

Opening Keynote Session “CIO and CMIO Dynamics: The Evolving Roles & Relationships”
29
iHT 2 January 2012 Michael Bakerman, MD, FACC, FACPE, MMM Chief Medical Informatics Officer Richard Mohnk, MSA, MT(ASCP) Associate Chief Information Officer Institute for Healthcare Technology Transformation UMass Memorial Health Care: CIO and CMIO Partnerships
-
Upload
health-it-conference-iht2 -
Category
Education
-
view
503 -
download
1
Transcript of Opening Keynote Session “CIO and CMIO Dynamics: The Evolving Roles & Relationships”

iHT2
January 2012
Michael Bakerman, MD, FACC, FACPE, MMM
Chief Medical Informatics Officer
Richard Mohnk, MSA, MT(ASCP)
Associate Chief Information Officer
Institute for Healthcare Technology Transformation
UMass Memorial Health Care:
CIO and CMIO Partnerships

2 iHT2 January 2012
Disclosures
We have no disclosures
We have no conflicts of interest
Describe the UMass Memorial System
Define our Cornerstone Strategy
Illustrate CIO and CMIO differences and opportunities for
collaboration
Case Presentations and discussion
3 iHT2 January 2012
UMass Memorial Health Care
7 Hospital System
Clinical Partner to
UMass Medical School
13,500 employees
3,000 registered nurses
Approximately 1,600
physicians
1,111 beds
$1.4b in Annual Revenue
~60,000 inpatient visits
~1,000,000 outpatient visits

4 iHT2 January 2012
UMass Memorial Healthcare Information Technology
Cornerstone Initiatives
Fundamental Goal: Move from a predominantly paper environment to one that is predominantly electronic – Core Ambulatory EMR
– Inpatient EMR/CPOE
– Inter & Intra Enterprise Identification
– Inter & Intra Enterprise ‘Interoperability’
– Connected Healthcare Community
Improve Availability and Flow of Information
Improve Quality and Safety
Increase Efficiency and Effectiveness

5 iHT2 January 2012
Private Medical
Practice
Inpatient EMR
Outpatient Enterprise EHR
University
Memorial Hahnemann
Community
Medical Group
Clinton
Hospital
HealthAlliance
Hospital
Wing Memorial
Hospital
Marlborough
Hospital
Private Medical
Practice Private Medical
Practice / Affiliate
Hospitals
The Future State
Medical Group
5
Ambulatory EHRs
Data Integration Application

6 iHT2 January 2012
Oct/Nov/Dec
2011
Jan/Feb/Mar
2011
Apr/May/Jun
2011
Jul/Aug/Sept
2011 Jan/Feb/Mar
2012
Jan/Feb/Mar
2013
Apr/May/Jun
2012
Jul/Aug/Sep
2012
Oct/Nov/Dec
2012 Apr/May/Jun
2013
Enterprise MPI LIVE with IDX
Registration and Scheduling 8/11
Hyland OnBase LIVE at the Med Ctr,
Marlboro, Clinton and Wing
Allscripts Enterprise LIVE - continued roll-out of new CMG practices, additional functionality (Orders, Tasking, Dictation) to the hospital clinics and physician offices
90 day
reporting
period to meet
2011 Stage 1
Meaningful Use
Allscripts 11.2 Upgrade
COMPLETED
Soarian Financials scheduled Live 1/15/12
Soarian Clinicals scheduled Live 1/15/12
Picis (ORIS) scheduled Live post Soarian
dbMotion (Phase 1) LIVE 5/11
CPOE Roll Out scheduled Live 5/12
MAK Roll Out scheduled Live 3/12
Soarian WING scheduled Live Summer/Fall
2012
HealthAlliance dbMotion/Soarian
Smart Button Live
Soarian Upgrade
HealthAlliance
Enterprise MPI scheduled Live with
Med Ctr Soarian Reg 3//12
Salar LIVE Hospitalist Programs at Med Center / Clinton / /Marlboro - continued roll-out to additional hospital departments
Picis PulseCheck – ED
TBD
CORNERSTONE TIMELINE (rev 12/2011)

7 iHT2 January 2012
Prior Philosophy of Physician Behavior
7
Is this the best way to motivate highly skilled and
intelligent people?
8 iHT2 January 2012
But Why Would You Want To?
8
9 iHT2 January 2012
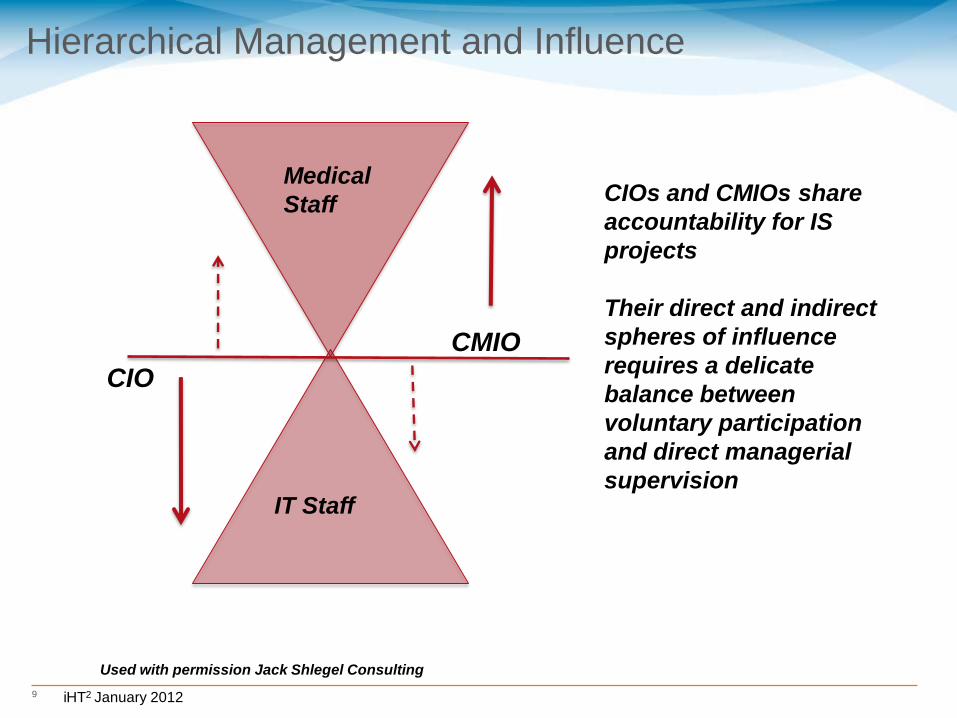
Hierarchical Management and Influence
CIO
CMIO
Medical
Staff
IT Staff
CIOs and CMIOs share
accountability for IS
projects
Their direct and indirect
spheres of influence
requires a delicate
balance between
voluntary participation
and direct managerial
supervision
Used with permission Jack Shlegel Consulting
10 iHT2 January 2012
CIO and CMIO Interactions
CMIO role is evolving
– Developed from traditional medical staff roles (CMO)
– Initially part time, but now fulltime
AMDIS 2011 Survey
– 64% are currently in first CMIO role, down from 81% in 2010
– 71% want to stay in CMIO role, 7% want to become CIO, 7% would
like to be CEO or COO and 4% would like to become CMO
– Wide range in compensation
• Largest areas range from $250,000 to $300,000 and $345,000 to $375,000
– 81% work at Integrated Health Systems, 9% work in stand alone
hospitals. Most have enterprise wide responsibilities
– Reporting structure
• 47% report to CIO
• 29% report to CMO
• 5% dually to CIO and CMO
• 19% report to CEO or COO
11 iHT2 January 2012
CMIO and CIO Can be True Partners
Extend each others influence
– Cover each others blind spots
– Let’s each do what they do best
– Teach each other
Understand the different perspectives
– Budget
– Personnel
– Project management versus clinical decisions
• Scope, resources and schedule
• Need for advocacy and accountability
Drive adoption of technology
– The journey is about adoption of technology and not simply implementation
– Understand the clinical workflow
– Know the strengths and weakness of the applications
– Work together to satisfy the end user (clinician, nurse, registration, etc)
12 iHT2 January 2012
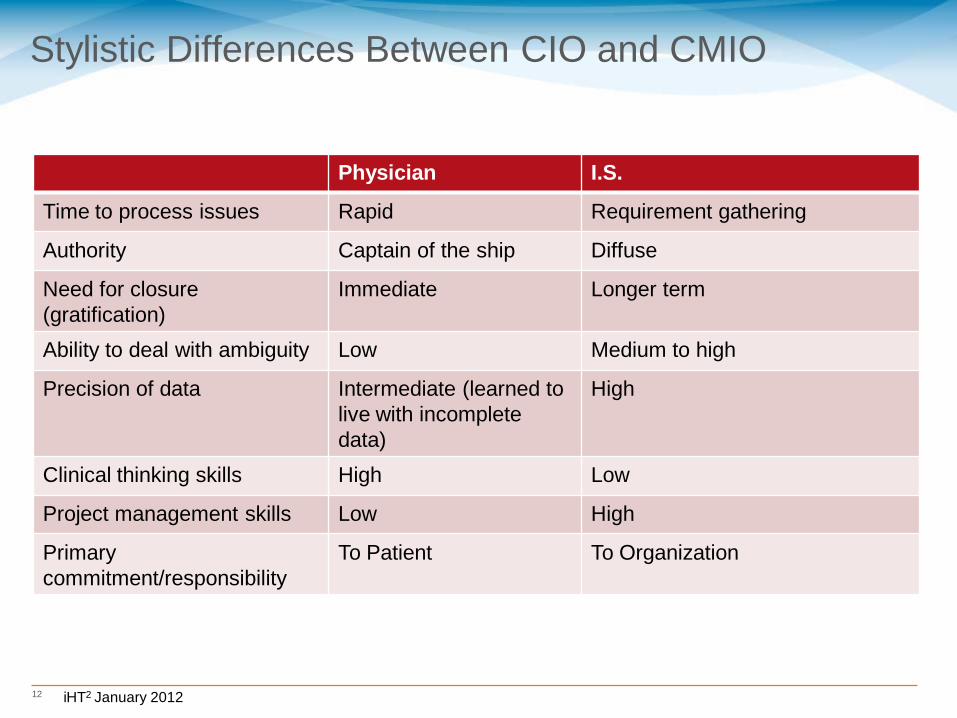
Stylistic Differences Between CIO and CMIO
Physician I.S.
Time to process issues Rapid Requirement gathering
Authority Captain of the ship Diffuse
Need for closure
(gratification)
Immediate Longer term
Ability to deal with ambiguity Low Medium to high
Precision of data Intermediate (learned to
live with incomplete
data)
High
Clinical thinking skills High Low
Project management skills Low High
Primary
commitment/responsibility
To Patient To Organization

13 iHT2 January 2012
Life is what happens between the time you plan
and execute your plan
• The roadmap is about adoption of new technology, not
implementation
• What we are discussing are clinical applications and not
IT projects
• Process change without personal growth and education is
not sustainable
• Physicians must be leaders, but must accept responsibility
and accountability

14 iHT2 January 2012
Opportunity assessment and metric definition
Set future-state goals
Model economic impact
Incorporate Benefits Realization into committee
structure
Develop implementation plans
Focus resources on improvement goals
Establish baseline measures pre-live
Conduct post-live measurement at specified intervals
Interpret results and continuously improve
performance
Planning:
Establish Metrics
and Value Goals
Implementation:
Strategy,
Resources &
Implementation
Measurement:
Baseline and Post-
live Measures
IS Can Also Drive the Management and Analysis of
Data

15 iHT2 January 2012
Case Discussion
Roll out of Follow Me Desk Top
Device Deployment Selection and plan
Development of Sign out process
Web launch point
16 iHT2 January 2012
Roll out of Follow Me Desk Top (FMD) and Single Sign On
(SSO)
Together, the CMIO and CIO develop the project principles
– Build the case and vision
• Speed, efficiency, less clicks
• Stable environment
CIO is key to listening first and then building
– Build a proof of concept to garner feedback
– Don’t just ask what is desired
– Listen to the need
– Partner and participate with the CMIO in physician meetings
CMIO is key to articulate the value to clinicians
– Ease of access
– Clinical use cases
– Test and provide constructive feedback
– Listen and brain storm approach with CIO

17 iHT2 January 2012
Web launch point for Single Sign On (SSO)
It was apparent to CIO that we could develop a communication
device as well:
– Create method to communicate
– Build ease of access
– Enhance redundancy and system reliability

19 iHT2 January 2012
Device Deployment Considerations
Perfect storm
– overlapping technology devices that can be useful,
– Variety of operational, clinical, nursing and engineering teams
involved
– Capital Planning, regulatory and environmental concerns needed to
be considered
Required to support clinical process,
– However, regulations and permit requests could be a roadblock
Each group, in isolation, had their primary concerns and needs
Required teams to live in current workflow, but think in a future
state
No matter what we choose, the technology and equipment will
continue to change
20 iHT2 January 2012
Device Deployment Guiding Principles:
Place a device in a patient room or exam room – Required to support the clinical and administrative process of
patient intake and assessment
– Should provide FTF opportunity for nursing to interview and talk with patient
Workstations on wheels (WOW) and/or fixed devices – Recommendations made by each clinical area during walkthrough
– Reviewed by IS and Capital Planning
– Approved by CMIO
– Signed off by Capital Planning
– Approved by ACNOs and IS.
Caveats – Phase 1 focused on nursing and back office
– Favor mobile workstations over fixed
– Storage and hallway traffic are important system constraints
– Built into assumption was no new construction
20
21 iHT2 January 2012
Device Deployment Guiding Principles
Devices cannot be deployed (stored) in hallways except when installed in Wall-a-roos.. – Added to hallway congestion
– Safety and regulatory issue
Power will be addressed on a case by case basis – Need to access room when patients are not there
– Optimize install process
– Certain facilities need to be prioritized for Capital Planning
Included assessment and implementation of any peripheral devices to support EMR – Printers, embossers, etc.
21

22 iHT2 January 2012
No WOWs initially
recommended. Added 6
after review. Will need to
determine storage policy
22

23 iHT2 January 2012
Recommendation Based on Nursing Device
Fairs and Analysis
Work Station on Wheels (WOW) – Clear consensus choice
– Assist with emerging and yet-unknown needs
– Alternative non-powered or laptop configurations
– Supply line economies of scale
– Local vendor support
23
24 iHT2 January 2012
Development of Sign Out process
The new EMR application did not support current workflow
– A round peg in a square hole, just will not work!
– Residents and Attending were frustrated and resisting
CMIO
– Agreed with physicians with the need to develop something different
and develop guiding principles
– Used a separate, but integrated application to satisfy the clinicians
needs
– Created the environment were IS team could work with clinicians
CIO
– Supported with resources, technology and experience
– Overcame internal resistance to change project plan
– Participated in development of solution and provided feedback
Win Win for all

25 iHT2 January 2012
Creating Sign Out (Work) Lists
The process:
Log in
Search for patient
Add the patient to a team
Click on the Sign out button
Edit the sign out fields for each individual
patient on the team

26 iHT2 January 2012
Sign Out (Work) List
Area for
Text
27 iHT2 January 2012
27
We Can Speak a Common Language
We will focus on the adoption of technology to provide information to providers
We will collaborate with providers in developing workflow automation and improvement, based on evidence based medical information
We will assist in providing performance measurements to improve care, improve efficiency and reduce harm
Our goal is to provide seamless applications that improve efficiency and provider satisfaction
Underlying consistency in our relationship
28 iHT2 January 2012
Overcoming Challenges
Pulling together
– Allow the system to act as a system
Physician leadership and engagement
– Senior leadership fully engaged
– Super users identified and supported
Work in today’s world, but think in the future world
– Communicate the vision of the ideal future state and work
towards that goal
– Avoid recreating broken and fragmented solution
Existing processes and procedures will need to be
revisited and adjusted
– Be flexible, open-minded and creative
You will be connecting parts of your system that have
never before been connected – ‘connected healthcare’
is just that – all inclusive for technology and people
– Communication, communication, communication
– Understanding of different environments of care
– One size does not fit all

Q & A / Thank You


















