
ONTARIO GUIDE TO CASE COSTING Ministry of Health and Long ... · 5.3.1 Operating Room ... case...
158
ONTARIO GUIDE TO CASE COSTING Ministry of Health and Long-Term Care Version 6.1 Fiscal Year 2008/2009
Transcript of ONTARIO GUIDE TO CASE COSTING Ministry of Health and Long ... · 5.3.1 Operating Room ... case...

ONTARIO GUIDE TO CASE COSTING
Ministry of Health and Long-Term Care
Version 6.1 Fiscal Year 2008/2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Changes for Fiscal Year 2008/09 are highlighted in yellow
ONTARIO GUIDE TO CASE COSTING
Table of Contents THIS GUIDE ...............................................................................................................................................................5
HOW THIS MANUAL IS ORGANIZED .................................................................................................................5
CHAPTER 1: WHY THE INVESTMENT IN CASE COSTING? .........................................................................7
CHAPTER 2: OVERVIEW OF THE CASE COSTING METHODOLOGY .......................................................8 2.1 Conceptual Model of Case Costing .....................................................................................................................8 2.2 Introduction to the OCCI Case Costing Methodology.........................................................................................9 2.3 Four Steps of Case Costing................................................................................................................................13 2.4 Evolution of the OCCI Case Costing Methodology ..........................................................................................13
2.4.1 Changing Hospital Production—Program Management ......................................................................14 2.4.2 Extending the Methodology to Ambulatory, Complex continuing Care, Mental Health and Rehabilitation.....................................................................................................................................................14 2.4.3 A Framework for “Case” Costing ...........................................................................................................15
CHAPTER 3: STEP 1: GATHER THE DATA ......................................................................................................16 3.1 Financial Data....................................................................................................................................................16
3.1.1 MIS Standards ..........................................................................................................................................16 3.1.2 Functional Centre Cost Assignment........................................................................................................18 Allowable Recoveries and Revenues in Case Costing .....................................................................................23 3.1.3 Separating Inpatient, Outpatient and Non-Patient Operating Costs ...................................................23 3.1.4 Patient Revenue ........................................................................................................................................24 3.1.5 Other Hospital Costs ................................................................................................................................24
3.2 Cost Distribution Bases .....................................................................................................................................26 3.2.1 Workload ...................................................................................................................................................26 3.2.2 Patient Hours Data ...................................................................................................................................30
3.3 Patient Descriptive Data ....................................................................................................................................30 3.3.1 Data Quality ..............................................................................................................................................30 3.3.2 CIHI and OCCI Coding Requirements ..................................................................................................31 3.3.3 Coding System...........................................................................................................................................34 3.3.4 Linkage of Patient Descriptive Data with Cost Data .............................................................................34 3.3.5 Useful Additional Patient Descriptive Data............................................................................................35
CHAPTER 4: STEP 2: ALLOCATE INDIRECT COSTS....................................................................................36 4.1 Allocation of Indirect Costs vs. Distribution of Direct Costs ............................................................................36 4.2 Indirect Cost Allocation Using SEAM ..............................................................................................................36 4.3 Indirect Cost Allocation Bases ..........................................................................................................................36 4.4 What TCC Costs are to be Allocated as Indirect Costs?....................................................................................37
CHAPTER 5: STEP 3: CALCULATE FUNCTIONAL CENTRE UNIT COSTS OR INTERMEDIATE PRODUCT COSTS ...................................................................................................................................................40
5.1 The General Ledger, Accounting Guidelines, and Variable and Fixed Costs ...................................................40 5.2 Functional Centre Unit Costs.............................................................................................................................41
5.2.2 The Functional Centre Unit Cost Calculation........................................................................................42 5.2.3 Type 1 - Using Nursing Workload to Calculate Functional Centre Unit Cost ....................................42
5.3 Using the Patient Hours Methodology...............................................................................................................45
OCCI Version 6.1 Page 2 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
5.3.1 Operating Room........................................................................................................................................45 5.3.2 Obstetrics...................................................................................................................................................45 5.3.3 Emergency Room......................................................................................................................................45 5.3.4 Rehabilitation Inpatients..........................................................................................................................46 5.3.5 Complex Continuing Care .......................................................................................................................46
5.4 Method 2: Calculating Intermediate Product Costs ...........................................................................................47 5.4.1 Information Required to Calculate Intermediate Product Costs .........................................................47 5.4.2 Intermediate Product Cost Calculation ..................................................................................................48
5.5 New Tests/Intermediate Products ......................................................................................................................49 5.6 Relative Value Units..........................................................................................................................................49
CHAPTER 6: STEP 4: DISTRIBUTE COSTS TO PATIENTS...........................................................................51 6.1.1 Type 1: Distributing Functional Centre Unit Cost to Patients based on Workload ........................................51 6.1.2 Type 2: Distributing Functional Centre Unit Cost to Patients based on Patient Hours ..................................52 6.2 Intermediate Product Costing ............................................................................................................................53 6.3 Patient Cost Distribution Bases .........................................................................................................................53
CHAPTER 7: BRINGING IT ALL TOGETHER..................................................................................................55 7.1 Departmental Data is Interfaced with the Case Costing System........................................................................55 7.2 Options for Reporting Case Costs .....................................................................................................................56
7.2.1 Costs by Day of Stay (Submission Requirement effective FY 05/06) ...................................................56 7.2.2 Variable/Fixed Detail - Option for Internal Reporting .........................................................................57 7.2.3 Service-Specific Data Elements ...............................................................................................................57 7.2.4 Procedure Detail .......................................................................................................................................58
7.3 A Framework for “Case” Costing......................................................................................................................58 CHAPTER 8: DEPARTMENTAL CASE COSTING STANDARDS ..................................................................61
8.1 Nursing Inpatient Functional Centres ................................................................................................................61 8.2 Allied Health......................................................................................................................................................61 8.3 Clinical Nutrition...............................................................................................................................................62 8.4 Clinical Laboratory............................................................................................................................................62 8.5 Diagnostic Imaging............................................................................................................................................65 8.6 Financial Services..............................................................................................................................................67 8.7 Health Records ..................................................................................................................................................67
8.7.1 Ensuring Quality of Patient Descriptive Data ........................................................................................67 8.7.2 Coding of Basic and Optional Data Items Needed for Case Costing....................................................68 8.7.3 CIHI Mandatory Data..............................................................................................................................68
8.8 Information Systems..........................................................................................................................................69 8.9 Pharmacy/Drug Costs ........................................................................................................................................70
CHAPTER 9: AMBULATORY, CHRONIC CARE AND MENTAL HEALTH STANDARDS.......................74 9.1 Ambulatory Care ...............................................................................................................................................74 9.2 Mental Health and Chronic Care .......................................................................................................................75
CHAPTER 10: COSTING IN A PROGRAM MANAGEMENT HOSPITAL ....................................................79 10.1 Gathering Data................................................................................................................................................79 10.2 Allocating Indirect Costs .................................................................................................................................80 10.3 Calculating and Distributing Product Costs.....................................................................................................80 10.4 Product Line Costing .......................................................................................................................................81
CHAPTER 11: IMPLEMENTING CASE COSTING...........................................................................................82 11.1 Challenges of Implementation .........................................................................................................................82 11.2 Implementation Time-Frames..........................................................................................................................83 11.3 Implementation Sequence................................................................................................................................84 11.4 Education/Promotion/Orientation....................................................................................................................84 11.5 Data Flow Models and Methodologies ............................................................................................................85
OCCI Version 6.1 Page 3 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
CHAPTER 12: EVALUATING CASE COSTING.................................................................................................87 12.1 The Approach to Evaluation ............................................................................................................................87 12.2 MIS Functional Centre Framework .................................................................................................................88 12.3 Patient Identification for Linkage ....................................................................................................................89 12.4 Workload Measurement...................................................................................................................................89 12.5 General and Patient-Specific Supply Costs .....................................................................................................90 12.6 Labour Hours...................................................................................................................................................91
CHAPTER 13: FREQUENTLY ASKED QUESTIONS........................................................................................93
APPENDIX 1: THE CASE COSTING METHODOLOGY IN ACTION: A NUMERICAL EXAMPLE........96
APPENDIX 2: ALLOWABLE RECOVERIES AND REVENUES IN CASE COSTING (FOR 2008/09) ....104
OCCI Version 6.1 Page 4 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
This Guide
In keeping with the previous version of the Ontario Guide to Case Costing, this manual is intended to serve as a primary resource for learning and implementing case costing. It presents the methodology used to produce case costs and many of the important details that should be considered to get case costing started. As the Guide is reviewed, there are additional materials, such as the Canadian Institute for Health Information’s MIS (Management Information System) Standards and Ontario’s version of the MIS Standards, the Ontario Healthcare Reporting Standards (OHRS), that can be used as a reference to compliment the Guide. A list of these reference materials is found in Appendix A. Case costing relies on financial, clinical and statistical data. Prior to costing, there must be a review of departmental information and data collection and reporting systems. This manual is a practical reference and guidance to:
• Evaluate current systems capability • Develop an action plan • Implement the systems and procedure changes needed for case costing
This Guide has been revised from earlier versions. The principal changes in this version occur in the following areas:
• Presentation of the conceptual basis of the case costing methodology • A more thorough presentation of the costing standards • An example of the case cost calculation • The standards for chronic care mental health and ambulatory care costing • The standards for Patient Hours as the alternative approach to nursing cost allocation • The case costing methodology applied to program management • A chapter dedicated to answering frequently asked questions
It is expected that modifications to the case costing standards will continue to be made as hospitals change their approach to service delivery. The case costing standards must adapt to hospital innovations so that case cost data remains relevant and useful for management decision-making at all levels. The Guide reflects the knowledge and experience of the Ontario Case Cost Initiative hospital participants. A history of the Project and a profile of OCCI hospitals are found in Appendices B and C. With the contribution of the OCCI hospitals to the Guide, it will fulfill its purpose: to provide readers with a good understanding of case costing, and the issues and details of implementing case costing in the hospital.
How this Manual is Organized
The material in this manual is presented in logical progression.
Chapter Content 1 Outlines the potential uses of case costing data at the hospital level 2 Provides an overview of the case costing methodology.
Describe in detail the four general steps of the OCCI case costing methodology: • gathering and organizing data (Chapter 3) • allocating indirect costs (Chapter 4)
3 to 6 • calculating functional centre unit costs/intermediate product costs (Chapter 5)
• distributing costs to patients (Chapter 6) A numerical example illustrating the case costing methodology is presented in Appendix 1.
7 Describes the process of bringing together statistical, financial and clinical data; discusses the final output of the case cost data.
OCCI Version 6.1 Page 5 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
8 Provides the case costing standards for nursing, allied health, clinical nutrition, clinical laboratory, diagnostic imaging, financial services, health records, information systems and pharmacy.
9 Explains the costing requirements for ambulatory care, chronic care and mental health.
10 Describes the application of the case costing methodology to hospitals organized by program.
11 Discusses a general approach to implementing case costing
12 Provides tips to help evaluate the newly implemented case costing.
13
Presents Project Managers’ frequently asked questions in a question and answer format where questions are related to the implementation of the case costing methodology.
OCCI Version 6.1 Page 6 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 1: Why the investment in case costing?
In recent years, case costing has generated considerable interest and enthusiasm. It provides much needed data to inform decision-making at all levels in the hospital. Hospital managers have turned to case costing information when faced with important decisions about the types of services to deliver and how to deliver them. Many hospitals with case costing systems find the information invaluable for strategic and operational planning and management, especially in the current environment of decreasing resources, increased demand for services, and greater emphasis on quality. Case cost data has also been used to demonstrate good value for resources used, which is increasingly relevant in today’s focus on accountability in health care.
Hospitals already have financial and management reporting structures in place for tallying costs and reporting by functional centre (also known as department or cost centre) so why implement case costing if departmental financial information is readily available? The reason is that case costing allows another perspective when analyzing financial information. Case costing provides answers to important management and planning questions that cannot traditionally be answered with departmental management and financial information alone. These questions include:
• What are our top patient businesses (e.g., by program, referral area, funding source, etc.)? • What are our revenues and expenses in each business area? • Is there an opportunity to improve resource utilization for specific patients or groups of patients? • What are the variations in resource use among clinically similar patients? How can these variations be
reduced to increase overall quality and to direct our resources more appropriately? • What are the cost impacts of realigning programs? • What is a fair price to charge an out-of-country patient for a craniotomy? • How do case costs compare to our peers for similar patients? • What are the differences in costs between treatment options for a particular type of case? • Is it more expensive to provide certain laboratory services in-house or to purchase them from another
facility?
Case costing provides information to support many kinds of analysis and initiatives. OCCI hospitals also report using case cost data for the following activities:
• Evaluation/development of patient care treatment maps/critical care paths • Development of program budgets and variance reporting • Feasibility and impact analysis, e.g., adding a new program, physician, etc. • Productivity analysis/evaluation of program efficiency • Modeling (“what if...”) and forecasting • Evaluation of moving from inpatient to outpatient procedures • Comparison of hospital position (costs) vs. funding
Not only is case cost data important for hospital decision-making, but it can also be used in health care system reform efforts by providing support to hospital funding, research and policy development initiatives. More information on current and expected uses and analyses of case cost data can be found in Appendix D. Implementation of case costing does not need to be cumbersome. It takes effort to gather patient-specific cost and workload data, but the overall impact can be managed by carefully designing these systems. The key is to gather patient-specific data as a by-product of care delivery documentation and communications. This manual provides some helpful tips for successful implementation of case costing. The case costing approach described in this Guide generates case costs by integrating financial, clinical and statistical data. With case costing fully in place, new views can be generated to help answer operational management and planning questions while still providing the necessary departmental management information that the hospital is accustomed to using.
OCCI Version 6.1 Page 7 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 2: Overview of the Case Costing Methodology
In order to develop good cost data, first identify and understand what will be costed. Once a solid understanding of the context in which patient-specific costs are generated, explore the methodology that will assist in developing case costs. The OCCI standards are rules specific to the OCCI that are largely based on the MIS Standards and the OHRS. The OCCI methodology is operationalized through the OCCI standards that have been developed to ensure comparability and quality of the data. This chapter presents the conceptual model on which the OCCI case costing methodology is based. Then, the four steps to the case costing methodology are introduced. Lastly, the current issues identified in the evolution of case costing are explored.
2.1 Conceptual Model of Case Costing
In order to understand how to distribute the costs of services a patient receives during a hospital visit, it is important first to discuss the context in which the hospital produces these services. The hospital production function model shown in Figure 2-1 represents patient-specific costing. The model illustrates how a hospital uses a number of inputs (labour equipment, etc.) to produce services (x-ray, laboratory tests, nursing services, etc.) that a patient receives from the hospital. The challenge of case costing is to accurately identify the costs of these services and then to distribute the costs to each patient reflecting the cost of the care delivered. The production function model shows that the output of a hospital is a mix of services, or intermediate products, specific for each patient. These intermediate products for patient care are produced by a number of departments (e.g., Nursing, Pharmacy, etc.). Each department produces a range of intermediate products by combining inputs such as labour and capital. For example, an x-ray would be considered an intermediate product of the Diagnostic Imaging department.
OCCI Version 6.1 Page 8 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 2-1
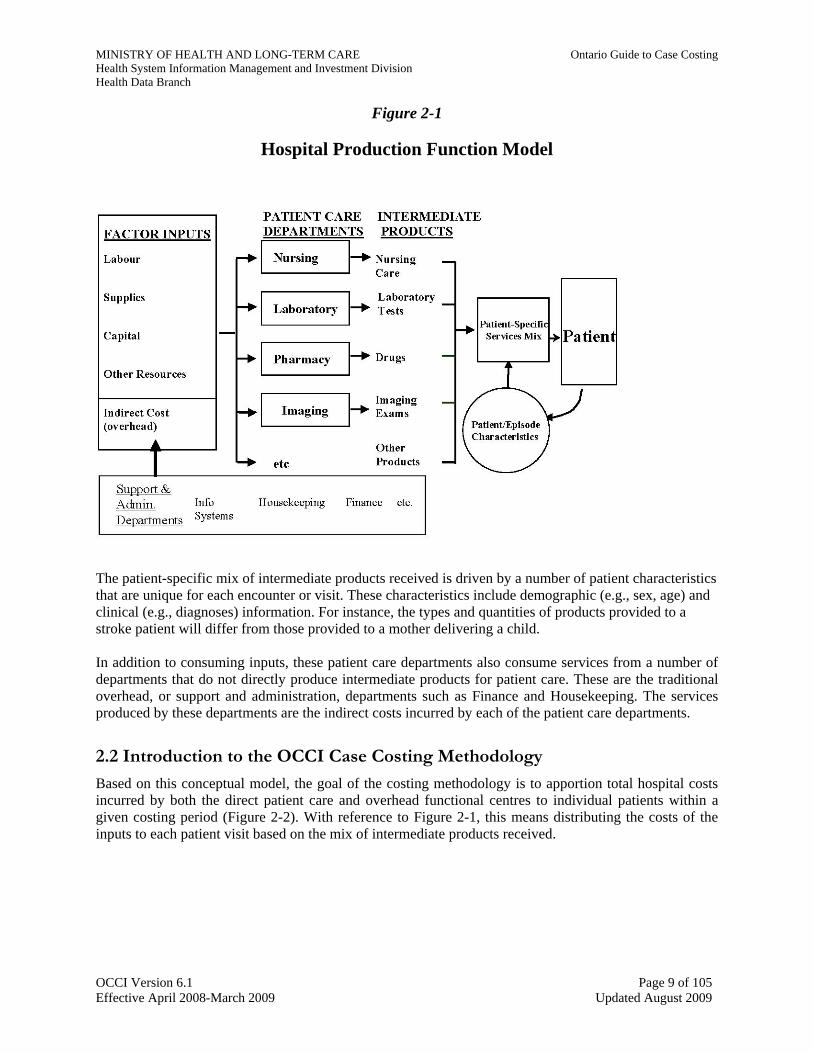
Hospital Production Function Model
The patient-specific mix of intermediate products received is driven by a number of patient characteristics that are unique for each encounter or visit. These characteristics include demographic (e.g., sex, age) and clinical (e.g., diagnoses) information. For instance, the types and quantities of products provided to a stroke patient will differ from those provided to a mother delivering a child. In addition to consuming inputs, these patient care departments also consume services from a number of departments that do not directly produce intermediate products for patient care. These are the traditional overhead, or support and administration, departments such as Finance and Housekeeping. The services produced by these departments are the indirect costs incurred by each of the patient care departments.
2.2 Introduction to the OCCI Case Costing Methodology
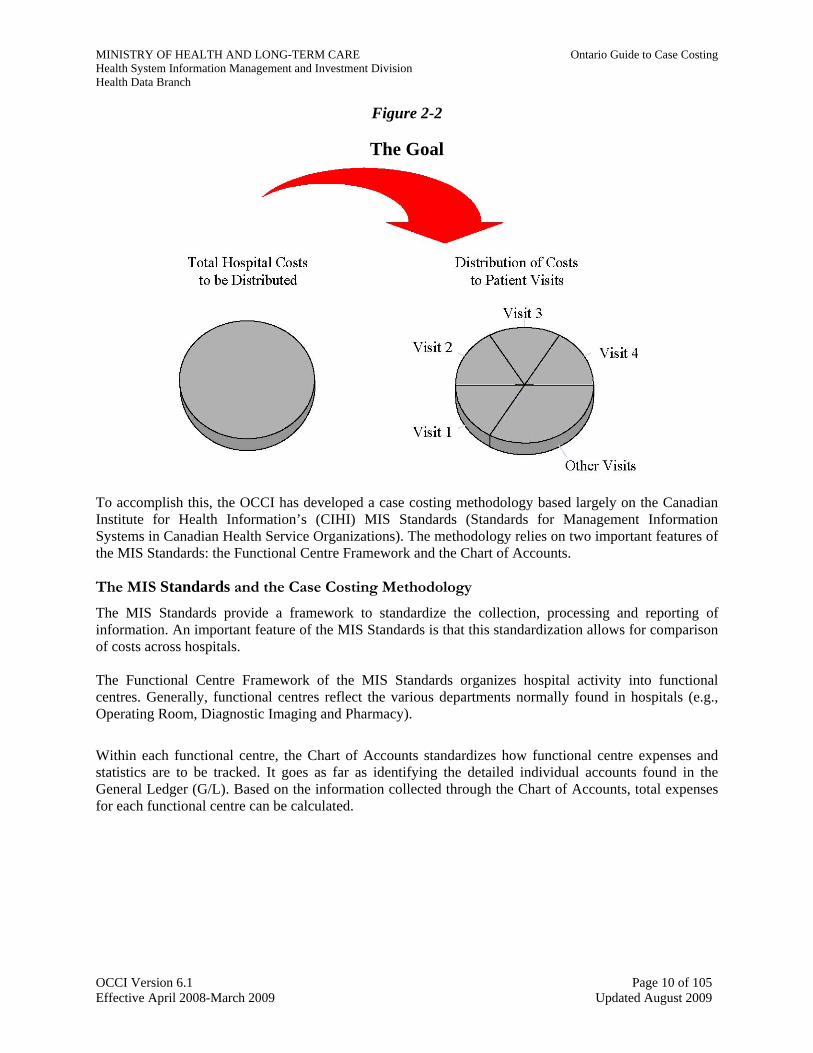
Based on this conceptual model, the goal of the costing methodology is to apportion total hospital costs incurred by both the direct patient care and overhead functional centres to individual patients within a given costing period (Figure 2-2). With reference to Figure 2-1, this means distributing the costs of the inputs to each patient visit based on the mix of intermediate products received.
OCCI Version 6.1 Page 9 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 2-2
The Goal
To accomplish this, the OCCI has developed a case costing methodology based largely on the Canadian Institute for Health Information’s (CIHI) MIS Standards (Standards for Management Information Systems in Canadian Health Service Organizations). The methodology relies on two important features of the MIS Standards: the Functional Centre Framework and the Chart of Accounts.
The MIS Standards and the Case Costing Methodology
The MIS Standards provide a framework to standardize the collection, processing and reporting of information. An important feature of the MIS Standards is that this standardization allows for comparison of costs across hospitals. The Functional Centre Framework of the MIS Standards organizes hospital activity into functional centres. Generally, functional centres reflect the various departments normally found in hospitals (e.g., Operating Room, Diagnostic Imaging and Pharmacy).
Within each functional centre, the Chart of Accounts standardizes how functional centre expenses and statistics are to be tracked. It goes as far as identifying the detailed individual accounts found in the General Ledger (G/L). Based on the information collected through the Chart of Accounts, total expenses for each functional centre can be calculated.
OCCI Version 6.1 Page 10 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 2-3
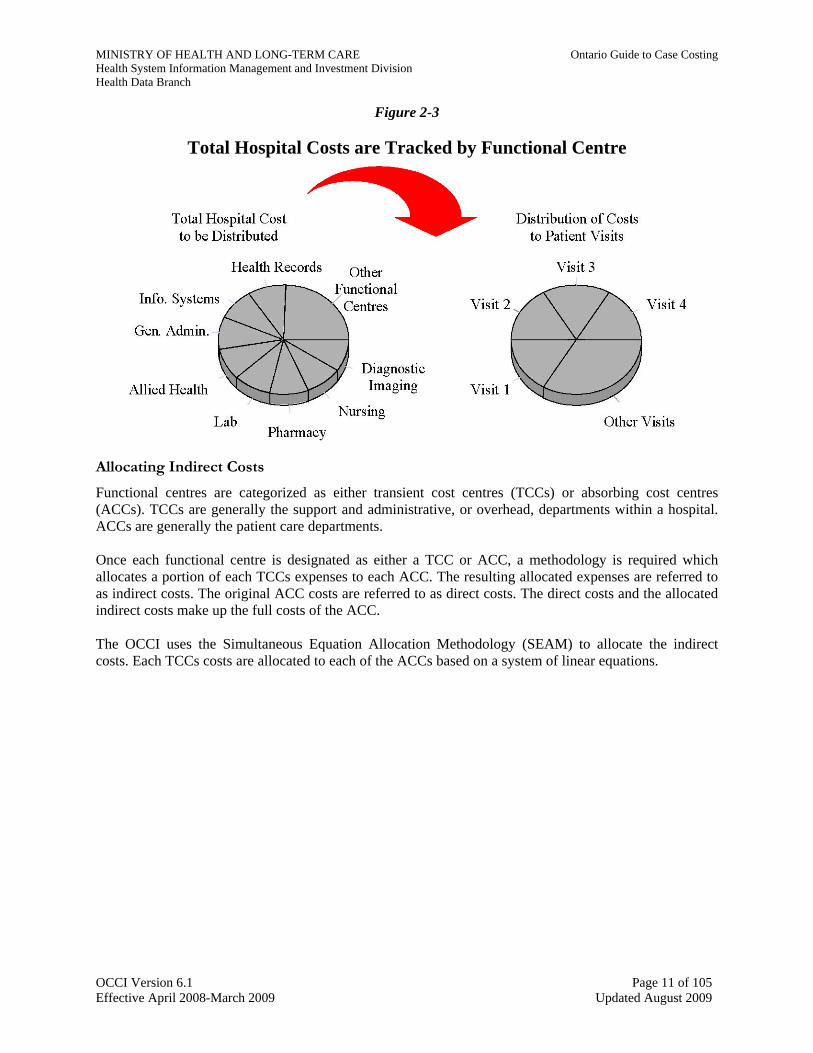
Total Hospital Costs are Tracked by Functional Centre
Allocating Indirect Costs Functional centres are categorized as either transient cost centres (TCCs) or absorbing cost centres (ACCs). TCCs are generally the support and administrative, or overhead, departments within a hospital. ACCs are generally the patient care departments. Once each functional centre is designated as either a TCC or ACC, a methodology is required which allocates a portion of each TCCs expenses to each ACC. The resulting allocated expenses are referred to as indirect costs. The original ACC costs are referred to as direct costs. The direct costs and the allocated indirect costs make up the full costs of the ACC. The OCCI uses the Simultaneous Equation Allocation Methodology (SEAM) to allocate the indirect costs. Each TCCs costs are allocated to each of the ACCs based on a system of linear equations.
OCCI Version 6.1 Page 11 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 2-4
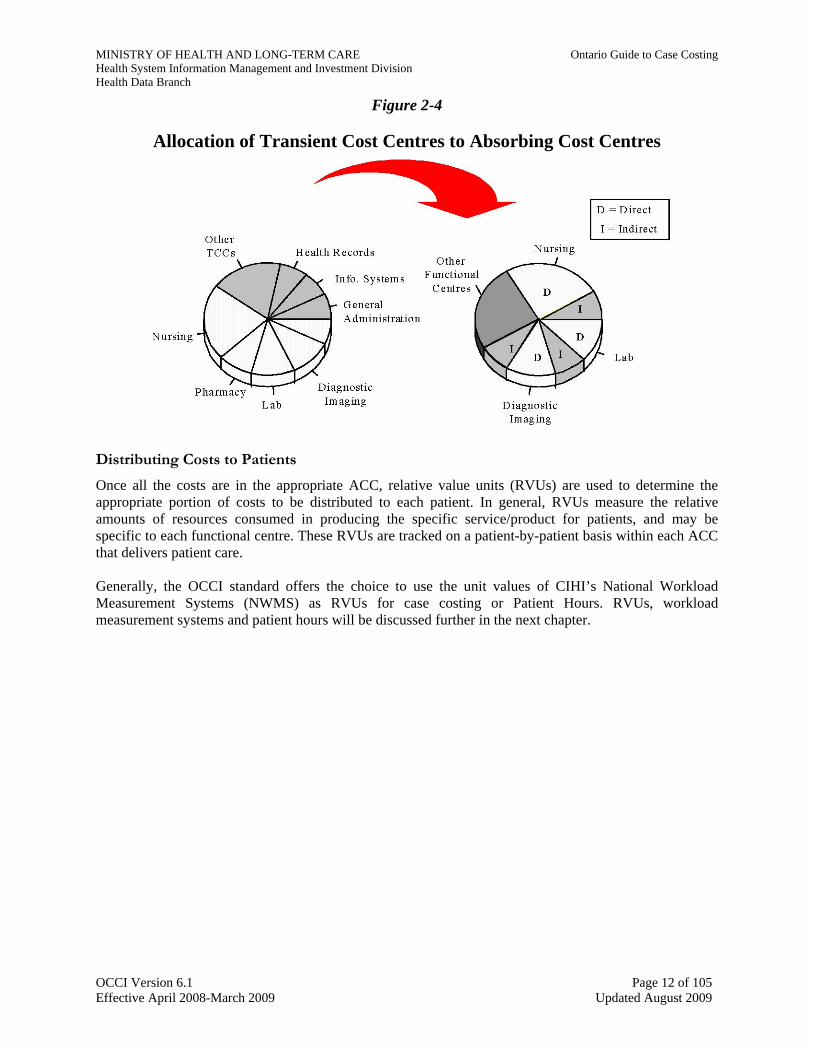
Allocation of Transient Cost Centres to Absorbing Cost Centres
Distributing Costs to Patients Once all the costs are in the appropriate ACC, relative value units (RVUs) are used to determine the appropriate portion of costs to be distributed to each patient. In general, RVUs measure the relative amounts of resources consumed in producing the specific service/product for patients, and may be specific to each functional centre. These RVUs are tracked on a patient-by-patient basis within each ACC that delivers patient care. Generally, the OCCI standard offers the choice to use the unit values of CIHI’s National Workload Measurement Systems (NWMS) as RVUs for case costing or Patient Hours. RVUs, workload measurement systems and patient hours will be discussed further in the next chapter.
OCCI Version 6.1 Page 12 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
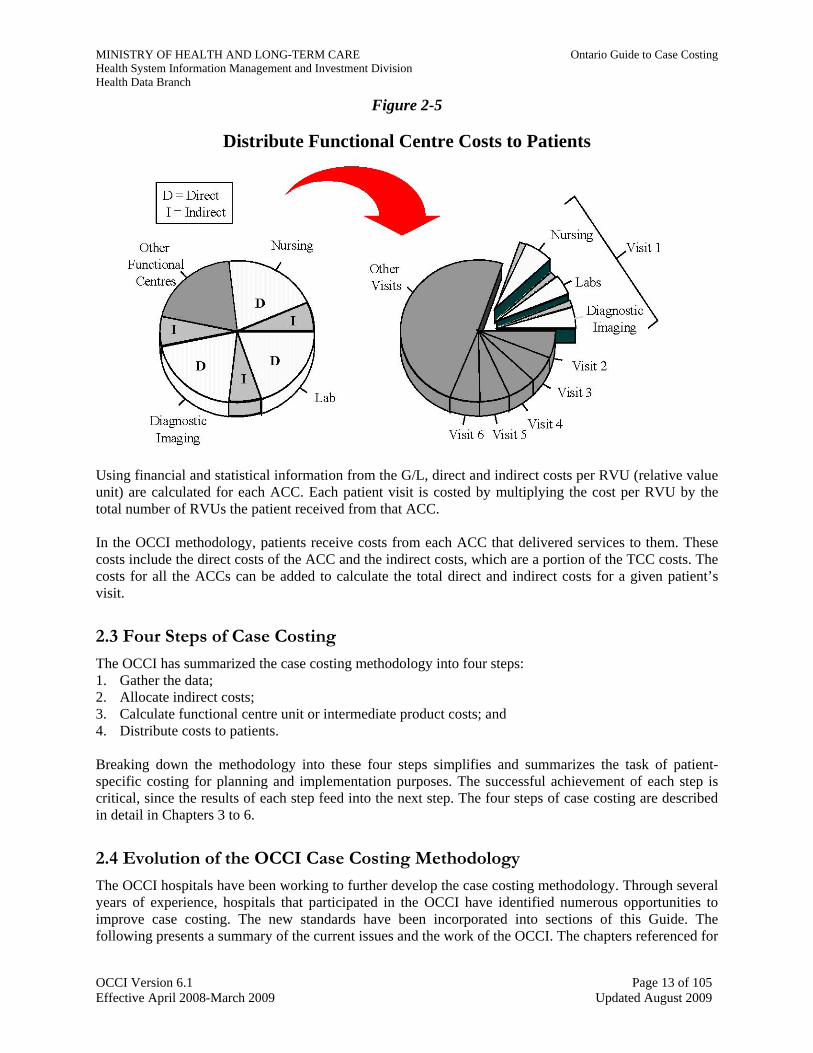
Figure 2-5
Distribute Functional Centre Costs to Patients
Using financial and statistical information from the G/L, direct and indirect costs per RVU (relative value unit) are calculated for each ACC. Each patient visit is costed by multiplying the cost per RVU by the total number of RVUs the patient received from that ACC. In the OCCI methodology, patients receive costs from each ACC that delivered services to them. These costs include the direct costs of the ACC and the indirect costs, which are a portion of the TCC costs. The costs for all the ACCs can be added to calculate the total direct and indirect costs for a given patient’s visit.
2.3 Four Steps of Case Costing
The OCCI has summarized the case costing methodology into four steps: 1. Gather the data; 2. Allocate indirect costs; 3. Calculate functional centre unit or intermediate product costs; and 4. Distribute costs to patients. Breaking down the methodology into these four steps simplifies and summarizes the task of patient-specific costing for planning and implementation purposes. The successful achievement of each step is critical, since the results of each step feed into the next step. The four steps of case costing are described in detail in Chapters 3 to 6.
2.4 Evolution of the OCCI Case Costing Methodology
The OCCI hospitals have been working to further develop the case costing methodology. Through several years of experience, hospitals that participated in the OCCI have identified numerous opportunities to improve case costing. The new standards have been incorporated into sections of this Guide. The following presents a summary of the current issues and the work of the OCCI. The chapters referenced for
OCCI Version 6.1 Page 13 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
each issue contain further details as well as some discussion of the impact they will have on the OCCI case costing methodology.
2.4.1 Changing Hospital Production—Program Management
Ontario hospitals have recently undergone radical changes in the way they deliver patient care. Traditionally, hospitals have been organized such that the departments that produce the intermediate products are divided along discipline-specific lines, shown in Figure 2-1.
Many hospitals have begun moving towards organizing and managing patient care delivery through the program management approach. This approach involves programs, instead of departments, being directly responsible for delivering direct patient care. The programs displace traditional functional centres as the primary organization unit for the production of intermediate products. Each program may produce a broad range of intermediate products, from nursing care to laboratory tests to social work services. Program management involves more than just re-organizing departments into programs. A key component of program management is the use of multi-skilled workers. Patient care staff, and possibly support staff, within a patient care program would be multi-skilled to provide a variety of services and products. Since any staff can provide a range of intermediate products, systems to accurately capture and cost each activity within the program are required. Hospitals have implemented many aspects of program management to varying degrees. The challenge now is to develop a costing methodology that can be applied to any hospital setting such that the costs produced are relevant for internal decision-making and are externally comparable to other hospitals, including those that are organized departmentally. The lack of a “standardized” approach for program management organization poses a number of issues. The OCCI has examined options to develop case costs in a program management organization. Chapter 11 presents the issues and methodology to calculate costs in this setting.
2.4.2 Extending the Methodology to Ambulatory, Complex continuing Care, Mental Health and Rehabilitation
The OCCI case costing methodology was originally developed to cost acute inpatients and was then modified for day surgery patients. The methodology has also been extended to cost Ambulatory, Complex Continuing Care patients, Mental Health and Rehabilitation. Many aspects of the methodology for Ambulatory, Complex Continuing Care , Mental Health and Rehabilitation are the same as for acute inpatients. Utilization/workload is captured on a patient-specific basis, financial information is tracked on a standardized basis using the MIS Standards, and patients are assigned costs based on the total number of intermediate products received. To collect the patient descriptive data for ambulatory care, the OCCI has adopted the CIHI National Ambulatory Care Reporting System (NACRS). NACRS is a service provider-based system whereby a minimum data set, with patient-specific demographic (e.g., age, sex) and clinical (e.g., diagnosis and procedure codes) data, is captured for each outpatient functional centre that has provided care. To define the complex continuing care and mental health encounter, the OCCI standards require the collection of the InterRAI Complex continuing Care Minimum Data Set (MDS v2), RAI –Mental Health Assessment and the Rehab Minimum Data Set. The OCCI case costing methodology and the case costing standards described in Chapters 3 to 6 apply to complex continuing care and ambulatory care, with specific standards summarized in Chapter 10.
OCCI Version 6.1 Page 14 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
2.4.3 A Framework for “Case” Costing The care provided for a given health condition can involve a variety of different interactions between the patient and the hospital. It would be of great value to be able to measure the cost of treating a patient over the entire episode of illness. For example, many patients now receive follow-up care on an outpatient basis after being admitted to hospital for a surgical procedure. The outpatient visit is related to the same health condition that required surgery. The ability to link the two visits together would provide a better estimate of the total costs for treating that condition. The OCCI has developed a six-level framework that links the various visits a patient has across different health care facilities for the treatment of a given health condition. The current information systems in Ontario hospitals allow the costs of the individual visit to be determined. Implementation of the proposed framework, described in Chapter 8, will identify the true “case” costs across various health care providers.
OCCI Version 6.1 Page 15 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 3: Step 1: Gather the Data A standardized methodology has been developed with the goal of producing high quality case cost data. Reliable and valid data— financial, statistical and patient descriptive data—is necessary to produce high quality case costs. To obtain the data, follow data preparation and collection rules, audit the processes that generate the data and ensures that a particular case’s costs can be traced.
Data Reliability and Validity Reliability is the degree of consistency with which an instrument measures the attribute it is supposed to be measuring. Validity is the degree to which an instrument measures what it is supposed to measure.
- Pollit and Humgler, 1983
In the four chapters that follow (Chapters 3 to 6), there is a focus on what must be done to produce high quality cost data, by categorizing, allocating, and distributing costs. These standards were originally developed for acute inpatient and day surgery costing. Gathering data is the first step in the case costing process. The OCCI data standards for gathering financial and statistical data are based largely on the MIS Standards, which provide the framework for collection and organization of hospital statistical and financial data. Standards are necessary to ensure the comparability of data. In this chapter, the OCCI standards for the collection of financial, statistical and patient descriptive data (health records data) are presented.
3.1 Financial Data
3.1.1 MIS Standards The MIS Standards define a framework for the compilation and comparison of financial and statistical data. Since the MIS Standards are the starting point for case costing, hospitals wishing to implement case costing should become familiar with the MIS Standards. The standards presented here expand or clarify accounting issues and their treatment, as well as any additions to or modifications of the existing MIS Standards needed for case costing purposes. Appendix E provides an overview of the MIS Standards and the Ontario Healthcare Reporting Standards (OHRS).
The Glossary of Terms in the MIS Standards and OHRS provides definitions for key accounting terms. Some of those definitions are reproduced in this manual. Some definitions have been modified or were developed specifically to meet the objectives of Ontario case cost development.
OHRS Account Codes Functional centre numbers are listed in the Ontario Healthcare Reporting System User Guide version 6.2, Appendix A. Revenue and expense codes are listed in the Ontario Healthcare Reporting System User Guide version 6.2, Appendix B. See the OHRS Glossary for functional centre and revenue and expense account definitions.
Hospitals must adhere to the account structure presented in the MIS Standards and the account codes presented in the OHRS Chart of Accounts. When they differ, the OHRS overrides the MIS Chart of Accounts. With the province-wide implementation of MIS Account Codes, hospitals are encouraged to convert fully. If a hospital does not use OHRS General Ledger account codes, it is required that the account codes used be mapped into OHRS functional centres and revenue and expense accounts.
OCCI Version 6.1 Page 16 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Note that the “roll-up” is built into the MIS Chart of Accounts numbering system. To safeguard the “roll-up”, be sure to define the functional centres at the lowest level needed to break out costs internally, and be sure that all of a lower level account rolls up to one account at the next level up. For fiscal year 05/06 submissions, small hospitals are required to submit case cost data at MIS Level 3 accounts while all other hospitals will need at least some MIS Level 4 accounts and some will need to go to MIS Level 5, depending upon size and complexity of service.
Functional Centres - High Cost Equipment
One way to isolate high equipment costs and distribute them to the patients who receive their benefit is to establish additional functional centres specifically for such high cost equipment. This approach is especially appropriate if the non-labour cost per service exceeds $250. Note that a suitable relative value unit system is needed to distribute costs to patients. This mechanism of establishing separate functional centres for high cost equipment enables hospitals to develop more accurate patient case costs. Hospitals can still compare their costs with those of hospitals that do not have these functional centres by rolling up to a common level, such as Level 3, and comparing at that level.
MIS Code Format Asterisks (*) are used in an account code to indicate that any valid code may be used in this position. For example, Acct 71 4 15 ** ** refers to all Diagnostic Imaging functional centres
Several specific functional centres that isolate high cost equipment have already been defined in the MIS Standards. They are listed in the table below.
Table 3.1
Functional Centres with High Cost Equipment OHRS Functional Centre
Number Functional Centre Cost Item
71 3 40 25 ** Day/Night Care, Surgical/Procedural Equip/Supplies 71 4 10 25 ** Clinical Chemistry Equipment 71 4 15 ** X-Ray Equip/Supplies 71 4 15 25 Computed Tomography Equipment 71 4 15 30 ** Diagnostic Ultrasound Equipment 71 4 15 40 Nuclear Medicine Equip/Supplies 71 4 15 44 Cardiac Catheterization Laboratory Supplies 71 4 15 70 Magnetic Resonance Imaging Equipment
Functional Centres for Patient Care Administration and Support
Patient Care departments with several functional centres and a large administrative and support staff may find it beneficial to set up a specific administrative and support functional centre for the department. The MIS Standards provide a suggested account structure for functional centres such as Laboratory, Diagnostic Imaging, Pharmacy and Nursing. It is easier to achieve a representative distribution of these administrative and support costs to patients using this approach. Some further considerations on the use of functional centres for departmental administration and support are discussed in section 3.1.2, Functional
OCCI Version 6.1 Page 17 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Centre Cost Assignment. Note that patient care administration and support functional centre costs are assigned to the patient care functional centres as a direct cost.
3.1.2 Functional Centre Cost Assignment The Functional Centre Reporting sections of the MIS Standards specify how financial and statistical data should be collected and organized for case costing. Assigning expenses to the proper functional centres is crucial to achieve accurate case costs. In this section, the OCCI standards are described, which are based on the MIS Standards for assigning hospital expenses to functional centres. There is also a detailed explanation of the OCCI standards associated with the following expenses: salaries and benefits, physician compensation, patient care administration and support, supplies, drugs, amortization and leasing of equipment, and maintenance of major clinical equipment.
Salaries and Benefits
Salaries and benefits are usually the largest component of a functional centre’s costs. The MIS secondary account codes for salaries and benefits are as follows:
310** Worked Salaries 330** Benefit Salaries 340** Benefit Contributions 390** Purchased Service Salary (or Fee-for-Service) Worked salaries, benefit salaries and purchased service salaries represent the three categories of salaries. Benefits contributions are also known as fringe benefits. The OCCI standards require that salaries and benefits of personnel be assigned to the functional centres in which they work. This standard applies to all unit-producing personnel (those capturing workload), medical personnel, and management and operational support personnel. More information on labour costs related to these broad occupational groups is found in this section under Labour Hours Data, Patient Care Administration and Support, and Physician Salaries and Fees. Education and research staff salaries are assigned differently from the salaries of other hospital personnel. If education and research staff perform unit-producing work instead of regular functional centre staff, these hours spent performing unit-producing work and the associated salaries are assigned to the functional centre receiving the service. Otherwise, their hours and salaries are assigned to the appropriate Education or Research functional centre. Students receiving compensation should have their costs distributed to the appropriate functional centres at the actual rate of compensation. Students who are not compensated by the hospital will have no labour expenses assigned to functional centres. An employee’s uncompensated overtime hours will also be assigned no value. Although worked hours are not reported for unpaid students and unpaid overtime hours, workload is still collected, effectively reducing the cost per RVU. There should be mechanisms in place to distribute benefits to the appropriate functional centres. Depending on the accounting system, there might be a need to post benefits into one account, and then distribute benefit costs to each functional centre in proportion to salaries. To maintain comparability of reporting among hospitals, costs such as benefit contribution expense must not be treated as overhead (indirect costs).
MIS Standards Change Benefits Accounting Hospitals historically have excluded benefits Contributions (Fringe Benefits) from functional centre reporting. MIS Standards require distribution of Benefits
OCCI Version 6.1 Page 18 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Hospitals should ensure that year-end payroll accruals are distributed to the functional centres. Both salaries and benefit contributions need to be accrued. Accruals are necessary in order to match salary and benefit contributions with workload statistics to provide a more accurate cost per workload unit.
Labour Hours Data
Labour costs account for about three-quarters of a hospital's operating costs. Because labour is such a large cost component, incorrectly assigned labour costs can lead to distorted case costs, even at the summary reporting level used for developing Ontario case costs. Most hospitals face a major challenge in documenting staff assignments, especially in Nursing where many temporary, casual, agency and float pool staff may work their shifts on different units each day. Developing correct labour costs for each functional centre requires good information on shifts worked in each functional centre.
It is expected that a hospital's recording system will have the ability to assign an employee’s hours to the functional centre in which they worked, to the nearest hour. This will ensure precise labour charges to each functional centre. For case cost development, it is also important that labour costs (hours), in each functional centre, are assigned to the proper MIS Secondary Account. Remember that staff involved in both unit-producing and management and support activities to a significant extent, must have their hours (and benefits) split between the Management and Operational Support (3 10 **), and Unit-Producing (3 50 **) Secondary Accounts. Accurate recording of labour hour data will provide meaningful information for managing workload and staffing levels, and for monitoring productivity and cost effectiveness. The division of labour hours into unit-producing and management and operational support hours is also important for Step 3 of the case costing process, when labour costs will be designated as variable or fixed (see Section 5.1). Medical personnel labour hours are treated differently than unit producing, management and operational support labour hours. Medical personnel are compensated for their professional medical services, either on a fee-for-service or salary basis. Physicians do not collect workload, and their labour hours and expenses are assigned to the Medical Personnel (3 90 **) Secondary Accounts. The section entitled Physician Salaries and Fees provides greater detail on how to handle physician activity. The hospital's central payroll time and attendance system will most likely be the feeder system which contributes the labour hours to the General Ledger Chart of Accounts and Statistics on an ongoing basis. Functional centres are responsible for accurately recording the time being inputted into the payroll system (either manually or electronically). As an alternative to using the payroll system, hours could be entered through a separate entry module linked to the workload management or costing system. The payroll system has the advantage that the labour cost output to the costing system module can come directly from the hospital's financial systems, so that existing management reports will reflect the more accurate labour distribution immediately. Any other approach could mean double data entry and create the potential for data reconciliation problems. Department-specific labour data requirements will be noted later in Chapter 8, Departmental Case Costing Standards.
Physician Salaries and Fees
Most hospitals have some physicians who are remunerated by the hospital through a contractual arrangement. Typically, physician remuneration consists of fee-for-service (e.g., radiologists) or salary
OCCI Version 6.1 Page 19 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
(e.g., pathologists). Compensation expenses for physicians, as with other hospital workers, should be charged as a direct cost to the functional centre in which the individual works.
Physicians who cannot be identified clearly with one functional centre prior to service provision should have their expenses charged to the appropriate Medical Resources functional centre (71207, 71307, 71507). These costs must be eventually cleared by assigning them to patient care functional centres, as direct costs, based on an estimate of time the physicians spent providing services to each of the functional centres. These costs should be distributed to patients based on workload collected in the functional centre.
Sometimes physicians perform management functions in addition to patient care work. In this case, remember that hours spent performing management functions must be assigned to the appropriate patient care administration functional centre, if this is a separate functional centre in the hospital. For example, a physician who is also the head of the Diagnostic Imaging department would have to record the hours spent performing management functions in the Diagnostic Imaging—Administration functional centre (7141510).
Note that for case costing is only interested in physician compensation if the physician is remunerated by the hospital. Many physicians (e.g., surgeons) working in the hospital are not compensated by the hospital but rather are directly compensated through the Ministry of Health and Long-Term Care via OHIP billings.
Patient Care Administration and Support
Particularly in larger hospitals, patient care administration and support functional centres have been established to isolate general management and support function staff and supply costs from those of the nursing, diagnostic or treatment areas. In smaller hospitals, these management and support functions are simply another activity of unit-producers and are already part of the functional centre’s costs. All costs contained in separate support and administration functional centres must be cleared through distribution to the functional centres that they support. These costs should be assigned as a direct cost to the patient care centres they support. Total functional centre workload, total department cost or estimates of the time staff spend providing services to functional centres can be used as the basis for the assignment. Patient care administration and support functional centres include the following:
• Inpatient Nursing
7120510 - Nursing Administration 7120520 - Clinical Resources (centralized)
20 - IV Therapy 40 - Enterostomal Therapy
2092 - Transplant Coordination/Organ Procurement 2094 - Palliative Care Team
7120600 - Program Management Administration • Ambulatory Care
7130500 - Ambulatory Care Administration 7130600 - Program Management Administration • Clinics
7135005 - Clinic Administration • Diagnostic and Therapeutic Services
7140600 - Program Management Administration
OCCI Version 6.1 Page 20 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
• Laboratory
7141010 - Clinical Laboratory - Administration 7141015 - Clinical Laboratory - Support Services 7141020 - Specimen Procurement and Dispatch • Diagnostic Imaging
7141510 - Diagnostic Imaging - Administration • Respiratory Therapy
7143510 - Respiratory Therapy - Administration • Pharmacy
7144010 - Pharmacy – Administration • Rehabilitation Services
7144900 - Rehabilitation Services - Administration • Community Services
7150500 - Community Services Administration
Supplies
For case costing purposes, distinguish between general and patient-specific supplies since these costs are distributed to patients differently. In the section that follows, general and patient-specific supplies are defined as well as how these costs are assigned to functional centres.
General Supplies General Supplies include all stationery, medical supplies, surgical supplies, ward stock drugs, laundry and other miscellaneous supply items. General supply items are charged to the functional centre using the supplies. The costs for general supplies are a component of each functional centre's total direct operating costs and are included when the functional centre's cost per unit is determined.
Patient-Specific Supplies It is not practical to “charge” all supplies to patients when doing case costing because it would mean accounting for each dressing, each tongue depressor, etc. However, if the costs of high-cost supplies are averaged, individual case costs could be distorted. To address this issue, a dollar limit has been established by the OCCI for tracking supplies or supply assemblies of $250 or greater to the patient. Therefore, any item or related grouping of supplies, or "supply assemblies" with a unit or assembly cost of $250 or more should be tracked to the patient as a patient-specific supply. A set of separate accounts in MIS broad group 5 is used to record patient-specific supplies.
Note that the MIS Standards have eliminated the $250 threshold for tracking patient-specific supplies as of April 1, 1999. The MIS Standards now require hospitals to track certain expensive supplies, which are “traceable” to patients. The OCCI does not require hospitals to capture supply or supply assemblies less than $250. However, decide to track items or assemblies that cost less than the $250 limit, especially those items which account for a large percentage of the functional centre's total supply cost. Typically, there are high cost supplies in the Operating Room and
OCCI Version 6.1 Page 21 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Diagnostic Imaging.
A supply assembly is a group of supply items that is used together in a patient-specific procedure. For example, a supply assembly for an orthopedic procedure may consist of one $100 prosthesis and six $50 screws. The patient-specific supply cost of this assembly totals $400.
The requirement to identify patient-specific supply costs could have a significant impact upon the hospital's current manual and automated supply management practices and systems. Examples of some of the issues that are likely to arise in many functional centres include:
• Are patient-specific supply items identified on an ongoing basis?
Patient-Specific Supplies Supplies and “supply assemblies” that cost over
$250. • Individually dispensed drugs, including PRN
medication, must be tracked and their costs assigned directly to the patient.
• Are the patient-specific supplies tracked that may account for a high proportion of the functional centre's supply budget but cost less than $250?
• Can the current materials management system track both inventory and non-inventory items? • Will direct purchase items need to be catalogued for ongoing tracking? • If supplies are charged back to the functional centres prior to usage (e.g., through the use of
exchange carts or departmental (unofficial inventories), how are actual usage identified? • Can the current materials management system support the tracking of patient-specific cost items
(i.e., either stand alone or integrated with the order entry/results reporting system and/or other ancillary systems)?
• Is a departmental materials management system or other specific programs required for the support of these functional centre specific requirements?
• Can the current systems support maintaining supply assembly lists and costs through a "bill of materials" or other methodology?
Drugs
Drugs are also classified as supplies. For case costing, distinguish between individually dispensed drugs and ward stock drugs. All individually dispensed drugs, regardless of their cost, are tracked and assigned directly to the patient. PRN (as needed) medication that is not kept as ward stock is also captured on a patient-specific basis. These patient-specific costs are excluded from the functional centre unit cost/intermediate product cost calculation. Ward stock drugs are general supplies and therefore are not captured on a patient-specific basis.
The MIS Standards (Section 3.3) specify that all drug costs (patient-specific and ward stock) must be distributed to the consuming functional centre. The OCCI case costing methodology differs from the MIS Standards. Individually dispensed drugs are charged to Pharmacy. However, ward stock drugs must be assigned to the appropriate Nursing functional centre. There are also some specific drugs and related items, administered through other functional centres, that must be charged to those functional centres. For example:
• Anaesthetic agents and other drug items administered through the Operating Room are assigned to the Operating Room.
• Non-medicated IV solution costs are charged to the appropriate Nursing functional centres. • Medical gas costs are charged to the administering department.
OCCI Version 6.1 Page 22 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Amortization and Leasing Expenses Historically, amortization and leasing expenses were simply charged to Administration. For case costing, amortization and leasing costs must be assigned to functional centres using the equipment. The patient cost distribution process will distribute these costs correctly to the patients receiving service from the functional centre as direct costs of the functional centre. Hospitals must comply with the OHRS requirements for amortization rates. In Ontario, the threshold for capitalization is a minimum of $1,000. Each corporation will be allowed to establish their threshold amount at $1,000 or higher.
Maintenance
Maintenance of major clinical equipment performed by the hospital's maintenance and/or biomedical department should be charged to the department receiving the service. The maintenance department should have a mechanism to document the service provided (i.e., work order system) and provide an input document for the accounting posting. At the end of the accounting period, when the cost allocation is performed, the maintenance department's costs would be reduced by the dollars charged directly to the departments served. The remainder would be allocated as indirect costs according to the cost allocation formula.
Major clinical equipment maintenance may also be provided through an external maintenance contract. Like maintenance provided by the hospital's maintenance and/or biomedical department, these charges must be assigned directly to the functional centres whose equipment is receiving the maintenance. Note that building and building equipment maintenance should be allocated as an indirect cost using the allocation statistics presented in this Guide, as there is little value in charging these costs to the absorbing cost centres directly.
Allowable Recoveries and Revenues in Case Costing
Refer to Appendix 3 “Allowable Recoveries and Revenues in Case Costing”
3.1.3 Separating Inpatient, Outpatient and Non-Patient Operating Costs Patient case costs should not be distorted by a hospital's other business activities. Our use of case cost data is best served when inpatient, outpatient, referred-in and ancillary operations are clearly and correctly separated. Hospitals are constantly seeking new ways to generate revenue. One approach is to take advantage of a hospital's strength in its support services (such as printing or food services) to provide products or services for non-hospital clients. Patient case costs should not be affected (understated or overstated) by the expenses or revenues associated with these revenue-generating activities. Wherever possible, isolate non-patient costs and revenues by establishing a separate functional centre for non-patient operations and using direct charge billing for ancillary operations that provide services both within the hospital and to outside customers. Whatever approach is used, it should support both case costing and the monitoring of the profitability and financial performance of the non-patient ancillary operations. In some instances, it may be difficult to separate patient and non-patient costs when the hospital has one functional centre containing expenses for both patient and non-patient operations. To estimate patient costs, non-patient revenue is to be used as a proxy for non-patient costs in this functional centre. This
OCCI Version 6.1 Page 23 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
means that there is a need to establish a mechanism to capture non-patient operating revenue, and net the same amount from the operating costs of the functional centre prior to reporting.
3.1.4 Patient Revenue Some hospitals distribute patient revenue to functional centre accounts for management reporting purposes to show departmental managers a more complete and balanced picture of their operations. If the hospital uses this approach, remember do not net the revenue for providing care to the patients when determining costs for distribution to patients. This approach applies to all patient revenue: Ministry of Health and Long-Term Care Allocation, OHIP, WCB, crutches, etc.
3.1.5 Other Hospital Costs
Which Functional Centres must be Costed? Hospitals may decide not to cost functional centres whose expenses are only a very small percentage of the total hospital costs. It may not provide much added benefit to set up systems to cost functional centres that contribute insignificantly to case costs. Nevertheless, aim to distribute a large portion of the operating costs. The OCCI has established standards for the functional centres that must be costed for certain patient populations:
Acute Inpatient For the first year of costing, hospitals must distribute at least 80% of acute inpatient operating costs to patients using approved workload measurement systems. The following core functional centres must be included as part of the 80% minimum: • 712**** to 7127*** - Nursing Inpatient Services • 71410** - Clinical Laboratory • 71415** - Diagnostic Imaging • 71440** - Pharmacy
Additional functional centres must be costed so that by the beginning of the third year of costing at least 95% of inpatient costs are distributed to patients.
Day Surgery In addition to the required functional centres for acute inpatients, the day surgery operating room must be costed. Hospitals are only required to submit qualifying day surgery cases to the OCCI as per the Joint Policy & Planning Committee definition, who receive services from either the main or day surgery operating rooms.
Ambulatory Care (excluding day surgery) Hospitals must distribute at least 80% of outpatient operating costs to patients using approved workload measurement systems. The following core functional centres must be included as part of the 80% minimum: • 71310** - Emergency • 713501070 - Medical Pre-Admission Clinic • 713501545 - Surgical Pre-Admission Clinic • 71410** - Clinical Laboratory
OCCI Version 6.1 Page 24 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
• 71415** - Diagnostic Imaging • 71430** - Other Diagnostic Laboratories • 71440** - Pharmacy • 71450 - Physiotherapy • 71455** - Occupational Therapy • 71470** - Social Work
If 80% of total outpatient costs cannot be distributed to patients by costing the above functional centres, a hospital-specific mix of additional ambulatory care functional centres must be costed to achieve the 80% minimum. Hospitals have the option to cost additional functional centres beyond the 80% minimum.
Chronic Care Hospitals must distribute at least 80% of chronic care operating costs to patients using approved workload measurement systems. The following core functional centres must be included as part of the 80% minimum: • 71295** - Long Term Care IP • 71450 - Physiotherapy • 71455** - Occupational Therapy • 71470** - Social Work
Mental Health
Hospitals must distribute at least 80% of mental health operating costs to patients using approved workload measurement systems. The following core functional centres must be included as part of the 80% minimum:
• 71276** - Mental Health • 71410** - Clinical Laboratory • 71415** - Diagnostic Imaging • 71430** - Other Diagnostic Laboratories • 71440** - Pharmacy • 71470** - Social Work
Rehabilitation Hospitals must distribute at least 80% of mental health operating costs to patients using approved workload measurement systems. The following core functional centres must be included as part of the 80% minimum: • 71281** - Rehabilitation
OCCI Version 6.1 Page 25 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
• 71450 - Physiotherapy • 71455** - Occupational Therapy • 71470** - Social Work
If costing the above functional centres cannot satisfy the 80% requirement, then a hospital-specific mix of functional centres with chronic care activity must also be costed to satisfy the minimum. Hospitals have the option to cost additional functional centres beyond the 80% minimum.
Appendix G (Calculation of Patient-Specific Cost Distribution Percentage) is a helpful tool to assess the impact of including or excluding particular functional centres. This form organizes the functional centre costs distributed to patients; the total inpatient, chronic care, mental health and outpatient costs for the reporting period; and the total functional centre costs not distributed to patients. To ensure that a consistent approach has been taken to the apportionment of costs between acute inpatient, chronic care, mental health and outpatient activity, use the information reported by the hospital’s OHRS Trial Balance submission to the Ministry of Health and Long-Term Care.
Non-Distributed Absorbing Cost Centre (ACC) Costs Hospitals will vary in the percentage of costs they distribute to patients. Some OCCI hospitals are distributing 100% of acute inpatient costs by costing all inpatient functional centres. Others, however, are including only some or none of the optional functional centres and are capturing closer to 85% of inpatient costs. Because of this variation, the OCCI employs a methodology that distributes acute inpatient costs of non-distributed patient care functional centres to patients. This methodology, to standardize the acute inpatient case cost data from OCCI hospitals, is required so that comparisons can be made between hospitals. It is only expected to be an interim measure, however, since hospitals are required to distribute 95% of total inpatient costs by the beginning of the third year of costing. Since the OCCI employs a methodology that distributes undistributed functional centre costs to patients, hospitals should ensure that they do not distribute or allocate these costs to patient care functional centres.
3.2 Cost Distribution Bases
Two data types can be used as cost distribution bases. The first type of cost distribution is based on workload. The workload cost distribution is described in the following section. Workload is described in the following section. The second type of data involves the collection of patient hours. This new methodology was developed in 2006 and is introduced in Section 3.2.2 of this guide and further discussed in Chapter 5 (see Appendix M for method details). Either workload or patient hours can be used to distribute nursing costs. Hospitals should select a system that meets their needs and is compatible with the appropriate MIS methodology.
3.2.1 Workload
Workload data serve as the cost distribution base for most functional centre costing purposes. Through order entry/results reporting, cost accounting or departmental information systems and intermediate products (such as exams, procedures and other services) are translated into workload units by functional centre for each patient. This information is linked to the specific patient through a unique encounter identifier.
Major Components of Workload Measurement Systems
• Identification and categorization of work • Identification and definition of activities
within each category • Time recording methodology • Reliability and validity measures
OCCI Version 6.1 Page 26 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
There are three time recording methodologies for workload measurement: average, standard and actual. The average time reflects the national average time to conduct the task, as identified by the National Workload Measurement System (NWMS). The Diagnostic workload measurement systems use average time methodologies, while the Nursing and most therapeutic workload measurement systems support both actual and standard time recording. The workload recording method should follow the NWMS that applies to the work done by the functional centre (see MIS Standards 2006, Chapter 4, for a complete list). These systems provide a standardized means of measuring the activities or outputs of each functional centre. Workload units are broadly divided into Service Recipient/Patient Care and Non-Service Recipient/Non-Patient Care workload.
Linking Workload Data to Other Case Cost Data Ideally, workload measurement can be done as a by-product of existing departmental functions. For diagnostic departments, an order entry/results reporting system can be used to minimize the impact of data collection and reporting. Case costing requires the collection and reporting of financial and statistical data on a patient-specific basis. This means a functional centre must be able to track and report workload units and services with the patient unique identifier. There is more information on linking patient and cost data in Chapter 8.
Monitoring The Workload Measurement System If realistic productivity ratios cannot be produced with the NWMS units, re-engineer the units to more appropriately reflect the workload required for various activities. Any changes should strictly follow the NWMS methodology outlined in the MIS Standards. Notify CIHI of significant differences so that an evaluation can be done about the need for revision to the NWMS. If the units are re-engineered, re-evaluate their continued use whenever the NWMS units are adjusted and whenever there is a change in technology or procedures.
Developing A Customized Workload Measurement System Some hospitals choose to develop a customized workload measurement system for functional centres where no NWMS exists. To ensure data comparability, OCCI hospitals have identified those functional centres and explained the approach used. The selection of a workload measurement methodology should ultimately rest upon the results of the methodology to reflect accurate and comprehensive outputs of the functional centre. The development of a workload measurement system must adhere to generally accepted workload measurement principles. Some of the desirable characteristics of a workload measurement system are listed below:
• Activities (procedures or intermediate products) are capable of being patient-specific. • Activities (procedures or intermediate products) are well defined, are recognizable, and are
elements of a cost centre’s function that can be considered separate outputs. • A workable number of activities (procedures or intermediate products)–normally less than 15–is
used, but enough to represent the largest portion (at least 80%) of a functional centre's worked hours.
• Relative values represent the ratios among average times necessary under average conditions to complete all aspects of measured work.
• Each activity (procedures or intermediate products) represents homogeneous elements of resource use.
• Activities (procedures or intermediate products) should be clinically and financially homogeneous.
OCCI Version 6.1 Page 27 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
To maintain data quality, productivity ratios for reported workload with each workload measurement system should be monitored. Productivity ratios must be maintained within an acceptable range to ensure that workload recording is complete. In particular, Allied Health workload measurement systems that record activity time are susceptible to recording problems if not monitored routinely. If the reported time units are significantly more or less than the number of minutes of therapy staff time, then the cause of the discrepancy should be investigated and corrective action taken. On the following pages, there is a generic six-step approach to developing, implementing, and maintaining a standard time workload measurement system. The standard time methodology uses facility-specific set values for high volume activities that demonstrate minimal variability.
Step 1: Review of Current Work Methods Start with a review of current work methods and processes to ensure that the time values or relative values assigned to activities are reflective of the lowest-cost, most efficient processes that yield acceptable quality. Conduct this review by breaking the work method/process into its component parts or elements. Analyze each component part or element separately so that the review of the work method/process becomes a series of fairly simple steps. The review may be aided by applying the concept of flow process analysis and charting. Flow process charting is a graphic representation of the sequence of all operations, transportation, inspections, and delays occurring during a process or procedure. By using these charts, hidden inefficiencies are located easily, such as bottlenecks, duplication of effort, etc. Here are some examples of checklist questions used to review the current process:
• Can it be eliminated? • Can it be changed or rearranged? • Can it be combined? • Can it be simplified? • Can it be improved?
The level of detail required for reviewing current work methods is unique to each hospital and department. The review of current processes should be a continuous effort, recognizing that further improvement is always possible.
Step 2: Identify Workload Elements Select workload elements or activities (procedures or intermediate products) which reflect the variability and complexity of the department's patient care workload. A group workshop session may be used to identify and reach consensus on workload activities that are well defined, recognizable, and are considered distinct department outputs. Patient Care Workload activities should be identified and categorized as follows:
• Service Recipient Those diagnostic, evaluative or therapeutic and support activities that are provided to, or on behalf of, specific patients.
• Non-Service Recipient
OCCI Version 6.1 Page 28 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Those activities that are part of the departmental activities but which do not involve the care of specific patients or cannot be linked to specific patients. A workable number of activities (procedures or intermediate products) is normally considered to be less than 15. The largest portion of the functional centre's worked hours (at least 80%) should be represented.
Step 3: Assign Time/Relative Unit Values Establish an allowed time or relative value unit for each of the workload activities identified in Step 2. Relative values represent the ratios among average times necessary under normal conditions to complete all aspects of measured work. Potential techniques that may be used to measure the work content of the activities include the following:
• Time Study The actual time spent on each workload activity is measured using logs, time ladders or other methods. This process is repeated until there is confidence that the time is reflective of the activity.
• Work Sampling Work sampling is used to determine the actual percent of time spent on the observed activity. Observations are regularly or randomly spaced over the total observation period or over several time periods.
• Estimates Using historical data, the relative work content value among the activities (procedures or intermediate products) may be estimated in a group workshop session or by the department manager.
Step 4: Ongoing Data Collection
Develop and implement data collection methods to collect the workload elements and labour hours on an ongoing basis. Case costing also requires that the time units or relative value units of the patient care activities be collected and reported on a patient-specific basis. Ideally, the collection of workload units and labour hours should occur as a by-product of departmental systems or hospital information systems. However, manual data collection forms may be developed as a short-term measure until further investments can be made in additional automated information systems.
Step 5: Establish Productivity Target The MIS Standards define productivity as a measure of efficiency shown through the ratio of outputs: the extent to which output is maximized with minimum input. Productivity targets should be established for each workload measurement system. Depending on the context, productivity may be stated as workload units per hour or hours per workload unit. For example, the MIS Standards use workload units per worked hour as an indicator of productivity. Whether using weighted units (based on adjustment of the total activity volume based on the relative value unit of each activity) or unweighted workload units, productivity targets must reflect a realistic balance between labour hours (input) and workload activities (output). Productivity can be calculated using only service recipient (patient care) workload or using total workload. Productivity targets can be initially established based upon preliminary data collection activities or estimates, but should ultimately be refined over time to more accurately reflect achievable levels of performance.
OCCI Version 6.1 Page 29 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Step 6: Monitor Key Relationships Monitoring productivity and other key relationships is an ongoing process that ensures productivity ratios are maintained within an acceptable range and that workload recording is complete. Productivity targets should be reflective of the current scope of services in the functional centre. Some key relationships to monitor include:
• Actual productivity to target productivity (units per hour); • Actual to budgeted workload volumes; • Percentage patient care hours to non-patient care hours; and • Comparisons of productivity among functional centres that use the same methodology to measure
workload.
3.2.2 Patient Hours Data
The second type of cost distribution is based on patient hours. This method is used primarily for nursing cost allocations. For further information refer to Chapter 5 and Appendix M.
CIHI The Canadian Institute for Health Information provides the reference standard for inpatient, day surgery, ambulatory care and chronic care data coding and abstracting. Make sure that the abstracting policies are consistent with CIHI rules for coding and the application of the definitions.
3.3 Patient Descriptive Data
Once costs have been established, the cost data must be linked to information about the patient and the course of diagnosis and treatment while in hospital. For acute inpatients, patient costs are identified for all cases that are discharged within the costing period. This includes any patients who are admitted before the beginning of the period and discharged during the period. This section describes the specific patient descriptive data requirements. For inpatients and day surgery cases, this information is gathered through the Health Records department using the CIHI abstract. Data quality is as important as the range and completeness of patient descriptive data elements collected. All hospitals in Ontario use CIHI’s abstracting rules and data requirements, which form the reference standard for patient descriptive data collection. Many OCCI hospitals have obtained a grouper. This software product is used to analyze abstracted patient records. It is useful for checking abstracted patient information for accuracy before submission to CIHI. Groupers will assign acute inpatient cases to Case Mix Groups (CMGs) using the same decision rules applied by CIHI. This will eliminate the turnaround time from CIHI to use grouped data. Ambulatory & Day Surgery cases are assigned to Comprehensive Ambulatory Classification System (CACS) by the grouper. Section 9.6 provides more information about the requirements for the Health Records department.
3.3.1 Data Quality The ultimate acceptance of case cost data hinges on the quality of the data used to calculate case costs. The CIHI coding manual, definitions, and rules must be observed to ensure consistent application and interpretation of the minimum data standards. It is critical that both Health Records staff and physicians
OCCI Version 6.1 Page 30 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
be included in educational programs designed to make sure that there is up to date information with coding standards and data requirements.
3.3.2 CIHI and OCCI Coding Requirements Requirements for coding and submission of patient descriptive data are dependent upon the patient populations for which the hospital is submitting costs.
3.3.2.1 Acute In-patient Abstracting CIHI has specified a mandatory set of data elements on the inpatient abstract. The list of these mandatory abstract items is published in the CIHI Abstracting Manual and in Appendix H. Hospital Health Records personnel are familiar with these basic abstracting requirements. In addition, certain data elements, normally optional on the CIHI abstract, are required for comprehensive case cost analysis. They are the following:
Pre-Admission Work-Up Indicator
This single digit code (CIHI valid numbers 0-9) is provided on the abstract to identify any examinations, x-rays, laboratory tests, etc., done prior to the patient's admission. Each hospital may assign meaning to code values. For basic case cost comparison it is important only to know that some pre-admission work was done. OCCI hospitals with pre-existing codes for pre-admission work-up continued to use their codes. Hospitals that have not been using this indicator may code any number (0-9) to indicate that pre-admission work has been done. A “blank” or null field indicates that none was done.
All Relevant Diagnoses, to a Maximum of 25
Most hospitals already code more than the CIHI minimum required number of diagnoses to ensure proper CMG assignment. The need for complete and correct diagnostic information, in particular the Most Responsible Diagnosis, is critical.
All Relevant Procedures, to a Maximum of 20
Most hospitals already code more than the CIHI minimum required number of procedures. The number and type of procedures play a significant role in CMG assignment. Note that operative procedures are separated from non-operative procedures. CIHI requires that the Principal Procedure be an operative procedure for surgical patients.
Service Transfers–Patients Awaiting Alternate Levels of Care (ALC)
CIHI describes an ALC patient as a patient who is finished with the acute care phase of his/her treatment. This patient is usually awaiting placement in a chronic unit, home for the aged, nursing home, rehabilitation facility, other extended care institution or home care program. Since the non-acute stay can be much longer than the acute phase, it is important to be able to identify the acute portion of the stay for case weighting and comparative analysis.
It is important that hospitals developing case cost data record the non-active treatment portion of the patient's stay as Patient Service 99. Thus, on the CIHI abstract, when the patient is no longer an active treatment patient, the non-active treatment portion of the stay must be recorded in the
OCCI Version 6.1 Page 31 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
service transfer area as Patient Service 99.
Effective capture of ALC placement and duration requires active participation and communication with Medical, Nursing, and Health Records staff.
Operating Room Number (optional for case costing, but requested)
The two-digit code for the operating room number where a procedure was performed is used by the OCCI for auditing purposes. Although this data element is optional, accurate coding of the OR number has proved to be a very good indicator of whether Operating Room costs should have been captured for a patient. The list of codes is included in the CIHI Abstracting Manual. In Ontario, hospitals are required to map the OR number to the appropriate functional centre to ensure matching of expenses with clinical data.
The OCCI has not established special data requirements for psychiatric patients in acute care facilities. The acute inpatient data abstract is used for collection of patient descriptive data and all general and departmental case costing standards apply.
3.3.2.2 Day Surgery Abstracting In Ontario, day surgery cases have been defined as those procedures performed on patients whose hospital stay/visit (from time of registration to discharge) occurs on the same calendar day or, if over the midnight hour, is less than 12 hours. A list of exclusions from this definition is provided in the CIHI Abstracting Manual. In addition to the data elements described above as required for case costing, the following data elements are also mandatory for day surgery cases.
Operating Room Number
The operating room number is a two-digit code. It is mandatory to record the operating room number for each day surgery episode. The list of codes is included in the CIHI Abstracting Manual.
3.3.2.3 Ambulatory Care Minimum Data Set As costs for providing care continue to increase, health care providers are looking for ways to continue to provide quality care in the most cost-effective manner. Many hospitals have responded to the challenges posed by shifting from inpatient to outpatient care. A National Ambulatory Care Reporting System (NACRS) to collect patient descriptive data for ambulatory care visits has been developed by CIHI. The CIHI Ambulatory Care Minimum Data Set contains a list and description of the required data elements. OCCI-mandated data elements are found in Appendix I. Certain data elements optional on the CIHI Ambulatory Care MDS are required for case costing. They are the following:
Encounter Number
A unique number assigned by the hospital, to associate the patient with a particular visit. The costs for the visit will be tracked to the encounter number.
OCCI Version 6.1 Page 32 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Mode of Visit/Contact
The nature of the contact will be used to verify that the costs are appropriate. For example, a telephone contact should not have any costs for clinical procedures.
3.3.2.4 Chronic Care Minimum Data Set CIHI has derived a minimum data set from the Minimum Data Set (MDS) version 2007 Chronic Care Assessment Tool to capture patient descriptive data for chronic care patients (residents) and Minimum Data Set (MDS) version 2 OMHRS (MDS) to capture patient descriptive data for mental health patients. The OCCI standards require the collection of the MDS to define the chronic care or mental health encounter. The data elements are collected through periodic assessments by clinical staff involved in the treatment of the chronic care or mental health patient. The purpose of the data collection is to gather information to address the needs and strengths of the patient in an individualized care plan.
A New Chronic Care Sub-Encounter Begins:
• On the first day of admission. • The day a significant change in status occurs. • The day after the quarterly assessment.
Assessment data is collected approximately every 90 days. However, assessment data can be collected in periods less than 90 days if there is a “significant change” in patient status. Certain situations may occur in which the question arises of whether or not an assessment should be done on a patient. For example, due to a lack of appropriate beds in the facility, a chronic care patient may be assigned to a rehabilitation or long-term care bed, or a rehabilitation patient may be admitted to a chronic care bed. How is it decided which patient receives an MDS assessment? The bed designation, and not the patient type, determines whether or not to do an assessment. Therefore, an MDS assessment is done for patients in a designated mental health or chronic care bed. Due to the lengthy nature of the mental health or chronic care visit, patients may have more than one MDS assessment throughout their hospital stay. The unique identifier for each assessment is the MDS assessment reference date. This date is the last day of the MDS observation period. The assessment period (usually 90 days) is defined as the time from the beginning day of an MDS assessment period to the day before the next assessment period. Each assessment defines a costing period in which all services and products delivered to the patient are to be tracked to that assessment period. The list of required MDS data elements for chronic care can be found in the CIHI Ontario Chronic Care Patient System (MDS) Manual, more detail about the assessment tool itself is presented in the MDS v2 Resident Assessment User’s Manual. A list of required MDS data elements for mental health as well as more detail about the assessment tool it can be found in the OMHRS Minimum Data Set Manual
3.3.2.5 Rehabilitation Minimum Data Set The minimum data set for rehabilitation is recorded at admission and at discharge for each rehabilitation visit, with the option of a follow up assessment record. Assessments include: a) The Functional Independence Measure (FIM instrument) b) CIHI cognitive assessment c) CIHI Instrumental Activities of Daily Living (IADL) (optional)
OCCI Version 6.1 Page 33 of 105 Effective April 2008-March 2009 Updated August 2009
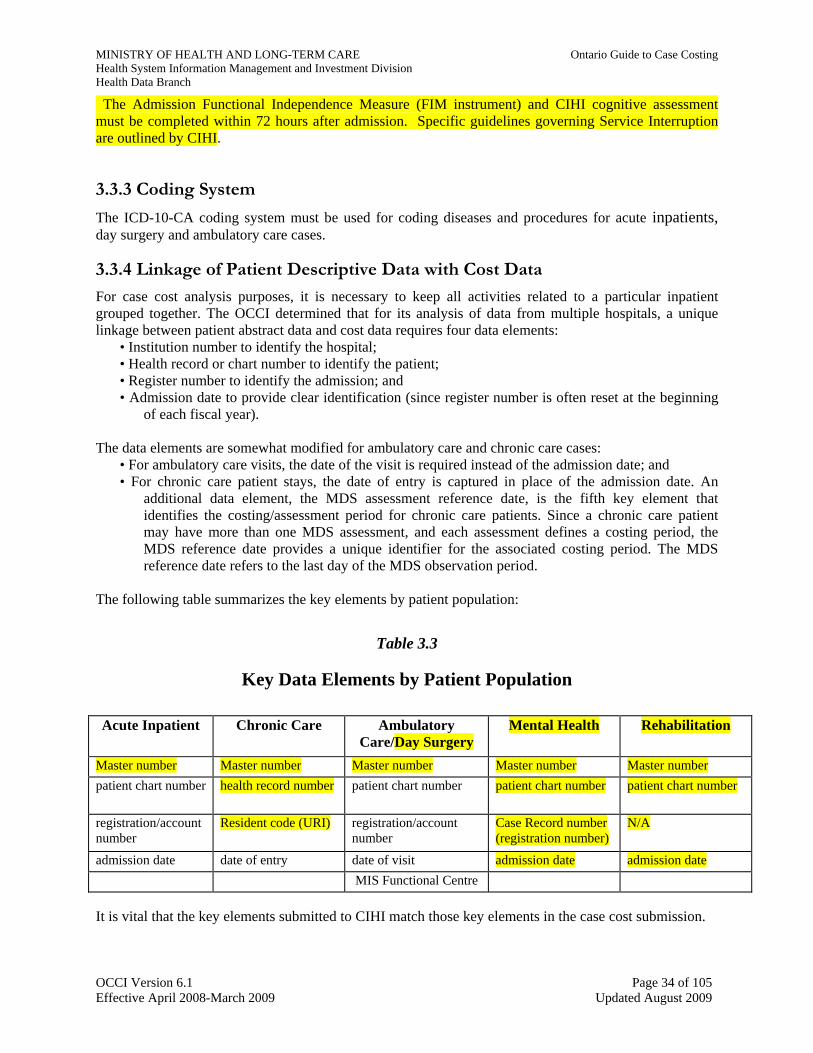
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
The Admission Functional Independence Measure (FIM instrument) and CIHI cognitive assessment must be completed within 72 hours after admission. Specific guidelines governing Service Interruption are outlined by CIHI.
3.3.3 Coding System The ICD-10-CA coding system must be used for coding diseases and procedures for acute inpatients, day surgery and ambulatory care cases.
3.3.4 Linkage of Patient Descriptive Data with Cost Data For case cost analysis purposes, it is necessary to keep all activities related to a particular inpatient grouped together. The OCCI determined that for its analysis of data from multiple hospitals, a unique linkage between patient abstract data and cost data requires four data elements:
• Institution number to identify the hospital; • Health record or chart number to identify the patient; • Register number to identify the admission; and • Admission date to provide clear identification (since register number is often reset at the beginning
of each fiscal year). The data elements are somewhat modified for ambulatory care and chronic care cases:
• For ambulatory care visits, the date of the visit is required instead of the admission date; and • For chronic care patient stays, the date of entry is captured in place of the admission date. An
additional data element, the MDS assessment reference date, is the fifth key element that identifies the costing/assessment period for chronic care patients. Since a chronic care patient may have more than one MDS assessment, and each assessment defines a costing period, the MDS reference date provides a unique identifier for the associated costing period. The MDS reference date refers to the last day of the MDS observation period.
The following table summarizes the key elements by patient population:
Table 3.3
Key Data Elements by Patient Population Acute Inpatient Chronic Care Ambulatory
Care/Day Surgery Mental Health Rehabilitation
Master number Master number Master number Master number Master number patient chart number health record number patient chart number patient chart number patient chart number
registration/account number
Resident code (URI) registration/account number
Case Record number (registration number)
N/A
admission date date of entry date of visit admission date admission date MIS Functional Centre It is vital that the key elements submitted to CIHI match those key elements in the case cost submission.
OCCI Version 6.1 Page 34 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
3.3.5 Useful Additional Patient Descriptive Data An additional patient descriptive data element has been considered optional for Ontario Case Cost development, but may be of interest to the hospital.
Health (OHIP) Card Number As more hospitals join the OCCI, it may become more feasible to track patient stays across hospitals. This would allow for more complete patient episode (across system) costing. The Health Card Number is a common patient-specific identifier that would allow for episode costing.
OCCI Version 6.1 Page 35 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 4: Step 2: Allocate Indirect Costs
4.1 Allocation of Indirect Costs vs. Distribution of Direct Costs
As described in Chapter 2, cost allocation involves allocating the costs of transient cost centres (TCCs) to the absorbing cost centres (ACCs) to establish the full costs of operating patient care functional centres. Generally, ACCs are associated with the patient care functional centres, whereas TCCs are associated with the administrative and support, or overhead, functional centres. Later in the costing process, the functional centre’s relative value units will be used to calculate a cost per unit of service. This cost can then be multiplied by the number of relative value units received by a patient to calculate the case cost. For case costing, refer to direct costs as those costs that were directly assigned to the ACCs according to the rules discussed in the previous chapter. Establish the full operating costs of the ACC through cost allocation, the process by which the costs of the TCCs are assigned to the ACCs. These allocated costs are referred to as indirect costs. A formula is used to allocate these TCC costs to the ACCs as indirect costs, based on an estimate of costs incurred by the ACC to provide particular services.
4.2 Indirect Cost Allocation Using SEAM
The Simultaneous Equation Allocation Method (SEAM) must be used to compute the indirect cost allocation. This algorithm allows us to determine the relative use of administrative and support services by each patient care functional centre. SEAM is a set of linear equations that can be solved using a spreadsheet program on a PC or with specifically designed management information system software currently available to hospitals. Many case costing systems have a cost allocation function with their General Ledger or cost accounting software. In essence, SEAM allocates a portion of the TCC costs as indirect costs to other TCCs as well as ACCs, then simultaneously allocates out all the TCC direct and indirect costs to all the ACCs as indirect costs. Further details and an example of SEAM are found in Appendix J.
4.3 Indirect Cost Allocation Bases
Each TCC is associated with a specific measure, termed the “allocation base,” that is used by SEAM to allocate the TCC costs to other functional centres. The allocation base provides a means of estimating the amount of TCC costs consumed by the ACCs in providing patient care. To ensure comparability of results, standard cost allocation bases are used by OCCI hospitals for case cost reporting. The allocation bases should be measured for the entire fiscal year and the bases should be updated annually. For example, if proportion of department cost is the basis for cost allocation, the cost figures should be the totals for the entire fiscal year. Cost allocation may be done at any MIS account level (3, 4 or 5), depending on the functional centre. Many of these cost allocation bases are listed in Appendix K Specific explanations which have been developed to clarify the intent of the cost allocation bases are included in the Glossary at the end of the Guide.
Actual Year-End Costs are used for the Cost Allocation Calculation Actual costs are the most appropriate calculation for Ontario case cost development. Hospitals that allocate and report indirect costs as part of their monthly management reporting typically use budget costs to establish the proportion of actual costs to allocate. OCCI hospitals recalculate the allocation at year-end to produce case costs based on actual costs for the period.
OCCI Version 6.1 Page 36 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
4.4 What TCC Costs are to be Allocated as Indirect Costs?
The costs of those functional centres that are traditionally classified as hospital support and administration or overhead are considered to be indirect costs. For example, Finance, Health Records and Information Systems are departments that do not provide direct patient care, but are necessary in order for the ACC to provide services to patients. Hospital departments and managed support functions have been organized in many different ways. As a result, different hospitals documenting and accounting for operations correctly could produce similar total case costs but with quite different ratios of direct and indirect costs. In addition, the hospital may not be costing some patient care functional centres, such as Allied Health. These functional centres should receive the appropriate indirect costs, but the costs of the Allied Health functional centres should remain undistributed. The OCCI standards on the types of expenses or functional centre costs that should be allocated as indirect costs or distributed as direct costs are as follows:
Laundry Hospitals with a Laundry and Linen Department or using contract laundry services have moved to charge departments for their usage of laundry services. OCCI hospitals should ensure that all laundry and linen costs are assigned to ACCs as direct costs. Note that hospitals with their own laundry and linen service may choose to use the Laundry and Linen functional centre throughout the year and then at year-end distribute the costs to the absorbing cost centre using a distribution base.
Hospital Library, Audiovisual, Medical Illustration and In-Service Education For case costing, the provision of Hospital Library, Audiovisual, Medical Illustration and In-service Education should be allocated as indirect costs to functional centres receiving these services as noted in Appendix K. (Costs associated with receiving in-service education are allocated to the receiving employee’s cost centre.) Note that OCCI standards are not consistent with the MIS Standards, which specify that Hospital Library and Medical Illustration are to remain undistributed. OCCI hospitals should also ensure that the expenses of "Special Functional Centres" are excluded from the cost allocation process and left undistributed. These Special Functional Centres are the Level 2 Framework Sections of Research (7), Education – Formal (8) and Undistributed Functional Centres (9). It was reasoned that the services of these functional centres are not associated with specific patients or programs and are outside the scope of a hospital’s patient care business.
Maintenance (General and Biomedical) The MIS Standards recommend the use of a work order system and the posting of maintenance activities as direct costs to each functional centre receiving service. Any residual maintenance cost not covered by the work order charges should be allocated as an indirect cost using net square metres or department total costs. Hospitals that do not have a work order system in place may allocate general maintenance costs. Biomedical maintenance must be distributed as direct costs through a work order system. Note that maintenance covered by maintenance contracts is charged as a direct expense to the functional centres receiving the service.
OCCI Version 6.1 Page 37 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Patient Care Administration and Support Functional Centres The costs of separate support and administration functional centres should be assigned as a direct cost to the patient care centres they support. More detail about patient care departmental support and administration cost distribution can be found in section 3.1.2.
Nursing Administration All Nursing Administration costs should be distributed as direct costs to nursing functional centres based on each nursing functional centre’s total costs as a proportion of total nursing costs. Where suitable patient-specific workload measurement systems are in place, clinical resources’ functional centre costs are to be distributed to patients based on workload. There are several functional centres for Nursing Administration (see also 3.1.2). These provide general management for both the Department of Nursing and Nursing Clinical Resources. Nursing Administration is included with General Administration and Support Services in the MIS Chart of Accounts as per the OHRS only if the person, in a non-program management setting, is responsible for functional centres in addition to Nursing. Only nursing costs in this administration functional centre (71110) are to be allocated as indirect costs. All other Nursing Administration costs are to be distributed as direct costs. These functional centres are then to be cleared to zero by charging the costs to the nursing patient care functional centres. The use of the other Nursing Administration functional centres listed will depend on the organizational structure of the facility.
71110 - General Administration (if person is responsible for other functional centres as well as Nursing)
71205 - Inpatient Nursing Administration (non-program management setting) 10 - Nursing Administration 20 - Clinical Resources (centralized) 2020 - IV Therapy 2040 - Enterostomal Therapy 2092 - Transplant Coordination/Organ Procurement 2094 - Palliative Care Team 71206 - Program Management Administration (program management setting)
71305 - Ambulatory Care Administration
71306 - Program Management Administration If a manager is responsible for both Inpatient Nursing functional centres and Ambulatory Care functional centres, then compensation for this individual should be split appropriately between 71205 and 71305.
Patient Transport How patient transport services are organized can impact the direct/indirect cost ratio. The labour costs of a porter who works in a specific absorbing cost centre are direct costs if that porter’s hours are posted as part of the functional centre’s hours. It is common in many hospitals to have porters assigned to Radiology or the Operating Room, for example. In many other hospitals, portering is provided by a central porter service established as a support functional centre. In this case the porter hours are charged directly to the portering functional centre, and the costs of portering are allocated to user ACCs as indirect costs based on the total costs of the using departments.
Materials Management Typically, Materials Management is responsible for providing hospital departments with timely supplies at the best possible cost. Because of varying system capabilities, the choices made can move costs between direct and indirect. For example, disposable supplies are most likely charged through the
OCCI Version 6.1 Page 38 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
inventory system as direct expenses, whereas reprocessing costs associated with reusable supplies are allocated as indirect costs. Shifting from disposables to reusables (or back) can affect the direct/indirect cost ratio.
Printing Services Internal printing may not be charged directly to a department, but outside printing and forms from stock are generally charged directly to the using departments. It is accepted that these cost categorization differences will arise and that they cannot be totally eliminated without extensive effort. Be mindful of these issues when conducting any detailed analysis and comparisons of hospitals’ case costs.
OCCI Version 6.1 Page 39 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 5: Step 3: Calculate Functional Centre Unit Costs or Intermediate Product Costs
The third step of the case costing process can be accomplished using two methods. The first method involves calculating unit costs for services provided by each nursing functional centre (ACC). It is described in the MIS Standards. This approach is referred to as the Functional Centre Unit Cost method. Calculating functional centre unit cost is typically used in nursing functional centres. The other method is the Intermediate Product Costing method, which is typically used in the Diagnostic and Laboratory functional centres. It is very similar to the Workload + (plus) Costing method described in the MIS Standards, Section 6.5. This method involves defining intermediate products (i.e., tests or procedures) in the patient care functional centres and calculating the cost of each intermediate product using financial, workload (and RVU), and utilization information. The Functional Centre Unit Costs and the Intermediate Product Costing methods both produce acceptable and valid results. In fact, both yield the same results when the same RVUs are used to distribute costs. The main difference between the two methods is that the Functional Centre Unit Cost method tracks patient-specific unit costs whereas the Intermediate Product method tracks patient-specific utilization of products. Either method can be used at the facility level; however, the level of detail and flexibility desired should be considered when deciding upon a method. The advantage of the Intermediate Product Costing method is that it details the types and quantity of services/products the patient received in the functional centre, rather than merely the costs incurred at the functional centre level. This information can be useful for patient care planning and utilization review. Furthermore, the Intermediate Product Costing method provides details of the costs of the various fixed and variable resource components of the products. This information will assist in cost analysis. Both methods are described below, followed by a discussion of the distribution bases for the calculations (workload and RVU development). A numerical example is provided in Chapter 7 to further illustrate the calculations used in both approaches.
5.1 The General Ledger, Accounting Guidelines, and Variable and Fixed Costs
The financial General Ledger (G/L) contains the hospital expenses for each functional centre. Remember that all financial G/L expenses (and functional centre codes) must adhere to the account structure presented in the MIS Standards and the account codes presented in the Healthcare Reporting Standards. If this is not the practice, it is a requirement to map the current account used to the OHRS account codes. The G/L feeds into the cost accounting system where calculations in Step 3 are performed. In some hospitals, the G/L feed will map the G/L expenses into cost categories. Generally, these costs are mapped into resource types: labour; patient-specific materials; other materials and supplies; referred-out; sundry and other; building, equipment and grounds; and other. The costs may be further categorized as fixed or variable. Placement of costs into categories must also be consistent with the MIS Standards, except as noted in this manual. Table 5.1 shows the MIS standard categories of costs and the MIS secondary accounts that correspond to each cost category (Note that all possible secondary accounts are shown, although not
Variable and Fixed Costs Variable costs should change with a moderate change in workload. Fixed costs should not be affected by a moderate change in workload.
OCCI Version 6.1 Page 40 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
all will apply to each functional centre). A description of the specific contents of the secondary accounts can be found in the specific OHRS Chapters and Chart of Accounts. Labour costs must be placed into the proper cost category. Management and Operational Support (M&O) and Unit-Producing (UP) labour costs are considered as fixed and variable costs respectively. When an employee performs functions in both the M&O and UP categories, which is often the case with supervisors in diagnostic and therapeutic departments, the appropriate time spent in each category should be recorded. Note also that medical fees based on fee-for-service payments should be considered a variable cost, but where a physician receives a salary, the salary (and benefits) costs are considered fixed costs.
Table 5.1
MIS Secondary Accounts by Variable and Fixed Cost Category Direct Variable Costs MIS Secondary Accounts Labour Compensation (Including Benefits):
3 50 ** Unit-producing 3 90 90 Medical Fee-for-Service
Material 4 ** ** Supplies 5 ** ** Patient-Specific Supplies
Other 8 ** ** Referred Out Direct Fixed Costs Labour Compensation (Including Benefits):
3 10 ** Management/Operational Support 3 90 10 to 3 90 85 Medical (Salaried Physicians)
Other–Sundry 6 ** ** Sundry Building, Equipment and Grounds 7 ** ** Equipment Expense (Including Amortization)
9 ** ** Undistributed (Building and Grounds)
5.2 Functional Centre Unit Costs
In the third step of the case costing process, unit costs are developed for services provided by each patient care functional centre (ACC). Functional centre unit costs will vary from period to period. For the calculation, functional centre unit costs should be based on annual statistics and expenditures. If periodic calculations are done, ensure that there are no significant, extraordinary cost items included or missing that will distort the unit cost calculation. Annual service expenditures like service contracts or major supplies shipments should be taken into consideration. Preliminary, or budget, unit costs are useful for management reporting and utilization review. Ensure that actual statistics and expenditures are used in the functional centre unit cost calculation. 5.2.1 Information Needed to Calculate Functional Centre Unit Costs
Direct Costs and Indirect Costs The key financial information required to calculate functional centre unit costs includes the ACCs total direct expenses for the costing period and the indirect costs allocated to each ACC for the same period. This information has already been obtained in Steps 1 and 2 of the case costing process. Separate totals
OCCI Version 6.1 Page 41 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
for direct costs and indirect costs are kept, even though the full costs of the ACCs are distributed to patients. Keeping them separate is useful for internal hospital management reporting and analysis. Direct expenses and indirect costs are also reported separately to the OCCI.
Patient-Specific Supplies and Drugs Patient-specific supplies that are over $250 and individually dispensed drugs are charged to the patient (microcosted) and should not be included in the functional centre total direct expenses when calculating the functional centre unit direct cost. These costs should be assigned directly to the patient and therefore should be subtracted from the functional centre direct expenses. The OHRS Chart of Accounts provides a separate expense account that can be used to accumulate patient-specific and drug charges so that the total patient-specific costs during the period can be easily separated and excluded from the calculation of functional centre unit direct costs.
Other Non-Workload Distributed Costs The costs associated with expense items that are being distributed by non-workload relative value units should be removed from the direct expenses before completing the functional centre unit cost calculation. This includes fee-for-service physician costs, as well as pathologists’ salaries and general supplies when non-workload RVUs are used.
Total Workload Units/Total Relative Value Units To complete the calculation, the total workload units or patient hours provided by the functional centre to patients are required for the period. Note that the patient-specific workload units used for distributing costs to patients are slightly different from standard reported departmental units. Departmental workload typically includes units for activities such as quality control that are not patient-specific, yet are valid, reported departmental workload. This will be explained in detail in section 5.2.3 If there are any non-unit cost distributed costs in the functional centre, the total RVUs associated with these items are required for the calculation. Total RVUs will be used instead of unit costs to distribute these costs to patients.
5.2.2 The Functional Centre Unit Cost Calculation The functional centre unit cost calculation is relatively simple. It is necessary to calculate separate unit costs for direct and indirect costs, since these costs are reported separately. There are two types of calculating functional centre unit costs for nursing. Type 1: Using Nursing Workload Type 2: Using Patient hours.
5.2.3 Type 1 - Using Nursing Workload to Calculate Functional Centre Unit Cost
Total “units of patient service” are workload units generated by the workload measurement system used in the functional centre. The terminology units of patient service is used to distinguish these units from the traditional workload units reported for Functional Centre Reporting. Traditional workload units as measured by the NWMS and reported for departmental workload include units that can be linked directly to a patient and those that are part of departmental activities but that do not involve the care of specific patients (i.e., service recipient and non-service recipient workload). Examples of non-service recipient workload that are measured but cannot be linked to a specific patient include quality control units for standards and controls in the Laboratory, quality control units in Diagnostic Imaging and some Clinical Pharmacy activities.
OCCI Version 6.1 Page 42 of 105 Effective April 2008-March 2009 Updated August 2009
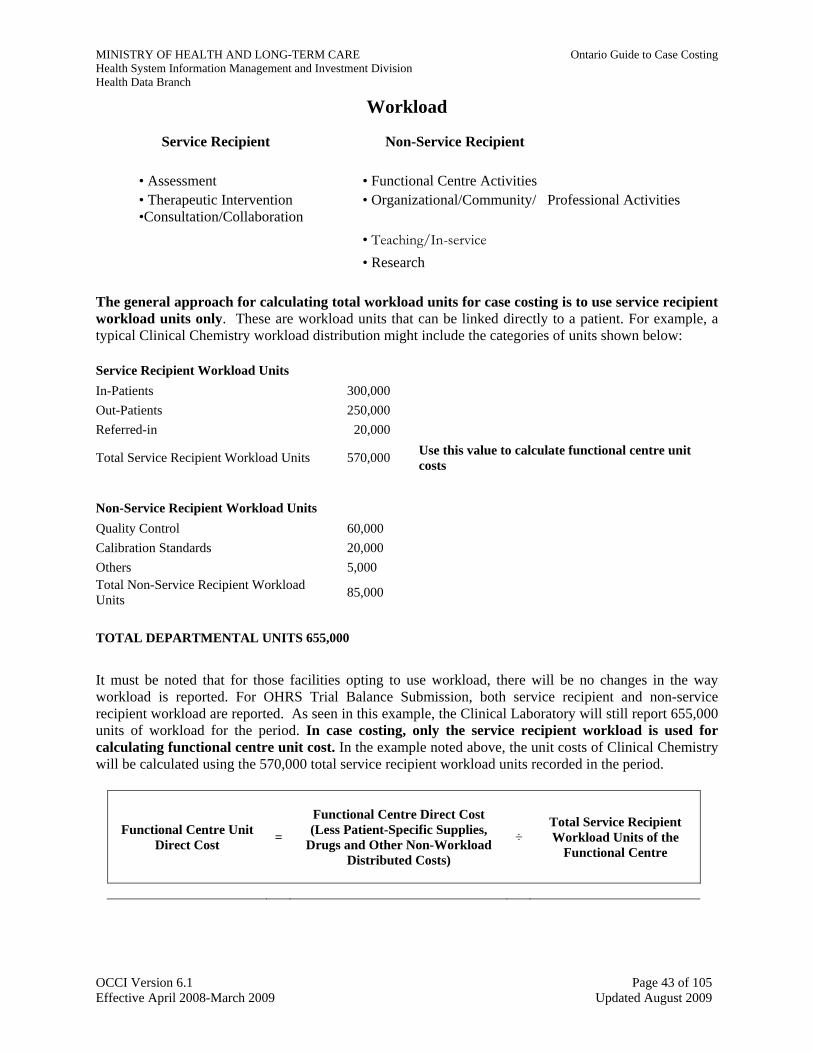
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Workload
Service Recipient Non-Service Recipient • Assessment
• Functional Centre Activities
• Therapeutic Intervention •Consultation/Collaboration
• Organizational/Community/ Professional Activities
• Teaching/In-service • Research
The general approach for calculating total workload units for case costing is to use service recipient workload units only. These are workload units that can be linked directly to a patient. For example, a typical Clinical Chemistry workload distribution might include the categories of units shown below:
Service Recipient Workload Units In-Patients 300,000 Out-Patients 250,000 Referred-in 20,000
Total Service Recipient Workload Units 570,000 Use this value to calculate functional centre unit costs
Non-Service Recipient Workload Units Quality Control 60,000 Calibration Standards 20,000 Others 5,000 Total Non-Service Recipient Workload Units 85,000
TOTAL DEPARTMENTAL UNITS 655,000
It must be noted that for those facilities opting to use workload, there will be no changes in the way workload is reported. For OHRS Trial Balance Submission, both service recipient and non-service recipient workload are reported. As seen in this example, the Clinical Laboratory will still report 655,000 units of workload for the period. In case costing, only the service recipient workload is used for calculating functional centre unit cost. In the example noted above, the unit costs of Clinical Chemistry will be calculated using the 570,000 total service recipient workload units recorded in the period.
Functional Centre Unit Direct Cost =
Functional Centre Direct Cost (Less Patient-Specific Supplies,
Drugs and Other Non-Workload Distributed Costs)
÷ Total Service Recipient Workload Units of the
Functional Centre
OCCI Version 6.1 Page 43 of 105 Effective April 2008-March 2009 Updated August 2009
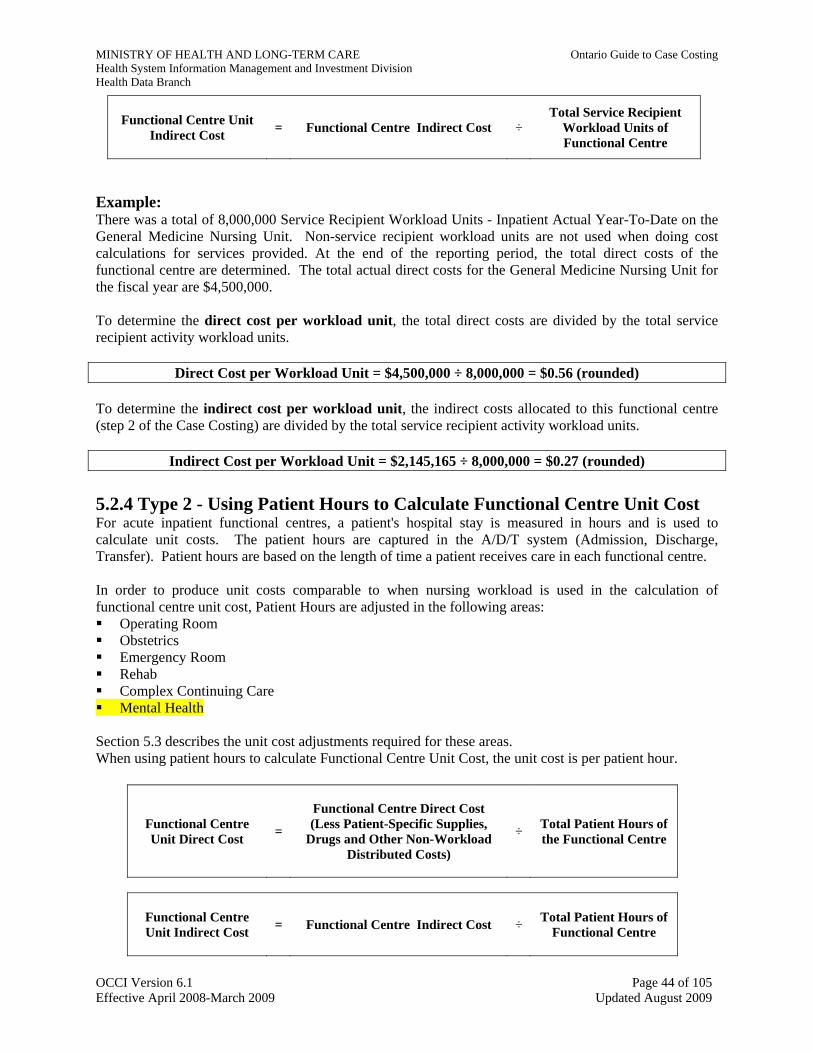
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Functional Centre Unit Indirect Cost = Functional Centre Indirect Cost ÷
Total Service Recipient Workload Units of Functional Centre
Example: There was a total of 8,000,000 Service Recipient Workload Units - Inpatient Actual Year-To-Date on the General Medicine Nursing Unit. Non-service recipient workload units are not used when doing cost calculations for services provided. At the end of the reporting period, the total direct costs of the functional centre are determined. The total actual direct costs for the General Medicine Nursing Unit for the fiscal year are $4,500,000. To determine the direct cost per workload unit, the total direct costs are divided by the total service recipient activity workload units.
Direct Cost per Workload Unit = $4,500,000 ÷ 8,000,000 = $0.56 (rounded) To determine the indirect cost per workload unit, the indirect costs allocated to this functional centre (step 2 of the Case Costing) are divided by the total service recipient activity workload units.
Indirect Cost per Workload Unit = $2,145,165 ÷ 8,000,000 = $0.27 (rounded) 5.2.4 Type 2 - Using Patient Hours to Calculate Functional Centre Unit Cost For acute inpatient functional centres, a patient's hospital stay is measured in hours and is used to calculate unit costs. The patient hours are captured in the A/D/T system (Admission, Discharge, Transfer). Patient hours are based on the length of time a patient receives care in each functional centre. In order to produce unit costs comparable to when nursing workload is used in the calculation of functional centre unit cost, Patient Hours are adjusted in the following areas: Operating Room Obstetrics Emergency Room Rehab Complex Continuing Care Mental Health
Section 5.3 describes the unit cost adjustments required for these areas. When using patient hours to calculate Functional Centre Unit Cost, the unit cost is per patient hour.
Functional Centre Unit Direct Cost =
Functional Centre Direct Cost (Less Patient-Specific Supplies,
Drugs and Other Non-Workload Distributed Costs)
÷ Total Patient Hours of the Functional Centre
Functional Centre Unit Indirect Cost = Functional Centre Indirect Cost ÷ Total Patient Hours of
Functional Centre
OCCI Version 6.1 Page 44 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
The Patient Hours unit cost calculation is illustrated in the example below: There are a total of 133,400 Patient Hours - Inpatient Actual Year-To-Date on the General Medicine Nursing Unit. At the end of the reporting period, the total direct costs of the functional centre are determined. The total actual direct costs for the General Medicine Nursing Unit for the fiscal year are $4,500,000. The total indirect costs are $2,145,165. The total direct costs are divided by the total patient hours to determine the direct cost per patient hour.
Direct Cost per Patient Hour = $4,500,000 ÷ 133,350 = $33.75 To determine the indirect cost per patient hours, the indirect costs allocated to this functional centre (determined in step 2 of Case Costing) are divided by the total patient hours in this functional centre.
Indirect Cost per Patient Hour = $2,145,165 ÷ 133,350 = $16.09 Note that non-workload-distributed costs, such as physician fee-for-service, are also removed from functional centre direct costs before the calculation of functional centre unit direct costs. A separate unit direct cost is calculated for non-workload-distributed costs by dividing these costs by the total functional centre RVUs that are used to distribute these costs. The functional centre unit costs are then applied to each patient as seen in Chapter 6.
5.3 Using the Patient Hours Methodology
5.3.1 Operating Room
The OCCI standard for distributing operating room costs other than patient-specific supplies is the door to door time, which is the time captured as the patient enters and exits the operating room to undergo the surgical procedure. Compared to skin to skin time, it better measures the total time to perform the procedure including patient preparation time. This information can be captured through the OR booking system or schedule.
5.3.2 Obstetrics To better reflect the type of care mothers and neonates receive in Obstetrics (Functional centres 71 25020**** to 71 25090****), the patient hour unit cost for neonates require adjustment. The neonate patient hours are scaled. The scaling factor is based on the birth weight of the neonates. The scaling factors are outlined in Table A. Table A Cost of Neonates greater than 2500g = (2/3) * patient hours * hourly unit cost Cost of Neonates between 2000g to 2500 g = (3/4) * patient hours * hourly unit cost Cost of Neonates less than 2000g (not scaled) = patient hours * hourly unit cost Cost of Mother (not scaled) = patient hours * hourly unit cost
5.3.3 Emergency Room
Emergency Room costs for outpatients can be based on standardized RVUs for each triage level. The Canadian Triage Acuity Scale (CTAS) defines 5 levels of triage according to the perceived need for physician assessment. Many hospitals have developed standardized workload values for each triage level
OCCI Version 6.1 Page 45 of 105 Effective April 2008-March 2009 Updated August 2009
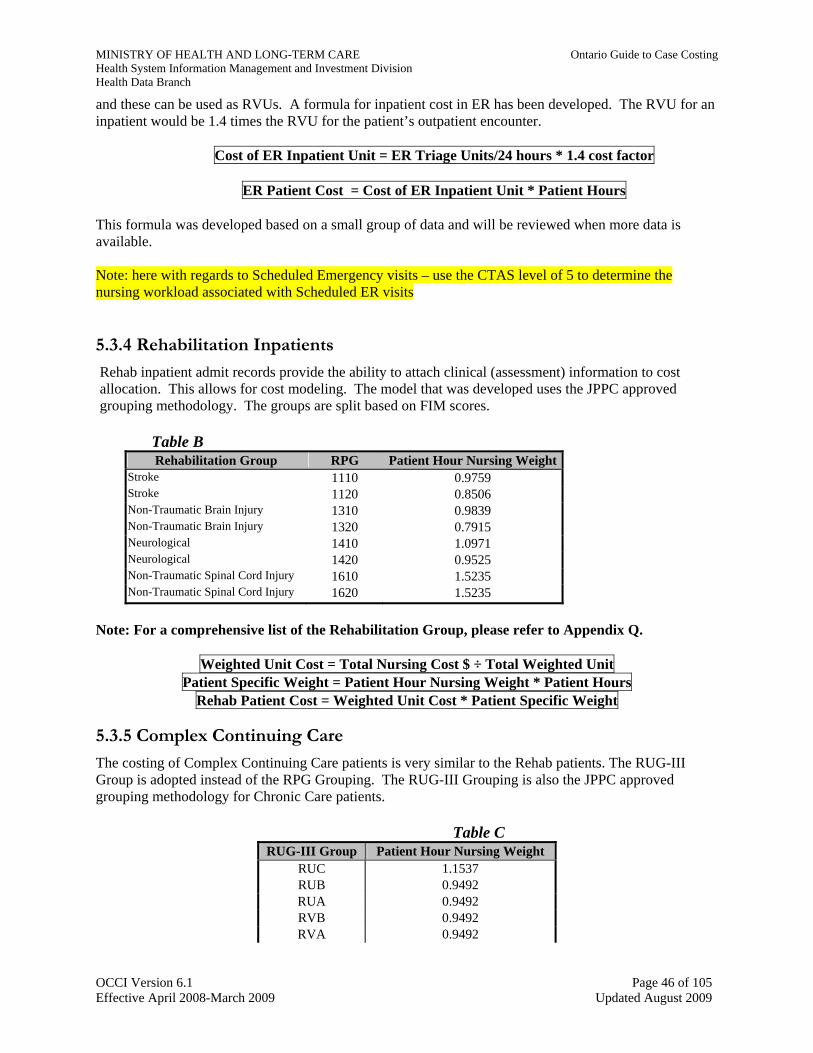
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
and these can be used as RVUs. A formula for inpatient cost in ER has been developed. The RVU for an inpatient would be 1.4 times the RVU for the patient’s outpatient encounter.
Cost of ER Inpatient Unit = ER Triage Units/24 hours * 1.4 cost factor
ER Patient Cost = Cost of ER Inpatient Unit * Patient Hours
This formula was developed based on a small group of data and will be reviewed when more data is available. Note: here with regards to Scheduled Emergency visits – use the CTAS level of 5 to determine the nursing workload associated with Scheduled ER visits
5.3.4 Rehabilitation Inpatients
Rehab inpatient admit records provide the ability to attach clinical (assessment) information to cost allocation. This allows for cost modeling. The model that was developed uses the JPPC approved grouping methodology. The groups are split based on FIM scores.
Table B Rehabilitation Group RPG Patient Hour Nursing Weight
Stroke 1110 0.9759 Stroke 1120 0.8506 Non-Traumatic Brain Injury 1310 0.9839 Non-Traumatic Brain Injury 1320 0.7915 Neurological 1410 1.0971 Neurological 1420 0.9525 Non-Traumatic Spinal Cord Injury 1610 1.5235 Non-Traumatic Spinal Cord Injury 1620 1.5235
Note: For a comprehensive list of the Rehabilitation Group, please refer to Appendix Q.
Weighted Unit Cost = Total Nursing Cost $ ÷ Total Weighted Unit Patient Specific Weight = Patient Hour Nursing Weight * Patient Hours
Rehab Patient Cost = Weighted Unit Cost * Patient Specific Weight
5.3.5 Complex Continuing Care
The costing of Complex Continuing Care patients is very similar to the Rehab patients. The RUG-III Group is adopted instead of the RPG Grouping. The RUG-III Grouping is also the JPPC approved grouping methodology for Chronic Care patients.
Table C RUG-III Group Patient Hour Nursing Weight
RUC 1.1537 RUB 0.9492 RUA 0.9492 RVB 0.9492 RVA 0.9492
OCCI Version 6.1 Page 46 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
RUG-III Group Patient Hour Nursing Weight RHC 0.9155 RHB 0.8560 RMC 0.8371
Note: For a comprehensive list of the RUG-III Group, please refer to Appendix Q.
Weighted Unit Cost = Total Nursing Cost $ ÷ Total Weighted Units
Patient Specific Weight = Patient Hour Nursing Weight * Patient Hours
CCC Patient Cost = Weighted Unit Cost * Patient Specific Weight Note: Facilities need to ensure that all assessments have the appropriate RUG (Resident Utilization Group) assigned. With some external vendors – BC1 & BC2 are not valid RUGs. These are indications of data Quality issues and will impact the calculations for determining workload. For RUG “ZZZ” = 0..8277
Caution: Different RUGs can be assigned for 1 resident stay - - caution must be made when this encountered – will have an impact on the proxy workload assigned..
5.4 Method 2: Calculating Intermediate Product Costs Costs are calculated for all intermediate products in the functional centre. Like functional centre unit costs, intermediate product costs will vary every period. The intermediate product calculation should also be based on a full year of actual statistics and expenditures.
5.4.1 Information Required to Calculate Intermediate Product Costs
Direct Costs (by Cost Category) and Indirect Costs Total direct expenses for the ACCs for the period have been gathered earlier in Step 1 of the case costing process. However, hospitals using this method of costing generally further assign the direct G/L cost data to fixed and variable cost categories. This is achieved by mapping secondary G/L (expense) accounts to the appropriate cost categories, as shown in Table 5.1. Direct costs are broken down into fixed and variable detail so that the cost of each resource component can be distributed using the most appropriate RVU. Total indirect costs for each ACC for the period are taken from the cost allocation calculation in Step 2 of the case costing process.
Total Relative Value Units (by Cost Category)
RVUs are assigned to each resource component of each intermediate product in the functional centre and serve as the basis for cost distribution. In most cases, the RVUs are based on workload units. If workload is used to distribute costs to patients, use only patient specific workload (service recipient workload). (see Section 5.6, Workload as a Basis for Cost Distribution—Patient-Specific vs. Non-Patient-Specific Units). For some intermediate products, use non-workload RVUs as the standard for cost distribution because they are more appropriate distribution bases.
OCCI Version 6.1 Page 47 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
For the Intermediate Product Costing approach, the products/services received by each patient must be tracked. Both utilization and relative value unit information is needed to calculate total RVUs.
Other Non-Workload Distributed Costs
These expenses, such as physician fee-for-service, should be mapped to a distinct cost category to separate them from workload distributed costs. This separation is necessary so that costs can be associated with more suitable RVUs that will serve as the basis for distributing these costs to patients.
Patient-Specific Supplies and Drugs
The costs of patient-specific supplies over $250, drugs and other microcosted items must be assigned directly to the patient. In practice, hospitals may accomplish this by creating intermediate products and assigning a variable supply RVU to the product that is equivalent to the cost of the item. All other cost categories are associated with RVUs equal to zero. When the cost calculations are completed, the cost of the microcosted item is assigned to the patient.
5.4.2 Intermediate Product Cost Calculation The intermediate product cost calculation is more complex than the functional centre unit cost calculation, and has therefore been broken down into four steps.
Step 1 – Calculate Total Relative Value Units
The first step is to calculate total RVUs for each cost category across all intermediate products in the functional centre. Use utilization and RVU information to determine total RVUs. First multiply intermediate product utilization for the period by the corresponding RVU for each product in the cost category. These RVUs are then totaled across all intermediate products in the cost category to produce the total RVUs by cost category.
Step 2 – For Each Cost Category, Calculate the Average Cost per Relative Value Unit
Next calculate an average cost per RVU for each cost category. This calculation involves dividing the total costs in each cost category by the total RVUs in the same cost category.
Average Cost per RVU = COST CATEGORY
TOTAL COSTS ÷ COST CATEGORY TOTAL RELATIVE VALUE UNITS
Step 3 – For each Intermediate Product, Calculate the Cost for each Cost Category
The average cost per RVU calculated in the previous step is then multiplied by the intermediate product’s RVU. This calculation is performed for all cost categories.
Cost Category Product Cost = Average Cost per
RVU × Product RVU
The result of the calculation is the cost for each resource component of the intermediate product.
Step 4 – Calculate the Total Direct and Total Indirect Cost for Each Product
The direct fixed and variable costs of the intermediate product are summed to produce the total direct cost of the product. In contrast, the indirect cost of the intermediate product is calculated using only the
OCCI Version 6.1 Page 48 of 105 Effective April 2008-March 2009 Updated August 2009
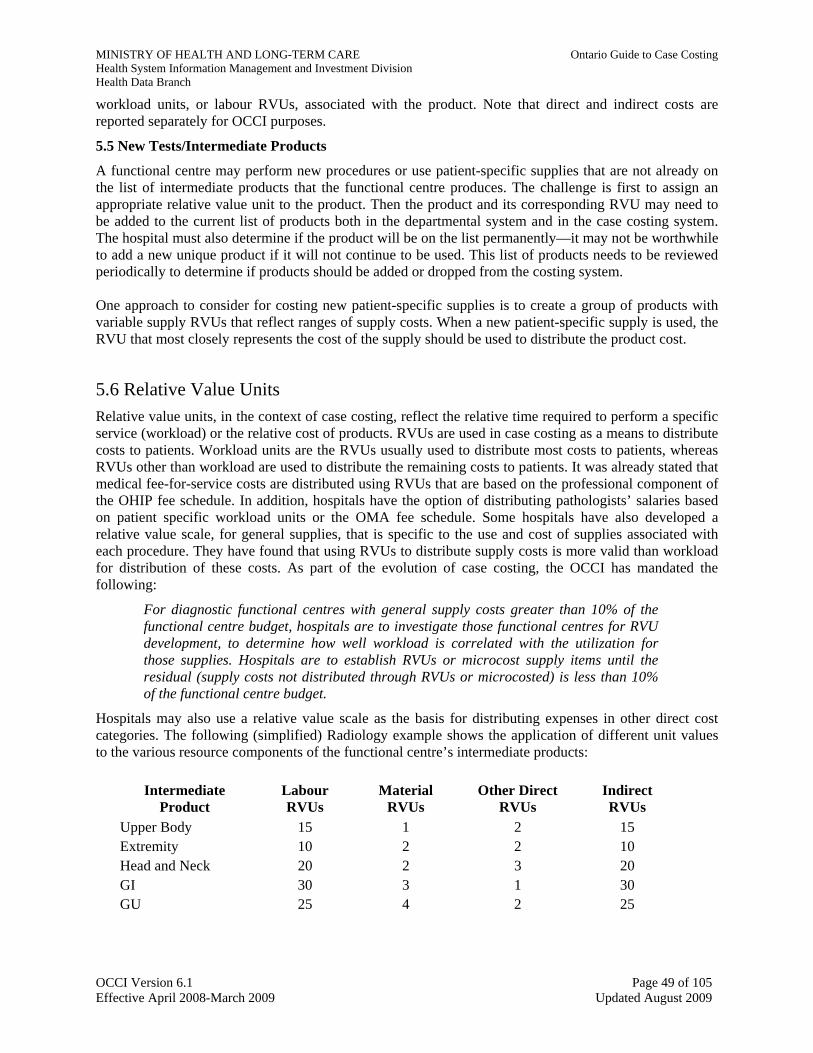
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
workload units, or labour RVUs, associated with the product. Note that direct and indirect costs are reported separately for OCCI purposes.
5.5 New Tests/Intermediate Products
A functional centre may perform new procedures or use patient-specific supplies that are not already on the list of intermediate products that the functional centre produces. The challenge is first to assign an appropriate relative value unit to the product. Then the product and its corresponding RVU may need to be added to the current list of products both in the departmental system and in the case costing system. The hospital must also determine if the product will be on the list permanently—it may not be worthwhile to add a new unique product if it will not continue to be used. This list of products needs to be reviewed periodically to determine if products should be added or dropped from the costing system. One approach to consider for costing new patient-specific supplies is to create a group of products with variable supply RVUs that reflect ranges of supply costs. When a new patient-specific supply is used, the RVU that most closely represents the cost of the supply should be used to distribute the product cost.
5.6 Relative Value Units Relative value units, in the context of case costing, reflect the relative time required to perform a specific service (workload) or the relative cost of products. RVUs are used in case costing as a means to distribute costs to patients. Workload units are the RVUs usually used to distribute most costs to patients, whereas RVUs other than workload are used to distribute the remaining costs to patients. It was already stated that medical fee-for-service costs are distributed using RVUs that are based on the professional component of the OHIP fee schedule. In addition, hospitals have the option of distributing pathologists’ salaries based on patient specific workload units or the OMA fee schedule. Some hospitals have also developed a relative value scale, for general supplies, that is specific to the use and cost of supplies associated with each procedure. They have found that using RVUs to distribute supply costs is more valid than workload for distribution of these costs. As part of the evolution of case costing, the OCCI has mandated the following:
For diagnostic functional centres with general supply costs greater than 10% of the functional centre budget, hospitals are to investigate those functional centres for RVU development, to determine how well workload is correlated with the utilization for those supplies. Hospitals are to establish RVUs or microcost supply items until the residual (supply costs not distributed through RVUs or microcosted) is less than 10% of the functional centre budget.
Hospitals may also use a relative value scale as the basis for distributing expenses in other direct cost categories. The following (simplified) Radiology example shows the application of different unit values to the various resource components of the functional centre’s intermediate products:
Intermediate Product
Labour RVUs
Material RVUs
Other Direct RVUs
Indirect RVUs
Upper Body 15 1 2 15 Extremity 10 2 2 10 Head and Neck 20 2 3 20 GI 30 3 1 30 GU 25 4 2 25
OCCI Version 6.1 Page 49 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Note that indirect costs should be distributed using workload units (the labour RVUs) and not other hospital-specific RVUs. If the hospital has developed RVUs to distribute any of the direct costs, submit a written description of the methodology to the OCCI for review. The description should include a point-form review and description of:
Rationale Why was this approach chosen? What other approaches were considered and rejected?
Comparison Data How do the RVUs differ on a procedure by procedure basis from the NWMS? Provide a list of groups, procedures within groups and relative unit values.
RVU Development Describe a one-time analysis or study that was completed to establish relative values or other factors. If grouped, describe how procedures were assigned to their respective groups.
State of Implementation Has this methodology been implemented? If implemented, how long has it been in use? What follow-up study has been done to validate the approach?
OCCI Version 6.1 Page 50 of 105 Effective April 2008-March 2009 Updated August 2009
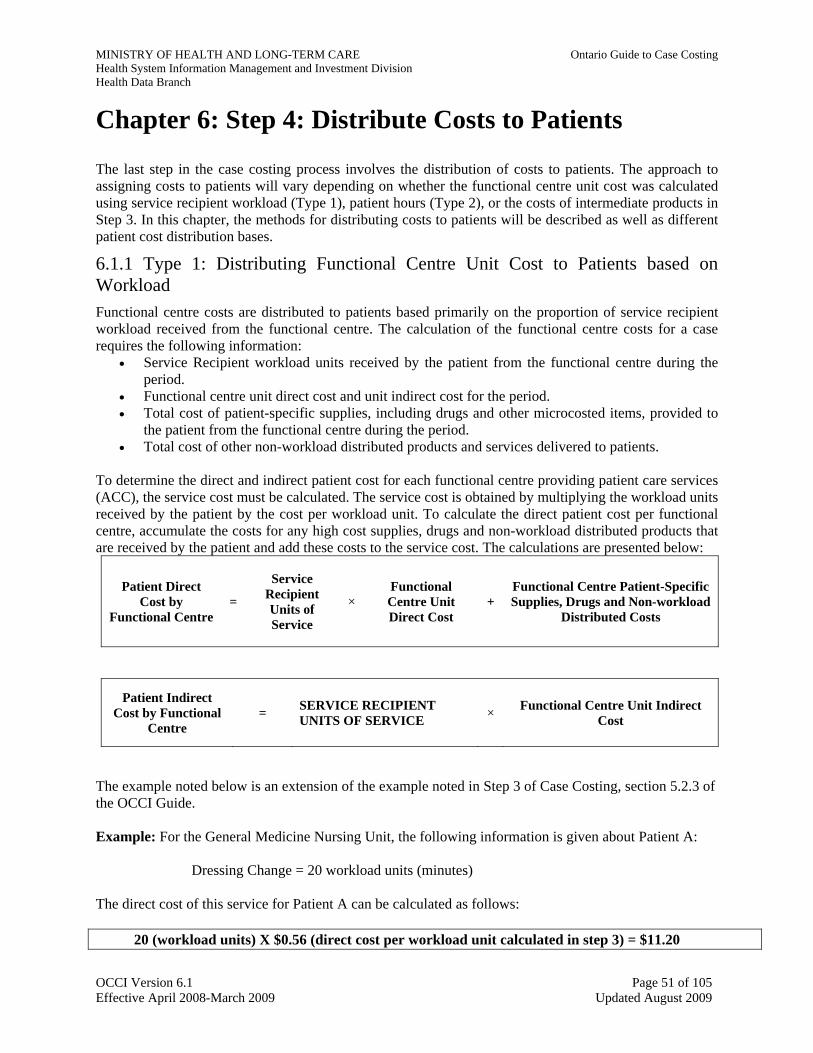
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 6: Step 4: Distribute Costs to Patients The last step in the case costing process involves the distribution of costs to patients. The approach to assigning costs to patients will vary depending on whether the functional centre unit cost was calculated using service recipient workload (Type 1), patient hours (Type 2), or the costs of intermediate products in Step 3. In this chapter, the methods for distributing costs to patients will be described as well as different patient cost distribution bases.
6.1.1 Type 1: Distributing Functional Centre Unit Cost to Patients based on Workload Functional centre costs are distributed to patients based primarily on the proportion of service recipient workload received from the functional centre. The calculation of the functional centre costs for a case requires the following information:
• Service Recipient workload units received by the patient from the functional centre during the period.
• Functional centre unit direct cost and unit indirect cost for the period. • Total cost of patient-specific supplies, including drugs and other microcosted items, provided to
the patient from the functional centre during the period. • Total cost of other non-workload distributed products and services delivered to patients.
To determine the direct and indirect patient cost for each functional centre providing patient care services (ACC), the service cost must be calculated. The service cost is obtained by multiplying the workload units received by the patient by the cost per workload unit. To calculate the direct patient cost per functional centre, accumulate the costs for any high cost supplies, drugs and non-workload distributed products that are received by the patient and add these costs to the service cost. The calculations are presented below:
Patient Direct Cost by
Functional Centre =
Service Recipient Units of Service
× Functional Centre Unit Direct Cost
+ Functional Centre Patient-Specific Supplies, Drugs and Non-workload
Distributed Costs
Patient Indirect Cost by Functional
Centre = SERVICE RECIPIENT
UNITS OF SERVICE × Functional Centre Unit Indirect Cost
The example noted below is an extension of the example noted in Step 3 of Case Costing, section 5.2.3 of the OCCI Guide. Example: For the General Medicine Nursing Unit, the following information is given about Patient A: Dressing Change = 20 workload units (minutes) The direct cost of this service for Patient A can be calculated as follows:
20 (workload units) X $0.56 (direct cost per workload unit calculated in step 3) = $11.20
OCCI Version 6.1 Page 51 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
The indirect cost of this service can be calculated as:
20 (workload units) X $0.27 (indirect cost per workload unit calculated in step 3) = $5.40 These steps are then repeated to determine the full (direct and indirect) cost for each patient seen and cared for by the functional centre.
As noted in the MIS Standards 2006, the level at which services are costed within a health service organization depend on the detail available from the workload measurement system, coupled with the desire of the user to know the costs by particular service or group of services for management purposes. For example, if care plans are in place, it can prove valuable to know the cost of the exact services each service recipient received when conducting utilization analysis. On the other hand, some of the nursing workload measurement systems, aggregate workload units related to all of the services provided to a service recipient during one inpatient day (e.g. change dressing, administer medication, take vital signs, ambulate with assistance, etc.).
Note that the patient’s portion of non-workload distributed direct costs is obtained by multiplying the service recipient RVUs by the cost per RVU.
6.1.2 Type 2: Distributing Functional Centre Unit Cost to Patients based on Patient Hours This process is similar to the workload costing method. It requires the following information:
• Patient hours received by the patient from the functional centre during the period. • Functional centre unit direct cost and unit indirect cost for the period. • Total cost of patient-specific supplies, including drugs and other microcosted items, provided to
the patient from the functional centre during the period. • Total cost of other non-workload distributed products and services delivered to patients.
To determine the direct and indirect patient cost for each functional centre providing patient care services (ACC), the service cost must be calculated. The service cost is obtained by multiplying the patient hours received by the patient by the cost per hour. To calculate the direct patient cost per functional centre, the costs for any high cost supplies, drugs and non-workload distributed products received by the patient must be added to the service cost. The calculations are presented below:
Patient Direct Cost by Functional
Centre = Patient-
Hours × Functional Centre Unit Direct Cost
+
Functional Centre Patient-Specific Supplies, Drugs and Non-workload Distributed
Costs
Patient Indirect Cost by Functional
Centre = PATIENT HOURS × Functional Centre Unit
Indirect Cost
OCCI Version 6.1 Page 52 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Example: For the General Medicine Nursing Unit, the following information is given about Patient A: Patient Hours in General Medicine Nursing Unit = 2 Hours The direct cost of this service for Patient A can be calculated as follows:
2 (Patient Hours) X $ 50 (direct cost per workload unit calculated in step 3) = $ 100 The indirect cost of this service can be calculated as
2 (Patient Hours) X $ 20 (indirect cost per patient hour calculated in step 3) = $40
Total Cost = Direct Cost + Indirect CostPatient A Total Cost = $ 100 + 40 These steps are then repeated to determine the full (direct and indirect) cost for each patient provided by the functional centre.
6.2 Intermediate Product Costing Intermediate product costs are also distributed to patients primarily through RVUs. The assignment of costs to patients is accomplished by tracking the type and number of different products received by the patient. The costs of these products (calculated in Step 3) are then attached to the patient.
6.3 Patient Cost Distribution Bases The suggested bases for distribution of direct expenses (Labour, Material, Other and Building and Equipment) to patients have been developed based on the MIS Standards, with minor refinements as noted below. The distribution bases are as shown in Table 6.1. In particular, note the following:
Direct Labour:
• Medical fee-for-service costs (MIS Secondary Account 3 90 90) are to be distributed to patients based on the units of service received. Units of service are computed using the professional component of the OHIP Fee Schedule as an RVU for services received.
• Pathologist salary costs can be distributed to patients based on either patient-specific workload units or the OMA Professional Fee Schedule.
• Other physician salaries (if applicable) can be distributed via patient care workload associated with the functional centres they provide service to.
Note that the patient-specific workload units used to distribute physician salary costs are those workload units associated with unit-producing functional centre staff (i.e., nurses, technicians, etc.). Remember that physicians are not required to collect workload.
Direct Material (Supplies):
• Patient-specific supplies (including drugs) are “charged” directly to the patient and accumulated based on actual costs incurred.
• General supplies in the diagnostic functional centres which are greater than 10% of the functional centre budget should be distributed to patients based on RVUs or microcosted
OCCI Version 6.1 Page 53 of 105 Effective April 2008-March 2009 Updated August 2009
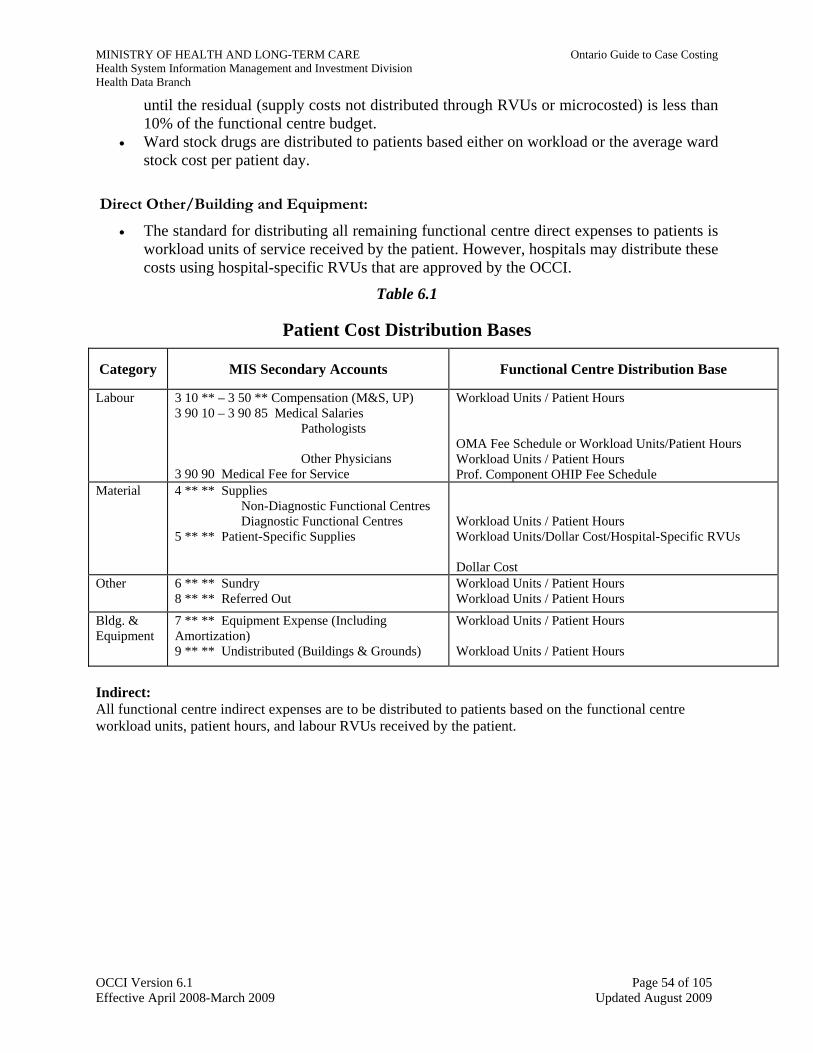
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
until the residual (supply costs not distributed through RVUs or microcosted) is less than 10% of the functional centre budget.
• Ward stock drugs are distributed to patients based either on workload or the average ward stock cost per patient day.
Direct Other/Building and Equipment:
• The standard for distributing all remaining functional centre direct expenses to patients is workload units of service received by the patient. However, hospitals may distribute these costs using hospital-specific RVUs that are approved by the OCCI.
Table 6.1
Patient Cost Distribution Bases
Category MIS Secondary Accounts Functional Centre Distribution Base
Labour 3 10 ** – 3 50 ** Compensation (M&S, UP) 3 90 10 – 3 90 85 Medical Salaries
� Pathologists
� Other Physicians 3 90 90 Medical Fee for Service
Workload Units / Patient Hours OMA Fee Schedule or Workload Units/Patient Hours Workload Units / Patient Hours Prof. Component OHIP Fee Schedule
Material 4 ** ** Supplies � Non-Diagnostic Functional Centres � Diagnostic Functional Centres
5 ** ** Patient-Specific Supplies
Workload Units / Patient Hours Workload Units/Dollar Cost/Hospital-Specific RVUs Dollar Cost
Other 6 ** ** Sundry 8 ** ** Referred Out
Workload Units / Patient Hours Workload Units / Patient Hours
Bldg. & Equipment
7 ** ** Equipment Expense (Including Amortization) 9 ** ** Undistributed (Buildings & Grounds)
Workload Units / Patient Hours Workload Units / Patient Hours
Indirect: All functional centre indirect expenses are to be distributed to patients based on the functional centre workload units, patient hours, and labour RVUs received by the patient.
OCCI Version 6.1 Page 54 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 7: Bringing It All Together Over the previous chapters, the four steps of case costing have been explained in detail. At this point, the cost data should be available for each patient from each functional centre that provided intermediate products to the patient during the hospital visit. The patient descriptive clinical data associated with each patient’s visit is also available from the Health Records abstracting system. The main objective of case costing is to combine these two types of data to calculate the costs of the patient-specific mix of products and services received by each patient. This chapter explains how to bring all of the statistical, financial and clinical data together and discusses the final output. It describes the format of the departmental feeds that input data into the case costing system as well as the format of the final case cost data. It is important to remember the definition of the encounter, since the costs are assigned to each patient based on the services/intermediate products received during the encounter. The definition of the encounter depends on the type of case (e.g., acute inpatient, day surgery, ambulatory care or chronic care).
7.1 Departmental Data is Interfaced with the Case Costing System
To understand how the data will come together, it is important to visualize where the data comes from. Each clinical functional centre has collected workload or patient hour units and statistical data on a patient-specific basis. The financial data has been recorded in the financial systems (e.g., payroll, general ledger, capital assets module, etc.). All of this data must be linked together and transferred to the case costing system to calculate the costs for each patient encounter. Most hospitals have an A/D/T (admission, discharge and transfer) system that collects each patient’s encounter data, which includes admission date, chart number and health insurance number. The A/D/T system assigns a registration number to each visit. The data from the A/D/T system uniquely identifies each patient encounter. In addition, the system usually tracks the patient through the hospital, recording the Nursing unit to which the patient is admitted. It is recommended that hospitals have mechanisms in place that interface the A/D/T information with each departmental information system, so that these data elements do not need to be re-entered at the department level. An interface to the A/D/T system also enables validation that all patients who are registered in a particular Nursing unit, for example, receive workload or patient hour units for each day of their stay. During the costing process, the financial and workload/statistical data from the departmental systems is fed into the case costing system. Depending on the costing system, either patient-specific workload or utilization is compiled into the costing system. Unit costs are calculated and then distributed to patients. Patient descriptive data is pulled in from the Health Records abstracting system to provide additional information, such as procedure and diagnosis detail and the case mix group (CMG) assignment, to the data.
OCCI Version 6.1 Page 55 of 105 Effective April 2008-March 2009 Updated August 2009
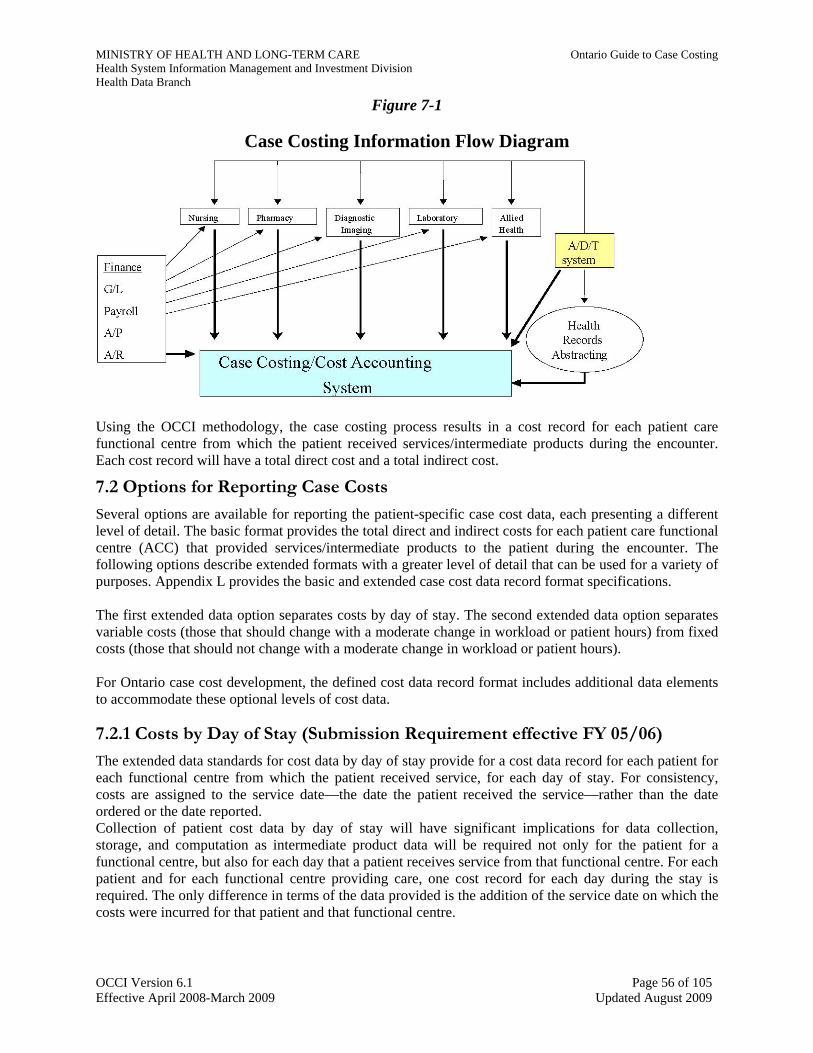
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 7-1
Case Costing Information Flow Diagram
Using the OCCI methodology, the case costing process results in a cost record for each patient care functional centre from which the patient received services/intermediate products during the encounter. Each cost record will have a total direct cost and a total indirect cost.
7.2 Options for Reporting Case Costs
Several options are available for reporting the patient-specific case cost data, each presenting a different level of detail. The basic format provides the total direct and indirect costs for each patient care functional centre (ACC) that provided services/intermediate products to the patient during the encounter. The following options describe extended formats with a greater level of detail that can be used for a variety of purposes. Appendix L provides the basic and extended case cost data record format specifications. The first extended data option separates costs by day of stay. The second extended data option separates variable costs (those that should change with a moderate change in workload or patient hours) from fixed costs (those that should not change with a moderate change in workload or patient hours). For Ontario case cost development, the defined cost data record format includes additional data elements to accommodate these optional levels of cost data.
7.2.1 Costs by Day of Stay (Submission Requirement effective FY 05/06) The extended data standards for cost data by day of stay provide for a cost data record for each patient for each functional centre from which the patient received service, for each day of stay. For consistency, costs are assigned to the service date—the date the patient received the service—rather than the date ordered or the date reported. Collection of patient cost data by day of stay will have significant implications for data collection, storage, and computation as intermediate product data will be required not only for the patient for a functional centre, but also for each day that a patient receives service from that functional centre. For each patient and for each functional centre providing care, one cost record for each day during the stay is required. The only difference in terms of the data provided is the addition of the service date on which the costs were incurred for that patient and that functional centre.
OCCI Version 6.1 Page 56 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
7.2.2 Variable/Fixed Detail - Option for Internal Reporting
A cost that varies directly with the volume of service or activity.
The fixed or variable categorization of MIS Secondary Accounts is shown in Table 7.1 for reference. The account definitions are described in detail in the MIS Standards. Section 5.1 of this Guide explains the MIS account definitions and their application to case costing.
Table 7.1
MIS Secondary Accounts by Variable/Fixed Detail Direct Variable Costs MIS Secondary Accounts
Labour Compensation (Including Benefits): 3 50 ** Unit Producing 3 90 90 Medical Fee-for-Service
Material 4 ** ** Supplies 5 ** ** Patient-Specific Supplies
Other 8 ** ** Referred Out Direct Fixed Costs
Labour Compensation (Including Benefits): 3 10 ** Management/Operational Support 3 90 10 to 3 90 85 Medical (Salaried Physicians)
Other—Sundry 6 ** ** Sundry Building, Equipment and Grounds 7 ** ** Equipment Expense (Inc. Amortization)
9 ** ** Undistributed (Building and Grounds)
These cost records provide a more detailed breakdown of the direct and indirect costs as follows:
• Direct Costs – Variable Labour – Variable Patient-Specific Material – Variable Material - Supplies – Variable Other - Referred out – Fixed Labour – Fixed Other - Sundry – Fixed Equipment, Building and Grounds
• Indirect Costs – Variable – Fixed
7.2.3 Service-Specific Data Elements In the case cost data record, there are two fields that are submitted only for chronic care cases: the MDS reference date and the MDS sequence number. The MDS reference date must match the date submitted to CIHI on the Chronic Care MDS for each patient. The MDS sequence number identifies the specific MDS assessment for each patient. For example, a patient’s first MDS assessment may get the MDS sequence number “1,” the second assessment would get the sequence number “2,” and so on.
OCCI Version 6.1 Page 57 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
For acute inpatient cases, hospitals have the option of reporting the CMG Complexity level from the hospital’s inpatient abstracting system and grouper, if available.
7.2.4 Procedure Detail It is an option to keep the intermediate products (procedure detail) available in a format that will facilitate further analysis if required. Much of this information is needed to calculate and distribute costs to patients. For example, workload units in different categories would be accumulated and used to calculate Pharmacy labour cost for reporting. There is no one standard coding system readily available to cover the wide range of possible procedures. Hospitals will use its own coding scheme for procedure detail, and any comparative analysis among hospitals will require reconciliation of the different hospitals' coding systems. It is recommended that hospitals that do not have established internal codes use NWMS or provincial fee schedule codes. OCCI hospitals do not submit procedure cost data routinely, but may keep it available at the hospital along with a list of procedures and relative value units associated with each procedure number used by the hospital. If there is a decision to keep procedure data, it should be organized into records with the following information in each:
• Patient Encounter Identifier: Register or Account Number • Functional Centre Code (to MIS Level 5) • Service Date • Code of Procedure Incurred (per hospital format) • Number of times procedure done on this date • Name of Procedure (optional) • Relative value/workload units of procedure (optional)
7.3 A Framework for “Case” Costing
The care provided for a given health condition can involve a variety of different interactions between the patient and the hospital. It would be of great value to be able to measure the cost of treating a patient over the entire episode of illness, to get the true “case” cost. For example, many patients have a surgical procedure done on an inpatient basis and are subsequently seen in the outpatient clinics for follow-up. Both the inpatient and outpatient costs are related to the same health condition. Linking the costs of the related visits together would provide a better estimate of treating that patient. The process of developing true “case” costs by linking related patient encounters is now more feasible with the addition of ambulatory (including day surgery) and chronic care costing. The OCCI has developed a basic conceptual framework to link related encounters (Figure 7-2).
OCCI Version 6.1 Page 58 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 7-2
Clinical Case Costing Framework
The framework is composed of six levels: 1. Product – the single intermediate product (or service) a patient receives; 2. Encounter – the unique presentation to the facility, usually recorded at the point of entry; 3. Episode – a roll-up of related encounters (e.g., acute inpatient, ambulatory, chronic care and
rehabilitation); 4. Reporting entity - the hospital in which the patient is being treated; 5. Case – the given health condition; and 6. Patient – the individual patient.
The framework starts at the bottom at Level 1. This is the level at which detailed information on intermediate product utilization is captured. These products are associated with a specific Encounter (e.g., an acute inpatient admission, an outpatient visit, or a chronic care stay). Each Encounter can be grouped into an Episode. Each Episode occurs at the Reporting Entity or the facility in which the patient is being treated. A Case is the underlying health condition that requires the use of health services at various Reporting Entities. Lastly, Level 6 is the individual patient. Currently, Level 2 of the Framework is achieved. The OCCI collects costs at the Encounter level. The critical piece of the framework is Level 5, the Case Level. A standardized Case Typing methodology that would allow related encounters of a given health condition to be linked is not yet available. This methodology has been referred to as an “Episode Grouper” or a “Super Grouper”. Some examples of a Case Type are Oncology, Dialysis, Pregnancy and Diabetes. These Case Types are intuitively appealing, as they are consistent with many hospitals’ programs.
OCCI Version 6.1 Page 59 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
OCCI hospitals have agreed that an informal Case Typing system can be developed and implemented on a pilot basis. The OCCI has developed a set of standards to guide the implementation of the framework, such that infrastructure can be built to accommodate future additions to the framework. For instance, the Case Typing system will likely be associated with a numerical system. Hospitals can then develop their information systems to eventually accommodate a number field for the Case Type.
The framework also facilitates the addition of other health care providers, such as doctor’s offices, community clinics and home care organizations, which can be added at Level 4 as other reporting entities. Although this is not likely to be implemented at the provincial level, local communities would be able to utilize this framework to better coordinate services (and information collection) to create a seamless health care delivery system.
OCCI Version 6.1 Page 60 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 8: Departmental Case Costing Standards
8.1 Nursing Inpatient Functional Centres
The costs Nursing Inpatient Functional Centres can be distributed using either nursing workload or patient hours. Both methods have been described in detail in Chapters 5 and 6.
Other Unit-Producing Nursing Staff Other Unit-Producing Nursing Staff such as Clinical Nurse Specialists, Enterostomal Therapists, and Patient Educators often provide services to patients on several units. Ideally, labour and benefits costs for these positions would be distributed to the responsible Nursing units on the basis of the proportion of time spent on each unit.
Reliability and Validity of Data The concern over data reliability and validity is a significant and widespread issue for all elements of the costing process. Since Nursing costs represent a major component of the cost of care, guidelines for the monitoring of Nursing workload measurement or Patient Hours should be followed closely to provide assurance of the reliability and validity of Nursing data. For Nursing Workload, there are two very different aspects to monitor the quality of data for case costing. The first aspect addresses the application of the workload measurement tool by the Nursing staff. The second relates to ensuring that patients are not missed, that workload is assigned consistently among nurses (inter-rater reliability) and that patient and unit specific Nursing workload data is transferred to the costing system without loss or error. For Patient Hours, the A/D/T system must be monitored and audited. One audit that is highly recommended is to compare Patient Hours with length of stay. This should be equal. This will ensure that patient hours were not missed during the patient's stay. It will ensure that the patient hours used to allocate costs to patients is of high quality. An important factor is to ensure inter-rater reliability with the registration staff. All registration staff should follow the same process for admitting, discharging and transferring patients. Ongoing education sessions are encouraged. The registration staff should be aware that the way a patient is admitted, discharged or transferred could have impacts to case costing.
Data Reliability Targets For workload measurement systems that are based on patient types, 90% reliability is expected, while for factorial or indicator driven systems the goal is 85% reliability.
8.2 Allied Health
In Ontario, hospitals are required to report Allied Health workload using the Generic Workload Reporting Framework. The development of multidisciplinary teams reporting to a single manager has created the need for comparable workload data across professions. The Joint Policy and Planning Committee (JPPC) has prepared a series of documents to assist the professions required to report under the new Generic Workload Reporting Framework. Appendix E also provides an overview of the Framework. The Framework for nursing workload can also be used for workload measurement in the Allied Health departments. Allied Health typically includes the following departments:
• Audiology;
OCCI Version 6.1 Page 61 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
• Child Life; • Chiropody; • Clinical Nutrition; • Occupational Therapy; • Pastoral Care; • Physiotherapy; • Psychology; • Rehabilitation Engineering; • Social Work; • Speech Language Pathology; and • Therapeutic Recreation.
Key issues for implementing case costing in these areas include the following:
• Capturing both departmental and patient-specific workload; • Capturing general and patient-specific supplies charges; • Capturing labour hours in the functional centre where the work is done; and • Setting up an audit program to ensure the reliability and validity of data produced.
NWMS have been developed for all of the allied health departments. A complete listing of National Workload Measurement Systems can be found in the MIS Standards 2006, Chapter 4. The original purpose of workload measurement was to get a picture of the full range of departmental activity. Statistics such as ‘total units produced’ and ‘ratio of service recipient to non-service recipient workload units’ were, and continue to be, important for departmental management. The challenge in implementing case costing is to work out how to organize data collection to produce both the statistics used traditionally and the number of service recipient workload units for each patient. The recording forms may already give a head start, so only re-organization is needed to summarize the units for reporting. Most of the NWMS provide sample forms for patient-specific recording. Patient-specific data recording can become cumbersome, as in the example that requires one record sheet per patient compared to several patients per record sheet in the basic patient care record. If workload statistics are accumulated and reported using a software package, make sure that the program can provide service recipient units by patient.
8.3 Clinical Nutrition
If the hospital opts to distribute patient-specific clinical nutrition costs, Clinical Nutrition should be set up in its own functional centre (OHRS Functional Centre 71445). Prior to April 1, 2004, Patient Food Services (OHRS Functional Centre 71195) costs were allocated as indirect costs using patient meal days as an allocation base. Effective April 1, 2004, Patient Food Services costs are to be distributed as direct costs.
8.4 Clinical Laboratory
The NWMS should be used to generate workload units for the Clinical Laboratory. Ontario hospitals have had some experience with OHIP LMS codes and units. This system exists to support laboratory licensing and, with unit values attached, supports billing/payments for private medical laboratories. This is a gross coding system that uses the same code for a test regardless of the specimen. For some tests there is a significant difference in workload between testing serum or testing plasma. Historically, the LMS unit values have not been representative of true workload and are thus not useful for case costing. The codes
OCCI Version 6.1 Page 62 of 105 Effective April 2008-March 2009 Updated August 2009
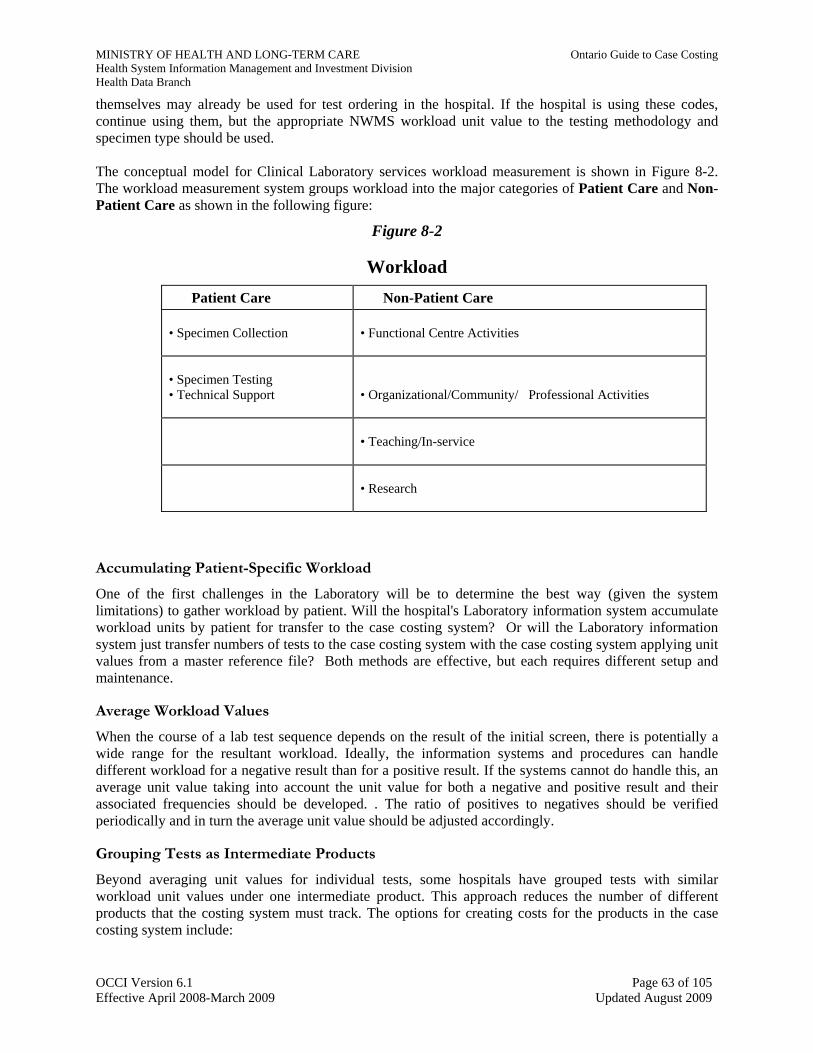
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
themselves may already be used for test ordering in the hospital. If the hospital is using these codes, continue using them, but the appropriate NWMS workload unit value to the testing methodology and specimen type should be used. The conceptual model for Clinical Laboratory services workload measurement is shown in Figure 8-2. The workload measurement system groups workload into the major categories of Patient Care and Non-Patient Care as shown in the following figure:
Figure 8-2
Workload Patient Care Non-Patient Care
• Specimen Collection
• Functional Centre Activities
• Specimen Testing • Technical Support
• Organizational/Community/ Professional Activities
• Teaching/In-service • Research
Accumulating Patient-Specific Workload One of the first challenges in the Laboratory will be to determine the best way (given the system limitations) to gather workload by patient. Will the hospital's Laboratory information system accumulate workload units by patient for transfer to the case costing system? Or will the Laboratory information system just transfer numbers of tests to the case costing system with the case costing system applying unit values from a master reference file? Both methods are effective, but each requires different setup and maintenance.
Average Workload Values When the course of a lab test sequence depends on the result of the initial screen, there is potentially a wide range for the resultant workload. Ideally, the information systems and procedures can handle different workload for a negative result than for a positive result. If the systems cannot do handle this, an average unit value taking into account the unit value for both a negative and positive result and their associated frequencies should be developed. . The ratio of positives to negatives should be verified periodically and in turn the average unit value should be adjusted accordingly.
Grouping Tests as Intermediate Products Beyond averaging unit values for individual tests, some hospitals have grouped tests with similar workload unit values under one intermediate product. This approach reduces the number of different products that the costing system must track. The options for creating costs for the products in the case costing system include:
OCCI Version 6.1 Page 63 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
• Individual Costs Only: Actual costs for each test. • Combination Individual and Grouping: Actual costs for high volume/cost tests and tests with
similar costs grouped and charged at an average cost for the group. • Full Grouping: Tests with similar costs grouped and charged at an average cost for the group.
If tests are grouped for costing, a record should be kept of this methodology for future reference when costs or groups must be updated in the system. There should be a routine mechanism in place to maintain the test costs in the system (whether using individual costs or cost groups). The number of workload units assigned to a group should be calculated using a weighted average (by volume) of the workload units of each lab test within the group.
Clinical Laboratory: One Functional Centre or Many? The MIS Standards provide a range of functional centre codes for the Laboratory. Setting up separate functional centres for each laboratory section will help generate better case costs, but at the penalty of added coding and management reporting. Some of the advantages of separate functional centres by laboratory section include:
• Patients receiving testing from sections with higher equipment or supply costs will also receive those higher costs; and
• Patients receiving testing from sections with higher quality control or calibration standards requirements will also receive the associated higher costs.
In terms of disadvantages, there will be a need to track all categories of workload units, labour hours, supply and equipment costs to each functional centre.
Alternative Distribution of Equipment and Supply Costs Some hospitals have found that labour workload is not representative of equipment or supply costs for particular tests, procedures or functional centres. This Guide recommends a case costing methodology that uses workload as the distribution base for functional centre costs to cases, as this approach provides reasonably good case costs with simplicity. The hospital may want to use a more refined approach, developing an RVU for equipment and supply costs, as mentioned in Section 6.3. If so, refer to Chapter 5 for further background.
Patient Care and Non-Patient Care Workload Some Clinical Laboratory patient care workload cannot be linked to specific patients. This patient care workload (in the left branch in Figure 9-2) is then related to quality control or calibration standards. These activities do generate valid workload, but not workload that can be readily assigned to each patient. Only patient-specific patient care units are used in case costing to calculate functional centre unit costs and to distribute costs to patients. The general approach for calculating unit costs is to use only patient-specific workload units, as described in Section 5.6. Using the workload distribution data shown in Section 5.6 as an example, the Clinical Chemistry Laboratory would report 655,000 units of workload for the period. However, for case costing purposes, the unit costs of Clinical Chemistry will be calculated using the 570,000 total patient-specific units recorded in the period. Note: Include inpatients, outpatients, and those referred-in when calculating the total workload units for the unit cost calculation.
OCCI Version 6.1 Page 64 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Referred-Out Tests For most hospitals, referred-out tests represent a small proportion of their clinical laboratory costs. The average cost for a referred-out test is established based on actual charges from invoices, and charged to the case as an expense. Although there is no workload associated with performing the test, the specimen handling workload units must still be assigned to the case.
New Tests/Intermediate Products As discussed in Chapter 5, the Laboratory functional centres may periodically introduce new tests that will need to be added to the list of intermediate products. Please consult Section 5.5 for more details on how to develop costs for new products. Some OCCI hospitals have found that their Laboratory information systems could not readily add new tests, so they accepted that the units for doing those added tests would simply be handled as other patient care workload that cannot be linked to specific patients.
Physician Fees and Salaries Hospital laboratories may have pathologists on staff, either dedicated entirely to several Laboratory functional centres or performing administrative duties in addition to unit-producing activities. Medical pathologist salary expenses are often a significant portion of the costs for the functional centres to which they provide services. First, the hospital must charge the pathologist expenses to those specific laboratory functional centres for which the pathologist provides services. For case costing purposes, the standards allow for two methods of distributing the costs to patients. The costs may either be distributed through the patient-specific workload associated with the laboratory tests or the hospital may develop RVUs, based on the OMA fee schedule. Section 6.3 provides a more detailed explanation of how to distribute these expenses.
8.5 Diagnostic Imaging
The conceptual model for Diagnostic Imaging services workload measurement is shown below. The workload measurement system groups workload into the major categories of patient care and non-patient care as shown in the following figure:
Figure 8-3
Workload Patient Care Non-Patient Care
• Technical Function
• Functional Centre Activities
• Technical Support Function
• Organizational/Community/ Professional Activities
• Teaching/In-service
• Research
Technical function workload includes all technical activities required to perform an examination, procedure or other care for a patient. Technical support function workload includes all of the support
OCCI Version 6.1 Page 65 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
activities that precede or follow the technical functions required to support patient-specific examinations or procedures, including patient reception, report typing and filing, and technical supervision. As previously mentioned, only patient-specific patient care units are used to calculate functional centre unit costs and to distribute costs to patients. In Diagnostic Imaging, the technical function units are the primary basis for calculating functional centre unit costs and distributing costs to patients. In many hospitals, technical support functions are provided by an administrative and support functional centre located within the department. Where such a functional centre has been established, its costs could be distributed to patients based on the proportion of technical support units generated. Alternatively, these functional centre costs could be allocated to the ACC functional centres in Diagnostic Imaging on the basis of proportion of services used by each ACC. The number of technical function units received by the patient would then drive the distribution of costs to patients. Note: 1. Include inpatients, outpatients, and those referred-in when calculating the total technical units for the
unit cost calculation. 2. In the calculation of functional centre unit costs for the department, include both patient-specific
technical and patient-specific technical support units. 3. In the calculation of functional centre unit costs for case costing, include only technical function units. 4. Diagnostic Imaging support and administration costs are to be distributed to the functional centres that
use these services based on: a) the proportion of costs of each diagnostic imaging functional centre; or b) the proportion of total workload of each diagnostic imaging functional centre; or c) the proportion of time spent/services used by each diagnostic imaging functional centre.
Workload units must be recorded for all in-hospital functional centre work (i.e., inpatient, outpatient, referred-in) and referred-out functional centre work. The assigned workload units are the data outputs required for determining unit costs. Technical function workload units must be captured for each patient. Technical function support units should also be tracked for each patient, but may be omitted if tracking is difficult. These units would then be excluded from the calculation of cost per unit.
Grouping Exams as Intermediate Products Some hospitals have grouped exams with similar workload unit values under one intermediate product to reduce the number of different products that must be tracked by the costing system. As with Clinical Laboratory, the options for setting exam products in the case costing system include using individual costs only, a combination of individual and grouping, or full grouping. Refer to Section 9.3 (Clinical Laboratory) for a detailed explanation.
New Procedures/Intermediate Products Refer to Section 9.3 (Clinical Laboratory) and Chapter 5 for details on how to handle costing of new intermediate products.
Physician Fees and Salaries Radiologist costs are often a significant portion of the costs in the Diagnostic Imaging functional centres. Hospitals may have salaried radiologists on staff, or (as in most hospitals) radiologists may be paid by the hospital on a fee-for-service basis. First, the hospital must identify and charge the radiologist salaries or fee-for-service expenses to those specific Diagnostic Imaging functional centres for which the radiologist performs work. Hospitals are required to use the professional component of the OHIP fee schedule as
OCCI Version 6.1 Page 66 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
RVUs to distribute the fee-for-service costs or salary expenses to patients. Chapter 6 (Section 6.3) provides details on the methodology to distribute these expenses.
8.6 Financial Services
Financial Services must be involved in the collection of both financial and statistical information. An understanding of the MIS Standards and the OHRS Chart of Accounts is crucial to avoid many case cost development problems. Key concerns for Financial Services in implementing case costing are discussed in Section 3.1 and Chapter 4. These include the following:
• Converting to the OHRS Chart of Accounts • Categorizing costs correctly; • Auditing data for validity and reliability; and • Implementing cost allocation.
See Appendix M for the questions used in the OCCI Milestone 1 Audit. These questions are designed to help check the progress so that there are no surprises later in the implementation!
Cost Allocation Implementation All functional centres must be included in the cost allocation, whether they provide patient services or not. The fair cost of administration to a Nursing unit is produced by charging all functional centres that benefit, including those that are undistributed or that are non-patient-care. The cost allocation process can be summarized as follows:
• Identify Transient Cost Centres (TCCs) and Absorbing Cost Centres (ACCs); • Determine the allocation base for each TCC; • Develop and maintain simultaneous equations (this step may take the form of entering
information from the first two steps into the cost allocation software); • Allocate total expenses of the TCCs (as indirect costs) to: • each other (reciprocal services) and • each ACC using these services; • Validate allocation of costs.
8.7 Health Records
Many of the important Health Records issues are covered earlier in the Guide (Chapter 3). There is some additional material to help plan and manage implementation. References to other sections are included where the material has been previously covered. Health Records ensures that patient descriptive data are gathered in support of case costing. Although Health Record Department staff typically handles final coding and abstracting, there is considerable organizational effort required so that care providers provide timely and accurate documentation of the patient's care. There are primary issues that Health Records must focus on:
• Ensuring the quality of patient descriptive data; and • Coding of the basic and optional data items needed for case costing.
8.7.1 Ensuring Quality of Patient Descriptive Data All Health Records coding staff must be up to date on current coding issues. One of the major responsibilities of Health Records is to ensure the reliability of coding such that all staff abstract the same
OCCI Version 6.1 Page 67 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
case with the same codes consistently. This can be tested through inter-rater reliability audits in which all coding staff abstract the same cases and compare any differences between coders. If any discrepancies are found, the hospital may need to look at current policies and practices to improve the data quality. Mechanisms must be in place to ensure that coding is complete and that there are no missing or invalid data elements. The abstracting system may have edits or error reports that identify any invalid or incomplete data fields and the abstracting period does not close until the errors are corrected in the system. The hospital may have other mechanisms in place to ensure that patient charts are completed, with policies to contact physicians for queries about the diagnoses or procedures. The value of case costing is the availability of timely data that will assist the hospital in decision making. At the end of the costing period, the OCCI receives the patient abstract data from CIHI. Delays in closing the period due to incomplete data or problems in coding cause a lag in the time that the cost data can be matched with the patient descriptive data. In addition, coding errors may result to patients being classified into the wrong case mix group, overestimating or underestimating the costs for that group. Therefore, the OCCI standards specify a maximum turnaround time of 45 days for charts to be abstracted and sent to CIHI and the data file returned to the hospital.
8.7.2 Coding of Basic and Optional Data Items Needed for Case Costing If a hospital decides to pursue costing of ambulatory or chronic care cases, there is a need to abstract in additional formats—the CIHI National Ambulatory Care Reporting System, Mental Health and Rehabilitation and the Chronic Care Minimum Data Set. These are discussed in Chapter 9.
8.7.3 CIHI Mandatory Data
Additional clarification of certain CIHI mandatory data elements for acute care and day surgery coding is included below. 01-02 Institution Identification
Most hospitals have separate institution numbers (CIHI master numbers) for their Acute Care, Chronic Care, Day Surgery, Rehabilitation Services and Ambulatory Care Services.
03-01 Health Care Number Only the health care number should be entered into this field. A blank will indicate that the number was unavailable. Accurate coding of the health care number will enable linking of patient data across different facilities. A separate field must be set up for the Chart Number that will serve as a unique identifier.
04-01 Admission Date The Ministry of Health and Long-Term Care guidelines recognize of the day of day surgery as the admission day if it leads to an inpatient admission. For inpatient admissions that originate in the Emergency Room, the day of admission into the inpatient unit should be used as the admission date.
02-01 Length of Stay Calculate using CIHI method: Discharge Day minus Admission Day.
04-05 Admission Category Standards for admission category codes do not exist, complicating inter-hospital comparisons.
05-04 Institution To Information should be provided, in the case of out-of-province transfers, on the type of hospital (acute or otherwise) the patient was transferred to.
07-01 Main Patient Service Interpretation may vary from hospital to hospital.
09-01 Doctor Type
OCCI Version 6.1 Page 68 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
CIHI defines Most Responsible Doctor as the physician/surgeon most responsible for the care of the patient and/or who provides care to the patient for the greatest number of days during that patient's hospital stay. Note that subjectivity is a factor in this designation.
09-03 Doctor Service Some physicians have more than one specialty. The hospital must maintain an up-to-date listing of its physicians and their corresponding service codes.
12-01 to 12-06 Therapies A blank indicates "No" for services provided and anything else indicates "Yes".
12-09 Pre-Admission Work-Up
This field indicates if a pre-admission work-up was done before admission––regardless of type or location. A blank field indicates none was done while an entry indicates that pre-admission work-up was done. This field is mandatory for case costing.
8.8 Information Systems
The various departmental requirements discussed in this Guide are the ‘building blocks’ for case costing, and information systems represent the ‘mortar’ holding case costing together. Case costing implementation is a team process, and Information Systems plays an important role in helping the organization implement the required information systems. It is important to ensure that the hospital's Information Systems Strategic Plan reflects the hospital's business plan to implement and use case costing. The Information Systems Department's priorities must be clear and compatible with the hospital's overall priorities. Because information systems are a factor in almost all aspects of case costing implementation, it is next to impossible to pull all significant information systems material from the various departments for presentation in this chapter. The reality is that information systems staff must be familiar with all aspects of case costing to provide the level of support needed. The MIS Standards 2006, Appendix 2 (Implementing the MIS Standards) provides a wealth of technical information with regard to selection and acquisition of information systems. In addition, Chapter 12 of this Guide provides further information on project organization and management. The approaches that hospitals have used to develop a case costing system can be categorized into four groups:
1. Single-Vendor Approach: This involves utilizing a single comprehensive solution for patient and financial information systems.
2. Mainframe-Based Approach: This involves utilizing a mainframe-based cost accounting system with data feeds from mainframe-based patient care and financial systems.
3. Multi-Vendor PC/Micro-Based Approach: There are several vendors who provide cost accounting systems adapted for PC or microcomputer platforms. There are similarly adapted patient care systems.
4. In-House Developed Systems Approach: Some hospitals have gone the route of designing their own cost accounting system based on a mini-computer. Patient-care and other financial systems are obtained from various vendors.
The approach that the hospital selects will depend on a number of factors, including the current design of the hospital’s information systems. In 2006, the MOHLTC decided to acquire and maintain a case costing solution that would be available to all Ontario hospitals.
OCCI Version 6.1 Page 69 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
8.9 Pharmacy/Drug Costs
Pharmacy and drug costs are distributed to patients through a combination of direct charge capture and distribution by formula. This approach to patient costing uses the Medication Profile (Pharmacy’s record of patient medication), not the Medication Administration Record (MAR) (Nursing’s record of actual medication administration). Although the MAR could provide an exact record for drug cost development, it is not a practical source document. The recommended approach produces useful costing based on orders, returns and standard cost distribution. It requires the following functionality in pharmacy information systems: that the automated medication profile system be merged with the inventory (cost) system to attach costs to the medication dispensed; and that there is another "field" in the medication profile system to allow the capture of an associated labour component based on dosage form.
Best Drug Cost Data The best drug cost distribution data are achieved with a computerized unit dose drug distribution system
Drug Costs Drugs can be considered under two broad categories for case costing purposes:
• Individually dispensed drugs, including PRN medication that is not kept as ward stock; and • Ward stock.
Hospitals that use a high proportion of ward stock will not be able to produce good drug cost data because of practical limitations. This occurs because distribution of ward stock costs requires the assumption that the daily ward stock drug cost for all patients on a nursing unit is the same in order to avoid onerous data capture. This assumption is acceptable where ward stock is a small portion of the patient's total drug cost (unit dose system) or where there is consistency in ward stock drug usage by patient (such as a short stay unit). Even automated information systems can be overloaded by too much detail. With thousands of drug/dosage forms, some OCCI hospitals found they had too much cost detail. They chose to group drugs for costing purposes, establishing average costs for groups of drugs. Options for setting drug costs in the system for case costing include:
• Individual Costs Only: Actual costs for each drug dosage form. • Combination of Individual and Grouping: Actual costs for high volume/cost drug dosage
forms; drug dosage forms with similar costs grouped and charged at an average cost for the group.
• Full Grouping: Drug dosage forms with similar costs grouped and charged at an average cost for the group.
Whatever method is used, it should produce representative drug costing. If drugs are grouped for costing, keep a record of the methodology for future reference when costs must be updated in the system. Also, put a routine mechanism in place to maintain the unit drug costs in the system (whether using individual costs or cost groups).
Individually Dispensed Drugs
Tracking the costs of individually dispensed drugs is relatively
OCCI Version 6.1 Page 70 of 105 Effective April 2008-March 2009 Updated August 2009
Costs of Individually Dispensed Drugs The Ontario Case Cost Project determined that hospitals should distribute costs of individually dispensed drugs based on actual drug costs and quantities dispensed for the patient.
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
straightforward, but does require the use of an automated Medication Profile. Hospital size does not affect this requirement. Since the automated information systems used in Pharmacies are able to apply unit costs to each drug dispensed (and credit specific returns), a patient's detailed drug cost can be produced at discharge. PRN (‘as needed’) medication orders for individually dispensed drugs are also entered into the Pharmacy information system. A PRN medication order presents a special challenge for costing since the patient may not want or need the PRN medication, or may continue to use it throughout his/her stay. Since PRN medication is typically low unit cost, the standard procedure is to enter the PRN medication order only once into the Pharmacy information system (unless it changes). To achieve a fair cost distribution with reasonable effort, the OCCI hospitals used the following approach for PRN medication orders:
• When dispensed PRN medication orders are entered, a hospital-developed estimate of patient usage is entered (the estimate could range from one day for a patient on a short-term unit to more than 30 days for a long-term care patient).
The overall cost impact of drug returns is considered to be small (typically 5% or less). Some pharmacy information systems have an auto-crediting feature that automatically credits drugs on discharge or death of the patient. This feature is helpful as long as the system does not credit drugs that cannot be reused. Ensure that one category of returns is being credited: • High cost reusable IV returns need be credited for costing purposes. The hospital must, of course, first
satisfy itself of the appropriateness of reusing a particular returned IV medication based on current practice standards (Canadian Society of Hospital Pharmacists Std. 6.5).
Ward Stock It is not practical to track ward stock on an individual case basis. The recommended approach is to use standard costs to provide an approximation. The first step is to establish an average ward stock cost per patient day for each Nursing unit. This average cost must be updated at least annually, although more a frequent cost adjustment, such as quarterly, is preferred. As an alternative to calculating and merging a drug cost with a patient day, the drug costs could become part of the direct operating costs of the Nursing unit and be distributed to the patients on the basis of patient-specific Nursing workload units. The record of drug cost details would then be captured with the secondary financial expense accounts for the nursing unit. Ward stock returns are unlikely to exceed $250 per occurrence or even per patient. However, if a Nursing unit does return a batch of reusable ward stock worth $250 or more, it should be credited against the Nursing unit ward stock drug cost for that period.
Drugs Administered Through Other Departments Some drugs are administered through departments other than Pharmacy. Traditionally, the costs of such drugs have remained with the Pharmacy and in the General Ledger as drug costs, even though Pharmacy has little to do with them. The following approaches for tracing the cost of drugs administered through other departments have been designed to ensure accurate case cost data:
• Non-medicated IV solution costs are distributed along with other material and supply costs incurred through the Nursing unit.
• Anesthetic agents and other drug items administered through the OR are tracked through the OR clinical record.
• Medical gas costs are tracked through the administering department.
OCCI Version 6.1 Page 71 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Depending on the capability of the financial information system, it should be possible for each functional centre to establish accounts for the drugs administered. This will allow drug costs to be tracked to the responsible functional centre. The next step is to select an approach to tracking patient-specific usage that will provide acceptably accurate case cost data. Potential approaches could range from distributing these drug costs along with other functional centre supply costs (e.g., for non-medicated IV solutions) to keeping detailed records and distributing costs based on consumption by patient.
Drug Costs for Inpatient and Outpatient Pharmacy Operations As with other functional centres, outpatient labour and supply (and drug) costs must be separated so that any cost distribution formulas distribute inpatient costs to inpatients and outpatient costs to outpatients.
Implications of Decentralized Drug Costs Some hospitals have already adopted a decentralized approach to tracking drug costs in an effort to improve responsibility and accountability for drug usage. The traditional (centralized) approach is to charge all drugs to Pharmacy. With the decentralized approach, drug costs are distributed to inpatient units based on drug usage by patients on the unit. If the hospital distributes drug costs in this manner, the financial system's features (and limitations) must be reviewed so that drug costs can be matched with the patient drug distribution data. Pharmacy Labour For costing purposes, pharmacy labour falls into four main categories:
• Drug Distribution Labour • Clinical Pharmacy Labour • Management and Operational Support Labour • In-House Manufacturing (IV Admixture and TPN Preparation)
Drug Distribution Labour The hospital should use the Pharmacy National Workload Measurement System (NWMS) to determine appropriate labour/workload units for each of the Pharmacy's labour categories. Remember to document how workload categories and unit values are defined for later verification, if needed. The accuracy of drug distribution workload measurement will depend to a great extent on the approaches used by the hospital to distribute drugs. Drug distribution by unit dose provides the most accurate workload, when workload is produced as a byproduct of Pharmacy processing using an automated medication profile. Drug distribution by ward stock does not facilitate data capture for labour costing. Typically, a hospital will use a combination of approaches, including ward stock for relatively inexpensive, general-purpose items. For most OCCI hospitals, ward stock does not represent a significant portion of drug distribution labour. Thus, the documented workload units associated with drug distribution from the automated medication profile could be used as relative values to distribute drug distribution labour cost to patients. If ward stock is a significant portion of the hospital's drug distribution labour, consider using the ward stock workload measurement capabilities incorporated in the Pharmacy NWMS. Distribution of drug distribution labour cost to patients requires the use of an automated medication profile with the ability to assign labour category attributes to each drug item in inventory. Drug distribution labour for a case would then be calculated as the product of the number of doses of each drug dispensed times the number of labour units established for the dispensing of one dose of that drug, summed for all drugs dispensed to the patient (Where a hospital is partially converted to a unit dose
OCCI Version 6.1 Page 72 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
system, two attributes for each dosage form would be needed, one for workload associated with unit dose drug distribution, and one for traditional drug distribution).
Clinical Pharmacy Labour As much as half of Pharmacy labour cost is clinical pharmacy activity. Clinical Pharmacy activity workload is not directly related to drug distribution labour––for example, the drugs required by patients in ICU may generate relatively few labour units for distribution while pharmacist clinical activity could be quite concentrated. Conversely, chemotherapy patients whose treatment plan has already been established receive high labour cost drugs with little concurrent clinical pharmacist activity. If the hospital's Clinical Pharmacy is a separate functional centre, use the Pharmacy NWMS so that clinical workload can be distributed more precisely to patients for case costing purposes. If Clinical Pharmacy activity represents a small proportion of the total Pharmacy workload, use drug distribution labour as the basis for distribution of clinical activity labour costs to cases. Hospitals using a clinical workload measurement system, should ensure that the workload units produced are compatible with distribution workload units. Ideally, total Pharmacy labour cost would be distributed to each patient based on the sum of the distribution and clinical workload units that the patient received.
Management and Operational Support Labour As in other functional centres, only patient-specific units can be used to distribute costs to patients. The denominator in the unit cost calculation formula is the total number of patient-specific units produced by the functional centre during the period. Costs for management and operational support, clinical labour, general supplies, and so on are all distributed to patients as direct costs in proportion to measured patient-specific unit producing labour.
In-House Manufacturing (IV Admixture and TPN Preparation) The MIS Standards (Section 3.3, Recording of Supplies Expenses) specify that where in-house manufacturing or compounding (such as sterile products from the Pharmacy, including TPN and IV additives) is done, the costs of manufacturing should be transformed into supply costs through the use of inventory accounting. Ideally, such manufacturing would be done in a separate functional centre with the manufactured products then "sold" to Pharmacy inventory. In this way, the labour, drug and material costs are converted to a drug cost in the Pharmacy inventory and charges are distributed to patients through the normal systems.
OCCI Version 6.1 Page 73 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 9: Ambulatory, Chronic Care and Mental Health Standards The OCCI case costing methodology was originally developed to cost acute inpatients. Minor modifications to the methodology have made it possible to cost day surgery cases. Further development of the standards was required with the addition of ambulatory mental health and chronic care case costing. It is crucial to keep in mind that most aspects of the methodology apply to all cases. Utilization is captured on a patient-specific basis, standardized financial information is tracked using the MIS Standards, and costs are distributed to patients based on the total number of services/intermediate products received from each functional centre. The most difficult issue when adapting the standards to ambulatory mental health and chronic care is to define the encounter. The acute inpatient encounter is defined as the time between admission and discharge dates. However, an ambulatory care encounter can be only ten minutes long while a mental health or chronic care encounter can be more than one year long. The challenge has been to maintain the standards while recognizing the differences in the encounter for different populations. Most of the differences in the methodology for mental health, chronic and ambulatory care are due to the nature of the visit or encounter. This chapter summarizes the costing standards and issues specific to ambulatory care, mental health and chronic care. All of the general and departmental standards presented in this Guide apply to the costing of these patient groups. Details of the costing standards are found in Chapters 3 to 6 and Chapter 8. Section 3.3 includes a thorough explanation of the patient descriptive data required for ambulatory care, mental health and chronic care costing.
9.1 Ambulatory Care
The general and departmental standards apply to ambulatory care cases. Minor modifications to the acute inpatient standards have been made to accommodate ambulatory care costing.
Assigning Costs to the Encounter The NACRS has recording guidelines that define when an ambulatory care data set is to be collected (refer to the CIHI Ambulatory Care Minimum Data Set). The current guidelines specify that one data set is recorded when services are provided by one or more staff within the same functional centre. Where services are provided by staff from different functional centres, a separate data set must be submitted for each functional centre. From a case costing perspective, the key issue is to ensure that the appropriate costs are distributed to the appropriate encounters. The hospital must generate the required data sets for each patient visit and then track the costs to each functional centre that provided the services/intermediate products. For the purposes of costing, an ambulatory care encounter (An encounter includes visits, diagnostic procedures, attendance days and telephone contacts—see Methodology for Costing Ambulatory Care—Version 2 for details) will be recognized in each of the following situations (based on the CIHI/MIS definitions):
1. Services provided to a registered hospital outpatient by an ambulatory care functional centre (Emergency, Day/Night Care and Clinics) as defined by the Ontario Healthcare Reporting Standards. • Only one visit is recorded for each patient per ambulatory care functional centre in a given
24-hour period. A second visit is only reported if: the visit is for a different medical problem
OCCI Version 6.1 Page 74 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
in the same 24-hour period, the patient is treated by a different physician or service in the same 24-hour period, or care is provided by a different shift of care providers.
• If a registered outpatient receives services from more than one OHRS ambulatory care functional centre, each set of services from an individual functional centre will be recognized as a separate encounter.
• Patient care services (e.g., consultations, therapy, etc.) provided through phone contacts to, or on behalf of, a registered outpatient will be recognized as an ambulatory care encounter. The ‘Mode of Visit’ field must be used to indicate that the encounter was a phone contact.
2. Services provided to a registered inpatient by an Allied Health (Therapeutic) functional centre. Outpatient attendance-days at the following centres will be recognized as encounters for costing: • Physiotherapy, Occupational Therapy, Speech/Language Pathology, Audiology, Psychology,
Social Work, Clinical Nutrition, Recreation Therapy, Child Life • Radiation Oncology • Therapeutic Services of Respiratory Therapy (e.g., hyperbaric chamber)
Additional services, provided to a patient in conjunction with an ambulatory care encounter, will be captured and costed as part of that ambulatory care encounter. In most cases, these services would be ordered through the ambulatory care functional centre: • Laboratory • Diagnostic Imaging • Other Diagnostic Laboratories (EEG, Echocardiography, etc.) • Pharmacy
9.2 Mental Health and Chronic Care
Assigning Costs to the Encounter A mental health or chronic care encounter is identified by the patient’s admission and discharge dates. Due to the length of stay of a mental health or chronic care visit (sometimes greater than one year), a mental health or chronic care encounter can be divided into a set of sub-encounters for the purposes of costing. The sub-encounter is defined as the time period between any two consecutive assessment periods, as illustrated in the next section. Each sub-encounter is identified by a mental health or chronic care MDS assessment period (usually 90 days) which is defined as the time from the beginning day of an MDS assessment period to the day before the next assessment period. The beginning of a new assessment period triggers the beginning of a new sub-encounter except when a significant change in status occurs. In this case, the new sub-encounter is triggered on the day the change in status has been identified. All services and products delivered to each patient are to be tracked for each assessment period. Figure 9-1 shows an example of the MDS assessment process:
OCCI Version 6.1 Page 75 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Figure 9 - 1
Conceptual View of MDS Assessment Process
Upon admission, the patient is assigned a registration number by the A/D/T system, which identifies the encounter. For the purpose of case costing, each encounter is then divided into a number of sub-encounters. Assessment reference date is the last day of the MDS observation period referring to the specific end-point in the MDS process and is captured as part of the MDS. This date triggers the start of a new assessment period, unless there is a significant change in status. Date of entry refers to the date upon which the patient was admitted into the facility and is captured as part of the MDS. Date signed as complete refers to the date upon which the RN Coordinator certifies that the assessment is complete and is captured as part of the MDS. Significant change in status refers to the date upon which a significant change in the patient’s condition is recognized. This is not captured as part of the MDS. The following example, illustrated in Figure 9-1, clarifies the standards for case costing.
• Sub-Encounter # 1 (Assessment Period #1)
The costing standards require that all services and products delivered to the patient from the day of admission to the last day (day 90) before the next MDS assessment period will be tracked to the patient as part of assessment period #1. Therefore, the beginning date of the first assessment period is day 0, the day of admission. All services and products received between the admission date and the initial assessment are associated with the first assessment period. It is critical to attach these first few days of stay to the first assessment period since a significant amount of care, and therefore costs, will be incurred in the first few days of stay. • Sub-Encounter #2 (Assessment Period #2)
The second assessment period, sub-encounter #2, begins on the day following the assessment reference date, usually day 91. All services and products delivered to the patient from the 91st day of stay to the last day (day 180) before the third MDS assessment will be tracked to the patient as part of assessment period #2. The care provided to patients (the products and services received) will reflect results of the quarterly assessment. • Other Sub-Encounters (Assessment Period #3, #4)
OCCI Version 6.1 Page 76 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Similar to sub-encounter #2, the third assessment period, sub-encounter #3, begins on the day following the assessment reference date, around day 181. All services and products delivered to the patient from the 181st day of stay to the last day (day 189 in this example) before assessment period # 4 will be tracked to the patient as part of assessment period #3. However, ten days into the third assessment period, the patient in our example has a significant change in status. Due to the change in the patient’s condition, attending care providers observe the patient as the patient stabilizes and complete a full assessment. The period then continues for 90 days, after which a quarterly assessment will be taken similar to previous quarterly assessments. In this case, encounter #4 is triggered on the day the significant change takes place (day 190) as opposed to when the assessment is completed, which can be several days after the change. All services and products delivered to the patient from the 190th day of stay to the last day (day 280) before assessment period #5 will be tracked to the patient as part of assessment period #4.
Tracking Costs for Readmissions
There may be occasions where a patient is discharged from a mental health or chronic care facility and is expected to be readmitted to the facility. For example, the patient may be temporarily admitted to another health care facility to receive a surgical or diagnostic procedure or the patient may be temporarily discharged home. As long as there is no significant change in the patient’s status after readmission, the same MDS assessment covers that sub-encounter until the next assessment. It is important that the costing of the encounter continue even while the patient is temporarily absent from the facility. If the entire assessment period is 90 days long and a patient was absent for four of those days, the costing period should represent the entire 90 days and all costs accumulated during the period. In the case where the patient’s status has changed, a new MDS assessment would initiate a new assessment period.
Using this approach to identifying chronic care sub-encounters implies:
• There must be, at a minimum, four MDS assessments (one full and three quarterly) within any given 12-month period.
• The maximum number of days any given assessment period can have is 90 days.
• Each day of stay must be associated with an assessment period.
For Rehabilitation patients: Service Interruption Status of 1 in the Discharge assessment is indicated according to the standards set by CIHI. When the Service Interruption of 1 is indicated the patient has been discharged and admitted to another facility and may be readmitted back to the rehab facility to continue with rehab treatment.
Hospital Data Submission Requirements Currently, hospitals internally are able to track utilization based on the register account number. For mental health, chronic care and rehabilitation case costing, the main challenge will be to track the utilization of products and services to each sub-encounter. Hospitals are required to develop mechanisms to uniquely identify each assessment period/sub-encounter. When reporting case costs to the OCCI, each sub-encounter is submitted as part of the cost submission and is identified through each patient’s:
1. Master Number
OCCI Version 6.1 Page 77 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
2. Chart number 3. Admission date 4. Registration number (as assigned by the ADT)
a) for Chronic Care – the Unique Registration Identifier is used b) for Mental Health – the Case Record number is used
5. Discharge date (if applicable) For Rehabilitation: The admission/discharge information is also submitted as part of the cost submission and is identified through each patient’s:
1. Master Number 2. Chart number 3. Admission date
These data elements are to be submitted in the OCCI case cost data submission (see Appendix L).
Nursing Workload Measurement Systems For rehabilitation or chronic care cases, it is acceptable for nursing workload to be captured on a weekly rather than on a daily basis. This is largely because the care provided to chronic care and rehab patients is relatively static in the short term. However, this is not always the case. The nature of the care provided to a given patient by some Nursing units might fluctuate on a daily basis, and therefore necessitate daily workload capture. The hospital will need to determine whether specific Nursing units require daily or weekly workload measurement and collection. The other alternative to capture Chronic Care and Rehabilitation Nursing Workload would be by proxy using the RUG or RPG as indicated in section 5.3.5 (see appendix Q)
Patient-Specific Supplies Generally, there will be few high cost patient-specific supplies (greater than $250) that will be costed directly to mental health, chronic care or rehab patients. The hospital may find that some supply items with a low unit cost are used in high volumes by certain patients and thereby account for a significant proportion of the total supply costs. For example, chronic care patients frequently use incontinence products, which are a large portion of the Nursing unit’s supply costs. These supply costs are usually spread to all patients based on workload, rather than being distributed directly to the patients who use them. The hospital can identify these high volume items and distribute the costs to those patients who use these supply items. Alternatively, the hospital may decide to lower the overall threshold for distributing patient-specific supplies.
OCCI Version 6.1 Page 78 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 10: Costing in a Program Management Hospital Many hospitals have been moving towards program management as an approach to providing patient care services. Under the program management model, traditional hospital functional centres are amalgamated to form a program. Each program produces a variety of traditional functional centre intermediate products such as nursing services, allied health services, simple laboratory tests, diagnostic imaging exams, and dispensed drug orders. The services delivered to patients (i.e., intermediate products) are essentially the same; however, production of these services has been shifted from the traditional functional centres to programs. The activities and organization of personnel working in a program management environment are typically different from those in the traditional hospital setting. Many program management hospitals employ multi-skilled workers. Multi-skilled workers are patient care workers who are cross-trained to provide a variety of services for the patient (e.g., lab tests, nursing services, etc.). Support staff may also be involved in providing patient care services. In addition to using multi-skilled workers, many traditional department staff are also ‘deployed’ to the individual programs or functional centres. An example is a social worker stationed and working within a chronic care program when no social work department exists in the hospital. The OCCI case costing methodology is derived from the MIS Standards, which are based on the assumption that hospitals are organized and managed using a traditional departmental approach. This approach presents challenges for case costing implementation in a program management hospital since it involves calculating case costs using the current OHRS functional centre perspective. In this chapter, the steps are discussed on how costs of products produced in programs are calculated by applying the current case cost methodology. An alternative costing methodology is also presented that is superior to the current methodology, but which is not practical to implement at the present time.
10.1 Gathering Data
Like departmentally based hospitals, program management hospitals require patient descriptive, financial and workload data for case costing. The collection and reporting of financial and workload data are the areas that need special attention. The collection and organization of financial data is complicated by the fact that all program expenses must be mapped and charged to an OHRS functional centre. The difficulty occurs in separating program expenses, such as supplies, which may be used by all disciplines. This often results in the majority of the costs being assigned to the Nursing functional centre, although they are shared by all disciplines. Program labour costs are distributed back to the functional centres associated with the discipline of the program’s employees. For example, the salary and benefits of a social worker working in the chronic care program are recorded in the Social Work functional centre. Program support and administration costs should be assigned as a direct cost to the functional centres they support, based on an estimate of the amount of time support and administrative staff spend managing the activities of each discipline. If there are many disciplines working in the program, it may be difficult to establish an estimate and immaterial to distribute these costs to each functional centre. As a result, some hospitals distribute all of the program support and administration costs to the Nursing functional centre. Some larger hospitals may have created a Program Management Administration (7120600) functional centre for recording the costs of administrative personnel responsible for inpatient programs. The costs in this functional centre should be assigned as a direct cost to the patient care functional centres it supports
OCCI Version 6.1 Page 79 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
based on the proportion of functional centre workload, functional centre direct costs, or time staff spend providing services to patient care functional centres. Workload data is collected in the same manner as in traditionally organized hospitals. That is, workload is collected by each discipline on a patient-specific basis using workload measurement systems that are MIS compliant. Because there are a variety of health disciplines working in a program, there may be more than one workload measurement tool being used. The workload collected must be assigned to the functional centre to which the discipline relates. If the hospital has multi-skilled workers, ensure that their workload and salaries are assigned to the same functional centre(s). Note that if any new products are created in the functional centres, the RVUs must be calibrated against the other products in the functional centre.
Gathering Data A key point to remember is that labour expenses and related workload must be recorded in the same functional centre.
10.2 Allocating Indirect Costs
The allocation of indirect costs is performed at the functional centre level using the methodology described in Chapter 4. Hospitals are required to use SEAM and the standard allocation bases to allocate the costs of TCCs to patient care functional centres. Cost allocation requires the collection of allocation statistics for each functional centre. Programs must map their allocation statistics back to the corresponding functional centres. Hospitals already gather some of these statistics on a functional centre basis since it is required for OHRS reporting. For instance, departmental total costs and worked hours are already tracked to functional centres. Other statistics are either not available or are not practical to estimate. For instance, department net square metres, used to allocate Plant Operation costs, are difficult to estimate for the functional centres that comprise the program. The approach hospitals have taken is to map these statistics to the Nursing functional centres which correspond to the program. The effect of this practice is that the Nursing functional centres will have a greater portion of the overhead and relatively high indirect costs. The other functional centres that provide services to the program will have understated indirect costs if all staff members are deployed to the program. If a separate department also exists for each discipline working within the program, then indirect costs for these functional centres will be similar to those in a departmentally organized hospital.
10.3 Calculating and Distributing Product Costs
At this point, all program costs are assigned to the OHRS functional centres. Intermediate products and workload produced within the program have also been assigned back to functional centres. In addition, indirect costs have been allocated to functional centres based on the allocation statistics collected for each of the functional centres. The calculation and distribution of case costs are made simple now that all expenses and statistics are assigned back to departments. The same case costing methodology described in Chapters 5 and 6 to calculate and distribute costs to patients is followed.
OCCI Version 6.1 Page 80 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
10.4 Product Line Costing
The difficulties of implementing a departmentally based case costing methodology in a program environment have underscored the need for a costing methodology which is applicable to a variety of organizational and management approaches. The product line costing methodology provides an alternative to the departmentally focused case costing methodology by approaching case costing from the program perspective. Product line costing differs from the current methodology in that workload and expense data are collected at the program level. One of the biggest challenges is in reorganizing the way the workload is collected. Capturing workload by program requires the identification of all products within a program, regardless of discipline, and development of a new RVU system that calibrates all products against each other. Workload collection would be simplified with the use of a new multidisciplinary workload measurement tool. Indirect cost allocation is less complicated and more precise in product line costing. Allocation statistics are collected for programs rather than functional centres and indirect costs are allocated to programs using the standard allocation bases. The last step is to calculate product costs. The calculations are performed on a program basis using total program costs and total program RVUs. This approach results in products that reflect a blended cost. For example, physiotherapist salaries along with all other expenses related to the program would be used to calculate the cost of a physiotherapy product within a given program. In contrast, the current functional centre approach results in a product cost that more specifically reflects the resources used to produce a given set of products. Following the same example, the cost of a physiotherapist product is calculated using only physiotherapy salaries and physiotherapy workload. Hospitals employing product line costing must still report costs to the OCCI by functional centre so that patient costs from different facilities can be compared to each other. Therefore, a hospital choosing to cost intermediate products of a program using a multidisciplinary workload measurement tool will be required to identify which products relate to each discipline (or traditional functional centre). These product costs will be mapped to functional centres to permit comparison with the costs of similar products produced in traditionally organized hospitals. Note that products may be grouped by program for internal reporting. It is not currently feasible to implement product line costing because hospitals are still required to report financial and statistical information on a departmental basis to meet OHRS reporting requirements. For product line costing to be a viable option, a standardized financial reporting system that accommodates both the traditional departmental and program management activities is required. The reporting system needs to provide the necessary structure of accounts and guidelines to ensure all expenses are accounted for in a comparable manner for all hospitals. A set of secondary accounts for labour expenses for each discipline working in the program would also be required. The product line costing approach would also make it difficult for hospitals to report departmental workload statistics to the Ministry of Health and Long-Term Care via OHRS reporting. Hospitals using a multidisciplinary workload measurement tool would still need to report workload activity on a discipline-specific basis to conform to OHRS requirements.
OCCI Version 6.1 Page 81 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 11: Implementing Case Costing Case costing involves implementing MIS Functional Centre Full Cost Reporting and Service Recipient Reporting with a specific target of developing case cost data for management and planning purposes. Appendix 2 (Implementing the MIS Standards) of MIS Standards 2006 should be reviewed prior to the case costing implementation. The information included in this chapter is intended to highlight the implementation issues that were found to be most important by the OCCI hospitals. The case costing implementation project will affect most hospital departments. Although case costing has many benefits for hospital management, the immediate impact on middle management and operating staff will be additional work, both for the implementation and for ongoing data collection. Senior management, and the Chief Executive Officer in particular, must be active supporters and promoters of the case costing initiative. The hospital must see that the CEO is committed to the project through involvement in the implementation effort, assignment of resources, commitment of necessary investments in information systems, and active participation in identifying executive information needs.
Implementation of MIS Standards
Appendix 2 of the MIS Standards 2006, provides detailed materials that can help plan and manage the implementation.
A Steering Committee for the project will help to facilitate acceptance of the case costing project as well as help the Project Manager stay on track and provide a forum for timely problem resolution. Since many case costing issues relate to information systems, many hospitals have added case costing to their Information Systems Steering Committee mandate. A Project Manager should be identified. This key position will require virtually full-time commitment for the duration of the implementation. The Project Manager functions as a general contractor with responsibility for the day-to-day management of the project. The general responsibilities of the Project Manager include the following:
• Communication of project mandate • Project organization • Project plan and planning process • Ensure appropriate participation by all required users • Perform audit and change control • Communicate project progress • Ensure that project charges are appropriate
The OCCI has developed four Milestone Reviews to assist hospitals with the implementation process and data quality verification. Appendix O describes the Milestones Reviews in greater detail.
11.1 Challenges of Implementation
There are many issues that are specific to the brand of information systems being used, but there were many general issues. The following are the main technical and organizational issues:
Organizational Challenges • New technology Þ new way of doing business Þ focus on "learning" • Buy-in by front-line users regarding technical and procedural changes needed in feeder systems
to meet the needs of the corporate system • Developing hospital confidence in cost data • Systems training • Coordinating the collection and entry of data where interfaces do not exist so that information is
OCCI Version 6.1 Page 82 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
entered on a timely and accurate basis (Nursing workload and various episodic area data)
Data Quality and Consistency Challenges • Conversion/Mapping to OHRS Chart of Accounts • Inconsistencies in data collection by feeder areas can make it difficult to match key data elements
from feeder systems • Ensuring the crediting of high cost drug returns • Assigning RVUs and grouping products (where these are key features of the system) • Collecting statistical data needed for cost allocation • Obtaining patient-specific laboratory workload data • Determining the most feasible method to capture nursing workload by patient without involving
significant human resources/professional staff • Identifying all patient-specific items that should be tracked, including ongoing identification of
new supplies that meet the criteria (or existing supplies whose value has increased over the threshold)
• Ongoing maintenance of the systems to ensure workload measurement systems, RVUs, statistical data and patient-specific items are kept up to date
Information Systems Challenges
• Selecting an appropriate Cost Accounting System • Vendor management—modification requirements, time frames, vendor/hospital communications,
costs • Designing an interface to merge encounter data from disparate systems in a multi-vendor environment • Interfacing clinical systems with the Cost Accounting System. In many cases the dictionaries and
functionality of the clinical system are not consistent with the needs of case costing. Sometimes rebuilding/major revamping of dictionaries is required or creative methods to work around the situation must be developed
• Ensuring the system tracks patient-specific workload from the various feeder systems. • The accurate documentation of the patient's movement throughout the hospital is essential. This will
yield accurate Patient Hours information that may be used in allocating nursing costs • Developing uploading capabilities for workload that is maintained on a peripheral PC program. • Developing a system/program to track patient-specific drug costs and pharmacy workload • Automating Nursing workload reporting to get patient-specific data • Developing reports to support the accuracy of the data being collected (such as length of stay report
for Nursing workload collection) • Archiving data to enable later verification/investigation of data and utilization
11.2 Implementation Time-Frames
A reasonable time frame depends significantly on how much of the required system functionality already exists in the hospital. If mature financial systems and the majority of clinical systems are already in place, a time frame of 12 to 18 months would be reasonable to get a working group and assign a dedicated team to focus on each of the following areas:
• Implementing the Cost Accounting System • Developing interfaces into Cost Accounting, including workload information • Developing financial and statistical data to ensure compliance with MIS Standards and OHRS
requirements • Developing an allocation routine for TCC costs and reviewing the suitability of the standard
allocation bases
OCCI Version 6.1 Page 83 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
If any of the major clinical (feeder) systems are missing, or requires overhaul, then it could take up to three years to achieve a solid implementation.
11.3 Implementation Sequence
The sequence of implementation for the several sub-systems that enable case costing can vary significantly depending on the starting point, the condition of already installed systems and the priorities for implementation. One observation of the Case Cost Project Managers is that knowledge of the requirements of case costing and the costing module is important when implementing the clinical feeder systems. In fact, several of the project hospitals suggested implementing the costing sub-system quite early in the process to facilitate the implementation of the feeder systems. Additional discussion of implementation sequence issues can be found in Appendix 2 of the MIS Standards 2006.
11.4 Education/Promotion/Orientation
A carefully designed internal promotion plan is an essential ingredient for ensuring case cost project success. It is critical to ‘sell’ case costing to all stakeholders so that they will invest the extra effort both in the short and long term to produce the additional data needed. In planning the promotion, address the following:
• Who are the stakeholders in case costing?
- Employees/Unions - Patients - Board - Ministry of Health and Long-Term Care - Management - Other - Medical Staff
• What are the stakeholders’ concerns?
- Quality of Care - Loss of power/status - Potential job loss - Change in work style/process - Potential for loss of income - Other
• What message should stakeholders receive?
- Potential benefits of case costing (hospital, health care system, individual) - DO control expectations - DO address contentious issues - DO focus on improving existing services versus reducing services - Other
• How will the message be delivered?
OCCI Version 6.1 Page 84 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
- Workshops - Newsletters - Education/orientation sessions - Other
• Who will carry out the promotion and when?
- Hospital Management and Staff - Medical Staff - External Resources - Other
11.5 Data Flow Models and Methodologies
As case costing is planned, make sure that the various aspects of the plan will come together to produce good case cost data. The Data Flow Models and Methodology Descriptions for the various case costing sub-systems will support the technical analysis of the approach devised.
Data Flow Model The Data Flow Model provides an overview of the input, processing, storage and output of data. Be concerned for Case Cost Data ONLY. Thus the cost, workload and patient descriptive data elements (and those that contribute to their creation) as described in earlier chapters and the Appendices are the focus. With a model, it is easier to test whether required source data will be available:
• Where and when it is needed; • In the right form (paper, electronic, verbal) so that required processing can be done; and • That correct output in the right form (paper, electronic, verbal) is produced.
There are no style standards (and no style points - this is a great reference for the hospital). Use a sketch or point form prose description. However, the Data Flow Model should be done in sufficient detail to show that cost and/or workload data are linked to specific patients as appropriate, and that an audit trail will exist as needed to verify cost data in later stages of the project and on an ongoing basis.
WMS Methodology The Workload Measurement System (WMS) Methodology description shows how to approach the measurement and capture of patient-specific workload. Even though the National WMS is used for an area, document how it was fine-tuned for implementation. Some possible reasons for using different approaches include:
• Features or limitations of the departmental information system; • Features or limitations of the case cost system; • Practical adaptation of the NWMS to patient-specific costing requirements; and • Practical adaptation of NWMS Unit Values to specific operating methods and differences in
clinical technology. It is important to document the methodology used for two reasons:
1. To ensure that the methodology used will generate acceptable patient-specific costs; 2. To identify as early as possible any differences in approach that could impact the reliability or
validity of cost data and its comparability with other hospitals' case costs. The written description of the methodology should provide a point-form description of:
OCCI Version 6.1 Page 85 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Rationale Why was this approach chosen?
What other approaches were considered and rejected?
Comparison Data How do the workload units differ on a procedure by procedure basis from the NWMS?
Provide a list of groups, procedures within groups, and relative value units (RVUs).
RVU Development Describe a one-time analysis or study that was completed to establish relative values or other factors.
If grouped, describe how procedures were assigned to their respective groups.
State of Implementation Has this methodology been implemented?
If implemented, how long has it been in use?
What follow-up study has been done to validate the approach?
OCCI Version 6.1 Page 86 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 12: Evaluating Case Costing The primary objective of this is to evaluate how a department's present information and data collection and reporting systems conform to the target environment. The target environment represents the collection and reporting of data in accordance with the standards established by the MIS Standards and the OCCI. The goals of this analysis are to:
• Define how the information/data is currently collected and reported; • Identify the specific differences between the current environment (current reality) and the target
environment (preferred future) in terms of missing or inconsistent data; • Assess the reliability and validity of current information; • Identify organizational or procedural constraints to be considered when planning the migration
from the current to the target environments; • Identify information systems constraints or enhancements to be considered when planning the
migration from the current to the target environments; and • Develop a task list.
The output from this evaluation analysis is not an action plan. It is a review and assessment of the current environment relative to the target environment. Further analysis of paper flow processes, information systems applications, data structure and files, technology, etc., may be identified as specific tasks to be undertaken. The outputs from this analysis are used to develop detailed action plans.
Target Environment The target environment is fully implemented case costing consistent with all applicable standards and guidelines.
12.1 The Approach to Evaluation
The evaluation analysis is conducted together with the Costing Manager, Department Managers, Information Systems staff and other key staff as necessary. The approach is structured to address each of the major data and information components. The data are categorized into the following major groups:
• Functional Centres • Patient Identification for Linkage • Workload Units • General and Patient-Specific Supplies • Labour Hours
The Project team begins with a high-level review of the department's functional centre framework and data relationships. This high-level review represents a "snap-shot" of the current environment in terms of the functional centre structure and the collection of data and is not influenced by current information systems and procedures. The purpose of this starting point is to identify early in the project the relative magnitude of the effort required to collect and report this data needed for case costing. Further analysis of each of the major data groups will isolate specific issues and concerns within each functional centre. Using the results of this review as a guide, the project team will be able to prioritize attention to specific areas of concern and deficiency.
OCCI Version 6.1 Page 87 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
12.2 MIS Functional Centre Framework
In this section, the current organization of cost centres in the department is examined for consistency with the Ontario Healthcare Reporting Standards (OHRS). First, list the department's functional centres in a copy of Table P.1 (Appendix P). Refer to the OHRS for the functional centre codes for functional centres in the department. Use the questions below to help assess the functional centre organization.
Functional Centre Framework Review Answer "Yes" or "No" to each of the following high-level review questions:
1. Does each departmental functional centre currently exist? Are there any others? If so, double-check that the MIS and OHRS definitions are understood. If there are still extras, add them to the list of functional centres in table P.1.
Functional Centre Framework The functional centre framework must conform to the OHRS and operate (budgets, workload reporting, etc.) at the level of the lowest functional unit that exists within the department.
For each existing functional centre: (note that for each existing functional centre within the department, questions 2 through 14 should ultimately be answered with a "Yes")
2. Is the functional centre identified as a separate operating unit within the department (has a unique cost centre code been assigned)?
3. Is the patient's Chart Number (or Health Record Number) collected when an examination or procedure is conducted?
4. Is a unique encounter number (account or register number) assigned for each patient encounter for examination or procedure?
5. Is the patient's date of service collected?
6. Is the patient's specific procedure or examination collected?
7. Are workload units collected?
8. Are workload units collected on a patient-specific basis?
9. Are general supply costs charged to the using functional centre?
10. Are supply items and "supply assemblies" greater than $250 collected on a patient-specific basis?
11. Are the actual labour hours (both worked and benefit) of unit-producing personnel regularly collected within the functional centre where staff are working?
12. Are the actual labour hours (both worked and benefit) of management and operational support personnel regularly collected within the functional centre where they work?
13. Are all physician fee-for-service costs collected on a patient-specific basis or procedure basis?
14. Are the actual labour hours (both worked and benefit) of medical staff on salary collected within
OCCI Version 6.1 Page 88 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
the functional centre where they work?
12.3 Patient Identification for Linkage
Use the form in Appendix P.2 to document the answers to the following questions about patient identification.
1. Are the functional centres collecting the following: a) Patient Chart or Health Record Number? b) Patient Register or Account Number? c) Date examination was performed (optional)? d) Name or code of specific exam? e) What constraining factors limit the collection of patient specific procedures/exams in each
functional centre? f) What changes are required to requisitions and reporting forms/documents?
2. Do the functional centres already report the specific procedures or examinations on a patient-specific basis to the accounting office? Is this procedure: a) Manual b) Automated, or c) Combination of both?
Target: Patient-Specific Data For each procedure or examination completed, the department must collect the patient chart number, register/encounter number, service date, and the specific procedure code (optional) at the lowest functional centre level within the department.
3. Are the department's Information Systems: a) Automated? b) Integrated with the hospital's Central Patient
Index and Ad-mission System? 4. If there is no automated Departmental
Information System, does the department have access to the hospital's Main Central Patient Index and Admission / Discharge / Transfer System?
12.4 Workload Measurement
In this section, establish the case cost readiness of the workload measurement systems. Remember that workload measurement is one of the key factors in distributing costs to patients. For each existing functional centre in the department, use Table P.3 (Appendix P) to identify a "Yes" or "No" response to each of the following review questions. Record answers to (1), (2), and (10) for each functional centre.
1. Is the NWMS implemented in each functional centre? a) What, if any, changes have been made to the system (unit values modified, patient-specific
workload redefined, etc.)? b) For those functional centres where an NWMS has not been implemented, what are the
constraining factors, if any, to implement workload measurement? c) What actions, if any, must be completed
before workload measurement can be implemented in these functional centres?
2. Where the NWMS is not used, is another system used to measure workload in the functional centre?
Target: Patient-Specific Workload Evaluating The Case Costing Ability Departments must collect the total and patient-specific workload units at the level of the lowest functional centre that exists within the department.
a) If another system is used, how have the
OCCI Version 6.1 Page 89 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
relative values been established?
Workload Measurement Systems typically organize the workload categories into major groups. For example, the Diagnostic Imaging NWMS uses the ‘technical function’ and ‘technical support function’ categories. Table P.3 is set up to accommodate up to three workload unit categories with the following headings. There should be answer for each functional centre using the analogous workload unit categories (i.e., replace categories in bold with the categories that are used). 3. Can the WMS identify and collect patient ‘technical function’ workload units? 4. Can the WMS identify and collect patient ‘technical support function’ workload units? 5. Can the WMS identify and collect other workload units? 6. Can the WMS readily produce the total inpatient workload units for each functional centre? 7. Can the WMS readily produce the total outpatient workload units for each functional centre? 8. Can the WMS readily produce the total referred-out workload units for each functional centre? 9. Can the WMS readily produce the total referred-in workload units for each functional centre? 10. Can the WMS readily produce patient-specific workload units for each functional centre?
a) What are the constraining factors, if any, for collecting patient-specific workload in each of the functional centres?
b) Are there any actions that must be completed for this collection to happen? 11. Is there a procedure/mechanism established to ensure products and workload units are accurately
tracked to the patient? a) What are these mechanisms?
12. Are productivity ratios established and monitored for each functional centre?
13. Is the internal collection of workload data: a) Manual? b) Automated?
14. How are workload units transferred to the hospital's Statistical Ledger: a) On manual data collection forms? b) Departmental workload measurement system is interfaced with General Ledger (either through
diskettes, batch, or on-line)? c) Are other feeder systems (e.g., Order Entry/Results Reporting System, Encounter Tracking
System, etc.) utilized to report the necessary information?
12.5 General and Patient-Specific Supply Costs
In this section, use the high-level review (Table P.1) and the answers to the following questions to provide further insight into the current capabilities for collecting and reporting general and patient-specific supplies at the functional centre level. Record the answers for each functional centre.
1. Are all supply items currently costed/charged back to the level of the lowest functional centre that exists within the department?
Target: Supplies Costs Departments must collect and report supply items or "supply assemblies" with a cost greater than $250 on a patient-specific basis, as well as total supply costs for each functional centre within the department.
a) If supply items are not costed/charged back to the lowest functional level, what are the constraining factors for costing/charging these items to the lowest level?
b) What limitations, if any, of the hospital's central Materials Management System must be overcome?
OCCI Version 6.1 Page 90 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
c) What action must be taken for supplies to be costed/charged back to the lowest level? d) What changes must be taken to requisitions and reporting forms/documents?
2. Are high-cost supply items and supply assemblies over $250 tracked on a patient-specific basis within each functional centre? a) If not, is it possible to identify patient-specific supplies and supply assemblies over $250 for each
functional centre? b) What are the constraining factors for identifying these high cost items? c) What limitations, if any, of the hospital's central Materials Management System must be
overcome? d) What actions must be taken for supplies to be collected and reported as patient-specific supplies
within each functional centre? e) What changes must be made to requisitions and reporting forms/documents?
12.6 Labour Hours
For each functional centre existing in the department, use Table P.4 (Appendix P) to identify a "Yes" or "No" response to each of the following review questions. Note that (2a), (2b), (2c), (2d), (3a), (3b), (3c) and (3d) are open-ended questions.
1. Are the department's staff currently identified as belonging to the following occupational groups within each functional centre?
Target: Labour Hours Departments must collect and report actual labour hours (worked and benefit) at the lowest functional centre that exists within the department.
• Unit Producing • Management and Operational Support • Medical Personnel
2. Are each employee's actual labour hours (worked and benefit) tracked to account for time spent within each functional centre?
a) If not, what factors are constraining the hospital from tracking actual hours in each functional centre?
b) What limitations, if any, of the hospital's central Payroll System must be overcome? c) What actions must be taken for labour hours to be tracked across each of the functional centres? d) What changes must be made to requisitions and reporting forms/documents?
3. Are unit-producing labour hours and management and operational support labour hours currently distinguished and recorded appropriately in the Secondary Chart of Accounts?
a) If not, what are the constraining factors, if any, from distinguishing unit- producing and management and operational support labour hours in each functional centre?
b) What limitations, if any, of the hospital's central Payroll System must be overcome? c) What actions must be taken for unit producing and management and operational support labour
hours to be tracked across each of the functional centres? d) What changes must be made to requisitions and reporting forms/documents?
4. Is the internal collection of labour hour data:
a) Manual? b) Automated?
5. How are labour hours transferred to the hospital's Payroll System:
OCCI Version 6.1 Page 91 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
a) On manual data collection forms? b) Departmental labour tracking system is interfaced with Payroll System Ledger (either through
diskettes, batch, or on-line)? c) Data entry/input is done in the department?
6. Does the Payroll System serve as a feeder system to the hospital's General Ledger system?
12.7 Patient Hours Does the hospital capture A/D/T data electronically for all OCCI mandated functional centres? Is there an audit to the compare Patient Hours with length of stay?
12.8 Other Statistics Case costing relies on other statistics in addition to workload, labour hours and supply costs. These other statistics are used in the cost allocation process. Examples are patient meal days, departmental total costs, etc. (see Appendix K for a list of the statistics used for cost allocation). To complete the evaluation of the hospital's case costing ability, review the Chart of Statistics:
• What needs to be collected? • What is currently being collected? • What is the source? • How is it collected?
From the answers to these questions, identify any missing data as well as any data collection problem areas. Be sure that the hospital staff’s understanding of the statistics is consistent with the MIS Standards definitions. These definitions are included in the Glossary at the end of this Guide.
OCCI Version 6.1 Page 92 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Chapter 13: Frequently Asked Questions
Cost Allocation Q: Our hospital has a Facilities Management functional centre which provides support to ten
areas, including Materials Management, Food Services, Housekeeping, Plant Operations, Plant Maintenance and Security. How do I allocate the costs of this department?
A: Distribute the costs in Facilities Management as a direct cost to the TCCs they support (Food Services, Housekeeping, Plant Operations, Plant Maintenance, etc.). Base the distribution on an estimate of the percentage of time staff spend supporting these functional centres. All the costs in these TCCs would then be allocated as indirect costs, via SEAM, to the patient care functional centres. The allocation statistics (percentage of time Facilities Management staff spend supporting the TCCs) will probably change from year to year, so update them on an annual basis.
Cost Distribution
Q: We have several ambulatory care functional centres that have only clerical staff, and all clinical work is done by a non-salaried physician. We do not collect workload for the physician. How do we distribute the costs associated with the operation of these functional centres?
A: In this situation it is reasonable that no patient care workload is collected. The hospital should calculate and distribute an average direct and indirect cost per visit for each functional centre. The direct costs should include the clerical staff salary and benefits expense. If the clerical staff perform activities for more than one functional centre, the associated costs should be distributed based on an estimate of the percentage of time the clerical staff spend supporting these functional centres.
Emergency Visits
Q: Some of our acute inpatients get admitted to Emergency and then proceed to be admitted as acute inpatients. Should I include the costs incurred in the Emergency visit with the acute inpatient stay?
A: The costs of all products received during the emergency visit should be associated with the emergency visit (e.g., lab tests, x-rays, emergency services) and not rolled into the acute inpatient stay.
Outsourced Services
Q: We outsource our laboratory services to another facility. How should we distribute these costs to patients?
A: The method used to distribute these costs will depend on the information that is available. Some hospitals negotiate a cost for each type of test performed by the facility. If this is what is done, then simply assign the cost of the tests received to the patient. Some hospitals enter into a blanket agreement with the facility whereby they agree to pay a certain fee for all tests performed during the year. In this case, there is no information on the cost of each type of laboratory test. Assign workload values to each test based on the NWMS, and then calculate unit costs.
OCCI Version 6.1 Page 93 of 105 Effective April 2008-March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Program Management Q: We have program management at our hospital. Our programs are staffed with nurses,
physiotherapists, occupational therapists and a social worker. A Program Manager oversees the programs. Where should I assign her salary?
A: The Program Manager’s labour hours and salary should be assigned as a direct cost to each of the four functional centres based on an estimate of the amount of time the Program Manager spends managing the activities of each discipline.
Research Q: We have staff performing research functions at our hospital. What do we do with these costs? A: If the staff are engaged in formal research activities, then all expenses associated with these activities
are to be captured in the Research functional centre. Any workload or expenses related to the provision of patient care or diagnostic and therapeutic services should not be recorded in the Research functional centre. Expenses in the Research functional centre are not allocated to patients, but remain undistributed.
If Research staff participate in unit producing work with ACC staff, this time is not recorded in the ACC. However, if these staff perform unit-producing work instead of regular functional centre staff, workload units and actual hours should be assigned to the functional centre receiving the service. The majority of their time should still be recorded in the Research functional centre.
ACC staff who participate in research by collecting and analyzing data or performing additional clinical interventions should have their hours recorded in the ACC. Capture patient-specific workload for the clinical interventions performed.
Restructuring
Q: How do I treat restructuring costs?
A: Costs that meet the OHRS definition of restructuring (see OHRS Version 6.2 ) should be charged to the Restructuring accounting centre (81970). These costs should remain undistributed since restructuring is considered to be outside the hospital’s production of patient services.
Revenues and Expenses
Q: The Pharmacy receives significant discounts or credits from the supplier on certain drugs that reduce the total expenses for those drug products. Should the discounts be netted from the cost of the drugs?
A: Purchasing discounts and credits should be netted from the expenses of supplies, drugs and equipment. While these discounts should be used to reduce the expenses for case costing purposes, they must be reported as ‘recoveries’ for Ministry of Health and Long-Term Care reporting purposes.
Q: How should we treat revenue in a patient care functional centre?
A: For case costing, patient care revenues should not be netted from expenses. The exception is where there is a functional centre with both patient and non-patient operations. In this situation non-patient
OCCI Version 6.1 Page 94 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
revenue is to be used as a proxy of non-patient costs, and netted from total expenses. Wherever possible, non-patient costs and revenues should be isolated by establishing a separate functional centre for non-patient operations. Patient care costs should not be distorted by a hospital’s other business activities.
Tracking Workload and Expenses
Q: We have nurses that work in Diagnostic Imaging. How do we cost the procedures performed by these nurses?
A: If the nurses are being substituted for Diagnostic Imaging technicians and are conducting tasks that are normally included as part of the procedure time, then the nursing activity should be captured through the diagnostic imaging workload measurement system. On the other hand, if the activity is not included as part of the diagnostic imaging workload measurement system, nursing standard times need to be added to the procedure’s time based on a Nursing workload measurement system. Salary and benefit expenses for these nurses should be tracked to the appropriate Diagnostic Imaging functional centres.
Tracking Workload
Q: In our hospital we assign the workload associated with the care of a newborn baby to its mother. How does this affect the case costs for our hospital?
A: Hospitals are required to assign workload associated with a newborn to the newborn’s account to accurately reflect the costs of the activities associated with each patient. In the situation where the newborn’s workload is assigned to the mother, the costs of the mother’s care will be overstated, and the newborn’s costs will be understated. This may significantly affect cost comparisons with other hospitals for neonatal and obstetrical cases.
Undistributed Functional Centres
Q: We are not costing some of our allied health functional centres. What should I do with these costs?
A: These costs should not be allocated to the other patient care functional centres or distributed to patients by the hospital. The OCCI employs a methodology to distribute undistributed patient care functional centre costs to patients. The hospital should still collect departmental workload, by patient type (inpatient, outpatient and referred-in) and these functional centres should receive indirect costs from TCCs.
OCCI Version 6.1 Page 95 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Appendix 1: The Case Costing Methodology in Action: A Numerical Example
The OCCI Guide described how to generate case costs by following the OCCI’s four-step case costing approach. This example reinforces the OCCI case costing methodology and concepts through a numerical example. The simplified example presented below follows the four steps of case costing introduced earlier. Step 1: Gather Data The data gathered for case costing includes:
• Financial data • Departmental workload and patient-specific workload or utilization statistics • Indirect cost allocation statistics • Patient descriptive data
Financial and statistical data are reported for each functional centre. The hospital in our example has the following TCCs and ACCs:
Table A.1
Hospital Functional Centres COST CENTRES
Transient Absorbing General Administration Nursing (OR) Housekeeping Laboratory Finance Diagnostic Imaging
The hospital’s financial data is found in the General Ledger (G/L), and expenses are tracked to each TCC and ACC as shown in Table A.2. The G/L shows the total costs for each TCC and ACC, as well as a further breakdown of total costs for the three ACCs.
Table A.2 General Ledger Costs
Functional Centre General Ledger Costs
General Administration $2,250,000 Housekeeping $1,000,000 Finance $750,000 Nursing (OR)
Labour $6,000,000 Patient-Specific Supplies $500,000
Laboratory Labour $2,000,000 General Supplies $750,000 Depreciation $250,000
OCCI Version 6.1 Page 96 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Diagnostic Imaging
Unit-producing Labour $2,000,000 Management and Support Labour $50,000 General Supplies (GS) $100,000 Patient-Specific Supplies (PSS) $150,000 Depreciation $100,000 Medical Fee-For-Service $100,000
In the statistical G/L, workload information is available. This hospital only provides services for acute inpatients and outpatients. Complex continuing care and rehabilitation workload would have been included in the total workload if these services were provided.
Table A.3 Departmental Workload Profiles
Workload Functional Centre
Acute Inpatient
Outpatient Referred-In Total
Nursing (OR) 2,700,000 300,000 0 3,000,000 Laboratory 1,500,000 1,000,000 500,000 3,000,000 Diagnostic Imaging 1,500,000 600,000 150,000 2,250,000
Remember that door-to-door time is captured in the OR on a patient-specific basis. Also, note that only patient-specific workload is used in the case costing calculations. Step 2: Allocate Indirect Costs The allocation of the total costs of TCCs to ACCs is achieved using the Simultaneous Equation Allocation Method (SEAM). SEAM uses allocation bases as a means of estimating the proportion of TCC costs that each ACC receives. These allocation bases are based on the MIS Standards.
Table A.4
Standard Allocation Bases
FUNCTIONAL CENTRE ALLOCATION NUMERATOR ALLOCATION DENOMINATOR
General Administration Total Department Cost Total Hospital Cost
Department Weighted Net Square Metres Hospital Weighted Net Square Metres Housekeeping (Total Department Cost is also acceptable
if Metres not available) (Total Hospital Cost is also acceptable if Metres not available)
Finance Total Department Cost Total Hospital Cost
OCCI Version 6.1 Page 97 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
SEAM allocates the costs of TCCs by solving a system of linear equations. Each equation determines the total allocation of TCC costs to a functional centre using a set of allocation statistics. The statistics are calculated for each functional centre using the Allocation Numerator and Denominator. These statistics act as approximations of TCC utilization by each functional centre.
Table A.5
Allocation Statistics
General Administration Housekeeping Finance
General Administration .1500 .1000 .0500 Housekeeping .0500 .0500 .0700 Finance .0250 .0250 .0300 Nursing (OR) .4250 .4750 .5000 Laboratory .2000 .2000 .1500 Diagnostic Imaging .1500 .1500 .2000 Total 1.0000 1.0000 1.0000
The end results of SEAM allocation are TCCs with no costs and ACCs with direct costs and indirect costs. The indirect costs are the allocated costs from the TCCs.
Table A.6
Results after SEAM Allocation
Functional Centre After Allocation
Starting Balance Add Subtract Ending Balance General Administration
$2,250,000 $2,250,000 $0
Housekeeping $1,000,000 $1,000,000 $0 Finance $750,000 $750,000 $0 Nursing (OR) $6,500,000 $2,500,000 $9,000,000 Laboratory $3,000,000 $800,000 $3,800,000 Diagnostic Imaging $2,500,000 $700,000 $3,200,000
$16,000,000 $4,000,000 $4,000,000 $16,000,000 Total
Step 3: Calculate Functional Centre Unit/Intermediate Product Costs
As outlined in Chapter 5, there are two approaches to calculating patient costs. Approach 1: Calculate Functional Centre Unit Costs (MIS Workload Costing) The basis of this approach is to calculate a direct and an indirect cost per unit based on the patient-specific workload units produced by each functional centre.
OCCI Version 6.1 Page 98 of 105 Effective April 2008-March 2009 Updated August 2009
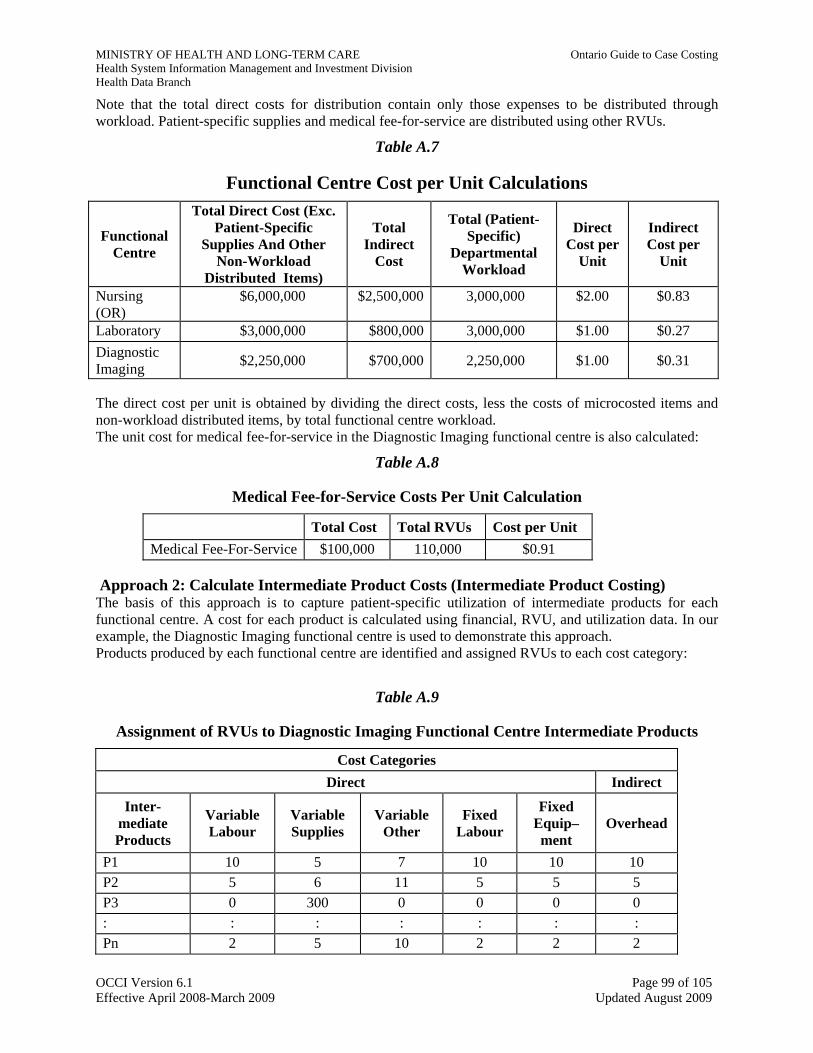
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Note that the total direct costs for distribution contain only those expenses to be distributed through workload. Patient-specific supplies and medical fee-for-service are distributed using other RVUs.
Table A.7
Functional Centre Cost per Unit Calculations Total Direct Cost (Exc.
Patient-Specific Supplies And Other
Non-Workload Distributed Items)
Total (Patient-Specific)
Departmental Workload
Direct Cost per
Unit
Indirect Cost per
Unit
Total Indirect
Cost
Functional Centre
Nursing (OR)
$6,000,000 $2,500,000 3,000,000 $2.00 $0.83
Laboratory $3,000,000 $800,000 3,000,000 $1.00 $0.27 Diagnostic Imaging $2,250,000 $700,000 2,250,000 $1.00 $0.31
The direct cost per unit is obtained by dividing the direct costs, less the costs of microcosted items and non-workload distributed items, by total functional centre workload. The unit cost for medical fee-for-service in the Diagnostic Imaging functional centre is also calculated:
Table A.8
Medical Fee-for-Service Costs Per Unit Calculation
Total Cost Total RVUs Cost per Unit Medical Fee-For-Service $100,000 110,000 $0.91
Approach 2: Calculate Intermediate Product Costs (Intermediate Product Costing) The basis of this approach is to capture patient-specific utilization of intermediate products for each functional centre. A cost for each product is calculated using financial, RVU, and utilization data. In our example, the Diagnostic Imaging functional centre is used to demonstrate this approach. Products produced by each functional centre are identified and assigned RVUs to each cost category:
Table A.9
Assignment of RVUs to Diagnostic Imaging Functional Centre Intermediate Products
Cost Categories Direct Indirect
Inter-mediate Products
Fixed Equip–ment
Variable Labour
Variable Supplies
Variable Other
Fixed Labour Overhead
P1 10 5 7 10 10 10 P2 5 6 11 5 5 5 P3 0 300 0 0 0 0 : : : : : : : Pn 2 5 10 2 2 2
OCCI Version 6.1 Page 99 of 105 Effective April 2008-March 2009 Updated August 2009
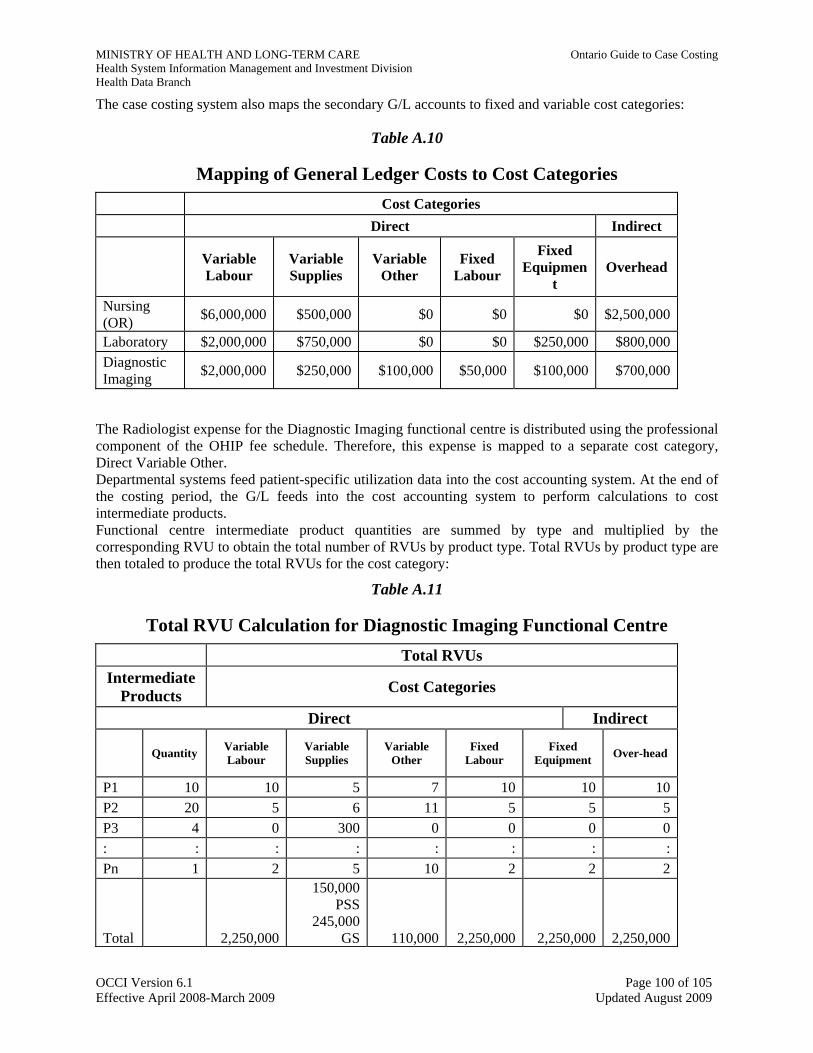
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
The case costing system also maps the secondary G/L accounts to fixed and variable cost categories:
Table A.10
Mapping of General Ledger Costs to Cost Categories Cost Categories Direct Indirect
Fixed Equipmen
t
Variable Labour
Variable Supplies
Variable Other
Fixed Labour Overhead
Nursing (OR) $6,000,000 $500,000 $0 $0 $0 $2,500,000
Laboratory $2,000,000 $750,000 $0 $0 $250,000 $800,000Diagnostic Imaging $2,000,000 $250,000 $100,000 $50,000 $100,000 $700,000
The Radiologist expense for the Diagnostic Imaging functional centre is distributed using the professional component of the OHIP fee schedule. Therefore, this expense is mapped to a separate cost category, Direct Variable Other. Departmental systems feed patient-specific utilization data into the cost accounting system. At the end of the costing period, the G/L feeds into the cost accounting system to perform calculations to cost intermediate products. Functional centre intermediate product quantities are summed by type and multiplied by the corresponding RVU to obtain the total number of RVUs by product type. Total RVUs by product type are then totaled to produce the total RVUs for the cost category:
Table A.11
Total RVU Calculation for Diagnostic Imaging Functional Centre Total RVUs
Intermediate Products Cost Categories
Direct Indirect
Variable Labour
Variable Supplies
Variable Other
Fixed Labour
Fixed Equipment Quantity Over-head
P1 10 10 5 7 10 10 10P2 20 5 6 11 5 5 5P3 4 0 300 0 0 0 0: : : : : : : :Pn 1 2 5 10 2 2 2
150,000 PSS
245,000 GS 110,000 2,250,000 2,250,000 2,250,000Total 2,250,000
OCCI Version 6.1 Page 100 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
PSS=patient-specific supplies GS=general supplies
To meet the minimum requirement of micro-costing supplies greater than $250, RVUs based on actual supply costs are assigned to products in the Direct Variable Supplies cost category. P3 is an example of a patient-specific supply product. Note that all other cost categories for this product have RVUs equal to 0. Separate workload totals are calculated for general supplies and patient-specific supplies. Radiologist expenses are distributed to patients using RVUs based on the professional component of the OHIP fee schedule. These RVUs are found in the Direct Variable Other cost category. An average cost per RVU is calculated for each cost category within each patient care functional centre:
Table A.12
Average Cost per Diagnostic Imaging RVU by Cost Category Cost Categories Direct Indirect
Variable Other
(Medical fee-for-service)
Variable Supplies (Patient-Specific)
Variable Supplies (General)
Variable Labour
Fixed Labour
Fixed Equipment Overhead
Total G/L Costs
$2,000,000 $100,000 $150,000 $100,000 $50,000 $100,000 $700,000
Total RVUs
2,250,000
2,250,000 2,250,000 245,000 150,000 110,000 2,250,000
Average Cost/RVU
$0.89 $0.41 $1.00 $0.91 $0.02 $0.04 $0.31
The cost of each product is determined by multiplying the RVU of the product by the average cost per RVU for each cost category. The average cost per RVU for general supplies is shown in the Variable Supplies cost category. For patient-specific supplies, the average cost per RVU is $1.00 since total RVUs are equal to the total costs of patient-specific supplies.
OCCI Version 6.1 Page 101 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Table A.13
Intermediate Product Costs for Diagnostic Imaging Functional Centre P1 P2 P3
Average Cost Per
RVU
RVU Profile
Total Cost
RVU Profile
Total Cost
RVU Profile Total Cost
Direct Variable Labour $0.89 10 $8.90 5 $4.45 0 $0
Direct Variable Supplies – General Supplies
$0.41 5 $2.05 6 $2.46 0 $0
Direct Variable Supplies – Patient-Specific Supplies
$1.00 0 $0 0 $0 300 $300.00
Direct Variable Other (Med. fee-for-service)
$0.91 7 $6.37 11 $10.01 0 $0
Direct Fixed Labour $0.02 10 $0.20 5 $0.10 0 $0
Direct Fixed Equipment $0.04 10 $0.40 5 $0.20 0 $0
Total Direct Product Cost $17.92 $17.22 $300.00
Overhead (Indirect Product Cost)
$0.31 10 $3.10 5 $1.55 0 $0
Total Cost of Product $21.02 $18.77 $300.00
Step 4: Distribute Costs to Patients Approach 1: Distribute Costs to Patients Based on the Total Number of Units Received For each functional centre from which the patient has received services, calculate the patient’s direct and indirect cost. The patient’s direct cost is obtained by multiplying the unit direct cost by workload units received by the patient, then adding the costs of all microcosted items (e.g., patient-specific supplies greater than $250, drugs) and other non-workload distributed costs (e.g., medical fee-for-service).
A patient receiving 25 workload units, 15 medical fee-for-service RVUs, and $900 of patient-specific supplies in Diagnostic Imaging, has the following patient costs:
OCCI Version 6.1 Page 102 of 105 Effective April 2008-March 2009 Updated August 2009
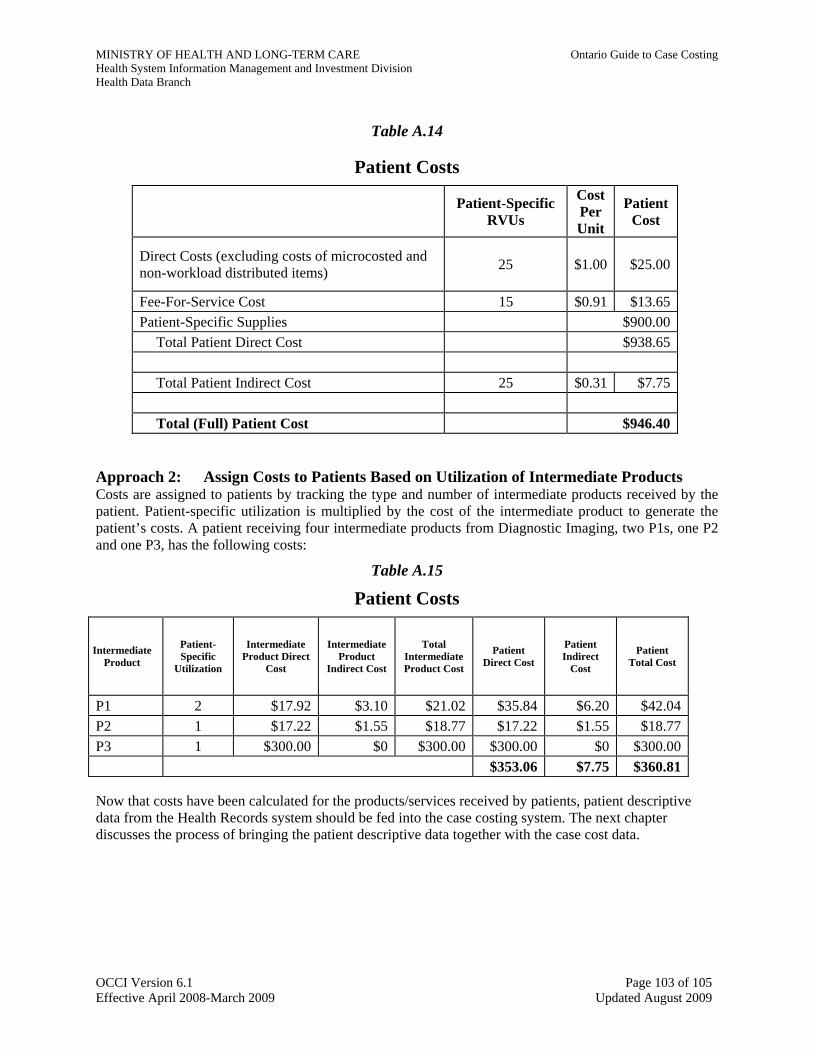
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Table A.14
Patient Costs Cost Per Unit
Patient-Specific RVUs
Patient Cost
Direct Costs (excluding costs of microcosted and non-workload distributed items) 25 $1.00 $25.00
Fee-For-Service Cost 15 $0.91 $13.65 Patient-Specific Supplies $900.00
Total Patient Direct Cost $938.65
Total Patient Indirect Cost 25 $0.31 $7.75
Total (Full) Patient Cost $946.40 Approach 2: Assign Costs to Patients Based on Utilization of Intermediate Products Costs are assigned to patients by tracking the type and number of intermediate products received by the patient. Patient-specific utilization is multiplied by the cost of the intermediate product to generate the patient’s costs. A patient receiving four intermediate products from Diagnostic Imaging, two P1s, one P2 and one P3, has the following costs:
Table A.15
Patient Costs
Patient-Specific
Utilization
Intermediate Product Direct
Cost
Intermediate Product
Indirect Cost
Total Intermediate Product Cost
Patient Indirect
Cost
Intermediate Product
Patient Direct Cost
Patient Total Cost
P1 2 $17.92 $3.10 $21.02 $35.84 $6.20 $42.04P2 1 $17.22 $1.55 $18.77 $17.22 $1.55 $18.77P3 1 $300.00 $0 $300.00 $300.00 $0 $300.00
$353.06 $7.75 $360.81 Now that costs have been calculated for the products/services received by patients, patient descriptive data from the Health Records system should be fed into the case costing system. The next chapter discusses the process of bringing the patient descriptive data together with the case cost data.
OCCI Version 6.1 Page 103 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
APPENDIX 2: ALLOWABLE RECOVERIES AND REVENUES IN CASE COSTING (FOR 2008/09) Key Notes ▪ Interdepartmental recoveries (FS 122**)/expenses (FS 697**) should be excluded from case costing.
The sum of FS 122* equals to that of FS 697** so the exclusion ensures zero impact. ▪ OHRS standards requires
o Cash discount (FS 12090) should be reported in Finance (PA 7*115), with the exception of Research (PA 7*7) and Marketed Services (PA 7* 920);
o Recovery Entity - Internal Laundering (FS 12196) should be reported in Laundry/Linen (PA 7*150);
o Recovery Entity - Biomedical Equipment Maintenance (FS 12195) should be reported in Bio - Medical (PA 7*1175);
o Recovery Entity - Food Services Outpatient (FS 12197) should be reported in Patient Food Services (PA 7*195).
▪ Referred - In recovery (FS 12030) and associated workload/patient activity, which are reported in home patient care functional centers, need to be handled as below:
Referred - In workload/patient activity/expenses need to included in case costing. However, the related recovery (FS 12030) cannot be used to net with departmental gross expenses.
▪ If Research (PA 7*7**)/Education (PA 7*8**)/Undistributed Functional Centers (PA 7*9**) share corporate admin and supportive services, they should absorb a part of admin and supportive expenses using the Simultaneous Equation Allocation Method (SEAM). Allowable recoveries/revenues in these departments are indicated in the table below.
▪ Net surplus (allowable revenues/recoveries greater than gross expenses) in Research (PA 7*7**)/ Education (PA 7*8**)/Undistributed Functional Centers (PA 7*9**) cannot be used to reduce expenses in other departments in the SEAM allocation. Also, the maximum for net cost in these departments is zero.
▪ Net Expenses in selected Undistributed Accounting Centers (PA 8*9**) listed below will be allocated to patients.
Functional Centre (PA) Recoveries Included Revenues Included
(FS Accounts) (FS Accounts) 7*1** Administration & Support 120*, 121* None
7*2** Nursing Inpatient 120* (except 12030), 121* 11016 and 11015 for
PA 7120710 and PA 71270; 11016 for other PA 712*
7*3** Ambulatory Care 120* (except 12030), 121* 11016 for PA 71305* & PA 71306*; 11016 & 11015 for PA 7130730 and PA 7130735; 11016 for PA 7131022; 11030 for PA 71330*; 11016 for PA 7134020
7*4* * Diagnostic & Therapeutic 120* (except 12030), 121* 11015 & 11016 for PA 7141040*; 11016 for all other PA 714* except
PA 71406 and PA 71490 7*5** Community Services 120* (except 12030), 121* None
OCCI Version 6.1 Page 104 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Health System Information Management and Investment Division Health Data Branch
Functional Centre (PA) Recoveries Included Revenues Included (FS Accounts) (FS Accounts)
7*7** Research 120*, 121* 13***, 14***,15***, 160**, 170**, 190**
7*8** Education 120*, 121* None
7*9** Undistributed Functional Centers 120*, 121* None 7*910 Non-Service Recipient Food Services 13***, 14***, 15***, 16***,
17***, 19*** 120*, 121* 7*920* Marketed Services 120*, 121* 13***, 14***, 15***, 16***,
17***, 19***
7*940
120*, 121* None 8*9** Selected Undistributed Accounting Centers included in case costing
Municipal Taxes (PA 81960) Other Undistributed Expenses - Operating (PA 81990) Employee Benefits Debit Clearing Account (PA 81995) Employee Benefits Credit Clearing Account (PA 81996) NEER Penalties (PA 81990) NEER Rebate (PA 81945) Employee Future Benefits (PA 81965)
OCCI Version 6.1 Page 105 of 105 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Ontario Guide to Case Costing Appendices
Changes for Fiscal Year 2008/09 are highlighted in yellow
Table of Contents APPENDIX A: ADDITIONAL REFERENCE MATERIALS................................................................................3
APPENDIX B: PROJECT HISTORY.......................................................................................................................4
APPENDIX C: HOSPITAL PROFILES...................................................................................................................6
APPENDIX D: CURRENT AND EXPECTED USES AND ANALYSES OF CASE COST DATA..................15 Atypical Acute Inpatient Ontario Case Weights/Factors .........................................................................................15 Ambulatory Care Weights .......................................................................................................................................15 Complex Continuing Care and Rehabilitation Weights/Factors..............................................................................16 Peer Hospital Factors and Hospital Effects .............................................................................................................16
APPENDIX E: OVERVIEW OF THE MIS STANDARDS AND OHRS.............................................................18 Introduction to MIS Standards.................................................................................................................................18 Frameworks .............................................................................................................................................................18 Functional Centre Reporting: Direct Cost, Full Cost and Service Recipient...........................................................18 Management Information Systems Application Framework ...................................................................................19 Functional Centre Framework .................................................................................................................................19 The Ontario Healthcare Reporting Standards ..........................................................................................................21
APPENDIX F: ABSORBING COST CENTRES AT OHRS FRAMEWORK LEVEL 3...................................22
APPENDIX G: CALCULATION OF PATIENT-SPECIFIC COST DISTRIBUTION PERCENTAGE.........24
APPENDIX H: CIHI ACUTE INPATIENT AND DAY SURGERY DATA RECORD .....................................27
APPENDIX I: AMBULATORY CARE COSTING PATIENT DESCRIPTIVE MINIMUM DATA SET ......31 Core Mandatory Data Elements...............................................................................................................................31 Service Specific Mandatory Data Elements ............................................................................................................31
APPENDIX J: INDIRECT COST ALLOCATION METHODOLOGY..............................................................32 Example of SEAM calculation ................................................................................................................................32 Other methods for reassigning overhead costs ........................................................................................................33
APPENDIX K: TRANSIENT COST CENTRE ALLOCATION METHODOLOGY TABLE .........................35
APPENDIX L: OCCI CASE COST RECORD.......................................................................................................39
APPENDIX M: PATIENT HOURS METHODOLOGY.......................................................................................41 Using Patient Hours to Calculate Functional Centre Unit Cost...............................................................................41 Operating Room ......................................................................................................................................................42 Obstetrics.................................................................................................................................................................42 Emergency Room ....................................................................................................................................................42 Rehabilitation Inpatients..........................................................................................................................................42 Complex Continuing Care .......................................................................................................................................43 Distributing Functional Centre Unit Cost to Patients based on Patient Hours.........................................................43
APPENDIX N: CASE COSTING SYSTEM REQUIREMENTS .........................................................................45
OCCI Version 6.1 Page 1 of 53 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Input to Departmental Systems and Case Costing System ......................................................................................45 Output from Departmental Systems ........................................................................................................................45 Output from Case Costing Systems .........................................................................................................................45 Tracking...................................................................................................................................................................45 Querying Tools ........................................................................................................................................................45 Audit Reports...........................................................................................................................................................45 Stand Alone System.................................................................................................................................................45 Batch/real time.........................................................................................................................................................45 Other ........................................................................................................................................................................45 Vendors....................................................................................................................................................................46
APPENDIX O: OCCI MILESTONE REVIEWS...................................................................................................47 Milestone 1 – Building Blocks ................................................................................................................................47 Milestone 2 – Pre-Go-Live Check ...........................................................................................................................47 Milestone 3 – Three Months Test Data ...................................................................................................................47 Milestone 4 – One Full Year of Data.......................................................................................................................48
APPENDIX P: EVALUATION CHECKLIST .......................................................................................................49 Appendix P-1: Overview of Data Collection and Reporting Within Functional Centre Framework ......................49 Appendix P-2: Patient Identification Data Collection and Reporting Within Functional Centre Framework.........49 Appendix P-3: Workload Data Collection and Reporting Within Functional Centre Framework ..........................50 Appendix P-4: Labour Hour Tracking Within Functional Centre Framework ........................................................50
APPENDIX Q: NURSING PER HOUR WEIGHTS FOR REHABILITATION AND COMPLEX CONTINUING CARE PATIENT GROUPS ..........................................................................................................51
OCCI Version 6.1 Page 2 of 53 Effective April 2008-March 2009 Updated August 2009
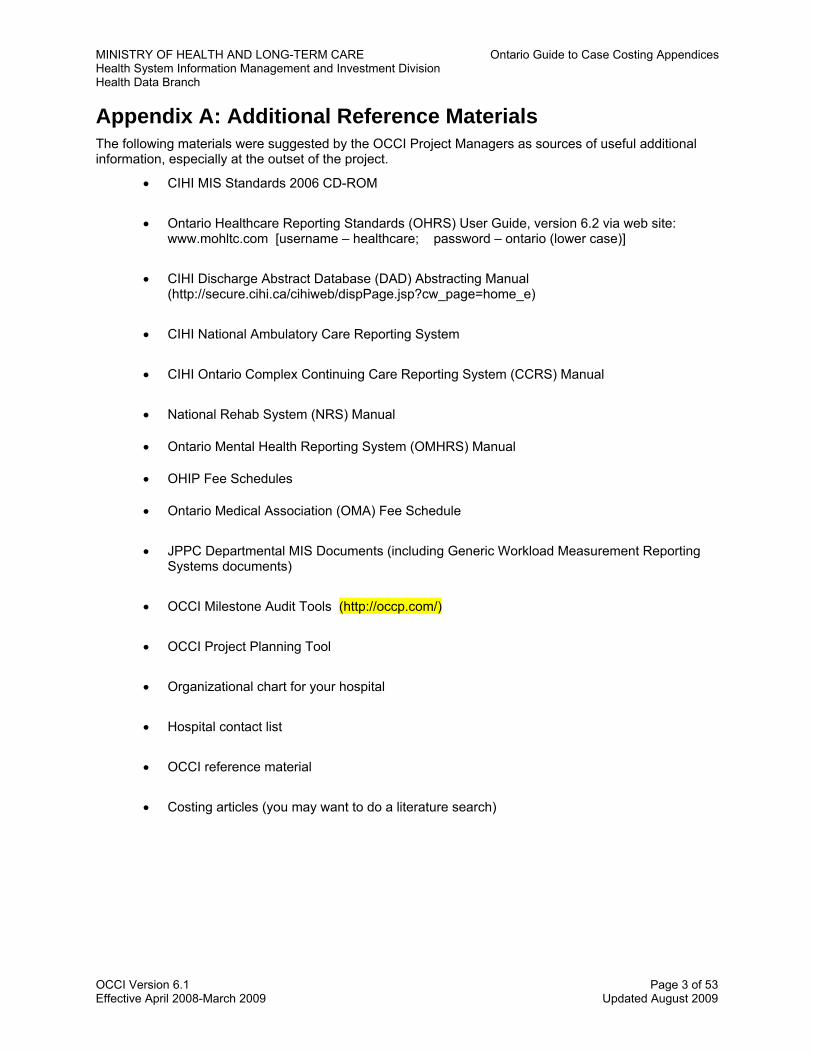
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix A: Additional Reference Materials The following materials were suggested by the OCCI Project Managers as sources of useful additional information, especially at the outset of the project.
• CIHI MIS Standards 2006 CD-ROM
• Ontario Healthcare Reporting Standards (OHRS) User Guide, version 6.2 via web site: www.mohltc.com [username – healthcare; password – ontario (lower case)]
• CIHI Discharge Abstract Database (DAD) Abstracting Manual (http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=home_e)
• CIHI National Ambulatory Care Reporting System
• CIHI Ontario Complex Continuing Care Reporting System (CCRS) Manual
• National Rehab System (NRS) Manual
• Ontario Mental Health Reporting System (OMHRS) Manual
• OHIP Fee Schedules
• Ontario Medical Association (OMA) Fee Schedule
• JPPC Departmental MIS Documents (including Generic Workload Measurement Reporting Systems documents)
• OCCI Milestone Audit Tools (http://occp.com/)
• OCCI Project Planning Tool
• Organizational chart for your hospital
• Hospital contact list
• OCCI reference material
• Costing articles (you may want to do a literature search)
OCCI Version 6.1 Page 3 of 53 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix B: Project History The Ontario case cost initiative was launched with the formation of the Ontario Case Cost Committee under Transitional Funding.1 This committee called for the development of:
•
• •
A more reliable case weight system than the 1985 New York2 charge-based Resource Intensity Weights (RIWs) More valid standards for the comparison of hospitals Better information to manage hospitals
To meet the above requirements, a case weight system based on Ontario case costs was proposed to enhance or replace the New York-based RIWs. To that end, a Hospital Incentive Fund (HIF) proposal was submitted early in 1992. In March of that same year, the Ministry of Health (MoH) approved $5.6 million in HIF funding for a project which would span three years and be operated jointly by the MoH and the Ontario Hospital Association (OHA). Thus, the Ontario Case Cost Project (OCCP) was born. An open invitation was presented to all Ontario hospitals interested in joining the OCCP. At the end of the screening process, thirteen hospitals were selected to participate in the Project. Each hospital was required to develop and implement the necessary systems and procedures to comply with the OCCP standards and methodology for producing case costs. To assist hospitals in this process, the OCCP created four Milestone Audit Tools. Each hospital was audited at the development, implementation and post-implementation stages of case costing. The Milestone audits were aimed at ensuring compliance with the case costing standards, and data quality. Each hospital received payment upon the completion of the requirements for each Milestone audit. Initially, these hospitals began collecting case cost data for acute inpatients on July 1, 1993. Subsequently, data for a one-year period starting October 1, 1993 was submitted to the OCCP to be included in a provincial database. On July 1, 1994, hospitals began collecting case cost data for the day surgery population. Second Generation In August 1995, a Second Generation of case costing hospitals was added to the Project. The Second Generation was initially comprised of seventeen acute care hospitals and five free standing specialty hospitals. In addition to increasing the number of acute inpatient and day surgery cases being costed, the Second Generation was intended to expand the scope of case costing to complex continuing care, rehabilitation and ambulatory care patient populations. The OCCP developed costing standards specifically for complex continuing care and ambulatory care based on the existing acute inpatient and day surgery standards. Like the First Generation, each Second Generation hospital received a grant upon passing each of the four Milestone audits. The acute care hospitals of the Second Generation went live with acute inpatient and day surgery case costing on April 1, 1996. Hospitals began complex continuing care costing on July 1, 1997. Rehabilitation costing was delayed pending development of a minimum data set. The OCCP Joint Committee manages the OCCP, and is responsible for the overall management and operation of the OCCP. This committee has representation from the OHA, the MoH and one OCCP hospital. There are two sub-committees under the OCCP Joint Committee:
1 Transitional Funding was formed in 1988 to correct for the imbalances and inequities of the global hospital funding system. A case-mix case cost approach within the context of global budgeting was introduced, with RIWs playing a prominent role as a measure of hospitals’ relative resource consumption between different case mix classifications.
2 Later, weights based on charge data from Maryland replaced New York charge data.
OCCI Version 6.1 Page 4 of 53 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Data Reliability and Validity Subcommittee: •
• •
Responsible for managing the quality of the data produced by the Project Representation from the MoH, OHA, Canadian Institute for Health Information, and hospitals not participating in the Project
Project Managers (First and Second Generation) Subcommittee: Responsible for the day-to-day operation of the hospital’s participation in the Project Representation from each of the Project hospitals
Governance Model
The agreement between the MOHLTC and the OHA expired on March 31, 2000. As case costing forms a basis for hospital funding methodologies, the founding partners agreed that the custodianship should be transferred to the MOHLTC. The database and the associated files were relocated to the MOHLTC offices located at 5700 Yonge Street in Toronto. In recognition of the on-going nature of the collection of case costing information, the name was changed to the Ontario Case Costing Initiative (OCCI).
OCCI Expansion In 2005, the Information Management Unit of the Ministry of Health and Long-Term Care put out an open invitation to facilities across Ontario to join the Ontario Case Costing Initiative. The decision to expand OCCI was based on the need to have more representative data for the province of Ontario. Following the open invitation, the Ministry received a positive response, and thirty-seven facilities signed on to join the Ontario Case Costing Initiative. For a full listing of new facilities, please refer to the “Participating Hospitals” link.
OCCI Version 6.1 Page 5 of 53 Effective April 2008-March 2009 Updated August 2009

MINISHealtHealt
OCCI Version Effective April
TRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendh System Information Management and Investment Division h Data Branch
6.1 Page 6 of 52008-March 2009 Updated August 2009
Appendix C: Hospital Profiles
ices
3
For First and Second Generation Participating Hospitals, the Total Discharge and Bed counts are based on data from FY 96/97. For Expansion Hospitals, the Bed counts are based on data from FY 04/05.
The tables on the following pages provide a brief profile of all First and Second Generation as well as Expansion hospitals participating in the OCCI.
Case Costing System Vendor indicates the case costing software the hospital is using. Note that the vendor may be providing a single vendor solution (the financial, departmental and case costing systems) or just the case costing application itself.

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
OCCP Hospital Profile First Generation January 1998
Original Hospital Name Current Hospital Name City Discharges Beds Type Case Costing System Vendor
Chedoke-McMaster Hospitals Hamilton Health Sciences Corporation Hamilton 16,112 744 Teaching In-house Hawkesbury and District General Hospital Hawkesbury 2,835 44 Community Phoenix Solutions Inc.
Hotel Dieu Hospital St. Catharines 5,733 122 Community Coopers and Lybrand Mount Sinai Hospital Toronto 19,867 418 Teaching Eclipsys St. Joseph’s Hospital North Bay General Hospital North Bay 11,070 218 Community Meditech
Oshawa General Hospital Lakeridge Health Corporation, Oshawa Campus Oshawa 19327 508 Community Meditech
Ottawa General Hospital Ottawa Hospital, General Campus Ottawa 17,798 401 Teaching Eclipsys Sunnybrook Health Sciences Centre
Sunnybrook and Women’s College Health Sciences Centre Toronto 17,000 1,100 Teaching Eclipsys
The Credit Valley Hospital Mississauga 17,796 297 Community Meditech
The Mississauga Hospital Trillium Health Centre, Mississauga Site Mississauga 21,316 414 Community Meditech
The Riverside Hospital of Ottawa
Ottawa Hospital,The Riverside Campus Ottawa 10,919 204 Community Meditech
University Hospital Victoria Hospital London Health Sciences Centre London 38,229 882 Teaching Eclipsys
OCCI Version 6.1 Page 7 of 53 Effective April 2008-March 2009 Updated August 2009
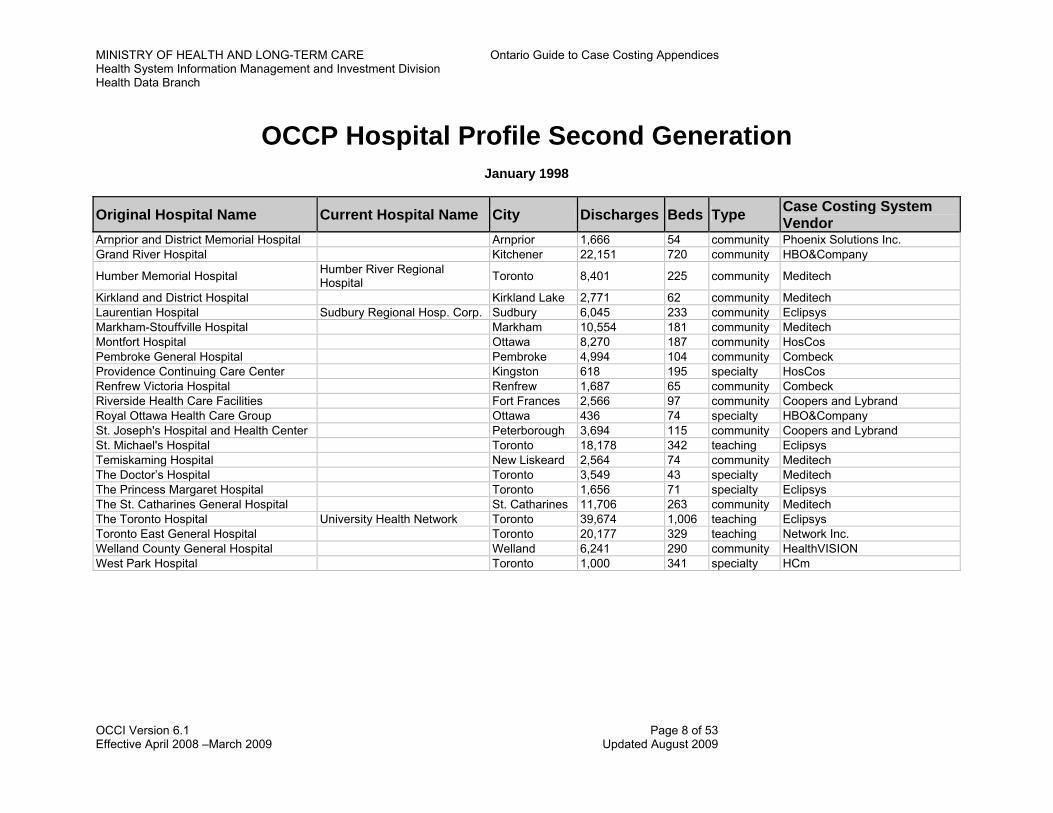
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
OCCP Hospital Profile Second Generation
January 1998
Original Hospital Name Current Hospital Name City Discharges Beds Type Case Costing System Vendor
Arnprior and District Memorial Hospital Arnprior 1,666 54 community Phoenix Solutions Inc. Grand River Hospital Kitchener 22,151 720 community HBO&Company
Humber Memorial Hospital Humber River Regional Hospital Toronto 8,401 225 community Meditech
Kirkland and District Hospital Kirkland Lake 2,771 62 community Meditech Laurentian Hospital Sudbury Regional Hosp. Corp. Sudbury 6,045 233 community Eclipsys Markham-Stouffville Hospital Markham 10,554 181 community Meditech Montfort Hospital Ottawa 8,270 187 community HosCos Pembroke General Hospital Pembroke 4,994 104 community Combeck Providence Continuing Care Center Kingston 618 195 specialty HosCos Renfrew Victoria Hospital Renfrew 1,687 65 community Combeck Riverside Health Care Facilities Fort Frances 2,566 97 community Coopers and Lybrand Royal Ottawa Health Care Group Ottawa 436 74 specialty HBO&Company St. Joseph's Hospital and Health Center Peterborough 3,694 115 community Coopers and Lybrand St. Michael's Hospital Toronto 18,178 342 teaching Eclipsys Temiskaming Hospital New Liskeard 2,564 74 community Meditech The Doctor’s Hospital Toronto 3,549 43 specialty Meditech The Princess Margaret Hospital Toronto 1,656 71 specialty Eclipsys The St. Catharines General Hospital St. Catharines 11,706 263 community Meditech The Toronto Hospital University Health Network Toronto 39,674 1,006 teaching Eclipsys Toronto East General Hospital Toronto 20,177 329 teaching Network Inc. Welland County General Hospital Welland 6,241 290 community HealthVISION West Park Hospital Toronto 1,000 341 specialty HCm
OCCI Version 6.1 Page 8 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
OCCI Hospital Profile Expansion Project 2006 to 2010
Facility Name Address City Postal
Code Type
(see Type abbreviations below)
No. of Beds
Campbellford Memorial Hospital
146 Oliver Road Campbellford K0L 1L0 AM, AT, CR, LT, AS 78
Hamilton Health Sciences 237 Barton Street East, General Site
Hamilton L8L 2X2 RT, AM, SR, AT, GR, MC 838
Headwaters Health Care Centre
100 Rolling Hills Drive Orangeville L9W 4X9 AM, AT, CR 112
Humber River Regional Hospital
200 Church Street Toronto M9N 1N8 AM, AT, GR, MC, MH, AM, AT 756
Northeast Mental Health Centre – North Bay campus
P.O.Box 3010 North Bay P1B 8G4 SF 44
Peterborough Regional Health Centre
1 Hospital Drive Peterborough K9J 7C6 AM, AT, CR, GR, LT, MH 341
Queensway Carleton Hospital 3045 Baseline Road Nepean K2H 8P4 AM, AT, GR, MH 248
Renfrew Victoria Hospital 499 Raglan Street North
Renfrew K7V 1P6 AM, AT, CR 54
Rouge Valley Health System 2867 Ellesmere Road Toronto M1E 4B9 AM, AT, GR, MH, CR, MC 473
Royal Victoria 201 Georgian Drive Barrie L4M 6M2 AM, AT, CR, GR, MH 299
Runnymede Healthcare Centre 625 Runnymede Road
Toronto M6S 3A3 CR 95
Salvation Army Grace Hospital 650 Church Street Toronto M4Y 2G5 CR, AT
OCCI Version 6.1 Page 9 of 53 Effective April 2008 –March 2009 Updated August 2009
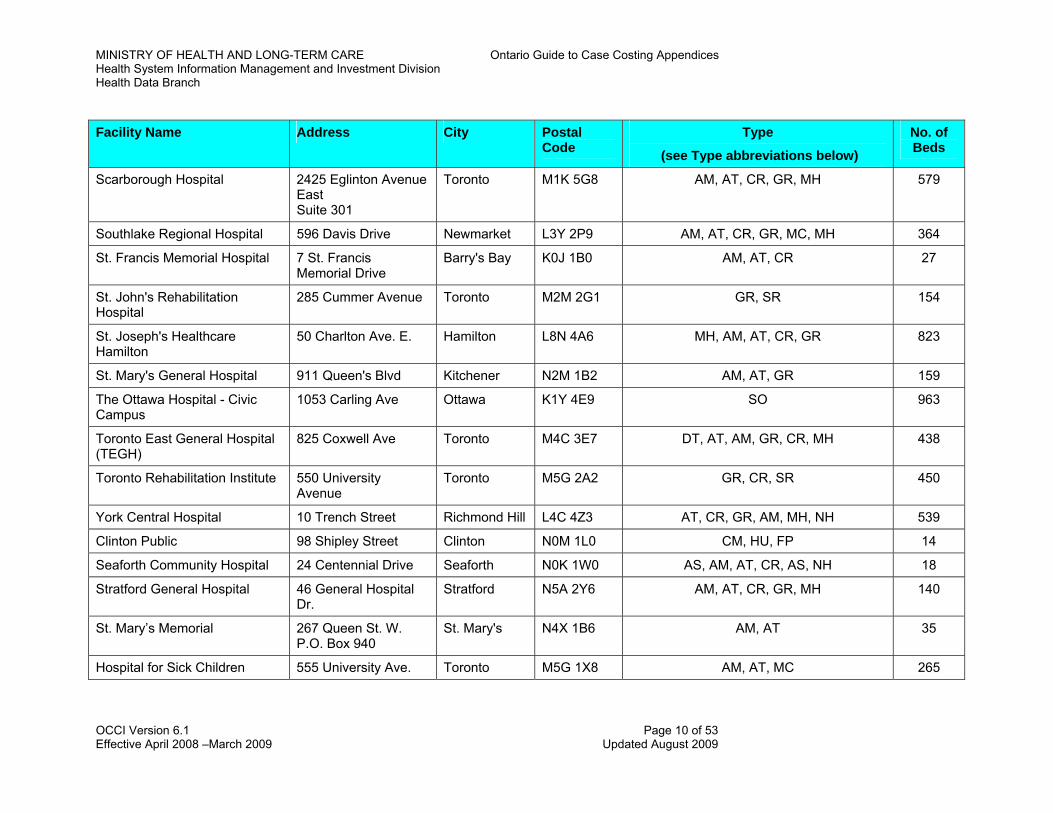
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Facility Name Address City Postal Type No. of Code Beds (see Type abbreviations below)
Scarborough Hospital 2425 Eglinton Avenue East Suite 301
Toronto M1K 5G8 AM, AT, CR, GR, MH 579
Southlake Regional Hospital 596 Davis Drive Newmarket L3Y 2P9 AM, AT, CR, GR, MC, MH 364
St. Francis Memorial Hospital 7 St. Francis Memorial Drive
Barry's Bay K0J 1B0 AM, AT, CR 27
St. John's Rehabilitation Hospital
285 Cummer Avenue Toronto M2M 2G1 GR, SR 154
St. Joseph's Healthcare Hamilton
50 Charlton Ave. E. Hamilton L8N 4A6 MH, AM, AT, CR, GR 823
St. Mary's General Hospital 911 Queen's Blvd Kitchener N2M 1B2 AM, AT, GR 159
The Ottawa Hospital - Civic Campus
1053 Carling Ave Ottawa K1Y 4E9 SO 963
Toronto East General Hospital (TEGH)
825 Coxwell Ave Toronto M4C 3E7 DT, AT, AM, GR, CR, MH 438
Toronto Rehabilitation Institute 550 University Avenue
Toronto M5G 2A2 GR, CR, SR 450
York Central Hospital 10 Trench Street Richmond Hill L4C 4Z3 AT, CR, GR, AM, MH, NH 539
Clinton Public 98 Shipley Street Clinton N0M 1L0 CM, HU, FP 14
Seaforth Community Hospital 24 Centennial Drive Seaforth N0K 1W0 AS, AM, AT, CR, AS, NH 18
Stratford General Hospital 46 General Hospital Dr.
Stratford N5A 2Y6 AM, AT, CR, GR, MH 140
St. Mary’s Memorial 267 Queen St. W. P.O. Box 940
St. Mary's N4X 1B6 AM, AT 35
Hospital for Sick Children 555 University Ave. Toronto M5G 1X8 AM, AT, MC 265
OCCI Version 6.1 Page 10 of 53 Effective April 2008 –March 2009 Updated August 2009
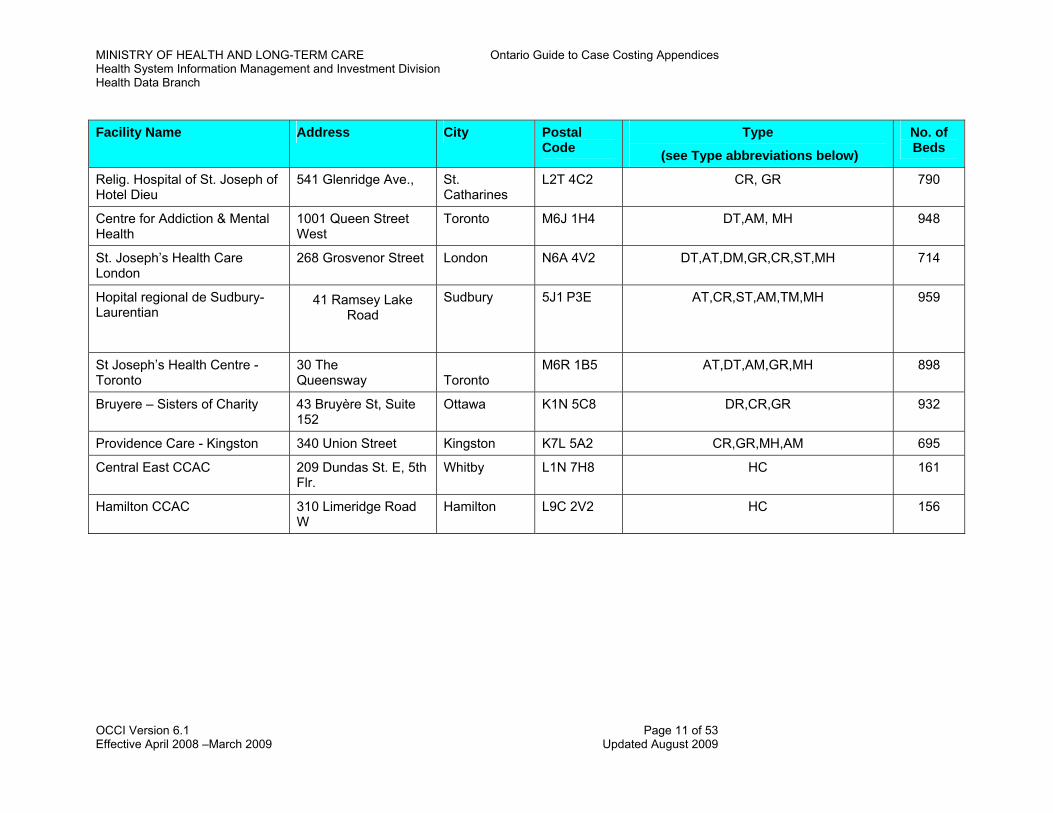
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Facility Name Address City Postal Type No. of Code Beds (see Type abbreviations below)
Relig. Hospital of St. Joseph of Hotel Dieu
541 Glenridge Ave., St. Catharines
L2T 4C2 CR, GR 790
Centre for Addiction & Mental Health
1001 Queen Street West
Toronto M6J 1H4 DT,AM, MH 948
St. Joseph’s Health Care London
268 Grosvenor Street London N6A 4V2 DT,AT,DM,GR,CR,ST,MH 714
Hopital regional de Sudbury-Laurentian
41 Ramsey Lake Road
Sudbury 5J1 P3E AT,CR,ST,AM,TM,MH 959
St Joseph’s Health Centre - Toronto
30 The Queensway
Toronto
M6R 1B5 AT,DT,AM,GR,MH 898
Bruyere – Sisters of Charity 43 Bruyère St, Suite 152
Ottawa K1N 5C8 DR,CR,GR 932
Providence Care - Kingston 340 Union Street Kingston K7L 5A2 CR,GR,MH,AM 695
Central East CCAC 209 Dundas St. E, 5th Flr.
Whitby L1N 7H8 HC 161
Hamilton CCAC 310 Limeridge Road W
Hamilton L9C 2V2
HC 156
OCCI Version 6.1 Page 11 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
PRE-EXISTING CASE COSTING FACILITIES THAT HAVE TRANSITIONED TO OCCI PROJECT (2010) Facility Name Address City Postal
Code Type
(see Type abbreviations below)
No. of Beds
Sunnybrook Health Sciences 2075 Bayview Ave. Toronto M4Y 1H1 SO, AT, CR, GR, MH, AM, NH 666
Arnprior and District Memorial Hospital
350 John Street North Arnprior K7S 2P6 AT,CR,AM 599
West Park Health Centre 82 Buttonwood Avenue
Toronto M6M 2J5 CR,SR 613
University Health Network 190 Elizabeth St Toronto M5G 2C4 DT,AT,AM,MH 947
St. Michael’s Hospital 30 Bond Street Toronto M5B 1W8 DT,AT,AM,MH 852
Lakeridge Health Corporation 850 Champlain Avenue, Unit 1
Oshawa L1J 8R2 AT,CR,GR,AM,MH 952
William Osler Health Centre 2100 Bovaird Dr. E. Brampton L6R 3J7 AT,CR,AM,GR,MH, 951
Credit Valley Hospital 2200 Eglinton Avenue West
Mississauga L5M 2N1 AT,CR,GR,AM,MH 731
Trillium Health Centre 100 Queensway West
Mississauga L5B 1B8 AT,CR,AM,GR,MH 949
Mount Sinai Hospital 600 University Avenue
Toronto M5G 1X5 AT,AM,MH 842
Quinte HealthCare Corporation 265 Dundas Street East
Belleville K8N 5A9 AT,CR,GR,AM,MH 957
Ottawa General 501 Smyth Rd Ottawa K1H 8L6 AT,AM,MH 958
London Health Sciences Centre
800 Commissioners Road East, PO Box 5010
London N6A 5W9
AT,AM,MH 936
OCCI Version 6.1 Page 12 of 53 Effective April 2008 –March 2009 Updated August 2009
MINISHealtHealt
OCCI Version Effective April
TRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices h System Information Management and Investment Division h Data Branch
6.1 Page 13 of 53 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
TYPE ABBREVIATIONS
TYPE CODE BROAD SERVICE CLASSIFICATION
AC Therapeutic Abortion Clinics AL Alternate Payments Program AM Ambulatory Care AS Ambulance Services AT Acute Care Treatment Hospital CA Children's Aid Society CC Correctional Centre CM Children's Mental Health Centre CO Community Health Centre CR Complex continuing Care Treatment Hosp. and Units of Hosp. DM Domiciliary Care Treatment Unit of Hospital DT Detoxification Centre FP Family Planning Unit GR Gen. Rehab. Hosp. and Units of Hosp. HC Home Care Program (Community Care Access Centres) HF Home for the Aged HL Public Health Laboratory HO Health Organization HU Public Health Unit IF Independent Facilities IN Min. Of Health Internally Used Classification LT Interim Long Term Care MH Mental Health Unit NH Nursing Home NS Nursing Station PR Approved Private Radiological Facilities PS Provider Services PT Physiotherapist (inc. Physiotherapy Centres) RT Rehab. Treatment Centre (Children's Treatment Centre) SF Schedule I and II Facilities SH Supportive Housing SO Health Service Organization SR Special Rehab. Hosp. & Units of Hospitals SS Special Schools TC Treatment Centre - Addiction TH Telehealh TM Temporary Long Term Care
OCCI Version 6.1 Page 14 of 53 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix D: Current and Expected Uses and Analyses of Case Cost Data The principal objective of the Ontario Case Costing Initiative is to produce a made-in-Ontario case cost database from which to develop Ontario Case Weights. The following provides a description of current and potential uses and analyses of case cost data, mostly in relation to hospital funding. This discussion is technical in nature, and is intended for those individuals who have some familiarity with hospital funding. Typical Acute Inpatient Ontario Case Weights Ontario case cost data is being used as the principal calibration database. CIHI (Canadian Institute for Health Information) uses the HSRV (Hospital-Specific Relative Value ) methodology for weight calibration. The HSRV calculates weights at the hospital level and then pools these hospital specific weights to calculate overall case weights. This method eliminates hospital specific factors that influence patient cost. Atypical Acute Inpatient Ontario Case Weights/Factors Separate RIW (Resource Intensity Weight) methodology is in place for atypical cases, such as:
1) Long-stay outliers 2) Deaths 3) Transfers In/Out 4) Sign-outs
Ambulatory Care Weights Day surgery cost data is already being provided by hospitals. Other ambulatory care cost data will be collected by some hospitals already participating in acute care costing and be grouped into MACs (Major Ambulatory Clusters). If enough data is collected, the types of analyses that would be done include:
•
• • • •
• • •
•
•
Calculations of average costs (as well as measures of central tendency and distribution) for each MAC; More detailed examinations of these costs:
Direct, indirect and total costs By cost category, where provided per extended standards Combinations of the above; and
Analyses directed at discerning hospital differences that affect the cost distribution: Scatter/other plots with hospitals differentiated Analyses with and without certain hospitals (for example, teaching, small, Northern, those with a specific Nursing patient classification scheme) Adjustments to account for the effects of one hospital in any given MAC (for example, taking the average of mean costs by hospital within each MAC).
From these analyses, meaningful average costs and the proposed new Ontario Case Weights3 can be developed, including adjustments for strong effects of high- or low-cost hospitals. Other analyses that could be performed include:
Correlation of cost with descriptive data and explanations of cost variance for each descriptive variable
3 Average Costs may not necessarily be proportional to Ontario Case Weights (e.g., if the MoH chooses to build
incentives into the Ontario Case Weights).
OCCI Version 6.1 Page 15 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
•
•
•
•
•
•
Comparisons of day surgery and surgical inpatient costs for the same operative procedure
In addition, linkages among encounters for the same patient will facilitate analyses: Pre-admission visits linked to acute inpatient and day surgery encounters would support the full costing of elective cases Links among outpatient visits may be meaningful in assessments of recurring outpatient cases and/or related outpatient encounters.
Complex Continuing Care and Rehabilitation Weights/Factors Cost data by separated case may be meaningful for some rehabilitation cases with lengths of stay of a few weeks or months, for example. For most complex continuing care activity, however, separation-based data is not meaningful due to the high variations in length of stay among patients (in addition, it would be difficult to analyze such long-term data). An alternate unit of measure is patient days over an assessment period, with differentiation of patients according to their RUGs III grouping. For complex continuing care inpatients (as well as for recurring outpatients and Day Hospital patients), the types of analyses that could be done would be similar to those for acute inpatients, but using costs per day or visit rather than costs per stay. Case cost data from complex continuing care cases are expected from some acute care case costing hospitals as well as from some free-standing complex continuing care facilities. Rehabilitation cost data is available as the the rehabilitation patient descriptive data set has been developed. Data from acute care and non-acute facilities would be useful in examining cost behaviour in complex continuing care and rehabilitation programs. Peer Hospital Factors and Hospital Effects
Data from case costing hospitals may provide some insight into differences in specific types of cases among hospitals (analyses of costs and nature of costs within a specific CMG for different hospitals in the sample).
However, there is potential for the skewing of average case costs by an individual hospital within a CMG or patient group if a small or unrepresentative sample of hospitals contributes data to a specific patient group or analysis. The proposed approach to dealing with this potential issue is:
Plot the case cost data for a specific patient group, using different characters to represent individual hospitals contributing to the sample. Also, compute descriptive statistics for each hospital within the patient group (mean/median cost, standard deviation, etc.), and perform tests to determine whether average costs vary by hospital. If there does appear to be a problem related to skewing by an individual hospital within a specific patient group, then different methods of dealing with the issue should be examined. These methods could include transforming the data for each hospital so that effects of variations in input costs are removed, adjusting per the Ontario average length of stay for the patient category, and/or adjusting average costs to treat each hospital's contribution equally (as if they contributed the same number of cases).
Other Potential Uses of Data/Methodology
Other potential uses of the costing methodology and Ontario case cost data include:
Ultimately, the development of a comprehensive weighted case index for each hospital that homogeneously incorporates all relevant patient-related output (Total Weighted Cases = Typical Acute Inpatient Weighted Cases + Atypical Acute Inpatient Weighted Cases + Day Surgery
OCCI Version 6.1 Page 16 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Weighted Cases + Ambulatory Care4 Weighted Cases + Complex continuing Care Equivalent Weighted Cases + Rehabilitation Equivalent Weighted Cases). This would reduce much of the work required in trying to account for costs (e.g. ambulatory and complex continuing care) related to outputs that are not now in the weighted case index.
•
•
•
•
•
Calculation of the Cost of Conservable Days — this is an estimate of projected savings, especially from clinical efficiencies. The proportion of costs that have been identified as Routine and Ancillary (i.e., variable) is expressed as a proportion of total costs. The use of costs by category/functional centre and other data to identify factors that affect costs of different cases and cost variations among hospitals. The use of procedure detail to examine the intermediate products that constitute the cost of a particular patient group/case (extended standards). Identification of CMGs that may have differences in inpatient Nursing costs between sets of hospitals with different Nursing workload measurement systems (primarily GRASP and Medicus), and for which differences in workload that are related to the Nursing WMS could be potentially investigated. Examinations of fixed and variable costs for a specific patient group to assist with marginal costing/funding (extended standards).
The OCCI is supporting Ontario hospital reform and research
The OCCI has been approached by various groups to provide assistance with Ontario hospital reform and research activity. In addition to the MOHLTC and the OHA, these organizations have included the Ontario Joint Policy and Planning Committee, Health Services Restructuring Commission, and Ontario Hospitals.
The OCCI has also participated in research activities with the Institute of Clinical Evaluative Sciences, Statistics Canada and various universities.
4 Excluding day surgery cases.
OCCI Version 6.1 Page 17 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix E: Overview of the MIS Standards and OHRS This appendix provides a general overview of the MIS Standards and the Ontario Healthcare Reporting Standards (OHRS). Specifically, it highlights sections of the MIS Standards that are important for case costing and introduces the OHRS. For more information, consult the MIS Standards 2006 and the OHRS User Guide, Version 6.2. Introduction to MIS Standards The MIS Standards are designed to provide a comprehensive framework to organize hospital management information at a national level. The objective of the MIS Standards is to establish standards to:
•
•
•
• •
Improve the timeliness and comparability of data collected within Canadian health care facilities for management, planning, evaluation, reimbursement and research purposes; and Better measure resources and activities by integrating financial, statistical and clinical operational databases.
The MIS Group originally developed the MIS Standards. The Canadian Institute for Health Information (CIHI) manages the ongoing development and maintenance of the MIS Standards, including the production of annual updates. Frameworks The MIS Standards use three frameworks to organize information collected in hospitals, namely:
The Functional Centre Direct Cost Reporting, Functional Centre Full Cost Reporting and Service Recipient Reporting Framework; The Management Information Systems Application Framework; and The Functional Centre Framework.
Functional Centre Reporting: Direct Cost, Full Cost and Service Recipient Functional Centre Direct Cost Reporting identifies the direct resources used to provide a specific service within a functional centre. Functional Centre Full Cost Reporting, previously called the Departmental Dimension of reporting, refers to the collection of activity data at the functional centre or departmental level through the identification of direct and indirect resources used to provide patient-specific services. This information allows for the management of resources from a departmental perspective. Service Recipient Reporting, or the patient-centered view (previously called the Global Dimension of reporting), refers to the collection of information to manage specific populations of patients. This involves the collection of departmental activity data, such as workload, on a patient-specific basis. Departmental activity under the MIS Standards is measured through the National Workload Measurement Systems (NWMS). Workload measurement systems (WMS) quantify departmental activity in terms of a standardized unit of time. They are used to quantify the staff time spent in patient care (e.g., patient assessment, completion of patient file) and non-patient care (e.g., staff meetings, in-service) activities. WMS tools can be used for the purposes of planning, staffing, budgeting and monitoring performance. Furthermore, comparisons can be made across hospitals since the NWMS standardize the measurement of departmental activity. The standardized unit of time is measured as a “unit of service” or workload unit. Each unit is equal to one minute of time. National unit values are available for selected health disciplines and activities. These national unit values were originally determined using time-motion studies and were averaged across Canada. An NWMS has been developed for each of the disciplines listed in Table 1.
OCCI Version 6.1 Page 18 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Table 1: Available National Workload Measurement Systems
Child Life/Recreation Pharmacy Clinical Laboratory Physiotherapy Clinical Nutrition Psychology
Diagnostic Imaging Radiation Oncology Electro-diagnosis Rehabilitation Engineering
Nursing Respiratory Therapy Occupational Therapy Social Work
Other Diagnostic Laboratories Speech/Language Pathology and Audiology Pastoral Care
More recently, CIHI has developed a WMS with a common reporting framework to address workload collection by multi-skilled, multi-disciplinary personnel. This WMS captures workload data through common data collection and reporting standards, and is more appropriate in multi-disciplinary and program management settings. The disciplines that the multi-disciplinary WMS applies to are listed in Table 2.
Table 2: Disciplines to which Multi-disciplinary WMS Applies Audiology Physiotherapy Child Life Psychology
Clinical Nutrition Social Work Nursing Speech Language Pathology
Occupational Therapy Therapeutic Recreation Pastoral Care/Spiritual Care
As opposed to the previous NWMS, the multi-disciplinary WMS provides a standardized framework for the classification of service recipient activities. Hospitals report unit values according to three service recipient activities (assessment, therapeutic intervention and consultation/collaboration) as well as non-service recipient activities. The multi-disciplinary WMS also standardizes the recording guidelines as they relate to service recipient activities.
Management Information Systems Application Framework The Management Information Systems Application Framework identifies the information systems needed to capture and process the data required to support Functional Centre Full Cost Reporting, Functional Centre Direct Cost Reporting and Service Recipient Reporting. This Framework provides detailed requirements for the various financial and clinical systems found in hospitals. A set of functional specifications that describe major system functions, data flows, interfaces, inputs, and outputs of these systems are part of the Framework. These detailed specifications are found in Appendix 1, Functional Specifications of the MIS Guidelines 1999.
Functional Centre Framework The Functional Centre Framework provides a standardized method of organizing, collecting and reporting financial and statistical information in a hospital. The Framework organizes hospital activity into functional centres. Functional centres are subdivisions of the hospital used in the accounting system to record revenue, expenses and statistics which pertain to a function or activity. Functional centres are also called primary accounts. The Functional Centre Framework features a five-level hierarchy. The hierarchy provides a structured method to collect and aggregate functional centre data. Starting from Level 1, each successive level represents a more detailed breakdown of data from the previous level.
OCCI Version 6.1 Page 19 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
The different levels of detail allow hospitals of varying sizes and complexity to use this framework to meet internal and external reporting needs. External comparative reporting can be accomplished through aggregating or ‘rolling-up’ accounts. The primary account code structure consists of five segments, totaling a maximum of nine coding positions. The first segment uses the first two digits to describe the account group and the fund type for primary accounts. All of the operating functional centres are in Broad Group 71 Revenue and Expense - Functional Centres (7) and Operating Fund (1).
• First and Second Digit (Level 1) - 71
The next segment describes the framework:
• Third Digit (Level 2 Functional Centre Framework)
1. Administrative and Support 2. Nursing Inpatient/Resident Services 3. Ambulatory Care Services 4. Diagnostic and Therapeutic Services 5. Community & Social Services 6. Medical Services 7. Research 8. Education 9. Undistributed (functional centres)
The remaining segments describe the type of service provided, or the functional centre:
•
•
•
•
Fourth and Fifth Digits (Level 3 Functional Centre)
Example: 71 4 15 - Diagnostic Imaging
Sixth and Seventh Digits (Level 4 Functional Centre)
Example: 71 4 15 30 - Diagnostic Ultrasound
Eighth and Ninth Digits (Level 5 Functional Centre)
Example: 71 4 15 30 80 - Neurological Ultrasound
Note that the higher level functional centres are more detailed than the lower level functional centres. A Level 5 functional centre describes more specific functional centres within a Level 4 functional centre. Similarly, a Level 4 functional centre describes more specific functional centres within a Level 3 functional centre. Secondary financial account codes describe the nature of revenues and expenses in the hospital. They are associated with functional centres (primary accounts). The five digits in the secondary account codes for revenue and expenses are organized into three groups as described below:
First Digit - Secondary Broad Group 1. Revenues 2. Inactive 3. Compensation 4. Supplies 5. Traceable Supplies and Other Expenses (termed “Service Recipient-Specific Supplies” in
Ontario) 6. Sundry 7. Equipment 8. Contracted-Out Services 9. Buildings and Grounds
• Second and Third Digits - Nature of Revenue or Expense
OCCI Version 6.1 Page 20 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Example: 4 50 - Food Supplies
•
•
Fourth and Fifth Digits – Capture Detail
Example: 4 50 26 - Butter
Secondary statistical account codes provide information on the nature of activities occurring in the hospital. They are also associated with functional centres. Secondary statistical accounts can be joined with information in the secondary financial account of the same functional centre to produce performance indicators. The secondary statistical accounts are organized specifically for statistics with a maximum of seven digits in the code.
First Digit – New Broad Groups of Secondary Statistical Accounts
1. Workload 2. Staff Activity 3. Earned Hours 4. Service Activity and Caseload Status (termed “Service Recipient Activity” in Ontario) 5. Inactive (in Ontario used for “Client Profile”) 6. Inactive (in Ontario used for “Personnel Profile”) 7. Functional Centre Operations 8. Health Service Organization Operation 9. Inactive (in Ontario used for Specialty and Priority Program Profile)
•
•
Second and Third Digits - Nature of Statistic
Fourth and Fifth Digits and Sixth and Seventh Digits - Capture Detail
The Ontario Healthcare Reporting Standards The provincial MIS initiative began in 1992 when the Ontario Ministry of Health (MoH) mandated the Functional Centre Reporting Framework (the Departmental Dimension) of the MIS Guidelines based on the recommendation of the former provincial MIS Steering Committee. All Ontario hospitals are required to submit their financial and statistical data in accordance with the standards established in the MIS Guidelines. The Ontario Healthcare Reporting Standards (OHRS) was developed to supplement the MIS Guidelines in defining provincial requirements for reporting. The OHRS also extended elements of the MIS Guidelines for Ontario-specific purposes. In Ontario and for the OCCP, the OHRS requirements supersede the requirements of the MIS Standards; i.e., the OHRS Chart of Accounts overrides the national MIS Chart of Accounts. Two Milestones were established to achieve Functional Centre Full Cost Reporting (i.e., Departmental reporting). The Milestone requirements included: Milestone 1 (implemented by April 1994)
• • • •
• • •
Conversion of financial Chart of Accounts New accounting policies and account definition changes Implementation of the Functional Centre and Accounting Centre Framework Implementation of partial statistical Chart of Accounts
Milestone 2 (implemented by April 1997) Completion of the statistical Chart of Accounts Distribution of detailed supply expenses Distribution of depreciation and maintenance costs
Milestone 3, Service Recipient Reporting (formerly Global Dimension reporting), or patient-specific costing, has not been mandated for Ontario hospitals. For more information on the OHRS, refer to the OHRS Version 6.2 documentation on the website, www.mohltc.fim.
OCCI Version 6.1 Page 21 of 53 Effective April 2008 –March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix F: Absorbing Cost Centres at OHRS Framework Level 3
Nursing Inpatient Services 7*205 Nursing Administration 7*206 Program Management Administration 7*207 Medical Resources 7*210 Medical 7*220 Surgical 7*230 Combined Medical/Surgical 7*240 Intensive Care 7*242 Cardiac Monitored Care 7*250 Obstetrics 7*260 Operating Room(s) 7*262 OR/PARR Combined 7*265 Post-Anesthetic Recovery Room(s) 7*270 Pediatric 7*276 Mental Health/Addictions 7*281 Rehabilitation 7*295 Long-Term Care Inpatient 7*297 All Inclusive Complex Continuing Care (CCC)
Ambulatory Care Services 7*305 Ambulatory Care Administration 7*306 Program Management Administration 7*307 Medical Resources 7*310 Emergency 7*320 Poison Information Centre 7*330 Tele-Health 7*340 Day/Night Care 7*350 Clinics 7*355 Private Clinics
Diagnostic and Therapeutic Services 7*406 Program Management Adminsitration 7*410 Clinical Laboratory 7*415 Diagnostic Imaging 7*425 Electrodiagnosis 7*430 Non-Invasive Cardiology and Vascular Laboratories 7*435 Respiratory Therapy 7*440 Pharmacy 7*444 Combined Therapeutics 7*445 Clinical Nutrition 7*449 Rehab Services Clinical Management 7*450 Physiotherapy 7*455 Occupational Therapy 7*460 Audiology and Speech/Language Pathology 7*465 Rehabilitation Engineering 7*466 Radiation Oncology
OCCI Version 6.1 Page 22 of 53 Effective April 2008 –March 2009 Updated August 2009
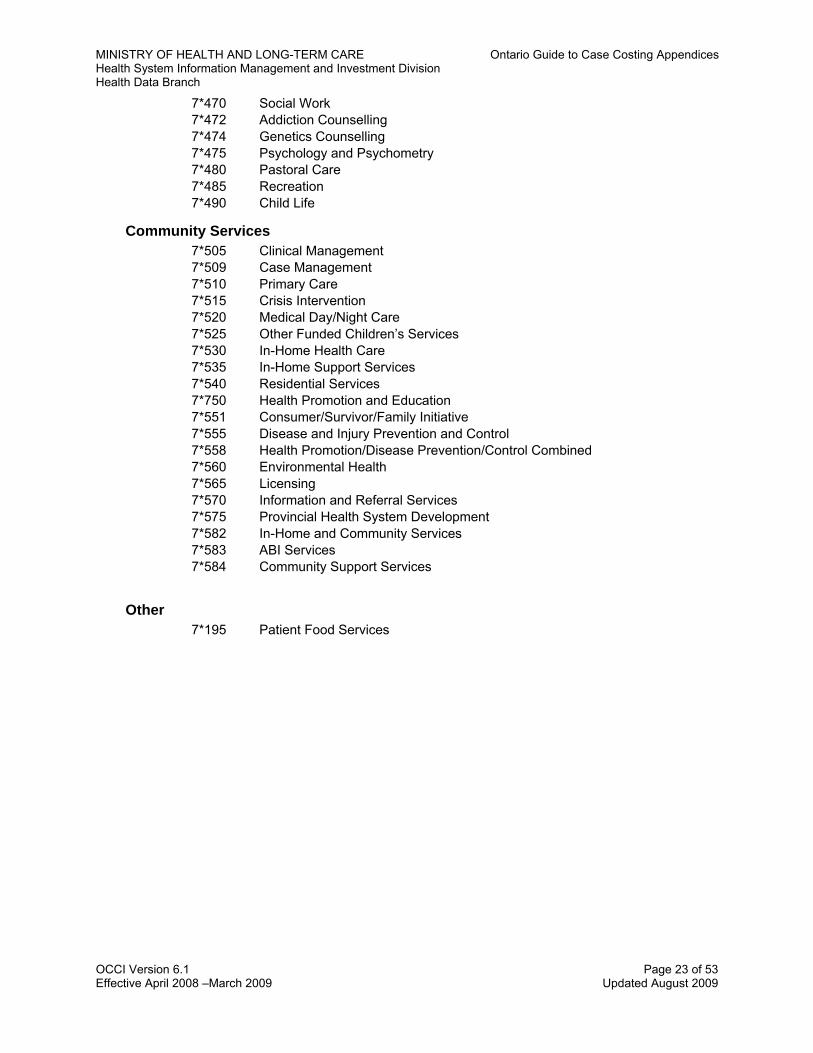
MINISHealtHealt
OCCI Version Effective April
TRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendh System Information Management and Investment Division h Data Branch
6.1 Page 23 of 53 2008 –March 2009 Updated August 2009
Other
Community Services
7*470 Social Work 7*472 Addiction Counselling 7*474 Genetics Counselling 7*475 Psychology and Psychometry 7*480 Pastoral Care 7*485 Recreation 7*490 Child Life
7*195 Patient Food Services
7*505 Clinical Management 7*509 Case Management 7*510 Primary Care 7*515 Crisis Intervention 7*520 Medical Day/Night Care 7*525 Other Funded Children’s Services 7*530 In-Home Health Care 7*535 In-Home Support Services 7*540 Residential Services 7*750 Health Promotion and Education 7*551 Consumer/Survivor/Family Initiative 7*555 Disease and Injury Prevention and Control 7*558 Health Promotion/Disease Prevention/Control Combined 7*560 Environmental Health 7*565 Licensing 7*570 Information and Referral Services 7*575 Provincial Health System Development 7*582 In-Home and Community Services 7*583 ABI Services 7*584 Community Support Services
ices

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
OCCI Version 6.1 Page 24 of 53 Effective April 2008-March 2009 Updated August 2009
Appendix G: Calculation of Patient-Specific Cost Distribution Percentage Hospital: ________________________________________________________ Fiscal Year: ____________________
Functional Centre Total Direct Percentage (2) Total Costs (3) Costs to be Distributed (4)
Cost (1) A/IP CC OP A/IP CC OP A/IP CC OP 7*210 Medical 7*220 Surgical 7*230 Combined Medical/Surgical 7*240 Intensive Care 7*250 Obstetrics 7*260 Operating Room 7*262 OR/PARR Combined 7*265 Post-Anesthetic Recovery Room
7*270 Pediatric 7*276 Mental Health/Addictions 7*281 Rehabilitation 7*295 Long-Term Care 7*310 Emergency 7*320 Poison Information Centre 7*330 Tele-Health 7*340 Day/Night Care 7*350 Clinics 7*355 Private Clinics 7*410 Clinical Laboratory

TRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices h System Information Management and Investment Division h Data Branch
6.1 Page 25 of 53 2008 – March 2009 Updated August 2009
Calculation of Patient-Specific Cost Distribution Percentage (cont.) Functional Centre Total Direct Percentage (2) Total Costs (3) Costs to be Distributed (4) Cost (1) A/IP CC OP A/IP CC OP A/IP CC OP 7*415 Diagnostic Imaging 7*425 Electrodiagnosis 7*430 Non-Invasive Cardio and Vascular Laboratories
7*435 Respiratory Therapy 7*440 Pharmacy Drugs 7*440 Pharmacy Labour and Supplies 7*444 Combined Therapeutics 7*445 Clinical Nutrition 7*450 Physiotherapy 7*455 Occupational Therapy 7*460 Audiology & Speech/Lang Path 7*465 Rehabilitation Engineering 7*470 Social Work 7*472 Addiction Counselors 7*474 Genetics Counseling 7*475 Psychology and Psychometry 7*480 Pastoral Care 7*485 Recreation 7*490 Child Life 7*5 Community Services
Totals (5) Percentages to be Distributed (6)
Minimum Required Percentage to be Distributed 80 80 80*
MINISHealtHealt
OCCI Version Effective April
* Does not include day surgery Operating Room costs
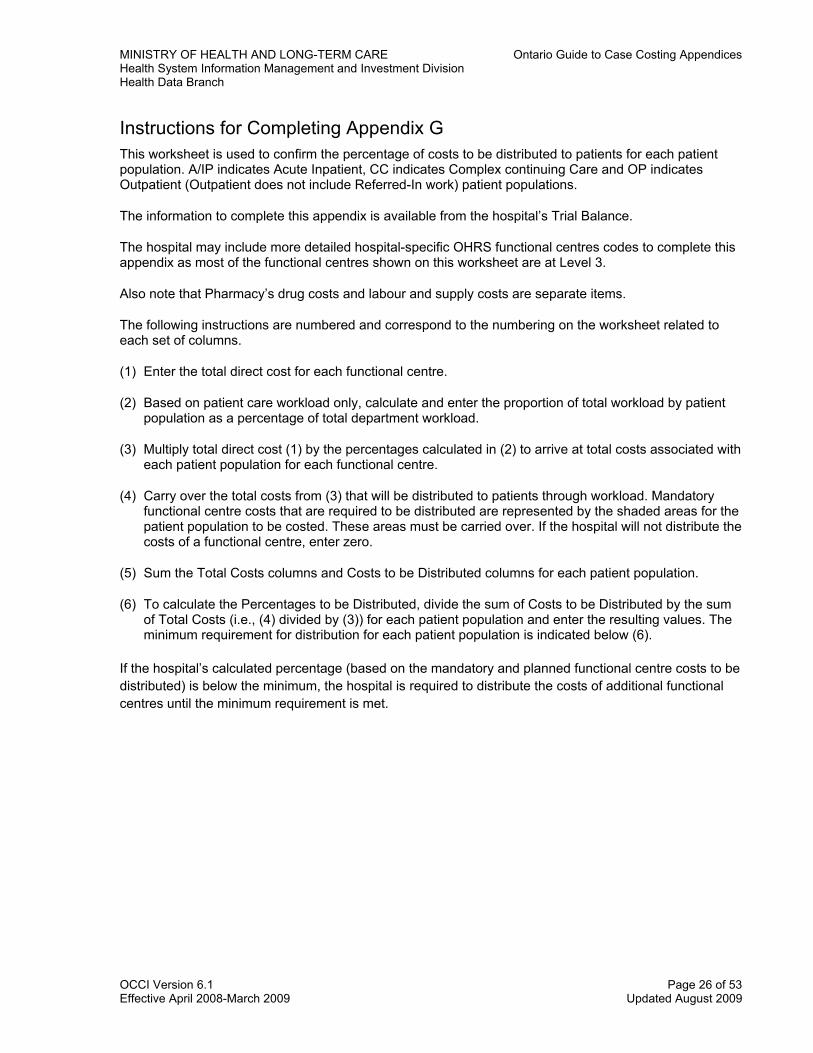
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Instructions for Completing Appendix G This worksheet is used to confirm the percentage of costs to be distributed to patients for each patient population. A/IP indicates Acute Inpatient, CC indicates Complex continuing Care and OP indicates Outpatient (Outpatient does not include Referred-In work) patient populations.
The information to complete this appendix is available from the hospital’s Trial Balance.
The hospital may include more detailed hospital-specific OHRS functional centres codes to complete this appendix as most of the functional centres shown on this worksheet are at Level 3.
Also note that Pharmacy’s drug costs and labour and supply costs are separate items.
The following instructions are numbered and correspond to the numbering on the worksheet related to each set of columns.
(1) Enter the total direct cost for each functional centre.
(2) Based on patient care workload only, calculate and enter the proportion of total workload by patient population as a percentage of total department workload.
(3) Multiply total direct cost (1) by the percentages calculated in (2) to arrive at total costs associated with each patient population for each functional centre.
(4) Carry over the total costs from (3) that will be distributed to patients through workload. Mandatory functional centre costs that are required to be distributed are represented by the shaded areas for the patient population to be costed. These areas must be carried over. If the hospital will not distribute the costs of a functional centre, enter zero.
(5) Sum the Total Costs columns and Costs to be Distributed columns for each patient population.
(6) To calculate the Percentages to be Distributed, divide the sum of Costs to be Distributed by the sum of Total Costs (i.e., (4) divided by (3)) for each patient population and enter the resulting values. The minimum requirement for distribution for each patient population is indicated below (6).
If the hospital’s calculated percentage (based on the mandatory and planned functional centre costs to be distributed) is below the minimum, the hospital is required to distribute the costs of additional functional centres until the minimum requirement is met.
OCCI Version 6.1 Page 26 of 53 Effective April 2008-March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix H: CIHI Acute Inpatient and Day Surgery Data Record Group # - Valid Values Attribute Name Format Field #
01-01 Province Number A,1 Per CIHI 01-02 Institution Number N,4 0000-9999 01-09 Chart Number A,10 Per CIHI 01-10 Register Number N,5 Per CIHI 01-11 Second Chart or Register Number N,7 Per CIHI 03-01 Health Care Number N,12 Per CIHI 03-02 Postal Code A,6 Per CIHI 03-03 Residence Code N,5 Per CIHI 03-04 Gender A,1 Per CIHI 03-07 Marital Status N,1 Per CIHI 03-08 Birthdate N,8 YYYYMMDD 03-09 Birthdate Is Estimated N,1 Per CIHI 04-01 Admission Date N,8 YYYYMMDD 04-02 Admission Hour N,2 Per CIHI 04-04 Institution From A,4 Per CIHI 04-05 Admission Category A,1 Per CIHI 04-06 Entry Code A,1 Per CIHI 04-07 Admit Via Ambulance A,1 Per CIHI 04-08 Readmission Code N,1 Per CIHI 04-09 Unplanned Readmission N,1 Per CIHI 04-10 Wait Time in Emergency Room N,4 Per CIHI 05-01 Discharge Date N,6 Per CIHI 05-02 Discharge Hour N,2 Per CIHI 05-04 Institution To A,4 Per CIHI 05-05 Date Ready For Discharge N,8
OCCI Version 6.1 Page 27 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Group # - Valid Values Attribute Name Format Field #
YYYMMDD 05-06 Reserve (optional) N,1 Per CIHI 06-01 Exit Alive Codes A,1 Per CIHI 06-02 Autopsy (optional) N,1 Per CIHI 06-03 Coroner/Medical Examiner (optional) N,1 Per CIHI 06-04 to 11 Death Codes A,1 Per CIHI 07-01 Main Patient Service N,2 Per CIHI 07-02 Main Patient Sub-Service (optional) N,1 Per CIHI 07-03 Weight N,4 Per CIHI 07-04 Abstract Overflow (optional) N,1 Per CIHI 08-01 Service Transfer Service N,2 Per CIHI 08-02 Service Transfer Sub-Service (optional) N,1 Per CIHI 08-03 Service Transfer Days (optional) N,5 Per CIHI 09-01 Doctor Type N,1 Per CIHI 09-02 Per CIHI Doctor Number N,5 09-03 Doctor Service N,2 Per CIHI Diagnoses 10-01 Diagnosis Prefix A,1 Per CIHI 10-02 Diagnosis Code A,5 ICD-10-CA 10-03 Diagnosis Suffix A,1 Per CIHI 10-04 Diagnosis Type A,1 Per CIHI Procedures 11-01 Procedure Date A,4 Per CIHI 11-02 Procedure Code A,4 ICD-10-CA 11-03 Procedure Suffix A,1 Per CIHI 11-04 Procedure Doctor Number (optional) A,5 Per CIHI 11-05 Procedure Doctor Service (optional) N,2 Per CIHI 11-06 Tissue Code (optional) N,1
OCCI Version 6.1 Page 28 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Group # - Valid Values Attribute Name Format Field #
Per CIHI 11-07 Procedure Time (optional) N,3 Per CIHI 11-08 Intervention Location Code (optional) N,2 Per CIHI 11-09 Anesthetist (optional) N,5 Per CIHI 11-10 Anesthetist Technique (optional) N,1 Per CIHI 11-11 Out of Hospital Institution No.(optional) N,4 Per CIHI 11-12 Unplanned Return to OR (optional) N,1 Per CIHI Therapeutic and Pre-Admission Information 12-01 to 06 Therapies N,1 Per CIHI 12-07 Discharge Planning N,1 Per CIHI 12-08 Social Services Per CIHI 12-09 Pre-Admission Work-up (optional) N,1 Per CIHI Special Care Units 13-01 SCU Death Indicator (optional) N,1 Per CIHI 13-02 SCU Unit Number (optional) N,2 Per CIHI 13-03 SCU Days (optional) N,2 Per CIHI Mental Health 15-02 Source of Referral N,1 Per CIHI 15-03 Method of Admission N,1 Per CIHI 15-04 Change in Legal Status From Admission N,1 Per CIHI 15-05 Absent Without Leave N,1 Per CIHI 15-06 Suicide N,1 Per CIHI 15-07 Previous Psychiatric Admission N,1 Per CIHI 15-08 Referred To N,1 Per CIHI 15-09 ECT Treatment N,1 Per CIHI 15-10 Number of ECT Treatments N,2 Per CIHI 15-12 Education N,1 Per CIHI 15-13 Employment Status N,1 Per CIHI 15-14 Financial Support N,1
OCCI Version 6.1 Page 29 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Group # - Valid Values Attribute Name Format Field #
Per CIHI Blood Information 17-01 Blood Transfusion Indicator A,1 Per CIHI 17-02 to 06 Blood Products A,1 Per CIHI 17-07 Auto Transfusion A,1 Per CIHI Therapeutic Abortion Information 18-01 Number of Previous Deliveries N,1 Per CIHI 18-02 Number of Previous Spontaneous Abortions N,1 Per CIHI 18-03 Number of Previous Induced Abortions N,1 Per CIHI 18-04 Clinical Gestation in Weeks N,2 Per CIHI 18-05 Date of Last Menses N,8 YYYYMMDD CIHI-GENERATED DATA DPG Number N,2 01-99 DPG Weight N,8.4 MCC Code N,2 01-25,99 Complexity CMG Code N,3 001-999 Complexity Grade List Indicator N,1 1,3,9 Complexity Level N,1 1-4, 9 Complexity Age Category N,1 1-3,9 Complexity ELOS N,5 N,5 CIHI RIW Exclusion Indicator N,1 0-9 CIHI Complexity RIW Value N,8.4 Provincial RIW Exclusion Indicator N,1 0-9 Provincial Complexity RIW Value N,8.4
OCCI Version 6.1 Page 30 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix I: Ambulatory Care Costing Patient Descriptive Minimum Data Set Bolded data elements indicate grouping variable. Core Mandatory Data Elements Type Data Element
Demographic 1. Chart Number 2. Postal Code 3. Gender 4. Birth date
Administrative 5. Visit MIS Functional Centre Code 6. Date of Visit
Clinical 7. Provider Type(s) 8. Primary Provider Type 9. Provider Identification Number 10. Visit Disposition 11. Main Problem 12. Other Problem(s) 13. External Cause of Injury/Poisoning 14. Main Intervention 15. Other Intervention(s)
Service Specific Mandatory Data Elements Service Data Element
ER/Day Surgery 16. Triage level 17. Date Visit Completed 18. Registration Time 19. Disposition Time
Other Data Elements 20. Encounter Number 21. Mode of Visit/Contact 22. Blood Transfused 23. Blood Components/Products
Provincially Defined 24. Geographic Code
OCCI Version 6.1 Page 31 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix J: Indirect Cost Allocation Methodology The Simultaneous Equation Allocation Methodology (SEAM) is the OCCI standard method for indirect cost allocation.
SEAM uses a series of linear algebraic equations to allocate the costs of the Administrative and Support functional centres to the patient care functional centres. These overhead functional centres, or transient cost centres (TCCs), do not contribute directly to the “product,” but they provide essential auxiliary support to the patient care or absorbing cost centres (ACCs). To calculate the percentage of indirect costs that go to each patient care functional centre, SEAM uses the allocation bases listed in Appendix K.
SEAM has been shown to be the best available method for case cost development. It is one of several approaches that have been developed to solve what is known as the “reciprocal service allocation problem.” This problem exists because the Administrative and Support functional centres provide services to each other. SEAM resolves this problem by allocating a portion of the TCC costs to other TCCs as well as to the ACCs, and then allocating all the TCC direct and indirect costs to all the ACCs as indirect costs simultaneously.
Example of SEAM calculation SEAM solves a set of linear equations to reallocate all the overhead functional centre costs simultaneously to other overhead functional centres (TCCs) and patient care functional centres (ACCs). A linear algebraic equation is developed for each functional centre which represents the total or full functional centre costs—direct and indirect costs. The indirect costs are the reassigned costs from the TCCs.
To illustrate the SEAM calculations with a simplified example, let us assume that a hospital has two transient cost centres, T1 and T2, that provide services to each other and to the hospital’s two absorbing cost centres, A1 and A2, with the following percentages:
Services provided from
Services provided to Total
T1 T2 A1 A2 T1 - 10% 40% 50% 100% T2 20% - 50% 30% 100%
OCCI Version 6.1 Page 32 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
The total costs charged to each functional centre are as follows:
T1 $ 30,000 T2 $ 20,000 A1 $200,000 A2 $100,000
The algebraic expression developed to represent the total costs for each cost centre:
T1 = 30,000 + 0.20 T2 T2 = 20,000 + 0.10 T1 A1 = 200,000 + 0.40 T1 + 0.50 T2 A2 = 100,000 + 0.50 T1 + 0.30 T2
Using substitution to solve the equation for each cost centre, we start by substituting the equation of T2 into T1:
T1 = 30,000 + 0.20(20,000 + 0.10 T1) T1 = 30,000 + 4,000 + 0.02 T1 0.98 T1 = 34,000 T1 = 34,694
Substituting the solution of T1 into the equation for T2:
T2 = 20,000 + 0.10(34,694) T2 = 20,000 + 3,469 T2 = 23,469
Finally substituting the solutions of T1 and T2 into A1:
A1 = 200,000 + 0.40(34,694) + 0.50(23,469) A1 = 200,000 + 13,878 + 11,735 A1 = 225,612
And substituting the solutions of T1 and T2 into A2:
A2 = 100,000 + 0.50(34,694) + 0.30(23,469) A2 = 100,000 + 17,347 + 7,041 A2 = 124,388
The final amounts in the ACCs represent the functional centre’s direct costs plus the proportion of indirect costs allocated from each TCC. The following table summarizes the resulting cost reassignments of the cost centres:
T1 T2 A1 A2 Total Costs before allocation $30,000 $20,000 $200,000 $100,000 $350,000 T1 allocation (34,694) 3,469 13,878 17,347 T2 allocation 4,694 (23,469) 11,735 7,041 Costs after allocation - - $225,612 $124,388 $350,000 Other methods for reassigning overhead costs Two other methods for reassigning overhead costs are the direct method and the step approach. A brief description of each method is provided here to illustrate the benefits of SEAM. A significant advantage to using SEAM over these methods is that SEAM takes into account the interaction of the TCCs with each other.
OCCI Version 6.1 Page 33 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
The direct method allocates overhead costs directly to the ACCs without consideration of the interdependence between TCCs. The exclusion of interdepartmental allocation is acceptable only if each overhead cost centre is providing approximately the same level of services to all the ACCs.
The step method reassigns TCC costs with some recognition of interdepartmental services. This method requires that management determine which TCC provides the most interdepartmental services. The costs of this TCC are then reassigned to the other TCCs and ACCs. This first TCC to be allocated does not receive any other TCC costs. The costs of the second TCC are reassigned in the same manner, having received indirect costs from only the first TCC. The TCC reassigned last will have had costs reassigned to it from all the other TCCs and will be allocated only to the ACCs. The reassignment of costs is based on the allocation statistics for only those cost centres to which that TCCs costs are allocated.
There is no generally accepted rule for determining the order for reassigning the TCC in the step method. The first TCC is chosen as the one that provides the most services to the other TCCs. The other TCCs follow in order based on their relative levels of interdepartmental services.
SEAM has proven to be the best available way to deal with the interrelationships between Administrative and Support functional centres. One potential advantage over the other methods is that the source and amount of administrative and support functional centre costs allocated to patient care functional centres can be identified. In addition, the cost results have much greater reliability since the method does not depend on a consistent order used to process records in the computation from hospital to hospital, and can be adjusted as a hospital’s activities change.
OCCI Version 6.1 Page 34 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix K: Transient Cost Centre Allocation Methodology Table Note: The asterisk * in the 2nd digit of functional center code indicates fund type. The OCCI includes fund types 1, 2 and 3. Functional Center Code
Transient Functional Centre Name Cost Allocation Numerator Cost Allocation Denominator
7*110 General Administration Department Total Costs Hospital Total Costs 10 Executive Offices Department Total Costs Hospital Total Costs 25 Utilization Management Department Total Costs Hospital Total Costs 30 Board of Trustees Department Total Costs Hospital Total Costs 40 Public Relations Department Total Costs Hospital Total Costs 50 Planning & Development Department Total Costs Hospital Total Costs 53 Privacy Officer Department Total Costs Hospital Total Costs 55 Risk Management Department Total Costs Hospital Total Costs 60 Quality Assurance Department Total Costs Hospital Total Costs 70 Internal Audit Department Total Costs Hospital Total Costs 90 French Language Services Department Total Costs Hospital Total Costs 7*115 Finance Department Total Costs Hospital Total Costs 10 General Accounting Department Total Costs Hospital Total Costs 20 Payroll Department Earned Hours Hospital Total Earned Hours 30 Accounts Receivable Department Total Costs Hospital Total Costs 40 Accounts Payable Department Total Costs Hospital Total Costs 50 Budget Control Department Total Costs Hospital Total Costs 60 Case Costing Department Total Costs Hospital Total Costs 7*120 Human Resources Department Earned Hours Hospital Total Earned Hours 20 Personnel Records Department Earned Hours Hospital Total Earned Hours
30 Employee Comp. and Benefits Mgmt Department Earned Hours Hospital Total Earned Hours
40 Labour Relations Department Earned Hours Hospital Total Earned Hours 60 Employee Health Department Earned Hours Hospital Total Earned Hours
80 Employee Assistance programs Department Earned Hours Hospital Total Earned Hours
90 Occupational Health and Safety Department Earned Hours Hospital Total Earned Hours
7*125 Information Systems Support Department Total Costs Hospital Total Costs
20 Data Processing Department Total Costs Hospital Total Costs 40 Systems Engineering Department Total Costs Hospital Total Costs
50 Implementation and Maintenance Department Total Costs Hospital Total Costs
7*130 Communications Department Total Costs Hospital Total Costs 20 Telecommunications Department Total Costs Hospital Total Costs 40 Visitor Information Department Total Costs Hospital Total Costs 60 Mail Service Department Total Costs Hospital Total Costs
7*135 Material Management Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
05 Administration
10 Purchasing Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
15 Capital Asset Control Dept Amortization Expense Total Amortization Expense
OCCI Version 6.1 Page 35 of 53 Effective April 2008 – March 2009 Updated August 2009
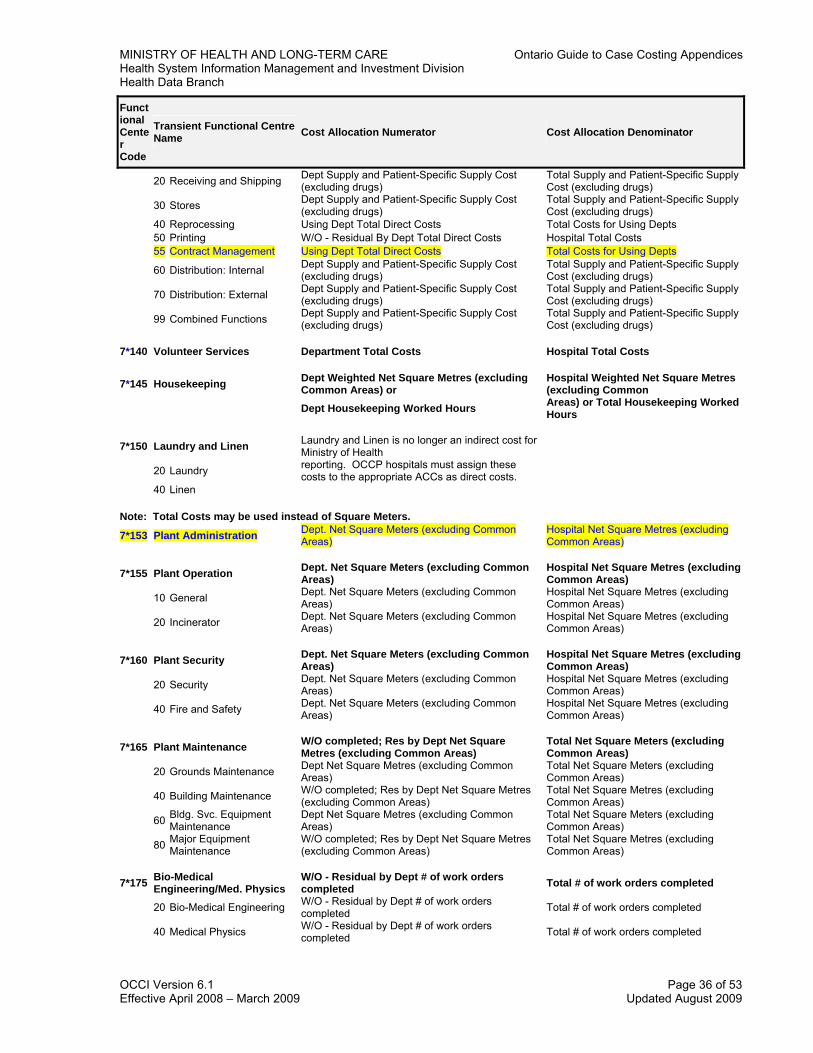
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Functional Center Code
Transient Functional Centre Cost Allocation Numerator Cost Allocation Denominator Name
20 Receiving and Shipping Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
30 Stores Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
40 Reprocessing Using Dept Total Direct Costs Total Costs for Using Depts 50 Printing W/O - Residual By Dept Total Direct Costs Hospital Total Costs 55 Contract Management Using Dept Total Direct Costs Total Costs for Using Depts
60 Distribution: Internal Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
70 Distribution: External Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
99 Combined Functions Dept Supply and Patient-Specific Supply Cost (excluding drugs)
Total Supply and Patient-Specific Supply Cost (excluding drugs)
7*140 Volunteer Services Department Total Costs Hospital Total Costs
7*145 Housekeeping Dept Weighted Net Square Metres (excluding Common Areas) or
Hospital Weighted Net Square Metres (excluding Common
Dept Housekeeping Worked Hours Areas) or Total Housekeeping Worked Hours
7*150 Laundry and Linen Laundry and Linen is no longer an indirect cost for Ministry of Health
20 Laundry reporting. OCCP hospitals must assign these costs to the appropriate ACCs as direct costs.
40 Linen Note: Total Costs may be used instead of Square Meters.
7*153 Plant Administration Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
7*155 Plant Operation Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
10 General Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
20 Incinerator Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
7*160 Plant Security Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
20 Security Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
40 Fire and Safety Dept. Net Square Meters (excluding Common Areas)
Hospital Net Square Metres (excluding Common Areas)
7*165 Plant Maintenance W/O completed; Res by Dept Net Square Metres (excluding Common Areas)
Total Net Square Meters (excluding Common Areas)
20 Grounds Maintenance Dept Net Square Metres (excluding Common Areas)
Total Net Square Meters (excluding Common Areas)
40 Building Maintenance W/O completed; Res by Dept Net Square Metres (excluding Common Areas)
Total Net Square Metres (excluding Common Areas)
60 Bldg. Svc. Equipment Maintenance
Dept Net Square Metres (excluding Common Areas)
Total Net Square Meters (excluding Common Areas)
80 Major Equipment Maintenance
W/O completed; Res by Dept Net Square Metres (excluding Common Areas)
Total Net Square Metres (excluding Common Areas)
7*175 Bio-Medical Engineering/Med. Physics
W/O - Residual by Dept # of work orders completed Total # of work orders completed
20 Bio-Medical Engineering W/O - Residual by Dept # of work orders completed Total # of work orders completed
40 Medical Physics W/O - Residual by Dept # of work orders completed Total # of work orders completed
OCCI Version 6.1 Page 36 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Functional Center Code
Transient Functional Centre Cost Allocation Numerator Cost Allocation Denominator Name
7*179 Interpretation/Translation Department Total Costs Hospital Total Costs
7*180 Registration (Admitting) Split costs by IP/Res/Client, then allocate by Dept Hospital Registrations Completed
Total Hospital Registrations Completed
20 Inpatient Registration Dept Inpatient/Resident Registrations Completed Total Inpatient/Resident Registrations Completed
40 Outpatient Registration Outpatient Dept Registrations Completed Total Outpatient Registrations Completed 60 Emergency Registration Emergency Registrations Total Emergency Registrations
80 Centralized Booking Split costs by IP/Resident/OP, then by Dept # of appointments scheduled Total # of Appointments Scheduled
7*182 Case Management Coordination Dept. Service Recipients Seen Total Service Recipients Seen
10 Admission Dept. Service Recipients Seen Total Service Recipients Seen 20 Discharge Dept. Service Recipients Seen Total Service Recipients Seen 7*185 Patient Transport Using Dept Total Costs Total Costs of Using Depts 20 Central Patient Portering Using Dept Total Costs Total Costs of Using Depts 40 External Patient Transport Using Dept Total Costs Total Costs of Using Depts
7*186 Non Service Recipient Transport Dept Total Costs Hospital Total Costs
Note: Patient Hours may be used instead of NWMS (nursing workload). Note: NWMS units may be used instead of # Separations/Visits for Health Records Functional Centres
7*190 Health Records Split costs by IP/Resident/OP, then allocate by Dept Health Records Processed Total Health Records Processed
05 Administration Split costs by IP/Resident/OP, then allocate by Dept Health Records Processed Total Health Records Processed
20 Transcription Split costs by IP/Resident/OP, then allocate by Dept Transcription Lines Processed Total Transcription Lines Processed
10 Medical Transcription NWMS Units for Department Total Functional Centre NWMS Units
20 Non-Medical Transcription NWMS Units for Department Total Functional Centre NWMS Units
40 Record Processing Split costs by IP/Resident/OP, then allocate by Dept Health Records Processed Total Health Records Processed
10 Clerical Record Processing NWMS Units for Department Total Functional Centre NWMS Units
20 Data Collection NWMS Units for Department Total Functional Centre NWMS Units
30 Release of Patient Information NWMS Units for Department Total Functional Centre NWMS Units
60 Health Data and information Services
Split costs by IP/Resident/OP, then allocate by Dept Health Records Processed Total Health Records Processed
Education 7*810 Hospital Library Using Dept Total Costs Total Costs of Using Depts 7*820 Audiovisual Using Dept Total Costs Total Costs of Using Depts 7*830 Medical Illustration Using Dept Total Costs Total Costs of Using Depts 7*840 In-Service Education Using Dept Total Costs Total Costs of Using Depts Selected Undistributed Accounting Centers
OCCI Version 6.1 Page 37 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Functional Center Code
Transient Functional Centre Cost Allocation Numerator Cost Allocation Denominator Name
8*955 Interest on Long Term Liabilities Using Dept Total Costs Hospital Total Costs
8*960 Municipal Taxes Using Dept Total Costs Hospital Total Costs 8*965 Employee Future Benefits Departmental Earned Hours Hospital Total Earned Hours
8*990 Other Undistributed Expenses – Operating (Including NEER Penalities)
Department Total Costs Hospital Total Costs
8*995 Employee Benefits Debit Clearing Account Departmental Earned Hours Hospital Total Earned Hours
8*996 Employee Benefits Credit Clearing Account Departmental Earned Hours Hospital Total Earned Hours
8*945 NEER Rebate Department Total Costs Hospital Total Costs NOTES
• Patient Food Services Costs in FC 71195 are classified as direct costs in OCCI. • Inclusion of the selected accounting centers is a methodological change, effective April 1st, 2004. • W/O - Most of the TCC's costs are to be distributed to departments receiving service from this TCC based on a costed
Work Order. Any undistributed costs at period end are allocated using the Cost Allocation Numerator and Denominator.
OCCI Version 6.1 Page 38 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix L: OCCI Case Cost Record Attribute
Number + Record
Location
Attribute Name Format Valid Values Description or Comments
Core Costing Data Elements C01-1 Institution ID A,4.0 0000-9999 Must match patient description
record submitted to CIHI by the hospital
C02-5 Chart Number A,10.0 per CIHI Must match patient description record submitted to CIHI by the hospital
C03-15 Register/Account Number A,12.0 per CIHI Must match patient description record submitted to CIHI by the hospital
C04-27 -- Reserved/Blank A,3.0 Unused area, leave blank
C04-30 Admission Date or Date of Registration
A,8.0 YYYYMMDD Must match patient description record submitted to CIHI
C05-38 Discharge Date A,8.0 YYYYMMDD Must match patient description record submitted to CIHI.
C06-46 Functional Center Code OHRS Level 3
A,5.0 OHRS compliant functional centre codes V6.2
C06A-51 OHRS Level 4 A,2.0 00-99 Please put zeroes instead of blanks
C06B-53 OHRS Level 5 A,2.0 00-99 Please put zeroes instead of blanks
C07-55 Date of Service A,8.0 YYYYMMDD C08-638 Variable Direct Labour $ N,9.2 000000.00 -
999999.00 Leading zeroes are permitted
C09-72 Variable Direct Supplies $ – Patient Specific
N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C010-81 Variable Direct Supplies $ – General
N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C11-90 Variable Direct Other $ N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C12-99 Fixed Direct Labour $ N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C13108 Fixed Direct Other $ N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C14-117 Fixed Direct Equipment $ N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C15-126 Indirect Variable Cost $ N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C16-135 Indirect Fixed Cost $ N,9.2 000000.00 - 999999.00
Leading zeroes are permitted
C17-144 Classification as assigned by hospital
A,3.0 valid grouper code
Patient classification assignment.
ALL FIELDS ARE TO BE RIGHT JUSTIFIED
OCCI Version 6.1 Page 39 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Note:
• In the Attribute Number field: i.e.: C02-5 C = Column 02 = second column from left 5 = starts at character/byte 5
• Format indicates the type and size of a variable: N = Numeric A= Alphanumeric Size: 4 = 9999 9.2 = 999999.99
OCCI Version 6.1 Page 40 of 53 Effective April 2008 – March 2009 Updated August 2009
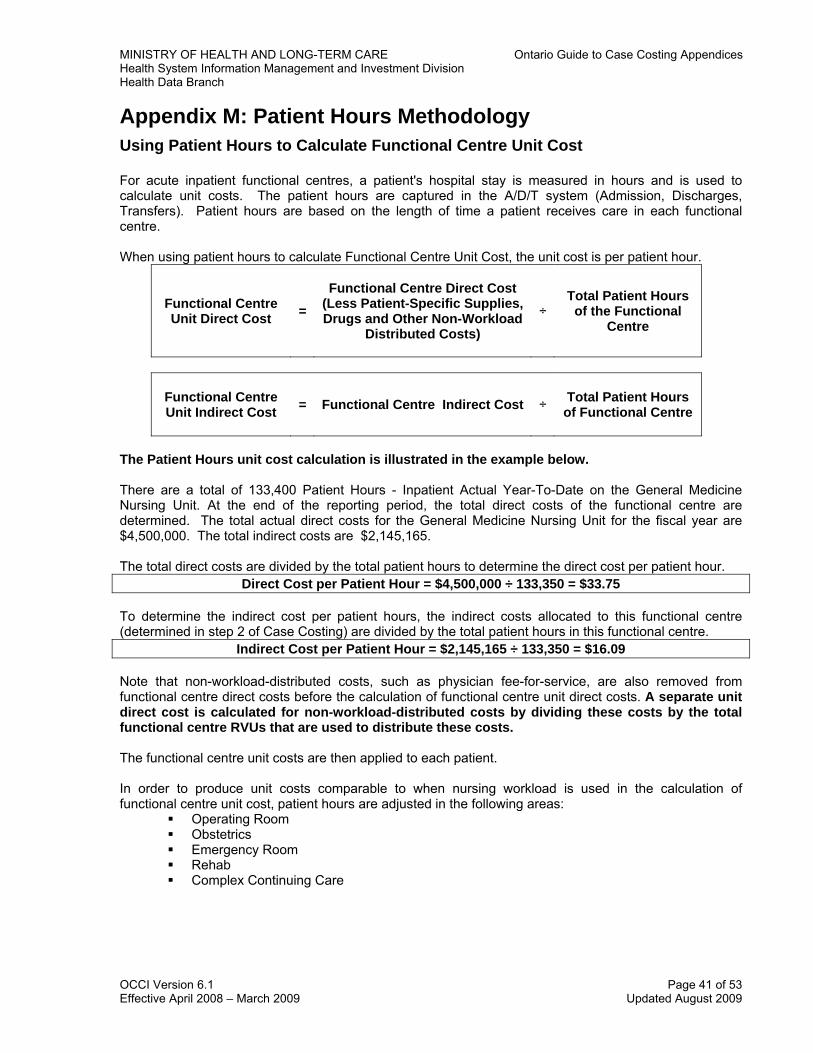
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix M: Patient Hours Methodology Using Patient Hours to Calculate Functional Centre Unit Cost For acute inpatient functional centres, a patient's hospital stay is measured in hours and is used to calculate unit costs. The patient hours are captured in the A/D/T system (Admission, Discharges, Transfers). Patient hours are based on the length of time a patient receives care in each functional centre. When using patient hours to calculate Functional Centre Unit Cost, the unit cost is per patient hour.
Functional Centre Unit Direct Cost =
Functional Centre Direct Cost (Less Patient-Specific Supplies, Drugs and Other Non-Workload
Distributed Costs) ÷
Total Patient Hours of the Functional
Centre
Functional Centre Unit Indirect Cost = Functional Centre Indirect Cost ÷ Total Patient Hours
of Functional Centre
The Patient Hours unit cost calculation is illustrated in the example below. There are a total of 133,400 Patient Hours - Inpatient Actual Year-To-Date on the General Medicine Nursing Unit. At the end of the reporting period, the total direct costs of the functional centre are determined. The total actual direct costs for the General Medicine Nursing Unit for the fiscal year are $4,500,000. The total indirect costs are $2,145,165. The total direct costs are divided by the total patient hours to determine the direct cost per patient hour.
Direct Cost per Patient Hour = $4,500,000 ÷ 133,350 = $33.75 To determine the indirect cost per patient hours, the indirect costs allocated to this functional centre (determined in step 2 of Case Costing) are divided by the total patient hours in this functional centre.
Indirect Cost per Patient Hour = $2,145,165 ÷ 133,350 = $16.09 Note that non-workload-distributed costs, such as physician fee-for-service, are also removed from functional centre direct costs before the calculation of functional centre unit direct costs. A separate unit direct cost is calculated for non-workload-distributed costs by dividing these costs by the total functional centre RVUs that are used to distribute these costs. The functional centre unit costs are then applied to each patient. In order to produce unit costs comparable to when nursing workload is used in the calculation of functional centre unit cost, patient hours are adjusted in the following areas:
Operating Room Obstetrics Emergency Room Rehab Complex Continuing Care
OCCI Version 6.1 Page 41 of 53 Effective April 2008 – March 2009 Updated August 2009
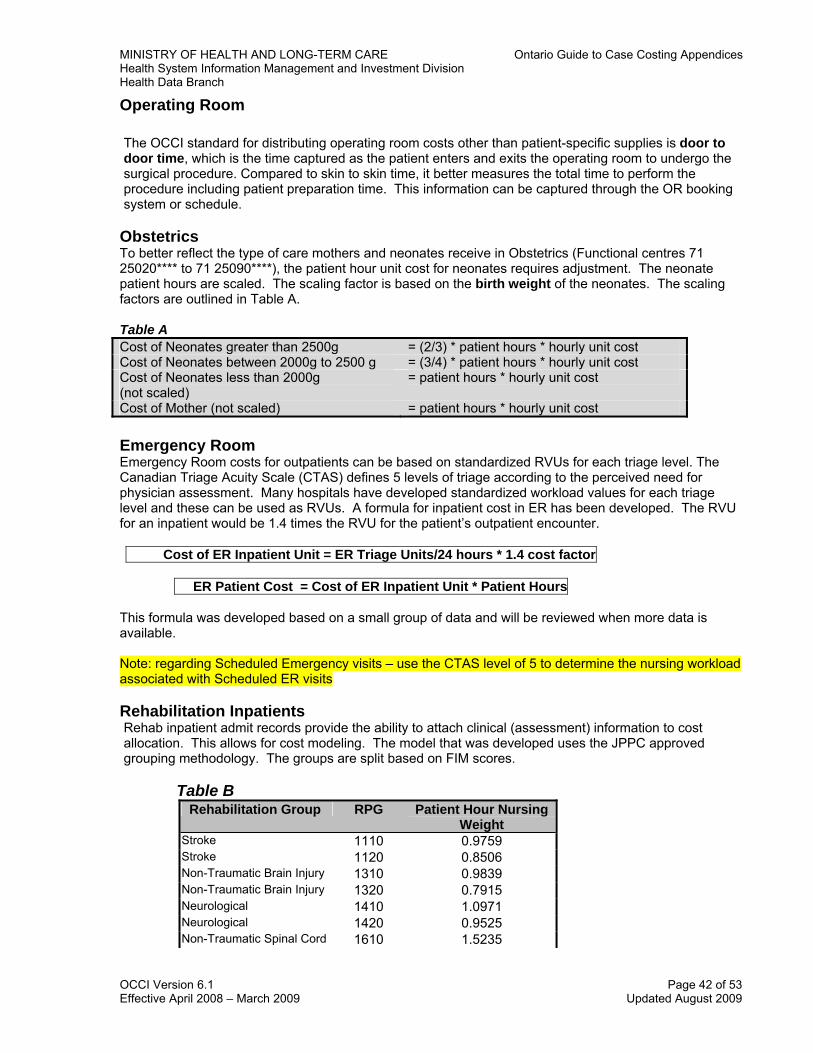
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Operating Room The OCCI standard for distributing operating room costs other than patient-specific supplies is door to door time, which is the time captured as the patient enters and exits the operating room to undergo the surgical procedure. Compared to skin to skin time, it better measures the total time to perform the procedure including patient preparation time. This information can be captured through the OR booking system or schedule.
Obstetrics To better reflect the type of care mothers and neonates receive in Obstetrics (Functional centres 71 25020**** to 71 25090****), the patient hour unit cost for neonates requires adjustment. The neonate patient hours are scaled. The scaling factor is based on the birth weight of the neonates. The scaling factors are outlined in Table A. Table A Cost of Neonates greater than 2500g = (2/3) * patient hours * hourly unit cost Cost of Neonates between 2000g to 2500 g = (3/4) * patient hours * hourly unit cost Cost of Neonates less than 2000g (not scaled)
= patient hours * hourly unit cost
Cost of Mother (not scaled) = patient hours * hourly unit cost Emergency Room Emergency Room costs for outpatients can be based on standardized RVUs for each triage level. The Canadian Triage Acuity Scale (CTAS) defines 5 levels of triage according to the perceived need for physician assessment. Many hospitals have developed standardized workload values for each triage level and these can be used as RVUs. A formula for inpatient cost in ER has been developed. The RVU for an inpatient would be 1.4 times the RVU for the patient’s outpatient encounter.
Cost of ER Inpatient Unit = ER Triage Units/24 hours * 1.4 cost factor
ER Patient Cost = Cost of ER Inpatient Unit * Patient Hours
This formula was developed based on a small group of data and will be reviewed when more data is available. Note: regarding Scheduled Emergency visits – use the CTAS level of 5 to determine the nursing workload associated with Scheduled ER visits Rehabilitation Inpatients Rehab inpatient admit records provide the ability to attach clinical (assessment) information to cost allocation. This allows for cost modeling. The model that was developed uses the JPPC approved grouping methodology. The groups are split based on FIM scores.
Table B Rehabilitation Group RPG Patient Hour Nursing
Weight Stroke 1110 0.9759 Stroke 1120 0.8506 Non-Traumatic Brain Injury 1310 0.9839 Non-Traumatic Brain Injury 1320 0.7915 Neurological 1410 1.0971 Neurological 1420 0.9525 Non-Traumatic Spinal Cord 1610 1.5235
OCCI Version 6.1 Page 42 of 53 Effective April 2008 – March 2009 Updated August 2009
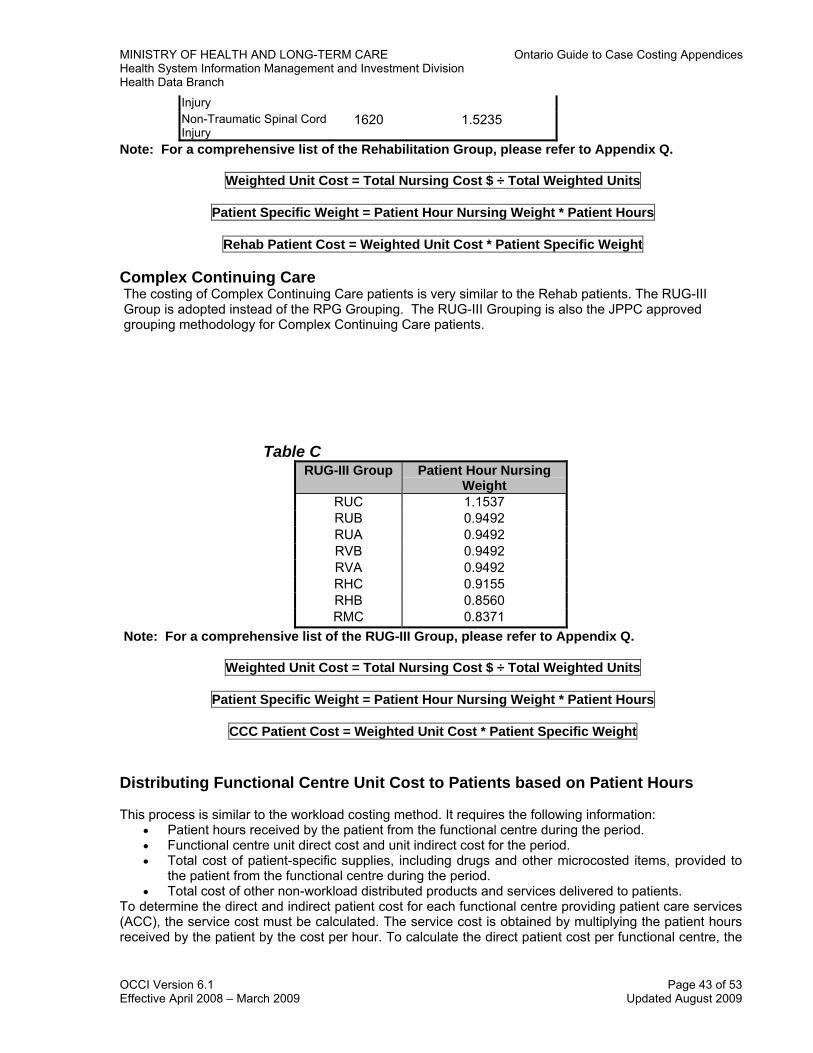
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Injury Non-Traumatic Spinal Cord Injury
1620 1.5235
Note: For a comprehensive list of the Rehabilitation Group, please refer to Appendix Q.
Weighted Unit Cost = Total Nursing Cost $ ÷ Total Weighted Units
Patient Specific Weight = Patient Hour Nursing Weight * Patient Hours
Rehab Patient Cost = Weighted Unit Cost * Patient Specific Weight Complex Continuing Care The costing of Complex Continuing Care patients is very similar to the Rehab patients. The RUG-III Group is adopted instead of the RPG Grouping. The RUG-III Grouping is also the JPPC approved grouping methodology for Complex Continuing Care patients.
Table C
RUG-III Group Patient Hour Nursing Weight
RUC 1.1537 RUB 0.9492 RUA 0.9492 RVB 0.9492 RVA 0.9492 RHC 0.9155 RHB 0.8560 RMC 0.8371
Note: For a comprehensive list of the RUG-III Group, please refer to Appendix Q.
Weighted Unit Cost = Total Nursing Cost $ ÷ Total Weighted Units
Patient Specific Weight = Patient Hour Nursing Weight * Patient Hours
CCC Patient Cost = Weighted Unit Cost * Patient Specific Weight Distributing Functional Centre Unit Cost to Patients based on Patient Hours This process is similar to the workload costing method. It requires the following information:
• Patient hours received by the patient from the functional centre during the period. • Functional centre unit direct cost and unit indirect cost for the period. • Total cost of patient-specific supplies, including drugs and other microcosted items, provided to
the patient from the functional centre during the period. • Total cost of other non-workload distributed products and services delivered to patients.
To determine the direct and indirect patient cost for each functional centre providing patient care services (ACC), the service cost must be calculated. The service cost is obtained by multiplying the patient hours received by the patient by the cost per hour. To calculate the direct patient cost per functional centre, the
OCCI Version 6.1 Page 43 of 53 Effective April 2008 – March 2009 Updated August 2009
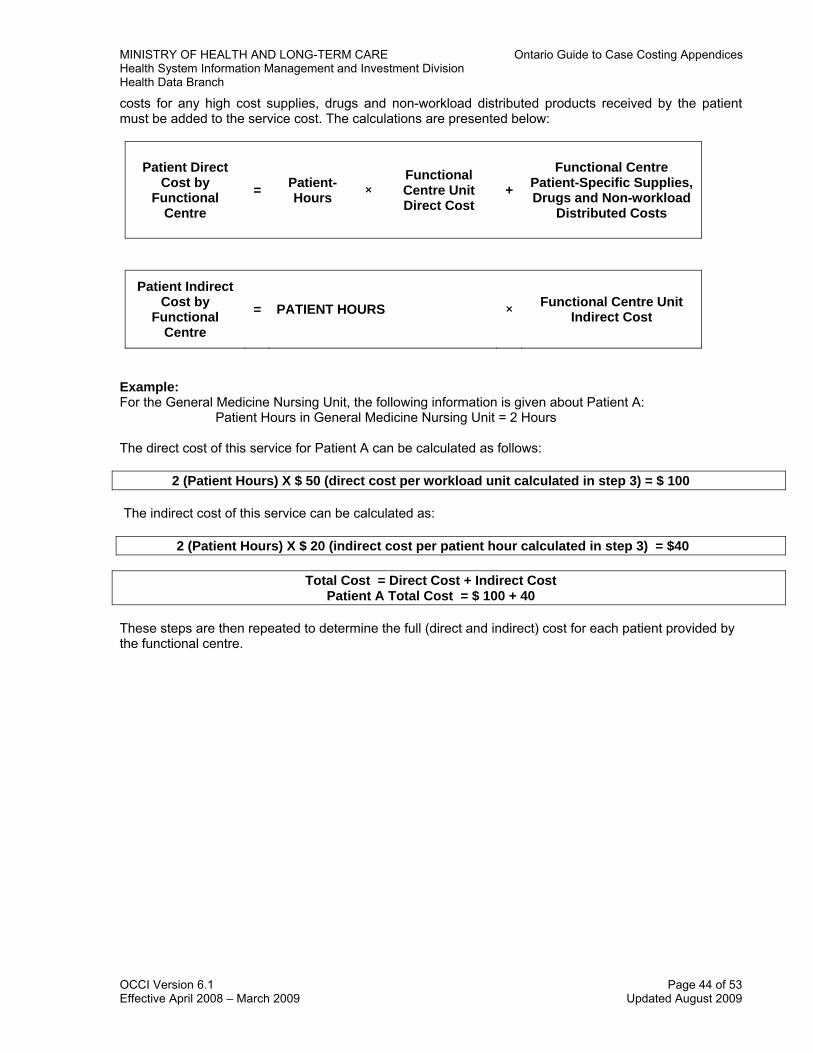
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
costs for any high cost supplies, drugs and non-workload distributed products received by the patient must be added to the service cost. The calculations are presented below:
Patient Direct Cost by
Functional Centre
= Patient- Hours ×
Functional Centre Unit Direct Cost
+
Functional Centre Patient-Specific Supplies, Drugs and Non-workload
Distributed Costs
Patient Indirect Cost by
Functional Centre
= PATIENT HOURS × Functional Centre Unit Indirect Cost
Example: For the General Medicine Nursing Unit, the following information is given about Patient A: Patient Hours in General Medicine Nursing Unit = 2 Hours The direct cost of this service for Patient A can be calculated as follows:
2 (Patient Hours) X $ 50 (direct cost per workload unit calculated in step 3) = $ 100 The indirect cost of this service can be calculated as:
2 (Patient Hours) X $ 20 (indirect cost per patient hour calculated in step 3) = $40
Total Cost = Direct Cost + Indirect Cost Patient A Total Cost = $ 100 + 40
These steps are then repeated to determine the full (direct and indirect) cost for each patient provided by the functional centre.
OCCI Version 6.1 Page 44 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix N: Case Costing System Requirements Information systems make case costing possible, practical and effective. Information systems and information systems staff play a key role in the implementation and sustained operation of a case costing system. In addition, information systems are a central focus of MIS implementation. Information systems are covered more extensively in the MIS Standards. Here we provide an example of some features and capabilities that are important in a departmental system for case costing. Input to Departmental Systems and Case Costing System
• Linked with Admission/Discharge/Transfer (A/D/T) System for patient identification number, encounter number and Patient Hours in each functional centre
• Can record procedure and workload for patient • Can record patient-specific supplies and other expenses to the patient • Can identify specific procedures and workload to specific functional centres
Output from Departmental Systems
• The format of the source data (e.g., Nursing, Operating Room, Health Records) should be examined to determine the optimal method of transferring data to the case costing system
Output from Case Costing Systems
• The capability for summary analysis of costs associated with patients • The capability to list patient-specific utilization and costs
Tracking
• The ability to track patients from admission to discharge • The ability to track patient demographics, clinical and resource utilization and case costs for
patients
Querying Tools • Data querying tools should be based on a relational database in which information is stored in
tables that relate to each other by user-defined queries, allowing efficient and accurate storage and retrieval
Audit Reports
• To ensure that what is passing to the costing system is the desired information • Should enhance the validation process and improve data integrity checks • Data quality checks should occur at the source data level and at the case costing system level
Stand Alone System
• Make sure you can enter and retrieve specific information at the patient level
Batch/real time • Make sure patient information is available on system when required • Ensure that data can be archived, rather than purged, to free up space
Other
• Patient billings • Check requirements (if any) of Case Costing System operating system • Have users assess user friendliness • Table driven system (relational) with user-maintained tables for workload values
OCCI Version 6.1 Page 45 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Vendors
• Follow RFP procedures • Be specific in questions • Usability, functionality and supplier capabilities are critical • Insist on demonstration and documented proof of performance • Selection team should be balanced with ‘technology enthusiasts’ and ‘healthy skeptics’ • Obtain references
OCCI Version 6.1 Page 46 of 53 Effective April 2008 – March 2009 Updated August 2009
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix O: OCCI Milestone Reviews All hospitals participating in the Ontario Case Cost Initiative undergo four Milestone reviews. The objectives of the reviews are:
• Educating hospital participants • Monitoring hospital progress • Minimizing reliability and validity error • Identifying corrective action if the hospital is not on track • Ensuring compliance with the OCCI costing methodology • Hospital payment
The reviews take place throughout the planning, development and implementation of hospital case costing systems to examine the capture, interface and processing of data. Criteria have been developed to ensure that hospitals adhere to the case costing standards. A variety of techniques are used including site visits, interviews, reconciliation and data analysis.
The following presents a brief summary of each Milestone review. Milestone 1 – Building Blocks The main objective of this initial review is to review and assess the status of the hospital in terms of planning and development of the required case costing systems. The review takes place at the onset of the planning stages.
The review involves a site visit to the hospital. Interviews are conducted with representatives of Finance, Information Systems, Health Records, Nursing, Laboratories, Diagnostic Imaging, Pharmacy and Allied Health (e.g., Physiotherapy). The Information Management Coordinators are the OCCI representatives and will review the status of the existing and planned procedures and mechanisms to capture all necessary data and ensure compliance with case costing standards.
Milestone 2 – Pre-Go-Live Check The review takes place approximately one to two months before the hospital goes live with collecting patient-specific data. The goal of the review is to examine the data capture, data interface and data quality mechanisms to ensure reliable and valid data from each of the components of the case costing system.
The review consists of a site visit. Interviews are conducted with front line staff and departmental representatives to ensure all is ready. Milestone 3 – Three Months Test Data This review is completed in two phases. Phase 1 consists of a site visit and takes place approximately three months after the hospital has gone live with the costing system. During the visit, Information Management Coordinator conducts reconciliation between the data from various feeder systems and the costing system. The costing system is analyzed to ensure accuracy, consistency and comprehensiveness of data collection for the three months of data. The hospital is to address all issues identified prior to submitting the data for Phase 2. Phase 2 of the Milestone 3 review involves a statistical review of the first three months of test data. The hospital cost data is brought together with the corresponding discharge abstract from CIHI. The data is analyzed for any irregularities that may indicate systematic problems in the case costing system and/or deviations from the case costing standards. For example, all cases with missing Nursing costs are identified. Hospitals are required to resolve all issues identified from both phases before submitting the full year of data.
OCCI Version 6.1 Page 47 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Milestone 4 – One Full Year of Data The Milestone 4 review consists of an analysis of one year of case cost data. The review methodology is identical to the analysis performed on the three months of data submitted as part of the Milestone 3 Phase 2 review. Hospitals are required to resolve all issues identified in the review report. Ad hoc support is provided for hospitals unable to resolve the issues identified. Once the hospitals have successfully completed this review, their data is incorporated into the OCCI database.
Details of the review methodologies are found in the Milestone Review Tools link.
OCCI Version 6.1 Page 48 of 53 Effective April 2008 – March 2009 Updated August 2009
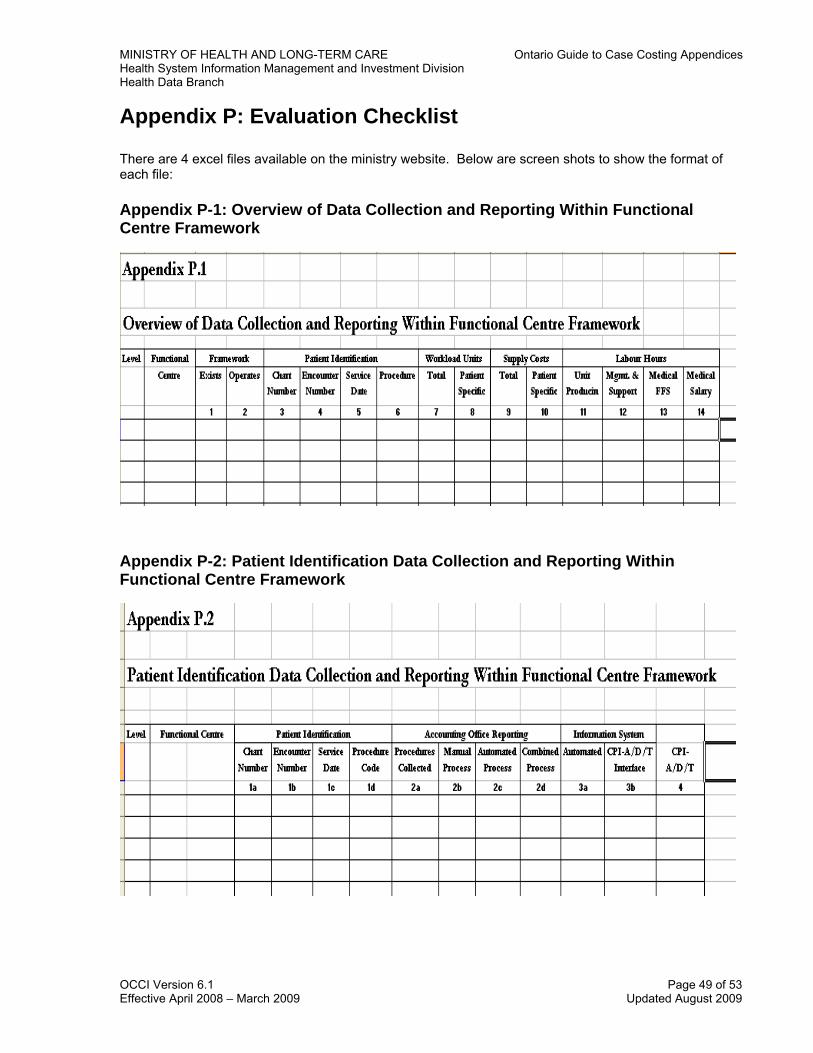
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix P: Evaluation Checklist
There are 4 excel files available on the ministry website. Below are screen shots to show the format of each file: Appendix P-1: Overview of Data Collection and Reporting Within Functional Centre Framework
Appendix P-2: Patient Identification Data Collection and Reporting Within Functional Centre Framework
OCCI Version 6.1 Page 49 of 53 Effective April 2008 – March 2009 Updated August 2009
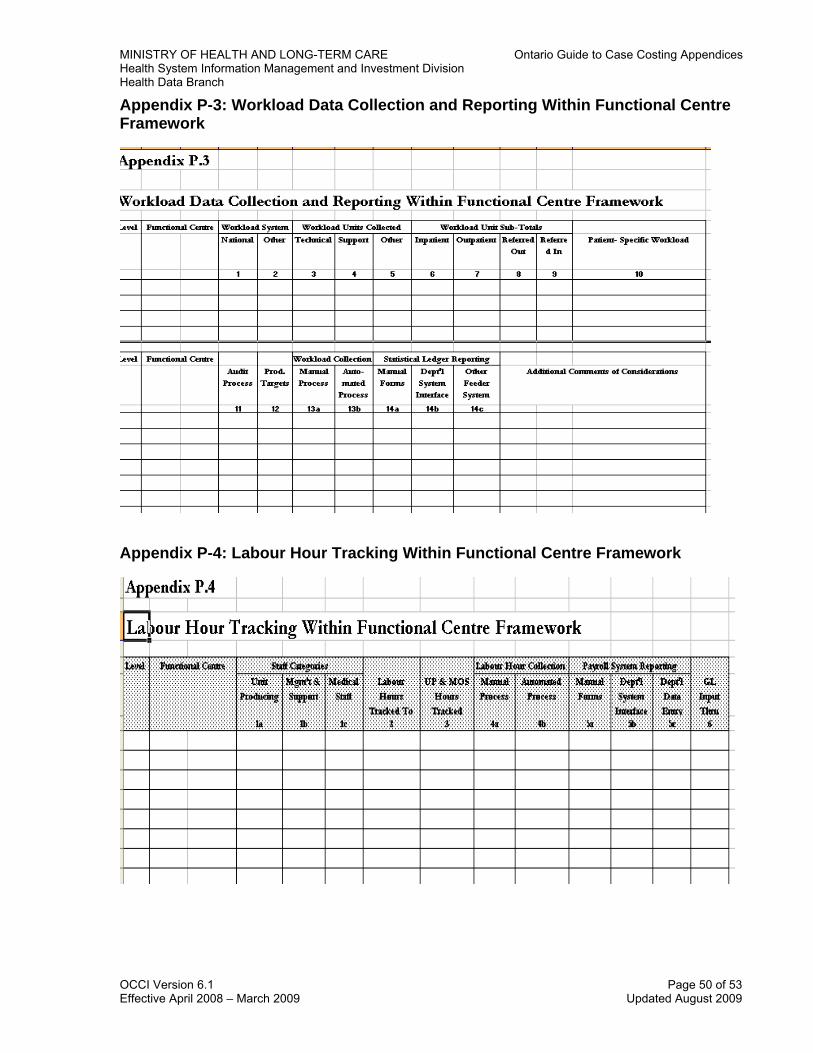
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix P-3: Workload Data Collection and Reporting Within Functional Centre Framework
Appendix P-4: Labour Hour Tracking Within Functional Centre Framework
OCCI Version 6.1 Page 50 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Appendix Q: Nursing Per Hour Weights for Rehabilitation and Complex Continuing Care Patient Groups Nursing Per Hour Weights for Rehabilitation Patient Groups
OCCI Version 6.1 Page 51 of 53 Effective April 2008 – March 2009 Updated August 2009

MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
OCCI Version 6.1 Page 52 of 53 Effective April 2008 – March 2009 Updated August 2009
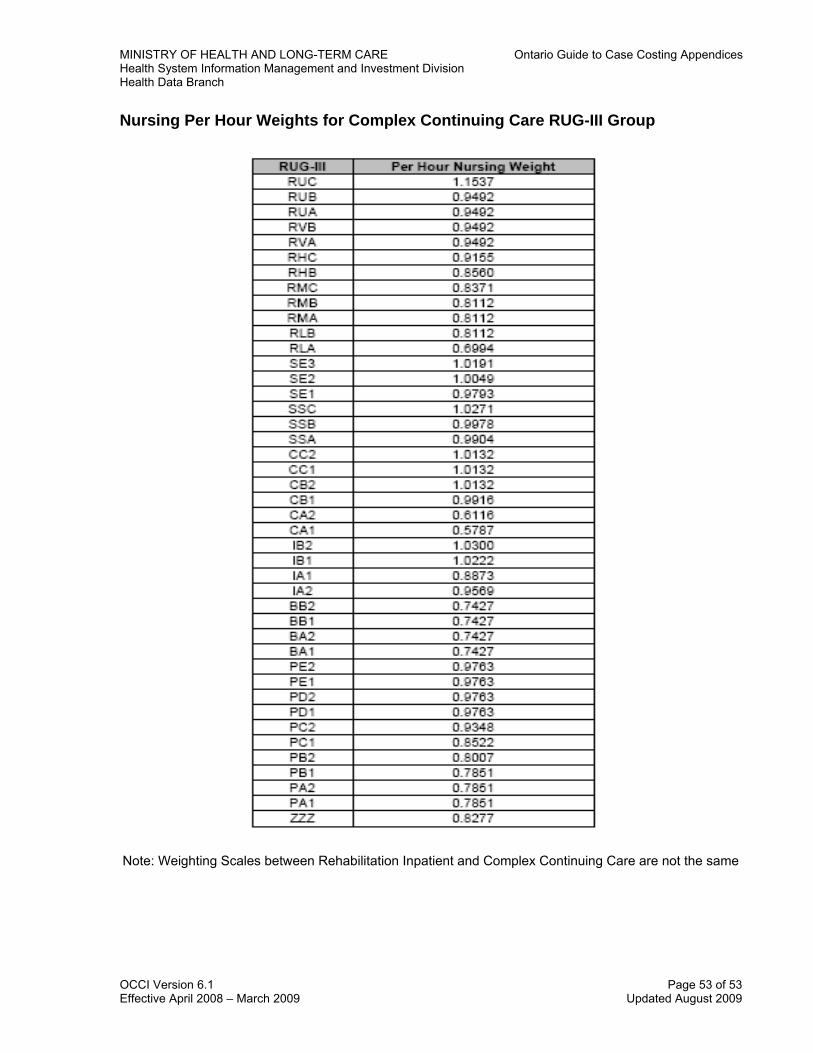
MINISTRY OF HEALTH AND LONG-TERM CARE Ontario Guide to Case Costing Appendices Health System Information Management and Investment Division Health Data Branch
Nursing Per Hour Weights for Complex Continuing Care RUG-III Group
Note: Weighting Scales between Rehabilitation Inpatient and Complex Continuing Care are not the same
OCCI Version 6.1 Page 53 of 53 Effective April 2008 – March 2009 Updated August 2009


















