Oral ginseng formulae for stable chronic obstructive … · REVIEW Oral ginseng formulae for stable...
12
REVIEW Oral ginseng formulae for stable chronic obstructive pulmonary disease: A systematic review Xuedong An a , Anthony Lin Zhang a , Angela Weihong Yang a , Lin Lin b , Darong Wu b , Xinfeng Guo b,e , Johannah Linda Shergis a , Francis Chung Kong Thien c , Christopher J. Worsnop d , Charlie Changli Xue a, * a Discipline of Chinese Medicine, School of Health Sciences, RMIT University, Bundoora, VIC 3083, Australia b Division of Clinical Epidemiology, Guangdong Provincial Hospital of Chinese Medicine, Guangdong 510120, China c Department of Respiratory Medicine, Box Hill Hospital and Monash University, Box Hill, VIC 3128, Australia d Department of Respiratory and Sleep Medicine, Austin Hospital, Heidelberg, VIC 3081, Australia e National DME Training Center, Guangzhou University of Chinese Medicine, Guangdong 510405, China Received 19 February 2010; accepted 12 November 2010 Available online 13 December 2010 KEYWORDS Chronic obstructive pulmonary disease; COPD; Chinese herbal medicine; Ginseng formulae; Systematic review Summary Ginseng alone or combined with other herbs has been increasingly used for chronic obstructive pulmonary disease (COPD). This review aims to evaluate the effectiveness and safety of oral Ginseng formulae for stable COPD. Four English databases and three Chinese databases were searched to identify randomized controlled trials. Methodological quality was assessed by Cochrane risk of bias and Jadad’s scale. Data were analyzed using Review Manager 5.0. Twelve studies overall of low quality, involving 1560 participants were included. Results of three studies showed a mean difference (MD) of 0.30 (95%CI 0.02 to 0.58) for forced expiratory volume in 1 s (FEV 1 ) improvement of Ginseng formulae versus placebo control. Findings of three studies re- vealed an MD of 9.43 (95%CI 3.64 to 15.21) of FEV 1 % predicted between Ginseng formulae and placebo control. Quality of life (Qol) measured by St. George’s Respiratory Questionnaire was Abbreviations: CHM, Chinese herbal medicine; CI, Confidence interval; COPD, Chronic obstructive pulmonary disease; FEV 1 , Forced expi- ratory volume in 1 second; GOLD, The global initiative for chronic obstructive lung disease; MD, Mean difference; Qol, Quality of life; RCTs, Randomized controlled trials; RR, Risk ratio; SGRQ, St. George’s respiratory questionnaire. * Corresponding author. Director, Traditional & Complementary Medicine Research Program, Health Innovations Research Institute, and Discipline of Chinese Medicine, School of Health Sciences, RMIT University, PO Box 71, Bundoora, VIC 3083, Australia. Tel.: þ61 3 99257745; fax: þ61 3 99257178. E-mail addresses: [email protected] (X. An), [email protected] (A.L. Zhang), [email protected] (A.W. Yang), [email protected] (L. Lin), [email protected] (D. Wu), [email protected] (X. Guo), [email protected] (J.L. Shergis), [email protected] (F.C.K. Thien), [email protected] (C.J. Worsnop), [email protected] (C.C. Xue). available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Respiratory Medicine (2011) 105, 165e176 0954-6111/$ - see front matter ª 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.rmed.2010.11.007
Transcript of Oral ginseng formulae for stable chronic obstructive … · REVIEW Oral ginseng formulae for stable...
Respiratory Medicine (2011) 105, 165e176
ava i lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / rmed
REVIEW
Oral ginseng formulae for stable chronic obstructivepulmonary disease: A systematic review
Xuedong An a, Anthony Lin Zhang a, Angela Weihong Yang a, Lin Lin b,Darong Wu b, Xinfeng Guo b,e, Johannah Linda Shergis a,Francis Chung Kong Thien c, Christopher J. Worsnop d,Charlie Changli Xue a,*
aDiscipline of Chinese Medicine, School of Health Sciences, RMIT University, Bundoora, VIC 3083, AustraliabDivision of Clinical Epidemiology, Guangdong Provincial Hospital of Chinese Medicine, Guangdong 510120, ChinacDepartment of Respiratory Medicine, Box Hill Hospital and Monash University, Box Hill, VIC 3128, AustraliadDepartment of Respiratory and Sleep Medicine, Austin Hospital, Heidelberg, VIC 3081, AustraliaeNational DME Training Center, Guangzhou University of Chinese Medicine, Guangdong 510405, China
Received 19 February 2010; accepted 12 November 2010Available online 13 December 2010
KEYWORDSChronic obstructivepulmonary disease;COPD;Chinese herbalmedicine;Ginseng formulae;Systematic review
Abbreviations: CHM, Chinese herbal mratory volume in 1 second; GOLD, TheRandomized controlled trials; RR, Risk* Corresponding author. Director, Tr
Discipline of Chinese Medicine, Schoolfax: þ61 3 99257178.
E-mail addresses: s3059829@[email protected] (L. Lin), [email protected] (F.C
0954-6111/$ - see front matter ª 201doi:10.1016/j.rmed.2010.11.007
Summary
Ginseng alone or combined with other herbs has been increasingly used for chronic obstructivepulmonary disease (COPD). This review aims to evaluate the effectiveness and safety of oralGinseng formulae for stable COPD.
Four English databases and three Chinese databases were searched to identify randomizedcontrolled trials. Methodological quality was assessed by Cochrane risk of bias and Jadad’sscale. Data were analyzed using Review Manager 5.0.
Twelve studiesoverall of lowquality, involving1560participantswere included. Results of threestudies showedamean difference (MD) of 0.30 (95%CI 0.02 to 0.58) for forced expiratory volume in1 s (FEV1) improvement of Ginseng formulae versus placebo control. Findings of three studies re-vealed an MD of 9.43 (95%CI 3.64 to 15.21) of FEV1 % predicted between Ginseng formulae andplacebo control. Quality of life (Qol) measured by St. George’s Respiratory Questionnaire was
edicine; CI, Confidence interval; COPD, Chronic obstructive pulmonary disease; FEV1, Forced expi-global initiative for chronic obstructive lung disease; MD, Mean difference; Qol, Quality of life; RCTs,ratio; SGRQ, St. George’s respiratory questionnaire.
aditional & Complementary Medicine Research Program, Health Innovations Research Institute, andof Health Sciences, RMIT University, PO Box 71, Bundoora, VIC 3083, Australia. Tel.: þ61 3 99257745;
t.rmit.edu.au (X. An), [email protected] (A.L. Zhang), [email protected] (A.W. Yang),[email protected] (D. Wu), [email protected] (X. Guo), [email protected] (J.L. Shergis),.K. Thien), [email protected] (C.J. Worsnop), [email protected] (C.C. Xue).
0 Elsevier Ltd. All rights reserved.

166 X. An et al.
improved (MD �10.32, 95%CI �14.99 to �5.65) with Ginseng formulae plus pharmacotherapyversus pharmacotherapy alone in one study. There were no severe adverse events reported.
Ginseng formulae for stable COPD patients show promising evidence of lung functions and Qolimprovement. However, the degree of benefit is uncertain due to potential risk of bias of theincluded studies.ª 2010 Elsevier Ltd. All rights reserved.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
Search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167Study selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167Data extraction and quality assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167Data analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
Description of studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167Methodological quality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171Assessment of risk of bias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171Assessment of Jadad’s scale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
Outcome measures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171Spirometric parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171Symptom improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172Quality of life . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172COPD exacerbations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172Adverse events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175
Introduction
Chronic obstructive pulmonary disease (COPD) is associatedwith significant morbidity and mortality, and is predicted tobecome the third leading cause of death worldwide by2020.1,2 Over 10% of the global population (age 40 or older)suffers fromstage II orhigherCOPDwith thefigurebeing14.3%for the United States.3 In China, COPD affects 8.2% of indi-viduals who are over 40 years old.4 COPD is characterized byprogressive, non-reversible airflow limitation.5 As there is nocure, symptom management, quality of life (Qol) improve-ment and reducing exacerbations become the primary treat-ment objectives.6 It is generally understood that currentpharmacotherapy does not prevent progression of COPD norimprove lung function.5 Moreover, they have been associatedwith significant adverse events such as oropharyngeal candi-diasis, bruising and risk of pneumonia.6 Complementary andalternative medicines are increasingly being used by patientswith chronic disease.7 Herbal medicines are used by 14% ofadults with chronic pulmonary conditions and specifically,Ginseng is used by 23% of herbal medicine consumers in theUS8 and 6% of the Victorian (Australia) herb users.9
In herbal medicine practice, stable COPD representsa pattern of Qi deficiency involving either Lung or Spleen.Qi is refined nutritive substance involved with functional
activities.10 Ginseng, the root of a perennial plant, isa single herb formula which is a potent tonic to restore andreplenish Qi of the Lung and Spleen to improve theirfunctions and it has been used for treating a wide range ofchronic respiratory conditions.11 There have been anincreasing number of Chinese herbal medicine (CHM) clin-ical trials for the management of stable COPD including theuse of Ginseng formulae (i.e. a combination of severalherbal ingredients).12
A recent systematic review on CHM randomized controlledtrials (RCTs) administered orally or through intravenousinjection for both stable COPD and in acute exacerbationconcluded that CHM had potential benefits for COPD subjectswith Ginseng being one of the most commonly used herbs.13
Two out of 14 included studies involved the use of Ginsengthat demonstrated promising benefits of Ginseng for COPD.However, Ginseng’s effectiveness and safety were notspecifically or thoroughly reviewed.
Orally administered CHM formulae is the traditionaladministration method. The use of Ginseng extract forintravenous and intramuscular injections is not commonlypractised in countries outside China. Therefore, to ensureclinical relevance of findings from this review and allowwidespread application, this review is to evaluate theeffectiveness and safety of orally administered CHM

Figure 1 Flowchart of the study selection process.
Ginseng for chronic obstructive pulmonary disease 167
formulae containing Ginseng or Ginseng extraction (here-after, Ginseng formulae) for stable COPD.
Methods
Search strategy
Guided by the Cochrane Airways Group methodology,14 thefollowing electronic databases were searched: PubMed,CINAHL, Cochrane Central Register of Controlled Trials(CENTRAL), EMBASE, China National Knowledge Infrastruc-ture (CNKI), Chinese Scientific Journals Full text Database(CQVIP) and Wanfang, from their respective inceptions toJune 2009, without language restriction.
Search terms usedwere the combination of COPD, chronicobstructive pulmonary disease, chronic obstructive lungdisease, chronic obstructive airway disease, chronic bron-chitis, emphysema, pulmonary disease and complementarytherapies, Chinese herbal medicine, plant extracts, Chineseherbs, Ginseng, randomized, controlled clinical trial andtheir synonyms.
Study selection
RCTs on stable COPD patients of all stages, of any age,gender or ethnic origin, with or without blinding wereconsidered. Orally administered interventions (i.e. decoc-tion, capsule, tablet, pill or powder) of Ginseng CHMformulae compared with placebo, no treatment, non-Ginseng formulae or pharmacotherapy were examined.Studies using Ginseng formulae combined with other
treatments such as acupuncture as a co-intervention wereexcluded even if the same co-intervention was applied toboth arms. Included studies needed to report at least oneof the following four primary outcome measurements: 1)Spirometric parameters; 2) Percentage of effectiveness ofsymptom changes; 3) Quality of life; 4) Frequency of COPDexacerbations. Adverse events reported in the includedstudies are recorded as a secondary outcome measure.
Data extraction and quality assessment
Details of trial design, sample size, methodological quality,participants, severity of COPD, syndrome differentiation,intervention, outcome measures and adverse events ofeach study were extracted.
Included studies were independently reviewed (XA andAY) for methodological quality, using the Cochrane risk ofbias assessment15 consisting of six domains of potential biaswhich were answered by denoting ‘yes’ (low risk of bias), or‘no’ (high risk of bias) or ‘unclear’ (uncertain risk).15
‘Randomization’, ‘double blinding’ and ‘withdrawals anddropouts’ were assessed using the Jadad’s scale (from0 Z worst to 5 Z best).16 Any disagreement was resolvedby discussion with one of two other reviewers (AZ and CX).
Data analysis
Data were analyzed using RevMan 5.0 software, developedby The Cochrane Collaboration. Dichotomous data werepresented as risk ratio (RR) and continuous outcomes asmean difference (MD) with 95% confidence intervals (CI).Heterogeneity was calculated by c2 and I2 statistics. Twoanalysis models (random effects and fixed effects) wereapplied. Thus, if I2 statistic was less than 50%, the fixedeffect model was applied whereas more than 50% therandom effect model was used.
Results
Description of studies
The initial searches identified 938 entries with 12 studiesmeeting the selection criteria (Fig. 1), 11 were conductedin China17e27 and one in Israel.28 The characteristics of theincluded studies are summarized in Table 1. There were nodisagreements in data extraction between the tworeviewers. The 12 studies involved a total of 1560 stableCOPD patients, ranging from 36 to 600 with four studieshaving more than 100 subjects.18,22,25,27 Eight subjectsdropped out and they were excluded in the originalreport,28 and 1552 subjects (1050 males and 502 females,mean age Z 63.73) were included in the data analysis.
As shown inTable 1, the severity of COPDof participants infive studies17,19,22,23,25 were classified asmild,moderate andsevere. Three studies,18,20,21 based on the classificationsdeveloped by the Chinese Medical Association of RespiratoryDiseases,29 stratified the severity of participants’ COPD asstages I to III. One study28 adapted the American ThoracicSociety’s Standardization of Spirometry30 and moderateseverity of COPD was defined as FEV1 50e65% of predicted.

Table 1 Characteristics of included studies.
First author,date (Ref)
Locationof Hospital
Source ofpatients
Number ofParticipants (R/A)
Number ofMale/Female
Age Mean �SD (years)
Severity of COPD SyndromeDifferentiationof CM
COPD HistoryMean � SD(years)
Chen, 200718 Chendu, China Outpatients T: 59/59 T: 45/14 T: 59.03 � 6.70 T: I: 13, IIA: 20, IIB: 18, III: 8 Lung & Kidneydeficiency
NSC: 58/58 C: 42/16 C: 58.59 � 6.29 C: I: 16, IIA: 19, IIB: 17, III: 6
Chen, 200417 Nanping, China Inpatients T: 30/30 35/25 65.00 � NA Mild 15, Moderate 26, Severe 19 NS 60.21 � NSC: 30/30
Gross, 200228 Tel Aviv, Israel NS T&C: 100/91 T: 30/21 T: 59.0 � 12.6 FEV1: 50e65% of predicted NS NST: 51; C: 41 C: 25/16 C: 62.0 � 10.5
Guo, 200819 Tangshan, China Outpatients T: 50/50 T: 36/14 T: 56.00 � NA T: mild 8, moderate 33, severe 9 NS T: 16.00 � NSC: 50/50 C: 34/16 C: 55.00 � NA C: mild 7, moderate 35, severe 8 C: 14.00 � NS
Hong, 200520 Zhangzhou, China Inpatients &outpatients
T: 18/18 T: 16/2 T: 67.56 � 5.19 T: II: 3, III: 15; C: II: 3, III: 15 Lung & Spleen &Kidney deficiency
T: 15.22 � 5.12C: 18/18 C: 15/3 C: 66.00 � 6.40 C: 14.17 � 6.15
Huang, 200521 Guangzhou, China Outpatients T: 32/32 T: 21/11 T: 69.50 � 11.80 T: II: 17, III: 15; C: II: 18, III: 13 NS T: 8.50 � 3.20C: 31/31 C: 23/8 C: 68.80 � 10.60 C: 8.30 � 3.50
Huang, 200222 Xuzhou, China Inpatients &outpatients
T: 300/300 T: 185/115 T: 52.50 � 4.40 Mild to moderate Lung & Kidneydeficiency
T: 7.20 � 4.40C: 300/300 C: 202/98 C: 57.20 � 10.40 C: 8.50 � 3.60
Li, 200623 Zhengzhou, China NS T: 31/31 T: 22/9 T: 72.00 � 5.00 T: mild 5,moderate 21, severe 6 Lung & Kidneydeficiency
T: 18.40 � 1.10C: 31/31 C: 23/8 C: 71.00 � 7.00 C: mild 4,moderate 21, severe 5 C: 19.50 � 6.60
Lin, 200324 Guangzhou, China Inpatients &outpatients
T: 30/30 T: 20/10 T: 62.00 � NS NS Spleen deficiency T: 16.00 � NSC: 30/30 C: 22/8 C: 60.50 � NS C: 15.40 � NS
Wu, 200625 Xinxiang, China Inpatients &outpatients
T: 100/100 T: 68/32 T: 71.87 � 4.37 T: mild 21, moderate 48,severe 31 C:
Lung & Kidneydeficiency
T: 18.70 � 3.72
C: 100/100 C: 72/28 C: 69.33 � 5.71 mild 23, moderate 51, severe 26 C: 17.81 � 4.57Xiong, 200826 Shenzhen, China Inpatients &
outpatientsT: 30/30 T: 20/10 T&C: 72.00 � NS Average of FEV1: 52.3% Lung & Kidney
deficiencyNS
C: 30/30 C: 21/9Xu, 199627 Luzhou, China Inpatients &
outpatientsT: 72/72 T: 52/20 T: 63.50 � NS; NS Qi deficiency T: 9.50 � NSC: 30/30 C: 21/9 C: 60.80 � NS C: 9.00 � NS
T: treatment; C: control; NS: not specified; COPD: chronic obstructive pulmonary disease; SD: standard deviation; CM: Chinese medicine.
168X.Anetal.
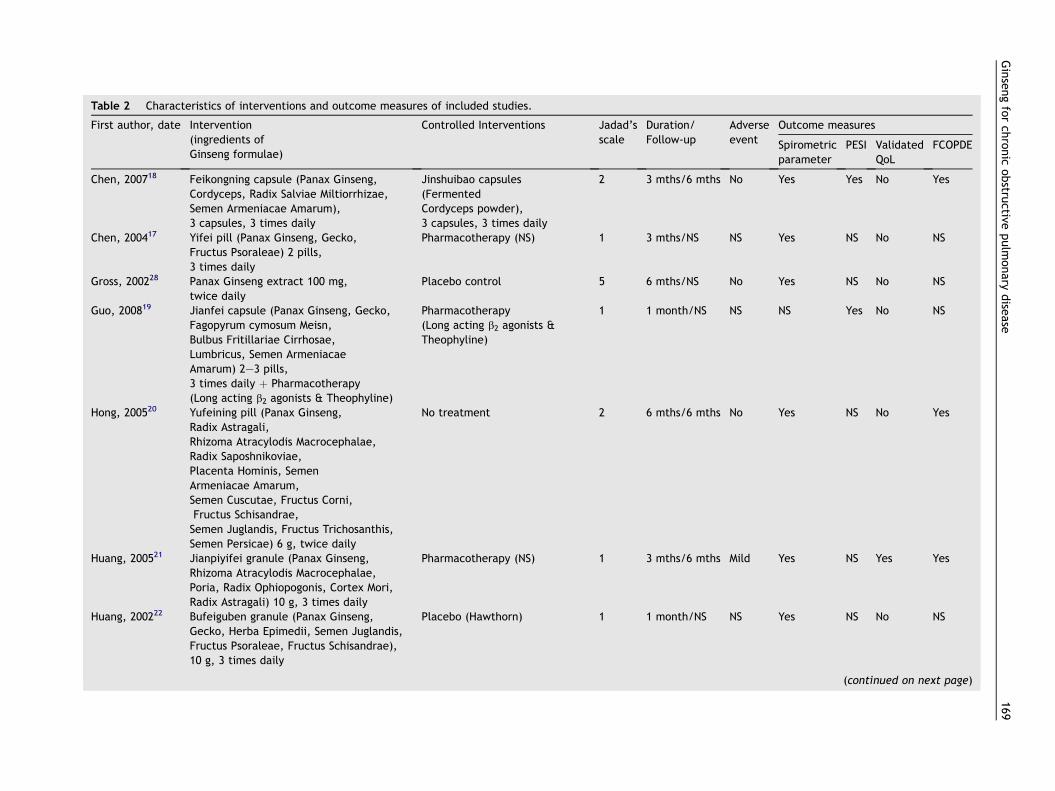
Table 2 Characteristics of interventions and outcome measures of included studies.
First author, date Intervention(ingredients ofGinseng formulae)
Controlled Interventions Jadad’sscale
Duration/Follow-up
Adverseevent
Outcome measures
Spirometricparameter
PESI ValidatedQoL
FCOPDE
Chen, 200718 Feikongning capsule (Panax Ginseng,Cordyceps, Radix Salviae Miltiorrhizae,Semen Armeniacae Amarum),3 capsules, 3 times daily
Jinshuibao capsules(FermentedCordyceps powder),3 capsules, 3 times daily
2 3 mths/6 mths No Yes Yes No Yes
Chen, 200417 Yifei pill (Panax Ginseng, Gecko,Fructus Psoraleae) 2 pills,3 times daily
Pharmacotherapy (NS) 1 3 mths/NS NS Yes NS No NS
Gross, 200228 Panax Ginseng extract 100 mg,twice daily
Placebo control 5 6 mths/NS No Yes NS No NS
Guo, 200819 Jianfei capsule (Panax Ginseng, Gecko,Fagopyrum cymosum Meisn,Bulbus Fritillariae Cirrhosae,Lumbricus, Semen ArmeniacaeAmarum) 2e3 pills,3 times daily þ Pharmacotherapy(Long acting b2 agonists & Theophyline)
Pharmacotherapy(Long acting b2 agonists &Theophyline)
1 1 month/NS NS NS Yes No NS
Hong, 200520 Yufeining pill (Panax Ginseng,Radix Astragali,Rhizoma Atracylodis Macrocephalae,Radix Saposhnikoviae,Placenta Hominis, SemenArmeniacae Amarum,Semen Cuscutae, Fructus Corni,Fructus Schisandrae,Semen Juglandis, Fructus Trichosanthis,Semen Persicae) 6 g, twice daily
No treatment 2 6 mths/6 mths No Yes NS No Yes
Huang, 200521 Jianpiyifei granule (Panax Ginseng,Rhizoma Atracylodis Macrocephalae,Poria, Radix Ophiopogonis, Cortex Mori,Radix Astragali) 10 g, 3 times daily
Pharmacotherapy (NS) 1 3 mths/6 mths Mild Yes NS Yes Yes
Huang, 200222 Bufeiguben granule (Panax Ginseng,Gecko, Herba Epimedii, Semen Juglandis,Fructus Psoraleae, Fructus Schisandrae),10 g, 3 times daily
Placebo (Hawthorn) 1 1 month/NS NS Yes NS No NS
(continued on next page)
Ginsengforch
ronic
obstru
ctivepulm
onary
dise
ase
169

Table 2 (continued )
First author, date Intervention(ingredients ofGinseng formulae)
Controlled Interventions Jadad’sscale
Duration/Follow-up
Adverseevent
Outcome measures
Spirometricparameter
PESI ValidatedQoL
FCOPDE
Li, 200623 Bufeiyishen granule(Panax Ginseng, Radix Astragali,Radix Saposhnikoviae, FructusPsoraleae, Fructus Schisandrae,Szechwan Lovage Rhizome, SemenArmeniacae Amarum, etc.)10 g, 3 times daily
Placebo control(Hawthorn fruit and Malt)
2 2 mths/NS NS Yes NS No NS
Lin, 200324 Jianpiyifei granule (Radix Ginseng,Rhizoma AtracylodisMacrocephalae, Poria,Radix Ophiopogonis,Cortex Mori, Radix Astragali),10 g, 3 times daily
Placebo control(Stroma granule)
1 2 mths/NS NS Yes Yes No NS
Wu, 200625 Jiaweishenge granule (Panax Ginseng,Gecko, Semen Armeniacae Amarum, BulbusFritillariae Cirrhosae, Poria, Cortex Mori,Radix Astragali, Rhizoma AtracylodisMacrocephalae, Cordyceps,Szechwan Lovage Rhizome,Lumbricus) 60.5 g/packet,1 packet, 3 times daily
Placebo control(Hawthorn, Fructus HordeiGerminatus, medicated leaven)
1 2 mths/NS No Yes NS No NS
Xiong, 200826 Shenge granule (Panax Ginseng,Gecko), 5 g, twice daily
Pharmacotherapy(Inhaled Salmeterol &fluticasone, 50/250 ug,one puff, twice daily)
1 6 mths/NS NS Yes Yes No NS
Xu, 199627 Yiqimianyi granule(Panax Ginseng, RhizomaAtracylodis Macrocephalae, Poria)20 g, 3 times daily
Zhenqi Fuzheng granule(Fructus Ligustri Lucidi,Radix Astragali) 15 g, twice daily
1 30 days/NS NS NS Yes No NS
NS: Not specified; PESI: Percentage of effectiveness of symptoms improvement; QoL: Quality of life; FCOPDE: Frequency of COPD exacerbation.
170X.Anetal.

Figure 2 Summary of assessment of risks of bias+ Yes (low risk of bias) ? Unclear (uncertain risk) − No (high risk of bias)
Ginseng for chronic obstructive pulmonary disease 171
Three studies24,26,27 did not specify the stages of COPD of theparticipants, and none of the papers referenced qualitystandards of spirometry performance.31
Guided by Chinese medicine syndrome differentiationguidelines such as the Chinese Medicine Clinical ResearchGuidelines for New Drugs,32 eight studies reported stableCOPD patients as Lung deficiency with Kidney and/orSpleen deficiency18,20,22e26 or Qi deficiency.27
Six of the 12 studies compared oral Ginseng formulae withplacebo or no treatment.20,22e25,28 Two studies compared
Ginseng formulae with other oral CHM formulae withoutGinseng.18,27 Four studies compared the Ginseng formulaeplus pharmacotherapy or Ginseng formulae alone with phar-macotherapy (inhaled b2 agonist and anti-cholinergic or oraltheophylline alone)17,19,21,26 (Table 2). Duration of treatmentranged from onemonth in three studies,19,22,27 twomonths inthree studies,23e25 three months in three studies,17,18,21 andsix months in three studies.20,26,28 Three studies mentioneda 6-month follow-up period.18,20,21 None of the includedstudies mentioned a run-in period.
Methodological quality
Assessment of risk of biasInformation of sequence generation was adequate for threestudies at low risk of bias (yes)18,20,28 and inadequate fornine studies with unclear risk of bias (unclear).17,19,21e27
The methods of allocation concealment were judged with‘unclear’ in all studies. Blinding was reported in two studieswith one described as double blind28 and another as singleblind.21 However blinding of participants, personnel andoutcome assessors in all studies was ‘unclear’. Low risk ofbias from incomplete outcome data was noted in 11 stud-ies,17e21,23e28 one was ‘unclear’22. Intention-to-treatanalysis was not conducted in any of these studies. Selec-tive outcome reporting was at low risk of bias in six stud-ies18,21e24,27 and at high risk of bias in sixstudies.17,19,20,25,26,28 Assessments of other sources of biasincluded early stopping and baseline imbalance. All 12studies indicated no significant difference of baseline databetween two groups; none of studies reported sample sizecalculation method, therefore information on early stop-ping was insufficient. Overall, other sources of bias were‘unclear’. Detailed information is provided in Fig. 2.
Assessment of Jadad’s scaleOnly one study was rated with a score of 5 (highestquality)28; three studies with a score of 218,20,23 and eightstudies with a score of 117,19,21,22,24e27 (Table 2).
Outcome measures
Spirometric parametersPre and post-treatment mean FEV1
18,20e23,25,26 (Fig. 3)and FEV1 % predicted17,18,20,23e26 (Fig. 4) were reportedin seven studies respectively. Another study did notreport post-treatment FEV1
28 and it was not included inthis analysis. Marginal but significant differences inabsolute FEV1 (MD 0.30, 95%CI 0.02 to 0.58)22,23,25 andFEV1 % predicted (MD 9.43, 95%CI 3.64 to 15.21)23e25
were found between Ginseng formulae and placebo.Similar changes were shown in studies comparing GinsengFormulae with non-ginseng formulae, absolute FEV1 (MD0.25, 95%CI 0.06 to 0.44), and FEV1% predicted (MD 4.76,95%CI 0.36 to 9.16)18. Such changes were not observedusing Ginseng formulae alone versus no treatment (FEV1
[MD 0.10, 95%CI �0.11 to 0.31] and FEV1 % predicted [MD2.32, 95%CI �6.84 to 11.48])20 or versus pharmaco-therapy alone (FEV1 [MD 0.25, 95%CI �1.84 to 2.34] andFEV1 % predicted [MD 2.03, 95%CI �2.63 to 6.69])26 (Figs.3 and 4).
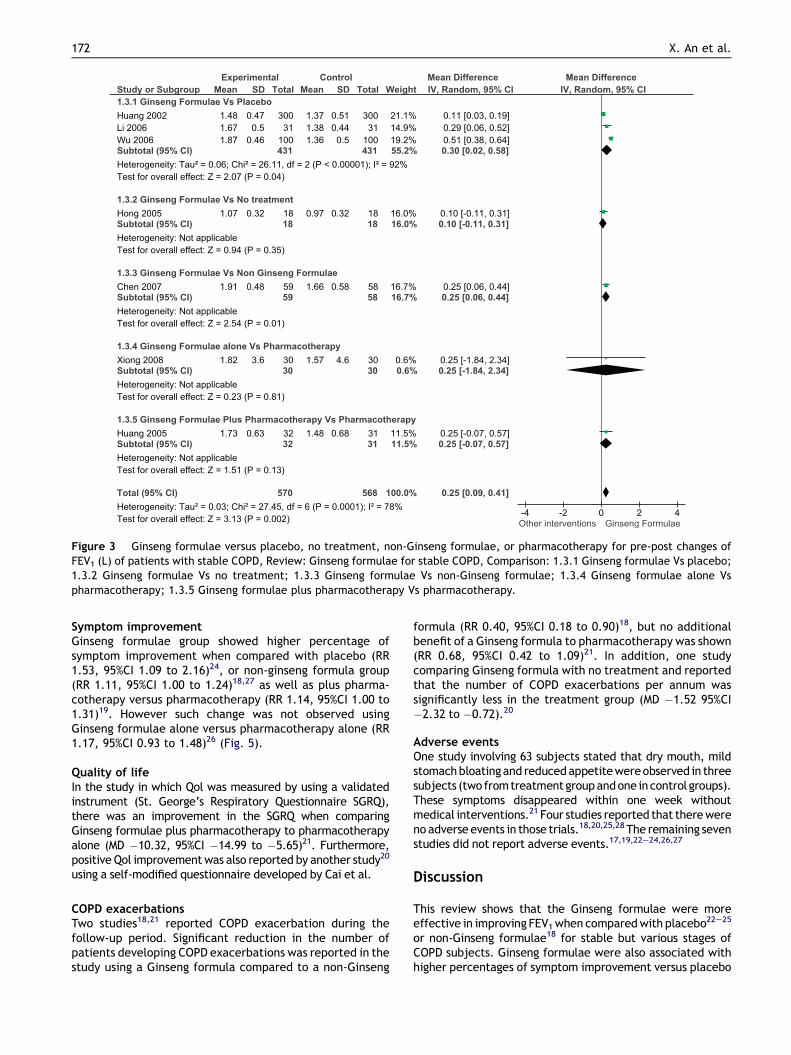
Figure 3 Ginseng formulae versus placebo, no treatment, non-Ginseng formulae, or pharmacotherapy for pre-post changes ofFEV1 (L) of patients with stable COPD, Review: Ginseng formulae for stable COPD, Comparison: 1.3.1 Ginseng formulae Vs placebo;1.3.2 Ginseng formulae Vs no treatment; 1.3.3 Ginseng formulae Vs non-Ginseng formulae; 1.3.4 Ginseng formulae alone Vspharmacotherapy; 1.3.5 Ginseng formulae plus pharmacotherapy Vs pharmacotherapy.
172 X. An et al.
Symptom improvementGinseng formulae group showed higher percentage ofsymptom improvement when compared with placebo (RR1.53, 95%CI 1.09 to 2.16)24, or non-ginseng formula group(RR 1.11, 95%CI 1.00 to 1.24)18,27 as well as plus pharma-cotherapy versus pharmacotherapy (RR 1.14, 95%CI 1.00 to1.31)19. However such change was not observed usingGinseng formulae alone versus pharmacotherapy alone (RR1.17, 95%CI 0.93 to 1.48)26 (Fig. 5).
Quality of lifeIn the study in which Qol was measured by using a validatedinstrument (St. George’s Respiratory Questionnaire SGRQ),there was an improvement in the SGRQ when comparingGinseng formulae plus pharmacotherapy to pharmacotherapyalone (MD �10.32, 95%CI �14.99 to �5.65)21. Furthermore,positive Qol improvementwas also reported by another study20
using a self-modified questionnaire developed by Cai et al.
COPD exacerbationsTwo studies18,21 reported COPD exacerbation during thefollow-up period. Significant reduction in the number ofpatients developing COPD exacerbations was reported in thestudy using a Ginseng formula compared to a non-Ginseng
formula (RR 0.40, 95%CI 0.18 to 0.90)18, but no additionalbenefit of a Ginseng formula to pharmacotherapy was shown(RR 0.68, 95%CI 0.42 to 1.09)21. In addition, one studycomparing Ginseng formula with no treatment and reportedthat the number of COPD exacerbations per annum wassignificantly less in the treatment group (MD �1.52 95%CI�2.32 to �0.72).20
Adverse eventsOne study involving 63 subjects stated that dry mouth, mildstomachbloatingand reducedappetitewereobserved in threesubjects (twofromtreatmentgroupandone incontrol groups).These symptoms disappeared within one week withoutmedical interventions.21 Four studies reported that therewereno adverseevents in those trials.18,20,25,28 The remaining sevenstudies did not report adverse events.17,19,22e24,26,27
Discussion
This review shows that the Ginseng formulae were moreeffective in improving FEV1when comparedwith placebo22e25
or non-Ginseng formulae18 for stable but various stages ofCOPD subjects. Ginseng formulae were also associated withhigher percentages of symptom improvement versus placebo

Figure 4 Ginseng formulae versus placebo or no treatment control, non-Ginseng formulae and pharmacotherapy for pre-postchanges of FEV1% predicted of patients with stable COPD, Review: Ginseng formulae for stable COPD, Comparison: 1.1.1 Ginsengformulae Vs placebo; 1.1.2 Ginseng formulae Vs no treatment; 1.1.3 Ginseng formulae Vs non-Ginseng formulae; 1.1.4 Ginsengformulae alone Vs pharmacotherapy; 1.1.5 Ginseng formulae plus pharmacotherapy Vs pharmacotherapy.
Ginseng for chronic obstructive pulmonary disease 173
or pharmacotherapy.18,19,24,27 A Ginseng formula was benefi-cial for Qol based on SGRQ21 and two Ginseng formulaereduced the frequencyofexacerbations.18,21 Overall,Ginsengformulae were well tolerated by subjects.
Unlike Guo’s review,13 this study focuses on evaluatingthe effectiveness of oral use Ginseng formulae for stableCOPD based on assessment of FEV1, symptom improvement,Qol and frequencies of exacerbations.
The majority of the 12 included studies suffered frommethodological weaknesses based on assessment of theCochrane risk of bias and the Jadad’s scale. The inadequacyof blinding and placebo control,33 allocation concealmentand sequence generation,34 were the major sources ofpotential bias. As well as treatment durations ranging fromone month19,22,27 to six months20,26,28 and using Ginsengformulae as an add-on treatment on routine pharmaco-therapy for COPD.17,19,21,26 Therefore, findings from thisreview need to be interpreted with caution.
Despite the methodological weakness and potential risk ofbias, the findings of the present review are promising.Particularly the improvement of the lung functions based onpre-post FEV1 and FEV1 % predicted between Ginsengformulae and placebo or no treatment or non-Ginsengformulae groups. These findings are consistent with recentRCTs on effect of a phosphodiesterase-4 (PDE4) inhibitor
(roflumilast)35 on lung function in patients with moderate tosevere COPD who were on salmeterol and tiotropium treat-ment. The two trials, involving 1676 COPD subjects concludedthat, compared with placebo, 24 weeks of roflumilast treat-ment significantly and consistently improved mean pre andpost-bronchodilator FEV1 (p < 0.0001).
A large study involving almost 6000 subjects conducted in37 countries demonstrated that prolonged intervention (4years) of a long acting bronchodilator, tiotropium, onmoderate COPD patients (GOLD Stage II) was effective inreducing the rate of decline of post-bronchodilator FEV1.However, such changes were not shown in prebronchodilatorFEV1 between the treatment groups.36 Tiotropium alsoimproved the general health status,Qol basedonSGRQaswellas reducing frequencies of exacerbations and subsequenthospitalisations.37 It was therefore concluded earlier andlong-term intervention is critical to the treatment of COPD.
When Ginseng formulae were compared with placebo ornon-Ginseng formulae, the observed benefits were clearlydemonstrated.17,18,22e26 Such findings showed the poten-tially important role that Ginseng might have played inthese studies, particularly in the study that only a stan-dardized Ginseng extract was used.28
Ginseng as the key herb possesses a broad range ofpharmacological activities which may offer plausible

Figure 5 Ginseng formulae versus placebo or no treatment control, non-Ginseng formulae and pharmacotherapy for pre-postchanges of improvement of effective rate of patients with stable COPD, Review: Ginseng formulae for stable COPD, Comparison:1.2.1 Ginseng formulae Vs placebo; 1.2.2 Ginseng formulae Vs non-Ginseng formulae; 1.2.3 Ginseng formulae alone Vs pharma-cotherapy; 1.2.4 Ginseng formulae plus pharmacotherapy Vs pharmacotherapy.
174 X. An et al.
explanations to the observed clinical benefits in thisreview. For example, Ginseng raw extract or purified gin-senosides have been shown to enhance markedly the actionof the diterpene forskolin in elevating intracellular Cyclicadenosine monophosphate (cAMP) levels in rat culturedglioma cell.38 Two ginsenosides, panaxadiol (PD) and pan-axatriol (PT) have been shown to have potent inhibitoryeffects on the expression of matrix metalloproteinase-9(MMP-9).39 Compound K of ginseng showed similar effects inan experiment with human astroglioma cells.40 In smokers,ginseng taken daily for 4 weeks has been found to linearlyincrease plasma concentrations of certain antioxidants.These findings are significant since oxidative damagecaused by free radicals associated with smoking is thoughtto contribute to the development of COPD.41 Proto-panaxadiol ginsenosides (PPDGs) such as Rb1 and Rb2 havebeen demonstrated to have significant potency as inhibitorsof lipopolysaccharide-induced production of tumor necrosisfactor-alpha (TNF-a) in murine (RAW264.7) cells and human(U937) macrophages.42 This effect was significantlyenhanced by various TNF-a antagonists.42
It is also important to note that due to the heterogeneityof the studies included in this review, the observed benefits
could be a combined outcome of inclusion of unspecifiedproportion of various stages of COPD, the use of a range ofherbal formulations, the uncertain quality of spirometricmeasurements; and the potential of real benefit of Ginsengin treating COPD.
Generally speaking adverse event reporting in theincluded studieswas inadequate. However, the safety profileof Ginseng has been demonstrated in a systematic review,concluding that Panax ginseng mono-preparations are rarelyassociated with adverse events or drug interactions.43
Conclusion
Despite the quality concerns of the included studies, theobserved benefits of Ginseng formulae are encouraging.Further trials are warranted to determine the true benefitsof Ginseng which also address the methodological problemsidentified in this review.
Conflict of interest
None declared.

Ginseng for chronic obstructive pulmonary disease 175
Acknowledgments
XA is supported by an Australian Postgraduate Award at RMITUniversity, Australia. This work was partially supported bya Project Grant from the National Health & MedicalResearch Council (Project Grant Number: 616609), a seedinggrant from the National Institute of Complementary Medi-cine, Australia and an International Research Grant from theGuangdong Provincial Academy of Chinese Medical Sciences,Guangdong Provincial Hospital of Chinese Medicine, China.
References
1. Chapman KR, Mannino DM, Soriano JB, et al. Epidemiology andcosts of chronic obstructive pulmonary disease. Eur Respir J2006;27:188e207.
2. Murray CJ, Lopez AD. Alternative projections of mortality anddisability by cause 1990-2020: global burden of disease study.Lancet 1997;349:1498e504.
3. Buist AS, McBurnie MA, Vollmer WM, et al. International vari-ation in the prevalence of COPD (the BOLD Study): a pop-ulation-based prevalence study. Lancet 2007;370:741e50.
4. Zhong N, Wang C, Yao W, et al. Prevalence of chronicobstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med 2007;176:753e60.
5. The Global Initiative for Chronic Obstructive Lung Disease(GOLD). Global Strategy for diagnosis management andprevention of COPD, http://www.goldcopd.org; 2008.
6. Abramson M, Crockett AJ, Frith PA, et al. The COPD-X Plan:Australian and New Zealand guidelines for the management ofchronic obstructive pulmonary disease 2009, http://www.copdx.org.au/guidelines; 2009.
7. Saydah SH, Eberhardt MS. Use of complementary and alterna-tive medicine among adults with chronic diseases. J AlternComplement Med 2002;2006(12):805e12. United States.
8. Mehta DH, Gardiner PM, Phillips RS, et al. Herbal and dietarysupplement disclosure to health care providers by individualswith chronic conditions. J Altern Complement Med 2008;14:1263e9.
9. Zhang AL, Story DF, Lin V, et al. A population survey on the useof 24 common medicinal herbs in Australia. Pharmacoepide-miol Drug Saf 2008;17:1006e13.
10. World Health Organization (WHO). International standardTerminologies on traditional medicine in the Western PacificRegion. WHO; 2007.
11. Shen JA. Za bing Yuan Liu Xi Zhu. Beijing: People’s MedicalPublishing House; 2006.
12. Ding XC, Wang Z. Review of chronic obstructive pulmonarydisease in stable stage treated with TCM. J Zhejiang UnivTradit Chin Med 2008;32:131e2.
13. Guo R, Pittler MH, Ernst E. Herbal medicines for the treatmentof COPD: a systematic review. Eur Respir J 2006;28:330e8.
14. Cochrane review groups. Search methods guide: http://www.airways.cochrane.org; 2008.
15. Higgins JPT,Green S.Cochranehandbook for systematic reviewsof interventions (version 5.0.1), http://www.cochrane-handbook.org; 2008.
16. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality ofreports of randomized clinical trials: is blinding necessary?Control Clin Trials 1996;17:1e12.
17. Chen QH. Clinical observation of the therapeutic effect of yifeipill in treatment of chronic obstructive pulmonary disease.Fujian J Tradit Chin Med 2004;35:13e4.
18. Chen YF, Hu XY. Clinical study on effect of feikangning capsuleon patients with chronic obstructive pulmonary disease instable phase. J Mod Clin Med 2007;33:332e4.
19. Guo WX, Yu F, Zhang CY, et al. Clinical observation of the ther-apeutic efffect jian fei capsule on chronic obstructive pulmo-nary disease stationary phase. Hebei J Traditional Chin Med2008;30:121e3.
20. Hong ML, Yang GZ, Chen WX, et al. Effect of yufeining oninduced sputum interleukin-8 in patients with chronicobstructive pulmonary disease at the stable phase. Chin JIntegr Med 2005;11:179e82.
21. Huang DH, Wu L, He DP, et al. Clinical observation of stablechronic obstructive pulmonary disease treated by integrationof traditional Chinese medicine and Western medicine. JFourth Milit Med Univ 2005;26:1611e3.
22. Huang DW, Chen P, Li YZ, et al. The influence of herb toreinforce lung and consolidate origin on the ventilative func-tion of lung in the patients of chronic obstructive pulmonarydisease. Chin J Inf Traditional Chin Med 2002;9:17e8.
23. Li SY, Zhou QW, Wang MH, et al. Effect of bufei yishen granuleon pulmonary ventilation function and immunological functionof patients with chronic obstructive pulmonary disease inremission phase: a randomized grouping and placebocontrolled study. Chin J Clin Rehabil 2006;10:145e7.
24. Lin L, Tang CY, Xu YJ. Clinical observation of spleen-lungnourishing granule in treating respiratory muscle fatigue ofstable chronic obstructive pulmonary disease. Shanghai JTraditional Chin Med 2003;37:10e2.
25. Wu B. Clinical observation of jiawei shenge granule on effect oflung function for chronic obstructive pulmonary disease atremission stage. Med Industry Information 2006;3:70.
26. Xiong G, Chen S, Xie W, et al. Clinical observation of shengegranule on effect of lung function and serum IL-8, TNF-a forstable chronic obstructive pulmonary disease. Chin J GeriatrCare 2008;6:37e9.
27. Xu XY, Liu QR, Chen J. Clinical observation of Qi deficiencysyndrome in 72 patients with chronic obstructive pulmonarydisease treated with yiqi mianyi granule. Zhongguo Zhong Xi YiJie He Za Zhi 1996;16:81e3.
28. Gross D, Shenkman Z, Bleiberg B, et al. Ginseng improvespulmonary functions and exercise capacity in patients withCOPD. Monaldi Arch Chest Dis 2002;57:242e6.
29. Chinese Medical Association of Respiratory Diseases (chronicobstructive pulmonary disease study group). Chronic obstruc-tive pulmonary disease diagnosis and treatment guidelines.Chin J Tuberculosis Respir 2002;25:453e60.
30. ATS. Standardization of spirometrye1987 update. Statement ofthe American Thoracic Society. Am Rev Respir Dis 1987;136:1285e98.
31. Miller MR, Hankinson J, Brusasco V, et al. Standardisation ofspirometry. Eur Respir J 2005;26:319e38.
32. Zheng XY. Chinese medicine clinical research of new drugs onthe guiding principles (for trial implementation). Beijing,China: China Medical Science and Technology PublishingHouse; 2002.
33. Qi GD, We DA, Chung LP, et al. Placebos used in clinical trialsfor Chinese herbal medicine. Recent Pat Inflamm Allergy DrugDiscov 2008;2:123e7.
34. Juni P, Altman DG, Egger M. Systematic reviews in health care:assessing the quality of controlled clinical trials. BMJ 2001;323:42e6.
35. Fabbri LM, Calverley PM, Izquierdo-Alonso JL, et al. Roflumilastin moderate-to-severe chronic obstructive pulmonary diseasetreated with longacting bronchodilators: two randomisedclinical trials. Lancet 2009;374:695e703.
36. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium inchronic obstructive pulmonary disease. N Engl J Med 2008;359:1543e54.
37. Tonnel AB, Perez T, Grosbois JM, et al. Effect of tiotropium onhealth-related quality of life as a primary efficacy endpoint inCOPD. Int J Chron Obstruct Pulmon Dis 2008;3:301e10.

176 X. An et al.
38. Swanson SM, Jiang JX, Chang YS, et al. A rapid and sensitivebioassay involving cultured rat glioma cells to screen forsubstances capable of elevating intracellular cyclic AMPconcentration. J Nat Prod 1988;51:929e36.
39. Park MT, Cha HJ, Jeong JW, et al. Glucocorticoid receptor-induced down-regulation of MMP-9 by ginseng components,PD and PT contributes to inhibition of the invasive capacityof HT1080 human fibrosarcoma cells. Mol Cells 1999;9:476e83.
40. Jung SH, Woo MS, Kim SY, et al. Ginseng saponin metabolitesuppresses phorbol ester-induced matrix metalloproteinase-9expression through inhibition of activator protein-1 and
mitogen-activated protein kinase signaling pathways in humanastroglioma cells. Int J Cancer 2006;118:490e7.
41. Lee BM, Lee SK, Kim HS. Inhibition of oxidative DNA damage, 8-OHdG, and carbonyl contents in smokers treated with antiox-idants (vitamin E, vitamin C, beta-carotene and red ginseng).Cancer Lett 1998;132:219e27.
42. Cho JY, Yoo ES, Baik KU, et al. In vitro inhibitory effect ofprotopanaxadiol ginsenosides on tumor necrosis factor (TNF)-alpha production and its modulation by known TNF-alphaantagonists. Planta Med 2001;67:213e8.
43. Coon JT, Ernst E. Panax ginseng: a systematic review of adverseeffects and drug interactions. Drug Saf 2002;25:323e44.