Oral kinetics and bioavailability of the cholinesterase reactivator HI-6 after administration of 2...
7
Toxicology Letters, 39 (1987) 85-91 Elsevier 85 TXL 01872 ORAL KINETICS AND BIOAVAILABILITY OF THE CHOLINESTERASE REACTIVATOR HI-6 AFTER ADMINISTRATION OF 2 DIFFERENT FORMULATIONS OF TABLETS TO DOGS (Organophosphorus poisoning; antidotes; oximes; pharmacokinetics) MATEJ MAKSIMOVIC, DUSAN JOVANOVIC, VELJKO KOVACEVIC and DUBRAVKO BOKONJIC Military Technical Institute, Belgrade (Yugoslavia) (Received 12 May 1987) (Revision received 6 July 1987) (Accepted 7 July 1987) SUMMARY A one-compartment open model with first-order absorption was used for comparing new oral formula- tions of the potent acetylcholinesterase reactivating oxime HI-6. Although mean peak plasma levels did not differ between retard and conventional tablets (21.38 and 20.74 pmol/I), the time for reaching peak levels was significantly longer (5.5 h) with retard than with conventional tablets (2.86 h). Among other pharmacokinetic estimates only absorption half-lives and areas under the concentration-time curve (AUC) were significantly different (P < 0.05). The AUC with retard tablets was 8.07% and that of con- ventional tablets 5.42% of intravenous AUC, indicating low bioavailability of oral HI-6 formulations. Potential therapeutic use of HI-6 requires, therefore, further investigations in order to improve its gastrointestinal absorption. INTRODUCTION Various oximes (pralidoxime, toxogonin and HI-6) are effective antidotes in organophosphorus poisoning. Therefore, the oximes have been accepted as part of the therapeutic regimen against poisoning by anticholinesterase compounds. In most studies the oximes were administered by the intravenous and intramuscular route. The oral route is less recommended because these drugs, being charged com- Address for correspondence: M. Maksimovic, Military Technical Institute, Kataniceva 15, 11002 Belgrade, Yugoslavia. Abbreviations: AUC, area under the concentration-time curve; HI-6, pyridinium-1-( [(4carbamoyl- pyridiniohnethoxylmethyl ) -2-(hydroxyiminomethyI)dichloride monohydrate. 03784274/87/$ 03.50 0 1987 Elsevier Science Publishers B.V. (Biomedical Division)
Transcript of Oral kinetics and bioavailability of the cholinesterase reactivator HI-6 after administration of 2...

Toxicology Letters, 39 (1987) 85-91 Elsevier
85
TXL 01872
ORAL KINETICS AND BIOAVAILABILITY OF THE CHOLINESTERASE REACTIVATOR HI-6 AFTER ADMINISTRATION OF 2 DIFFERENT FORMULATIONS OF TABLETS TO DOGS
(Organophosphorus poisoning; antidotes; oximes; pharmacokinetics)
MATEJ MAKSIMOVIC, DUSAN JOVANOVIC, VELJKO KOVACEVIC and
DUBRAVKO BOKONJIC
Military Technical Institute, Belgrade (Yugoslavia)
(Received 12 May 1987)
(Revision received 6 July 1987)
(Accepted 7 July 1987)
SUMMARY
A one-compartment open model with first-order absorption was used for comparing new oral formula-
tions of the potent acetylcholinesterase reactivating oxime HI-6. Although mean peak plasma levels did
not differ between retard and conventional tablets (21.38 and 20.74 pmol/I), the time for reaching peak
levels was significantly longer (5.5 h) with retard than with conventional tablets (2.86 h). Among other
pharmacokinetic estimates only absorption half-lives and areas under the concentration-time curve
(AUC) were significantly different (P < 0.05). The AUC with retard tablets was 8.07% and that of con-
ventional tablets 5.42% of intravenous AUC, indicating low bioavailability of oral HI-6 formulations.
Potential therapeutic use of HI-6 requires, therefore, further investigations in order to improve its
gastrointestinal absorption.
INTRODUCTION
Various oximes (pralidoxime, toxogonin and HI-6) are effective antidotes in organophosphorus poisoning. Therefore, the oximes have been accepted as part of the therapeutic regimen against poisoning by anticholinesterase compounds. In most studies the oximes were administered by the intravenous and intramuscular route. The oral route is less recommended because these drugs, being charged com-
Address for correspondence: M. Maksimovic, Military Technical Institute, Kataniceva 15, 11002
Belgrade, Yugoslavia.
Abbreviations: AUC, area under the concentration-time curve; HI-6, pyridinium-1-( [(4carbamoyl-
pyridiniohnethoxylmethyl ) -2-(hydroxyiminomethyI)dichloride monohydrate.
03784274/87/$ 03.50 0 1987 Elsevier Science Publishers B.V. (Biomedical Division)

86
pounds, are poorly absorbed from the gastrointestinal tract [l-4]. However, as sug-
gested earlier [2,5], in cases of mild poisoning or when oximes are given
prophylactically, the oral administration of oximes may be feasible. In such cases
oximes have to be taken 2-4 times daily because of their relatively short elimination
half-lives of 2-3 h. If a simpler treatment regimen is needed, it is more convenient
to use long-acting formulations of oximes. Consequently, regarding the persistence
of the oxime in the blood of dogs, Cvetkovic et al. [6] reported that pralidoxime
retard tablets were superior to the conventional ones.
To assess how well HI-6 (pyridinium-1-([(4-carbamoyl-pyridinio)methoxy]-
methyl ) -2-(hydroxyiminomethyl)dichloride monohydrate), one of the most effec-
tive oximes, is absorbed after oral administration, the absorption and elimination
profiles of conventional and retard tablets of HI-6 were studied in dogs and com-
pared to those following i.v. injection of HI-6.
MATERIALS AND METHODS
Animals and test drugs Two studies of oral and one study of intravenous HI-6 kinetics were carried out
in 11 German shepherd dogs of both sexes, weighing 20-28 kg (mean 25.1 kg). Prior
to the experiment, the animals were fasted for 24 h; water was available ad libitum.
Conventional and retard tablets of HI-6, containing 472.3 and 257.1 mg of HI-6,
respectively, were formulated by the Bosnalijek drug company (Sarajevo).
Procedures
Hi-6 retard tablets were administered to all 11 dogs (mean HI-6 dose was 0.27
mmol/kg). To 7 of them conventional tablets were administered (mean dose 0.24
mmol/kg), and 3 other dogs received HI-6 i.v. (0.27 mmol/kg), with one week be-
tween each treatment period.
In the oral studies the dogs swallowed intact tablets together with minced raw
meat. For oxime determination blood samples were drawn from the femoral vein
at 0.5, 1 and every following hour up to 11 h after administration. Samples were
centrifuged and plasma was analysed for HI-6 by the spectrophotometric method
of Maksimovic and Vojvodic [7], with a detection limit of 2.5 pmol/l.
In the i.v. study blood samples were taken at 2, 5, 7, 10, 15, 20, 40, 60, 80, 120,
180, 240, 300 and 360 min, and plasma was analysed for HI-6.
Data analysis Plasma HI-6 concentrations versus time curves were analysed using a two-
compartment model for the i.v. data and a one-compartment model with first-order
absorption for the oral data. Experimental points were fitted by linear regression
(HP-97 calculator). All pharmacokinetic data were calculated according to Ritschel
[8]. Statistical analysis and comparison of the various pharmacokinetic parameters

obtained with retard and conventional tablets of HI-6 were performed using Stu- dent’s paired t-test. Statistics were calculated with a HP-97 calculator. Differences were considered to be significant at P<O.OS.
RESULTS
The plot of log HI-6 plasma concentrations versus time following 0.27 mmol/kg i.v. in 3 dogs is shown in Fig. 1. Mean initial plasma HI-6 concentration was 1458.8 -t 204.1 pmol/l, falling to 22.0 + 1.9 pmol/l at 6 h. The plasma concentration ver-
0 40 80 120 160 200 240 280 320 360
TIME (m(n)
Fig. 1. Log plasma HI-6 concentrations (mean + SD) versus time following an i.v. dose of 0.27 mmol/kg
to 3 dogs (best computer-fitted line to mean data).
TABLE I
PHARMACOKINETIC PARAMETERS OF HI-6 IN DOGS GIVEN 0.27 mmol/kg i.v.
Pharmacokinetic Dog Mean + SD parameter?
1 2 3
cf, min-’ 0.1962 0.328 0.2658 0.2633 f 0.0659
110~. min 3.53 2.11 2.61 2.75 + 0.72
0, min- ’ 0.0105 0.0109 0.0101 0.0105 f 0.004
tt/2, min 65.9 63.3 68.9 66.03 k 2.8
AUC, pmol/ml/min 93.5 102.87 82.48 92.95 * 10.21
Cl ml/min/kg I0I. 2.98 2.71 3.38 3.02 k 0.34
Vdr I/kg 0.28 0.25 0.33 0.29 k 0.04
a OL, distribution rate constant ti/za, distribution half-life; f3, elimination rate constant; fi/2, elimination
half-life; AUC, area under the curve from zero to infinite; Clt,t, total body clearance, Vd, volume of
distribution.

88
sus time curve was biexponential so that the two-compartment model used for data
analysis. The various pharmacokinetic parameters calculated for the i.v. dose are
shown in Table I.
The mean distribution half-life was 2.75 min, and distribution was complete in
5-15 min. The elimination half-life was 66.03 min and the AUC was 92.95
pmol/ml/min. Total body clearance was 3.02 ml/min/kg, and volume of distribu-
tion was 0.29 l/kg.
During the first 15 min after HI-6 injection all dogs showed tremor, moderate
hypersalivation and irregular respiration that were transient and ceased without se-
quelae.
Fig. 2 shows the plasma concentration vs. time curves for conventional and retard
tablets. The absorption of HI-6 from conventional tablets was more rapid than from
retard tabiets. The mean values of maximal HI-6 plasma levels were similar while
the times at which the maxima were reached were statistically different (Table II).
The elimination rate constants and elimination half-lives for conventional tablets
were very close to those observed for retard tablets. Among other pharmacokinetic
estimates only the AUCs were found to be significantly different. The AUC of con-
ventional tablets was 67% of that for retard tablets.
Only 5.42% of HI-6 was absorbed from conventional tablets and 8.07% HI-6
from slow-release tablets, indicating poor absolute bioavailability. No behavioral
disturbances followed the administration of both forms of tablets to dogs.
l CONVENTIONAL TBL, N=7
0 RETARD TEL, N=ll
u 9-
0 1 2 3 4 5 6 7 a 9 10 11
Fig. 2. Conventional and retard HI-6 tablets: comparison of plasma HI-6 concentrations in dogs. Open
and filled circles are the means. The solid line is the best computer-fitted curve to mean data.
89
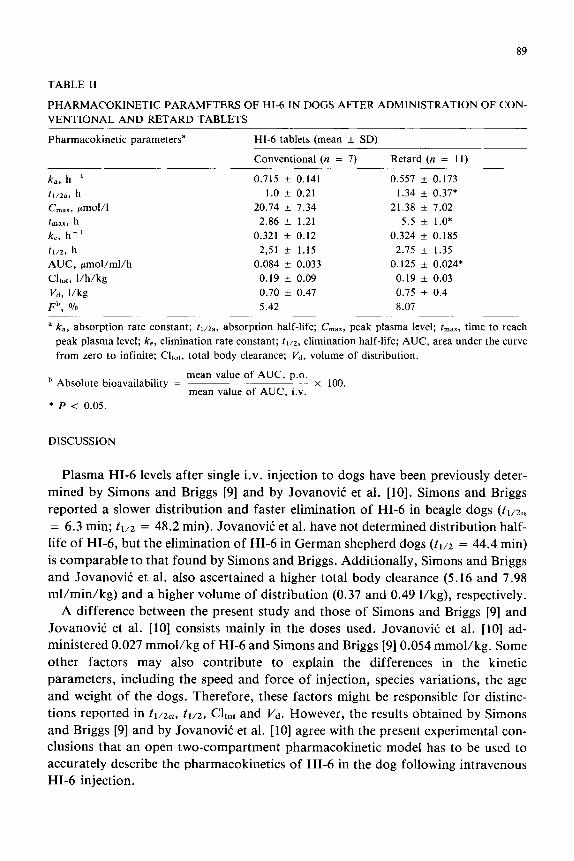
TABLE II
PHARMACOKINETIC PARAMETERS OF HI-6 IN DOGS AFTER ADMINISTRATION OF CON-
VENTIONAL AND RETARD TABLETS
Pharmacokinetic parametersa HI-6 tablets (mean + SD)
Conventional (n = 7) Retard (n = 11)
k,, h-’
t1/2a, h
C maX, pmol/l
tln,x, h
k,, h-’
ft/z, h
AUC, gmol/ml/h
Cl,,,, l/h/kg
I’d, l/kg
Fb, %
0.715 + 0.141
1.0 + 0.21
20.74 f 7.34
2.86 * 1.21
0.321 * 0.12
2,51 + 1.15
0.084 + 0.033
0.19 ?Z 0.09
0.70 f 0.47
5.42
0.557 + 0.173
1.34 + 0.37*
21.38 k 7.02
5.5 + 1.0*
0.324 + 0.185
2.75 + 1.35
0.125 + 0.024*
0.19 * 0.03
0.75 * 0.4
8.07
a k,, absorption rate constant; tt/za. absorption half-life; C,,,, peak plasma level; tmax, time to reach
peak plasma level; k,, elimination rate constant; tt/z, elimination half-life; AUC, area under the curve
from zero to infinite; Cl,,,, total body clearance; Vd, volume of distribution.
b Absolute bioavailability = mean value of AUC, p.o.
x 100. mean value of AUC, i.v.
* P < 0.05.
DISCUSSION
Plasma HI-6 levels after single i.v. injection to dogs have been previously deter-
mined by Simons and Briggs [9] and by Jovanovic et al. [ 101. Simons and Briggs
reported a slower distribution and faster elimination of HI-6 in beagle dogs (tr,zol
= 6.3 min; tl/z = 48.2 min). Jovanovic et al. have not determined distribution half-
life of HI-6, but the elimination of HI-6 in German shepherd dogs (ti/2 = 44.4 min)
is comparable to that found by Simons and Briggs. Additionally, Simons and Briggs
and Jovanovic et al. also ascertained a higher total body clearance (5.16 and 7.98
ml/min/kg) and a higher volume of distribution (0.37 and 0.49 l/kg), respectively.
A difference between the present study and those of Simons and Briggs [9] and
Jovanovic et al. [lo] consists mainly in the doses used. Jovanovic et al. [lo] ad-
ministered 0.027 mmol/kg of HI-6 and Simons and Briggs [9] 0.054 mmol/kg. Some
other factors may also contribute to explain the differences in the kinetic
parameters, including the speed and force of injection, species variations, the age
and weight of the dogs. Therefore, these factors might be responsible for distinc-
tions reported in tl/za, tl/z, CL,, and vd. However, the results obtained by Simons
and Briggs [9] and by Jovanovic et al. [ 101 agree with the present experimental con-
clusions that an open two-compartment pharmacokinetic model has to be used to
accurately describe the pharmacokinetics of HI-6 in the dog following intravenous
HI-6 injection.

90
In a study of new oral preparations of HI-6 we have compared the kinetics of con- ventional to retard HI-6 tablets following a single dose. The peak plasma HI-6 levels of both conventional and retard tablets were similar, but the time to reach the peak was significantly longer after administration of retard tablets. Similar results were obtained in dogs using two formulations of pralidoxime [6].
Cvetkovic et al. [6] studied the pharmacokinetics of pralidoxime at about 2-fold higher dose (0.58 mmol/kg), and, in contrast to the present report, found 5-6 times higher levels of pralidoxime following retard and conventional tablets. Evaluating pharmacokinetic parameters from that study [6] we found significant differences (P<O.O5) between conventional and retard pralidoxime tablets in the half-lives of absorption (1.21 and 1.99 h) and in the times at which peak plasma pralidoxime levels were reached (4.2 and 8.3 h). Calculated AUC values for both formulations were similar: 1.21 and 1.18 pmol/ml/h respectively. As the AUC reflect the amount of oxime absorbed, there is a disparity between the plasma levels of HI-6 and pralidoxime. Within the ranges studied, 2-3 times more HI-6 than pralidoxime is needed for a similar blood level.
The low bioavailability of HI-6 after oral administration may reflect a poor ab- sorption of the oxime itself, or could be due to the biotransformation of HI-6 to compounds not detectable by our method. From kinetic studies with HI-6 in rats [4,11,12], dogs [9,13] and man [14] emerges that 40-90’70 of HI-6 is excreted un- changed in urine after i.m. or i.v. administration. Hence extensive biotransforma- tion is unlikely, although the metabolism of HI-6 may be different when it is administered by various routes.
In conclusion, the data presented show significantly different rates of absorption and amounts of HI-6 absorbed (in terms of AUC values) from both oral formula- tions. Very high oral doses of HI-6 will be necessary to achieve therapeutic plasma levels in dogs, since the bioavailability of oral formulations is poor. From the point of further therapeutic promise of HI-6 additional investigations aimed on improve- ment of its absorption are indicated.
ACKNOWLEDGEMENTS
We are indebted to them. Azra Ciranov and them. Svetlana Lazarev from Bosnalijek drug company, Sarajevo, for the skillful synthesis of HI-6, to Ph.c. Lea Levi and Ph.c. Sanja Stjepanovic from Bosnalijek for preparing the tablets and to Mr. Ljubomir TaSiC and Mr. Vladimir Vlaisavljevic for competent technical assistance.
REFERENCES
1 F.R. Sidell, W.A. Groff and R.1. Ellin, Blood levels of oxime and symptoms in humans after single
and multiple doses of 2-pyridine aldoxime methochloride, J. Pharm. Sci., 58 (1969) 1093-1098.

91
2 F.R. Side11 and W.A. Groff, Toxogonin: oral administration to man, J. Pharm. Sci., 60 (1971)
860-863.
3 G.A. Simon, M.S. Tirosh and H. Edery, Administration of obidoxime tablets to man: plasma levels
and side reactions, Arch. Toxicol., 36 (1976) 83-88.
4 M. Maksimovic, Oximes HI-6 and PAM-Cl: comparative pharmacokinetic studies after in-
tramuscular and oral administration to the rat [in Serbocroatian, with summary in English], Arh.
Hig. Rada Toksikol., 30 (1979) 227-239.
5 G.E. Quinby, Feasibility of prophylaxis by oral pralidoxime, Arch. Environ. Health, 16 (1968)
812-820.
6 M. Cvetkovid, D. Jovanovic, S. DuraSinovid and B. BoSkoviC, Kinetics of absorption and elimination
of slow-release pralidoxime tablets in dogs, Iugoslav. Physiol. Pharmacol. Acta, 19 (Suppl. 2) (1983)
23-25.
7 M. Maksimovic and V. Vojvodic, Selection of the method for determination of oxime content in
biological material [in Serbocroatian, with summary in English], Arh. Hig. Rada Toksikol., 20 (1969)
173-176.
8 W.A. Ritschel, Graphic Approach to Clinical Pharmacokinetics, J.R. Prous Publishers, Barcelona,
1984, pp. 74-77.
9 K.J. Simons and C.J. Briggs, The pharmacokinetics of HI-6 in beagle dogs, Biopharm. Drug Disp.,
4 (1983) 375-388.
10 D. Jovanovic, M. Maksimovic and V. KovaEeviC, The pharmacokinetics of HI-6 oxime in atropine
and soman treated dogs, Iugoslav. Physiol. Pharmacol. Acta, 21 (Suppl. 3) (1985) 149-150.
11 D.A. Ligtenstein and S.P. Kossen, Kinetic profile in blood and brain of the cholinesterase reac-
tivating oxime HI-6 after intravenous administration to the rat, Toxicol. Appl. Pharmacol., 71 (1983)
177-183.
12 K.J. Simons and C.J. Briggs, Disposition of HI-6 oxime in rats after intravenous and intramuscular
administration, J. Pharm. Pharmacol., 37 (1985) 367-369.
13 R. Klimmek and P. Eyer, Pharmacokinetics and pharmacodynamics of the oxime HI-6 in dogs,
Arch. Toxicol., 59 (1986) 272-278.
14 R. Ku%, B. BoSkoviC, V. Vojvodic and D. Jovanovic, HI-6 in man: blood levels, urinary excretion,
and tolerance after intramuscular administration of the oxime to healthy volunteers, Fundam. Appl.
Toxicol., 5 (1985) S89-S97.