
Optimizing Outcomes for Patients With...
69
Copyright © 2011 Neuroscience Education Institute. All rights reserved. Optimizing Outcomes for Patients With Anxiety (page 303 in syllabus) William M. Sauvé, MD Clinical Director of Military Programs Poplar Springs Hospital Sponsored by the Neuroscience Education Institute Additionally sponsored by the American Society for the Advancement of Pharmacotherapy This activity is supported solely by the sponsor, Neuroscience Education Institute.
Transcript of Optimizing Outcomes for Patients With...

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Optimizing Outcomes for
Patients With Anxiety
(page 303 in syllabus)
William M. Sauvé, MD
Clinical Director of Military Programs
Poplar Springs Hospital
Sponsored by the Neuroscience Education Institute
Additionally sponsored by the American Society for the Advancement of Pharmacotherapy
This activity is supported solely by the sponsor, Neuroscience Education Institute.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Faculty Editor / Presenter
William M. Sauvé, MD, is the clinical director of military programs at Poplar
Springs Hospital in Petersburg, VA.
Speakers Bureau: Pfizer
Individual Disclosure Statement

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Learning Objectives
• Explain the neurobiology of both normal and
pathological stress and anxiety
• Identify the environmental and genetic factors that
can contribute to the development of an anxiety
disorder
• Identify new treatment options in development for
PTSD
• Customize treatment regimens for patients with
PTSD based on symptom profile, comorbidities, and
life situations
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Pretest Question 1
38y/o male with PTSD, alcohol dependence, and chronic back
and knee pain presents on these medications: quetiapine
(Seroquel) 50mg qHS, prazosin 3mg qHS, duloxetine (Cymbalta)
90mg daily, gabapentin 300mg TID, clonidine 0.1mg TID,
zolpidem (Ambien) 10mg qHS and clonazepam (Klonopin) 1mg
up to TID as needed. His complaints include ongoing
nightmares, exaggerated startle, depressed mood, difficulty
staying asleep and poor memory. What might you do FIRST to
optimize this patient's medication regimen?
1. Increase quetiapine dose
2. Increase prazosin dose
3. Change the clonazepam to from PRN to BID
4. Discontinue the hypnotics (zolpidem) and the benzodiazepines
(clonazepam)
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
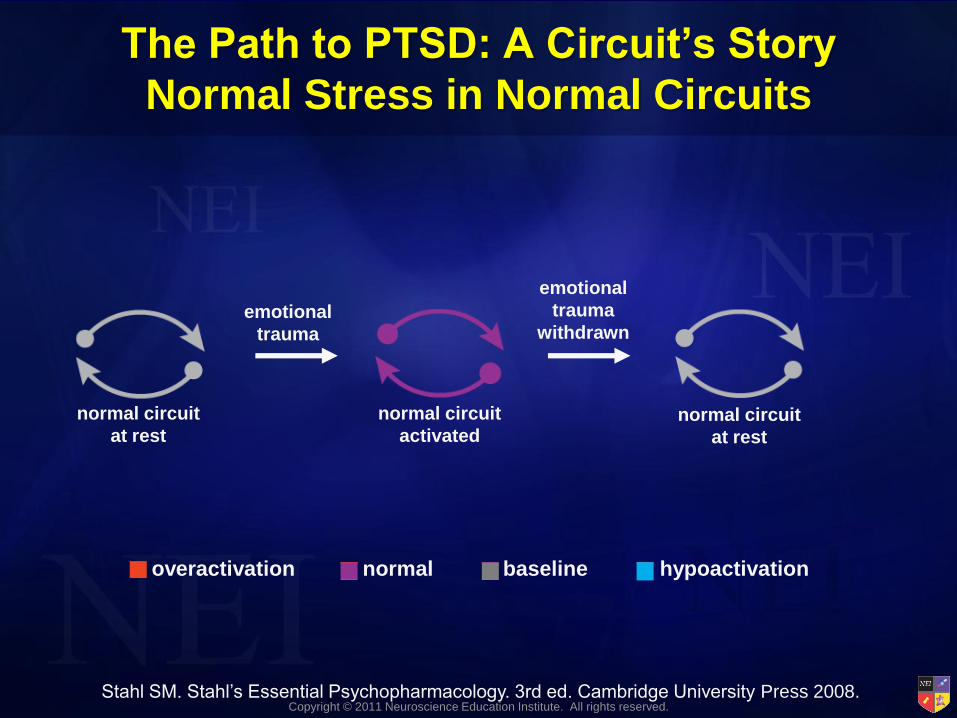
The Path to PTSD: A Circuit’s Story
Normal Stress in Normal Circuits
normal circuit
at rest
normal circuit
activated normal circuit
at rest
emotional
trauma
emotional
trauma
withdrawn
overactivation normal baseline hypoactivation
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
The Path to PTSD: A Circuit’s Story
Stress Sensitization in Normal Circuits
normal circuit
at rest
normal circuit
activated irreversible
stress
sensitization
emotional
trauma
emotional
trauma
withdrawn
normal circuit
continuously
activated
sustained,
repeated
emotional
trauma
overactivation normal baseline hypoactivation
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
The Path to PTSD: A Circuit’s Story
Progression From Stress Sensitization
vulnerable but
presymptomatic
prodromal
symptoms
subsyndromal
symptoms
psychiatric
symptoms
lack of
compensation
emotional
trauma
emotional
trauma
withdrawn
decompensation with
either overactivation
or breakdown
emotional
trauma
continues
irreversible
stress
sensitization
decompensation
is sustained
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
THE STRESS DIATHESIS
MODEL
Trauma is necessary but not sufficient for the
precipitation of anxiety disorders such as PTSD
Only 5-30% of trauma victims develop PTSD
Mahan, Ressler. TINS 2011;Epub ahead of print.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Stress Diathesis Model:
A Tale of Two Influences, Part 1
normal genes
life events
bad
childhood divorce
virus or
toxin
overactivation
normal
baseline
hypoactivation
normal
circuit
normal
activation
normal phenotype
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Stress Diathesis Model:
A Tale of Two Influences, Part 2 risk gene
single life event stressor
divorce
“biased”
circuit
normal phenotype
overactivation
inefficient information
processing
overactivation
normal
baseline
hypoactivation
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Stress Diathesis Model:
A Tale of Two Influences, Part 3
risk gene
risk gene
risk gene
risk gene
multiple life events
bad childhood divorce
virus or toxin
psychiatric symptoms
“biased”
circuit
diathesis stress
hypoactivation
with
malfunction
unsuccessful compensation
overactivation
normal
baseline
hypoactivation
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
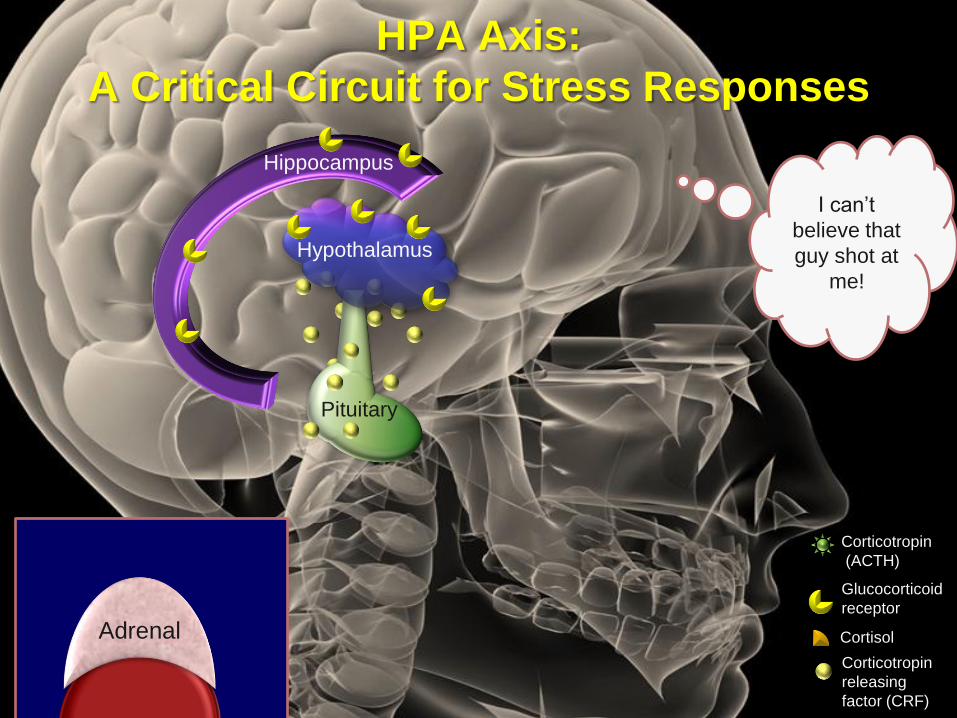
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses
I can’t
believe that
guy shot at
me!
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses
I can’t
believe that
guy shot at
me!

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses
I can’t
believe that
guy shot at
me!

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses
I can’t
believe that
guy shot at
me!

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses
I can’t
believe that
guy shot at
me!

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses
I can’t
believe that
guy shot at
me!

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
A Critical Circuit for Stress Responses

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
Chronic Stress
I am so tired from
working 60 hours
per week, taking
care of my small
children and my
elderly parents, and
not being able to
pay the bills.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
Chronic Stress
I am so tired from
working 60 hours
per week, taking
care of my small
children and my
elderly parents, and
not being able to
pay the bills.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
HPA Axis:
Chronic Stress
I am so tired from
working 60 hours
per week, taking
care of my small
children and my
elderly parents, and
not being able to
pay the bills.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Reduced Hippocampal Volume and Stress:
Cause or Effect?
coronal plane coronal plane
normal stress/PTSD
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008;
Woon, Hedges. Hippocampus 2008;18:729-36.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Most Common Mental Illnesses Associated
With Trauma
Depressed mood
Loss of interest/pleasure
Appetite/weight changes
Suicidality
Guilt/worthlessness
Anxiety
Worry
Irritability
Muscle tension
Phobic avoidance
Compulsions
Panic attacks Sleep
Concentration
Fatigue
Psychomotor
MDD

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Who Is At Risk?
Trauma type
Small hippocampus
Genetic
polymorphisms
??? MODERATE STRONG
Life stress
Lack of social support
Other previous trauma
Other adverse childhood
experience
Trauma severity
Psychiatric history
Childhood abuse
Family psychiatric
history
Wittchen et al. CNS Spectr 2009;14(Suppl 1):5-12.
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
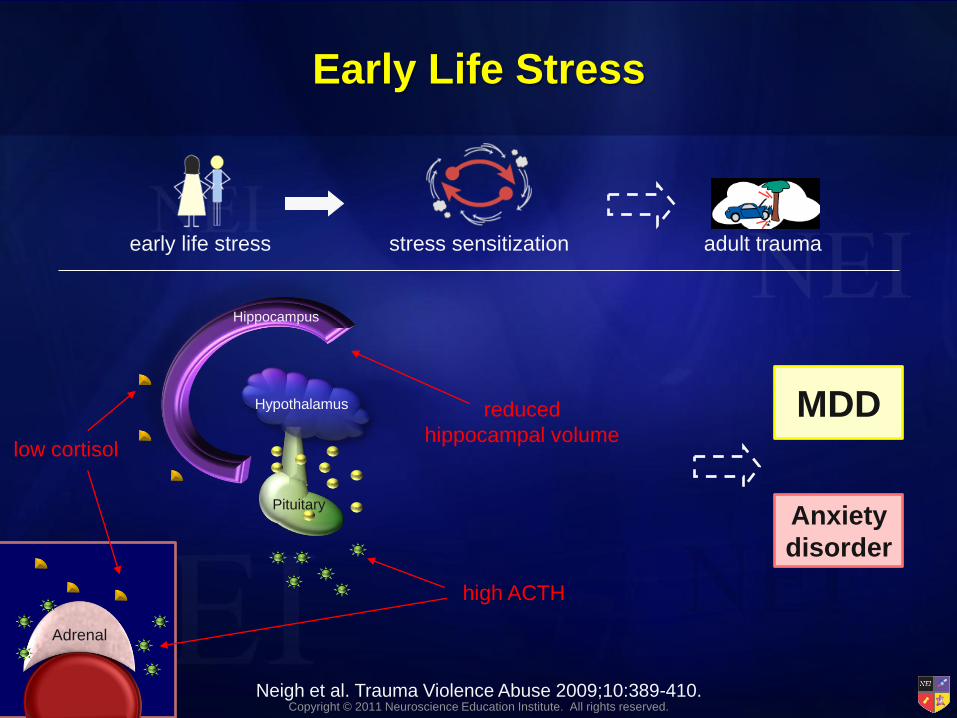
Hippocampus
Early Life Stress
early life stress adult trauma
low cortisol
high ACTH
reduced
hippocampal volume
Neigh et al. Trauma Violence Abuse 2009;10:389-410.
stress sensitization
MDD
Anxiety
disorder
Adrenal
Pituitary
Hypothalamus

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Early Life Stress: Is It All Bad?
amygdala
multiple
adult life
stressors
mild stress
in infancy
reduced reactivity
to stress
child abuse
stress sensitization
but no symptoms of
anxiety or depression
no stress
in infancy
normal stress
activation
no psychiatric disorder
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.
MDD Anxiety
disorder

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Genetic Risk Factors Under Investigation
DA transporter gene
(SLC6A3 9 allele)
An excess of 9 tandem
repeats found in patients
who developed PTSD
5-HT transporter gene
(“s” allele)
Increased risk of PTSD in
high-risk environments
Glucocorticoid receptor
co-chaperone FKBP5 gene
Interaction with childhood abuse
May contribute to increased
sensitivity of the amygdala and
HPA axis
BDNF gene (Val66Met)
Met/Met carriers have
greater recruitment of
amygdala and PFC during
memory formation and
retrieval
Heim, Nemeroff. CNS Spectr 2009;14(Suppl 1):13-24; Mahan, Ressler. TINS 2011;Epub ahead of print;
Binder et al. JAMA 2008;299(11):1291-1305; Shalev et al. Psychoneuroendocrinol 2009;34(3):382-8.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Risks in the Military: More Than Just Combat
Seal et al. Am J Public Health 2009;99:1651-8;
Friedman. Am J Psychiatry 2006;163:586-93;
Stein, McAllister. Am J Psychiatry 2009;166:768-76.
easy weapon access
sepa ration
sepa ration
destruction
readjustment
combat
sepa ration
unpredictable threats
lack of public support
WAR

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
PTSD and the HPA Axis
Hippocampus
low cortisol
Adrenal
Pituitary
Hypothalamus
downregulated
CRF receptors
increased sensitivity
to negative cortisol
feedback
increased
CRF
reduced
hippocampal volume

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Neuroimaging Findings in PTSD
Brain Region Functional Structural Potential Implications
Amygdala ↑ Exaggerated fear
response
Deficits in extinction,
emotion regulation,
attention, contextual
processing
rACC ↓ ↓ volume
dACC ↑ Exaggerated fear
learning
Hippocampus ↑↓ ↓ volume Deficits in contextual
processing
Intrusive memories
Insular cortex ↑↓ ↓ volume Increased anxiety
proneness
Shin, Liberzon. Neuropsychopharmacol 2009;Epub;
Lanius et al. J Psychiatr Res 2006;40:709-29.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Brain Atrophy in PTSD is Ongoing
Cardenas VA et al. Psychiatry Res: Neuroimaging 2011;193:93-100.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
PTSD
non-pharmacy
adjunctive
1st-line
2nd-line
PTSD “Non-Pharmacy”
exposure
therapy
cognitive
restructuring
stress
inoculation
acceptance and
commitment
therapy
dialectical
behavior therapy
seeking safety
therapy motivational
interviewing
eye movement
desensitization
and reprocessing
Zayfert C et al. J Trauma Stress 2005;18(6):637-45;
Bisson J, Andrew M. Cochrane Database Syst Rev 2007;(3):CD003388.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Virtual Exposure Therapy
Rizzo et al. Ann NY Acad Sci 2010;1208:114-25.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
PTSD
pharmacy
adjunctive
mirtazapine
hypnotic SDA/
DPA beta blocker (preemptive) lamotrigine
topiramate acamprosate
naltrexone
1
antagonist
1st-line
SNRI SSRI
2nd-line
BZ gabapentin/ pregabalin
MAOI TCA
PTSD “Pharmacy”
Only sertraline and paroxetine are FDA-approved to treat PTSD.
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
5-HT Signaling Increases BDNF Release,
Which Modifies 5-HT Innervation
5-HT
PKA CaMK
CREB
BDNF
synaptogenesis
neuroplasticity
neurogenesis
cell survival
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Sertraline
• SSRI
• FDA-approved for the treatment
of PTSD
• Most common side effects are
sexual dysfunction,
gastrointestinal issues, and CNS
problems
• Weight gain and sedation
unusual
• Initial dosing at 25 mg/day
increased to 50 mg/day after
1 week; maximum dose
200 mg/day single dose
• 169 outpatient veterans in randomized, double-blind comparison of sertraline vs placebo
– 12 wks flexible dose (25-200 mg/day)
– Scales: CAPS, Impact of Events, Clinical Global Impressions (CGI-I)
• No significant difference noted between sertraline and placebo
• 37 patients in randomized, double-blind comparison of sertraline vs nefazodone
– 12 wks flexible dose (avg. 153 mg/day sertraline)
– Scales: CAPS, CGI-I
• Both treatment groups showed improvement; no difference between groups in efficacy
Stahl. Prescriber’s Guide 2008; Friedman et al. J Clin Psychiatry 2007;68:711-20;
McRae et al. Depr Anx 2004;19:190-6.
DRI
SRI

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Paroxetine for Non-Combat-Related PTSD
• SSRI
• FDA-approved for PTSD treatment
• Aids in treatment of re-experiencing, avoidance, and hyperarousal
• Effective antidepressant and anxiolytic
0
10
20
30
40
0 4 8 12
Weeks of Treatment
David
so
n P
TS
D S
cale
avoidance
hyperarousal
intrusive symptoms
*
*
*
*
* †
†
† † †
† †
n = 10
* Denotes significance between 4-week intervals at p < .05
† Denotes significance between weeks 0 and 8 at p <.001
† † Denotes significance between weeks 4 and 12 at p < .001
Adapted from Marshall et al. J Clin Psychiatry 1998;18(1):10-1.
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Other Medications
• Other SSRIs/SNRIs: rationale and some
published data in support of efficacy
• Benzodiazepines: negative studies
• MAOIs: mixed data
• Atypical antipsychotics: mixed data
– Possibly beneficial as adjuncts for psychotic
symptoms, sleep
Ipser, Seedat. Cochrane Database Syst Rev 2006;(1):CD002795.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Pretest Question 2
38y/o male with PTSD, alcohol dependence, and
chronic back and knee pain presents on these
medications: quetiapine 50mg qHS, prazosin 3mg
qHS, duloxetine 90mg daily, gabapentin 300mg TID,
clonidine 0.1mg TID, zolpidem 10mg qHS. He has also
recently started on clonazepam 1mg BID. His
complaints include ongoing nightmares, depressed
mood, difficulty staying asleep and poor memory.
What might you do now to optimize this patient's
medication regimen?
1. Increase quetiapine dose
2. Decrease quetiapine dose
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
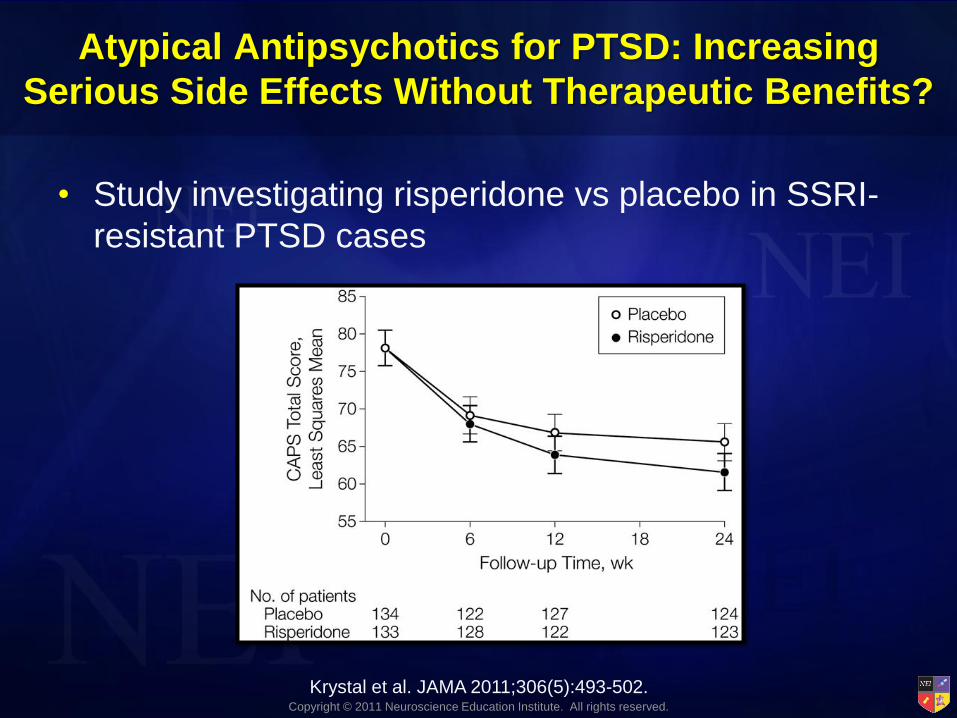
Atypical Antipsychotics for PTSD: Increasing
Serious Side Effects Without Therapeutic Benefits?
• Study investigating risperidone vs placebo in SSRI-
resistant PTSD cases
Krystal et al. JAMA 2011;306(5):493-502.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Noradrenergic Hyperactivity in Anxiety
anxiety / panic attacks
tremor
sweating
tachycardia
hyperarousal
nightmares
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Alpha-1 Adrenergic Blockers to Treat Anxiety and Nightmares
anxiety / panic attacks
tremor
sweating
tachycardia
hyperarousal
nightmares
1 receptor
1 blocker
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Pretest Question 3
38y/o male with PTSD, alcohol dependence, and chronic
back and knee pain presents on these medications:
quetiapine 50mg qHS, prazosin 3mg qHS, duloxetine 90mg
daily, gabapentin 300mg TID, clonidine 0.1mg TID,
zolpidem 10mg qHS. He has also recently started on
clonazepam 1mg BID and his quetiapine dose was
increased to 300 mg/day. His is still complaining of ongoing
nightmares, but his depression has improved. He also still
has difficulty staying asleep, chronic knee and back pain,
and poor memory. What might you do now to optimize this
patient's medication regimen?
1. Increase prazosin dose
2. Increase neurontin dose
3. Both of the above

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Prazosin (Minipress)
• Alpha-1 adrenergic blocker
• Antihypertensive drug
• Used to prevent nightmares in patients with PTSD; normalizes slow-wave sleep
• Not extensively studied in PTSD
• Dose not established; studied at 1–20 mg/day at bedtime or in divided doses
• Side effects include orthostatic hypotension, insomnia/fatigue, depression, nervousness, dizziness, syncope, headache, gastrointestinal effects
• Side effects generally decrease with time
• Notable interactions: diuretics, other antihypertensive drugs
Raskind et al. J Clin Psychiatry 2002;63(7):565-8.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Prazosin vs. Quetiapine
Byers MG et al. J Clin Psychopharmacol 2010;30:225-9.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Beta Adrenergic Blockers to Treat Anxiety
anxiety / panic attacks
tremor
sweating
tachycardia
hyperarousal
nightmares
ß1 receptor
beta blocker
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
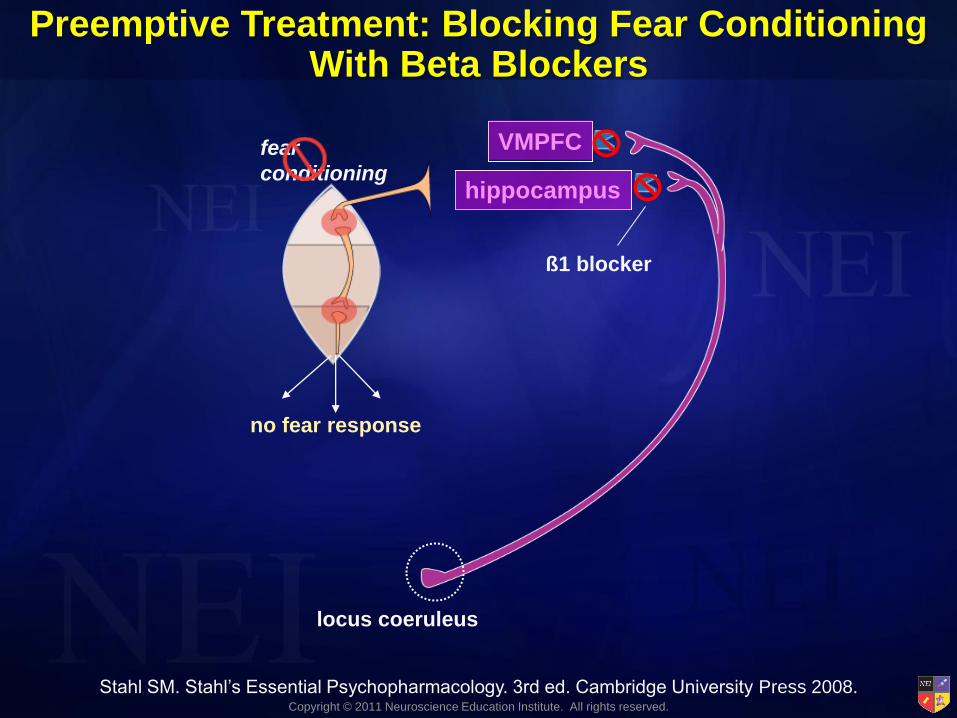
Preemptive Treatment: Blocking Fear Conditioning With Beta Blockers
VMPFC
hippocampus
locus coeruleus
fear
conditioning
fear response!!!
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008; Orr et al. Biol
Psychiatry 2006;73:262-71; Pitman et al. Biol Psychiatry 2002;51:189-92;
Vaiva et al. Biol Psychiatry 2003;54:947-9.
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
VMPFC
hippocampus
locus coeruleus
fear
conditioning
ß1 blocker
no fear response
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.
Preemptive Treatment: Blocking Fear Conditioning With Beta Blockers

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Propranolol (Inderal)
• Beta blocker and antihypertensive drug
• Might block effects of stress from prior traumatic experiences
• Usual dose range: up to 240 mg/day; effective dose varies greatly
• Side effects include insomnia/fatigue, depression, vivid dreams, gastrointestinal effects
• Notable interactions: most atypical antipsychotics, alcohol, ibuprofen/NSAIDs, SSRIs, duloxetine
• A recent study showed that propanolol was ineffective for reducing PTSD-like onset in a rat model
Cohen H et al. Eur Neuropsychopharmacol 2011;21:230-40.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Pharmacotherapy Following Traumatic Injury
May Prevent Development of PTSD
• 696 injured U.S. military personnel
• Intravenous administration of morphine during
resuscitation and trauma care
Odds Ratio Adjusted for Injury Severity Score (95% CI): 0.48 (0.34–0.68) p<0.001
0
20
40
60
80
100
PTSD No PTSD
Morphine Use
60% 76%
Holbrook TL, Galarneau MR, Dye JL et al. N Engl J Med. 2010;362(2):110-7.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Prophylactic Use of Cortisol
• PTSD may develop as a result of subadequate
cortisol response
• High dose hydrocortisone treatment given in first few
hours immediately following trauma
Zohar et al. Eur Neuropsychopharmacol 2011;Epub ahead of print.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Cortisol Following Stress Increases BDNF in
Hippocampus
Zohar et al. Eur Neuropsychopharmacol 2011;Epub ahead of print.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Fear Conditioning vs Fear Extinction
VMPFC
hippocampus
sensory cortex
thalamus
VMPFC
hippocampus
lateral amygdala
central amygdala
intercalated cell mass
no fear response
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Fear Conditioning vs Fear Extinction VMPFC
hippocampus
sensory cortex
thalamus
VMPFC
hippocampus
no fear response
new learning
= glutamate
= GABA
fear response!!!
fear
conditioning
no fear response
fear
extinction
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Facilitating Fear Extinction: Enhancing Inhibitory
Learning With the NMDA Agonist D-Cycloserine
D-cycloserine
facilitates
learning
D-cycloserine
no fear response
Stahl SM. Stahl’s Essential Psychopharmacology. 3rd ed. Cambridge University Press 2008.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Adrenal
Hippocampus
Glucocorticoid
receptor
Cortisol
Corticotropin
releasing
factor (CRF)
Corticotropin
(ACTH)
Pituitary
Hypothalamus
vasopressin 1B
antagonist
glucocorticoid
antagonist
Potential Sites of Action
for Novel Treatments for PTSD
CRF-1
antagonist

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Common Comorbidities and Complications
Anxiety/Re-experiencing
Worry
Sleep
Irritability
Avoidance/Numbing
Concentration problems
Arousal
Traumatic
brain
injury
Suicidality Alcohol and
drug
dependence
Other
anxiety
disorders
Depression
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
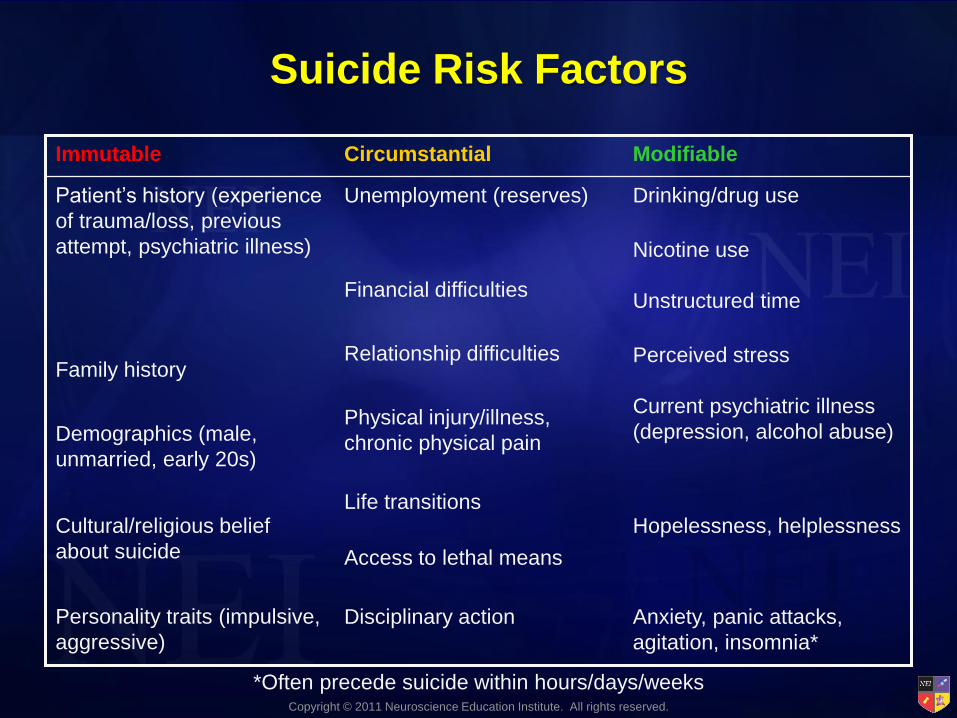
Suicide Risk Factors
Hopelessness, helplessness
Access to lethal means
Personality traits (impulsive,
aggressive)
Anxiety, panic attacks,
agitation, insomnia*
Current psychiatric illness
(depression, alcohol abuse)
Perceived stress
Unstructured time
Nicotine use
Drinking/drug use
Modifiable
Disciplinary action
Life transitions Cultural/religious belief
about suicide
Physical injury/illness,
chronic physical pain Demographics (male,
unmarried, early 20s)
Relationship difficulties Family history
Financial difficulties
Unemployment (reserves) Patient’s history (experience
of trauma/loss, previous
attempt, psychiatric illness)
Circumstantial Immutable
*Often precede suicide within hours/days/weeks

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Are Some Symptoms Precursors to
Suicidality?
• Anxiety
• Agitation
• Panic attacks
• Insomnia
• Irritability
• Hostility
• Aggressiveness
• Impulsivity
• Restlessness
• Hypomania and mania

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Suicide Risk Is Highest When:
• The person sees no way out and fears things may get worse
• The predominant emotions are hopelessness and helplessness
• The person is anxious, agitated, and has insomnia
• Thinking is constricted with a tendency to perceive his or her situation as all bad
• Judgment is impaired by use of alcohol or other substances
• There is a lack of future orientation
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Suicide Assessment
• Conduct a thorough assessment and reassessment of suicide risk
• Involve patient and family in treatment plan
• Choose appropriate treatment setting and means of monitoring patient based on risk assessment
• Document your thinking about suicide risk and your decision-making based on your assessment
• Remember: 3 out of 4 suicide victims had contact with their primary care provider within 90 days of their suicide
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
PTSD and Substance Abuse
• Trauma memories may elicit cravings
• Childhood trauma can increase the risk of PTSD in substance abuse patients, especially if multiple traumas have been witnessed as an adult
• Unresolved PTSD can result in a higher risk of substance abuse
• Childhood traumas are a better predictor of adulthood substance abuse cravings than adolescent traumatic events
Schumacher et al. Am J Addict 2006;15:422-5.
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
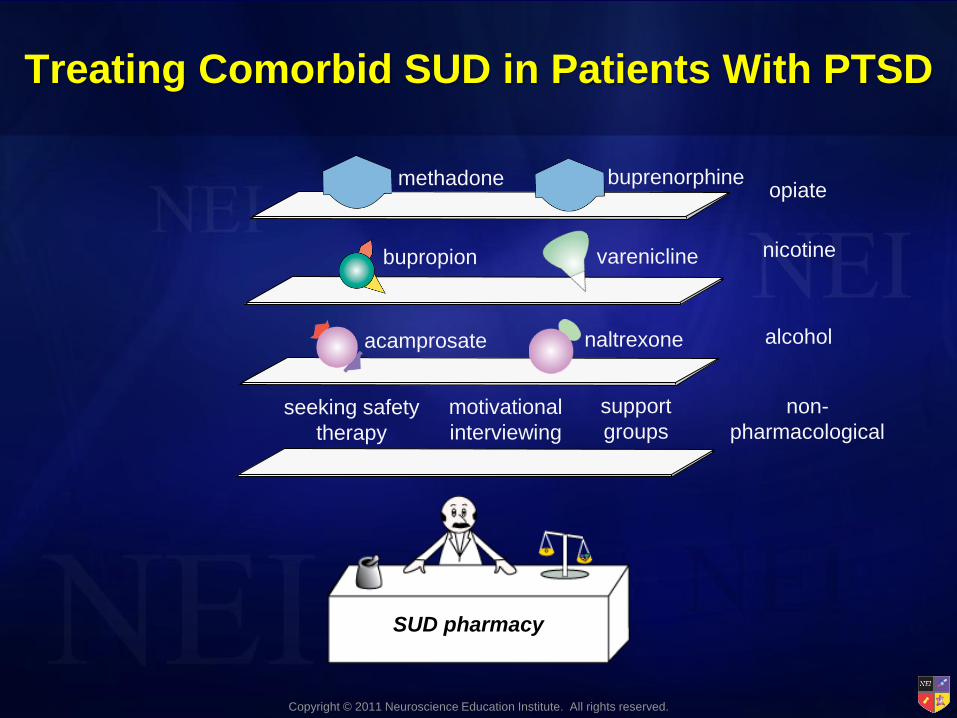
Treating Comorbid SUD in Patients With PTSD
acamprosate
varenicline
naltrexone
SUD pharmacy
bupropion
buprenorphine methadone
alcohol
nicotine
opiate
non-
pharmacological
seeking safety
therapy
motivational
interviewing
support
groups

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Gabapentin + Naltrexone
Anton RF et al. Am J Psychiatry 2011;168:709-17.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
PTSD, Chronic Pain, and Depression
• 80% rate of chronic pain in sample of Vietnam vets with PTSD
• PTSD more influential than depression and other disorders in leading to poor physical health
• Depression found to mediate the relationship between PTSD and pain
• Treatment for PTSD and pain should take potential depressive symptoms into account
Poundja et al. J Traum Stress 2006;19(5):747-51.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Persistent Postconcussive Syndrome (PPCS)
and PTSD: Symptom Overlap
Nightmares
Flashbacks
Guilt
Headaches
Sensitivity to
light/sound
Memory
deficit
Dizziness
Disinhibition
Emotional lability
Depression
Irritability/anger
Concentration/ attention problems
Fatigue
Hyperarousal
Avoidance
Apathy
PTSD PPCS
Stein, McAllister. Am J Psychiatry 2009;166:768-76.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Brain Regions Vulnerable to TBI:
Overlap With PTSD?
DLPFC
OFC
subcortical
white matter
hippocampus
TBI TBI and PTSD
Stein, McAllister. Am J Psychiatry 2009;166:768-76.

Copyright © 2011 Neuroscience Education Institute. All rights reserved.
PTSD
pharmacy
adjunctive
mirtazapine
hypnotic CBT
SDA/
DPA beta blocker (preemptive) lamotrigine
topiramate acamprosate
naltrexone
1
antagonist
1st-line
SNRI SSRI
2nd-line
BZ gabapentin/ pregabalin
MAOI TCA
PTSD and Comorbid TBI “Pharmacy”
Kennedy et al. JRRD 2007;44:895-920.
Copyright © 2011 Neuroscience Education Institute. All rights reserved.
Summary
• Many factors, both environmental and genetic, may contribute to whether one develops mental illness following trauma
• PTSD is a disorder with significant impact on functioning and quality of life
• Anxiety disorders, including PTSD, should be diagnosed and treated according to the best available evidence
• Maximizing treatment outcomes may require an integrated approach that encompasses both pharmacological and non-pharmacological interventions


















