Open-Bite Malocclusion1 Etiology of open-bite malocclusion 1 Karina Freitas and Rodrigo Cançado...
30
Transcript of Open-Bite Malocclusion1 Etiology of open-bite malocclusion 1 Karina Freitas and Rodrigo Cançado...



Open-Bite Malocclusion


Open-Bite MalocclusionTreatment and Stability
Edited by
Guilherme Janson
Fabrício Valarelli

This edition first published 2014 © 2014 by John Wiley & Sons, Inc.
Editorial offices: 1606 Golden Aspen Drive, Suites 103 and 104, Ames, Iowa 50010, USAThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK9600 Garsington Road, Oxford, OX4 2DQ, UK
For details of our global editorial offices, for customer services and for information about how to apply for permission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell.
Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted by Blackwell Publishing, provided that the base fee is paid directly to the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923. For those organizations that have been granted a photocopy license by CCC, a separate system of payments has been arranged. The fee codes for users of the Transactional Reporting Service are ISBN-13: 978-1-1183-3598-7/2014.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book.
The contents of this work are intended to further general scientific research, understanding, and discussion only and are not intended and should not be relied upon as recommending or promoting a specific method, diagnosis, or treatment by health science practitioners for any particular patient. The publisher and the author make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of fitness for a particular purpose. In view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. Readers should consult with a specialist where appropriate. The fact that an organization or Website is referred to in this work as a citation and/or a potential source of further information does not mean that the author or the publisher endorses the information the organization or Website may provide or recommendations it may make. Further, readers should be aware that Internet Websites listed in this work may have changed or disappeared between when this work was written and when it is read. No warranty may be created or extended by any promotional statements for this work. Neither the publisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication DataOpen-bite malocclusion: treatment and stability / edited by Guilherme Janson, Fabrício Valarelli. p. ; cm. Includes bibliographical references and index. ISBN 978-1-118-33598-7 (pbk.) I. Janson, Guilherme, editor of compilation. II. Valarelli, Fabricio, editor of compilation. [DNLM: 1. Open Bite–therapy. 2. Open Bite–etiology. 3. Orthodontics, Corrective–methods. 4. Orthognathic Surgical Procedures–methods. WU 440] RK523 617.6'43–dc23 2013029969
A catalogue record for this book is available from the British Library.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available in electronic books.
Cover image: main image © tshortellCover design by Nicole Teut
Set in 9.5/12 pt Palatino LT Std by Toppan Best-set Premedia Limited
1 2014

To my parents:My father, Waldyr A. Janson, who motivated me to follow in the
same profession and provided me with an excellent example.My mother, Déborah R.P. Janson, who dedicated her heart to the
family supporting us in every situation.—Guilherme Janson


Contents
List of Contributors xi
Foreword xiiiAngelos Metaxas
Foreword xvGreg J. Huang
Preface xvii
Acknowledgments xix
1 Etiology of open-bite malocclusion 1Karina Freitas and Rodrigo Cançado
Environmental factors 2Deleterious habits 2
Pacifier and thumb-sucking 2Anterior tongue posture and tongue thrust 7
Mouth breathing 9Upper respiratory obstacles 9Lower respiratory obstacles 13
Traumatisms 16Genetic factors 16
Growth pattern 16Pathologies 17
Craniofacial anomalies 17References 18
2 Open-bite treatment in the deciduous and mixed dentitions 23Guilherme Janson and Fabrício Valarelli
Overbite measurement 24Treatment in the deciduous dentition 25
vii

viii Contents
Treatment in the mixed dentition 30Open bite associated with different types of malocclusions 37
Open-bite and Class I malocclusions 37Open bite associated to Class II and III malocclusions 73Open-bite and Class II malocclusions 75Open-bite and Class III malocclusions 121
Treatment stability in the deciduous and mixed dentitions 124References 126
3 Open-bite treatment in the permanent dentition 129Guilherme Janson and Fabrício Valarelli
Differential diagnosis 129Open-bite nonextraction treatment 130
Usual clinical procedures 131Additional procedures during treatment to aid in
open-bite closure 138Mesial angulation of the attachments 138Association of tongue crib or spurs during treatment 139Reversing and accentuating the curve of Spee 141
Clinical cases 141Class I malocclusions 143Class II malocclusions 164Class III malocclusions 197
Stability of nonextraction open-bite treatment 214Open-bite treatment with extractions 231
Clinical cases 233Class I malocclusions 233Class II malocclusions 249Molar extractions 283
Stability of extraction open-bite treatment 299Stability of extraction versus nonextraction open-bite treatment 313
Treatment of open bite with occlusal adjustment 317Clinical procedure 317Patient selection 320Cephalometric changes expected with the procedure 320Functional occlusion changes 322Dentinal sensitivity 324Clinical considerations 324Stability of open-bite treatment with occlusal adjustment 328
Open-bite treatment and root resorption 331Clinical implications 339
References 339
4 Open-bite correction with posterior teeth intrusion 349Sérgio Barros and Daniela Garib
Introduction 349Types of skeletal anchorage for open-bite correction 351

Contents ix
Skeletal anchorage positioning for molar intrusion 352Molar intrusion mechanics with skeletal anchorage 354Dentoskeletal effects of molar intrusion for open-bite closure 361Open-bite correction with skeletal anchorage,
conventional mechanics, and orthognathic surgery: a critical analysis 366Clinical cases 368
Stability of anterior open-bite treatment by posterior teeth intrusion 377Clinical cases 384
References 397
5 Orthodontic-surgical treatment of anterior open bite 403Eduardo Sant’ana, Marcos Janson, and Roberto Bombonatti
Combined orthodontic-surgical treatment of skeletal anterior open bite 403
Orthodontic-surgical preparation to correct skeletal anterior open bite 404Diagnosis of skeletal anterior open bite 404Stages of combined orthodontic-surgical treatment 406
Treatment planning 406Orthodontic treatment 408Presurgical impression and revaluation of dental positioning 411Presurgical records and definite treatment planning 411Plaster model surgery and construction of an
intermediary splint 411Orthognathic surgery 411Bracket rebonding, finishing procedures,
and appliance removal 414Retention and final records 414
Stability of orthodontic-surgical anterior open-bite correction 433References 436
Index 439

List of Contributors
Editors
Guilherme JansonProfessorBauru Dental SchoolUniversity of São PauloBauru, São Paulo, Brazil
Fabrício ValarelliAssociate ProfessorIngá Dental SchoolMaringá, Paraná, Brazil
Contributors
Sérgio BarrosAssociate ProfessorOrthodonticsDental School of the Federal University of Rio Grande do SulPorto Alegre, Rio Grande do Sul, Brazil
Roberto BombonattiAssistant ProfessorOrthodonticsState University of West ParanáCascavel, Paraná, Brazil
Rodrigo CançadoAssociate ProfessorOrthodonticsIngá Dental SchoolMaringá, Paraná, Brazil
xi

xii List of Contributors
Karina FreitasAssociate ProfessorOrthodonticsIngá Dental SchoolMaringá, Paraná, Brazil
Daniela GaribAssociate ProfessorOrthodonticsBauru Dental School—University of São PauloBauru, São Paulo, Brazil
Greg J. HuangProfessor and ChairDepartment of OrthodonticsUniversity of WashingtonSeattle, WashingtonUSA
Marcos JansonPrivate PracticeBauru, São Paulo, Brazil
Angelos MetaxasAssociate ProfessorDepartment of OrthodonticsFaculty of DentistryUniversity of TorontoToronto, Canada
Eduardo Sant’anaAssociate ProfessorOral SurgeryBauru Dental School—University of São PauloBauru, São Paulo, Brazil

Foreword
Open bite malocclusions are one of the most difficult and challenging orthodontic conditions to properly diagnose, effectively treat, and success-fully retain. At the same time, since the anterior teeth define the smile, which is the first facial feature that draws attention, anterior open bite problems tend to be one of the most disturbing malocclusions for patients aesthetically as well as functionally.
The multifactorial etiology of these orthodontic problems involving skeletal, environmental/neuromuscular, and/or dentoalveolar compo-nents requires adequate diagnostic and treatment knowledge and experi-ence together with the understanding that these malocclusions demand continuous and persistent monitoring during retention since stability is frequently a challenge to achieve. Furthermore, the common involvement of the tongue, which is one of the most difficult soft tissues to modify in size or posture, in these types of malocclusions creates an even greater challenge and concern for any orthodontic clinician or researcher.
This textbook on open bite malocclusions by Dr. Janson and his col-leagues is an oasis in the middle of confusion, frustration, and misunder-standing. Not so much because it provides all the answers to this complicated orthodontic condition but rather because it helps the reader’s understanding with a clear, crisp, and concise explanation of the etiologic factors, supported by a large number of case studies treated with a multi-plicity of therapeutic approaches and at various developmental stages. Each chapter is properly and sufficiently organized and presented; however, the core of the textbook is Chapters 2 and 3, by Drs. Janson and Valarelli. These two chapters cover essentially 90% of most open bite malocclusions treated without surgical intervention by most practitioners from the decid-uous to the permanent dentition. Factors such as type of malocclusion, age of patient, extraction versus nonextraction approach, benefits of occlusal adjustment, and root resorption associated with open bites are thoroughly presented and well documented.
It has definitely been a privilege to write a foreword for this excellent book. Dr Janson’s exposure to university and academic teaching for such a long time has provided him with a large pool of patients with this type
xiii

xiv Foreword
of malocclusion. His findings and experience, together with an extensive list of references in each of the five chapters, will be very helpful to any clinician, researcher, or student involved with these type of malocclusions. I am not aware of another textbook that has put together such an extensive, well-documented, and well-presented collection of clinical information on this topic. I very much hope that it will be recognized by the orthodontic community and will be an important addition to every orthodontist’s or university’s library.
Angelos Metaxas

Foreword
For teeth to function and be useful, they must touch the opposing teeth. Fortunately, in humans, this is largely the norm. However, in about 3% of the population, the eruption of incisors is altered, and the upper and lower incisors cannot touch each other. These anterior open-bite malocclusions have challenged the orthodontic profession for decades, and orthodontists have searched mightily for answers regarding etiology, treatment, and stability. Hundreds, maybe thousands, of papers have been written regard-ing the treatment of open-bite malocclusions. However, with all the research, techniques, and experience that orthodontists have amassed, these malocclusions continue to prove very difficult to correct and maintain.
In this landmark textbook, Dr. Janson and his colleagues have assem-bled all the latest evidence on the topic of open-bite malocclusions. From etiology to treatment to retention, the comprehensiveness of this text is impressive. In the etiology section, habits, mouth breathing, trauma, and genetics are all covered thoroughly. Next, treatment approaches are dis-cussed, based on various stages of growth. For each stage, the treatment options are presented, and at the end of each section, stability of correction is addressed. Two relatively recent approaches, surgical treatment and skeletal anchorage, are described in detail, as well as a sometimes under-utilized option, occlusal equilibration.
Each section also is supplemented by multiple case reports illustrating the concepts described in the text. These case reports are particularly helpful, as they are thoroughly documented and present practical, interest-ing, and creative approaches to address a wide variety of open-bite malocclusions.
The authors understand the importance of long-term stability, and their honest and thorough reporting of this topic serves as an excellent example of an evidence-based approach to orthodontics. It is important that the profession reports treatment and retention information accurately, so that we can appropriately compare treatments and determine which ones offer the best chance for excellent, stable results.
xv

xvi Foreword
While anterior open-bite malocclusions will continue to be challenging to address, every orthodontist will have a better understanding of these malocclusions after reading this text, and this greater knowledge will translate into better treatment for our patients. This is a text that every orthodontist will wish to have in his or her library.
Greg J. Huang

Preface
Writing a book on anterior open-bite treatment is certainly a difficult task to accomplish because it consists in treating vertical malocclusion prob-lems, which are one of the greatest challenges in orthodontics. Therefore, we thought that only describing the several treatment procedures would not completely cover the different aspects of handling this problem. Treat-ment stability should also be approached. It is most frustrating, especially for a young orthodontist, to deal with relapse when following up patients, without knowing what to expect. Experiencing some relapse may have a negative impact on the clinician′s self-confidence. One may think that the case was not handled adequately and that it was the cause for the relapse. We think that for each orthodontic abnormality a thorough knowledge of its management has to include an understanding of the long-term behavior of its treatment. Without it, there will always be some apprehension in following up patients. Besides, by knowing the expected relapse percent-age, one can use specific retention strategies that will be able to improve stability.
As we have conducted a few studies on open-bite treatment stability we thought that we would share this experience with colleagues, demonstrat-ing how this has influenced our approach to open-bite treatment.
The book does not suggest a unique approach to open-bite treatment that should be followed but shows the most usual approaches in different stages of the dentition and what can be expected regarding stability, based on scientific evidence. It was written in a clinically oriented language to be easily understood by the clinician, illustrated with several clinical cases. The changes that contributed to treatment are emphasized and demon-strated with superimpositions and tables. Some academic language is used in the stability sections of each chapter. However, it is easy to follow.
The chapters are organized in an ascending order of treatment difficulty of the open-bite, beginning with treatment in the deciduous and mixed dentition, then in the permanent dentition, and last with the orthodontic-surgical approach. This approach probably is the best way to learn how to handle this problem and parallels the programs in most dental schools: undergraduate programs include treatment only in the deciduous and
xvii
xviii Preface
mixed dentition, and graduate programs study treatment in the permanent dentition.
We hope that this work will contribute to the understanding of the variables involved in the treatment and stability of this orthodontic abnormality.
Guilherme JansonFabrício Valarelli

Acknowledgments
Dr. Janson acknowledges Drs. Décio Rodrigues Martins, Marcos Roberto de Freitas, José Fernando Castanha Henriques, Arnaldo Pinzan, and Renato Rodrigues de Almeida, professors of the Orthodontic Department at Bauru Dental School, University of São Paulo, for the support and contributions in his academic career.
He also acknowledges Drs. Donald G. Woodside and Angelos Metaxas, professors of the Orthodontic Department, Faculty of Dentistry, University of Toronto, for the opportunity to expand his Orthodontic education in the department.
The authors would like to acknowledge the following persons who contributed to this book:
Drs. Claudia Cristina da Silva, Danilo Pinelli Valarelli, Maria Fernanda Antônio Silva, Mayara Paim Patel, Thais Marchini de Oliveira, Daniele Paulani dos Santos, Soraya Rolim Mouammar Rodrigues da Costa, Adriano Bandeca, Tiago Peluso Velho, Juliana Curi Paccini, Virgílio de Miranda Camargo, Ricardo Lincoln Fernandes Silva, Hediberton Aguiar, Andréia Boff Lemos, Daniela Olívia Ferrari Carvalho and José Eduardo Prado de Souza, who treated or supervised the patients’ treatments, and collected the records.
Fabrício Rodrigues and Otávio Farah, from Maggna—Creative Presen-tations, for the illustrations.
Alessandra Jatobá, Léia Cristina Garcia de Lira, and Viviane and Dany Ellen, who took the patients’ clinical photographs.
Daniel Francisco Rascão Selmo, who treated and prepared the figures.Drs. Rejane Targino Soares Beltrão, Marcus Crepaldi, and Francisco
Ajalmar Maia, who conducted the investigations on open-bite treatment stability and root resorption in open-bite treatment during their graduate years.
xix


Open-Bite Malocclusion


1
1Anterior open-bite malocclusion is defined as the absence of contact between the maxillary and mandibular incisor edges consequently present-ing a negative overbite (Nielsen 1991; Ngan and Fields 1997). Generally, it deteriorates the facial aspect, impairs mastication and speech, subjecting the patient to uncomfortable situations (Janson et al. 2003). The frequency of this malocclusion in the mixed dentition is high (17% [Worms et al. 1971]), and the prognosis for correction varies from good to deficient, depending on its severity and on the patient’s age. Before undertaking any treatment alternative, knowledge of the etiology of this malocclusion is important because in many instances, not only the morphological charac-teristics have to be corrected, but also the etiological factors have to be eliminated not only to assure treatment success, but also to provide long-lasting stability. Therefore, this chapter covers the most common etiological factors of anterior open-bite to help in managing the correction of this malocclusion in the different stages of the dentition it may present.
The etiologic factors of the malocclusions can be divided into environ-mental and genetic factors. However, all malocclusions are multifactorial and result from interactions of environment and genetics (Mossey 1999a, 1999b). The face and the dentition are influenced by the complex interac-tion of both. It can be stated that the etiology of a particular malocclusion is predominantly environmental or genetic, and this will determine how much this malocclusion can be corrected by therapeutic intervention, that is, the prognosis of orthodontic correction. The greater the influence of
Open-Bite Malocclusion: Treatment and Stability, First Edition. Edited by Guilherme Janson and Fabrício Valarelli.© 2014 John Wiley & Sons, Inc. Published 2014 by John Wiley & Sons, Inc.
Etiology of open-bite malocclusionKarina Freitas and Rodrigo Cançado

2 Open-Bite Malocclusion: Treatment and Stability
environmental factors in the etiology of a malocclusion, the better the orthodontic treatment prognosis, as long as the causative factor is elimi-nated. When there is a strong genetic etiologic factor, most likely the best approach would consist in an orthodontic-surgical approach (Beane 1999). Because environmental open bites are more amenable to an orthodontic approach, this chapter will first cover the environmental etiologic factors and secondly the genetic factors.
ENVIRONMENTAL FACTORS
Anterior open bite can be considered as functional consequent to its func-tional etiologic factors. The most important functional factors are deleteri-ous oral habits, (Popovich and Thompson 1973; Mahalski and Stanton 1992; Johnson and Larson 1993) and oral breathing (Proffit and Mason 1975; Lowe and Johnston 1979; Harvold et al. 1981; Linder-Aronson et al. 1986; Nagahara et al. 1996; Yashiro and Takada 1999). Some other factors may contribute in the environmental etiology such as traumatisms and pathologies (Prosterman et al. 1995).
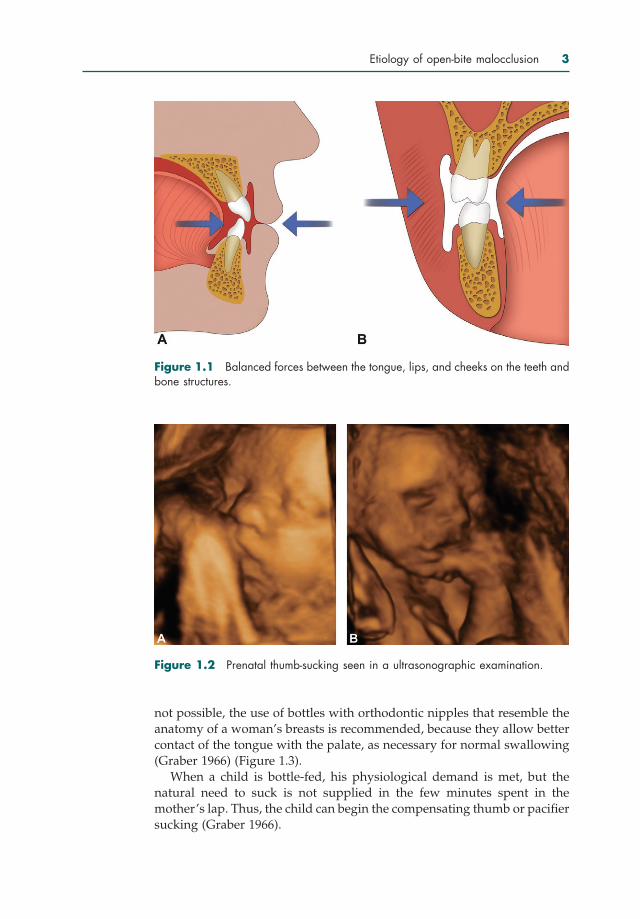
Deleterious habitsIn a normal occlusion, there is a balanced relationship among the oral structures, basal bones, teeth, and intra and extraoral musculature, reflect-ing in a correct function of the stomatognathic system (Moyers 1988). This is denominated the buccinator mechanism. Thus, the teeth are in a bal-anced position receiving opposing forces arising internally by the tongue and externally by the lips and cheeks (Figure 1.1) (Graber 1966).
The solution of this muscular balance for some abnormal function of the oral muscles has a negative impact on the teeth position and occlusion. Nonnutritive sucking habits, such as pacifier and thumb-sucking, atypical tongue thrust, and anterior tongue posture, all considered deleterious oral habits, can break this muscular balance.
Pacifier and thumb-sucking
Humans start sucking fingers, tongue, and lips during fetal life, in the maternal womb (Figure 1.2). At birth, the infant has a well-developed func-tion of sucking to receive the nutrients essential for life. It is during suction developed in breastfeeding that the children not only get the nutrients that need to meet the physiological demands, as well as feelings of security, warmth, and acceptance necessary for their welfare and for their proper emotional development. At this stage, suction is a mean of communication of the infant with the environment (Newman 1990).
The early well-developed oral perception provides a sense of comfort, safety, and emotional satisfaction during sucking. When breastfeeding is
Etiology of open-bite malocclusion 3
Figure 1.1 Balanced forces between the tongue, lips, and cheeks on the teeth and bone structures.
Figure 1.2 Prenatal thumb-sucking seen in a ultrasonographic examination.
not possible, the use of bottles with orthodontic nipples that resemble the anatomy of a woman’s breasts is recommended, because they allow better contact of the tongue with the palate, as necessary for normal swallowing (Graber 1966) (Figure 1.3).
When a child is bottle-fed, his physiological demand is met, but the natural need to suck is not supplied in the few minutes spent in the mother’s lap. Thus, the child can begin the compensating thumb or pacifier sucking (Graber 1966).

4 Open-Bite Malocclusion: Treatment and Stability
Figure 1.3 Breastfeeding provides the natural need to suck to the child.
Pacifier or thumb-sucking are considered as mechanisms of emotional supply of the child. Consequently, pacifier or thumb-sucking in the early child development is considered normal. Through these habits, the child releases the emotional tensions from lack of affective care resulting from conflicting relationship between child and parents, which becomes a way to draw attention from people close to them (Moyers 1988). Parental oppo-sition to these habits can determine negative psychological consequences. When children grow and develop other means of communication with the external environment, they usually spontaneously abandon the sucking habit. Interruption of sucking habits during the deciduous dentition can provide self-correction of the anterior open bite. However, persistence of the habit until the mixed dentition represents a deviation from normality, because these habits are potent etiologic malocclusion factors, particularly for anterior open bite (Ogaard et al. 1994; Bishara et al. 2006).
Pacifier or thumb-sucking act as mechanical obstacles, preventing erup-tion of the anterior teeth and establishing an open bite (Moyers 1988; Proffit et al. 2007) (Figure 1.4). Anterior open-bite malocclusion due to pacifier use is characteristically restricted to the anterior teeth and circular (Figure 1.5). Anterior open bite consequent to thumb-sucking is characterized by labial inclination of spaced maxillary incisors and lingual inclination of the man-dibular incisors (Figure 1.6). Anterior open bite may be associated to maxil-lary constriction and uni- or bilateral posterior crossbite, because, during sucking, the tongue is lowered, without contact with the maxillary poste-rior teeth (Moore 1996).
However, a deleterious oral habit does not always necessarily results in an open bite. First, it depends on how the habit is exercised, that is, it
Etiology of open-bite malocclusion 5
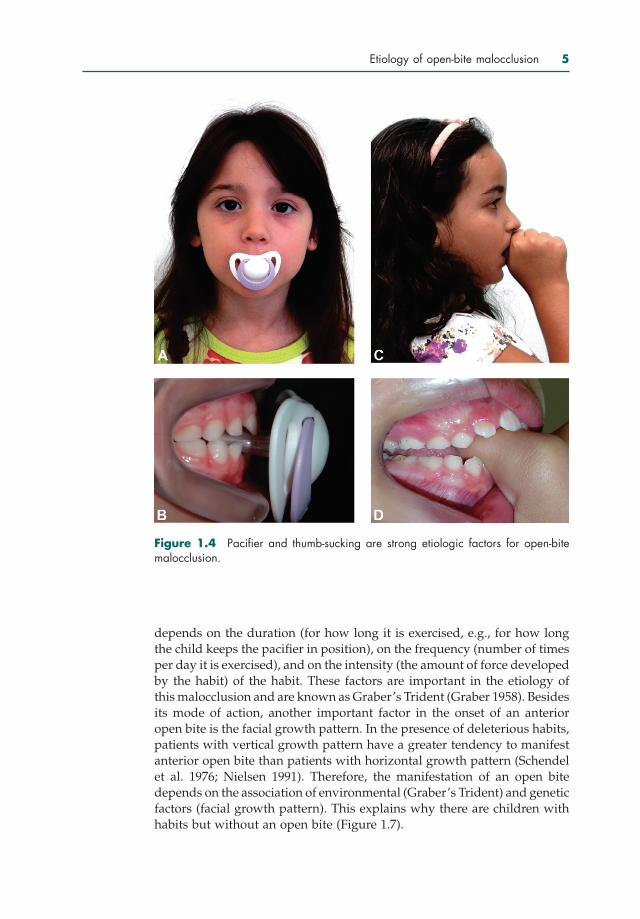
Figure 1.4 Pacifier and thumb-sucking are strong etiologic factors for open-bite malocclusion.
depends on the duration (for how long it is exercised, e.g., for how long the child keeps the pacifier in position), on the frequency (number of times per day it is exercised), and on the intensity (the amount of force developed by the habit) of the habit. These factors are important in the etiology of this malocclusion and are known as Graber’s Trident (Graber 1958). Besides its mode of action, another important factor in the onset of an anterior open bite is the facial growth pattern. In the presence of deleterious habits, patients with vertical growth pattern have a greater tendency to manifest anterior open bite than patients with horizontal growth pattern (Schendel et al. 1976; Nielsen 1991). Therefore, the manifestation of an open bite depends on the association of environmental (Graber’s Trident) and genetic factors (facial growth pattern). This explains why there are children with habits but without an open bite (Figure 1.7).

Figure 1.5 Anterior open bite caused by the use of pacifier is characterized by being restricted to the anterior region of the dental arches and circular.
Figure 1.6 Thumb-sucking characteristically causes labial inclination of the maxil-lary incisors and lingual inclination of the mandibular incisors.
6





![New Pacifier APT - Bitdefender › resources › files › News › ... · 2017-08-31 · Turla Group [2] hite Paper Executive Summary: New components belonging to the Pacifier APT](https://static.fdocuments.us/doc/165x107/5f1d374c6b3fad46c15aca47/new-pacifier-apt-bitdefender-a-resources-a-files-a-news-a-2017-08-31.jpg)