
ANALYSIS OF EXPERIENCED PHARMACIST CLINICAL A DISSERTATION …
Optimizing Clinical Quality Performance with Pharmacist-Driven Programs
Presented By:Lee Klevens, Pharm.D. – [email protected] Ho, Pharm.D. – [email protected] Chuong, Pharm.D. – [email protected] Kim, Pharm.D. – [email protected] County Regional Medical Center (RCRMC)January 18, 2011
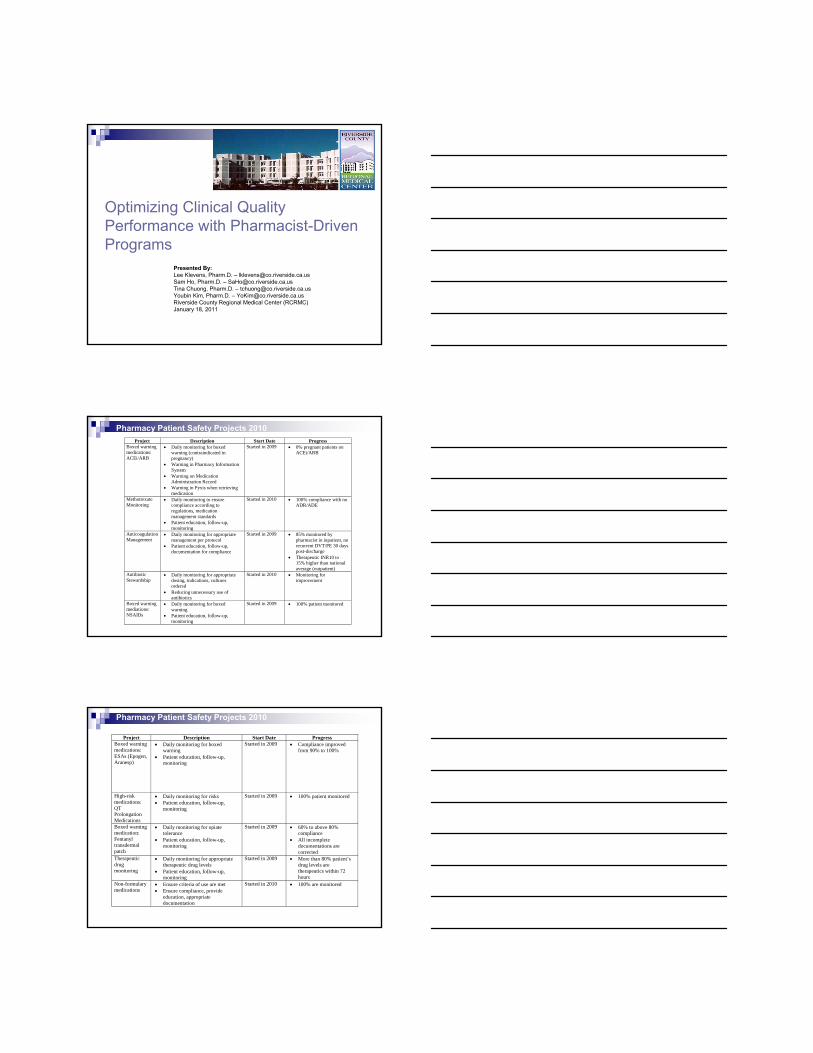
Pharmacy Patient Safety Projects 2010Project Description Start Date Progress
Boxed warning medications: ACEi/ARB
• Daily monitoring for boxed warning (contraindicated in pregnancy)
• Warning in Pharmacy Information System
• Warning on Medication Administration Record
• Warning in Pyxis when retrieving medication
Started in 2009 • 0% pregnant patients on ACEi/ARB
Methotrexate Monitoring
• Daily monitoring to ensure compliance according to regulations, medication management standards
• Patient education, follow-up, monitoring
Started in 2010 • 100% compliance with no ADR/ADE
Anticoagulation Management
• Daily monitoring for appropriate management per protocol
• Patient education, follow-up, documentation for compliance
Started in 2009 • 85% monitored by pharmacist in inpatient, no recurrent DVT/PE 30 days post-discharge
• Therapeutic INR10 to 15% higher than national average (outpatient)
Antibiotic Stewardship
• Daily monitoring for appropriate dosing, indications, cultures ordered
• Reducing unnecessary use of antibiotics
Started in 2010 • Monitoring for improvement
Boxed warning mediations: NSAIDs
• Daily monitoring for boxed warning
• Patient education, follow-up, monitoring
Started in 2009 • 100% patient monitored
Pharmacy Patient Safety Projects 2010
Project Description Start Date Progress Boxed warning medications: ESAs (Epogen, Aranesp)
• Daily monitoring for boxed warning
• Patient education, follow-up, monitoring
Started in 2009 • Compliance improved from 90% to 100%
High-risk medications: QT Prolongation Medications
• Daily monitoring for risks • Patient education, follow-up,
monitoring
Started in 2009 • 100% patient monitored
Boxed warning medication: Fentanyl transdermal patch
• Daily monitoring for opiate tolerance
• Patient education, follow-up, monitoring
Started in 2009 • 60% to above 80% compliance
• All incomplete documentations are corrected
Therapeutic drug monitoring
• Daily monitoring for appropriate therapeutic drug levels
• Patient education, follow-up, monitoring
Started in 2009 • More than 80% patient’s drug levels are therapeutics within 72 hours
Non-formulary medications
• Ensure criteria of use are met • Ensure compliance, provide
education, appropriate documentation
Started in 2010 • 100% are monitored
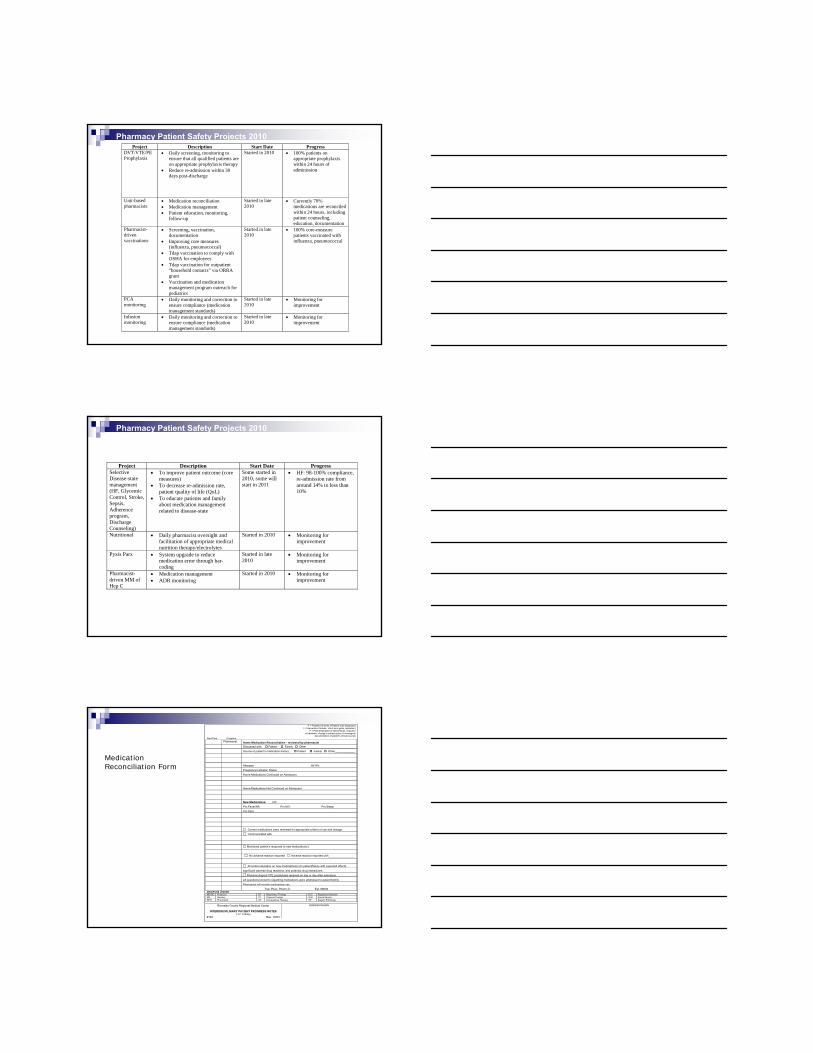
Pharmacy Patient Safety Projects 2010Project Description Start Date Progress
DVT/VTE/PE Prophylaxis
• Daily screening, monitoring to ensure that all qualified patients are on appropriate prophylaxis therapy
• Reduce re-admission within 30 days post-discharge
Started in 2010 • 100% patients on appropriate prophylaxis within 24 hours of adminission
Unit-based pharmacists
• Medication reconciliation • Medication management • Patient education, monitoring,
follow-up
Started in late 2010
• Currently 70% medications are reconciled within 24 hours, including patient counseling, education, documentation
Pharmacist-driven vaccinations
• Screening, vaccination, documentation
• Improving core measures (influenza, pneumococcal)
• Tdap vaccination to comply with OSHA for employees
• Tdap vaccination for outpatient “household contacts” via ORRA grant
• Vaccination and medication management program outreach for pediatrics
Started in late 2010
• 100% core-measure patients vaccinated with influenza, pneumococcal
PCA monitoring
• Daily monitoring and correction to ensure compliance (medication management standards)
Started in late 2010
• Monitoring for improvement
Infusion monitoring
• Daily monitoring and correction to ensure compliance (medication management standards)
Started in late 2010
• Monitoring for improvement
Pharmacy Patient Safety Projects 2010
Project Description Start Date Progress Selective Disease-state management (HF, Glycemic Control, Stroke, Sepsis, Adherence program, Discharge Counseling)
• To improve patient outcome (core measures)
• To decrease re-admission rate, patient quality of life (QoL)
• To educate patients and family about medication management related to disease-state
Some started in 2010, some will start in 2011
• HF: 98-100% compliance, re-admission rate from around 14% to less than 10%
Nutritional • Daily pharmacist oversight and facilitation of appropriate medical nutrition therapy/electrolytes
Started in 2010 • Monitoring for improvement
Pyxis Parx • System upgrade to reduce medication error through bar-coding
Started in late 2010
• Monitoring for improvement
Pharmacist-driven MM of Hep C
• Medication management • ADR monitoring
Started in 2010 • Monitoring for improvement
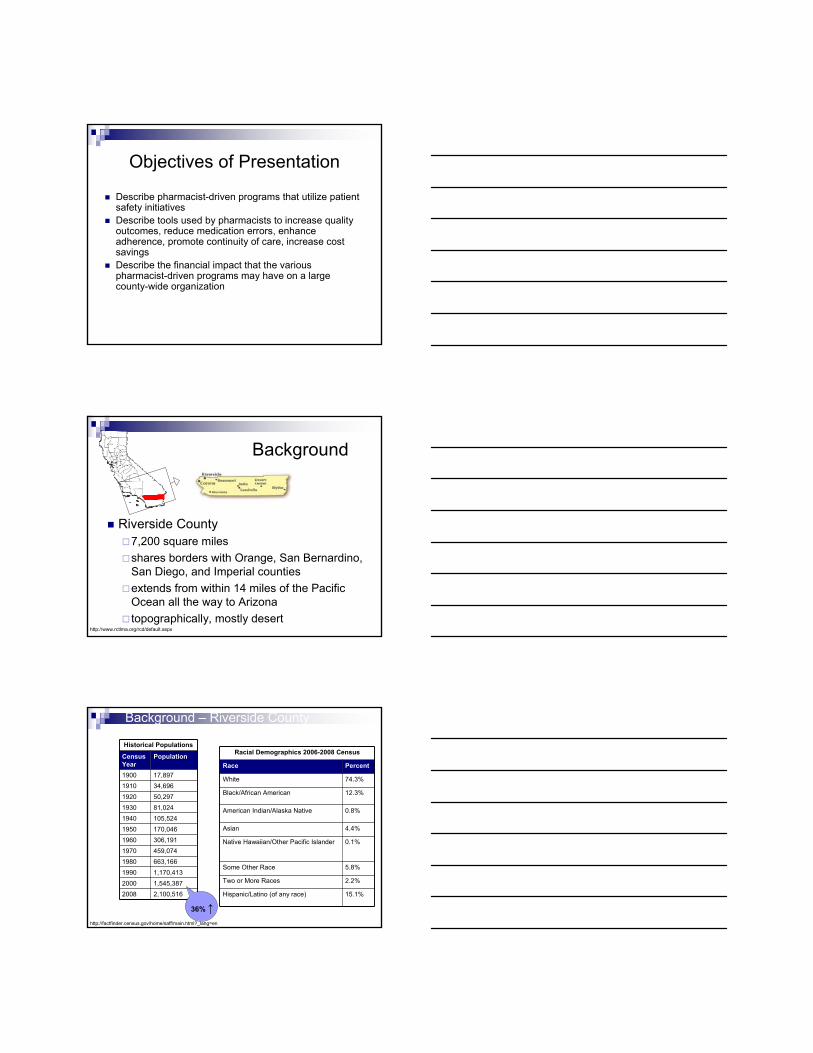
P = Problem (In terms of Patient Care Diagnosis)I = Intervention (Include: short term goals, education)
P = Plan (Evaluation of interventions, response to treatment, change in patient status, chronological
documentation of patient’s clinical course) Date/Time Discipline
Pharmacist Home Medication Reconciliation - reviewed by pharmacist Discussed with: Patient Family Other _______________________________
Source of patient’s medication history: : Patient Family Other_____________
Allergies: Ht/ Wt: Pregnancy/Lactation Status: Home Medications Continued on Admission: Home Medications Not Continued on Admission: New Medications: IVF: Prn Fever/HA Prn N/V: Prn Sleep: Prn Pain: Current medications were reviewed for appropriate criteria of use and dosage. Communicated with Monitored patient’s response to new medication(s):
No adverse reaction reported Adverse reaction reported with_________________
Provided education on new medications(s) to patient/family with expected effects, significant adverse drug reactions, and potential drug interactions. Pharmacological VTE prophylaxis received on day or day after admission. All questions/concerns regarding medications were addressed to patient/family Pharmacist will monitor medications use. Tran Phan, Pharm.D Ext: 66636 DISCIPLINE LEGEND: MD/DO Physician RT Respiratory Therapy R.D. Registered DieticianRN Nursing PT Physical Therapy S.W. Social ServiceRPH Pharmacist OT Occupational Therapy SP Speech Pathology
Riverside County Regional Medical Center
INTERDISCIPLINARY PATIENT PROGRESS NOTES P.I.P. Charting
#104 Rev. 10/03
ADDRESSOGRAPH
Medication Reconciliation Form
Objectives of Presentation
Describe pharmacist-driven programs that utilize patient safety initiativesDescribe tools used by pharmacists to increase quality outcomes, reduce medication errors, enhance adherence, promote continuity of care, increase cost savings Describe the financial impact that the various pharmacist-driven programs may have on a large county-wide organization
Background
Riverside County7,200 square miles shares borders with Orange, San Bernardino, San Diego, and Imperial counties extends from within 14 miles of the Pacific Ocean all the way to Arizonatopographically, mostly desert
http://www.rctlma.org/rcd/default.aspx
Background – Riverside County
Historical Populations
Census Year
Population
1900 17,8971910 34,6961920 50,2971930 81,0241940 105,5241950 170,0461960 306,1911970 459,0741980 663,1661990 1,170,4132000 1,545,3872008 2,100,516
http://factfinder.census.gov/home/saff/main.html?_lang=en
Racial Demographics 2006-2008 Census
Race Percent
White 74.3%
Black/African American 12.3%
American Indian/Alaska Native 0.8%
Asian 4.4%
Native Hawaiian/Other Pacific Islander 0.1%
Some Other Race 5.8%
Two or More Races 2.2%
Hispanic/Latino (of any race) 15.1%
36% ↑
Background - RCRMC
Institution > 100 years, new location since March 1998 –Moreno ValleyLevel II adult & pediatric trauma center439 beds – 362 at RCRMC and 77 at separate psychiatric facility12 operating roomsIntensive care units (adult, pediatric, neonatal)24 hour physician staffingImmediate OR accessAdjacent helipad
Complete radiology services (MRI, CT)Occupational and physical therapy servicesComplete laboratory servicesComplete pulmonary services (Hyperbaric oxygen treatments)Complete diagnostic services (EEG, ECG, ECHO)Full pediatric servicesEmergency room and Level II trauma centerPharmacy with Clinical Pharmacists on site
http://rcrmc.org/home/
System Change
Transactional ChangeIndividual tasks, skills, abilities
Transformational ChangeAltered paradigmShift in valuesReform in beliefs
Cost Control is Cost Control is TransactionalTransactional
Quality Improvement is Quality Improvement is TransformationalTransformational
““Transformed means that when Transformed means that when times are tough, we invest more times are tough, we invest more in qualityin quality””
Charles Buck – retired GE executive
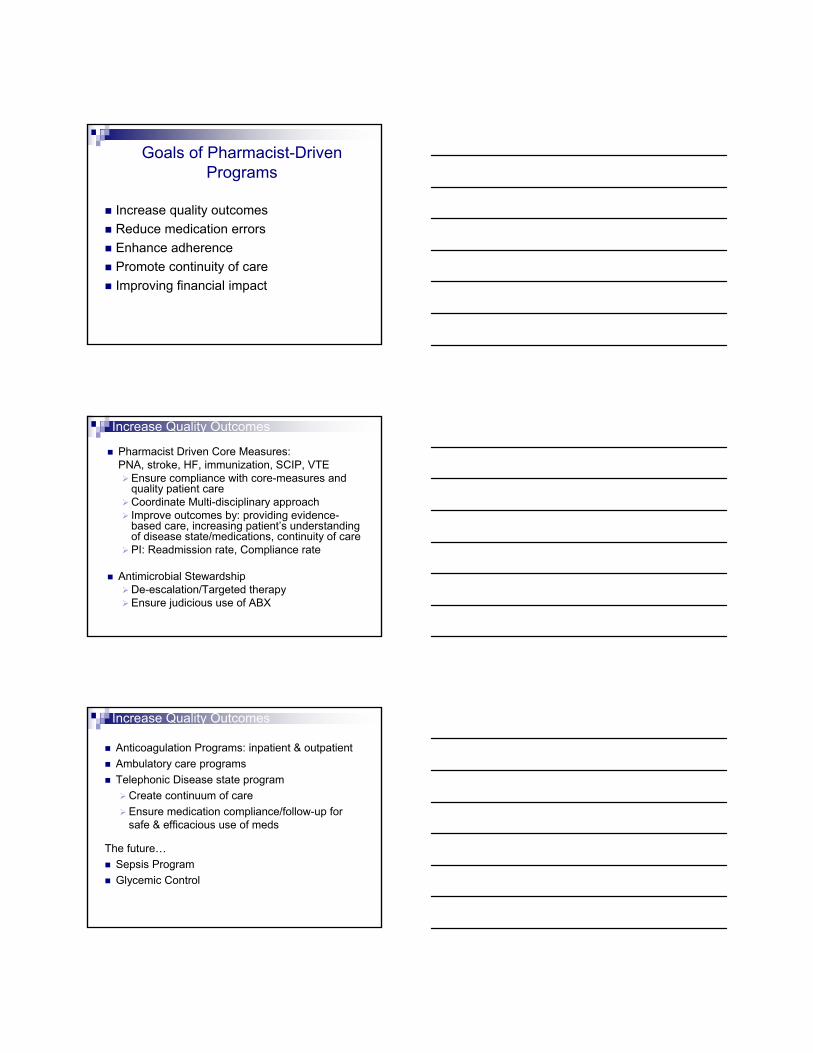
Inpatient
Outpatient
Admission Pharmacists
Unit Based Pharmacists
Core Measures Pharmacists
Discharge PharmacistsOutpatient Pharmacists
Telephonic Disease
Management Pharmacists
Ambulatory Care Pharmacists
KineticsPharmacists
Specialty Service Pharmacists
ED Pharmacists
Community / School Based Clinic Pharmacists
Mail Order Pharmacists
ID Pharmacists
Managed CarePharmacists
Medication Safety Pharmacists
ITPharmacists
Goals of Pharmacist-Driven Programs
Increase quality outcomes Reduce medication errorsEnhance adherencePromote continuity of careImproving financial impact
Increase Quality Outcomes
Pharmacist Driven Core Measures: PNA, stroke, HF, immunization, SCIP, VTE
Ensure compliance with core-measures and quality patient careCoordinate Multi-disciplinary approachImprove outcomes by: providing evidence-based care, increasing patient’s understanding of disease state/medications, continuity of carePI: Readmission rate, Compliance rate
Antimicrobial StewardshipDe-escalation/Targeted therapyEnsure judicious use of ABX
Anticoagulation Programs: inpatient & outpatientAmbulatory care programsTelephonic Disease state program
Create continuum of careEnsure medication compliance/follow-up for safe & efficacious use of meds
The future…Sepsis ProgramGlycemic Control
Increase Quality Outcomes
Pharmacist-Driven Sepsis Program
Pharmacists will respond with rapid response teamsAssess patients hospital-wide to meet criteria for sepsis criteriaEligible patients will be activated into the 24-hour sepsis bundle and followed by the clinical pharmacistThe clinical pharmacist will ensure that the 24-hour sepsis bundle are being followed
Increase Quality Outcomes
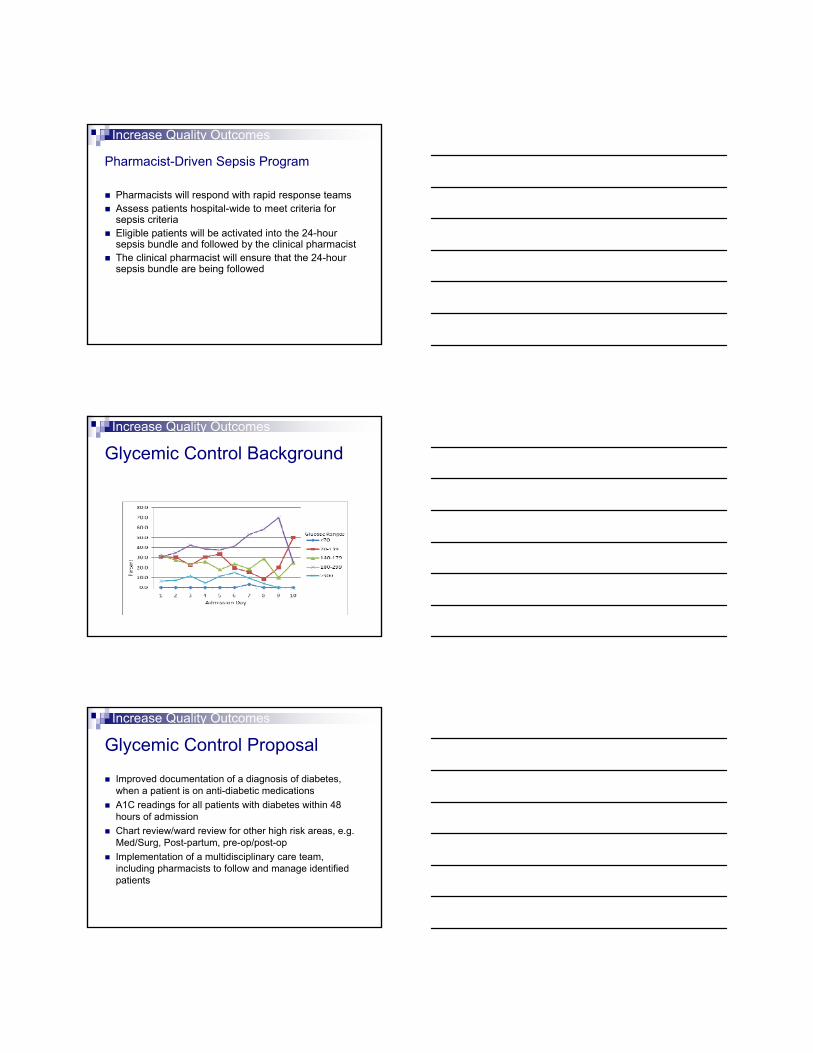
Glycemic Control BackgroundIncrease Quality Outcomes
Glycemic Control Proposal
Improved documentation of a diagnosis of diabetes, when a patient is on anti-diabetic medicationsA1C readings for all patients with diabetes within 48 hours of admissionChart review/ward review for other high risk areas, e.g. Med/Surg, Post-partum, pre-op/post-opImplementation of a multidisciplinary care team, including pharmacists to follow and manage identified patients
Increase Quality Outcomes

Example: Heart Failure Program
HF Admission
HF Inpatient
HF DischargeHF ‐Telephonic Disease State Management
HF Ambulatory
Clinic
Discharge –Non‐HF Admits
Physician Referrals
Increase Quality Outcomes
Reduction in Readmission Rates
24.0%
15.3% 15.3% 17.6% 17.2% 14.7%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Prior to HF Program
May 2010 Jun 2010 July 2010 Aug 2010 Sept 2010
Increase Quality Outcomes
P = Problem (In terms of Patient Care Diagnosis) I = Intervention (Include: short term goals, education)
P = Plan (Evaluation of interventions, response to treatment, change in patient status, chronological
documentation of patient’s clinical course) Date/Time Discipline
Pharmacy HF Initial Progress Note EF: _______%
PMH:
If patient is diagnosed with HF or admitted for HF exacerbation or has a history of HF w/ ↓ LVEF (<40%), recommend patient be discharged with the following:
ACEI/ARB Current Dose
Benazepril (Lotensin)
Losartan (Cozaar)
Beta-Blocker
Carvedilol (Coreg)
Metoprolol XL (Toprol XL)
Only sustained release form of metoprolol has been proven to reduce mortality. Please consider changing metoprolol (Lopressor) to metoprolol XL (Toprol XL)
NOTE: If patient cannot be discharged with these medications please document the reason (ie. contraindication, allergy, bradycardia)
Patient Consultation:
Discussed low-salt diet, fluid restriction, healthy life-style, activity level, smoking cessation, avoidance of EtOH & illicit drugs, daily weight monitoring.
Educated patient on s/sx of worsening HF and what to do if symptoms worsen.
HF verbal and written education given to patient addressing 1. Activity level, 2. Diet 3. Follow-up monitoring 4. Weight monitoring, 5. What to do if symptoms worsen
Educated patient on HF medications, proper use, expected effects, significant ADRs, and potential drug interactions
Spanish translation provided if Spanish-speaking
Intervention:
Recommend considering alternate agent for NSAID __________. NSAID can cause sodium retention and peripheral vasoconstriction and can attenuate the efficacy and enhance the toxicity of diuretics and ACE inhibitors.
Recommend considering alternate agent for antiarrhythmic agent __________. Antiarrhtymic agent can exert important cardiodepressant and proarrhythmic effects. Only amiodarone and dofetilide have been shown not to adversely affect survival.
Recommend considering alternate agent for Calcium Channel Blocker __________. Calcium channel blockers can lead to worsening HF and have been associated with an increased risk of cardiovascular events. Only the vasoselective ones have been shown not to adversely affect survival.
Other recommendation:
Please feel free to contact with any questions.
Pharmacist: PharmD. Ext 30222 - pager 344-5646
Riverside County Regional Medical Center
NTERDISCIPLINARY PATIENT PROGRESS NOTES 04
Rev. 5/10
ADDRESSOGRAPH
HF Initial HF Initial Progress Progress NotesNotes
Increase Quality Outcomes
P = Problem (In terms of Patient Care Diagnosis)I = Intervention (Include: short term goals, education)
P = Plan (Evaluation of interventions, response to treatment, change in patient status, chronological
documentation of patient’s clinical course) Date/Time Discipline
Pharmacy Pharmacy Discharge Progress Note: Discharge Medication Reconciliation/Consultation
ACUTE MYOCARDIAL INFARCTION
Patient is being discharged with the following: If not, reason stated:
Aspirin Beta-Blocker
ACEI or ARB for LVSD Statin
HEART FAILURE EF: % Patient is being discharged with the following: If not, reason stated:
ACEI/ARB Beta-Blocker
HF written and verbal education provided to patient addressing the following: 1. Activity level, 2. Diet, 3. Discharge medications, 4. Follow-up appointment, 5. Daily weight monitoring, 6. What to do if symptoms worsen
STROKE
Patient is being discharged with the following: If not, reason stated
Antithrombotic therapy Statin
Anticoagulation therapy for Afib/flutter N/A
Stroke verbal and written education given to patient addressing: 1. Activation of emergency medical system 2. Follow-up after discharge 3. Discharge Medications 4. Risk factors for stroke 5. Warning signs and symptoms of stroke
Assessed for Rehabilitation ALL PATIENTS
Patient has received Pneumococcal and Influenza vaccination (Oct-Mar) prior or during hospital stay If not, reason stated:
Smoking cessation advice/Counseling
Discharge medication reconciliation performed by pharmacist. Educated patient on medications, changes in medication regimen and proper use, expected effects, significant ADRs, and potential drug interactions. Patient was given a written list of complete discharge medications.
Educated patient to STOP following medications:
Spanish translation provided if Spanish-speaking.
Follow-up Appointments: Per discharge summary
Pharm.D Ext DISCIPLINE LEGEND: MD/DO Physician RT Respiratory Therapy R.D. Registered DieticianRN Nursing PT Physical Therapy S.W. Social Service RPH Pharmacist OT Occupational Therapy SP Speech Pathology
Riverside County Regional Medical Center
INTERDISCIPLINARY PATIENT PROGRESS NOTES P.I.P. Charting
#104 Rev. 05/10
ADDRESSOGRAPH
Pharmacist Discharge Medication Reconciliation/Consultation
Increase Quality Outcomes
IV infusion ProgramPCA monitoringUnit-based pharmacist: daily review of medication profiles, med reconciliation on admission and dischargeBlack box warningsHigh risk medicationsNon-Formulary processPeer Review
Reduce Medication Errors
Rm Name IV/Med
CkTime
DateOrdered
Rate/FreqOrdered
Rate On MAR
RateOnPump
Med GivenOn Time
Discrepancy/Note
IV Infusion Pump Monitoring Record
Reduce Medication Errors

P = Problem (In terms of Patient Care Diagnosis)I = Intervention (Include: short term goals, education)
P = Plan (Evaluation of interventions, response to treatment, change in patient status, chronological
documentation of patient’s clinical course) Date/Time Discipline
Pharmacist Medication management performed by Pharmacist
Review transfer medication reconciliation
Reviewed physician orders and patient’s medication profile
Reviewed medications for appropriate criteria of use and dosage
Reviewed current / new medication(s) with patient regarding expected
effects, significant ADRs, potential drug interactions
Checked medication administration record
Monitored patient’s response to new medication(s):
Adverse reaction reported with_________________
No adverse reaction reported
All questions, concerns regarding medications were addressed to patient.
DISCIPLINE LEGEND: MD/DO Physician RT Respiratory Therapy R.D. Registered DieticianRN Nursing PT Physical Therapy S.W. Social Service RPH Pharmacist OT Occupational Therapy SP Speech Pathology
Riverside County Regional Medical Center
INTERDISCIPLINARY PATIENT PROGRESS NOTES P.I.P. Charting
#104 Rev. 10/03
ADDRESSOGRAPH
Reduce Medication Errors
Medication Management Progress Note
Example 1: APAP MonitoringMedication
Safety Goal Numerator /Denominator 2009 2010
APAP totalAbove
4grams/day0%
# pt getting more than 4 g a day per MAR review/# patients on APAP
Qtr 1 Qtr 2 Qtr 3 Qtr 4 2009 Qtr 1 Qtr 2 Qtr 3 Qtr 4 2010
Rate 10% 13% 9% 11% 1% 3% 2%
Numerator 27 62 32 121 2 6 4
Denominator 282 481 375 1138 279 233 170
Daily Acetaminophen Usage Less Than 4 g/Day
0%
10%
20%
Qtr 1 '09
Qtr 2 '09
Qtr 3 '09
Qtr 4 '09
Qtr 1 '10
Qtr 2 '10
Qtr 3 '10
Qtr 4 '10
Reduce Medication Errors
Example 2: Erythropoetin Monitoring
GoalNumerator /Denominator 2009 2010
Erythropetinonly
in patients WithHgb<12
100%
# patients with Hgb less than 12/# patients on EPO Qtr1 Qtr2 Qtr3 Qtr4 Year
2009 Qtr1 Qtr2 Qtr3 Qtr4Year2010
Rate (%) 93 94 94 95 94 94 96 100
Numerator (N)117 08 111 119 137 83
Denominator (D)124 115 117 127 143 83
EPO Only Dispensed to Patients with Hgb less than 12
60%
70%
80%
90%
100%
Qtr 1 '09
Qtr 2 '09
Qtr 3 '09
Qtr 4 '09
Qtr 1 '10
Qtr 2 '10
Qtr 3 '10
Qtr 4 '10
Reduce Medication Errors
WHO – Statistics50% of patients take medications incorrectlyOveruse, underuse or misuse of medicines harms people and wastes resources > 50% of all countries do not implement basic policies to promote rational use of medicines
World Health Organization: www.who.int/mediacentre
Enhance Adherence
United States:The direct & indirect costs ~ $100 billion/yearUnfilled prescriptions ~140 million prescriptions/year ≈ $2.8 billion125,000 deaths annually are attributed to nonadherenceUp to 11% of hospital admissions and 40% of nursing home admissions are due to lack of adherence with medication therapy
American Pharmacists Association: www.pharmacist.com
Enhance Adherence
Provider-related BarriersLack of counseling
Financial BarriersInability to pay for medications
Patient-related BarriersLack of transportationDisease-related: memory loss, cognitive impairmentLack of understanding (language, regimen)
American Pharmacists Association: www.pharmacist.com
Enhance Adherence
Admission
Hospital StayDischarge
Medication Reconciliation
•Home Medication Reconciliation
•Review Meds for dosing, appropriateness, ADR
•Patient Education
•Confirm coverage upon discharge
Enhance Adherence
Patient Assistance Program (PAP)PAP Coordinator within Dept. of PharmacyFree or discounted medications from Pharmacompanies
Low-income, uninsured or under-insuredWhy use PAP?
PAP medications supplement and expand formularyEases workflow in the Dispensary
Relief of financial burden on MISPCalifornia clinics were less likely to use PAP than other states in 2003*
*Duke KS et al. Patient-assistance programs: assessment of and use by safety-net clinics. AJHP. 2005;62:726-731.
Enhance Adherence
Mail Order Services90-days supplyWaived co-pays10-days compliance callsDiabetic supplies for indigent patients
Enhance Adherence
Generalized Plan for Clinical Pharmacy DSM Call Center
New Rx for Atypical Antipsychotics* – list from
FSI
CHF patients d/c from RCRMC – list from CHF
pharmacists
Pilot Disease/Medications
CHF Antipsychotics
Pilot Population of Focus - PoF
Telephone Scripts
Technician/OAs/students - TBD
Pharmacists/Interns - TBD
Roles and Responsibilities
Technician/OAs/Students • Confirm patient picked up
medications upon discharge • Assist patient in filling/refilling
RX, refer to mail order • Confirm patient’s current
medication regimen – call pharmacies, check med rec/charts, etc.
• Interview patients and collect information** for pharmacist’s review
• Refer to pharmacist for questions/concerns
Pharmacist/Interns • Answer questions/concerns from
referred patients • Educate patient on medications as
needed, importance of compliance/adherence, diet, physical exercise, etc.
• Review information gathered by tech/OA for appropriateness of drug therapies***
• Set up clinic appt for follow-up as necessary
• Set up lab appt prior to follow-up as necessary
• Prescriptive authority for 1x refill until clinic appt if necessary?
• Document review/consultation/recommendation as progress note in charts****
Enhance Adherence
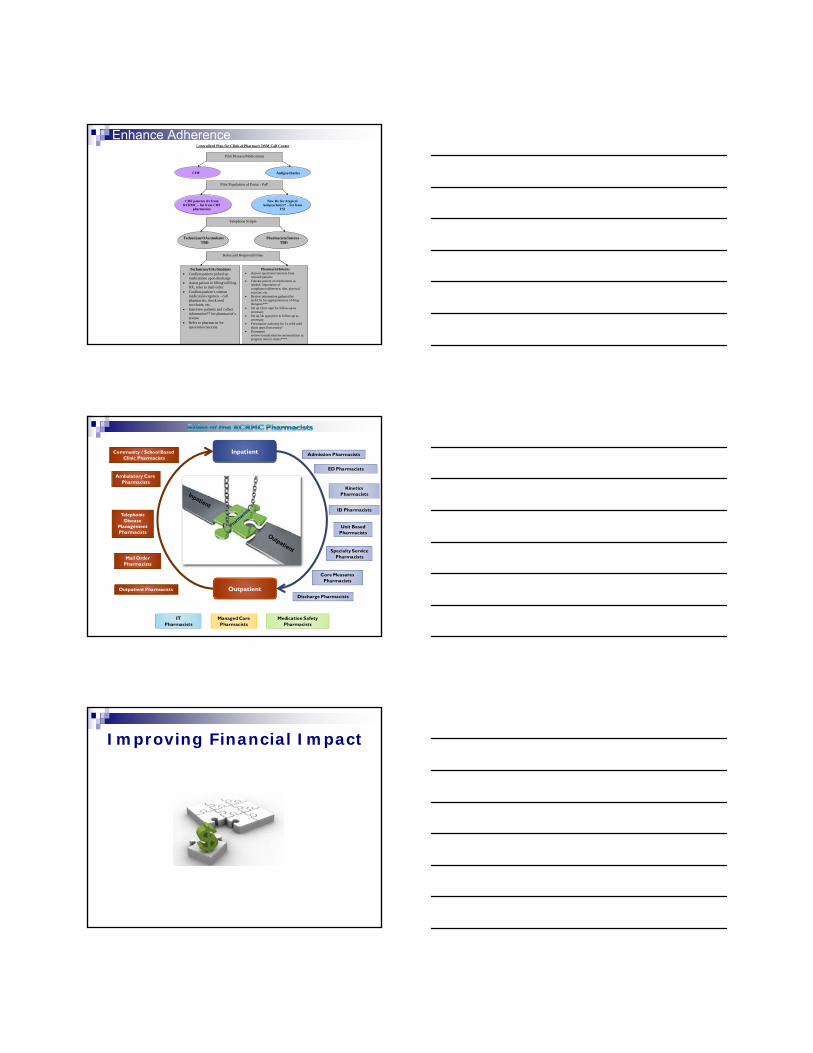
Inpatient
Outpatient
Admission Pharmacists
Unit Based Pharmacists
Core Measures Pharmacists
Discharge PharmacistsOutpatient Pharmacists
Telephonic Disease
Management Pharmacists
Ambulatory Care Pharmacists
KineticsPharmacists
Specialty Service Pharmacists
ED Pharmacists
Community / School Based Clinic Pharmacists
Mail Order Pharmacists
ID Pharmacists
Managed CarePharmacists
Medication Safety Pharmacists
ITPharmacists
Improving Financial Impact

Perez et al. Economic Evaluation of Pharmacy Services 2001-2005, ACCP
Improving Financial Impact
$0
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
$700,000
$800,000
$900,000
$1,000,000
Jul 09 Aug 09 Sept 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 10 Sept 10 Oct 10 Nov 10
Pharmacist-Run Indigent Managed Care Program
Improving Financial Impact
$0
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
$700,000
$800,000
$900,000
$1,000,000
Jul 09 Aug 09 Sept 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 10 Sept 10 Oct 10 Nov 10
~ $450,000 / month
= ~$5.4 M / year
Gross Savings
Pharmacist-Run Indigent Managed Care Program
Improving Financial Impact
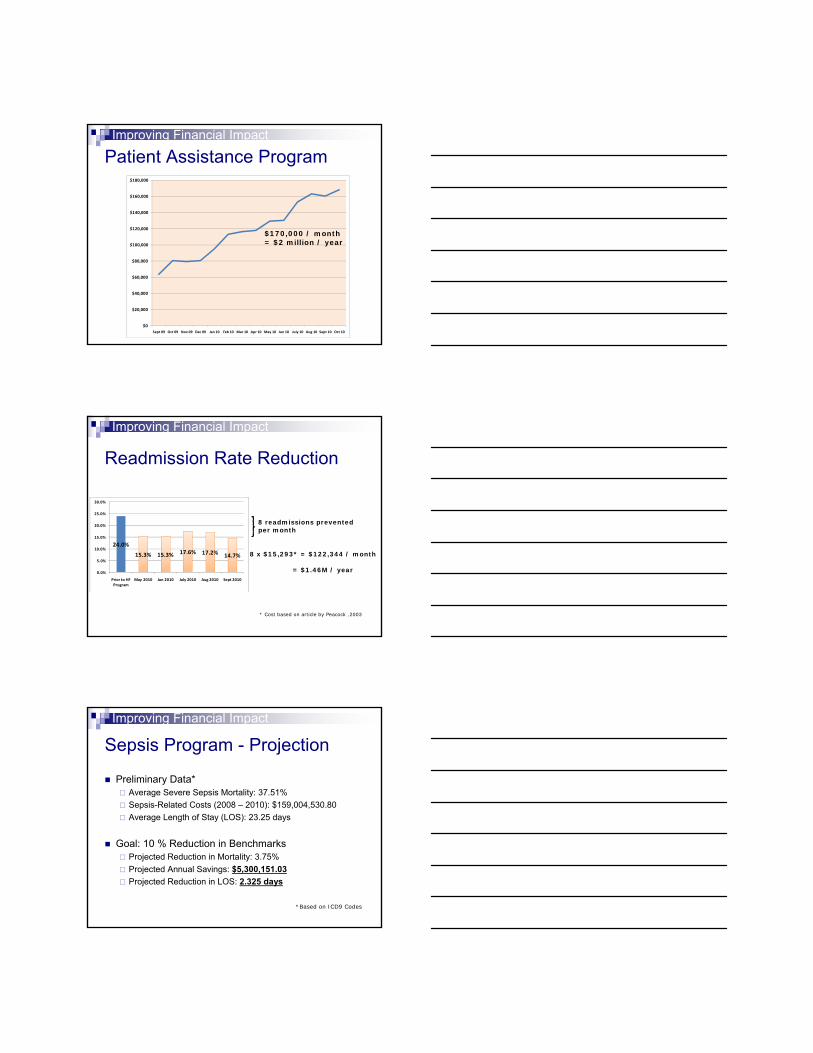
Patient Assistance Program
$0
$20,000
$40,000
$60,000
$80,000
$100,000
$120,000
$140,000
$160,000
$180,000
Sept 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 July 10 Aug 10 Sept 10 Oct 10
$170,000 / month= $2 million / year
Improving Financial Impact
8 readmissions prevented per month
8 x $15,293* = $122,344 / month
= $1.46M / year
* Cost based on article by Peacock ,2003
24.0%
15.3% 15.3% 17.6% 17.2% 14.7%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Prior to HF Program
May 2010 Jun 2010 July 2010 Aug 2010 Sept 2010
Readmission Rate Reduction
Improving Financial Impact
Sepsis Program - Projection
Preliminary Data*Average Severe Sepsis Mortality: 37.51%Sepsis-Related Costs (2008 – 2010): $159,004,530.80Average Length of Stay (LOS): 23.25 days
Goal: 10 % Reduction in BenchmarksProjected Reduction in Mortality: 3.75%Projected Annual Savings: $5,300,151.03Projected Reduction in LOS: 2.325 days
*Based on ICD9 Codes
Improving Financial Impact
Glycemic Control - Projections
Reduce hyper/hypoglycemic events.Reduce LOS due to poor glycemic control.Reduce ER visits and readmission.
Estimated $3 - 5 million / year saved.
Improving Financial Impact
CE Questions1. Name 3 pharmacist-driven programs at RCRMC that have played a role in patient
safety initiatives:A. Medication Safety, Unit-Based, Core MeasuresB. Admissions, Discharge, Ambulatory CareC. Mail Order, Ambulatory Care, Telephonic Disease State ManagementD. A, B and C
2. Which tool is used by pharmacists to increase medication safety, improve patient safety, and improve Core Measure data?
A. Giving patients free lunchB. Compliance callsC. Patient consultation upon admission and dischargeD. Both B and C
3. What kind of financial impact may pharmacist-driven programs have on a large hospital organization?
A. Minimal from any pharmacist-driven programB. The sepsis program shows a projected decrease in the length of stay in the hospitalC. The CHF program have shown an increase in readmission rateD. Both A and C


















