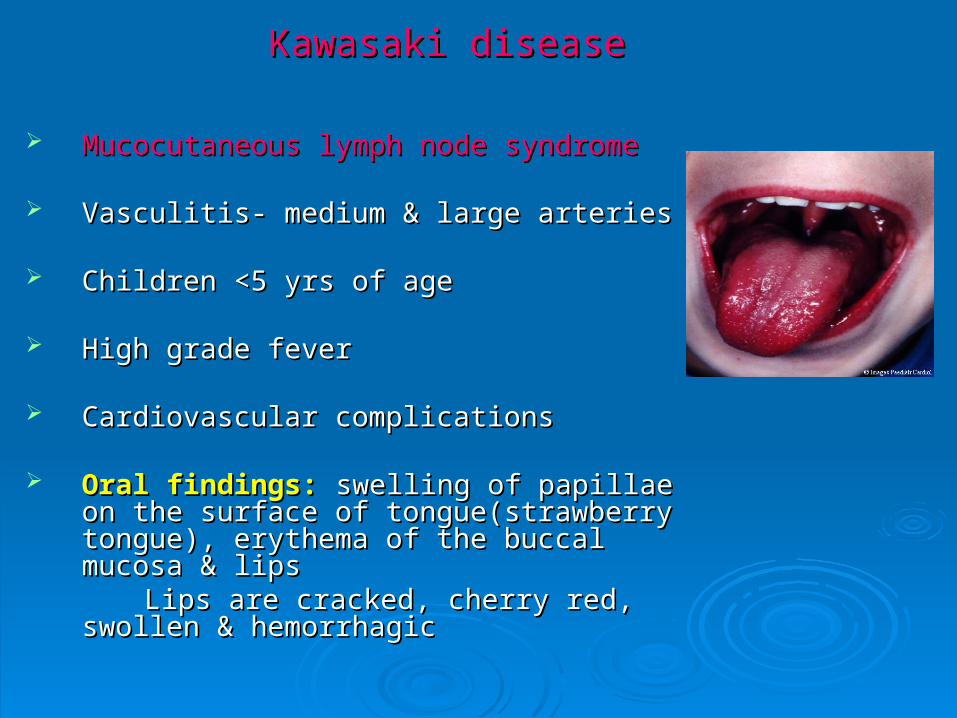
Kawasaki diseaseKawasaki disease
Mucocutaneous lymph node syndromeMucocutaneous lymph node syndrome
Vasculitis- medium & large arteriesVasculitis- medium & large arteries
Children <5 yrs of ageChildren <5 yrs of age
High grade feverHigh grade fever
Cardiovascular complicationsCardiovascular complications
Oral findings:Oral findings: swelling of papillae on the swelling of papillae on the surface of tongue(strawberry tongue), surface of tongue(strawberry tongue), erythema of the buccal mucosa & lipserythema of the buccal mucosa & lips
Lips are cracked, cherry red, swollen & Lips are cracked, cherry red, swollen & hemorrhagichemorrhagic

Laboratory tests:Laboratory tests: polymorphonuclear leukocytosis, polymorphonuclear leukocytosis, thrombocytosis, raised ESR & CRPthrombocytosis, raised ESR & CRP
Diagnosis:Diagnosis: 4 out of 6 clinical features with evidence of 4 out of 6 clinical features with evidence of coronary dilatationcoronary dilatation
1.Fever persisting>5 days1.Fever persisting>5 days2.Bilateral conjunctival congestion2.Bilateral conjunctival congestion3.Erythema of lips, buccal mucosa & tongue3.Erythema of lips, buccal mucosa & tongue4.Acute non-purulent cervical lymphadenopathy4.Acute non-purulent cervical lymphadenopathy5.Polymorphous exanthema5.Polymorphous exanthema6.Erythema of palms & soles (edema6.Erythema of palms & soles (edemadesquamation)desquamation)
Treatment:Treatment: Aspirin, IVIg Aspirin, IVIgSteroid avoided- risk of worsening coronary artery Steroid avoided- risk of worsening coronary artery
dilatationdilatation
Dermatomyositis-PolymyositisDermatomyositis-Polymyositis
Immunologic disease muscle Immunologic disease muscle Tongue & the upper portion of the Tongue & the upper portion of the
esophagusesophagus Clinical features:Clinical features:
-Difficulty in phonation, chewing & -Difficulty in phonation, chewing & deglutitiondeglutition
-Stomatitis-Stomatitis Difficulty in swallowingDifficulty in swallowingaspiration aspiration
pneumoniapneumonia Xerostomia & salivary hypofunction Xerostomia & salivary hypofunction
(2* sjogren’s syndrome)(2* sjogren’s syndrome)

Wegener’s GranulomatosisWegener’s Granulomatosis
Rare chronic granulomatous disease Rare chronic granulomatous disease ImmunologicalImmunological Clinical features: Clinical features: necrotizing necrotizing
granulomatousgranulomatous lesions of the lesions of the respiratory tract, generalized focal respiratory tract, generalized focal necrotizing vasculitis, and necrotizing necrotizing vasculitis, and necrotizing glomerulitisglomerulitis
Oral lesions:Oral lesions: solitary or multiple solitary or multiple irregular ulcers, surrounded by an irregular ulcers, surrounded by an inflammatory zoneinflammatory zone
Tongue, palate, buccal mucosa & Tongue, palate, buccal mucosa & gingivagingiva
Laboratory tests: Laboratory tests: HPE, c-ANCAHPE, c-ANCA Treatment:Treatment: Steroids, Azathioprine,Steroids, Azathioprine, & &
CyclophosphamideCyclophosphamide

SarcoidosisSarcoidosis
Systemic granulomatous diseaseSystemic granulomatous disease Any organAny organ Noncaseating granuloma:Noncaseating granuloma: -characteristic lesion-characteristic lesion
Oral manifestations:Oral manifestations: multiple, nodular, multiple, nodular, painless ulceration of the gingiva, painless ulceration of the gingiva, buccal mucosa, tongue, lips, & palatebuccal mucosa, tongue, lips, & palate
Salivary gland swellingSalivary gland swelling
Diagnosis:Diagnosis: Biopsy Biopsy
Treatment:Treatment: Systemic steroids Systemic steroids

Heerfordt SyndromeHeerfordt Syndrome
Uveoparotid FeverUveoparotid Fever
Rare form of SarcoidosisRare form of Sarcoidosis
Clinical features:Clinical features: B/L painless, firm, B/L painless, firm, parotid swelling, ocular parotid swelling, ocular involvement(uveitis, conjunctivitis, involvement(uveitis, conjunctivitis, keratitis), facial paralysis, low grade keratitis), facial paralysis, low grade fever, sublingual & submandibular fever, sublingual & submandibular gland may also enlargegland may also enlarge
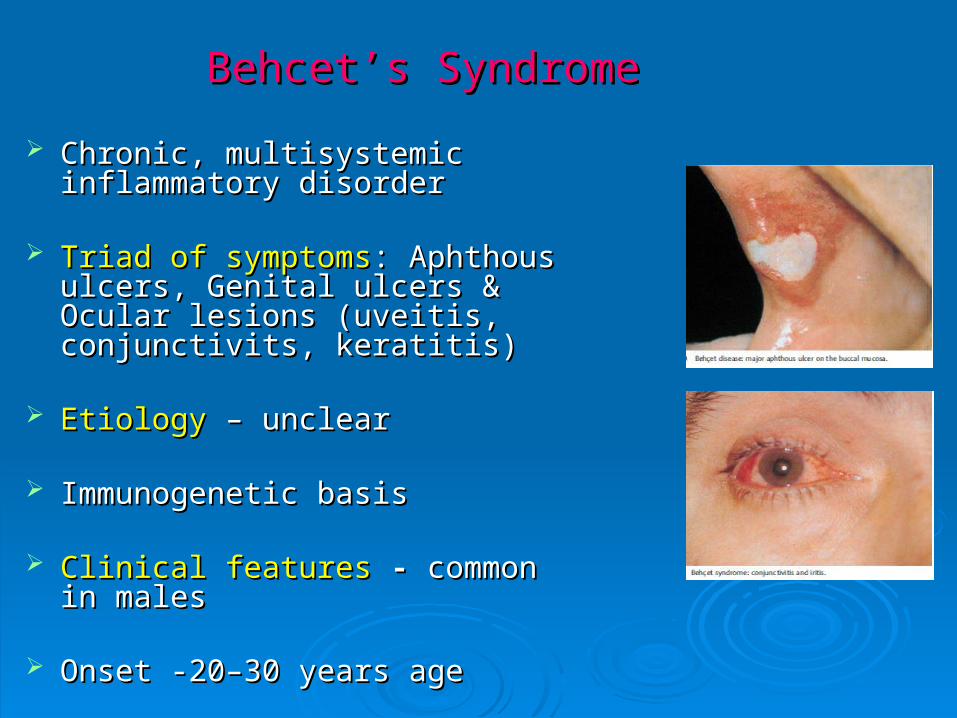
Behcet’s SyndromeBehcet’s Syndrome
Chronic, multisystemic inflammatory Chronic, multisystemic inflammatory disorderdisorder
Triad of symptomsTriad of symptoms: Aphthous ulcers, : Aphthous ulcers, Genital ulcers & Ocular lesions Genital ulcers & Ocular lesions (uveitis, conjunctivits, keratitis)(uveitis, conjunctivits, keratitis)
EtiologyEtiology – unclear – unclear
Immunogenetic basisImmunogenetic basis
Clinical featuresClinical features - - common in malescommon in males
Onset -20–30 years age Onset -20–30 years age

Diagnostic criteria :Diagnostic criteria :1.1. Recurrent oral ulcers (aphthaeRecurrent oral ulcers (aphthae))2.2. Recurrent genital ulcersRecurrent genital ulcers3.3. Ocular lesions (conjunctivitis, iritis Ocular lesions (conjunctivitis, iritis
with hypopyon, uveitis, retinal with hypopyon, uveitis, retinal vasculitis, reduced visual acuityvasculitis, reduced visual acuity
4.4. Skin lesions (papules, pustules, Skin lesions (papules, pustules, folliculitisfolliculitis, , erythema nodosum, erythema nodosum, ulcers, & rarely necrotic lesions)ulcers, & rarely necrotic lesions)
5.5. Positive Pathergy test: Positive Pathergy test: The test is called positive, when the The test is called positive, when the
needle puncture causes a sterile needle puncture causes a sterile red nodule or pustule that is greater red nodule or pustule that is greater than 2mm in diameter at 24 to 48 than 2mm in diameter at 24 to 48 hourshours

Diagnosis:Diagnosis: For accurate diagnosis, recurrent oral For accurate diagnosis, recurrent oral
ulcers plus two of the four criteria must ulcers plus two of the four criteria must be presentbe present
Treatment:Treatment: Mild cases- Topical steroidMild cases- Topical steroid Severe cases- Systemic steroid, & other Severe cases- Systemic steroid, & other
immunosuppressive drugs (Ciclosporin, immunosuppressive drugs (Ciclosporin, Thalidomide, Colchicine, Dapsone)Thalidomide, Colchicine, Dapsone)

Rheumatoid ArthritisRheumatoid Arthritis Progressive destruction of articular & Progressive destruction of articular &
periarticular structure eg. TMJperiarticular structure eg. TMJ
TMJ pathology: clicking, locking, crepitus, TMJ pathology: clicking, locking, crepitus, tenderness in the preauricular area, pain tenderness in the preauricular area, pain during mandibular movementduring mandibular movement
Oral cavity involvement-not commonOral cavity involvement-not common
Association with secondary Sjogren’s Association with secondary Sjogren’s SyndromeSyndrome
Immunosuppressive drugsImmunosuppressive drugsacute stomatitis, acute stomatitis, candidiasis, recurrent HSV infectioncandidiasis, recurrent HSV infection
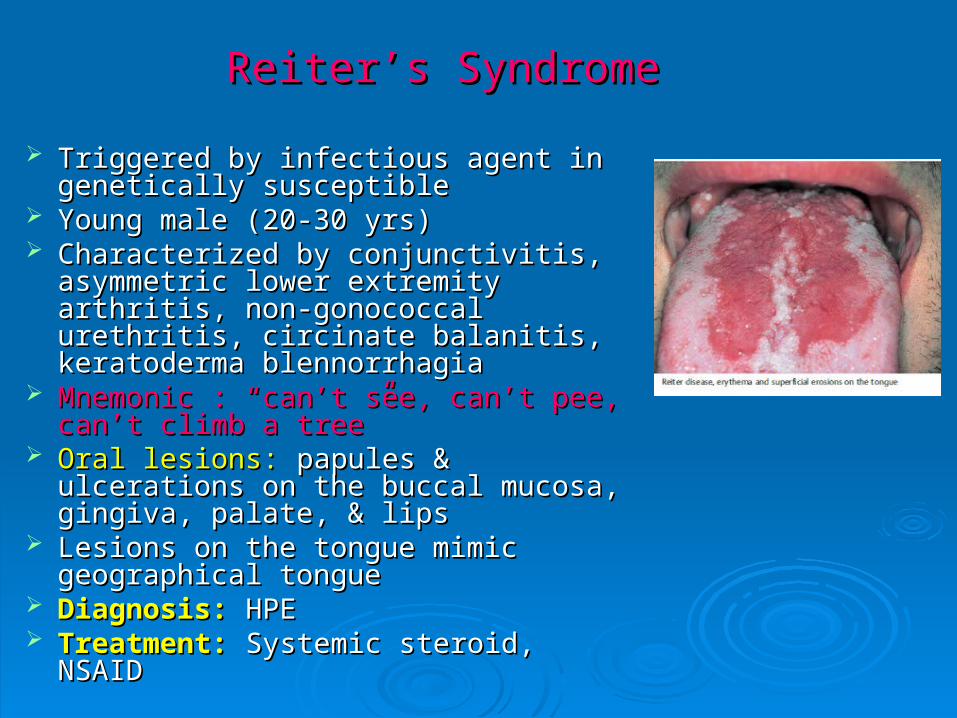
Reiter’s SyndromeReiter’s Syndrome
Triggered by infectious agent in Triggered by infectious agent in genetically susceptiblegenetically susceptible
Young male (20-30 yrs)Young male (20-30 yrs) Characterized by conjunctivitis, Characterized by conjunctivitis,
asymmetric lower extremity arthritis, asymmetric lower extremity arthritis, non-gonococcal urethritis, circinate non-gonococcal urethritis, circinate balanitis, keratoderma blennorrhagiabalanitis, keratoderma blennorrhagia
Mnemonic : “can’t see, can’t pee, can’t Mnemonic : “can’t see, can’t pee, can’t climb a tree”climb a tree”
Oral lesions:Oral lesions: papules & ulcerations on papules & ulcerations on the buccal mucosa, gingiva, palate, & the buccal mucosa, gingiva, palate, & lipslips
Lesions on the tongue mimic Lesions on the tongue mimic geographical tonguegeographical tongue
Diagnosis:Diagnosis: HPE HPE Treatment:Treatment: Systemic steroid, NSAID Systemic steroid, NSAID

Sweet SyndromeSweet Syndrome
Acute febrile neutrophilic dermatosisAcute febrile neutrophilic dermatosis Etiology:Etiology: unknown unknown Fever, leukocytosis, arthralgia, Fever, leukocytosis, arthralgia,
myalgia, & ocular involvementmyalgia, & ocular involvement Oral lesions:Oral lesions: painful, aphthous like painful, aphthous like
ulcer-lips, tongue, buccal mucosa, & ulcer-lips, tongue, buccal mucosa, & palatepalate
Skin lesions: nonpruritic, Skin lesions: nonpruritic, erythematous papules, & erythematous papules, & vesiculobullous lesionsvesiculobullous lesions
Diagnosis:Diagnosis: HPE HPE Treatment: Treatment: Systemic Steroid/DapsoneSystemic Steroid/Dapsone

AmyloidosisAmyloidosis
Deposition of amyloid protein (fibrillar Deposition of amyloid protein (fibrillar protein) in tissuesprotein) in tissues
1.1. Primary:Primary: Idiopathic or Multiple Myeloma Idiopathic or Multiple Myeloma2.2. Secondary:Secondary: Chronic or Inflammatory Chronic or Inflammatory
diseasedisease Oral manifestations:Oral manifestations: macroglossia, macroglossia,
decreased mobility, yellow nodules on decreased mobility, yellow nodules on lateral surfacelateral surface
Deposition on salivary glandDeposition on salivary gland hyposalivationhyposalivation
Submandibular swelling & tongue Submandibular swelling & tongue enlargementenlargement respiratory obstruction respiratory obstruction
Diagnosis:Diagnosis: HPE (congo red staining) HPE (congo red staining) Treatment:Treatment: Symptomatic Symptomatic

Hematological DiseasesHematological Diseases
1.1. Iron Deficiency Anaemia Iron Deficiency Anaemia 2.2. Sickle Cell AnaemiaSickle Cell Anaemia3.3. Langerhans Cell HistiocytosisLangerhans Cell Histiocytosis4.4. Osler-Weber-Rendu disease (HHT)Osler-Weber-Rendu disease (HHT)5.5. Plummer-Vinson SyndromePlummer-Vinson Syndrome6.6. Leukaemia Leukaemia 7.7. Agranulocytosis Agranulocytosis 8.8. Myelodysplastic SyndromeMyelodysplastic Syndrome9.9. Cyclic Neutropenia Cyclic Neutropenia 10.10. Idiopathic Thrombocytopenic PurpuraIdiopathic Thrombocytopenic Purpura11.11. Multiple MyelomaMultiple Myeloma

Iron Deficiency AnaemiaIron Deficiency Anaemia
Oral manifestations:Oral manifestations:
Atrophic glossitis, mucosal Atrophic glossitis, mucosal pallor, angular stomatitis, pallor, angular stomatitis, flattening of tongue papillae, flattening of tongue papillae, geographic glossitisgeographic glossitis

Langerhans Cell Histiocytosis (Histiocytosis X)Langerhans Cell Histiocytosis (Histiocytosis X)
Abnormal clonal proliferation of Langerhans Abnormal clonal proliferation of Langerhans cells(dendritic cells) & Eosinophilscells(dendritic cells) & Eosinophils
Etiology:Etiology:UnknownUnknown
1.1. Eosinophillic granulomaEosinophillic granuloma (most common (most common form)form)
2.2. Hand–Schüller–Christian disease Hand–Schüller–Christian disease
3.3. Letterer–Siwe disease Letterer–Siwe disease Clinical features:Clinical features:
Oral lesions-all forms Oral lesions-all forms solitary or multiple ulceration on the gingiva solitary or multiple ulceration on the gingiva
and the palate usually associated with bone and the palate usually associated with bone destruction & tooth loosening or loss destruction & tooth loosening or loss (“floating teeth”)(“floating teeth”)
Diagnosis:Diagnosis: Biopsy (eg.Skin,lung)-Birbeck Biopsy (eg.Skin,lung)-Birbeck granules(electron microscopy)granules(electron microscopy)
Treatment: Treatment: Steroids, Vinblastine+/- EtoposideSteroids, Vinblastine+/- Etoposide
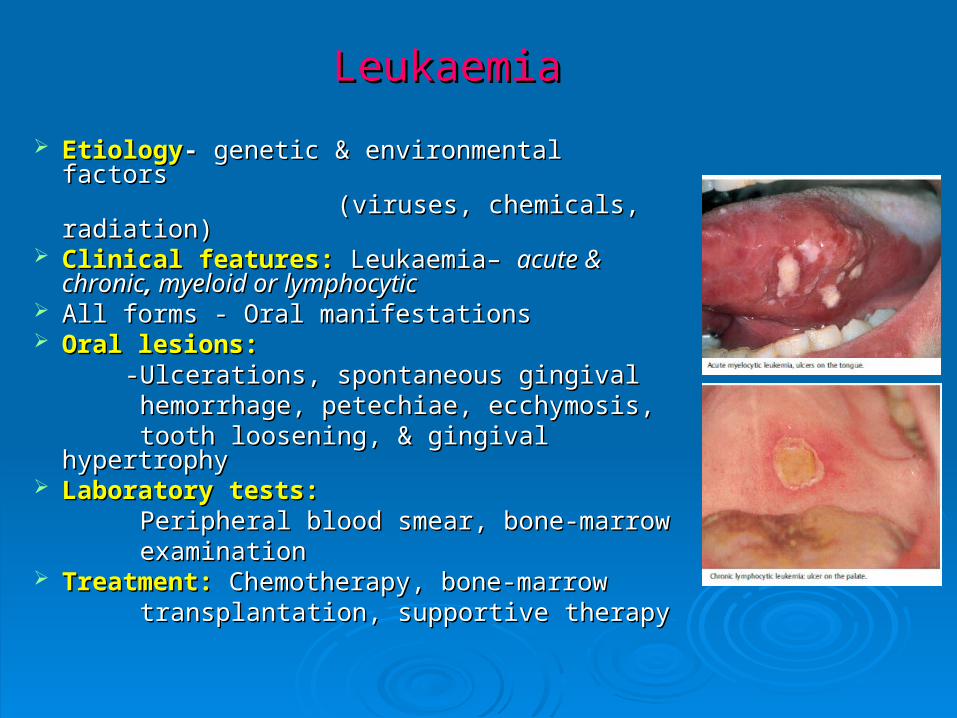
LeukaemiaLeukaemia
EtiologyEtiology- - genetic & environmental factors genetic & environmental factors (viruses, chemicals, radiation)(viruses, chemicals, radiation) Clinical features:Clinical features: Leukaemia– Leukaemia– acute & acute &
chronicchronic, , myeloid or lymphocyticmyeloid or lymphocytic All forms - Oral manifestationsAll forms - Oral manifestations Oral lesions:Oral lesions: -Ulcerations, spontaneous gingival -Ulcerations, spontaneous gingival hemorrhage, petechiae, ecchymosis, hemorrhage, petechiae, ecchymosis, tooth loosening, & gingival hypertrophytooth loosening, & gingival hypertrophy Laboratory tests:Laboratory tests: Peripheral blood smear, bone-marrow Peripheral blood smear, bone-marrow examinationexamination Treatment:Treatment: Chemotherapy, bone-marrow Chemotherapy, bone-marrow transplantation, supportivetransplantation, supportive therapytherapy
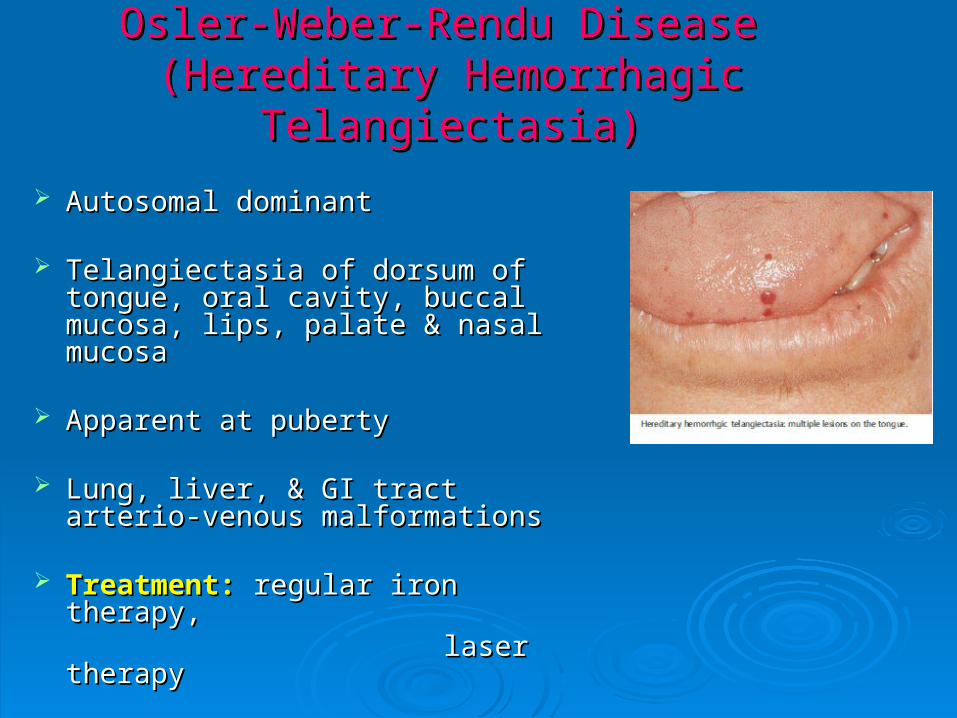
Osler-Weber-Rendu Disease Osler-Weber-Rendu Disease (Hereditary Hemorrhagic Telangiectasia)(Hereditary Hemorrhagic Telangiectasia)
Autosomal dominant Autosomal dominant
Telangiectasia of dorsum of tongue, Telangiectasia of dorsum of tongue, oral cavity, buccal mucosa, lips, oral cavity, buccal mucosa, lips, palate & nasal mucosapalate & nasal mucosa
Apparent at pubertyApparent at puberty
Lung, liver, & GI tract arterio-venous Lung, liver, & GI tract arterio-venous malformationsmalformations
Treatment:Treatment: regular iron therapy, regular iron therapy, laser therapylaser therapy

Plummer Vinson SyndromePlummer Vinson Syndrome(Patterson-Brown-Kelly Syndrome)(Patterson-Brown-Kelly Syndrome)
Oral manifestations:Oral manifestations: Dysphagia, iron Dysphagia, iron def. anaemia, atrophic glossitis, angular def. anaemia, atrophic glossitis, angular stomatitis, & koilonychiastomatitis, & koilonychia
Female, in fourth decadeFemale, in fourth decade Barium swallow: web in post-cricoid Barium swallow: web in post-cricoid
regionregion Pre-malignant Pre-malignant Post-cricoid carcinomaPost-cricoid carcinoma Treatment: Treatment: -Esophageal dilatation-Esophageal dilatation (if symptoms from web)(if symptoms from web) -Follow up-developing carcinoma-Follow up-developing carcinoma
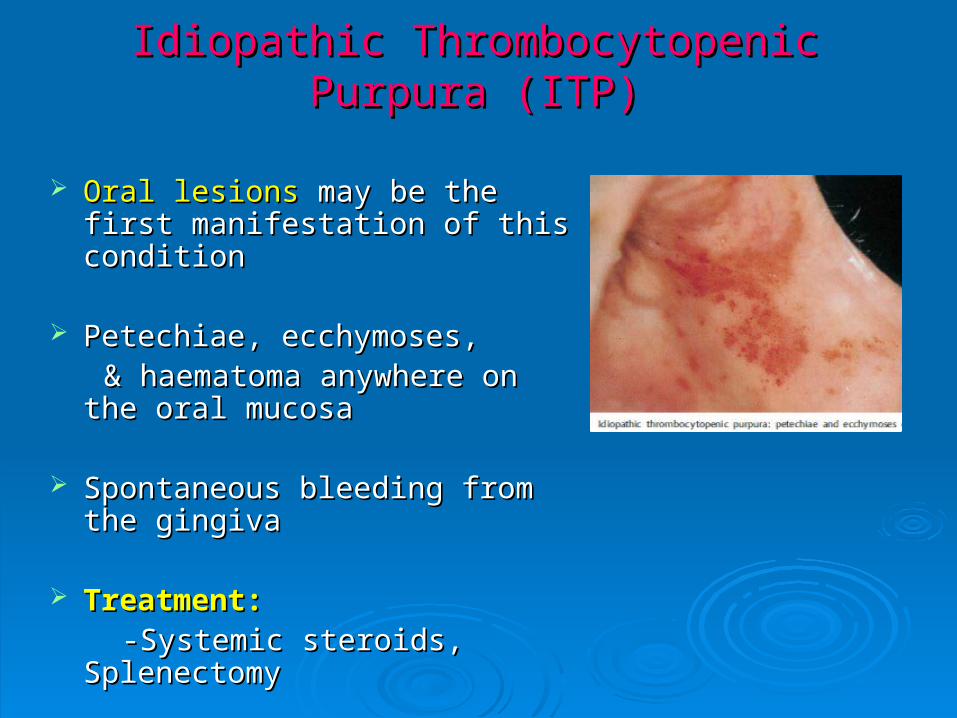
Idiopathic Thrombocytopenic Purpura (ITP)Idiopathic Thrombocytopenic Purpura (ITP)
Oral lesionsOral lesions may be the first may be the first manifestation of this conditionmanifestation of this condition
Petechiae, ecchymoses,Petechiae, ecchymoses, & haematoma anywhere on the & haematoma anywhere on the
oral mucosaoral mucosa
Spontaneous bleeding from the Spontaneous bleeding from the gingivagingiva
Treatment:Treatment: -Systemic steroids, Splenectomy-Systemic steroids, Splenectomy

AgranulocytosisAgranulocytosis
EtiologyEtiology:: Drug or infection Drug or infection Clinical features:Clinical features: Oral lesions -multiple necrotic ulcers Oral lesions -multiple necrotic ulcers
covered with dirty pseudomembranecovered with dirty pseudomembrane Buccal mucosa, tongue, palate,Buccal mucosa, tongue, palate, & tonsillar & tonsillar
area area Severe necrotizing gingivitis Severe necrotizing gingivitis Laboratory tests:Laboratory tests: White blood countWhite blood count &&
bone-marrow aspirationbone-marrow aspiration Treatment:Treatment: Antibiotics, white blood cell Antibiotics, white blood cell
transfusions, granulocyte colony-transfusions, granulocyte colony-stimulating factor (G-CSF) or granulocyte-stimulating factor (G-CSF) or granulocyte-macrophage colony-stimulating factor macrophage colony-stimulating factor (GM-CSF)(GM-CSF)

Cyclic NeutropeniaCyclic Neutropenia
Regular periodic reduction of the Regular periodic reduction of the neutrophil neutrophil
Etiology:Etiology: hereditary autosomal hereditary autosomal dominantdominant
Clinical features:Clinical features: childhood,reduction childhood,reduction of neutrophils - regularly in a 21-day of neutrophils - regularly in a 21-day cycle - low-grade fever, headache, cycle - low-grade fever, headache, malaise, anorexia, arthralgia, cervical malaise, anorexia, arthralgia, cervical lymphadenopathy, gastrointestinal lymphadenopathy, gastrointestinal disorders, skin & oral manifestationsdisorders, skin & oral manifestations
Oral lesions -Oral lesions - painful ulcer - whitish painful ulcer - whitish membranemembrane
Localized gingivitisLocalized gingivitis Laboratory tests:Laboratory tests: peripheralperipheral bloodblood countcount Treatment:Treatment: Supportive, Corticosteroid, Supportive, Corticosteroid,
granulocyte colony stimulating factor(G-granulocyte colony stimulating factor(G-CSF)CSF)

Gastrointestinal DiseasesGastrointestinal Diseases
1.Inflammatory Bowel Disease1.Inflammatory Bowel Disease
(Crohn’s disease & Ulcerative colitis)(Crohn’s disease & Ulcerative colitis)
2.Gastro-esophageal Reflux2.Gastro-esophageal Reflux
3.Peutz-Jegher’s Syndrome3.Peutz-Jegher’s Syndrome
4.Celiac disease4.Celiac disease
5.Chronic liver disease5.Chronic liver disease
6.Malabsorption Diseases6.Malabsorption Diseases

Crohn’s DiseaseCrohn’s Disease
Diffuse nodular swelling in lips Diffuse nodular swelling in lips (painless), angular cheilitis, (painless), angular cheilitis, cobblestone appearance ofcobblestone appearance of buccal mucosabuccal mucosa or mucosal tag, or mucosal tag, Aphthous ulcerAphthous ulcer
May precede intestinal symptoms May precede intestinal symptoms or may be the only or may be the only manifestations in some casesmanifestations in some cases
Systemic steroidsSystemic steroids

Ulcerative ColitisUlcerative Colitis
Destructive oral ulceration due to Destructive oral ulceration due to immune mediated vasculitisimmune mediated vasculitis
Polystomatitis Vegetans:Polystomatitis Vegetans: microabscess on lips, palate, microabscess on lips, palate, ventral tongueventral tongue
May manifests as aphthous ulcersMay manifests as aphthous ulcers
Exacerbation & remissionExacerbation & remission

Gastroesophageal Reflux DiseaseGastroesophageal Reflux Disease
Mucosal & gingival erosion Mucosal & gingival erosion caused by acidcaused by acid
Erosion of tooth enamelErosion of tooth enamel
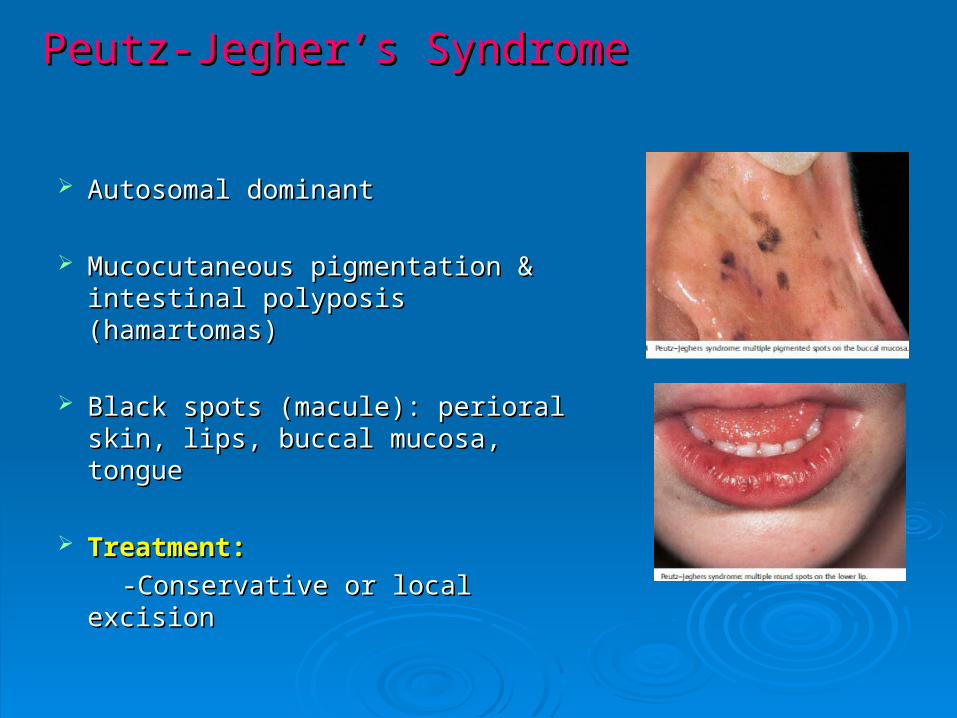
Peutz-Jegher’s SyndromePeutz-Jegher’s Syndrome
Autosomal dominantAutosomal dominant
Mucocutaneous pigmentation & Mucocutaneous pigmentation & intestinal polyposis (hamartomas)intestinal polyposis (hamartomas)
Black spots (macule): perioral skin, Black spots (macule): perioral skin, lips, buccal mucosa, tonguelips, buccal mucosa, tongue
Treatment:Treatment:
-Conservative or local excision-Conservative or local excision
Endocrine DiseasesEndocrine Diseases
1.1. Diabetes MellitusDiabetes Mellitus
2.2. Thyroid DisordersThyroid Disorders
3.3. Cushing’s DiseaseCushing’s Disease
4.4. Addison’s DiseaseAddison’s Disease
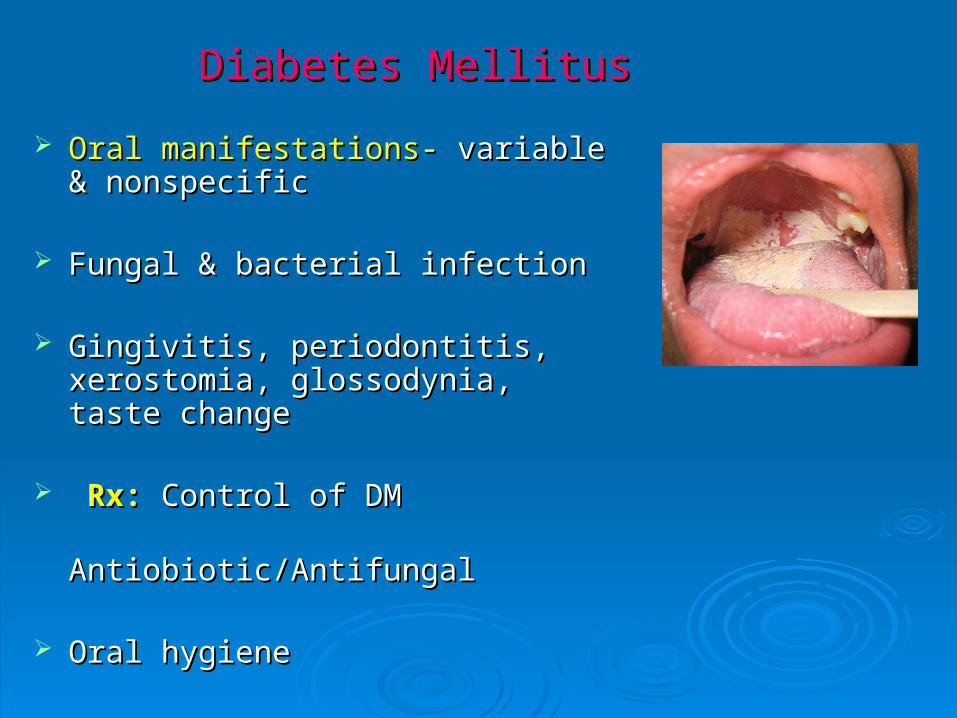
Diabetes MellitusDiabetes Mellitus
Oral manifestations-Oral manifestations- variable & variable & nonspecificnonspecific
Fungal & bacterial infectionFungal & bacterial infection
Gingivitis, periodontitis, xerostomia, Gingivitis, periodontitis, xerostomia, glossodynia, taste changeglossodynia, taste change
Rx:Rx: Control of DM Control of DM Antiobiotic/AntifungalAntiobiotic/Antifungal
Oral hygieneOral hygiene

Thyroid DiseasesThyroid Diseases
Hypothyroidism:Hypothyroidism: Macroglossia Macroglossia
Congenital Hypothyroidism:Congenital Hypothyroidism: Macroglossia, Macroglossia, pronounced lips, & delayed tooth eruption pronounced lips, & delayed tooth eruption with malocclusionwith malocclusion
Hyperthyroidism: Hyperthyroidism: Facial & skin manifestations:Facial & skin manifestations: upper eyelid upper eyelid
retraction, exophthalmous, retraction, exophthalmous, hyperpigmentation, & skin erythema hyperpigmentation, & skin erythema
Oral manifestations:Oral manifestations: early loss of primary early loss of primary teeth with subsequent rapid eruption of teeth with subsequent rapid eruption of permanent teeth(young children)permanent teeth(young children)
lymphoid tissue hyperplasia- tonsillar & lymphoid tissue hyperplasia- tonsillar & oropharynx (Grave’s disease)oropharynx (Grave’s disease)
Cushing’s SyndromeCushing’s Syndrome
Long term, high dose corticosteroid Long term, high dose corticosteroid administrationadministration
Moon or round face, buffalo humps, Moon or round face, buffalo humps, central obesity, osteoporosis, DM, central obesity, osteoporosis, DM, HTNHTN
Oral symptoms: Oral symptoms: -Increased susceptibility to oral -Increased susceptibility to oral infections (candidiasis)infections (candidiasis) -Muscle weakness-Muscle weakness difficulty with difficulty with speaking, & swallowingspeaking, & swallowing
Dx:Dx: Dexamethasone suppression test Dexamethasone suppression test
RxRx: Depends on the cause: Depends on the cause

Addison’s DiseaseAddison’s Disease
Primary adrenal insufficiencyPrimary adrenal insufficiency Destruction of adrenal cortex eg. Destruction of adrenal cortex eg.
autoimmune, metastasis, infection, autoimmune, metastasis, infection, haemorrhagehaemorrhage
Oral manifestations:Oral manifestations: diffuse or patchy diffuse or patchy pigmentation of the skin & mucous pigmentation of the skin & mucous membranesmembranes (due to increased ACTH- (due to increased ACTH-cross reacts with melanin receptors)cross reacts with melanin receptors)
Buccal mucosa, palate, lips, & gingivaBuccal mucosa, palate, lips, & gingiva Diagnosis:Diagnosis: ACTH test ACTH test Treatment: Treatment: Replace steroid Replace steroid
(glucocorticoid/mineralocorticoid)(glucocorticoid/mineralocorticoid)
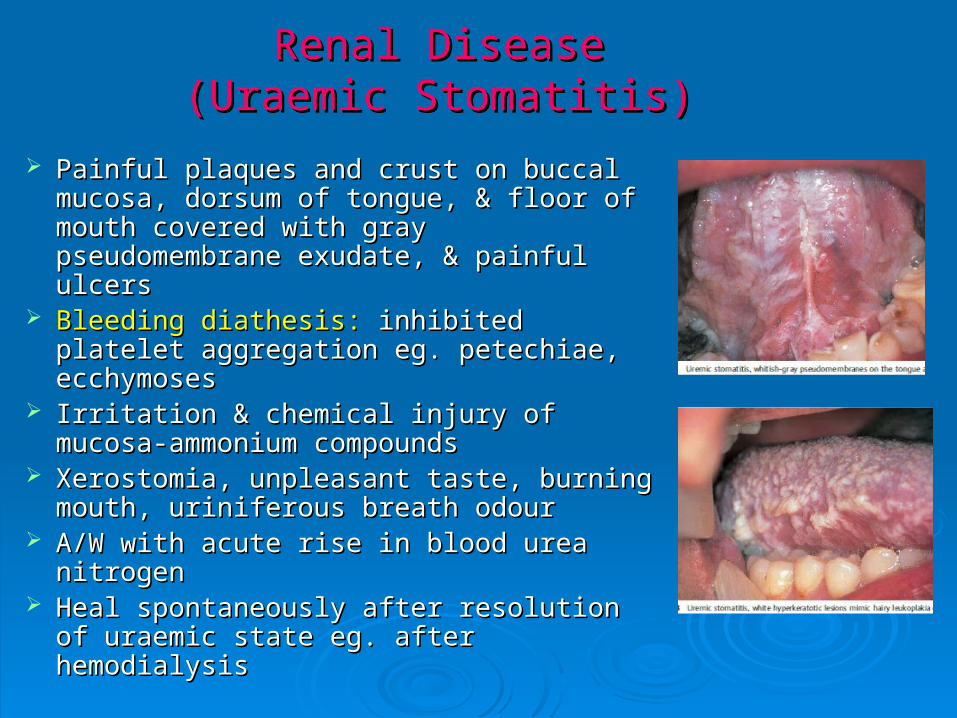
Renal DiseaseRenal Disease(Uraemic Stomatitis)(Uraemic Stomatitis)
Painful plaques and crust on buccal Painful plaques and crust on buccal mucosa, dorsum of tongue, & floor of mucosa, dorsum of tongue, & floor of mouth covered with gray mouth covered with gray pseudomembrane exudate, & painful pseudomembrane exudate, & painful ulcersulcers
Bleeding diathesis:Bleeding diathesis: inhibited platelet inhibited platelet aggregation eg. petechiae, ecchymosesaggregation eg. petechiae, ecchymoses
Irritation & chemical injury of mucosa-Irritation & chemical injury of mucosa-ammonium compoundsammonium compounds
Xerostomia, unpleasant taste, burning Xerostomia, unpleasant taste, burning mouth, uriniferous breath odourmouth, uriniferous breath odour
A/W with acute rise in blood urea nitrogenA/W with acute rise in blood urea nitrogen Heal spontaneously after resolution of Heal spontaneously after resolution of
uraemic state eg. after hemodialysisuraemic state eg. after hemodialysis

Dermatologic ConditionsDermatologic Conditions
1.1. Lichen PlanusLichen Planus
2.2. Pemphigus VulgarisPemphigus Vulgaris
3.3. Mucous Membrane PemphigoidMucous Membrane Pemphigoid
4.4. Erythema MultiformeErythema Multiforme
5.5. Stevens-Jhonson SyndromeStevens-Jhonson Syndrome
6.6. Toxic Epidermal NecrolysisToxic Epidermal Necrolysis

Lichen PlanusLichen Planus
Chronic, mucocutaneous, Chronic, mucocutaneous, autoimmune disorderautoimmune disorder
Precipitating factors: genetic Precipitating factors: genetic predisposition, stress, drug, foodpredisposition, stress, drug, food
Oral manifestations: Oral manifestations: White papules -White papules -coalesce, forming acoalesce, forming a networknetwork of lines of lines (Wickham’s striae)(Wickham’s striae)
Buccal mucosa, gingiva, & tongue, Buccal mucosa, gingiva, & tongue, lips & palatelips & palate
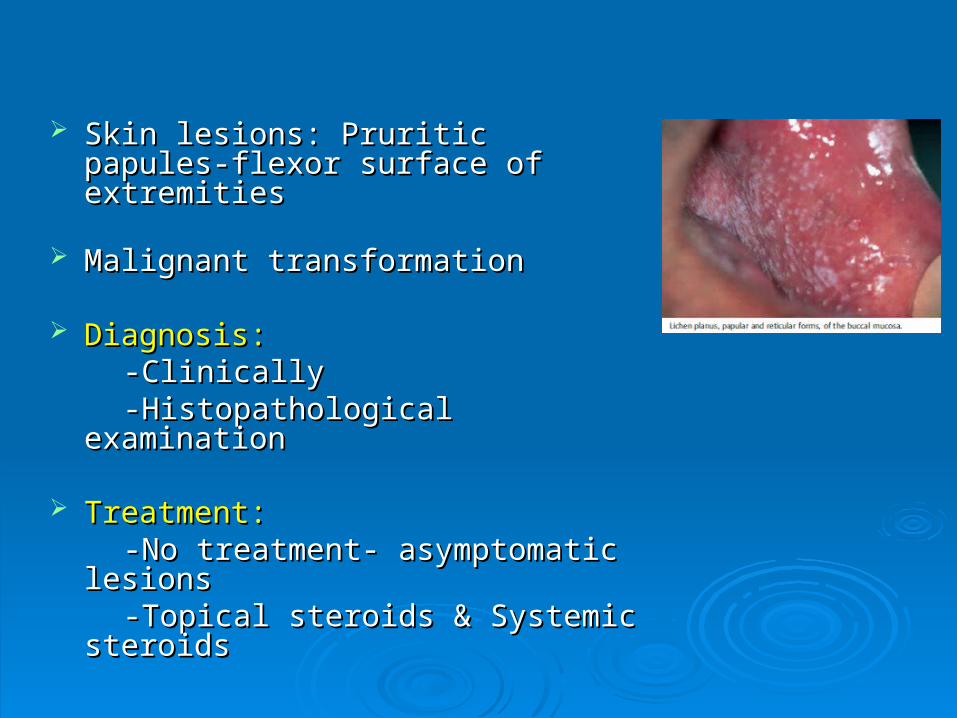
Skin lesions: Pruritic papules-flexor Skin lesions: Pruritic papules-flexor surface of extremitiessurface of extremities
Malignant transformationMalignant transformation
Diagnosis:Diagnosis: -Clinically-Clinically -Histopathological examination -Histopathological examination
Treatment:Treatment: -No treatment- asymptomatic-No treatment- asymptomatic lesionslesions -Topical-Topical steroids & Systemic steroidssteroids & Systemic steroids
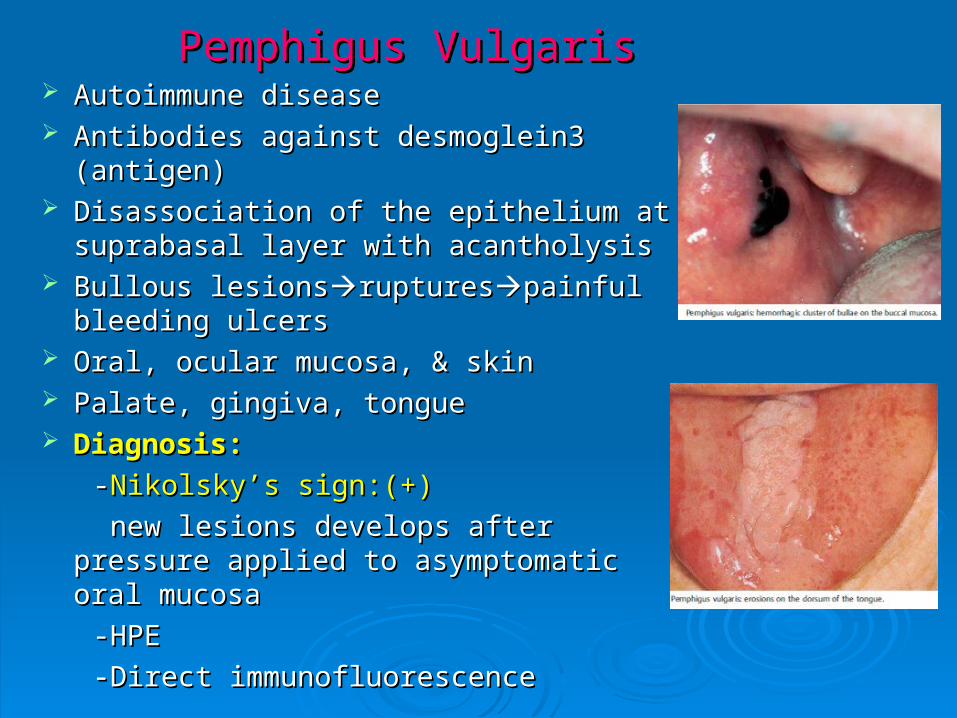
Pemphigus VulgarisPemphigus Vulgaris Autoimmune diseaseAutoimmune disease Antibodies against desmoglein3 (antigen)Antibodies against desmoglein3 (antigen) Disassociation of the epithelium at Disassociation of the epithelium at
suprabasal layer with acantholysissuprabasal layer with acantholysis Bullous lesionsBullous lesionsrupturesrupturespainful painful
bleeding ulcersbleeding ulcers Oral, ocular mucosa, & skinOral, ocular mucosa, & skin Palate, gingiva, tonguePalate, gingiva, tongue Diagnosis: Diagnosis:
--Nikolsky’s sign:(+)Nikolsky’s sign:(+)
new lesions develops after pressure new lesions develops after pressure applied to asymptomatic oral mucosa applied to asymptomatic oral mucosa
-HPE-HPE
-Direct immunofluorescence-Direct immunofluorescence
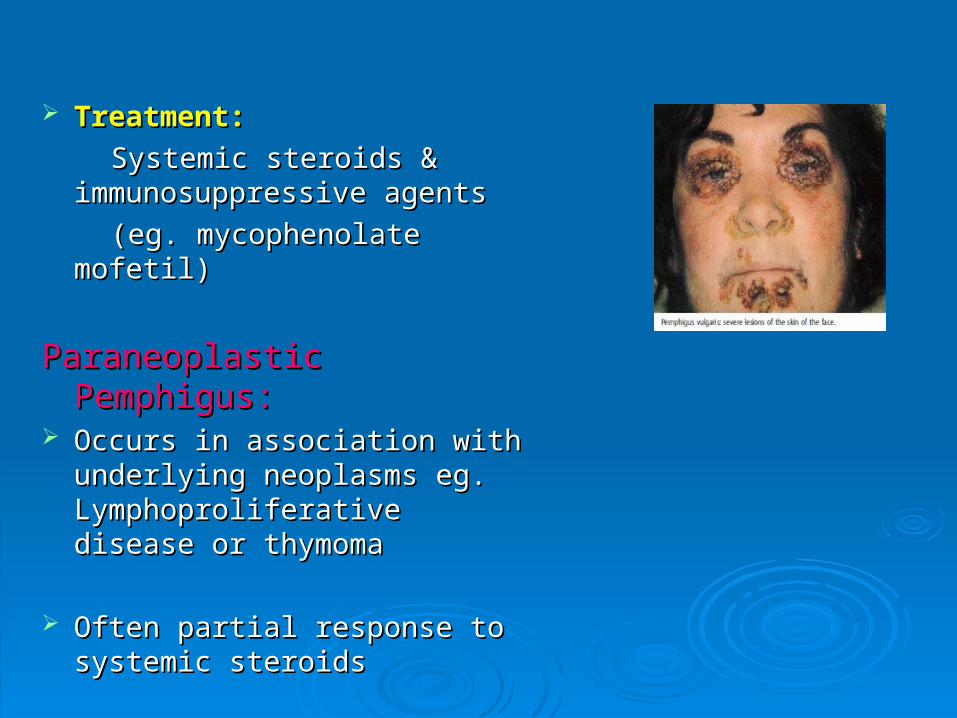
Treatment: Treatment:
Systemic steroids & Systemic steroids & immunosuppressive agents immunosuppressive agents
(eg. mycophenolate mofetil)(eg. mycophenolate mofetil)
Paraneoplastic Pemphigus:Paraneoplastic Pemphigus: Occurs in association with Occurs in association with
underlying neoplasms eg. underlying neoplasms eg. Lymphoproliferative disease or Lymphoproliferative disease or thymomathymoma
Often partial response to Often partial response to systemic steroidssystemic steroids

Mucous Membrane PemphigoidMucous Membrane Pemphigoid
Antigen: Human alpha-6 integrinAntigen: Human alpha-6 integrin
Oral manifestations-Oral manifestations- recurrent vesicles recurrent vesicles or bullae (persists longer than or bullae (persists longer than pemphigus) that rupture, leaving large, pemphigus) that rupture, leaving large, superficial painful ulcerssuperficial painful ulcers
Gingival involvement - Gingival involvement - desquamative desquamative gingivitis gingivitis characterised bycharacterised by erythematous, sore gingivaeerythematous, sore gingivae
Diagnosis:Diagnosis: BiopsyBiopsy Treatment:Treatment: topical steroid/systemic topical steroid/systemic
immunosuppressive drugsimmunosuppressive drugs

Erythema MultiformeErythema Multiforme Skin and mucous membranesSkin and mucous membranes Immunologically mediatedImmunologically mediated Triggered by: infective agents (eg. HSV), Triggered by: infective agents (eg. HSV),
drugs (sulphonamides, barbiturates), food drugs (sulphonamides, barbiturates), food additives or chemical, immunizationadditives or chemical, immunization
( BCG,HBV)( BCG,HBV)
Oral lesions:Oral lesions: begins as erythematous begins as erythematous areaareablisterblisterrupturesrupturesirregular painful irregular painful ulcersulcers
Lips, buccal mucosa, tongue, soft palate, & Lips, buccal mucosa, tongue, soft palate, & floor of mouth floor of mouth
Skin manifestations:Skin manifestations: erythematous, flat, erythematous, flat, round macules, papules, or plaques, round macules, papules, or plaques, usually in a symmetrical pattern- usually in a symmetrical pattern- target or target or iris like lesionsiris like lesions
HPE & ImmunostainingHPE & Immunostaining TreatmentTreatment:: supportive, systemic steroids supportive, systemic steroids

Stevens–Johnson SyndromeStevens–Johnson Syndrome
Severe form of erythema multiforme, involving oral Severe form of erythema multiforme, involving oral mucous membrane, eyes, & genital areamucous membrane, eyes, & genital area
EtiologyEtiology:: Drugs (salicylates, sulfonamides, Drugs (salicylates, sulfonamides, penicillin, barbiturates,carbamazepine, phenytoin penicillin, barbiturates,carbamazepine, phenytoin etc.)etc.)
oral lesions -oral lesions - vesicle formation, followed by painful vesicle formation, followed by painful erosions - grayish-white or hemorrhagic erosions - grayish-white or hemorrhagic pseudomembranes - extend to the pharynx, larynx, pseudomembranes - extend to the pharynx, larynx, and esophagusand esophagus
Ulceration of skin & mucosal surfaces(eg. mouth, Ulceration of skin & mucosal surfaces(eg. mouth, urethra, conjunctiva, & lungs)urethra, conjunctiva, & lungs)
Typical target lesions on palms & soles with Typical target lesions on palms & soles with blistering in the centreblistering in the centre
DiagnosisDiagnosis:: Clinical presentationClinical presentation
TreatmentTreatment:: --self limitingself limiting -Supportive, & Systemic steroids-Supportive, & Systemic steroids
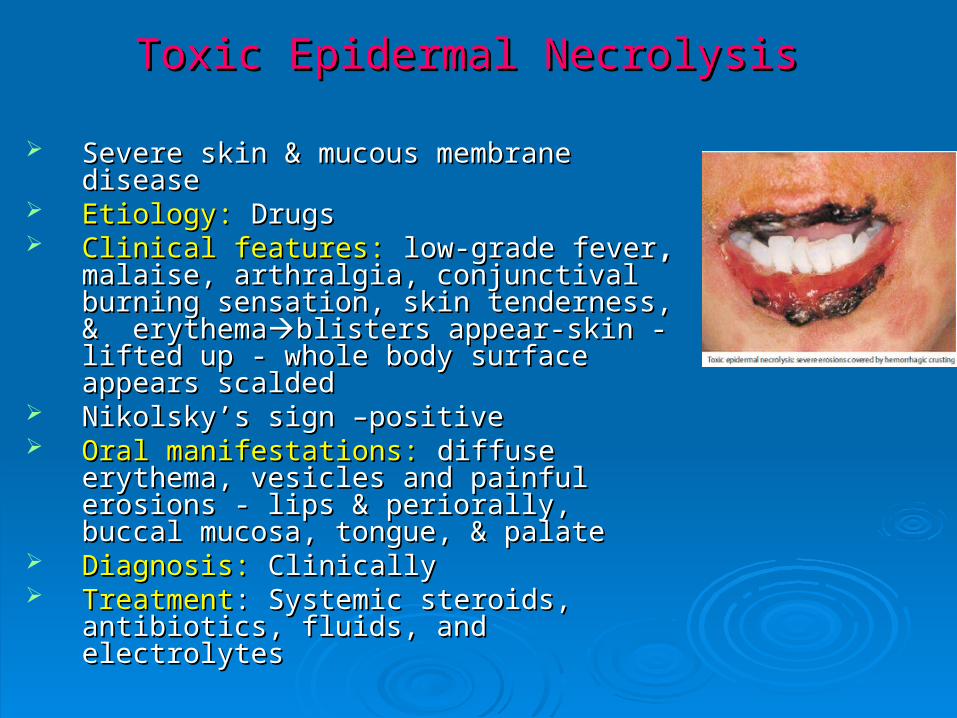
Toxic Epidermal NecrolysisToxic Epidermal Necrolysis
Severe skin & mucous membrane Severe skin & mucous membrane diseasedisease
Etiology: Etiology: DrugsDrugs Clinical features: Clinical features: low-grade feverlow-grade fever, ,
malaise, arthralgia, conjunctival burning malaise, arthralgia, conjunctival burning sensation, skin tenderness, & sensation, skin tenderness, & erythemaerythemablisters appear-skin - lifted up blisters appear-skin - lifted up - whole body surface appears scalded- whole body surface appears scalded
Nikolsky’s sign –positiveNikolsky’s sign –positive Oral manifestations: Oral manifestations: diffuse erythema, diffuse erythema,
vesicles and painful erosions - lips & vesicles and painful erosions - lips & periorally, buccal mucosa, tongue, & periorally, buccal mucosa, tongue, & palate palate
Diagnosis: Diagnosis: ClinicallyClinically TreatmentTreatment: Systemic steroids, antibiotics, : Systemic steroids, antibiotics,
fluids, and electrolytesfluids, and electrolytes

Neurologic DiseasesNeurologic Diseases
1.1. Parkinson’s DiseaseParkinson’s Disease
2.2. Alzheimer’s DiseaseAlzheimer’s Disease
3.3. Bell’s PalsyBell’s Palsy
4.4. Moebius syndromeMoebius syndrome
5.5. Melkersson-Rosenthal SyndromeMelkersson-Rosenthal Syndrome
6.6. Guillain-Barre SyndromeGuillain-Barre Syndrome
7.7. Bulbar palsyBulbar palsy
8.8. Multiple SclerosisMultiple Sclerosis
9.9. Myasthenia GravisMyasthenia Gravis
10.10. Myotonic Muscular DystrophyMyotonic Muscular Dystrophy
11.11. Tuberous SclerosisTuberous Sclerosis

Parkinson’s DiseaseParkinson’s Disease
Extrapyramidal symptomsExtrapyramidal symptoms Loss of facial expressionLoss of facial expression Difficulty with mastication, slow Difficulty with mastication, slow
speech, & tremors of head, lips, & speech, & tremors of head, lips, & tonguetongue
Esophageal dysmotility & Esophageal dysmotility & dysphagiadysphagia
Impaired lip sealImpaired lip seal drooling drooling fungal infection of lip commissure fungal infection of lip commissure (angular cheilitis)(angular cheilitis)
Alzheimer’s DiseaseAlzheimer’s Disease
DementiaDementia
Inability to perform self care (oral hygiene)- Inability to perform self care (oral hygiene)- self neglect & loss of cognitive and motor skillsself neglect & loss of cognitive and motor skills
Poor oral hygiene- increased prevalence of Poor oral hygiene- increased prevalence of dental plaque, dental caries, & gingival dental plaque, dental caries, & gingival bleedingbleeding
Multiple SclerosisMultiple Sclerosis
Demyelination of central nervous Demyelination of central nervous systemsystem
Remitting & exacerbating courseRemitting & exacerbating course Loss of muscle coordination, Loss of muscle coordination,
weakness of the tongue, & loss of weakness of the tongue, & loss of upper extremityupper extremity severely impairs severely impairs orodental hygieneorodental hygiene
Trigeminal neuralgia- also commonTrigeminal neuralgia- also common
characterized by excruciating, characterized by excruciating, unilateral pain of the lips, gingiva, unilateral pain of the lips, gingiva, or chin triggered by contact with or chin triggered by contact with certain areas of the face, lips, or certain areas of the face, lips, or tonguetongue
Bell’s PalsyBell’s Palsy
Idiopathic unilateral lower motor Idiopathic unilateral lower motor neuron palsy (7neuron palsy (7thth cranial nerve) cranial nerve)
Lack of control of the muscles of Lack of control of the muscles of facial expressionfacial expressiondistortion of facial distortion of facial appearance appearance
Loss of functional ability of cheek & Loss of functional ability of cheek & lips (affected side)lips (affected side)poor oro-dental poor oro-dental hygienehygiene

Melkersson-Rosenthal SyndromeMelkersson-Rosenthal Syndrome
Characterized by -unilateral facial palsy, recurrent facial Characterized by -unilateral facial palsy, recurrent facial swelling, & lingua plicata (fissured tongue)swelling, & lingua plicata (fissured tongue)

Nutritional DeficiencyNutritional Deficiency
Vitamins & trace elements Vitamins & trace elements
1.1. Inadequate intakeInadequate intake
2.2. Impaired digestion & absorptionImpaired digestion & absorption
3.3. Increased lossesIncreased losses
Vitamin A deficiency: Vitamin A deficiency:
-Dyskeratotic changes of the skin & mucous -Dyskeratotic changes of the skin & mucous membranesmembranes
-Angular cheilitis-Angular cheilitis
-Defects in the dentin & enamel of -Defects in the dentin & enamel of developing teethdeveloping teeth
Vitamin B2 (Riboflavin) deficiency:Vitamin B2 (Riboflavin) deficiency:
-Angular cheilitis-Angular cheilitis
-Burning pain in the lips, mouth, & tongue-Burning pain in the lips, mouth, & tongue
Vitamin B3 (Niacin) deficiency (Pellagra):Vitamin B3 (Niacin) deficiency (Pellagra):
-Dermatitis, dementia,& diarrhoea-Dermatitis, dementia,& diarrhoea
-Oral manifestations: glossitis (red, swollen) & -Oral manifestations: glossitis (red, swollen) & stomatitis, burning tonguestomatitis, burning tongue

Vitamin B6 deficiency: Vitamin B6 deficiency:
-Peripheral neuropathy-Peripheral neuropathy
-Oral lesions-similar to pellagra -Oral lesions-similar to pellagra
(i.e. glossitis & stomatitis)(i.e. glossitis & stomatitis)
Vitamin C deficiency (Scurvy):Vitamin C deficiency (Scurvy):
-Cofactor for collagen synthesis-Cofactor for collagen synthesis
-Weakened vessels are responsible for -Weakened vessels are responsible for petechiae, ecchymoses, delayed wound petechiae, ecchymoses, delayed wound healing healing
Deficiency of Vitamin B12 & Folic acid:Deficiency of Vitamin B12 & Folic acid:
-Megaloblastic anemia-Megaloblastic anemia
-Oral findings: angular cheilitis, recurrent -Oral findings: angular cheilitis, recurrent aphthous ulcers, & glossitisaphthous ulcers, & glossitis
Vitamin D deficiency & Calcium deficiency:Vitamin D deficiency & Calcium deficiency: -Calcium metabolism-Calcium metabolism -Mandibular osteopenia/osteoporosis, enamel -Mandibular osteopenia/osteoporosis, enamel
hypoplasiahypoplasia Vitamin k deficiency:Vitamin k deficiency: -Haemorrhagic diathesis-Haemorrhagic diathesis -Oral haemorrhagic bullae-Oral haemorrhagic bullae
Zinc deficiency:Zinc deficiency: -Taste changes-Taste changes -Acrodermatitis Enteropathica: angular cheilitis, -Acrodermatitis Enteropathica: angular cheilitis,
ulcers, glossitis, crusting, scaling of the lips as well ulcers, glossitis, crusting, scaling of the lips as well as ulcers, erosions & fissuresas ulcers, erosions & fissures

Oral lesions associated with HIVOral lesions associated with HIV
Early recognition, diagnosis, & treatment of Early recognition, diagnosis, & treatment of HIV associated oral lesions - reduce morbidityHIV associated oral lesions - reduce morbidity
Oral lesions-Oral lesions- -Early diagnostic indicator of HIV infection-Early diagnostic indicator of HIV infection -Stage of HIV infection-Stage of HIV infection -Predictor of the progression of HIV disease-Predictor of the progression of HIV disease

Oral lesions associated with HIV Oral lesions associated with HIV
Fungal Infection: Bacterial Infection:Fungal Infection: Bacterial Infection:
-Candidiasis -Linear Gingival Erythema -Candidiasis -Linear Gingival Erythema
-Histoplasmosis -Necrotizing Ulcerative -Histoplasmosis -Necrotizing Ulcerative PeriodontitisPeriodontitis
-Cryptococcosis -Mycobacterium Avium Complex-Cryptococcosis -Mycobacterium Avium Complex Viral Infection: Neoplastic:Viral Infection: Neoplastic:
-Herpes simplex -Kaposi’s Sarcoma-Herpes simplex -Kaposi’s Sarcoma
-Herpes zoster -Non-Hodgkin’s Lymphoma-Herpes zoster -Non-Hodgkin’s Lymphoma
-HPV Infection -HPV Infection Others:Others:
-CMV Infection -Recurrent Aphthous Ulcers-CMV Infection -Recurrent Aphthous Ulcers
-Hairy Leukoplakia -Salivary Gland Disease-Hairy Leukoplakia -Salivary Gland Disease
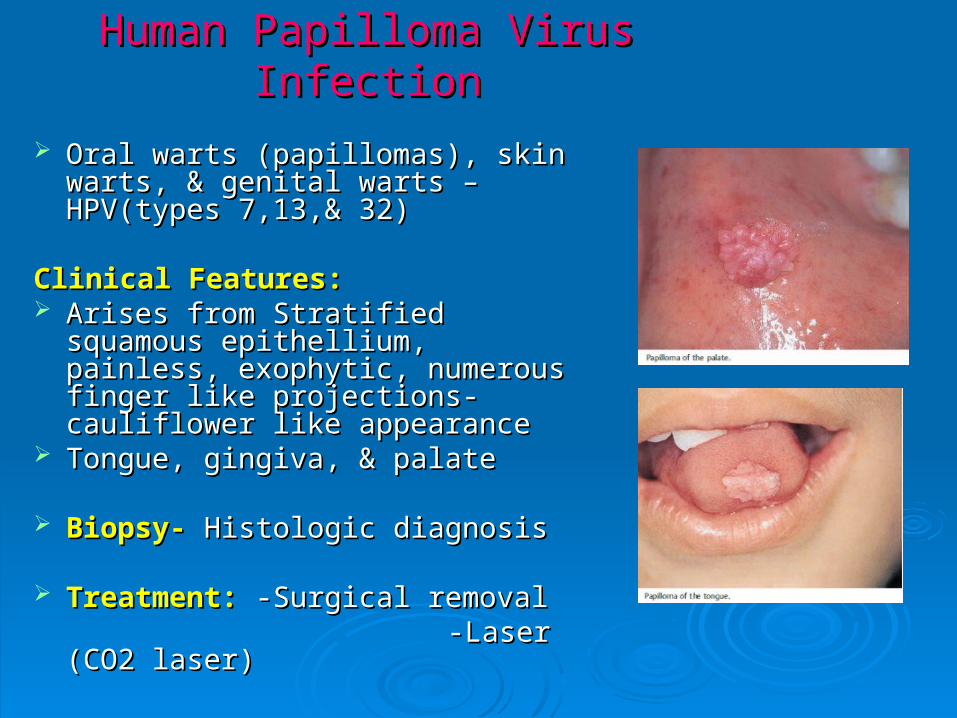
Human Papilloma Virus InfectionHuman Papilloma Virus Infection
Oral warts (papillomas), skin warts, & Oral warts (papillomas), skin warts, & genital warts – HPV(types 7,13,& 32)genital warts – HPV(types 7,13,& 32)
Clinical Features:Clinical Features: Arises from Stratified squamous Arises from Stratified squamous
epithellium, painless, exophytic, epithellium, painless, exophytic, numerous finger like projections- numerous finger like projections- cauliflower like appearancecauliflower like appearance
Tongue, gingiva, & palateTongue, gingiva, & palate
Biopsy-Biopsy- Histologic diagnosisHistologic diagnosis
Treatment:Treatment: -Surgical removal-Surgical removal -Laser (CO2 laser)-Laser (CO2 laser)
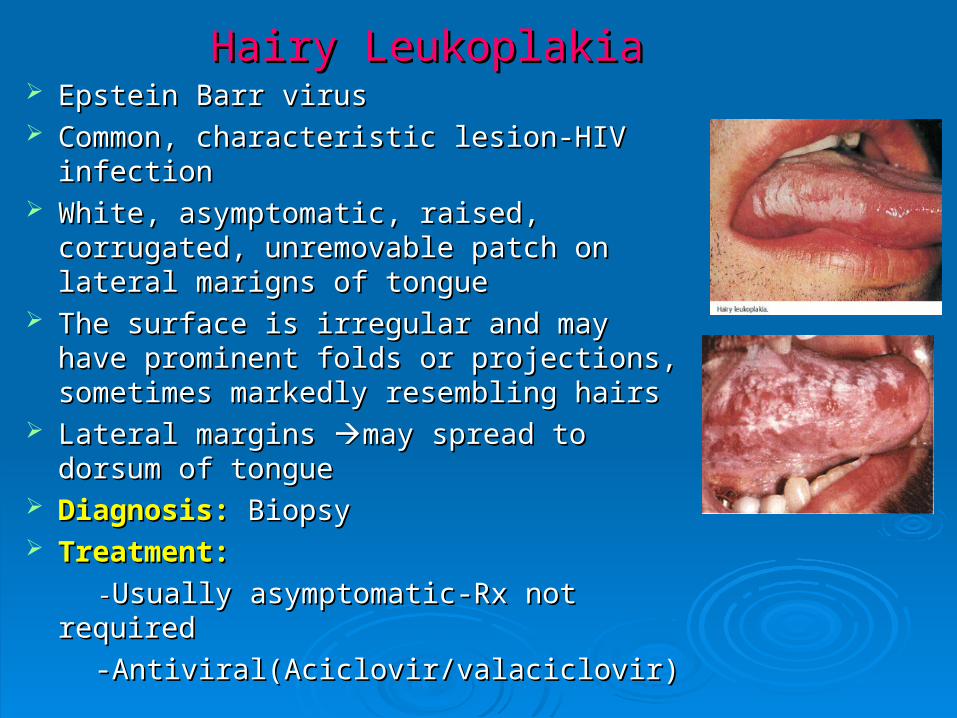
Hairy LeukoplakiaHairy Leukoplakia Epstein Barr virusEpstein Barr virus Common, characteristic lesion-HIV infectionCommon, characteristic lesion-HIV infection White, asymptomatic, raised, corrugated, White, asymptomatic, raised, corrugated,
unremovable patch on lateral marigns of unremovable patch on lateral marigns of tonguetongue
The surface is irregular and may have The surface is irregular and may have prominent folds or projections, sometimes prominent folds or projections, sometimes markedly resembling hairsmarkedly resembling hairs
Lateral margins Lateral margins may spread to dorsum of may spread to dorsum of tonguetongue
Diagnosis:Diagnosis: Biopsy Biopsy Treatment:Treatment:
--Usually asymptomatic-Rx not required Usually asymptomatic-Rx not required
-Antiviral(Aciclovir/valaciclovir)-Antiviral(Aciclovir/valaciclovir)

Kaposi’s SarcomaKaposi’s Sarcoma Most common malignancy in HIV (+Ve)Most common malignancy in HIV (+Ve) Human Herpes Virus-8(KSHV)Human Herpes Virus-8(KSHV) Derived from capillary endothelial cellsDerived from capillary endothelial cells Occur intraorally, either alone or in a/w Occur intraorally, either alone or in a/w
skin & disseminated lesions (lymph skin & disseminated lesions (lymph nodes, salivary gland)nodes, salivary gland)
Intraorally-Intraorally- hard palate, buccal mucosa, & hard palate, buccal mucosa, & gingivagingiva
-bluish, purple or red patches or -bluish, purple or red patches or papulespapulesnodular, ulcerate & bleednodular, ulcerate & bleed
Diagnosis:Diagnosis: Biopsy Biopsy Treatment:Treatment: -Low dose radiation & chemotherapy -Low dose radiation & chemotherapy
(eg.Vinblastine)(eg.Vinblastine) -Surgical excision (eg.CO2 laser)-Surgical excision (eg.CO2 laser) -Immunotherapy (Interferon)-Immunotherapy (Interferon)
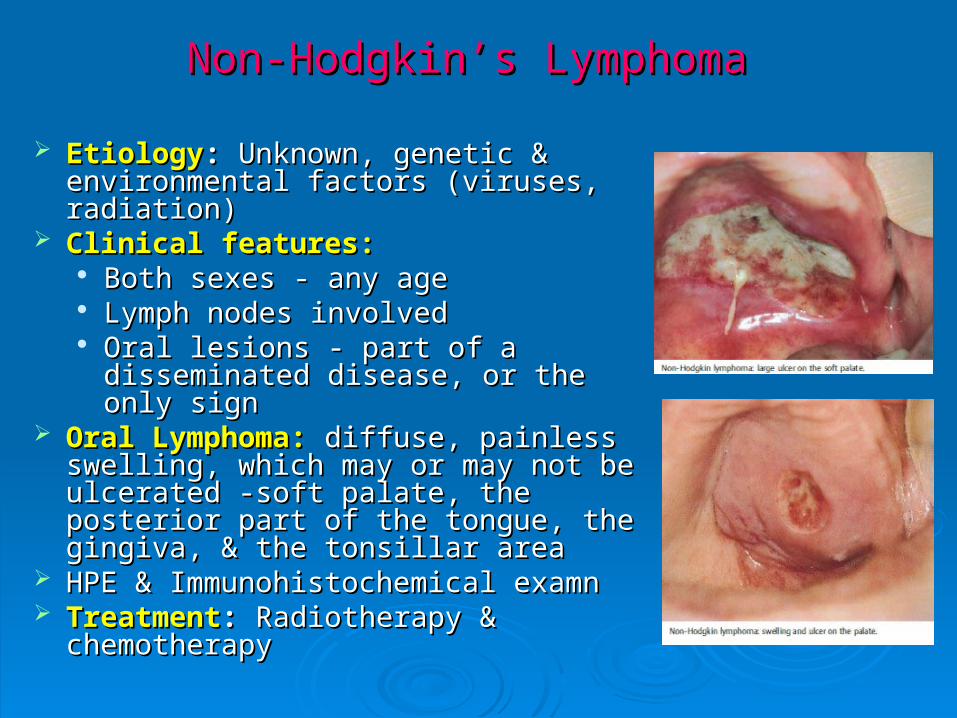
Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
EtiologyEtiology:: Unknown, genetic & Unknown, genetic & environmental factors (viruses, environmental factors (viruses, radiation)radiation)
Clinical features:Clinical features: Both sexes - any age Both sexes - any age Lymph nodes involvedLymph nodes involved Oral lesions - part of a disseminated Oral lesions - part of a disseminated
disease, or the only signdisease, or the only sign Oral Lymphoma:Oral Lymphoma: diffuse, painless diffuse, painless
swelling, which may or may not be swelling, which may or may not be ulcerated -soft palate, the posterior part ulcerated -soft palate, the posterior part of the tongue, the gingiva, & the of the tongue, the gingiva, & the tonsillar area tonsillar area
HPE & Immunohistochemical examnHPE & Immunohistochemical examn TreatmentTreatment:: Radiotherapy & Radiotherapy &
chemotherapychemotherapy

Salivary gland DiseaseSalivary gland Disease
XerostomiaXerostomia Generalised enlargement of parotid Generalised enlargement of parotid
glandsglands
Lymphoepithelial cysts-Lymphoepithelial cysts- parotid parotid glandgland