Optimal Management of ACS Invasive vs Conservative Strategy Layth Mimish Consultant Cardiologist The...
74
Optimal Management of ACS Invasive vs Conservative Strategy Layth Mimish Consultant Cardiologist The Cardiovascular Consultant Group Jeddah KSA
-
date post
19-Dec-2015 -
Category
Documents
-
view
220 -
download
0
Transcript of Optimal Management of ACS Invasive vs Conservative Strategy Layth Mimish Consultant Cardiologist The...

Optimal Management ofACS
Invasive vs Conservative StrategyLayth Mimish
Consultant Cardiologist
The Cardiovascular Consultant Group
Jeddah KSA



Approach To ACS
Risk stratification Appropriate acute medical management Identify coronary anatomy in higher risk
patients, otherwise exercise imaging PCI vs CABG based on extent of coronary
disease, LV function, and co morbid factors Long term medical management ; risk factors
modification

TIMI Risk Score for ACSUnfractionated Heparin Cohort TIMI 11B (n=1957)
Age > 65 years> 3 CAD risk factorsPrior CAD Stenosis > 50%ST segment changes on presentation> 2 anginal events in last 24 HrsASA use < 7years Increased serum cardiac markers


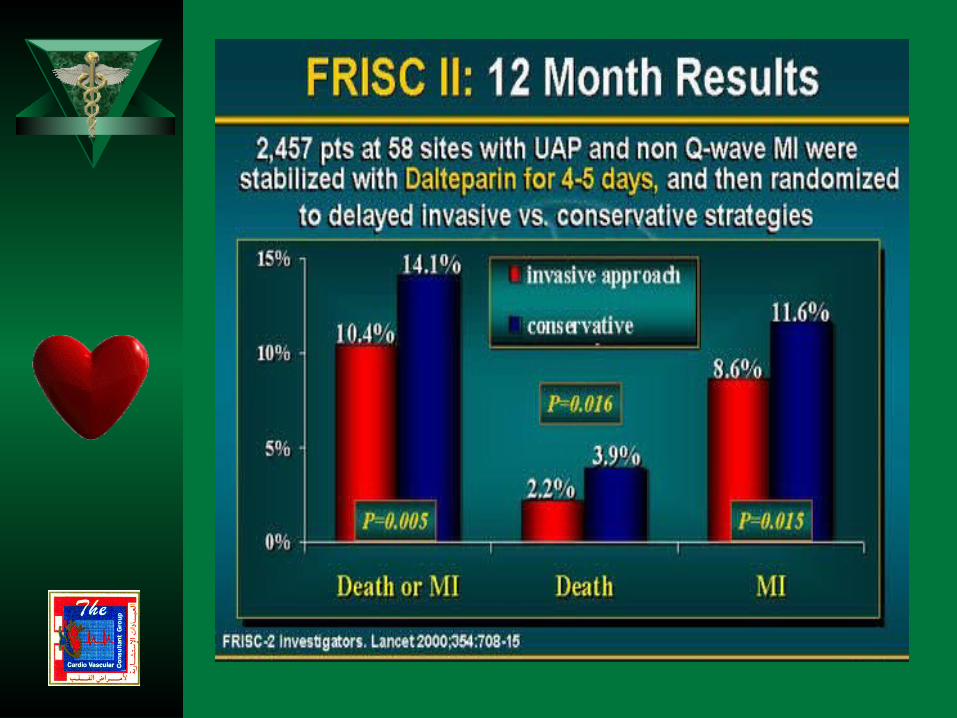
FRISC Score
Age>70 yearsDiabetes MellitusPrevious MIAngina > 30 daysST depressionElevated TroponinElevated FibrinogenElevated II-6 (2P)
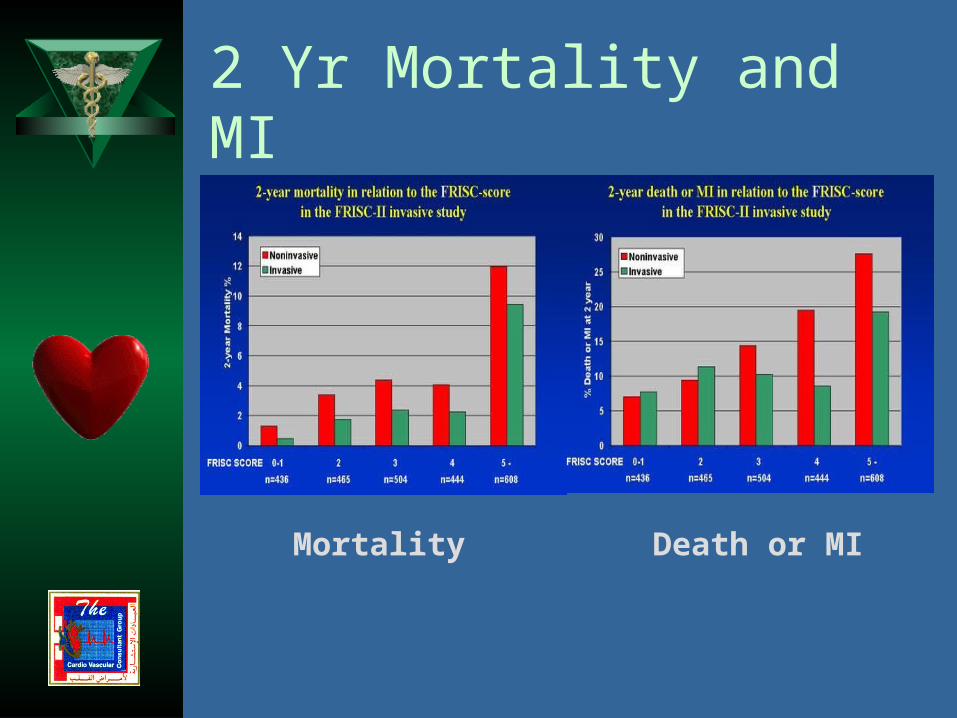
2 Yr Mortality and MI
Mortality Death or MI



Culprit Lesion Morphology & Troponin Levels in UAP



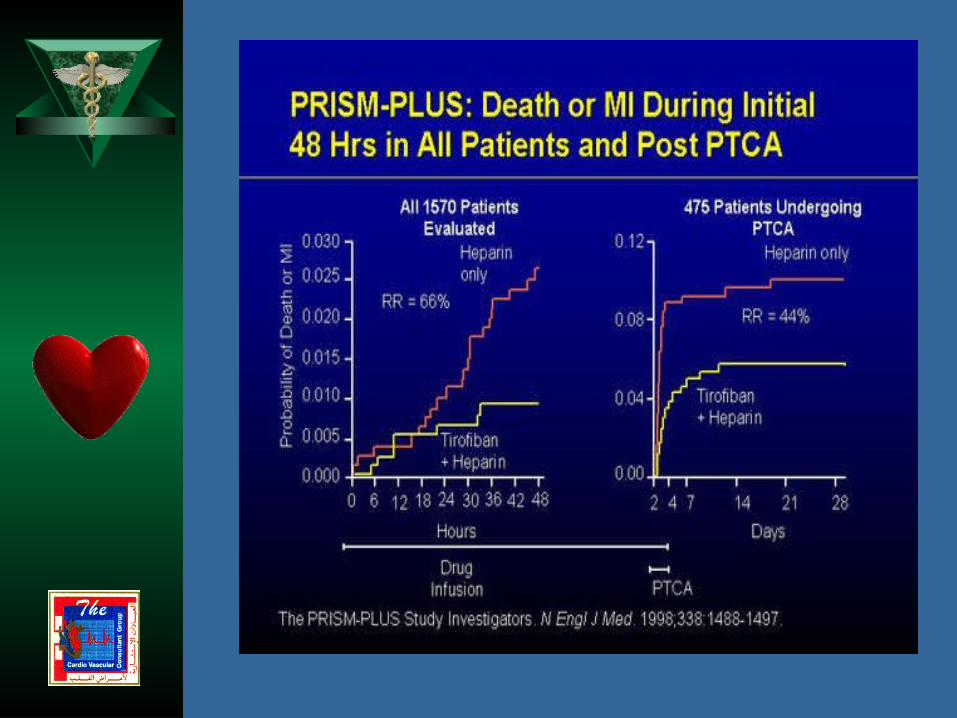
Antithrombotic approaches in ACS
Acute Medical Management ASA & LMWH ( FRIC, FRISC I&II, ESSENCE, TIMI 11B) Direct Thrombin Inhibitors (GUSTO IIB, OASIS-2) GP IIb/IIIa Inhibitors (4P Trials, Oral trials, GUSTO-IV ACS,
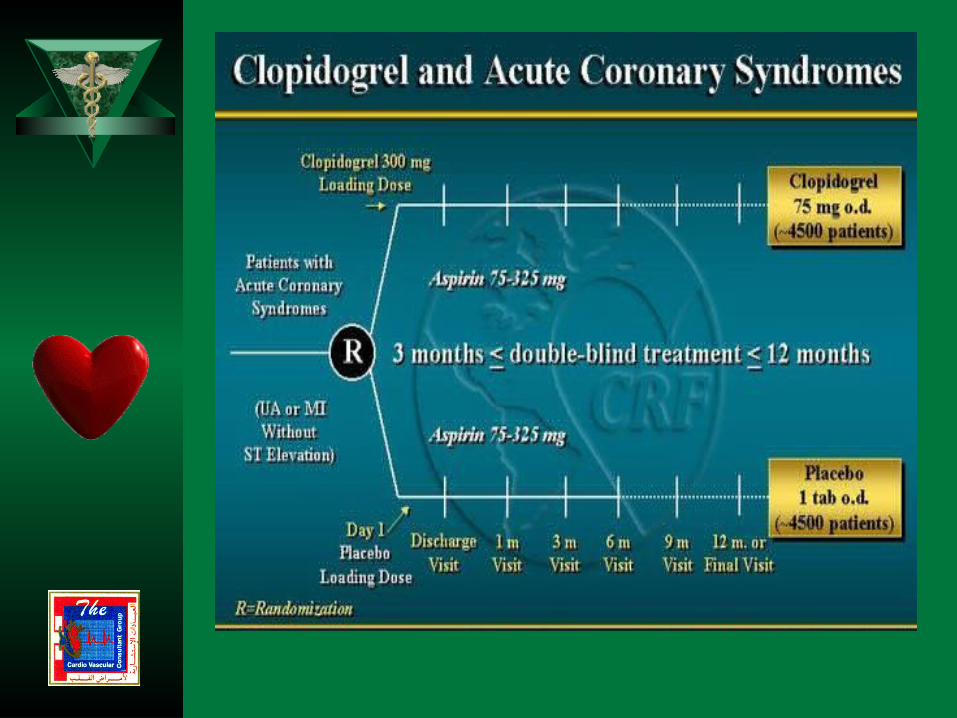
TIMI-18) ASA & Clopidogril (CURE)
Coronary Interventions Direct Thrombin Inhibitors (HELVETICA, Hirulog Trials) GIIbIIa Inhibitors (EPIC, EPILOG, CAPTURE, EPISTENT,
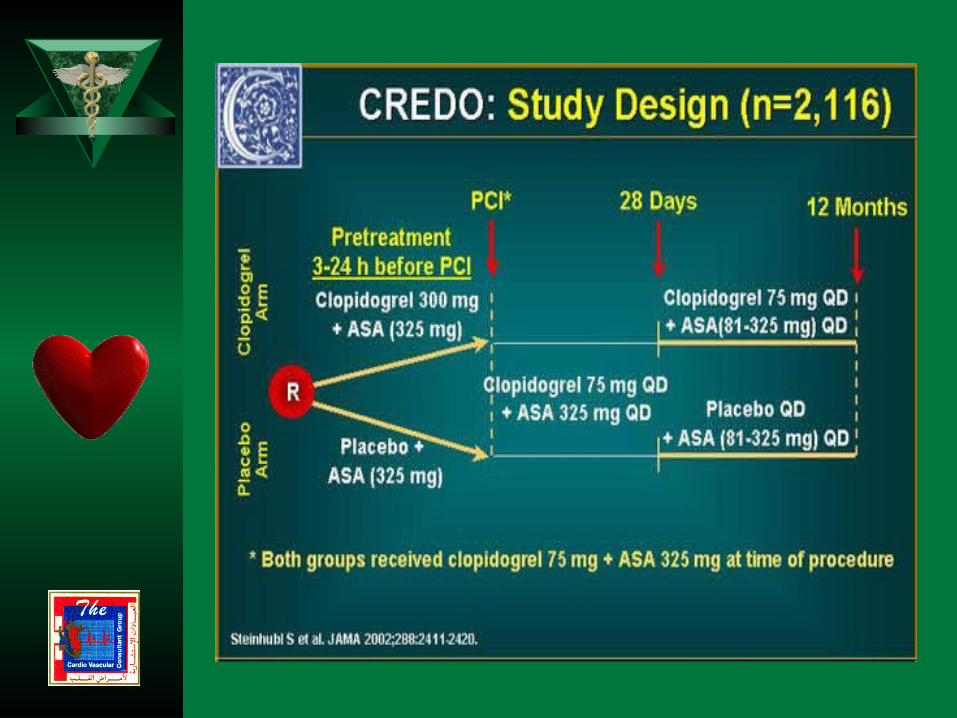
IMPACT-2, RESTORE, ESPIRIT, TARGET) LMWH & GPIIb/IIIa Inhibitors(NICE Registry) ASA & Clopidogril (CREDO)











Overview of GP IIb/IIIa Trials by Pooled Analysis


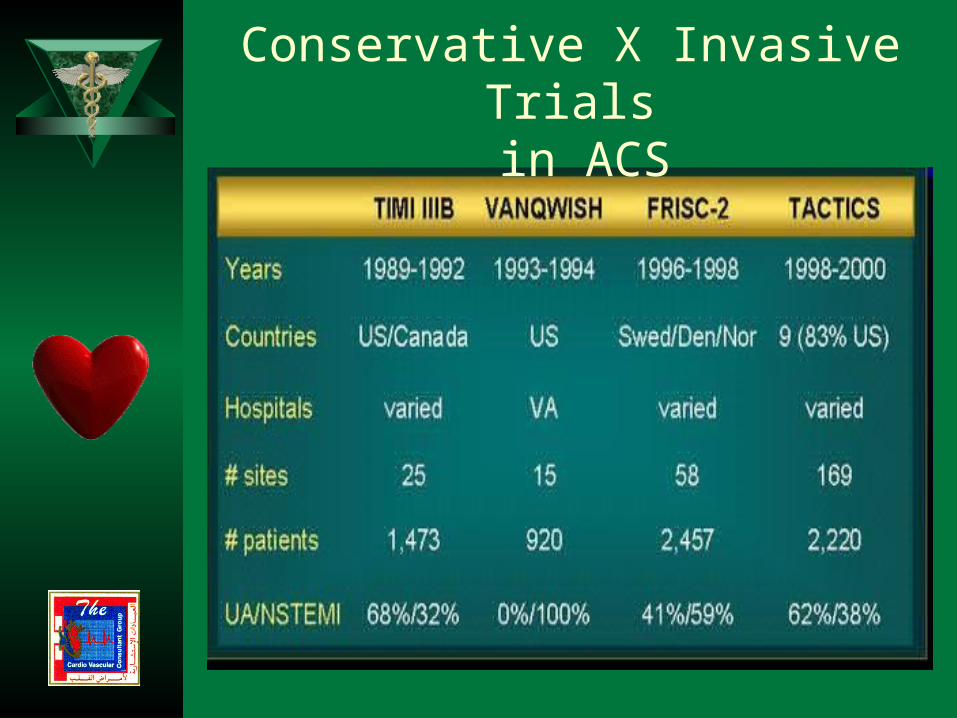
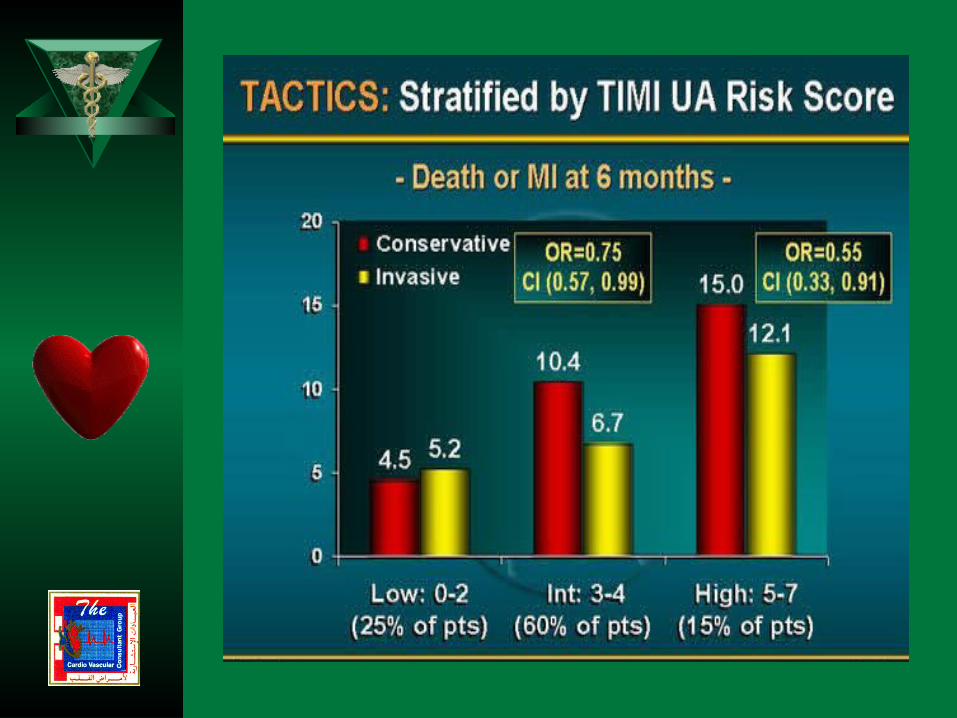
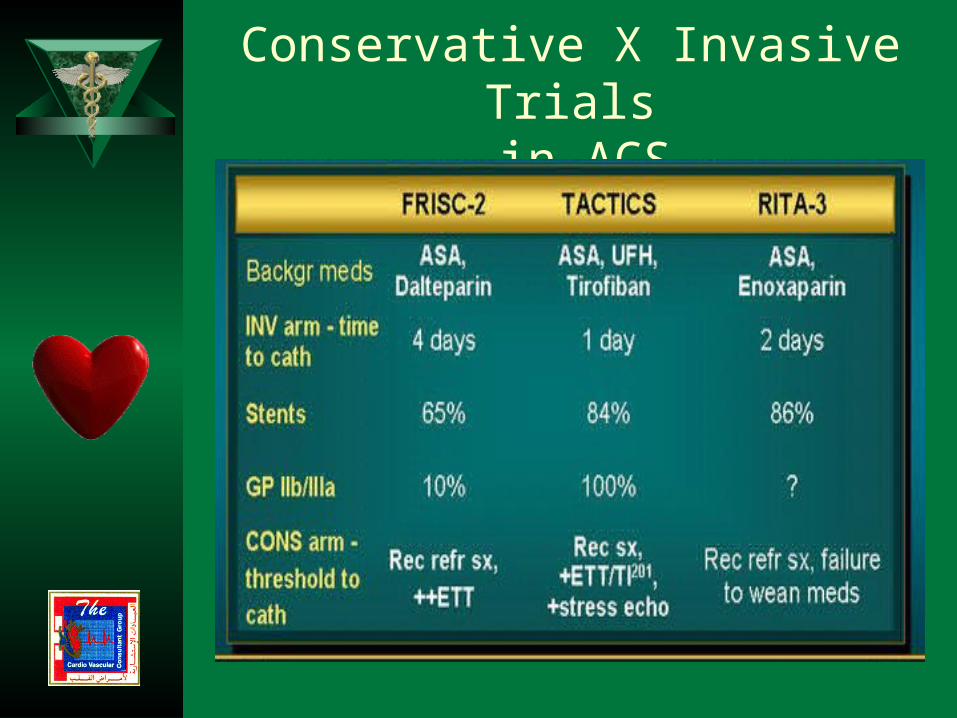
Conservative X Invasive Trials in ACS

Conservative X Invasive Trials in ACS

TIMI - IIIB




Study Limitations of VANQUISH
High surgical mortality (7.7%) & 12% in invasive arm
PTCA performed prior to era of stents and GPIIb/Iia blockers
No PTCA for multivessel diseaseResults not necessarily applicable
to females
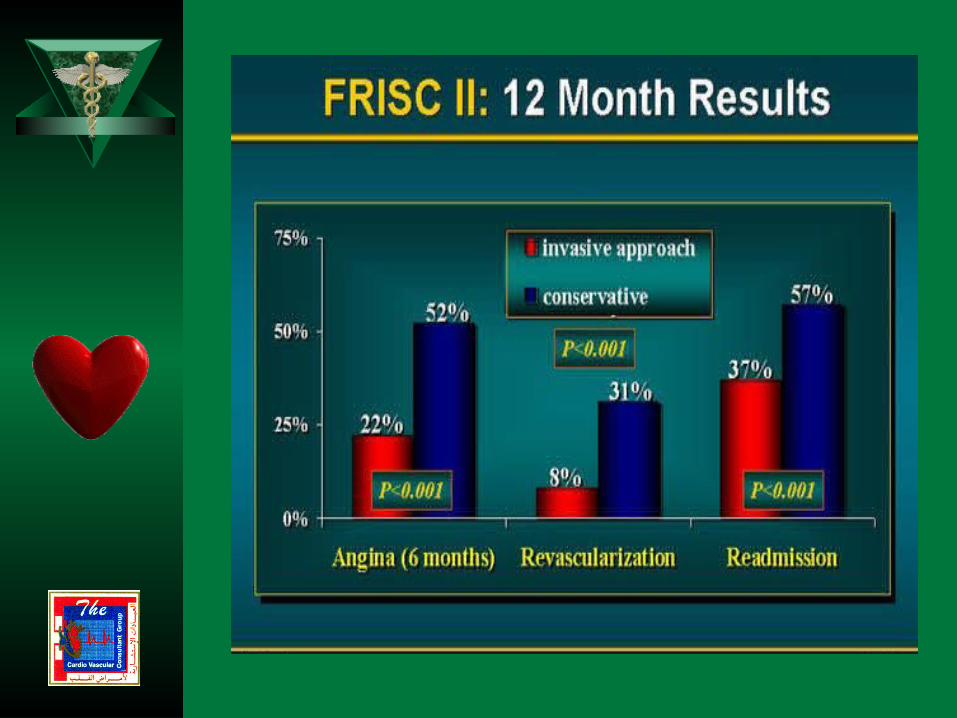



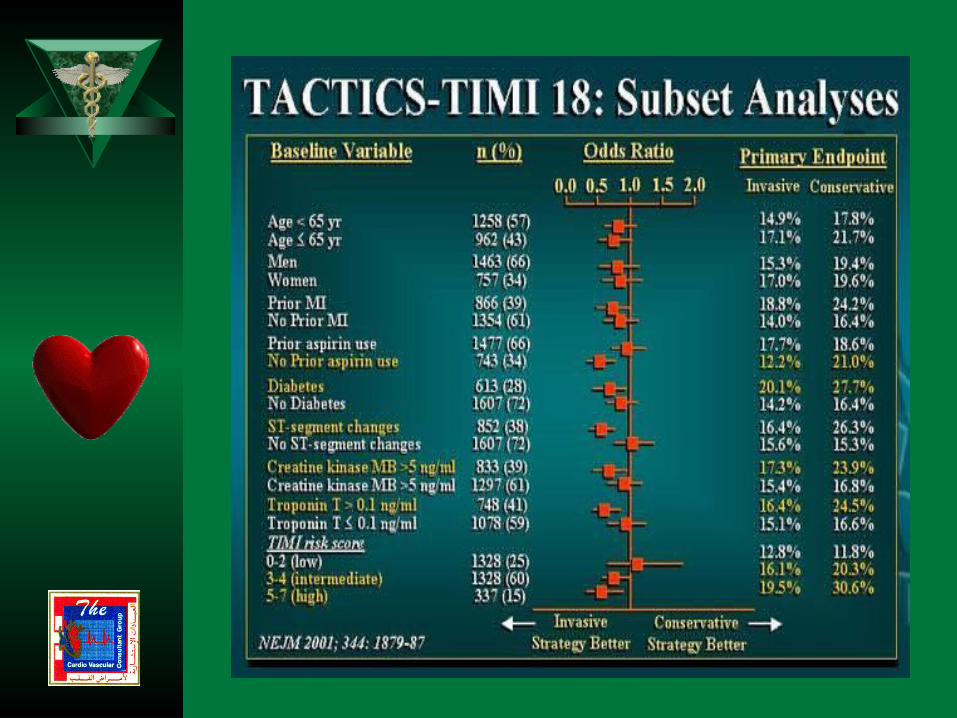

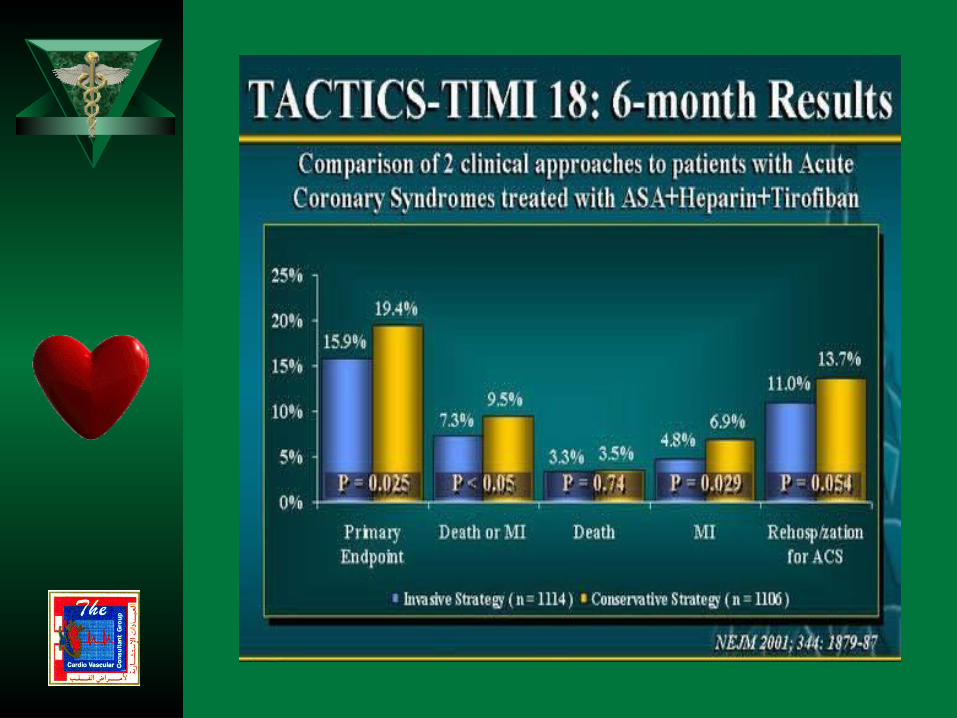
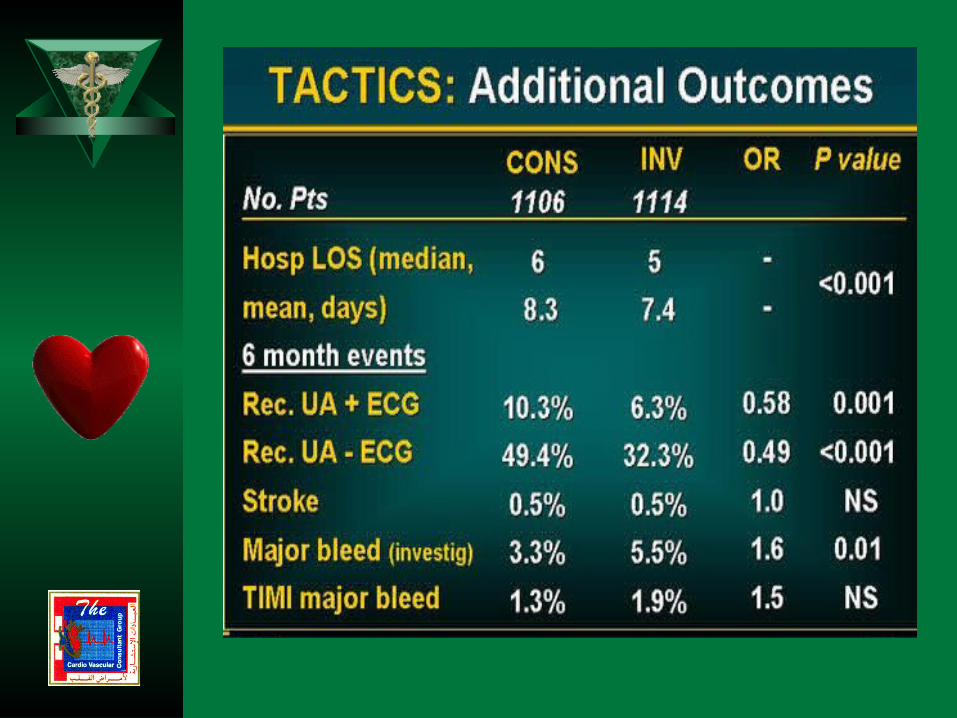
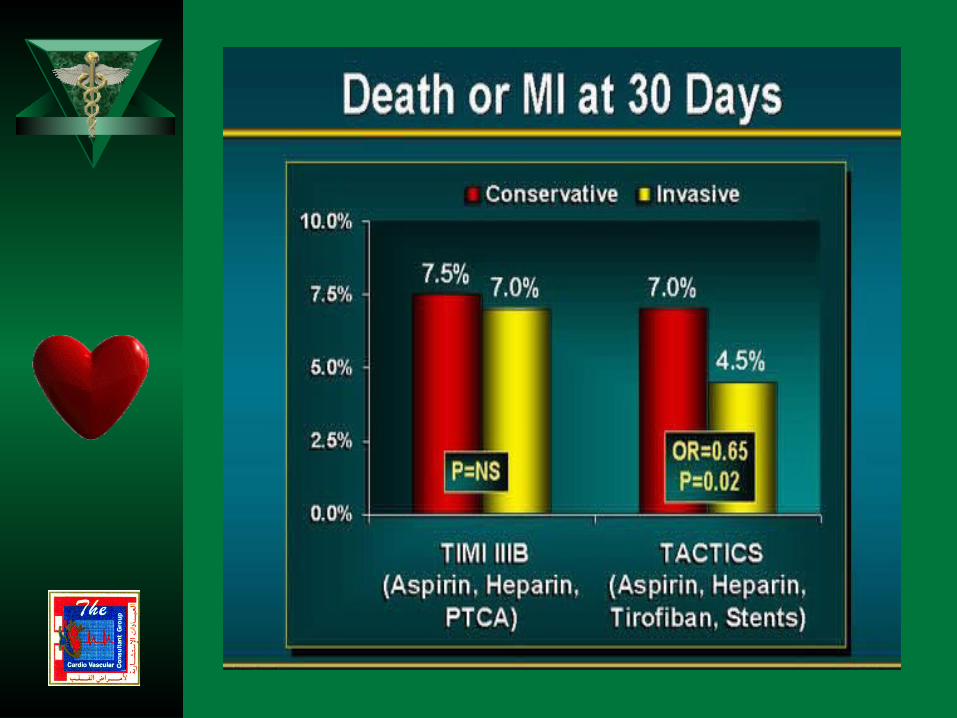





Conservative X Invasive Trials in ACS

Conservative X Invasive Trials in ACS
Conservative X Invasive Trials in ACS
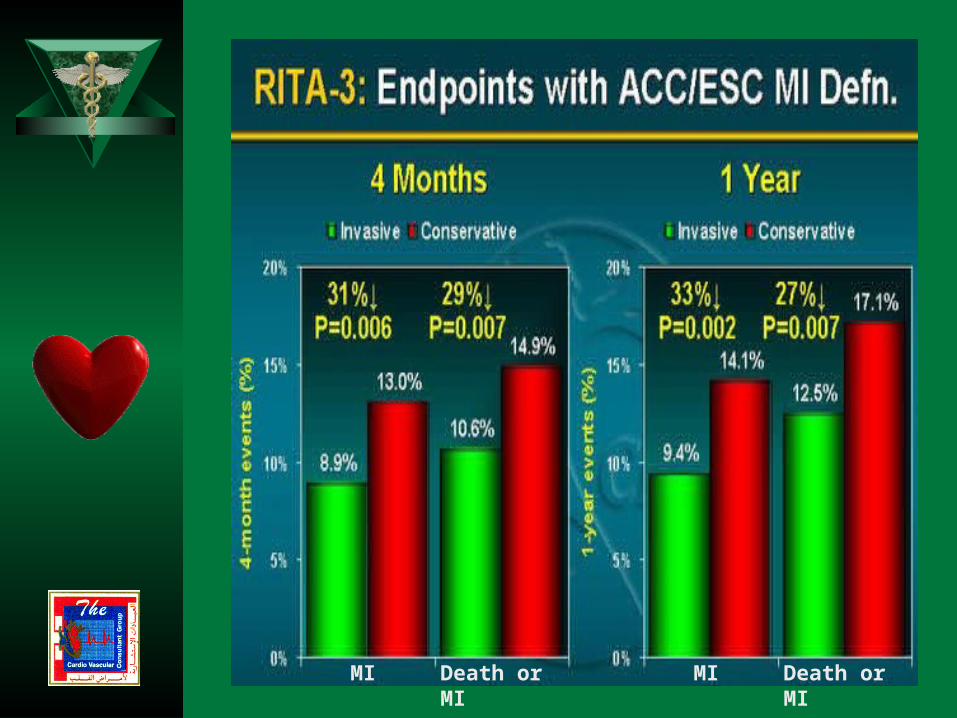
MIDeath or MIMI Death or MI