Open access Research Intersectoral and integrated ... · in achieving the right to health for...
13
1 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407 Open access Intersectoral and integrated approaches in achieving the right to health for refugees on resettlement: a scoping review Shirley Ho, 1 Dena Javadi, 1 Sara Causevic, 2,3 Etienne V Langlois, 1 Peter Friberg, 2,4 Göran Tomson 2,5 To cite: Ho S, Javadi D, Causevic S, et al. Intersectoral and integrated approaches in achieving the right to health for refugees on resettlement: a scoping review. BMJ Open 2019;9:e029407. doi:10.1136/ bmjopen-2019-029407 ► Prepublication history for this paper is available online. To view these files, please visit the journal online (http://dx.doi. org/10.1136/bmjopen-2019- 029407). Received 25 January 2019 Revised 17 May 2019 Accepted 21 May 2019 1 Alliance for Health Policy and Systems Research, World Health Organization, Geneva, Switzerland 2 Swedish Institute for Global Health Transformation, Royal Swedish Academy of Sciences, Stockholm, Sweden 3 Global and Sexual Health, Department of Public Health Sciences, Karolinska Institute, Stockholm, Sweden 4 Institute of Medicine, Sahlgrenska Academy, Gothenburg, Sweden 5 Medical Management Centre, Department of Learning, Informatics, Management, Ethics, Karolinska Institute, Stockholm, Sweden Correspondence to Shirley Ho; [email protected] Research © Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ. ABSTRACT Background Better understanding, documentation and evaluation of different refugee health interventions and their means of health system integration and intersectoral collaboration are needed. Objectives Explore the barriers and facilitators to the integration of health services for refugees; the processes involved and the different stakeholders engaged in levaraging intersectoral approaches to protect refugees’ right to health on resettlement. Design Scoping review. Methods A search of articles from 2000 onward was done in MEDLINE, Web of Science, Global Health and PsycINFO, Embase. Two frameworks were applied in our analysis, the ‘framework for analysing integration of targeted health interventions in systems’ and ‘Health in All Policies’ framework for country action. A comprehensive description of the methods is included in our published protocol. Results 6117 papers were identified, only 18 studies met the inclusion criteria. Facilitators in implementation included: training for providers, colocation of services, transportation services to enhance access, clear role definitions and appropriate budget allocation and financing. Barriers included: lack of a participatory approach, insufficient resources for providers, absence of financing, unclear roles and insufficient coordination of interprofessional teams; low availability and use of data, and turf wars across governance stakeholders. Successful strategies to address refugee health included: networks of service delivery combining existing public and private services; system navigators; host community engagement to reduce stigma; translation services; legislative support and alternative models of care for women and children. Conclusion Limited evidence was found overall. Further research on intersectoral approaches is needed. Key policy insights gained from barriers and facilitators reported in available studies include: improving coordination between existing programmes; supporting colocation of services; establishing formal system navigator roles that connect relevant programmes; establishing formal translation services to improve access and establishing training and resources for providers. INTRODUCTION Upholding the right to health is a funda- mental challenge for governments world- wide, particularly when providing services to vulnerable or hard to reach populations such as refugees. The Office of the United Nations High Commission for Human Rights iden- tifies the right to health as a fundamental part of human rights, first articulated in the 1946 Constitution of WHO. 1 Entitlements under the right to health include universal health coverage—now a target under Sustain- able Development Goal (SDG) 3—broadly covering access to preventative and curative services, essential medicines, timely basic health services, health-related education, participation in health-related decision making at both national and community levels, as well as financial protection. 1 2 Espe- cially relevant to the plight of refugees, the right to health includes non-discrimination whereby health services, commodities and facilities must be provided to all without Strengths and limitations of this study ► Our study employs a systematic approach by using two frameworks, the ‘framework for analysing inte- gration of targeted health interventions in systems’ and ‘Health in All Policies’ framework for country action to develop a stronger understanding of the processes and actors involved in integration and intersectoral action. ► Our findings can be applied for policy and action aiming to enhance the integration of refugee health services within health systems, and identifying research needs to advance the right to health for refugees. ► The lack of evidence on intersectoral and integrated approaches from low-income and middle-income countries may impact the generalisability of the findings. on July 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2019-029407 on 1 July 2019. Downloaded from
Transcript of Open access Research Intersectoral and integrated ... · in achieving the right to health for...

1Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
Intersectoral and integrated approaches in achieving the right to health for refugees on resettlement: a scoping review
Shirley Ho,1 Dena Javadi,1 Sara Causevic,2,3 Etienne V Langlois,1 Peter Friberg,2,4 Göran Tomson2,5
To cite: Ho S, Javadi D, Causevic S, et al. Intersectoral and integrated approaches in achieving the right to health for refugees on resettlement: a scoping review. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
► Prepublication history for this paper is available online. To view these files, please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjopen- 2019- 029407).
Received 25 January 2019Revised 17 May 2019Accepted 21 May 2019
1Alliance for Health Policy and Systems Research, World Health Organization, Geneva, Switzerland2Swedish Institute for Global Health Transformation, Royal Swedish Academy of Sciences, Stockholm, Sweden3Global and Sexual Health, Department of Public Health Sciences, Karolinska Institute, Stockholm, Sweden4Institute of Medicine, Sahlgrenska Academy, Gothenburg, Sweden5Medical Management Centre, Department of Learning, Informatics, Management, Ethics, Karolinska Institute, Stockholm, Sweden
Correspondence toShirley Ho; Shirley. ho@ jhu. edu
Research
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
AbstrACt background Better understanding, documentation and evaluation of different refugee health interventions and their means of health system integration and intersectoral collaboration are needed. Objectives Explore the barriers and facilitators to the integration of health services for refugees; the processes involved and the different stakeholders engaged in levaraging intersectoral approaches to protect refugees’ right to health on resettlement.Design Scoping review.Methods A search of articles from 2000 onward was done in MEDLINE, Web of Science, Global Health and PsycINFO, Embase. Two frameworks were applied in our analysis, the ‘framework for analysing integration of targeted health interventions in systems’ and ‘Health in All Policies’ framework for country action. A comprehensive description of the methods is included in our published protocol.results 6117 papers were identified, only 18 studies met the inclusion criteria. Facilitators in implementation included: training for providers, colocation of services, transportation services to enhance access, clear role definitions and appropriate budget allocation and financing. Barriers included: lack of a participatory approach, insufficient resources for providers, absence of financing, unclear roles and insufficient coordination of interprofessional teams; low availability and use of data, and turf wars across governance stakeholders. Successful strategies to address refugee health included: networks of service delivery combining existing public and private services; system navigators; host community engagement to reduce stigma; translation services; legislative support and alternative models of care for women and children. Conclusion Limited evidence was found overall. Further research on intersectoral approaches is needed. Key policy insights gained from barriers and facilitators reported in available studies include: improving coordination between existing programmes; supporting colocation of services; establishing formal system navigator roles that connect relevant programmes; establishing formal translation services to improve access and establishing training and resources for providers.
IntrODuCtIOnUpholding the right to health is a funda-mental challenge for governments world-wide, particularly when providing services to vulnerable or hard to reach populations such as refugees. The Office of the United Nations High Commission for Human Rights iden-tifies the right to health as a fundamental part of human rights, first articulated in the 1946 Constitution of WHO.1 Entitlements under the right to health include universal health coverage—now a target under Sustain-able Development Goal (SDG) 3—broadly covering access to preventative and curative services, essential medicines, timely basic health services, health-related education, participation in health-related decision making at both national and community levels, as well as financial protection.1 2 Espe-cially relevant to the plight of refugees, the right to health includes non-discrimination whereby health services, commodities and facilities must be provided to all without
strengths and limitations of this study
► Our study employs a systematic approach by using two frameworks, the ‘framework for analysing inte-gration of targeted health interventions in systems’ and ‘Health in All Policies’ framework for country action to develop a stronger understanding of the processes and actors involved in integration and intersectoral action.
► Our findings can be applied for policy and action aiming to enhance the integration of refugee health services within health systems, and identifying research needs to advance the right to health for refugees.
► The lack of evidence on intersectoral and integrated approaches from low-income and middle-income countries may impact the generalisability of the findings.
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

2 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
any discrimination. Lastly, these health services must be accessible, medically and culturally appropriate, available in adequate amount and quality, which includes having a trained health workforce, safe products and sanitation.2
‘Refugees’ are individuals fleeing armed conflict or persecution as defined by the 1951 Refugee Convention which also identifies their basic rights, specifically that refugees should not be returned to situations that are deemed a threat to their life or freedom.3 A key distinc-tion of refugee rights is that they are a matter of national legislation, and of international law.4 Despite these legal protections, refugees face many challenges in accessing health services, especially more vulnerable groups like women and children.5 Many states explicitly exclude refu-gees from the level of protection afforded to their citizens, instead choosing to offer ‘essential care’ or ‘emergency healthcare’, which is differentially defined across coun-tries.6 The Committee on the Elimination of Racial Discrimination, and the Committee on Economic, Social and Cultural Rights, both include general statements that hold States accountable to ‘the right of non-citizens to an adequate standard of physical and mental health by, inter alia, refraining from denying or limiting their access to preventive, curative and palliative health services’.7 The increasing number of refugees over the past years makes the realisation and protection of these rights both a legal, ethical and a logistical challenge.5 In addition, the boundaries of the right to health have expanded due to increased understanding of social determinants of health and the health impacts of the lived environment.8 9 Refu-gees face challenges in navigating health, legal, educa-tion, housing, social protection and employment services, which further threatens their quality of life and health status.10 Therefore, a lack of coordination and integration across these services undermines their effectiveness.11
Much like the shift from the more vertical approaches of the millennium development goals towards the more integrated SDGs, the protection of the right to health calls for an intersectoral approach whereby health is applied to all policies for all people.12 As such, for states to effectively protect the right to health for refugees, there is a need to work across sectors and disciplines to better integrate targeted programmes and initiatives, thereby improving standards of care during resettlement. Some evidence exists that supporting collaboration and coordination across social services for refugees improves the effective-ness and quality of care received.10 Many fragmented psychosocial programmes exist across sectors to attempt to address the unique challenges faced by refugees but these are largely unevaluated and lack sustainability.13 14 Better understanding, documentation, evaluation and reporting of the dynamic nature of different interven-tions, and their means of health system integration and intersectoral collaboration, are necessary to ensure that lessons learnt are implemented in the design of future policies and programmes.
Therefore, we conducted a scoping review that describes the barriers and facilitators to integrated health services
for refugees; the process involved in protecting refugee health; and the different stakeholders engaged in lever-aging intersectoral approaches to protect refugees’ right to health on resettlement. We focused on three specific research questions:1. What are the barriers and facilitators in integrating
targeted services for refugees within existing health systems?
2. What strategies are involved in addressing refugees’ right to health on resettlement?
3. Which stakeholders are involved in leveraging intersec-toral approaches to protect refugees’ right to health?
MethODsstudy designWe selected the scoping review method as we were inter-ested in mapping the concepts relevant to the complex nature of this topic, the changing global landscape around it, and the emerging and diverse knowledge base, which makes the method well matched to our research objectives.15 16 We drafted a scoping review protocol following the methods outlined by the Joanna Briggs Insti-tute Methods Manual for scoping reviews.17 Our protocol was registered with the Open Science Framework,18 and published in BMJ Open.19 Since our full methods are avail-able in the published protocol, a summary is provided below.19
Information sources and search strategyA search of articles was done by two experienced librarians at the Karolinska Institutet using the following electronic databases: MEDLINE, Web of Science, Global Health and PsycINFO, Embase. See online supplementary appendix I for the comprehensive search strategy. Search terms included umbrella terms for three topics: refugees (eg, immigrants, migrants, asylum seekers, transients); health and social services (eg, healthcare, patient experience, health services, interdisciplinary, intersectoral collabo-ration, access to care)and health equity (eg, disparities, social determinants, rights-based approaches). These were combined to comprise the search (detailed search terms in online supplementary appendix).
eligibility criteriaPopulationRefugees as defined by the 1951 Refugee Convention.3
InterventionA programme, approach or technical innovation that aims to protect refugees’ right to health, including inter-ventions aimed at addressing the social determinants of health. Interventions outside of the health sector that affect health were included.
ComparatorsThis component was not necessary as the focus was on gauging the state of evidence.
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

3Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
OutcomesEligible studies and papers include those discussing plans for action, strategies, barriers, facilitators or outcomes using an intersectoral approach.
Types of studies includedRandomised control trials, pre–post design evaluations, qualitative evaluations and economic evaluations were included. Further, implementation research and opera-tions research studies were eligible for inclusion, as well as studies or reports outlining stakeholder experiences and plans.
Exclusion criteriaPapers published in a language other than English were excluded. Other categories of migrants were not included as their legal entitlements are different to those of refu-gees which are protected under international law. If the studies did not display some level of integration nor inter-sectorality, they were not assessed further.20 Studies or commentaries that solely discuss theories and conceptual models were excluded.
Time periodOnly studies from 2000 onward have been included.
SettingEligible studies are set in countries receiving refugees and asylum seekers (who may eventually qualify for refugee status) and serving as hosts for resettlement.
Frameworks to address research questionsTwo published frameworks were used in our analysis to understand integration of health services within health systems and to analyse intersectoral approaches to support these services. The first framework by Atun et al,21 is a tool for analysing integration of targeted health inter-ventions in health systems, where integration is defined as ‘the extent, pattern and rate of adoption and eventual assimilation of health interventions into each of the crit-ical functions of a health system’.21 The framework for integration was also used to assess the process, and actors involved in integration.20
The second framework applied in our analysis is that of the Health in All Policies (HiAP) framework for country action. HiAP is defined as a way for countries to protect population health through ‘an approach to public poli-cies across sectors that systematically takes into account the health implications of decisions, seeks synergies and avoids harmful health impacts in order to improve popu-lation health and health equity’.22 Components of this framework, adapted to refugee needs, were used in the review to frame barriers and facilitators in integrating refugee services through intersectoral collaboration.
Data abstractionA data abstraction chart was developed based on the two frameworks used in this study. The chart was tested by two researchers and revised as appropriate. The revised chart
was used by the same researchers to abstract descriptive and qualitative data as relevant to the elements of the frame-works used. Elements included in the chart were: inter-vention description; barriers and facilitators; contextual details; target population; type of evaluation; outcomes; stakeholder involvement in governance, financing, plan-ning, service delivery, monitoring and evaluation, and engagement. Deductive reasoning was used to identify barriers and facilitators in intersectoral collaboration for refugee health. Open coding was applied to visualise themes across interventions as well as barriers and facilita-tors.23 Axial coding was applied to then draw connections to enabling strategies for intersectoral collaboration.23 General conclusions were drawn based on these themes, leading to suggestions for strengthening programmes and policies.
Patient and public involvementThere was no patient or public involvement required in conducting this scoping review.
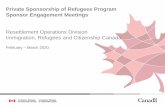
resultsOf the 6117 records identified through the search strategy, 1302 abstracts were screened after removing dupli-cates. A total of 1141 were excluded based on exclusion criteria described above as assessed by two independent reviewers, 131 full texts were assessed, with the references of 15 selected articles additionally screened for inclusion criteria, a total of 18 studies were included in our review (see figure 1). Five studies were programmes or inter-ventions carried out in the USA, one in Australia, two in Canada, one in Ethiopia and Uganda, and one in each of the following: Italy, Lebanon, Mexico, the Netherlands, New Zealand, Spain and the UK (See table 1). Six studies were interventions at the district/local level, four at a broader regional level and five at the national level. The interventions outlined in the included studies addressed mostly all genders and all age ranges with the exception of six that targeted vulnerable groups: two studies on mothers and children24 25; one on the elderly26; one on students27 and two on women and girls.28 29 Interventions targeting women and children in particular used alter-native models of care such as mobile health clinics28 29 and school-based interventions.24 27 Seven studies applied qualitative approaches (primarily in-depth interviews) for evaluation,27–33 four studies used survey tools or standardised assessment tools25 26 34 35; four studies used descriptive and routine data24 36–38; and three studies were mainly descriptive analysis reporting on and looking at the outcomes of case examples and policies.39–41
To respond to research question 1, each of the inter-ventions and summarised barriers and facilitators are described in table 1 and grouped by common themes in table 2. Common facilitators identified in programmes and approaches to protect refugee health through inter-sectoral approaches and integration of services include: strong communication of programme availability, tools
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

4 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
and training for providers, colocation of services, trans-portation services to enhance access, clear role definitions, interprofessional team and relationship management across providers, appropriate allocation of budget and financing and coordinated refugee-specific policies.
Barriers articulated include: lack of a participatory approach, poor communication leading to stigma and underuse of services, insufficient resources given to providers, absence of financing, unclear roles and insuf-ficient coordination of interprofessional teams, exclu-sionary refugee policies, low availability and use of data and turf wars across governance stakeholders. Table 2 highlights the studies that expand on these themes as barriers or facilitators.
To respond to research question 2, this section will summarise common themes identified as enabling strategies that support intersectoral collaboration to promote refugee health. Strategies identified in this review include: establishing networks of service delivery through a combination of existing public and private services, establishing a system navigator role, engaging host communities to reduce stigma, ensuring availability of translation services, outreach, and advocacy and legis-lative support. Table 3 highlights the studies that address each of these strategies. In Italy, for example, networks were promoted among private and public authorities and service providers, including health, employment, vocational training and continuing education services.34 In this model, users moved through the pathways of inte-gration and can receive support for any combination of
health needs, access to education, housing support and legal assistance.34 Collaborative design and delivery of services was also demonstrated in Australia with support from multidisciplinary, intersectoral teams, but a lack of funding presented barriers to the potential success of this initiative.27 Similarly in the USA, the ‘Bridge Project’ faced insufficient funding in the coordination of care despite seeing promising results from use of a system navigator—or primary care nurse ‘bridge’—to connect primary care and mental healthcare services.37 A network of ‘gateway services’ was also tested in Canada using a ‘Reception House’ model.35 These services are characterised by being person-centred, interprofessional, communica-tion-focused and comprehensive across the continuum of care.35 Relationship management between the Recep-tion House, health professionals, translation services and social services was acknowledged as a key component for success.35 Input from international medical graduates in training also supported this work by enhancing culturally appropriate service delivery by this network of partners.35
Striking a balance between providing tailored, cultur-ally appropriate care and integrating health and social services for refugees into existing services in the host community can be especially challenging. Policy reviews suggest that taking a ‘one-policy, one-level, one-outcome’ approach or focusing refugee management under one ministry is not sufficient in addressing the wide range of obstacles that both host and refugee communities are facing as a result of the current political climate.40 41 The Ethiopian government, for example, had success in
Figure 1 Scoping review flow chart.
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

5Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
Tab
le 1
S
umm
ary
of in
clud
ed s
tud
ies
Aut
hor
Year
Tit
leIn
terv
enti
on
Bar
rier
sFa
cilit
ato
rsC
oun
try
Cal
vo e
t al
3020
14Th
e E
ffect
of U
nive
rsal
S
ervi
ce D
eliv
ery
on t
he In
tegr
atio
n of
Mor
occa
n Im
mig
rant
s in
Sp
ain:
A
Cas
e S
tud
y fr
om
an A
nti-
Op
pre
ssiv
e P
ersp
ectiv
e
Ad
dre
ssin
g st
igm
a an
d h
ost
com
mun
ity
per
cep
tions
; sys
tem
na
viga
tor
(inte
rcul
tura
l m
edia
tor)
.
Min
imal
invo
lvem
ent
of t
arge
t co
mm
unity
in d
esig
n of
p
rogr
amm
e; c
onsi
der
atio
ns
of fo
rced
ass
imila
tion
thro
ugh
inte
grat
ion.
Dec
reas
ed p
reju
dic
e d
ue t
o in
crea
sed
con
tact
b
etw
een
host
and
imm
igra
nt
com
mun
ities
; cle
ar
com
mun
icat
ion
to h
ost
com
mun
ity a
roun
d a
lloca
tion
of r
esou
rces
the
reb
y re
duc
ing
per
ceiv
ed t
hrea
t of
co
mp
etiti
on.
Sp
ain
Cat
arci
3420
12C
once
ptio
ns a
nd
Str
ateg
ies
for
Use
r In
tegr
atio
n ac
ross
R
efug
ee S
ervi
ces
in
Italy
Inte
grat
ed r
ecep
tion
of
refu
gees
and
asy
lum
se
eker
s (n
etw
ork
of
hosp
itals
and
hea
lth
serv
ices
, pub
lic
emp
loym
ent
serv
ices
, vo
catio
nal t
rain
ing
and
co
ntin
uing
ed
ucat
ion
agen
cies
, etc
).
Ser
vice
coo
rdin
ator
s la
ck t
ools
to
sup
por
t in
tegr
ated
ser
vice
s; la
ck
of c
ontin
uity
bet
wee
n th
eory
and
p
ract
ice
in c
ontin
uing
ed
ucat
ion
sup
por
t.
Ser
vice
coo
rdin
ator
s w
ith
acce
ss t
o co
ntin
uing
ed
ucat
ion
wer
e m
ore
likel
y to
rep
ort
adeq
uate
sup
por
t;
cont
inui
ng e
duc
atio
n w
ith
intim
ate
know
led
ge o
f the
co
ntex
t, u
ser
need
s an
d
legi
slat
ion
rela
ted
to
refu
gee
incl
usio
n; c
oord
inat
ors
shou
ld a
lso
have
a s
olid
ne
twor
k an
d a
n ab
ility
to
dis
tingu
ish
bet
wee
n re
sour
ces.
Italy
Cow
ell e
t al
2520
09C
linic
al T
rail
Out
com
es
of t
he M
exic
an
Am
eric
an P
rob
lem
S
olvi
ng P
rogr
am
(MA
PS
)
A c
ogni
tivel
y b
ased
p
rob
lem
sol
ving
p
rogr
amm
e d
eliv
ered
on
link
ed h
ome
visi
ts t
o m
othe
rs a
nd a
fter
sch
ool
pro
gram
me
clas
ses
to
child
ren.
Diffi
culty
man
agin
g ca
se lo
ad b
y sc
hool
nur
se o
f hom
e vi
sits
and
cl
asse
s.
Com
mun
icat
ion
and
en
gage
men
t w
ith t
he
com
mun
ity; p
artn
ersh
ip w
ith
the
scho
ol.
US
A
Gel
tman
and
C
ochr
an38
2005
A P
rivat
e-S
ecto
r P
refe
rred
Pro
vid
er
Net
wor
k M
odel
fo
r P
ublic
Hea
lth
Scr
eeni
ng o
f New
ly
Res
ettle
d R
efug
ees
Pub
lic–p
rivat
e p
artn
ersh
ips
usin
g a
pre
ferr
ed p
rovi
der
net
wor
k m
odel
for
cond
uctin
g re
fuge
e he
alth
scr
eeni
ng.
Lack
of a
pp
rop
riate
fund
ing
mod
el le
adin
g to
del
ays
in h
ealth
sc
reen
ing.
Fund
ing
stre
ams
app
rove
d
allo
wed
pro
cure
men
t of
ser
vice
s; n
etw
ork
of
pro
vid
ers
crea
ted
; ded
icat
ed
trai
ning
of p
hysi
cian
s w
ithin
th
e ne
twor
k.
US
A
Gur
uge
et a
l2920
10Im
mig
rant
wom
en’s
ex
per
ienc
es o
f re
ceiv
ing
care
in a
m
obile
hea
lth c
linic
Mob
ile h
ealth
clin
ic fo
r re
pro
duc
tive
heal
th
serv
ices
for
imm
igra
nt
wom
en.
Lack
of a
war
enes
s of
ava
ilab
le
serv
ices
and
nav
igat
ing
heal
th
syst
ems;
lang
uage
bar
rier;
fear
of
dep
orta
tion
lead
ing
to la
ck o
f use
of
ser
vice
s.
Col
ocat
ion
of s
ervi
ces
due
to
the
mob
ile n
atur
e of
the
cl
inic
.
Can
ada
Con
tinue
d
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

6 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
Aut
hor
Year
Tit
leIn
terv
enti
on
Bar
rier
sFa
cilit
ato
rsC
oun
try
Kim
et
al36
2002
Prim
ary
heal
th c
are
for
Kor
ean
imm
igra
nts:
su
stai
ning
a c
ultu
rally
se
nsiti
ve m
odel
Tran
slat
ion
sup
por
t;
inte
grat
ed h
ealth
and
so
cial
car
e; m
enta
l he
alth
sup
por
t;
bili
ngua
l ad
vanc
ed
nurs
e p
ract
ition
er a
nd
com
mun
ity a
dvo
cate
se
rve
as s
yste
m
navi
gato
rs.
Bud
geta
ry r
estr
ictio
ns; e
xist
ing
rest
rictio
ns in
the
rol
es t
hat
nurs
es
can
pla
y in
out
reac
h.
Effe
ctiv
e co
mm
unic
atio
n ar
ound
ava
ilab
ility
of n
ew
pro
gram
me;
effe
ctiv
e co
mm
unic
atio
n to
ann
ounc
e ne
w o
utre
ach
and
nav
igat
ion
role
; effo
rts
to b
uild
co
nsen
sus
and
coh
eren
ce
acro
ss in
terp
rofe
ssio
nal
team
s; c
lear
art
icul
atio
n of
th
e ro
le o
f ad
vanc
e nu
rse
pra
ctiti
oner
s an
d t
heir
com
ple
men
tary
rol
e.
US
A
Lille
ston
et
al28
2018
Eva
luat
ion
of a
mob
ile
app
roac
h to
gen
der
-b
ased
vio
lenc
e (G
BV
) se
rvic
e d
eliv
ery
amon
g S
yria
n re
fuge
es in
Le
ban
on
GB
V m
obile
sup
por
t se
rvic
e, p
rovi
din
g sa
fe
spac
es, c
omm
unity
ou
trea
ch, p
sych
osoc
ial
sup
por
t ac
tiviti
es,
safe
lega
l and
med
ical
re
ferr
als,
sur
vivo
r-
app
roac
h, a
dhe
renc
e to
con
fiden
tialit
y an
d
acce
ss t
o fa
ce-t
o-fa
ce
and
pho
ne-b
ased
cas
e m
anag
emen
t.
Trus
t b
uild
ing
is a
key
ele
men
t an
d s
o co
nsta
nt m
obili
ty o
f tar
get
aud
ienc
e p
rese
nted
a c
halle
nge
as
did
ref
erra
l of s
ervi
ces
as q
ualit
y m
edic
al a
nd le
gal s
ervi
ces
wer
e no
t al
way
s sa
fe o
r av
aila
ble
.
Inte
grat
ion
of le
gal a
nd
med
ical
tea
ms
in m
obile
GB
V
sup
por
t te
ams;
com
mun
ity
mob
ilise
rs/s
yste
m n
avig
ator
ro
le is
a k
ey fu
nctio
n.
Leb
anon
Mac
farla
ne e
t al
3320
09La
ngua
ge b
arrie
rs
in h
ealth
and
soc
ial
care
con
sulta
tions
in
the
com
mun
ity: A
co
mp
arat
ive
stud
y of
re
spon
ses
in Ir
elan
d
and
Eng
land
Tran
slat
ion
sup
por
tU
se o
f unp
aid
inte
rpre
ters
from
p
atie
nts’
soc
ial n
etw
orks
is
com
ple
x; o
nly
one
accr
edite
d
cour
se fo
r p
rofe
ssio
nal i
nter
pre
ters
; us
e of
pro
fess
iona
l int
erp
rete
rs
pat
chy
due
to
low
qua
lity
and
in
stitu
tiona
l cha
lleng
es in
the
ir ac
qui
sitio
n.
In E
ngla
nd w
here
the
re is
a
pol
icy
to u
se la
ngua
ge
serv
ices
(rac
e eq
ualit
y p
olic
y),
ther
e is
mor
e us
e th
an in
Ire
land
but
imp
lem
enta
tion
rem
ains
poo
r.
UK
McM
urra
y et
al
3520
14In
tegr
ated
Prim
ary
Car
e Im
pro
ves
Acc
ess
to H
ealth
care
for
New
ly
Arr
ived
Ref
ugee
s in
C
anad
a
Tran
slat
ion
sup
por
t;
inte
grat
ed h
ealth
and
so
cial
car
e; G
atew
ay
serv
ices
and
sys
tem
na
viga
tors
.
Sho
rtag
e of
prim
ary
care
p
hysi
cian
s w
hich
is t
he g
atew
ay;
bur
eauc
racy
whe
n b
illin
g C
anad
a’s
Inte
rim F
eder
al H
ealth
P
rogr
am t
hat
pro
vid
es c
over
age
for
heal
thca
re c
osts
unt
il p
rovi
ncia
l he
alth
insu
ranc
e is
ava
ilab
le.
Rel
atio
nshi
ps
bet
wee
n lo
cal
phy
sici
an c
omm
unity
and
ca
se w
orke
rs (n
avig
ator
s);
timel
y tr
ansf
er o
f rec
ord
s;
ongo
ing
cons
ulta
tions
pos
t-tr
ansf
er.
Can
ada
Tab
le 1
C
ontin
ued
Con
tinue
d
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

7Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
Aut
hor
Year
Tit
leIn
terv
enti
on
Bar
rier
sFa
cilit
ato
rsC
oun
try
McN
augh
ton
et a
l2420
10D
irect
ions
for
Refi
ning
a
Sch
ool N
ursi
ng
Inte
rven
tion
for
Mex
ican
Imm
igra
nt
Fam
ilies
Act
ive
case
find
ing
and
p
rob
lem
sol
ving
thr
ough
ed
ucat
ion
syst
em (s
choo
l nu
rses
); tr
ansl
atio
n su
pp
ort
Sch
ools
with
no
exis
ting
nurs
ing
outr
each
pro
gram
me
wer
e d
ifficu
lt to
sta
rt a
t.
Nur
sing
rol
e w
as r
ecog
nise
d
and
acc
epte
d b
y im
mig
rant
co
mm
uniti
es; s
choo
ls t
hat
had
a n
ursi
ng p
rogr
amm
e al
read
y co
uld
exp
and
it t
o ac
tive
case
find
ing
with
im
mig
rant
fam
ilies
.
Mex
ico
Mor
tens
en31
2011
Pub
lic H
ealth
Sys
tem
R
esp
onsi
vene
ss
To R
efug
ee G
roup
s In
New
Zea
land
: A
ctiv
atio
n Fr
om T
he
Bot
tom
Up
Phy
sici
an-d
riven
nee
ds-
bas
ed p
rogr
amm
es in
p
rimar
y ca
re.
Mis
mat
ch b
etw
een
pol
icie
s at
na
tiona
l ver
sus
loca
l lev
el; l
ack
of
dem
ogra
phi
c d
ata;
no
long
-ter
m
pla
nnin
g or
pro
ject
ed n
eed
s; lo
w
linka
ges
bet
wee
n d
istr
ict
heal
th
bra
nch,
pub
lic h
ealth
offi
ces
and
no
n-go
vern
men
tal o
rgan
isat
ions
(N
GO
s); l
ow h
ealth
lite
racy
due
to
lack
of t
rans
late
d m
ater
ials
.
Quo
ta r
efug
ees
have
sam
e ac
cess
to
serv
ices
as
host
co
mm
uniti
es; l
ocal
act
ion
activ
ated
by
phy
sici
ans
and
com
mun
ity le
ader
s le
d t
o m
ore
cove
rage
and
hi
gher
qua
lity
serv
ices
in
spec
ific
area
s th
at h
ad m
ore
advo
cacy
.
New
Zea
land
Phi
lbin
et
al40
2018
Sta
te-l
evel
imm
igra
tion
and
imm
igra
nt-
focu
sed
pol
icie
s as
d
river
s of
Lat
ino
heal
th
dis
par
ities
in t
he U
SA
Pol
icie
s to
ad
dre
ss s
ocia
l an
d le
gal d
eter
min
ants
of
hea
lth a
s th
ey r
elat
e to
im
mig
rant
pop
ulat
ions
.
Exc
lusi
onar
y p
olic
ies
affe
ct s
ocia
l d
eter
min
ants
of h
ealth
, esp
ecia
lly
in m
ixed
sta
tus
fam
ilies
; fam
ilies
un
will
ing
to p
artic
ipat
e in
soc
ial
pro
gram
mes
due
to
fear
and
co
nfus
ion
over
ent
itlem
ents
; st
ruct
ural
rac
ism
; res
tric
tions
in
acc
essi
ng e
duc
atio
n an
d
emp
loym
ent;
low
mob
ility
and
re
loca
tion
to r
emot
e ar
eas
with
lo
w a
vaila
bili
ty o
f int
egra
ted
soc
ial
serv
ices
.
Elim
inat
ion
of w
aitin
g p
erio
d
in s
ever
al s
tate
s fo
r ac
cess
to
Med
icai
d r
egar
dle
ss o
f im
mig
ratio
n st
atus
; ext
ra
fund
ing
to fe
der
ally
qua
lified
he
alth
cen
tres
.
US
A
Ste
war
t et
al32
2008
Mul
ticul
tura
l Mea
ning
s of
Soc
ial S
upp
ort
amon
g Im
mig
rant
s an
d
Ref
ugee
s
Pol
icie
s to
ad
dre
ss s
ocia
l an
d le
gal d
eter
min
ants
of
hea
lth a
s th
ey r
elat
e to
im
mig
rant
pop
ulat
ions
; so
cial
net
wor
king
.
Inad
equa
te fi
nanc
ial a
nd h
uman
re
sour
ces,
lim
ited
age
ncy
man
dat
es, i
neffe
ctiv
e co
llab
orat
ion
with
oth
er s
ecto
rs, a
nd lo
w s
taff
mor
ale;
col
lab
orat
ion
imp
eded
b
y th
e vo
lum
e of
org
anis
atio
ns
invo
lved
.
Exi
stin
g ne
twor
ks o
f lon
ger
term
imm
igra
nts
wer
e su
pp
ortiv
e in
ove
rcom
ing
acce
ss b
arrie
rs.
Can
ada
Tab
le 1
C
ontin
ued
Con
tinue
d
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

8 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
Aut
hor
Year
Tit
leIn
terv
enti
on
Bar
rier
sFa
cilit
ato
rsC
oun
try
Tuep
ker
and
C
hi41
2009
Eva
luat
ing
inte
grat
ed
heal
thca
re fo
r re
fuge
es
and
hos
ts in
an
Afr
ican
co
ntex
t
Inte
grat
ing
host
and
re
fuge
e he
alth
care
by
reor
gani
sing
min
istr
ies
to in
corp
orat
e re
fuge
e se
rvic
es in
to e
xist
ing
por
tfol
ios
rath
er t
han
und
er o
ne m
inis
try.
Lack
of e
vid
ence
on
the
add
ed
valu
e of
inte
grat
ed c
are;
con
cern
ar
ound
min
imis
ing
exce
ptio
nal
stat
us o
f ref
ugee
s; n
o le
gal
oblig
atio
n to
pro
vid
e in
tegr
ated
ca
re; t
urf w
ars
acro
ss o
rgan
isat
ions
an
d s
ecto
rs.
Fund
ing
stre
ams
from
in
tern
atio
nal o
rgan
isat
ions
to
natio
nal h
ealth
ser
vice
s.
Eth
iop
ia a
nd U
gand
a
Verh
agen
et
al26
2013
Cul
tura
lly s
ensi
tive
care
for
eld
erly
im
mig
rant
s th
roug
h et
hnic
com
mun
ity
heal
th w
orke
rs (C
HW
s):
des
ign
and
d
evel
opm
ent
of a
com
mun
ity
bas
ed in
terv
entio
n p
rogr
amm
e in
the
N
ethe
rland
s
Use
of e
thni
cally
sim
ilar
CH
Ws
to d
eliv
er h
ealth
an
d s
ocia
l car
e; a
ctiv
e ca
se fi
ndin
g; c
omm
unity
-d
riven
pro
ble
m s
olvi
ng
with
ove
rsig
ht b
y C
HW
s.
Lack
of p
artic
ipat
ion
by
targ
et
com
mun
ity in
cul
tura
lly s
ensi
tive
des
ign;
lim
ited
kno
wle
dge
by
targ
et
com
mun
ity a
roun
d a
vaila
bili
ty o
f se
rvic
es.
Use
of e
thni
cally
sim
ilar
CH
Ws.
Net
herla
nds
Woo
dla
nd e
t al
2720
16E
valu
atio
n of
a s
choo
l sc
reen
ing
pro
gram
me
for
youn
g p
eop
le fr
om
refu
gee
bac
kgro
und
s
Act
ive
case
find
ing
and
p
rob
lem
sol
ving
thr
ough
ed
ucat
ion
syst
em (s
choo
l nu
rses
); tr
ansl
atio
n su
pp
ort.
Poo
r in
tegr
atio
n of
mul
tiple
ser
vice
p
rovi
der
s; la
ck o
f fun
din
g.In
tegr
atio
n w
ithin
the
sch
ool;
info
rmal
com
mun
icat
ion
bet
wee
n cl
inic
ians
and
the
sc
hool
.
Aus
tral
ia
Woo
dla
nd e
t al
3920
10H
ealth
ser
vice
del
iver
y fo
r ne
wly
arr
ived
re
fuge
e ch
ildre
n: A
fr
amew
ork
for
good
p
ract
ice
Com
pre
hens
ive,
scr
eeni
ng
serv
ices
; par
tner
ship
s b
etw
een
com
mun
ity a
nd
heal
th s
ervi
ces
(refu
gee
heal
th n
urse
as
syst
em
navi
gato
r); t
rans
por
tatio
n se
rvic
es t
o ac
cess
ce
ntre
s; s
pec
ific
trai
ning
p
rovi
ded
to
phy
sici
ans
and
oth
er c
are
pro
vid
ers,
in
clud
ing
refe
rral
p
athw
ays;
Pha
rmac
eutic
al
ben
efit
sche
me
add
ress
ing
refu
gee
need
s.
Lack
of c
oord
inat
ed p
olic
y fo
r al
l cat
egor
ies
of r
efug
ees
and
as
ylum
see
kers
; ad
min
istr
ativ
e b
urd
en o
f prim
ary
heal
th c
are
(PH
C) c
oord
inat
ion;
lack
of
info
rmat
ion
for
man
agin
g co
nditi
ons
spec
ific
or p
rom
inen
t to
re
fuge
es.
Fam
ily-b
ased
ser
vice
s (c
oloc
atio
n to
ad
dre
ss
fam
ily n
eed
s); r
efug
ee h
ealth
nu
rses
(sys
tem
nav
igat
ors)
d
ecre
ase
adm
inis
trat
ive
bur
den
of c
oord
inat
ion;
co
nsum
er p
artic
ipat
ion
and
co
nsul
tatio
n; c
oloc
atio
n of
scr
eeni
ng s
ervi
ces;
tr
ansp
orta
tion
sup
por
t fo
r ge
ttin
g to
ser
vice
s; s
tron
g he
alth
info
rmat
ion
syst
ems;
d
ata
and
con
sulta
tions
use
d
to in
form
the
dire
ctio
n of
in
ters
ecto
ral c
olla
bor
atio
n an
d n
atur
e of
par
tner
ship
s b
etw
een
heal
th a
nd
com
mun
ity s
ervi
ce p
rovi
der
s.
Aus
tral
ia
Tab
le 1
C
ontin
ued
Con
tinue
d
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

9Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
reorganising ministries to incorporate refugee manage-ment into existing portfolios rather than a refugee-spe-cific one, moving refugee assistance programmes out of camps and promoting more collaboration across govern-ment and non-governmental programmes.41
In terms of stakeholders involved (research question 3) in implementing, monitoring or facilitating the afore-mentioned strategies, studies did not always report on the parties involved in governance, financing, planning, service delivery, monitoring and evaluation or demand generation (elements drawn from the integration frame-work by Atun et al.21 Where they were mentioned, stake-holders responsible for the governance of interventions addressing refugee health were composed of primary care centres,35 37 municipal governments,30 38 depart-ments of social services and/or public health,30 36 central services responsible for coordination of refugee services and provision of assistance to local services,34 35 national governments31 32 and international bodies.28 Stakeholders responsible for health financing consisted of individual fundraising by service providers,31 33 government30 31 35 38 41 and international bodies or donors.1 28 36 37Programme and policy planning stakeholders encompassed national governments,31 38 41 departments of social services and/or public health,27 30 36 central services responsible for coordination of refugee services and provision of assis-tance to local services,29 34 35 researchers,24 26 30 36 37 service providers27 28 35 37 and international bodies or donors.28 36 41 Service delivery stakeholders included national depart-ments of social services and/or public health,27 30 33 36 38–41 networks of local service providers in health, education, socialisation, translation and/or employment,24 31 34 36 healthcare providers,27 33 35 37 38 central services respon-sible for coordination of refugee services and provision of assistance to local services,32 34 35 community health workers26 and international bodies.28 41 Stakeholders responsible for monitoring and evaluation were seldom explicitly mentioned. For demand generation, stake-holders included central services responsible for the coor-dination of refugee services and provision of assistance to local services,35 local media in the language of the target population,36 community leaders and/or community health workers,26 28 31 32 home health outreach services28 31 and healthcare providers.33 37
DIsCussIOnThe findings from the existing but scarce literature highlight critical factors necessary in facilitating inter-sectoral collaboration and the successful integration of refugee services within existing health systems. The three research questions studied demonstrated barriers and facilitators, enabling strategies recorded in the liter-ature and the stakeholders involved. This section will summarise key themes across these topics and discuss implications for programme implementation, policy and future research.A
utho
rYe
arT
itle
Inte
rven
tio
nB
arri
ers
Faci
litat
ors
Co
untr
y
Yeun
g et
al37
2004
Inte
grat
ing
psy
chia
try
and
prim
ary
care
im
pro
ves
acce
pta
bili
ty
to m
enta
l hea
lth
serv
ices
am
ong
Chi
nese
Am
eric
ans
Sp
ecifi
c tr
aini
ng p
rovi
ded
to
phy
sici
ans
and
oth
er
care
pro
vid
ers;
men
tal
heal
th s
upp
ort
(col
ocat
ion
of m
enta
l hea
lth s
ervi
ces)
; p
rimar
y ca
re n
urse
as
a b
ridge
/sys
tem
nav
igat
or
for
refe
rral
s.
Fund
ing
for
coor
din
atio
n ou
tsid
e p
urvi
ew o
f ess
entia
l se
rvic
es; l
ack
of k
now
led
ge o
n cu
ltura
lly a
pp
rop
riate
men
tal h
ealth
se
rvic
es.
Col
ocat
ion
of p
rimar
y ca
re
and
men
tal h
ealth
ser
vice
s;
des
igna
ted
sta
ff as
the
b
ridge
; tra
inin
g of
ser
vice
p
rovi
der
s.
US
A
Tab
le 1
C
ontin
ued
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

10 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
Coordination of existing public and private servicesA networked approach to service delivery during the initial reception of refugees can often mitigate some of the difficulties encountered by refugee communities. Some examples of coordination of services were seen in Italy,34 Australia,27 the USA37 and Canada.35 In Canada, where a network of ‘gateway services’ was tested using the ‘Reception House’ model, it successfully provided respon-sive and culturally sensitive primary care.35 By partnering community and translation services, as well as healthcare providers with the Reception House, it decreased wait times and improved healthcare access through refer-rals and coordination of services.35 Further analysis with costing studies on a tailored package of health services for vulnerable populations could help to support improved financing of efforts to coordinate services across sectors.
Introduction of a system navigator roleIntegration works through establishing relationships across networks of local stakeholders and service providers. To coordinate this effectively, a system navigator role can be established—the evidence suggests that this role is most effective in the early stage of resettlement.35 The system navigation role can be played by an organi-sation or by people within the existing health or social systems. It connects incoming refugees to timely, cultur-ally appropriate care in the community without creating parallel structures that either threaten host communi-ties or further stigmatise refugees.30 35 The likelihood of success of a system navigator role is further strengthened when providers have access to the knowledge, tools and
training needed to address the specific needs of refugees, including the more vulnerable subgroups (eg, the elderly, women and children). Providers need to understand the context in which they work and the available features and services, user needs, and legislation as it relates to refugees.34 Those playing a coordination or system navi-gation role should also be able to build strong networks with allied specialists, identify appropriate resources and reach out to users.34 35 The risk here, however, is that integrating refugee care may eliminate some determina-tion procedures, potentially undermining the protection mandate and underestimate the tailored needs of refu-gees dealing with significant trauma.41 Future research on the required competencies of the system navigator role is needed to ensure that appropriate professionals are recruited and trained.
Advocacy and legislative supportExclusionary immigration policies can play a consider-able role in marginalisation and discrimination against refugee communities leading to decreased health-seeking behaviours and use of available integrated or intersec-toral services.40 Effective advocacy needs to target the policy-making levels in order to counteract the negative impacts of exclusionary policies. Advocacy by healthcare providers can be influential at the institutional level to push for better allocation of services and funding.31 A multipronged approach may be necessary to continue to advocate for the right to health for refugees by addressing legal challenges, establishing timely and accurate data and information systems to capture needs, creating
Table 2 Barriers and facilitators commonly discussed across studies
Elements Element present as barrier Element present as facilitator
Community engagement Calvo et al30: Verhagen et al26 Kim et al36; Mortensen31; McMurray et al35; Cowell et al25
Communication between host and refugee communities
Calvo et al30; Woodland et al27
Tools/training for service providers to support integrated services
Catarci34; MacFarlane et al33; Woodland et al39
Woodland et al39; Yeung et al37; Geltman and Cochran38
Colocation of services Woodland et al39; Yeung et al37; Lilleston et al28; Guruge et al29
Transportation Woodland et al39
Networks between providers Catarci34; Stewart et al32; Geltman and Cochran38
Budget/appropriate funding streams Kim et al36; McMurray et al35; Stewart et al32
Philbin et al40; Tuepker and Chi41; Geltman and Cochran38
Role definitions Kim et al36 McNaughton et al24; Lilleston et al28; Yeung et al37
Interprofessional team management Stewart et al32; Woodland et al,27 Kim et al36
Refugee-specific policies Mortensen31; Philbin et al40; Tuepker and Chi41; Woodland et al39; Lilleston et al28
MacFarlane et al33; Philbin40
Data Mortensen31; Tuepker and Chi41
Organisational turf Stewart et al32; Tuepker and Chi41
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

11Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
health promoting environments, investing in person-cen-tred, culturally appropriate and easily accessible services, and evaluating coordination and service delivery efforts. Engaging policy-makers in knowledge translation and evidence-informed decision-making is one way to effec-tively advocate and provide legislative support in refugee health. In Lebanon, for example, where there are huge demands in meeting the health needs of a large Syrian refugee population, researchers engaged policy-makers in knowledge production (ie, research priority-setting), translation and uptake activities.42 This ultimately led to the hiring of a refugee health coordinator by the Lebanese Ministry of Public Health. The refugee health coordinator role functioned to support intersectoral collaboration, assisting in strategic planning and imple-mentation of action plans to respond to the health needs of Syrian refugees including helping with the development of refugee health information systems at the Ministry of Public Health.42 The UCL-Lancet Commission on Migra-tion and Health also supports knowledge translation by bringing together academics, policy-makers and health system experts to take an interdisciplinary approach to reviewing evidence, develop policy recommendations and disseminate these findings globally among policy-makers and institutions.43
Alternative models of care to reach vulnerable women and childrenAmong the studies that reported targeted interventions for women and children, alternative models of care were used. This included mobile health clinics, and programmes linked to schools to support screening and active case finding. These alternate models increased accessibility of essential health services, increased detec-tion of health conditions and improved coordination of care, and reduced feelings of social isolation.27 28 This suggests that flexible service delivery and innovation in mode of delivery should be considered when attempting to reach at risk refugee groups. Better collection and use of evidence on the needs of vulnerable refugee subgroups and how to target them are essential next steps to design appropriate service delivery models.
Policy insightsFrom the available evidence, the following are policy insights to inform greater integration of services and/or intersectoral collaboration. These recommendations are based on consistent facilitators and barriers identified across studies included in this review. They are critical starting points in enhancing programmes to better serve refugees while promoting efficiency in health systems.1. Strengthening the coordination between existing pro-
grammes through financing stronger referral systems and colocation of services.
2. Incentivising health and social service authorities to es-tablish and finance formal system navigator roles that connect all relevant services–provision of information Ta
ble
3
Ena
blin
g st
rate
gies
pre
sent
acr
oss
stud
ies
Str
ateg
yS
tud
ies
Hos
t co
mm
unity
en
gage
men
tC
alvo
et
al30
Sys
tem
nav
igat
ion
Cal
vo e
t al
30K
im e
t al
36M
cMur
ray
et a
l35W
ood
land
et
al39
Yeun
g et
al37
Lille
ston
et
al28
Inte
grat
ed h
ealth
and
so
cial
ser
vice
s th
roug
h ne
twor
ked
ap
pro
ach
Cat
arci
34K
im e
t al
36M
cMur
ray
et a
l35Ye
ung
et a
l37
Tran
slat
ion
sup
por
tK
im e
t al
36M
acFa
rlane
et
al33
McM
urra
y et
al35
McN
augh
ton
et a
l24W
ood
land
et
al27
Cow
ell e
t al
25G
urug
e et
al29
Act
ive
case
find
ing/
outr
each
McN
augh
ton
et a
l24Ve
rhag
en e
t al
26W
ood
land
et
al27
Gur
uge
et a
l29
Ref
ugee
-sp
ecifi
c se
rvic
e d
eliv
ery
and
acc
ess
to h
ealth
and
soc
ial
netw
orks
Mor
tens
en31
Phi
lbin
et
al40
Ste
war
t et
al32
Verh
agen
et
al26
Legi
slat
ive
sup
por
tP
hilb
in e
t al
40Tu
epke
r an
d C
hi41
Woo
dla
nd e
t al
39G
eltm
an a
nd C
ochr
an38
Cha
nges
in fu
ndin
g m
odal
ities
Tuep
ker
and
Chi
41
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

12 Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
technology tools can help support this function and better manage the network of available programmes.
3. Engaging host communities to enhance understand-ing, reduce stigma and to create an enabling environ-ment for policies that protect refugees and their rights to social determinants of health.
4. Communicating the availability of programmes and services through cultural mediators and establishing formal translation and transport services to improve access.
5. Establishing training and resources for providers to (A) better understand the needs of refugee communi-ties, (B) be aware of available and relevant services for referral across sectors and (C) more efficiently manage cases.
limitations and future directionsOur review was limited by the scarcity of evidence in this area. Due to this, all relevant studies were included, there-fore, quality and rigour may vary. Some key programmes and approaches may be missing due to interventions occurring at the individual level instead of at the systems level, as well as not having been published in academic literature. Individual health providers or organisations will navigate barriers in health systems through tacit and experiential knowledge that is often not documented. Data will be further amplified by conducting key infor-mant interviews in selected countries.
As others have noted, the literature on intersectoral collaboration disproportionately focuses on high-income countries.44 It is, therefore, no surprise that the evidence for this review largely came from high-income countries with only two studies conducted in upper-middle income and two in low-income countries. This may affect the generalisability of the findings reported here as low-in-come and middle-income countries have greater coordi-nation challenges to overcome due to fragmented systems and weak governance.45 Additionally, according to the latest report from the United Nations Refugee Agency, approximately 85% of refugees are hosted in developing nations.46 More evidence and special consideration is needed in these contexts with respect to refugee health, particularly for those most at risk subgroups such as women, children and the elderly.
Although there exists reaffirmed enthusiasm in inter-sectoral approaches to achieving global health agendas such as the SDGs, it has been found that the lack of quality evidence represents an essential hurdle to evidence-informed decision-making for the development of cross-cutting policies and governance required for sustained intersectoral collaboration.44 This pattern of a dearth of evidence was seen in our review. Additionally, most of what has been written has not been grounded in relevant theories or frameworks.45 Our use of frameworks to structure our analysis is a step forward in addressing this issue. Generating high-quality data in health systems and policy research for migrant health and on inter-sectoral approaches has been identified as a research
priority.44 47 Future research should, therefore, also consider the structured evaluation of evidence through a frameworked approach.
COnClusIOnRefugees experience individual, institutional and system-level obstacles when seeking healthcare. To ensure adequate health services tailored to this vulnerable population, conducting research and gathering quality evidence on integrated and intersectoral approaches is a top priority. This scoping review has highlighted important gaps in current knowledge and made sugges-tions for future research relevant to key themes.
Our findings indicate that policies aiming at inte-grating services and fostering intersectoral action should consider system-level approaches such as the coloca-tion of services, transportation support and establishing system navigator roles. Communication challenges due to language barriers should also be addressed with a view of providing culturally sensitive programmes. There is also a need to strengthen the capacities of front-line providers and managers, to improve their knowledge of available services as well as their ability to provide care to special-ised vulnerable groups such as refugees. Engaging host communities around a human rights-focused strategy to the health of refugees is also fundamental to address discrimination and stigma. Current gaps in knowledge found in our study represent an untapped potential for improvements to financial and human resource efficiency in health systems. Given the limited evidence, we found in our scoping review, the momentum for continued research should be sustained.
Acknowledgements The authors would like to thank Karolinska Institutet librarians, Magdalena Svanberg and Gun Brit Knutssön, for their contributions, specifically in running the search and identifying appropriate databases. We are also grateful to WHO Euro for their discussions and suggestions in the early stages of this project.
Contributors GT together with librarians at Karolinska Institutet identified databases and planned the literature search. SH and DJ drafted the paper and incorporated coauthor feedback, SH and DJ abstracted data from peer-reviewed literature. SC, EVL, GT and PF provided critical feedback and comments on the manuscript. SC and SH acted as secondary reviewers.
Funding No funding was obtained for this project. In-kind time contributions from staff at the Alliance for Health Policy and Systems Research and SIGHT have made this possible.
Competing interests None declared.
Patient consent for publication Not required.
ethics approval Ethics approval was not required for this scoping review as human subjects are not involved.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No data are available.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from

13Ho S, et al. BMJ Open 2019;9:e029407. doi:10.1136/bmjopen-2019-029407
Open access
reFerenCes 1. OHCHR. The Right to Health. Geneva, Switzerland, 2008. 2. Tangcharoensathien V, Mills A, Palu T. Accelerating health equity: the
key role of universal health coverage in the Sustainable Development Goals. BMC Med 2015;13:101.
3. UNHCR. Convention and Protocol relating to the status of refugees. Geneva, Switzerland, 2010.
4. UNHCR. UNHCR viewpoint: ‘Refugee’ or ‘migrant’ – Which is right? Geneva, Switzerland, 2016.
5. Rechel B, Mladovsky P, Ingleby D, et al. Migration and health in an increasingly diverse Europe. Lancet 2013;381:1235–45.
6. Council for the EU. Council Directive 2003/9/EC of 27 January 2003 Laying Down 453 Minimum Standards for the Reception of Asylum Seekers in Member States. Off J Eur Union 2003.
7. OHCHR. General Recommendation 30. Discrimination against non-citizens. Geneva, Switzerland, 2004.
8. Jackson-Bowers E, Cheng I-H. Meeting the primary health care needs of refugees and asylum seekers. Res Roundup 2010.
9. Gostin LO, Magnusson RS, Krech R, et al. Advancing the Right to Health-The Vital Role of Law. Am J Public Health 2017;107:1755-1756.
10. Joshi C, Russell G, Cheng IH, et al. A narrative synthesis of the impact of primary health care delivery models for refugees in resettlement countries on access, quality and coordination. Int J Equity Health 2013;12:88.
11. Citizenship AGD of I and. Fact sheet 60 - Australia’s refugee and humanitarian program, 2012.
12. UN. Integrated Approaches to Sustainable Development Planning and Implementation. New York, USA, 2015.
13. Kett ME. Internally displaced peoples in Bosnia-Herzegovina: impacts of long-term displacement on health and well-being. Med Confl Surviv 2005;21:199–215.
14. Patel N, Kellezi B, Williams AC. Psychological, social and welfare interventions for psychological health and well-being of torture survivors. Cochrane Database Syst Rev 2014;11:CD009317.
15. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19–32.
16. Tricco AC, Lillie E, Zarin W, et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med Res Methodol 2016;16:15.
17. Peters MDJ, Godfrey CM, Khalil H, et al. The Joanna Briggs Institute Reviewers’ manual: methodology for JBI scoping review. Adelaide, Australia, 2015.
18. Center for Open Science. Open science framework. https:// osf. io/ 19. Javadi D, Langlois EV, Ho S, et al. Intersectoral approaches and
integrated services in achieving the right to health for refugees upon resettlement: a scoping review protocol. BMJ Open 2017;7:e016638.
20. Walt G, Shiffman J, Schneider H, et al. 'Doing' health policy analysis: methodological and conceptual reflections and challenges. Health Policy Plan 2008;23:308–17.
21. Atun R, de Jongh T, Secci F, et al. Integration of targeted health interventions into health systems: a conceptual framework for analysis. Health Policy Plan 2010;25:104–11.
22. WHO. Health in all policies: framework for country action. Geneva, Switzerland, 2014.
23. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8:45.
24. McNaughton DB, Hindin P, Guerrero Y. Directions for refining a school nursing intervention for Mexican immigrant families. J Sch Nurs 2010;26:430–5.
25. Cowell JM, McNaughton D, Ailey S, et al. Clinical Trial Outcomes of the Mexican American Problem Solving Program (MAPS). Hisp Heal Care Int 2009;7:178–89.
26. Verhagen I, Ros WJ, Steunenberg B, et al. Culturally sensitive care for elderly immigrants through ethnic community health workers: design and development of a community based intervention programme in the Netherlands. BMC Public Health 2013;13:227.
27. Woodland L, Kang M, Elliot C, et al. Evaluation of a school screening programme for young people from refugee backgrounds. J Paediatr Child Health 2016;52:72–9.
28. Lilleston P, Winograd L, Ahmed S, et al. Evaluation of a mobile approach to gender-based violence service delivery among Syrian refugees in Lebanon. Health Policy Plan 2018;33:767–76.
29. Guruge S, Hunter J, Barker K, et al. Immigrant women's experiences of receiving care in a mobile health clinic. J Adv Nurs 2010;66:350–9.
30. Calvo R, Rojas V, Waters MC. The effect of universal service delivery on the integration of moroccan immigrants in Spain: a case study from an anti-oppressive perspective. Br J Soc Work 2014;44:i123–i139.
31. Mortensen A. Public health system responsiveness to refugee groups in New Zealand: activation from the bottom up. Soc Policy J New Zeal 2011.
32. Stewart M, Anderson J, Beiser M, et al. Multicultural meanings of social support among immigrants and refugees. Int Migr 2008;46:123–59.
33. Macfarlane A, Singleton C, Green E. Language barriers in health and social care consultations in the community: a comparative study of responses in Ireland and England. Health Policy 2009;92:203–10.
34. Catarci M. Conceptions and strategies for user integration across refugee services in Italy. J Educ Cult Psychol Stud 2012.
35. McMurray J, Breward K, Breward M, et al. Integrated Primary Care Improves Access to Healthcare for Newly Arrived Refugees in Canada. J Immigr Minor Health 2014;16:576–85.
36. Kim MJ, Cho HI, Cheon-Klessig YS, et al. Primary health care for Korean immigrants: sustaining a culturally sensitive model. Public Health Nurs 2002;19:191–200.
37. Yeung A, Kung WW, Chung H, et al. Integrating psychiatry and primary care improves acceptability to mental health services among Chinese Americans. Gen Hosp Psychiatry 2004;26:256–60.
38. Geltman PL, Cochran J. A private-sector preferred provider network model for public health screening of newly resettled refugees. Am J Public Health 2005;95:196–9.
39. Woodland L, Burgner D, Paxton G, et al. Health service delivery for newly arrived refugee children: a framework for good practice. J Paediatr Child Health 2010;46:560–7.
40. Philbin MM, Flake M, Hatzenbuehler ML, et al. State-level immigration and immigrant-focused policies as drivers of Latino health disparities in the United States. Soc Sci Med 2018;199:29–38.
41. Tuepker A, Chi C. Evaluating integrated healthcare for refugees and hosts in an African context. Health Econ Policy Law 2009;4:159–78.
42. Langlois E V, Daniels K, Akl EA. Evidence synthesis for health policy and systems: a methods guide. Geneva, Switzerland 2018.
43. The UCL-Lancet Commission on Migration and Health. 2018. 44. Glandon D, Meghani A, Jessani N, et al. Identifying health policy
and systems research priorities on multisectoral collaboration for health in low-income and middle-income countries. BMJ Glob Health 2018;3:e000970.
45. Bennett S, Glandon D, Rasanathan K. Governing multisectoral action for health in low-income and middle-income countries: unpacking the problem and rising to the challenge. BMJ Glob Health 2018;3:e000880.
46. UNHCR. Global Trends Forced Displacement in 2017. Geneva, Switzerland, 2018. https://www. unhcr. org/ 5b27be547. pdf
47. Abubakar I, Aldridge RW, Devakumar D, et al. The UCL-Lancet Commission on Migration and Health: the health of a world on the move. Lancet 2018;392:2606–54.
on July 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2019-029407 on 1 July 2019. Dow
nloaded from