Optimizing Transitions: Addictions and Mental Health 2015.
52
Optimizing Transitions: Addictions and Mental Health 2015
Transcript of Optimizing Transitions: Addictions and Mental Health 2015.

Optimizing Transitions: Addictions and Mental Health 2015

Presentation Objectives
1. To review emerging practices for developmentally appropriate care for TAY
2. To describe the components of a successful program for TAY
3. To describe key elements in optimizing transitions for TAY from hospital to community services
4. To describe an evaluation framework used by the LOFT, Sickkids, and CAMH partnership
5. To share preliminary results

Some facts about TAY with MH and Substance Use Problems
Youth experience more disconnection and are therefore less likely to receive appropriate support services in the transition to adulthood (Brown and Wilderson, 2010)
For more than 70% of adults living with mental health problems, symptoms developed when they were young. “Identifying youth at risk and intervening as early as possible improves their life trajectories, their productivity as Canadians and reduces the prevalence of mental health problems in adulthood.” (Mental Health Commission of Canada, Youth Council, 2010)

Transitional Age Youth
Characteristic of the Population
Access and
Navigating Services
Delivery of Services
Service Offerings
System Issues
Challenges for Transitional Age Youth with MHA

Developmentally-informed Practice
Consider sex & gender, trauma, culture Without support, youth with serious
mental health and substance use concerns face significant challenges in achieving developmental milestones Younger youth - school success, social skill
development Older youth – vocational success,
developing intimate relationships With support and/or early achievement,
positive outcomes are more likely
5

Considerations in working with TAY
Need clinical services PLUS services that promote independent living AND coordinated care
Need services that address needs directly AND processes that reflect the needs of TAY
Need to consider youth goals re: adulthood
6

Services for older youth to promote independence
Employment Education Housing Community involvement (social/recreational
activities) and social support Money management Training on basic living skills (cooking,
shopping, etc.), problem-solving and informed decision-making’
What exists in your community?
7

Key attributes of service delivery Informal Flexible Individualized, youth involvement in goal
setting Involve supports Build on strengths Prepare youth for transition, across
services and sectors Support youth through transitions
8

Parallel with MI principles Youth input Active listening Non-judgmental Avoid lecturing Express empathy Offer assistance Encourage, offer descriptive praise,
express enthusiasm
9

Developmentally-specific services
Developmentally-specific services are targeted to meet the needs of youth considering their developmental stage (not, chronological age)
For example, developmentally-specific groups, services, residential programs, within child/adolescent and adult services
10

Transitions: Challenges/Issues/Barriers
Lack of experience/difficulties addressing parental issues
Youth/family reluctance Lack of institutional support Lack of planning Lack of developmentally-informed adult
services Lack of two-way communication Confidentiality & consent issues
Brodie, Goldman & Clapton (2011), Davidson, S. & Cappelli, M. (2011), Singh, S. et al. (2008)
11

Transitions: Challenges/Issues/Barriers
Time/Resources/high workload, staffing shortages, long wait lists
Training Differing perspectives (youth, family, providers) Attitudes/Discomfort/lack of confidence of providers Limited applicability of services Difficulty accessing resources Poor intra-agency & inter-agency coordination Individual vs. family approaches Developmental vs. diagnostic approaches Lack of flexibility Protective vs. responsibility approach
Brodie, Goldman & Clapton (2011), Davidson, S. & Cappelli, M. (2011), Singh, S. et al. (2008)
12

Transitions: Challenges/Issues/Barriers
Limited specific research regarding how to prepare youth and family for transition – greater focus on policy & procedure, less focus on clinical practice
Inconsistent documentation/information systems/transfer systems
Organizational culture differences Lack of shared information about service
structures Different thresholds & eligibility criteria for service Lack of off-hours services
Brodie, Goldman & Clapton (2011), Davidson, S. & Cappelli, M. (2011), Singh, S. et al. (2008)
13

Recommendations from the evidence
Youth and family perspectives should be considered in service planning generally & for their own care
Developmentally appropriate communication and information for youth
Accessible communication and information for families Worker support, co-located & multi-agency services Accessible & flexible services dedicated to youth (i.e.
community-based, friendly, informal, flexible venues, hours of service, types of service, & dealing with missed appointments)
Well-trained practitioners, advocacy, mentoring
Brodie, Goldman & Clapton (2011), Davidson, S. & Cappelli, M. (2011), Singh, S. et al. (2008)
14

Example: A model of care for TAY
Transition to Independence Process (TIP)

“Discovery rather than Recovery”
16

TIP Overview
TIP is a promising practice for: Transitional aged youth with
emotional/behavioural difficulties Appropriate for youth 14-29 years old Applicable across multiple services and
sectors in community-based settings Model operationalized through seven
guidelines & core practices
17
Clark et al. (1995)

TIP Transition Domains18

Key Facts about TIP
Cross sectoral applicability Rooted in evidence based approaches
such as Motivational Interviewing and Cognitive Behavioural Therapy
Can integrate into existing worko TIP used intentionally and purposefully
Role of supervisor important to maintain fidelity
19

Example: A model for transitions of care for TAY
TRACK

TRACK Criteria for Optimal Transition
Continuity of care – engaged with AMHS for 3 months or appropriately discharged (long-term continuity)
Period of parallel care – period of time when involved with both CAMHS & AMHS (relational continuity)
At least one transition planning meeting – meeting to discuss transition; involve youth, family, and key SPs, before transfer (cross-boundary/team continuity)
Optimal information transfer – referral letter, summary of services, current assessment (informational continuity)
21

TRACK: Improving the Transition
Alignment Attitudinal adjustment to promote view of services as
complementary Map all services available to youth/TAY Interagency development of care pathways
Preparation of service users before transition Information/what to expect Differences re: services/confidentiality/parental
involvement
22

TRACK: Improving the Transition
Transition process Flexibility “Age windows” Planned and occur at times of relative stability
Crisis is a contra-indication Improving info transfer
Specific protocol for information transfer Detailed info should go with youth
23

TRACK: Improving the Transition
Improve liaison between the Child and Adolescent Mental Health System (CAMHS) and the Adult Mental Health System (AMHS) Improved knowledge, communication & understanding
between CAMHS & AMHS Joint training, continuous professional development re:
transition Changes to service structures & functioning Supervision, clinical accountability Designated transition workers
24

What Youth Like! (YSSR, 2010-2014)
Positive relationships with service providers
IncentivesFlexibilitySupport for autonomyAddressing reasons for usingNon-judgmental treatment
(YSSR, 2010-2014)
25

Essentials to building bridges with hospital (Heather’s perspective)
1. Align community practices to best practice/research
2. learn language and roles 3. know common client and need 4. build trust 5. formal MOU 6. lead a summit 7. learn together!

Complimentary services
Barrier free admission: GAIN Short Screener to screen for possible diagnosis
On the ground service coordination works: Taking youth to appointments, connecting them to primary care, crisis plans, finding and maintaining housing, etc.
Peer power: peer support workers, drop-in, groups, and opportunities for social connection
Crisis support– that is how young people re-engage with supports if they disengaged
Staff send on average 2500 texts/month Supportive housing

Being nervous is a normal part of the process. You are very passionate about your career, I think
that will show during your interview.
I’m just so nervous for the interview. I really want to get into this program.
Simple. The same way you just told me.
But how do I tell them that I really want this opportunity and I will wake up at 5am every morning if
I have to?
TAY TXT

Community and Peers
Peer support is a vital part of the program (paid vs unpaid)
Exploring new ways to have fun and learn: ex. Art therapy, visiting new places
Pathways to Recovery groups

Components of LOFT’s TAY MH and Addiction program
Weekly psychiatrist
Trained peer
mentors
Specialized Addiction program
Supportive Housing- low,
med , high support
Focus on tight referral
pathways
Care coordinatio
n pilot through
Health Links
Monthly psychologi
st staff consult
Focus on engagementPriority referral source is
hospitalOn the ground support
Evaluation framework (CAMH): GAIN SS
Formal partnerships with 3 hospitals
Research: Sean Kidd
Crisis phone/text
24/7
Staffing Mon-Fri
9am-9pmSat: 1-9pm
Groups and
recreational
activities
MCYS , TCLHIN
and donor funded

ACT Community Treatment project
Funded in 2013 For Transitional age youth (age 16-25)
with addictions (from harm reduction perspective)
Partners: CAMH, HSC and LOFT Focus on optimizing transitions from
hospital Team launch included people across
partners Education provided across sectors Offered in sites across Toronto

Optimizing transitions
Primary referral source is hospital (2 formal MOUs- Hospital for Sick Children and CAMH)
Robust evaluation framework Service gaps come at critical time when first onset of
mental health issues may occur; we use standard tools to start mental health care coordination
Partnership with Urgent Care clinic (CAMH) and psychiatry

Appreciative Inquiry: An exercise
Think of a time that you had the most amazing experience of either making a referral, receiving a referral or being referred.
Please talk about that experience in detail using the worksheets.
You will be asked to report back to the group what your partner said

What works in building bridges? Appreciative inquiry exercise: Make it
fun! Client or patient– who cares? Get it done. Pulled out principles of how we will work
together Contact list and intake flow chart in a
drop box ACT training together Regular team meetings to touch base
and open door to feedback



Our team!


Objectives to be evaluated
Improved access to evidence-based community addictions treatment for youth
Improved transitions from hospital to community, and from youth into adult care systems
Improved outcomes for youth with addictions issues

Components of our Evaluation Framework
Contemplation ladder (every meeting) GAIN Short Screener every 12 weeks Self-efficacy tool (every 12 weeks) Determinants of Health Outcomes (intake, 1
month, 3 month, 6 month, exit/discharge). Focus group annually Client satisfaction questionnaire annually Binder kept at program to keep anecdotal
feedback/comments

41
GAIN-SS
brief screening tool for clients age 10+ identifies difficulties in 4 dimensions:
internalizing disorders (e.g. depression, anxiety) externalizing disorders (e.g. ADHD) substance use problems crime and violence
CAMH-version of GAIN-SS includes 7 additional items to screen for: eating-related issues trauma-related distress disordered thinking gambling, gaming and internet misuse
*GAIN-SS was developed by Chestnut Health Systems, Copyright © 2005

Evaluation results Nov 2014
Total # of surveys collected to date = 231Domains assessed:
Mental health (GAIN-SS Revised) Internalizing Disorders Externalizing Disorders Substance Use Crime/Violence Screener Additional questions assessing disordered eating, traumatic distress,
disordered thinking, gambling, gaming, internet misuse
Social determinants of health (Transitional Age Youth Program Measure)
Motivation (Contemplation Ladder) Self-Efficacy (General Self-Efficacy Scale) Service User Feedback
43

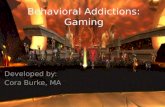
Transitional Age Youth Program Measures
64.7% male; mean age = 21.7 Scale 1 = Excellent, 2=Good, 3=Fair, 4 =Poor
higher scores = more difficulty in that domain
0
1
2
3
4
Means at Program Intake
PO
OR
ER
STA
TU
S
44

GAIN Short-Screener: Summary
Percentage of youth endorsing severe problems in each domain (score of 3+)
Internalizing Disorders = 87.9% Externalizing Disorders = 75.7% Substance Use = 44.6% Crime/Violence = 15%
45

Motivation – Contemplation Ladder
Pre-contemplation = 1 – 3Contemplation = 4 – 6Preparation = 7,8Action and Maintenance = 9,10
46

Motivation – Contemplation Ladder
LOFT mean Ladder score = 8.5 Typical items youth selected
“I have made a plan to change my substance use, and have begun to make some of those changes”
“I have changed my substance use, but still worry about slipping back. I need to keep working on the changes I’ve made”
LOFT Importance score: “How important is it for you to change your
substance use?” Scale 1 (not at all important) – 4 (very important) Importance mean = 2.7
47

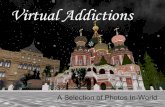
Self-Efficacy
General Self-Efficacy N=43 Scale: 1 (not true at all) – 4 (exactly true)
Total scale: 10 (very low SE) to 40 (very high SE)
LOFT Youth mean = 28.1 “I can solve most problems if I invest the
necessary effort” 90% selected true or somewhat true)
“I can remain calm when facing difficulties because I can rely on my coping abilities”
57% selected true or somewhat true
48
True/Somewhat
True
Not true/hardly true
0
20
40
60
True/Somewhat
True
Not true/hardly true
0
20
40
60
80
100

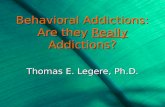
Service User Feedback
4-point scale 1 (Strongly Disagree) to 4 (Strongly Agree)
Total LOFT mean = 37.7, N= 24
49
Satisfied with support from staff
Services relevant to needs
Have right to approve services
Know where to go if services not good
Staff interested in my improvement
Happy with living situation
Recommend program to others
My opinions/ideas count
Can influence MH/Social service system
Could work if given opportunity
Program offered opportunities to get involved
0 10 20 30 40 50 60 70 80 90 100
AgreeDisagree

Summary - Risk
LOFT youth Present with many social, health (mental and
physical), employment, and housing challenges (i.e., social determinants of health)
High internalizing problems (e.g., depression) and externalizing problems (e.g., difficulty paying attention)
Distressing memories/dreams about past Eating disturbances Substance use issues
50

Summary - Resilience
HOWEVER, LOFT youth are also: Highly motivated to change problematic
substance use and maintain those changes Have a sense of self-efficacy to handle
challenges/stressors in their lives And, importantly, LOFT youth report
moderate to high satisfaction in most domains
51

Thank-you for your time
Gloria Chaim, MSW, RSWAssociate Director, Child Youth and Family Services Centre for Addiction and Mental [email protected]
Heather McDonald, MSWDirector of Adult and Youth ServicesLOFT Community [email protected]