
Opioid free Emergency Department?
21
Opioids Free ED Hassan Zahoor
-
Upload
scgh-ed-cme -
Category
Health & Medicine
-
view
167 -
download
0
Transcript of Opioid free Emergency Department?
Opioids Free ED
Hassan Zahoor

Concept Of Opiate Free Ed
Dr Sergey Motov MD, with particular interest in Pain management in ED, ran ED shift without prescribing single opiate as part of research work, also and website painfree.com with lectures and resources.
Swedish Ed physicians in most medical centres have taken initiative of oxy fee ED based on risks associated with opiates prescription
2

Areas To Cover
Concept and rationale of opiate free ED: Why do we need alternatives to opioids in ED
Different analgesic options depending upon patient population
Choosing right opioids if you have to

Need Of Alternative to Opiates ( Problems with opiate prescribing)
1. Severe Side effects esp. elderly patients
http://www.ncbi.nlm.nih.gov/pubmed/24033733

2. Addiction and Misuse ( non medical use)
Clear Evidence of overdose, injection related harms, and dependance
Data from the United States FDA Adverse Event Reporting System shows that oxycodone contributed to the largest number (5548) of all drug-related deaths in North America during the period 1998 to 2005 (morphine ranked fourth, contributing to 1616 deaths).11
In another study investigating North American accidental pharmaceutical overdose deaths, non-medical use of pharmaceuticals was involved in 63%.
http://www.ncbi.nlm.nih.gov/pubmed/24629443

3. No consensus on optimum opioid doses (weight-based, fixed, nurse initiated?)
http://www.ncbi.nlm.nih.gov/pubmed/20825766
4. Poor Titration Practices
http://www.ncbi.nlm.nih.gov/pubmed/21908134

5. Regulatory Concerns of prescribing opiates? Concerns from AHPRA? only consultants will be authorised to prescribe oxycodone.

Pain Team at SCGH
Acute pain service will support any measures to reduce oxycodone prescription in this hospital, as it is too addictive, and there are equally efficacious analgesics which do not cause social carnage and hyperalgesic consequences.
Focus is on avoiding oxycodone prescribing except in elderly people.

Practical Consideration
Dual/tripple analgesia combination
Different classes of analgesia together provide synergistic effect
small doses of each agent result in decreased potential of adverse effects
less sedation, early mobilisation and decreased LOS with opioid free analgesia
Multimodal Receptor Targeted analgesiaNSAIDS COX1-2 eg celecoxib, naproxen, meloxicam
NMDA receptors eg ketamine, NO
Central Ca receptors eg pregabalin, gabapentin
Less Addictive opioids
Alpha 2 central agonists eg clonidine
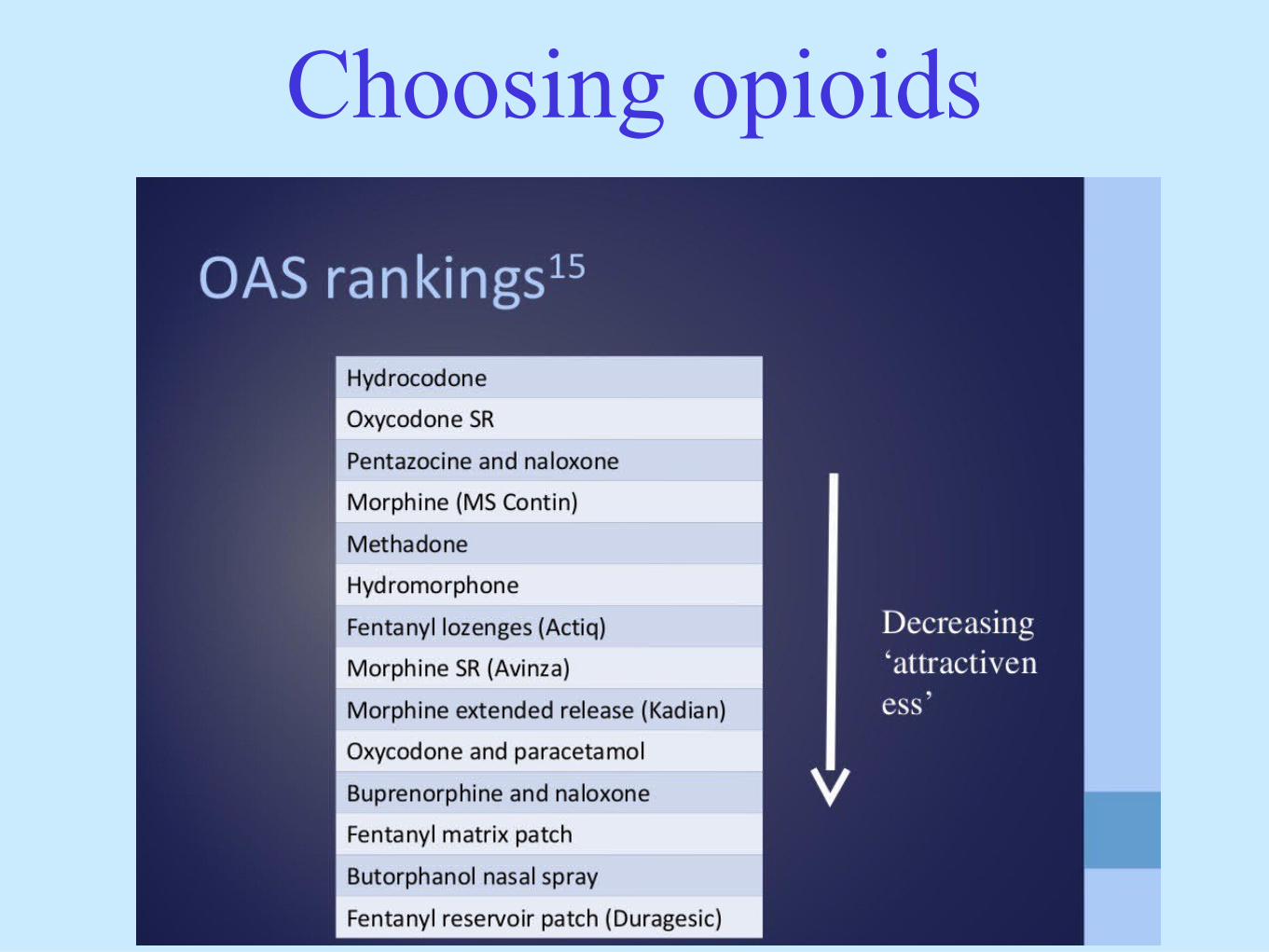
Choosing opioids


What options we have
Tramadol :
Centrally acting , atypical opioid analgesic
Serotinine and NA reuptake inhibitor
Active metabolites similar to opioids
Oral or IV 50-100 mg 4/24 PRN

BuprenorphinePartial Mu opioid agonist ( Ceiling Effect)
High receptor affinity
SL route, transdermal patch onset 12-24 hours
Minimal gut effect
Primary site of action is spine not brain, less
abuse potential
Gabapentinoids
Inhibit presynaptic ca channels
Also inhibit NMDA receptors
Modulate pain and inhibit central sensitisation
Antihyperalgesic
Reduce opioid requirements
Gabapentinoids
Reduce opioids side effects
Reduce post operative ch pain by 50-90 percent
No pharmacokinetic drug interactions
Not lethal in overdose
Easily dialiasable
22 years old male, BIBA , involved in motor bike accident, sustaining right open tib-fib fracture, splinted by SJA. haemodynamically stable, nil active bleeding, crying with pain. What will you give??or what have you used in past??
http://www.ncbi.nlm.nih.gov/pubmed/25197290
http://www.ncbi.nlm.nih.gov/pubmed/23602757
http://www.ncbi.nlm.nih.gov/pubmed/23041484
45 years old male, presented to Ed with left sided renal colicky pain, previous h/o same side kidney stone, pain feels the same. What will you use??/what have you used in past??? What will you give on discharge??
http://www.ncbi.nlm.nih.gov/pubmed/25197573
http://www.ncbi.nlm.nih.gov/pubmed
/24381620
50 year old female, known ch back pain , recent acute exacerbation with radiculopathy signs left side , nil motor weakness or red flags, nil infection or tumor signs. What are the options??or what have you used in past?? What will you give on discharge??
http://www.ncbi.nlm.nih.gov/pubmed/25682273


















