
Operative dentistry Motamiz OPRD 41 LECTURES lecture 3 WED ...
40
Operative dentistry Motamiz OPRD 41 LECTURES lecture 3 WED 1-4-2020
Transcript of Operative dentistry Motamiz OPRD 41 LECTURES lecture 3 WED ...

Operative dentistry Motamiz OPRD 41
LECTURES lecture 3
WED 1-4-2020
Care of gingival tissues

the Chapter of Objectives
The student will be able to recognize:
(1) Types of irritating factors affecting
the periodontium.
(2) Methods of gingival retraction.
(3) Steps of gingival retraction.

-Restorations must be not only compatible with
the pulp-dentin organ, but also with the periodontium.
-Physiologically, the periodontium considered as
one organ, composed of gingiva, dento-gingival
attachment, periodontal ligaments and alveolar
bone.

If foreign body is forced in normal gingival crevice, it regains its
shape and dimensions once the foreign body is removed. However, if
this space is violated by a foreign body for a long period of time, it
will not regain its shape

Normal gingiva
Diseased gingiva
If the interdental col area inflamed as a
result of operative procedure and this
inflammation did not resolved, pocket
formation and marginal periodontitis
will happen.
periodontium the to factors Irritating
Caries Teeth separation Rubber dam application Cavity preparation Matricing Gingival retraction Impression procedures Temporary restorations Permanent restorations

1- Caries
Surface roughness will enhances plaque
accumulation which increased with
advanced cavitation of the teeth.
The condition ranges from gingivitis to
marginal periodontitis, depending on the
severity of tooth destruction.

2- Teeth separation
Tooth separation by wedges
Tooth separation by elastic separators
prolonged separation can cause irreversible ischemia to
the periodontal ligament blood vessels.

3- Rubber dam application
-Unsuitable clamp or incorrect clamp
application. -If the dental floss used to seat the
rubber dam is pushed forcibly against
the periodontal tissues. - If the floss used as ligature → lacerates entrapped gingiva.

4- Cavity preparation
Gingival laceration due to cavosurface
margin preparation
Prepared proximal box
with injured adjacent
gingival tissues
Vibration due rotary inst. During C. P is the most irritating
factor to the periodontium → laceration of PDL
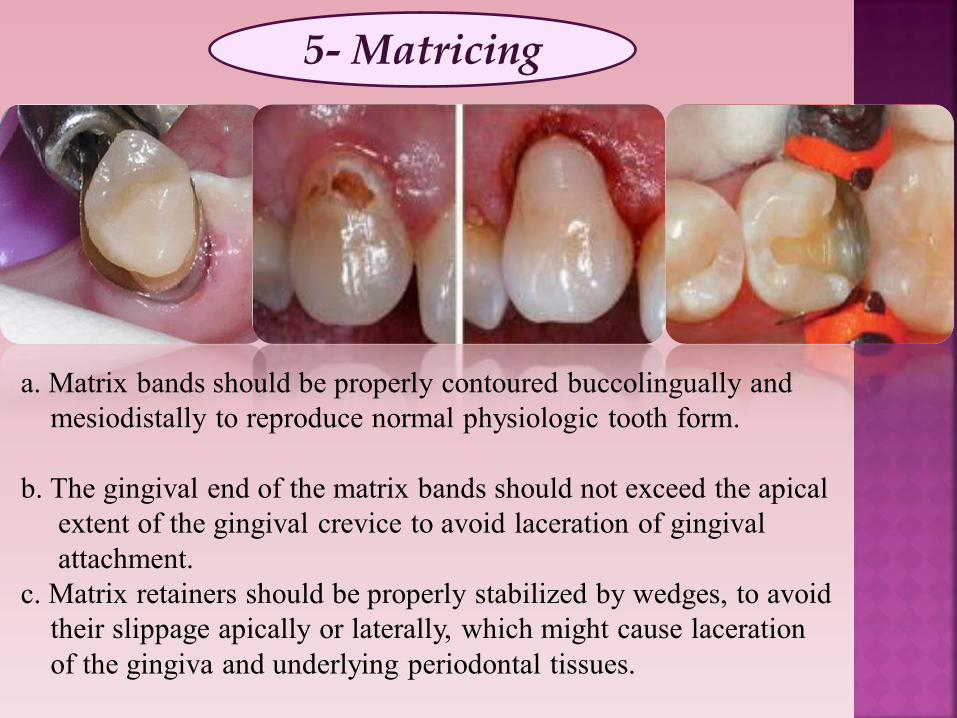
5- Matricing
a. Matrix bands should be properly contoured buccolingually and
mesiodistally to reproduce normal physiologic tooth form. b. The gingival end of the matrix bands should not exceed the apical extent of the gingival crevice to avoid laceration of gingival attachment. c. Matrix retainers should be properly stabilized by wedges, to avoid
their slippage apically or laterally, which might cause laceration
of the gingiva and underlying periodontal tissues.

6- Gingival retraction
A diagram showing the correct position of the gingival retraction cord
-Cause physical trauma if pushed
beyond the apical extent of the
gingival crevice,
-Constricting chemicals may cause
gingival inflammation with slight
gingival recession

7- Impression procedure
a. Mechanical trauma caused by insertion and
removal of impression materials. b. Catalysts and chemical by-products of rubber
elastomeric impression materials can cause allergic
reactions.

8- Temporary restorations
a. Mechanical trauma and gingival irritation from temporary
restoration try-in, adjustment, cementation and removal. b. Irritating qualities of the cementing medium. c. Excessive residual monomer of resinous temporary
restorations

9- Permanent restorations
Narrow contact Broad contact
vertical food impaction will
occur.
pressure on the interdental col
area and change its anatomy
Restorations made with open contact, not only result in food
stagnation interproximally, but also lead to disruption of the
anterior component of forces which subsequently cause
mesial drifting of teeth.

9- Permanent restorations
Improper occlusal anatomy Improper facial contour
vertical loading on the
periodontium as a
result of high spots
and/or over eruption of
the opposing teeth.
- Over contoured facial and lingual
surfaces deprive gingival tissues from healthy
massaging and stimulating effect of food
deflection, leading to gingival atrophy and
abrasion.
- Under contoured facial and lingual
surfaces encourage food stagnation
and plaque accumulation

9.2- Surface finish of the restorations
Improper surface finish Proper surface finish
-No restoration available which can duplicate the surface
glaze of tooth enamel. -Rough surfaced restorations result in gingival irritation due
to bacterial irritation as a result of plaque accumulation

9.3. Marginal discrepancies
Overhanging margins with Pocket formation
Marginal overhangs and underhangs, in proximity to
the gingival tissues, will harbor bacterial plaque
especially if they are located subgingivally, where
natural and artificial cleansing is difficult.
9.4. Chemical make up of
R.M.
-There are inherent irritating ingredients in the
restorative materials that could participate in
periodontal breakdown:- e.g. Mercury and corrosion products in amalgam - Acid etchants and residual monomers in resin based
tooth colored restorations.

Methods of gingival retraction
1. Physico-mechanical methods
2. Chemical methods
3. Electrosurgical methods
4. Surgical methods

1. Physicomechanical methods:
Gingival retraction cord
Gingival retraction paste Custom made Temporary restoration
2. Chemical methods Chemicals are applied in retraction cords or soft loose cotton rolls or cotton pellets. a. Vasoconstrictors to decreasing hemorrhage. b. Fluid coagulants such as 100% alum, 25% aluminum chloride, 10% aluminum potassium sulphate. They coagulate blood and tissue fluids.

3. Electrosurgical methods
The localized electric energy induces tissue changes and creates surface coagulation of tissues, fluids and oozed blood.

4. Surgical methods It is a process by which the unneeded gingival tissues are surgically removed in the same manner as in periodontal surgery.

Fate of the periodontium: We cannot avoid some gingival irritation which is
reparable and reversible dependent on the following factors:
1. The preoperative condition of the gingiva. 2. The nature of the operative and restorative procedures. 3. Proximity of restoration margins to the gingiva. 4.The restoration form (contact, contour and occlusal
anatomy). 5. Post-restorative healing environment (plaque control measures).

7Evaluation sheet no
1- Mention 3 factors cause gingival irritation?
1- Mention 2 methods of gingival retraction?


CHAPTER 5:
Care of Gingival Tissues
Chapter outline
Irritating factors to the periodontium
Caries
Teeth separation
Rubber dam application
Cavity preparation
Matricing
Gingival retraction
Impression procedures
Temporary restorations
Permanent restorations
Methods of gingival retraction
Physico-mechanical methods
Chemical methods
Electrosurgical methods
Surgical methods
Fate of the periodontium

-2-
Objective of Chapter (5)
In the end of this chapter, the student will be able to
recognize:
(1) Types of irritating factors affecting the periodontium.
(2) Methods of gingival retraction.
(3) Steps of gingival retraction.

-3-
Restorations must be not only compatible with the
pulp-dentin organ, but also with the periodontium.
Destroyed pulp tissues can be replaced using inert filling
materials; yet destroyed periodontal tissues cannot be
replaced. Physiologically, the periodontium considered as
one organ, composed of gingiva, dento-gingival
attachment, periodontal ligaments and alveolar bone. Any
irritation affecting one of these components will be
followed by a reaction in the rest of the components.
The normal free gingival margin has a knife-edge
relationship to the facial and lingual surfaces of teeth. This
knife-edge relationship discourages food and plaque
accumulation in these areas. Any inflammation in the
gingiva will render it edematous, and will predispose to
food and plaque accumulation.
If foreign body is forced in normal gingival crevice,
it regains its shape and dimensions once the foreign body is
removed. However, if this space is violated by a foreign
-4-
body for a long period of time, it will not regain its shape.
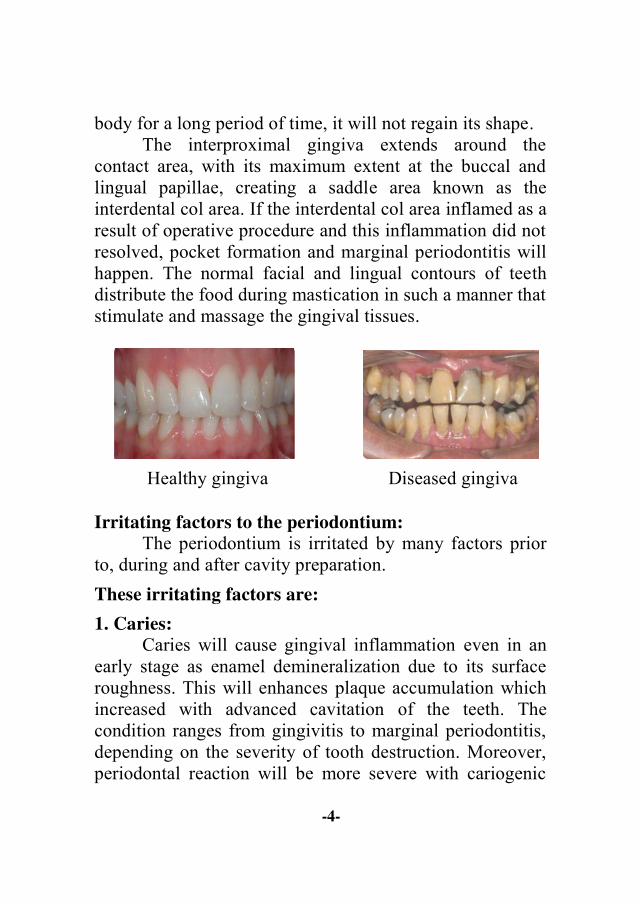
The interproximal gingiva extends around the
contact area, with its maximum extent at the buccal and
lingual papillae, creating a saddle area known as the
interdental col area. If the interdental col area inflamed as a
result of operative procedure and this inflammation did not
resolved, pocket formation and marginal periodontitis will
happen. The normal facial and lingual contours of teeth
distribute the food during mastication in such a manner that
stimulate and massage the gingival tissues.
Healthy gingiva Diseased gingiva
Irritating factors to the periodontium:
The periodontium is irritated by many factors prior
to, during and after cavity preparation.
These irritating factors are:
1. Caries:
Caries will cause gingival inflammation even in an
early stage as enamel demineralization due to its surface
roughness. This will enhances plaque accumulation which
increased with advanced cavitation of the teeth. The
condition ranges from gingivitis to marginal periodontitis,
depending on the severity of tooth destruction. Moreover,
periodontal reaction will be more severe with cariogenic

-5-
loss of contact and contour.
2. Teeth separation:
Teeth separation for examination or accessibility
could irritate the periodontium. If
teeth separation exceeded the
periodontal ligament space (0.2 - 0.5
mm), the periodontal ligaments will
be compressed on one side of the
teeth and torn on the other side.
Moreover, prolonged separation can
cause irreversible ischemia to the periodontal ligament
blood vessels.
3. Rubber dam application:
Rubber dam could be hazardous to the gingiva and
the periodontal ligaments. Many factors can traumatize
gingival tissues during rubber dam application as the use of
unsuitable clamp or incorrect clamp application. In
addition, if the dental floss used to seat the rubber dam is
pushed forcibly against the periodontal tissues and finally
if the floss used as a ligature strangulates or lacerates
entrapped gingiva.

-6-
4. Cavity preparation:
a. Vibration due to rotary instrumentation is the most
irritating factor to the periodontium. It can lead to
laceration of the periodontal ligament fibers.
b. Preparation of proximal portion of any tooth can
usually cause injury to the adjacent gingival tissues.
The gingival tissues can be protected by preserving
the proximal plate of enamel during gross cavity
preparation. Also placement of wedges
interproximally will protect the underlying
periodontium from mechanical trauma by
instrumentation.
c. Preparation of the gingival cavosurface margins can
cause laceration of the gingival tissues.
5. Matricing:
a. Matrix bands should be properly contoured
buccolingually and mesiodistally to reproduce
normal physiologic tooth form.
b. The gingival end of the matrix bands should not
exceed the apical extent of the
gingival crevice to avoid
laceration of gingival
attachment.
c. Matrix retainers should be
properly stabilized by wedges,
to avoid their slippage apically
or laterally, which might cause laceration of the
gingiva and underlying periodontal tissues.

-7-
6. Gingival retraction:
Gingival retraction procedures are designed to control
the peripheral components of the periodontium prior to
impression procedures. Some destruction could happen if:
a. Gingival retraction cords can cause physical trauma
if pushed beyond the apical extent of the gingival
crevice, or if they strangulated gingival tissues
against the tooth surface. Gingival laceration may
occur which may be followed by alveolar bone
resorption.
b. Constricting chemicals may cause gingival
inflammation with slight gingival recession. In
severe cases, acute inflammation may occur with
considerable gingival recession.
7. Impression procedures:
The periodontium could be affected by impression
procedures and materials as a result of:
a. Mechanical trauma caused by insertion and removal
of impression materials.
b. Catalysts and chemical by-products of rubber
elastomeric impression materials can cause allergic
reactions.

-8-
8. Temporary restorations:
These restorations and their fabrication could be traumatic
as a result of:
a. Mechanical trauma and
gingival irritation from
temporary restoration try-in,
adjustment, cementation and
removal.
b. Irritating qualities of the cementing medium.
c. Excessive residual monomer of resinous temporary
restorations.
9. Permanent restorations:
9.1 . Anatomy of permanent restorations:
Final restorations should properly restore contact, contour
and occlusal anatomy.
a. Under contoured facial and lingual surfaces
encourage food stagnation and plaque accumulation.
b. Over contoured facial and lingual surfaces deprive
gingival tissues from healthy massaging and
stimulating effect of food deflection, leading to
gingival atrophy and abrasion.
c. Restorations made with open contact, not only result
in food stagnation interproximally, but also lead to
disruption of the anterior component of forces which
subsequently cause mesial drifting of teeth.
d. Restorations made with too broad proximal contact
will cause pressure on the interdental col area and
change its anatomy.
e. If the contact areas are made too narrow, vertical
food impaction will occur.

-9-
f. Restorations made with defective occlusal anatomy
will cause either vertical loading on the periodontium
as a result of high spots and/or overeruption of the
opposing teeth.
9.2. The surface finish of the restorations:
There is no restoration available which can duplicate
the surface glaze of tooth enamel. Rough surfaced
restorations result in gingival irritation due to bacterial
irritation as a result of plaque accumulation.
9.3. Marginal discrepancies:
Marginal overhangs and
underhangs, in proximity to the
gingival tissues, will harbor
bacterial plaque especially if they
are located subgingivally, where
natural and artificial cleansing is
difficult.
9.4. Chemical make-up of the restorative materials:
There are inherent irritating ingredients in the
restorative materials that could predispose or participate in
periodontal breakdown. These irritating ingredients are e.g.
mercury and corrosion products of amalgam, acid etchants
as well as residual monomer in resin based tooth-colored
restoratives.
Methods of gingival retraction:
1. Physico-mechanical methods:
The gingiva is forced away from the tooth surface,
laterally and apically. Usually one of three techniques is

-10-
used:
a. Custom made temporary restorations with bulky
temporary cements like ZOE results in gingival
retraction after 24 hours.
b. Rolled cotton or synthetic cords are forced into the
gingival sulcus which results in gingival retraction
within 30 minutes.
c. Heavy weight rubber dam with proper interseptal
dimensions produces an immediate effect.
2. Chemical methods:
Chemicals are carried out to the field of operation in
cords or soft loose cotton rolls or cotton pellets. Chemicals
used are either:
a. Vasoconstrictors that decrease the size of blood
capillaries, thus decreasing hemorrhage, tissue fluid
seepage and consequently the size of the free
gingiva.
b. Fluid coagulants such as 100% alum, 25% aluminum
chloride and 10% aluminum potassium sulphate.
They coagulate blood and tissue fluids locally,
creating a surface layer that is sealant against blood
and crevicular fluid seepage.
Steps of gingival retraction: Use of well compacted woven cords, or drawn cotton
rolls. Measure the tooth diameter before cutting the cord. Start packing from one end of the cord going to the
other end. The packing tools should be blunt. Apply steady static load directed apically and
slightly towards the tooth Surface to preserve

-11-
periodontal attachment. Remove the packed retraction cord in the presence of
moisture to act as a lubricant. After completion of the impression procedure or the
direct wax pattern, remove the remaining packed items and curette the field to create a healthy blood clot for healing.
For assuring healthy healing, adequate temporary restoration and efficient plaque control measures should be carried out.
3. Electrosurgical methods:
Alternating electric current will
be used for gingival retraction.
Electric current pass through human
body without inducing shocks. The
localized energy induces tissue
changes limited to the superficial 2-3
cell layers. It creates surface
coagulation of tissues, their fluids and oozed blood results
in physical removal of the gingival tissues.
4. Surgical methods:
It is a process by which the unneeded gingival
tissues are surgically removed in the same manner as in
periodontal surgery. Apical repositioning of the periodontal
attaching apparatus is performed to create a healthy
gingiva that can be safely and easily retracted by one or
more of the above mentioned methods.
-12-
Fate of the periodontium:
The most meticulous operator cannot avoid some
irritation to the periodontium. However, such irritation is
repairable and reversible depending on the following
factors: 1. The preoperative condition of the gingiva (previously
healthy). 2. The nature of the operative and restorative procedures. 3. Proximity of the restoration margins to the gingiva. 4. The restoration form (contact, contour, and occlusal
anatomy). 5. Post-restorative healing environment (plaque control
measures).


















