Optimal ambulance routing for mass casualty events
40
Optimal Ambulance Routing for Mass Casualty Events Conference on Dynamics of Disasters Athens, Greece, October 5–7, 2006 by Alkis Vazacopoulos
-
Upload
alkis-vazacopoulos -
Category
Technology
-
view
842 -
download
2
Transcript of Optimal ambulance routing for mass casualty events

Optimal Ambulance Routing
for Mass Casualty Events
Conference on Dynamics of Disasters Athens, Greece,
October 5–7, 2006
by Alkis Vazacopoulos

2
Research Team
Dash Optimization
– Alkis Vazacopoulos, PHD
– Gabriel Tavares
– Horia Tipi
Weill Medical College of
Cornell University
– Nathaniel Hupert, MD, MPH
– Eric Hollingsworth
– Wei Xiong

3
Imagine…
Katrina, Rita, Andrew, Allison…
London, Madrid, Beslan, 9/11…
Boca Raton, Brentwood, Hamilton…
1918, 1957, 1968…
What is an acceptable disaster response?
What medical and logistical systems are needed?

4
…But
Most science of disasters is pointed at
estimating casualty numbers, not at what to
do once those casualties appear on your
doorstep

5
Outline
• Dispatching Problem
• Methodology
– MIP
– Simulation
• An Example Scenario
– Description
– A MIP based Greedy-Heuristic
– Visualization and Analysis of Results

6
Mass Casualty Incident (MCI)
• A MCI is an event which causes multiple casualties, and will strain the resources of the local healthcare system
• At the site of a MCI, victims await medical treatment and transportation to hospital facilities
• In a MCI, there is a limited number of ambulances available to transport patients to hospitals, requiring ambulances to make multiple trips from site to hospital
• Hospitals have different characteristics, including:
– number of beds; patient throughput; distances, etc

7
The Dispatching Question
• Where do we send the patients in order
to minimize the amount of time it takes to
treat them all?
transportation + waiting + treatment

8
Related Questions
• Which hospitals should be included in
the response?
• Where should ambulances transport the
casualties?
• How many casualties should be
transported to each hospital?

9
Hospitals Decision Tradeoffs
• Taking patients to nearby hospitals reduces the demand on ambulance time, however, it increases the burden that nearby hospitals must bear
• Taking patients to remote hospitals increases demand for ambulance time, but spreads out demand for hospital services more evenly

10
Why is the
Dispatching Question Important?
1. Improved patient outcomes
2. Effective use of resources
3. Difficult to correct dispatching errors
after the fact
4. Determine which hospitals should be
used in a response

11
1. Improved Patient Outcomes
• Patient outcomes suffer when patients are transported to the incorrect hospital
– Patients should be treated to the facility most capable of providing the type of care they need
– Longer delay to treatment time leads to a higher mortality rate

12
2. Effective Use of Resources
• Resources are wasted when patients are
transported to the incorrect hospital
– Available resources at other hospitals
wasted
– During 9/11, uptown hospitals had an
abundance of staff on call and available space,
while downtown hospitals were overwhelmed
– Patients must be re-transported, which
wastes ambulance and paramedic time

13
3. After the Fact Difficulties
• It may be difficult to “fix” incorrect patient
routing decisions after the fact
– Once patients are transported to a hospital, it may
be difficult to re-transport them
– They may need immediate medical care, and cannot wait
for re-transport
– There may be legal restrictions requiring the hospital to
treat them

14
4. Determine which Hospitals
should be Used in a Response
• Hospitals a large distance from the disaster site may have available capacity, but is the long transportation time worth it?
– Which hospitals should respond to a MCI of a given size?
– Which hospitals are too far away to help?

15
Dispatching Today
• Currently, dispatching is handled manually
by trained dispatchers
• Dispatching skill comes from experience
• Personal connections between the
dispatcher and officials at local hospitals
are important

16
Our Goals
• Develop quantitative models of
ambulance dispatching which can
determine optimal ambulance routings
• Distill heuristics from the results of the
model which can assist dispatch
decisions during an MCI

17
Methodology
• Formulate and solve the routing problem as a
Mixed Integer Program (MIP)
– Using Xpress-Mosel
• Build a simulation model in order to verify the
results
– Using Arena
• Develop a visualization tool to analyze,
evaluate and propose “interesting” solutions
– Using Xpress-XAD

18
Proposed MIP model
• Objective is to find the minimum completion time, which includes transportation + treatment times
• Underlying problem is a
Minimum Makespan Scheduling Problem:
– Assign a set of jobs (patients) to a set of machines (ambulances+hospitals)

19
General Framework Considered
• The patients (jobs) have different treatment
(processing) times
• The patient treatment time also depends on
the hospital (machine)
• Every ambulance may return to the disaster
site a certain number of times (trips)
• Every hospital has a capacity (number of beds)

20
Problem Structure
• Two phases:
– Transportation
– Treatment
• Decisions made in the transportation phase
affect the treatment phase
– The assignment of patients first needs to consider
transportation and only after their treatment
(sequential assignment)

21
Transportation MIP Component
• Key Decision Variables:
– assign an ambulance to a patient:
assign(patient,ambulance,trip)
• Time Decision Variables:
waitTimeForTransportation(patient)
arrivalTimeToSite(ambulance,trip)

22
Treatment MIP Component
• Key Decision Variables:
– assign a patient to a hospital bed:
treatmentOrder(patient,hospital,bed)
• Time Decision Variables:
– starting time of patient treatment
startTime(bed,hospital)
– completion time of treatment
completionTime(bed,hospital)

23
Transportation and Treatment
MIP Components Integration
• Key Decision Variables:
– assign a hospital to the ambulance’s trip
flow(hospital,ambulance,trip)
• Time Decision Variables:
– time to go to the hospital in a given trip
timeToHospital(ambulance,trip)
– time to go from the hospital to the disaster site
timeFromHospital(ambulance,trip)

24
Xpress-Mosel Implementation
• Xpress-Mosel is a Language for both
Mathematical Modeling and
Programming

25
MIP Goal
• Minimize the time needed to transport
and treat all patients from the disaster
site

26
MIP is hard
• In general MIP is NP-hard
• Standard Vehicle Routing MIPs are
usually very hard to optimize, and the
optimality gap of the relaxed problems is
traditionally large

27
How can our Problem be Solved?
• Decompose the problem into smaller
MIPs
• Develop heuristic methods:
– Implement greedy, local-descent heuristics
– Implement meta-heuristics
– Use MIP to find feasible solutions
– Use MIP to improve solutions

28
We use Xpress-Optimizer for MIP
• To find starting feasible solutions
• To improve existing solutions
• To produce a guaranteed optimality gap

29
An Example Scenario
• A bombing at the New York Stock Exchange
(NYSE) in downtown Manhattan leaves 150
trauma victims in need of emergency medical care
• The city has the following resources to respond:
– 50 ambulances
– 10 available hospitals of different size located
throughout lower Manhattan

30
Treatment Facilities Considered for
NYSE Attack Scenario
Hospital Distance
(minutes) Capacity
Throughput
(patients/hour)
NEW YORK DOWNTOWN HOSPITAL 2 48 1
BELLEVUE HOSPITAL CENTER 11 370 8
BETH ISRAEL MEDICAL CENTER 10 332 6
NY EYE AND EAR 9 31 1
HOSPITAL FOR JOINT DISEASES 10 50 2
NY UNIVERSITY MEDICAL CENTER 11 212 4
NEW YORK HOSPITAL-NEW YORK 15 644 6
ST VINCENTS HOSPITAL & MEDICAL CENTER 8 45 4
ST LUKES ROOSEVELT/ROOSEVELT 16 323 5
LENOX HILL HOSPITAL 18 196 5

31
Scenario Framework
• 1 Disaster Site (NYSE)
• 150 Victims with treatment times
~normal(60,15) minutes / Hospital Throughput
• 50 Ambulances with Single Patient Capacities
– Assume that ambulances initially arrive to the disaster
site 8 min after the attack
• 10 Hospitals in Manhattan

32
NYSE Scenario MIP Statistics
• 508 860 constraints
• 361 379 variables (197 300 are binary)
• 3 313 838 non-zero elements

33
NYSE Scenario LP relaxation
• LP relaxation is 220 min
• Found using Xpress-2006B with the Barrier algorithm – CPU time was 3300 sec
– Found on – dual AMD Athlon 64bit, 4800+ 2.41 GHz CPU with 4GB RAM
Optimal completion time is greater than 3h 40m

34
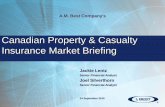
Ambulances Dispatcher
Xpress-XAD Visualization Tool

35
A MIP feasible solution
• The overall completion time is 301 min
• The average pickup time is 96 min
• Not all 50 ambulances are assigned immediately after the attack

36
MIP based Greedy-Heuristics
Implemented Using Xpress-Mosel
• Assign all patients to a given hospital – Assign first patients with smallest expected completion time
• Assign patients to a specified number of
ambulance trips – Assign first patients to hospitals which have smallest expected
hospital completion time, according to the previous patient
assignments
• Use Xpress-Optimizer to solve Reduced MIP
obtained with the previous assignments

37
A MIP based
Greedy-Heuristic solution
• The overall completion time is 262 min
• The average pickup time is 47 min
• All 50 ambulances are assigned immediately after the attack
The greedy-heuristic
solution time was found in
2200 sec in a dual Xeon
3.0 GHz 4 GB RAM.

38
Treatment Facilities Considered for
NYSE Attack Scenario
Hospital Throughput
(pt/hr)
Patients
Allocated
Waiting
Time/Patient
Completion
Time
NEW YORK DOWNTOWN HOSPITAL 1 3 51’ 207’
BELLEVUE HOSPITAL CENTER 8 30 62’ 254’
BETH ISRAEL MEDICAL CENTER 6 23 74’ 262’
NY EYE AND EAR 1 3 60’ 224’
HOSPITAL FOR JOINT DISEASES 2 7 56’ 253’
NY UNIVERSITY MEDICAL CENTER 4 14 56’ 240’
NEW YORK HOSPITAL-NEW YORK 6 21 62’ 249’
ST VINCENTS HOSPITAL & MEDICAL CENTER 4 15 74’ 253’
ST LUKES ROOSEVELT/ROOSEVELT 5 17 57’ 244’
LENOX HILL HOSPITAL 5 17 66’ 250’

39
Improving the MIP heuristic
• Use Local-Search heuristics
• Use Reduced MIP Search
• The initial solution is probably within 5-to-10 min of being optimal
****************************** Beth Israel Medical Center ******************************
Patient 21 arrived at 28 waited 0 and finish at 38.9127(10.9127)
Patient 25 arrived at 28 waited 10.9127 and finish at 48.533(9.62032)
Patient 27 arrived at 28 waited 20.533 and finish at 64.8155(16.2825)
Patient 36 arrived at 28 waited 36.8155 and finish at 74.9802(10.1646)
Patient 40 arrived at 28 waited 46.9802 and finish at 86.4991(11.5189)
Patient 16 arrived at 28 waited 58.4991 and finish at 97.5059(11.0067)
Patient 43 arrived at 54 waited 43.5059 and finish at 109.702(12.1965)
Patient 85 arrived at 56 waited 53.7023 and finish at 118.856(9.15339)
Patient 71 arrived at 58 waited 60.8557 and finish at 131.901(13.0454)
Patient 86 arrived at 60 waited 71.9012 and finish at 141.893(9.99153)
Patient 77 arrived at 68 waited 73.8927 and finish at 150.167(8.27402)
Patient 60 arrived at 70 waited 80.1667 and finish at 163.536(13.3689)
Patient 47 arrived at 74 waited 89.5356 and finish at 173.336(9.79992)
Patient 137 arrived at 86 waited 87.3355 and finish at 177.917(4.58128)
Patient 90 arrived at 88 waited 89.9168 and finish at 186.698(8.78111)
Patient 129 arrived at 88 waited 98.6979 and finish at 193.457(6.75863)
Patient 111 arrived at 88 waited 105.457 and finish at 204.848(11.3916)
Patient 140 arrived at 96 waited 108.848 and finish at 212.415(7.56672)
Patient 132 arrived at 100 waited 112.415 and finish at 217.704(5.28914)
Patient 148 arrived at 104 waited 113.704 and finish at 228.242(10.5379)
Patient 92 arrived at 116 waited 112.242 and finish at 240.188(11.946)
Patient 101 arrived at 116 waited 124.188 and finish at 248.046(7.85816)
Patient 94 arrived at 146 waited 102.046 and finish at 262.156(14.1099)
Hospital 3 completion time is after 262.156 minutes
the total waiting time in the ER is 1702.15 minutes
and the number of patients allocated to it is 23

40
Conclusions • MIP model is highly adaptable to different scenarios
– Simultaneous attacks; non-homogeneous transporters; introducing priority patients according to their condition, etc
• MIP based greedy-heuristics provide good starting feasible solutions – Alternative heuristics can easily be tested/programmed using
Xpress-Mosel
• The Ambulances Dispatcher Xpress-XAD Visualization Tool is very helpful in planning, detecting bottlenecks and possible improvements, and in demonstrating the value of the MIP model to the dispatchers and officials